
Abstract
Background
Posture assessment is an important part of clinical physical examination. Head posture changes should be considered in the measurement of the craniofacial morphology and hyoid bone position.
Objective
To compare the craniofacial morphology and hyoid bone position in the neutral head posture (NHP) and forward head posture (FHP) in healthy individuals.
Methods
Forty healthy participants (16 men and 24 women) were included in this study. Using lateral cephalograms, we assessed the craniofacial, craniocervical, and hyoid bone positions based on 27 distinct variables. The paired-samples t-test and Pearson's correlation analysis were employed to compare the postures.
Results
Significant differences in the craniocervical angles were noted between the NHP and FHP. For the hyoid bone position, all parameters except one presented differences. Vertical variables of craniofacial morphology were influenced by head posture. Pearson's correlation coefficients showed that head posture was significantly correlated with craniofacial morphology, particularly for vertical variables.
Conclusions
This study identified a relationship between the craniocervical and hyoid positions and craniofacial morphology. These findings suggest that different head postures can influence the hyoid position and craniofacial morphology. Hence, for studies involving these parameters and related conditions, maintaining cervical spine posture is crucial.
Introduction
Posture assessment is an important part of clinical physical examination. Different postural alignments can exert distinct stresses on joints, muscles, soft tissues, and bones and can consequently affect them.1–3 Among the alignments, a forward head posture (FHP) is the most common deviation from the neutral head posture (NHP). 4
In the standing lateral view, the earlobe, acromion, and hip are aligned in the NHP.4,5 The NHP provides musculoskeletal balance, which involves a minimal amount of stress and strain on the temporomandibular joint, occlusion, cervical region, and associated muscles.6,7 The FHP is a protracted position in which the lower cervical region is flexed and glides anteriorly, and the upper cervical complex is extended. 8 The FHP increases the load on the neck and fatigue of the neck extensors, 9 affects craniofacial growth, 10 interacts with temporomandibular joint disorder (TMD), changes craniofacial morphology and hyoid bone position,11,12 and affects upper airway morphology. 13 Therefore, head posture changes should be considered in the measurement of the craniofacial morphology and hyoid bone position.
Some studies have explored the relationship between disease classification and cervical posture. For example, the FHP in patients with severe TMD is significantly more pronounced than that in patients with mild TMD. 14 Moreover, TMD with or without disk reduction significantly influences the craniocervical posture and hyoid bone position.11,15 These studies have linked disease to cervical posture or structural morphology. However, no strict cervical spine posture has been defined for cephalograms.
In clinical practice, some patients present with these syndromes but do not exhibit such changes, whereas others do not present with the syndromes but nevertheless exhibit the changes. Patients exhibiting these changes have a common clinical condition: FHP. To our knowledge, no studies have discussed the relationship between the FHP and the craniocervical posture and hyoid bone position, and it remains unclear whether changing the head posture similarly influences the craniocervical posture, hyoid bone position, and craniofacial morphology in individuals without TMD.
This study aimed to compare the craniofacial morphology and hyoid bone position in the NHP and FHP in healthy individuals.
Materials and methods
Participants
Based on data from a previous study,11,15 a sample size of 38 participants was calculated using G*Power, version 3.1.9.2 (Heinrich Heine University Düsseldorf, Düsseldorf, Germany; 1-β: 0.90, α: 0.05, and effect size: 1.029). The inclusion criteria were (1) age of 20–50 years and (2) no history of neck pain within 3 months. The exclusion criteria were (1) cervical spine injuries (fracture, sprain, strain, or whiplash), (2) obvious spinal deformities, (3) neurological or neuromuscular disorders, (4) chronic headache, (5) TMD, (6) rheumatic disease, (7) obstructive sleep apnoea, and (8) balance disorders. 16
This study was conducted in the Rehabilitation Department of Shanghai Ninth People's Hospital, Shanghai Jiao Tong University School of Medicine, between June and July 2023. Procedures involving experiments on human participants were performed in accordance with the ethical standards of the Declaration of Helsinki of 1964. Ethical approval was obtained from the Shanghai Ninth People's Hospital Institutional Ethics Committee (approval code SH9H-2021-TK12-1), and written informed consent was obtained from each participant. All methods described below were performed in accordance with the relevant guidelines and regulations.
Head posture establishment
In this study, we designed and manufactured a fixation device that can be used to fix the head and neck angles during radiation examinations (figure 1). The instrument consists of a cryogenic thermoplastic plate to which several inclinometers are attached to each plane in space. It is composed of two parts: a brace for the trunk and a fixator for fixing the height and front position of the head. The height of the fixator is adjusted based on its position relative to the brace. The front position of the head is changed by adjusting the nut of the fixator.
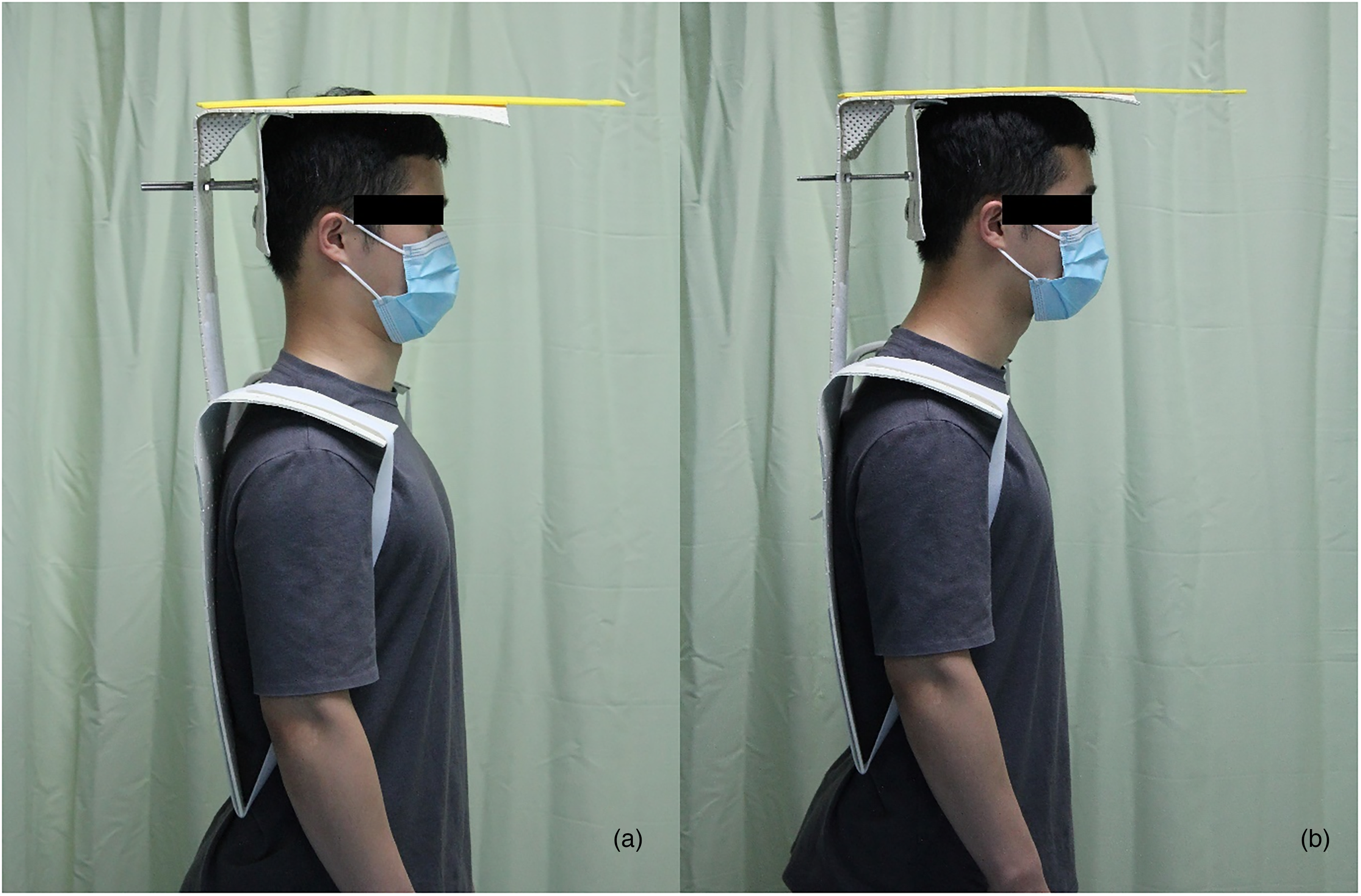
Participant wearing fixation devices in (a) the normal head posture (NHP) and (b) the forward head posture (FHP).
The head and neck postures were determined by measuring the craniovertebral angle (CVA). At present, the CVA is considered to be the most appropriate way to measure the head and neck postures on the body surface.6,16 The CVA is the angle between the horizontal line passing through the spinous process of C7 and a line extending from the tragus of the ear to C7. The NHP alignment in the standing lateral view was fixed to the earlobe acromion in one plane. A smaller CVA indicates a more acute FHP, and a CVA of <48–50° is defined as an FHP. 17 Therefore, in this study, the surface FHP CVA was set at 48°, and the NHP was set at the earlobe and acromion in line. The CVA on the body surface was measured and fixed by a physiotherapist (PT) with 3 years of experience in posture assessment, and another PT immediately placed the fixator on the participant. Lateral cephalometric films of the participants were obtained while they wore the fixation device.
Cephalometric analysis
All cephalograms were obtained by the same radiologist using an AL01C II Collimator (Siemens, Munich, Germany), with an exposure of 0.5 s, a voltage of 70 kV, and a current of 320 mA. For both the NHP and FHP, the participants were given cephalometric films and instructed not to swallow during the cephalometric procedure. The NHP and FHP were determined by the PT.
The lateral cephalograms were traced and measured using medical software (AMIRA, FEI SVG; Thermo Fisher Scientific, Waltham, MA, USA). Twenty landmarks were recorded on each radiograph, and 28 variables, including 11 linear distances and 17 angles, were measured. The positions and definitions of the landmarks are shown in figure 2. Measurements for the craniocervical posture are shown in figure 3, those for the hyoid bone position are shown in figure 4, and those for the craniofacial morphology are shown in figure 5.
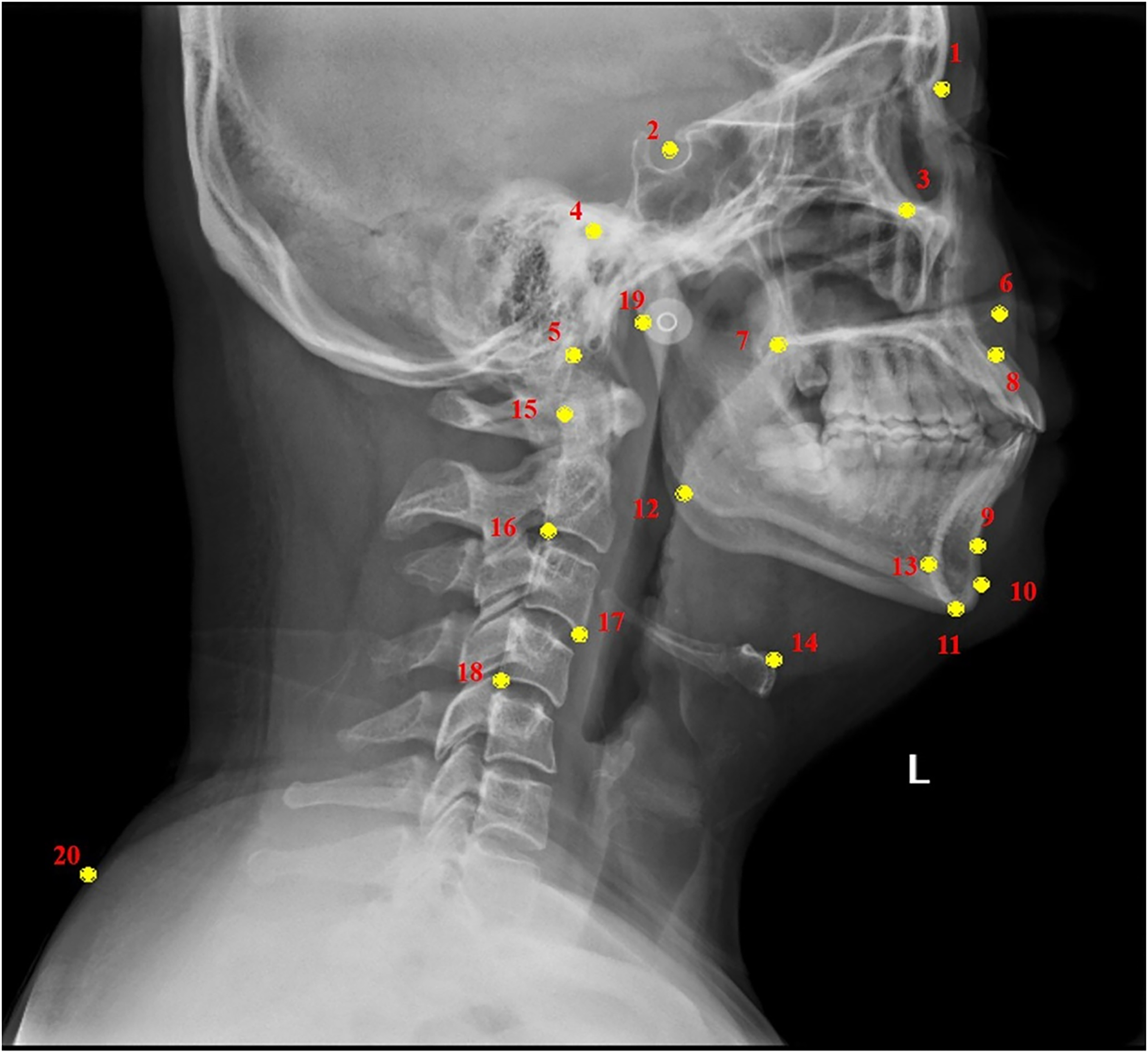
Landmarks used in this study. (1) Nasion; (2) sella; (3) orbitale; (4) porion; (5) basion; (6) anterior nasal spine; (7) posterior nasal spine; (8) point A; (9) point B; (10) pogonion; (11) menton; (12) gonion; (13) retrognathion (RGn) (most protrusive point of retrognathion); (14) hyoidale (Hy; most superior and anterior point on the body of the hyoid bone); (15) cv2tg (tangent point of the superior-posterior extremity of the second cervical vertebra); (16) cv2ip (most posterior-inferior point on the second cervical vertebra); (17) cv3ia (most anterior-inferior point on the third cervical vertebra); (18) cv4ip (most posterior-inferior point on the fourth cervical vertebra); (19) point C (point on the left tragus of the ear); and (20) point D (point at the skin-marker interface at the spinous process of the seventh cervical vertebra).
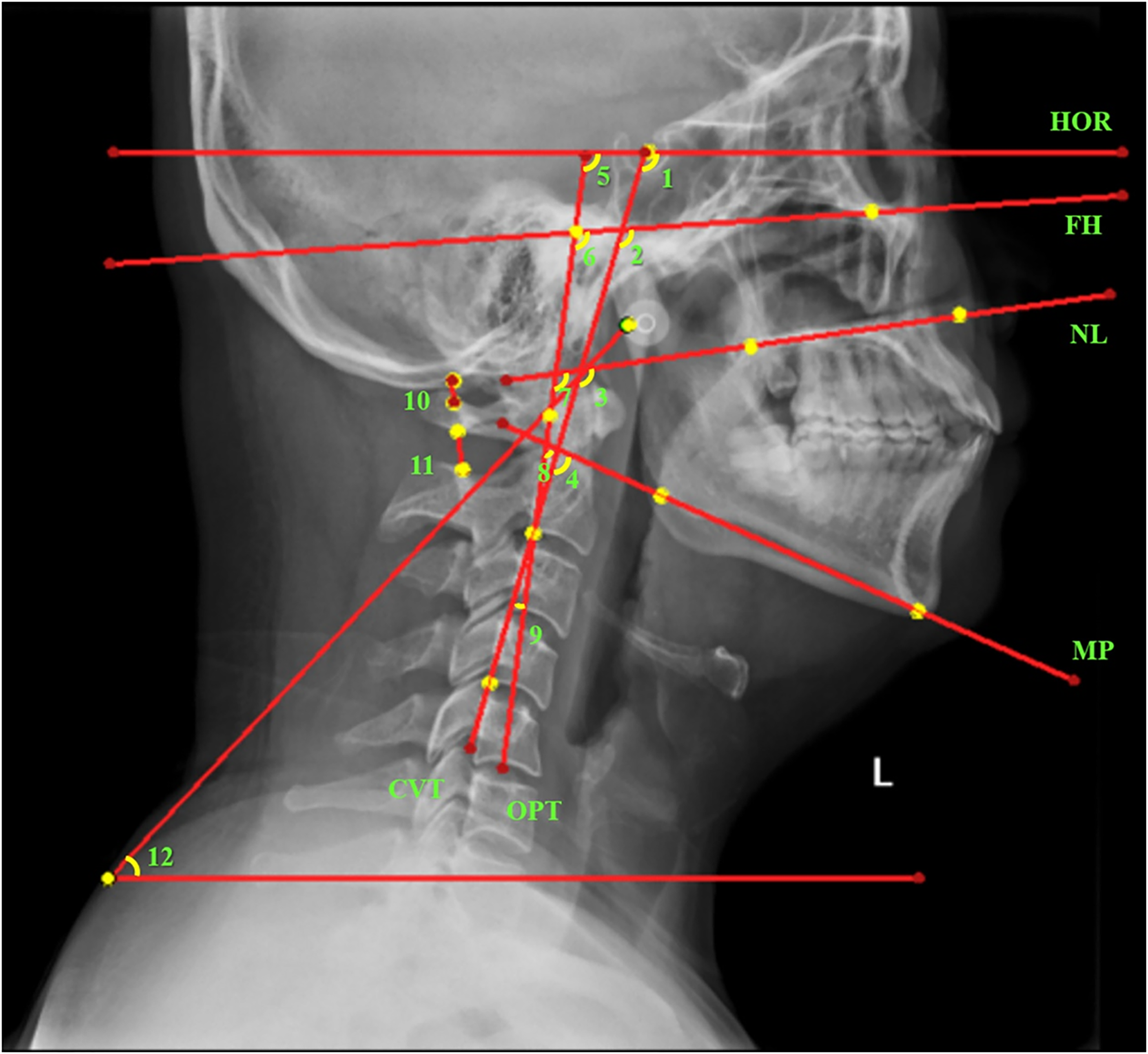
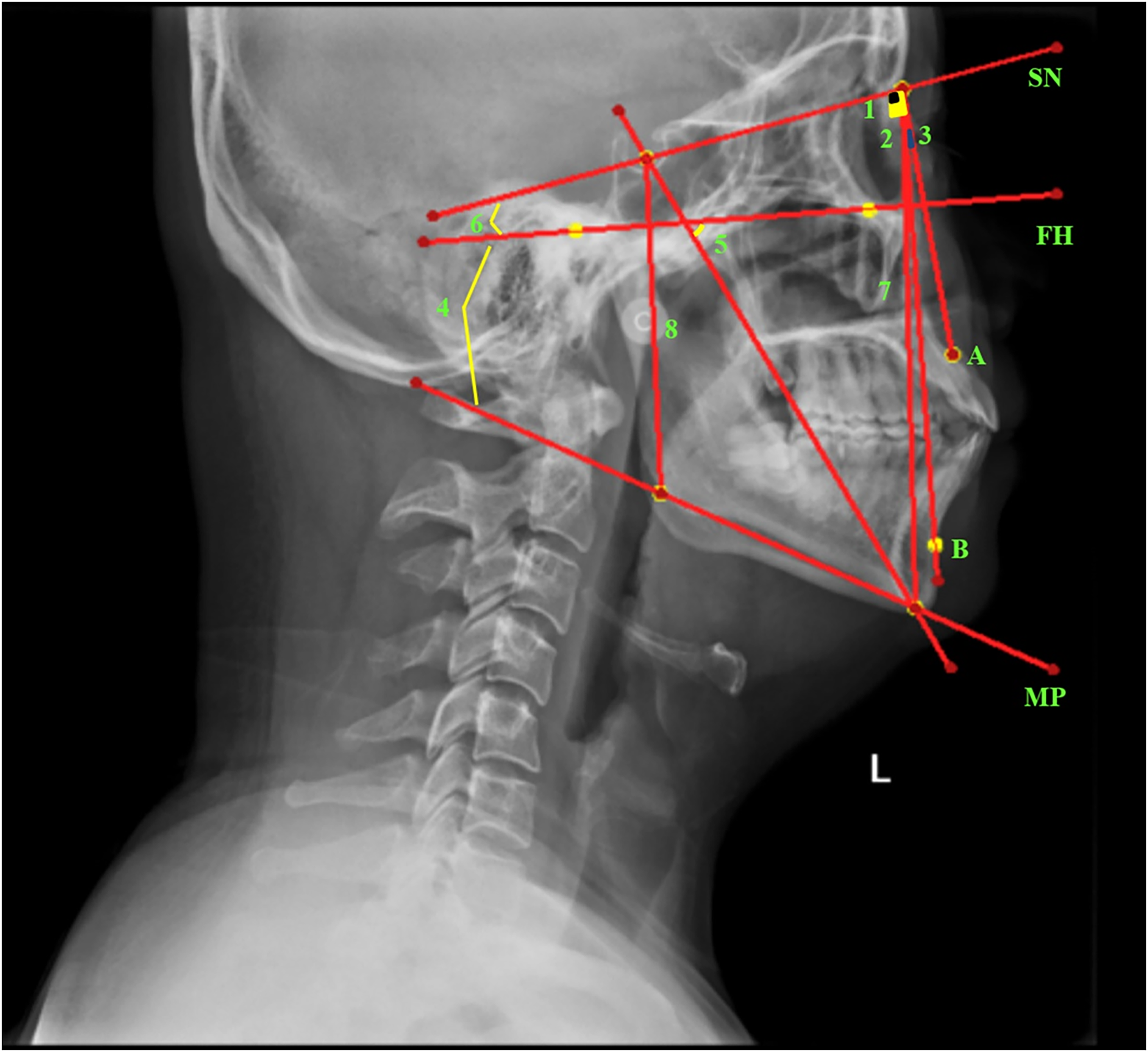
Variables of craniocervical posture. (1) Angle between the true horizontal line and upper part of the cervical vertebrae (HOR/CVT); (2) angle between the Frankfort horizontal line and upper part of the cervical vertebrae (FH/CVT); (3) angle between the nasal line and upper part of the cervical vertebrae (NL/CVT); (4) angle between the mandibular plane and upper part of the cervical vertebrae (MP/CVT); (5) angle between the true horizontal line and odontoid line (HOR/OPT); (6) angle between the Frankfort horizontal line and odontoid line (FH/OPT); (7) angle between the nasal line and odontoid line (NL/OPT); (8) angle between the mandibular plane and odontoid line (MP/OPT); (9) angle between the odontoid line and upper part of the cervical vertebrae (OPT/CVT); (10) linear distance between the base of the occiput and the posterior arch of the atlas (C0–C1); (11) linear distance between the posterior arch of the atlas and spinous process of C2 (C1–C2); and (12) angle between a horizontal reference line and line connecting points C and D (craniovertebral angle [CVA]).
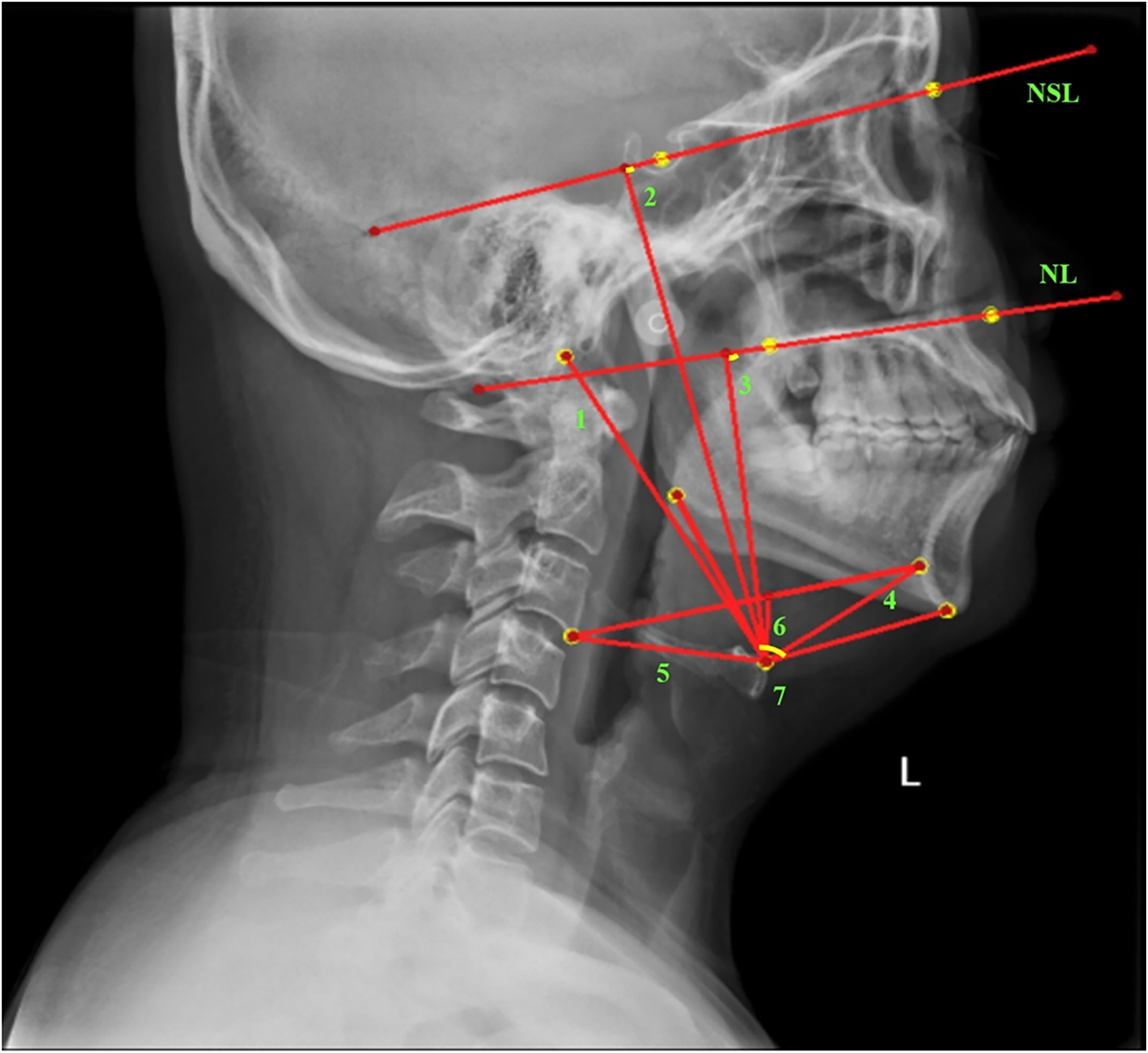
Variables of the hyoid bone position. (1) Linear distance between the hyoidale and basion (Hy–Ba); (2) perpendicular distance between the hyoidale and nasion-sella line (Hy–NSL); (3) perpendicular distance between the hyoidale and nasal line (Hy–NL); (4) linear distance between the hyoidale and retrognathion (RGn) (Hy–RGn); (5) linear distance between the hyoidale and inferior-anterior point on the body of the third cervical vertebra (cv3ia) (Hy–cv3ia); (6) perpendicular distance between the hyoidale and cv3ia–RGn plane (Hy–cv3ia–RGn); and (7) angle between the gonion and hyoidale and menton (Go/Hy/Me).
Variables of craniofacial morphology. (1) Angle between the sella/nasion plane and nasion/A plane (SNA); (2) angle between the sella/nasion plane and nasion/B plane (SNB); (3) angle between lines NA and NB (ANB); (4) angle between the Frankfort horizontal plane and mandibular plane (FMA); (5) angle between the sella-gnathion line and Frankfort horizontal line (Y-axis); (6) angle between the Frankfort horizontal plane and sella/nasion plane (FH/SN); (7) linear distance between the nasion and menton (anterior facial height, AFH); (8) linear distance between the sella and gonion (posterior facial height, PFH); and (9) ratio of the posterior facial height to the anterior facial height (facial height ratio, FHR).
Statistical analyses
Data were evaluated using SPSS software (version 22.0; IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to analyse the normality of the data distribution. The paired-samples t-test was used to compare the two postures when the data showed a normal distribution. Pearson's correlation analysis was employed to determine correlations between the craniofacial and hyoid bone positions and craniofacial variables in both postures. The level of significance was set at p < 0.05.
Results
Forty healthy participants were enrolled in this study, comprising 16 men and 24 women. Their age range was 21–44 years, with a mean age of 26.9 ± 6.6 years. Their mean height and weight were 166.8 ± 8.5 cm and 63.9 ± 15.1 kg, respectively. The craniocervical measurements of the participants are presented in Table 1. Notably, significant differences were observed in all parameters across different head and neck postures. The mean CVA was 55.31 ± 4.65° in the NHP and 43.6 ± 4.61° in the FHP. This last value is consistent with the results of the body surface measurement and meets the definition of an FHP.16,17 As the head extends forward, the linear distance between the base of the occiput and the posterior arch of the atlas (C0–C1) and that between the posterior arch of the atlas and the spinous process of C2 (C1–C2) decreases, and other angles become larger than that in the neutral position. This forward head movement leads to extension of the upper cervical vertebrae and flexion of the lower cervical vertebrae. 18
Comparison of craniocervical measurements between the postures (n = 40).
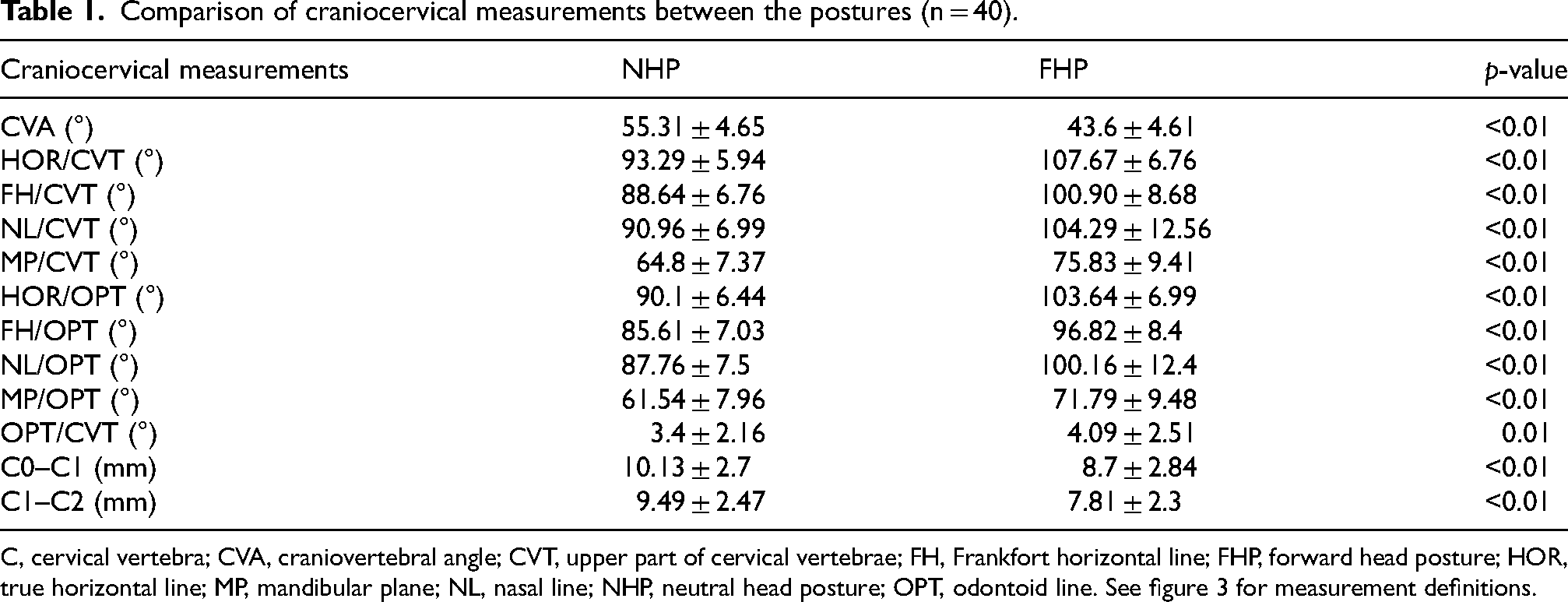
C, cervical vertebra; CVA, craniovertebral angle; CVT, upper part of cervical vertebrae; FH, Frankfort horizontal line; FHP, forward head posture; HOR, true horizontal line; MP, mandibular plane; NL, nasal line; NHP, neutral head posture; OPT, odontoid line. See figure 3 for measurement definitions.
Hyoid bone position measurements of the participants in both the FHP and NHP are shown in Table 2. Notably, significant differences were observed in all parameters between the NHP and FHP, except for the linear distance between the hyoidale and the inferior-anterior point on the body of the third cervical vertebra (cv3ia) (Hy‒cv3ia). This indicates that the position of the hyoid bone relative to C3 was relatively stable, whereas the positions of the skull and mandible shifted. In the FHP, certain measurements decreased, including the linear distance between the hyoidale and basion, the perpendicular distance between the hyoidale and nasion-sella line, the perpendicular distance between the hyoidale and nasal line, the perpendicular distance between the hyoidale and cv3ia–retrognathion (RGn) plane, and the angle between the gonion and hyoidale and menton, while the linear distance between the hyoidale and the RGn (Hy–RGn) increased.
Comparison of hyoid bone position measurements between the postures (n = 40).
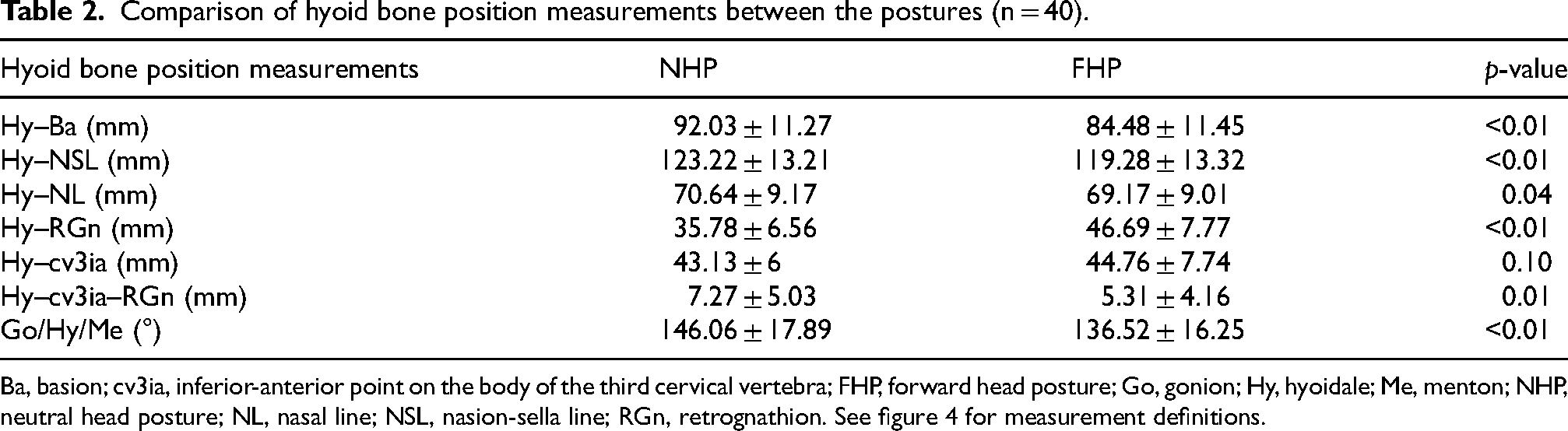
Ba, basion; cv3ia, inferior-anterior point on the body of the third cervical vertebra; FHP, forward head posture; Go, gonion; Hy, hyoidale; Me, menton; NHP, neutral head posture; NL, nasal line; NSL, nasion-sella line; RGn, retrognathion. See figure 4 for measurement definitions.
Craniofacial measurements of the participants are presented in Table 3 and revealed significant differences among the participants in terms of the angle between the Frankfort horizontal plane and mandibular plane (FMA), anterior facial height (AFH), and facial height ratio (all p < 0.05). The FMA and AFH were larger in the FHP than in the NHP.
Comparison of craniofacial morphology measurements between the postures (n = 40).
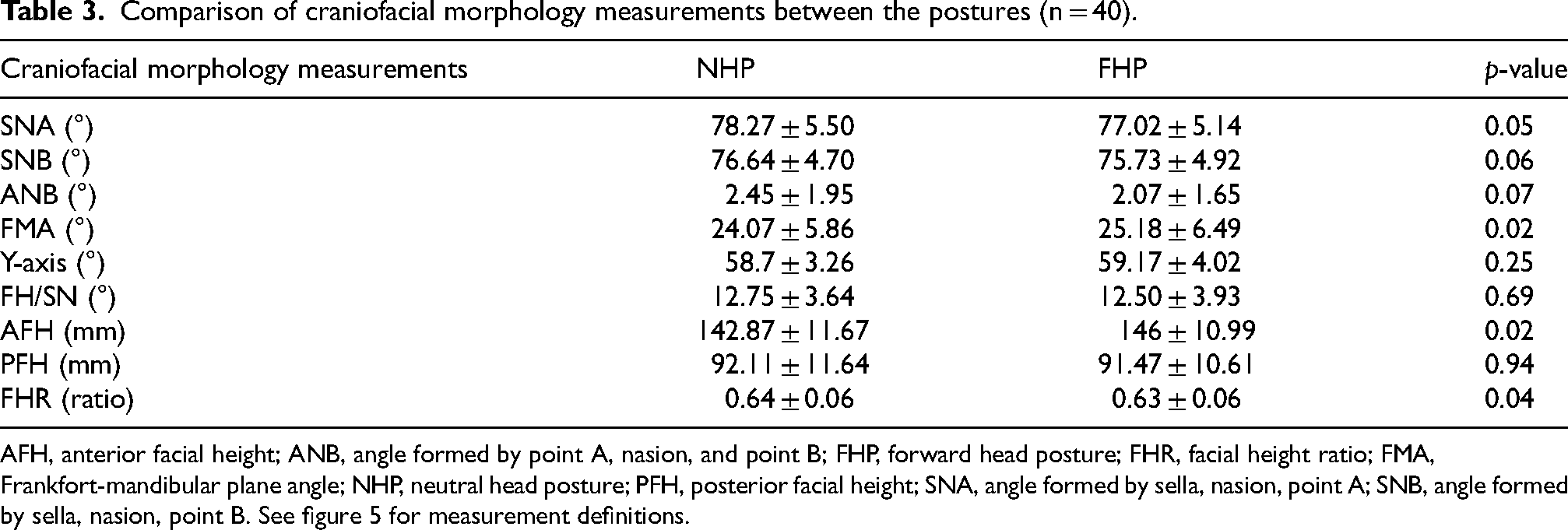
AFH, anterior facial height; ANB, angle formed by point A, nasion, and point B; FHP, forward head posture; FHR, facial height ratio; FMA, Frankfort-mandibular plane angle; NHP, neutral head posture; PFH, posterior facial height; SNA, angle formed by sella, nasion, point A; SNB, angle formed by sella, nasion, point B. See figure 5 for measurement definitions.
The correlations between craniocervical and hyoid bone position measurements and craniofacial measurements are provided in Table 4. Certain craniocervical and hyoid bone position measurements were strongly and positively correlated with craniofacial measurements. Vertical variables, such as AFH and posterior facial height (PFH), were more common among the correlated measurements.
Correlations between craniofacial morphology and craniocervical posture or hyoid bone position in the postures.
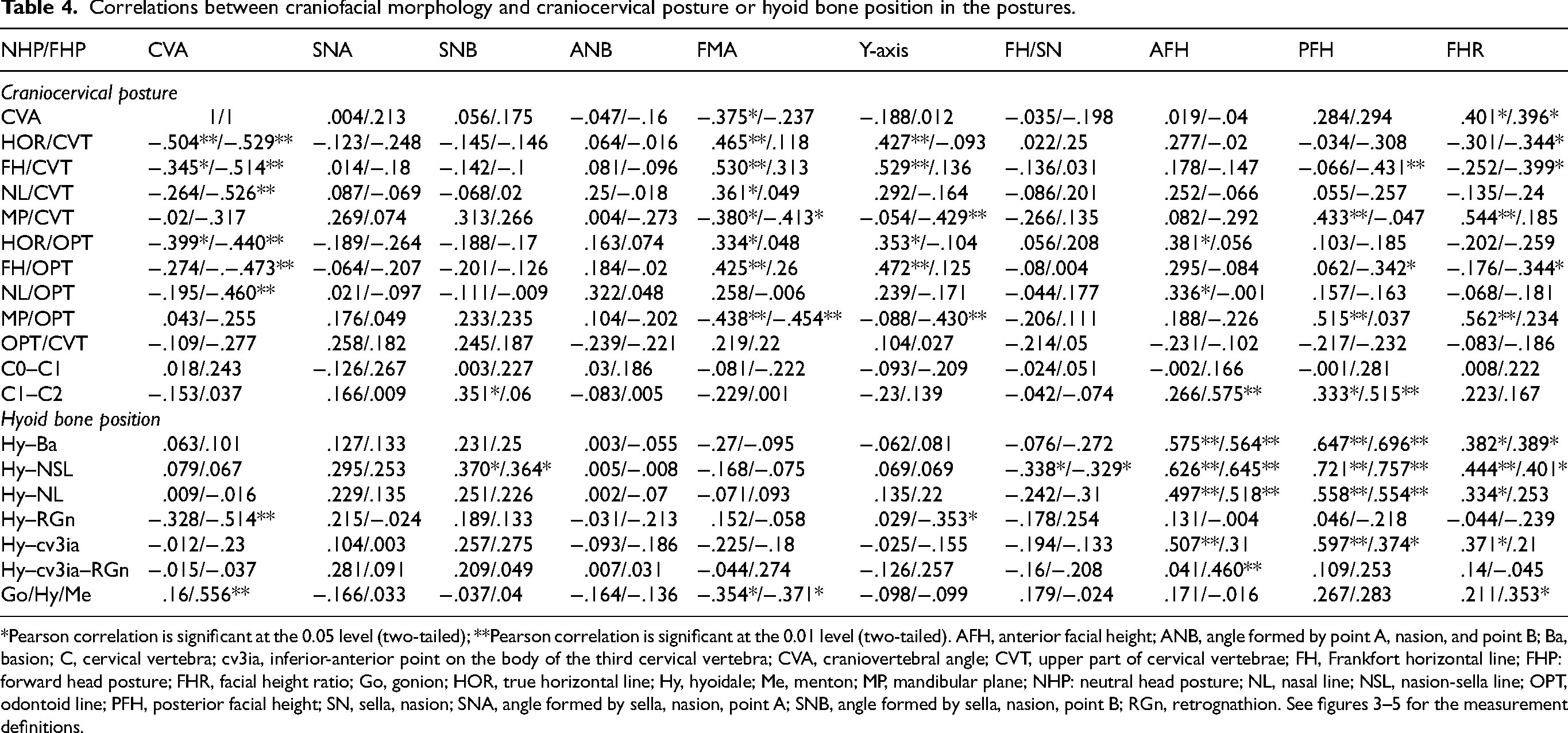
*Pearson correlation is significant at the 0.05 level (two-tailed); **Pearson correlation is significant at the 0.01 level (two-tailed). AFH, anterior facial height; ANB, angle formed by point A, nasion, and point B; Ba, basion; C, cervical vertebra; cv3ia, inferior-anterior point on the body of the third cervical vertebra; CVA, craniovertebral angle; CVT, upper part of cervical vertebrae; FH, Frankfort horizontal line; FHP: forward head posture; FHR, facial height ratio; Go, gonion; HOR, true horizontal line; Hy, hyoidale; Me, menton; MP, mandibular plane; NHP: neutral head posture; NL, nasal line; NSL, nasion-sella line; OPT, odontoid line; PFH, posterior facial height; SN, sella, nasion; SNA, angle formed by sella, nasion, point A; SNB, angle formed by sella, nasion, point B; RGn, retrognathion. See figures 3–5 for the measurement definitions.
Discussion
To the best of our knowledge, this cross-sectional study is the first to investigate changes in the craniofacial morphology and hyoid bone position between the NHP and FHP in healthy individuals. During the testing phase, a large X-ray frame was selected to capture the cervical spine position, while a specially designed and manufactured head and neck brace was used to stabilise the head and neck. We found that the positions of the craniocervical bone and hyoid bone and craniofacial morphology changed under different head and neck postures. Moreover, a significant correlation was observed among the craniocervical position, hyoid bone position, and vertical craniofacial morphology. These results are consistent with those of previous studies.3,7,17,19
The craniocervical position is directly influenced by the cervical spine position. Compared with the NHP, the FHP causes the upper cervical vertebrae to extend and the lower cervical vertebrae to flex, 18 resulting in significant disparities across all measurements. Specifically, owing to the extension of the upper cervical vertebrae, the C0‒C1 and C1‒C2 decrease. In our study, the average C0‒C1 and C1‒C2 values in the NHP were 10.13 ± 2.7 mm and 9.49 ± 2.47 mm, respectively, while those in the FHP were 8.7 ± 2.84 mm and 7.81 ± 2.3 mm, respectively. Notably, Matheus et al. 12 examined 60 participants and discovered that in healthy individuals, 57% of the C0‒C1 values were between 4 and 9 mm, with the remaining exceeding 9 mm. Furthermore, the proportions of C1‒C2 were 81% and 14%, respectively. However, these results did not consider head and neck postures, nor did they provide an average measurement, which may result in biases. The C0‒C1 and C1‒C2 values obtained in our study are thus more reliable. The decrease in C0‒C1 and C1‒C2 values may cause tension in the posterior cervical muscles and their fascia. This may in turn lead to compression of occipital nerves and headaches. 20 Therefore, adjusting cervical posture may help prevent these symptoms. 21
Additionally, the overall movement of the cervical vertebrae contributed to the significant increase observed in the angle between the true horizontal line and upper part of the cervical vertebrae, between the Frankfort horizontal line and upper part of the cervical vertebrae, between the nasal line and upper part of the cervical vertebrae, between the mandibular plane and upper part of the cervical vertebrae, between the true horizontal line and odontoid line, between the Frankfort horizontal line and odontoid line, between the nasal line and odontoid line, between the mandibular plane and odontoid line, and between the odontoid line and upper part of the cervical vertebrae.
The hyoid bone is a ‘floating bone’, and its position is affected by muscles, 22 posture, 23 breathing and chewing patterns, and craniofacial morphology. 3 As the head moves forward, the hyoid bone is fixed in relation to the third cervical vertebra, and there is no difference in the Hy‒cv3ia. Using cone-beam computed tomography, Chen et al. 24 reported the same results in patients with skeletal Class I and II with different vertical growth patterns. Simultaneously, the hyoid bone moves away from the mandible and closer to the skull. The Hy‒RGn in the FHP (46.69 ± 7.77 mm) was larger than that in the NHP (35.78 ± 6.56 mm) in our study, with other parameters showing smaller values. This means that the hyoid bone moves downward and backward, causing it to be free of suspensory muscular actions. 19 Extended maintenance of the FHP may alter muscular activity and influence facial morphology, potentially resulting in dolichofacial features, a Class II skeletal frame, and substantial divergence of the maxillary bases. 25 These changes in the hyoid position and FHP may also be related to TMD, 6 obstructive sleep apnoea, 26 and Class II skeletal malocclusion, 24 among other conditions.
The present study showed that the vertical variables of craniofacial morphology, such as the AFH and PFH, can be significantly influenced by head posture. Across different postures, the craniocervical and hyoid positions were mostly related to the angle formed by the sella, nasion, and point B; FMA; and AFH. The FHP caused the mandible to retract and rotate clockwise. However, previous studies in patients with TMD11,27 or skeletal Class II malocclusion 23 showed similar results, although the specific CVA was not standardised. This suggests the need for further research into the standardisation of the craniocervical position in patients. According to the design of our study, participants can be grouped based on their classified craniocervical angle for subsequent analyses. As the craniocervical and hyoid positions have a direct impact on facial structure, it is advisable for clinicians to evaluate these relationships before initiating orthodontic treatment. In particular, mandibular retraction and rotation and hyoid bone subsidence may cause decreased swallowing strength or TMD during orthodontic treatment.
This study had some limitations. This was a cross-sectional study that included healthy participants and excluded individuals with relevant medical conditions. Future research endeavours should explore the relationship between craniocervical and hyoid positions and craniofacial morphology in patients with TMD or malocclusion. Additionally, this study had a small sample size. Therefore, future studies should assess these relationships and confirm our results using a larger population of participants.
Conclusions
This study revealed a significant relationship between craniocervical and hyoid positions and craniofacial morphology. Moreover, our findings underscore the impact of varying head postures on hyoid position and craniofacial morphology. These interconnected factors emphasise the importance of maintaining optimal cervical spine posture. Moving forward, studies investigating the nexus between these parameters and related diseases should prioritise the role of cervical spine posture as a potential avenue for prevention and intervention.
Footnotes
Acknowledgements
The authors have no acknowledgements.
Ethical approval
Ethical approval was obtained from the Shanghai Ninth People's Hospital Institutional Ethics Committee (approval code SH9H-2021-TK12-1).
Informed consent
Written informed consent was obtained from each participant.
Author contributions
Conceptualisation, JY, LJ, and RC; data curation, JY and RC; formal analysis, LJ and XL; production of brace, YY; funding acquisition, LX and BC; methodology, JY and RC; project administration, JY, LJ, RC, BC,ZF, and T-yT; resources, LJ and ZF; software, RC and T-yT; supervision, JY, SC, LX, and T-yT; validation, JY, LJ, LX, and RC; visualisation, SC and XL; writing—original draft, JY, LJ, and RC; writing—review and editing, JY, RC, and T-yT. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Shanghai Municipal Health Commission Key Supporting Disciplines [grant number 2023ZDFC0303], the Cross-disciplinary Research Fund of Shanghai Ninth People's Hospital, Shanghai JiaoTong University School of Medicine [grant number JYJC202307], and the Fundamental Research Funds for the Central Universities [grant number YG2021QN70].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available from the corresponding author (Z.F), upon reasonable request.