
Abstract
Background
Low back pain (LBP) is a leading contributor to global disability, with lumbar disc herniation (LDH) being a common etiology. Despite the coexistence of LDH and piriformis muscle thickness, their potential relationship remains underexplored.
Objective
To investigate the correlation between LDH and piriformis muscle thickness in individuals diagnosed with LDH with no history of piriformis syndrome.
Methods
This cross-sectional study enrolled 107 participants diagnosed with LDH at the Neurology Outpatient Clinic in Siloam Hospital from September to November 2024. Piriformis muscle thickness was measured bilaterally using ultrasonography. Demographic data, clinical presentations, and magnetic resonance imaging (MRI) findings were collected.
Results
The mean age was 54.39 ± 12.69 years, with 58.9% being male. Affected sides demonstrated significantly increased piriformis muscle thickness compared to the unaffected sides (1.17 ± 0.22 cm vs. 0.93 ± 0.18 cm, p < 0.05). Age, weight, and body mass index (BMI) significantly influenced piriformis muscle thickness on the affected side. Age exhibited a negative correlation (r = −0.308), whereas weight and BMI demonstrated positive correlations (r = 0.218/0.192).
Conclusion
This study highlights significant thickening of the piriformis muscle on the affected side in patients with LDH, likely due to mechanical and inflammatory adaptations.
Keywords
Introduction
Low back pain (LBP), is defined as pain originating from the area between the 12th rib and the inferior gluteal fold with or without radiation to the lower limbs. It is one of the most prevalent conditions worldwide, exerting a significant disease burden. 1 According to the 2020 Global Burden of Disease Report, LBP affects approximately 619 million people worldwide, and this number is projected to increase to 843 million cases by 2050. It is the leading cause of disability worldwide, as measured by years lived with disability (YLD), indicating substantial socioeconomic implications.2,3 The incidence of LBP increases with age, peaking in individuals aged 50 to 55, highlighting its significance in ageing populations. Among the numerous etiologies of LBP, lumbar disc herniation (LDH) is one of the most common aetiology, with an annual incidence ranging from 5 to 20 cases per 1000 adults. 4 LDH is characterized by the displacement of the intervertebral disc material, resulting in nerve root compression manifesting as radicular pain, motor weakness, and sensory deficits. These symptoms often mimic or overlap with those caused by piriformis syndrome, a condition involving sciatic nerve entrapment by the piriformis muscle in the gluteal region.5,6
The piriformis muscle plays a pivotal role in hip stability and movement, functioning as an external rotator, abductor, or flexor, depending on the body's position. Originating from the sacrum and inserted into the greater trochanter, the muscle lies in close proximity to the sciatic nerve, making it susceptible to morphological changes that may lead to nerve compression, particularly in patients with LDH.7,8 Case reports have frequently documented the co-occurrence of LDH and piriformis syndrome, including instances in which piriformis syndrome emerged as a complication of LDH.9–12 However, despite extensive research into the management of LDH and piriformis syndrome as two distinct conditions, the relationship between these pathologies remains poorly understood. LDH can disrupt postural alignment, causing lumbopelvic instability that places increased mechanical stress on the piriformis muscle, leading to further hypertrophy as an adaptive response to stabilize the pelvis. 13 Mechanical compression of the nerve roots in LDH can trigger neuronal apoptosis in the dorsal root ganglion, leading to the release of proinflammatory cytokines such as TNF-α, which contributes to muscle spasms, oedema, and altered neuromuscular function, ultimately inducing compensatory hypertrophy of the piriformis muscle and exacerbating sciatic nerve irritation. 14 Recent anatomical study highlights the topographic proximity between the piriformis muscle and sacral nerve branches, particularly S1 and S2, as a potential anatomical basis for deep gluteal and piriformis syndromes. 15 This intimate relationship implies that even minor changes in nerve structure can affect the piriformis muscle and vice versa, potentially contributing to pain and dysfunction. Furthermore, a longitudinal study indicates that patients with current LBP may exhibit adaptive hypertrophy of the piriformis muscle, reflected by increased cross-sectional area. 16 Beyond this, morphological changes in the piriformis muscle have also been observed in axial spondyloarthritis, with a reported 10% incidence of radiological signs suggestive of piriformis syndrome, 17 indicating that morphological alterations of pelvic muscles may occur as a response to spinal pathologies. Supporting these observations, recent shear wave elastography studies in athletes demonstrated significantly increased piriformis muscle stiffness in unexplained LBP, 18 highlighting reflex spasms possibly triggered by sacroiliac and facet joint dysfunctions. These findings reinforce the hypothesis that spinal pathologies can induce secondary morphological and functional changes in the piriformis muscle.
Advances in musculoskeletal imaging, such as ultrasound and magnetic resonance imaging (MRI), have significantly improved the evaluation of soft tissue structures, including muscle thickness and morphology. Ultrasonography in particular offers a practical, safe, and cost-effective imaging modality for dynamic assessments of muscle thickness and morphology without exposure to ionizing radiation.19–21 Evaluating piriformis muscle thickness in patients with LDH represents a novel approach in understanding the potential relationship between spinal and pelvic pathologies, particularly in cases presenting with radicular symptoms.
Although various causes of piriformis syndrome, such as age, previous gluteal injuries, overuse, and poor lifestyle, have been identified, 22 the relationship between piriformis syndrome and LDH has not yet been objectively studied. Existing research primarily highlights an association between piriformis syndrome and increased piriformis muscle thickness, as measured by ultrasonography. 23 For example, a study by Othman et al. in Malaysia reported a statistically significant difference in the mean thickness of the piriformis muscle between individuals with and without LBP. 13 Despite these findings, a notable gap exists in the literature, as no studies have yet assessed piriformis muscle thickness specifically in patients with LDH with no prior history of piriformis syndrome symptoms. Therefore, this study aims to address this knowledge gap by investigating the correlation between herniated lumbar discs and piriformis muscle thickness using ultrasonography in individuals with LDH who have no prior history of piriformis syndrome symptoms.
Materials and methods
This cross-sectional study was conducted from September to November 2024 involving 107 participants diagnosed with LDH confirmed by clinical assessment and MRI at the Neurology Outpatient Clinic, Siloam Hospital Lippo Village, Tangerang, Indonesia. Participants were recruited using a consecutive sampling method to ensure systematic and unbiased selection. All subjects met predefined inclusion and exclusion criteria to enhance the reliability of the data. This study was conducted in accordance with ethical principles and was approved by the Ethics Committee of the Faculty of Medicine, Pelita Harapan University (approval number: 253/K-LKJ/ETIK/IX/2024). Written informed consent was obtained from all participants prior to their enrollment in the study.
Inclusion criteria
Participants aged 18 to 80 years who were cooperative and diagnosed with LDH were considered eligible. Diagnosis was established based on a comprehensive clinical evaluation, detailed medical history, MRI findings, and clinical examination. Clinical symptoms indicative of active radiculopathy—such as pain, hypoesthesia, paresthesia, or paresis—were required for inclusion, supported by positive findings on physical examination, including Lasegue's Straight Leg Raise (SLR) test and Bragard's test. MRI findings confirmed the presence of disc pathology, such as bulging, protrusion, extrusion, or sequestration with associated nerve root irritation. Nerve irritation was defined based on specific radiological criteria, including lateral recess narrowing and neural foraminal stenosis, as evaluated by a board-certified radiologist. In cases of multiple or parallel disc herniations, documentation was based on the clinically active lesion, corresponding to the dermatomal pain distribution. Patients presenting with unilateral symptoms were included even if MRI demonstrated bilateral involvement, with documentation focused on the symptomatic side. However, patients with significant bilateral symptoms and MRI-confirmed bilateral neural compression were excluded to reduce potential confounding factors.
Exclusion criteria
Participants with a history of hip or buttock pain, previous lumbar or hip surgery, spinal deformities, psychiatric disorders, autoimmune diseases, or a confirmed diagnosis of piriformis syndrome were excluded from this study. The diagnosis of piriformis syndrome was determined by the presence of clinical signs and positive outcomes on one or more diagnostic physical tests, including external palpation of the piriformis region, the flexion, adduction, and internal rotation (FAIR) test, Pace's sign, Freiberg's sign, and the Beatty maneuver. Additionally, participants with asymptomatic degenerative changes alone, such as age-related spondylotic findings without clinical or radiological evidence of active nerve root irritation, were also excluded.
Measurement of piriformis muscle thickness
Each participant was instructed to lie in a prone position on the examination table. An imaginary line was drawn connecting the midpoint of the sacral border and the greater trochanter to guide the probe placement. Clear ultrasound gel was applied, and a curvilinear probe with a 3.5 MHz to 5 MHz transducer was positioned along the longitudinal plane of the imaginary line, producing an image as shown in (Figures 1 and 2). The sonologist then adjust the probe's position to identify the piriformis muscle by moving it caudally, at which point two distinct muscle layers, the gluteus maximus, and the piriformis muscle, became visible. The participant's knee was flexed, and the hip joint was rotated externally and internally to confirm the piriformis muscle while optimizing the depth and focus of the ultrasound image. Piriformis muscle thickness was measured at the medial tip of the ischium, parallel to the longitudinal plane at the sciatic notch. All ultrasound examinations were conducted by a single certified interventional pain sonologist using the PHILIPS AFFINITI 70, serial number US117F776. A single certified interventional pain sonologist performed all ultrasound examinations, with reliability ensured by averaging three consecutive measurements per side. All ultrasound measurements were obtained on the same day as the initial clinical assessment. The sonologist was blinded to the symptomatic side to minimize observer bias during measurements.
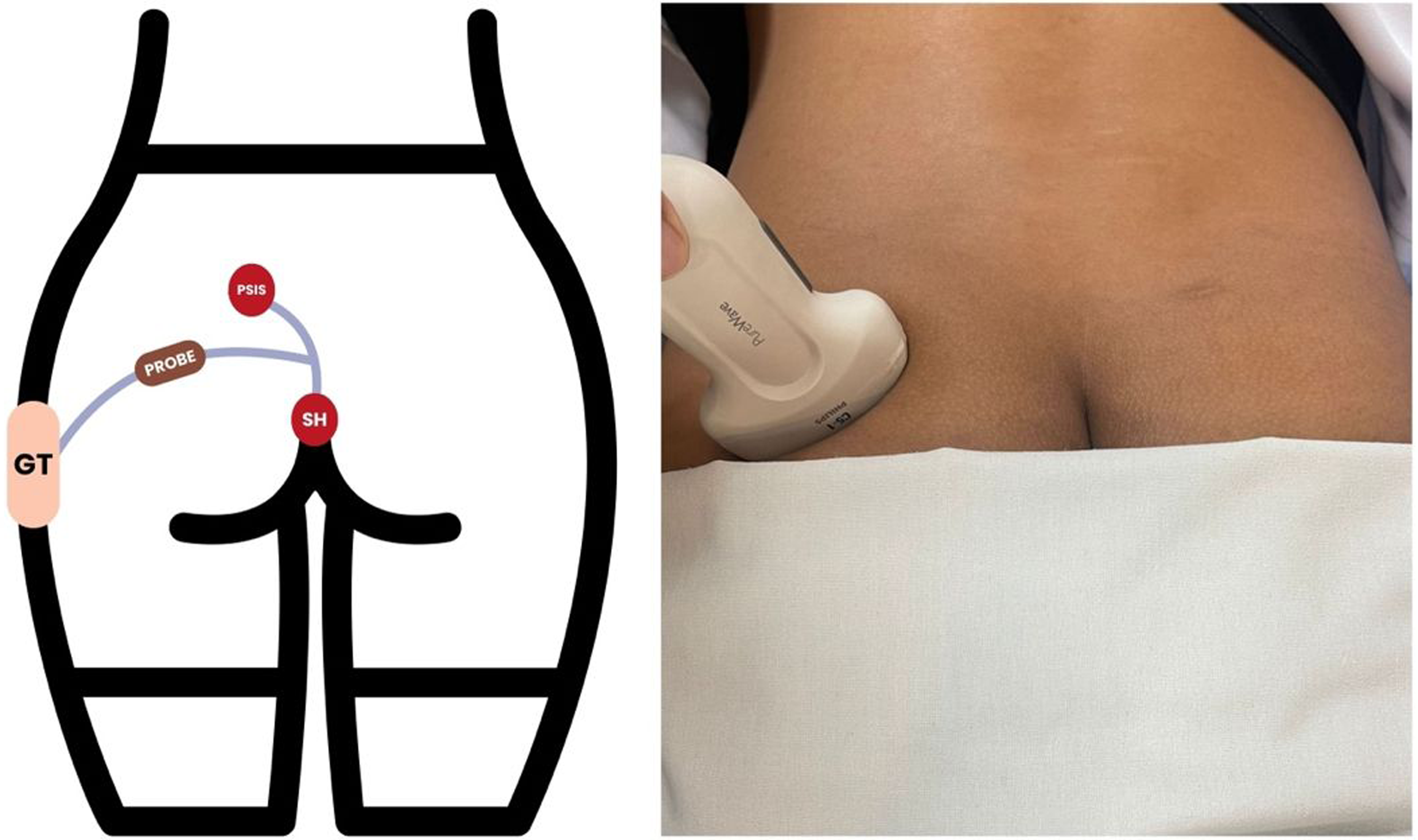
The location for ultrasound probe placement to identify the piriformis muscle (defined as the midpoint of an imaginary line between the sacral border and the greater trochanter).
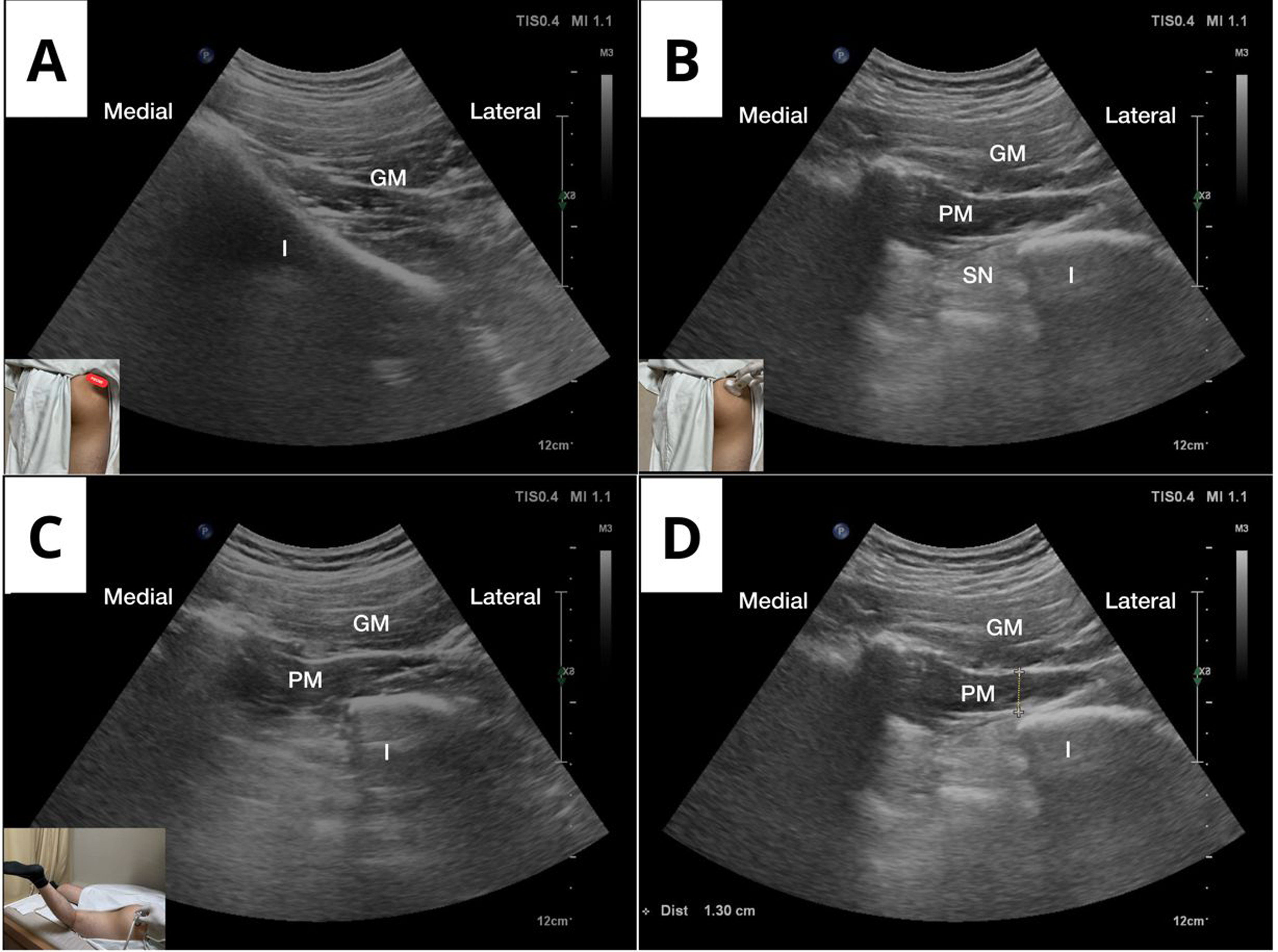
Longitudinal ultrasonographic images of the piriformis muscle (PM) were captured using a curvilinear transducer set at 2.5–5 MHz. Initial probe placement was performed at the midpoint between the sacral border and the greater trochanter. B. Caudal probe adjustment to enhance visualization of the piriformis muscle. C. Ultrasound image acquired with the subject's leg abducted and internally rotated, D. Thickness measurement: the piriformis muscle was measured at the medial part of the ischial tip, parallel to the longitudinal plane at the sciatic notch.
Statistical analyses
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 27. The Kolmogorov-Smirnov test was used to assess data normality. Normally distributed data are presented as the mean ± standard deviation (SD), while non-normal data are reported as the median with interquartile range. Categorical variables are represented as frequencies and percentages. The reliability of muscle thickness measurements obtained via ultrasound was assessed using the Intraclass Correlation Coefficient (ICC) with a two-way mixed-effects model and consistency definition. Given that three repeated measurements were averaged, ICC(3,k) was calculated to evaluate the reliability of the mean values. The ICC values were interpreted as follows: poor (<0.50), moderate (0.50–0.75), good (0.75–0.90), and excellent (>0.90).
Paired T-testing was used compared the thickness of the piriformis muscle on the affected and unaffected sides. A post-hoc power analysis was conducted to evaluate the adequacy of the sample size used in this study (n = 107). This analysis was performed in G*Power version 3.1, applying a paired t-test model with a two-tailed hypothesis. The effect size (dz) was determined to be 1.05, based on the observed differences between group means and standard deviations. An alpha level of 0.05 was utilized to calculate the statistical power (1-β), which was found to be 0.99. This value exceeds the generally accepted threshold of 0.80, indicating that the sample size was sufficient to detect significant effects with a very large effect size.
Additionally, factors influencing piriformis muscle thickness were analyzed. Pearson correlation was performed to assess relationships between numerical variables and piriformis muscle thickness for normally distributed data, while Spearman correlation was applied for non-normally distributed data. Differences in muscle thickness based on categorical variables were evaluated using the one-way analysis of variance test (ANOVA) for comparisons between the affected and unaffected sides. Linear regression analysis was also performed to examine the influence of age, body weight, and body mass index on piriformis muscle thickness. A two-tailed p-value of < 0.05 was considered statistically significant for all analyses.
Results
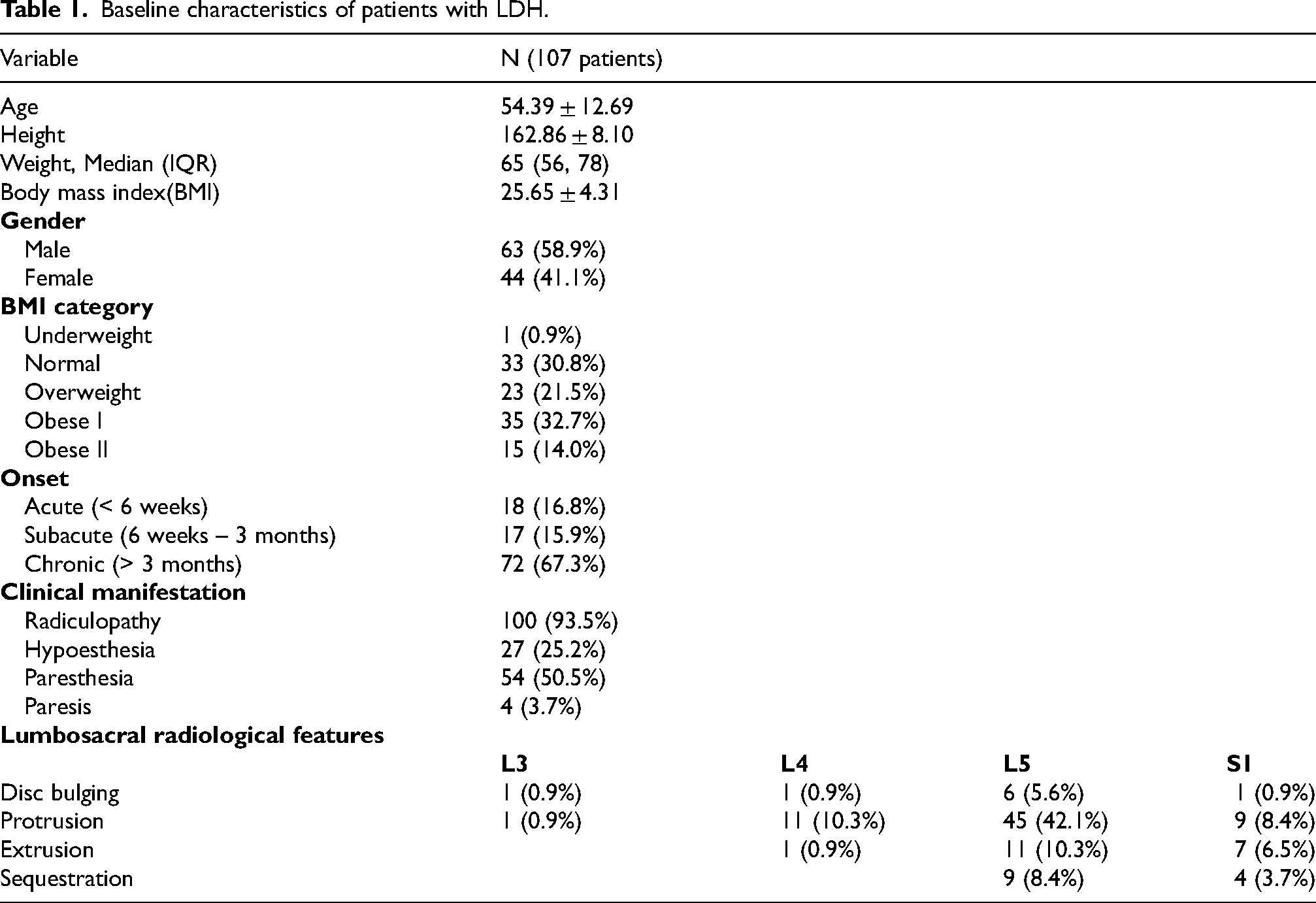
This study included 107 patients clinically and radiographically diagnosed with LDH with a mean age of 54.39 ± 12.69 years. Table 1 summarizes the demographic and anthropometric characteristics of the participants. Most participants were male (58.9%), with an average body mass index (BMI) of 25.65 ± 4.31; overall, 32.7% were categorized as obese class I, and 14.0% as obese class II. Symptom onset was reported as acute in 16.8%, subacute in 15.9%, and chronic in 67.3% of participants. Clinical manifestations included radiculopathy (93.5%), paresthesia (50.5%), hypoesthesia (25.2%), and paresis (3.7%).
Baseline characteristics of patients with LDH.
Data normality was assessed using the Kolmogorov-Smirnov test, which yielded a p-value greater than 0.05, confirming a normal distribution. The intra-rater reliability analysis of the ultrasound measurement, based on three repeated sonographic muscle thickness measurements, demonstrated excellent reliability, with ICC(3,k) values of 0.909 for the affected side (95% CI: 0.874–0.935) and 0.870 for the unaffected side (95% CI: 0.821–0.908) (Table 2). A paired t-test was subsequently used to compare the thickness of the piriformis muscle between the affected and unaffected sides. The results showed a significant difference, with the affected side exhibiting a mean thickness of 1.17 ± 0.22 cm compared to 0.93 ± 0.18 cm on the unaffected side (p < 0.05) (Table 2).
Intra-Rater reliability and comparison of Piriformis muscle thickness in patients with lumbar disc herniation.

Further analysis examined the relationship between piriformis muscle thickness and demographic as well as clinical variables. On the affected side, a significant negative correlation was found between age and muscle thickness (r = −0.308, p = 0.001), while weight (r = 0.218, p = 0.024) and BMI (r = 0.192, p = 0.047) were positively correlated. No significant correlations were observed with height (p = 0.210) or Numeric Rating Scale (NRS) pain scores (p = 0.198). On the unaffected side, only age showed a significant negative correlation (r = −0.252, p = 0.009), with no other variables showing significant associations (Table 3). These findings indicate that age, weight, and BMI may influence piriformis muscle thickness, particularly on the affected side.
Correlation between the Piriformis muscle thickness and demographic, anthropometric, and clinical variables in patients with LDH.
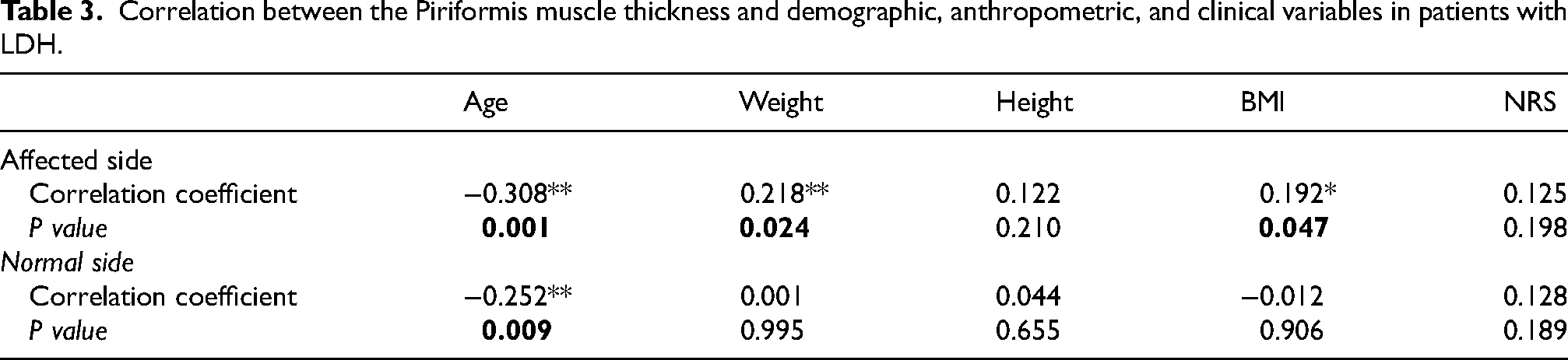
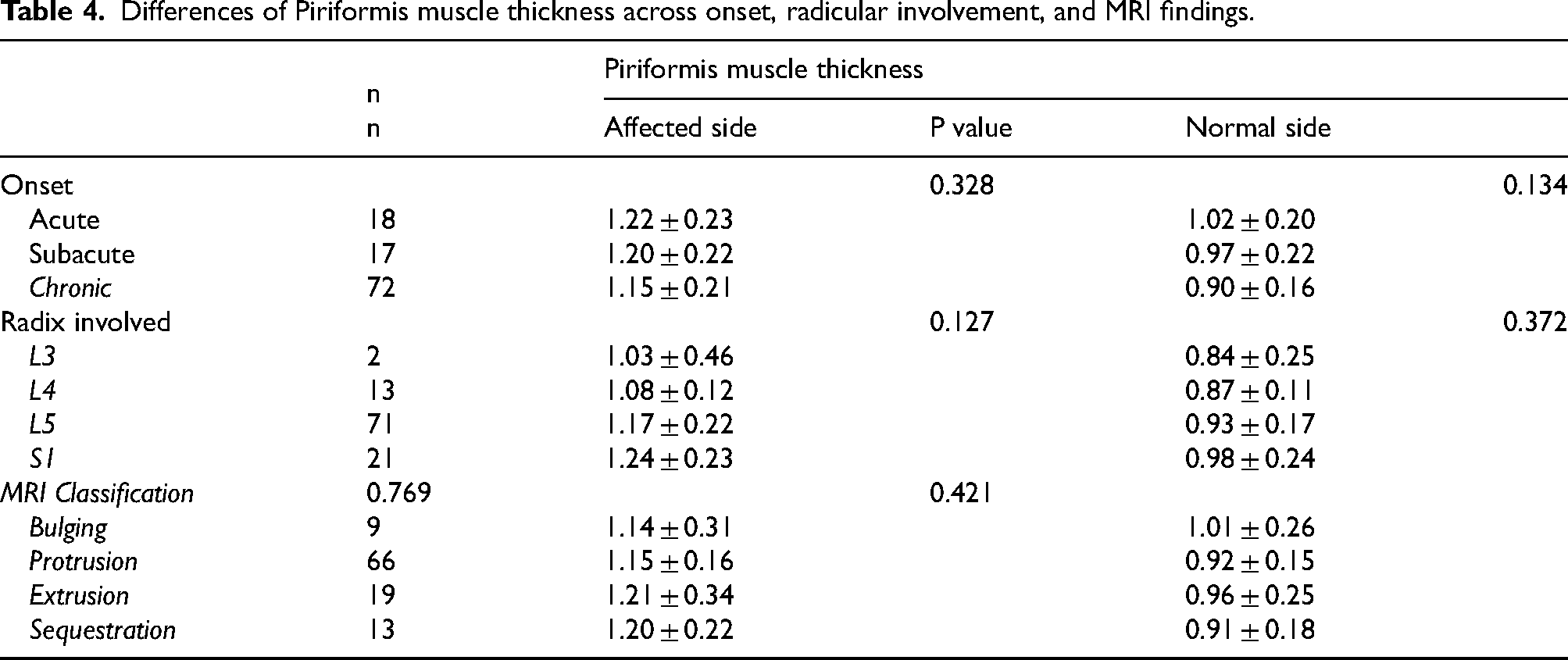
Table 4 outlines the differences in piriformis muscle thickness based on clinical symptom onset, nerve root involvement, and MRI classifications as radiological parameters. Participants with acute onset demonstrated the greatest mean muscle thickness on both the affected (1.22 ± 0.23 cm) and unaffected sides (1.02 ± 0.20 cm), followed by those with subacute and chronic onset disease. However, these differences were not statistically significant (p = 0.328 and p = 0.134, respectively). Muscle thickness was also observed to be higher in patients with lower nerve root involvement, particularly at the S1 (1.24 ± 0.23 cm) and L5 levels (1.17 ± 0.22 cm), compared to higher radices such as L4 (1.08 ± 0.12 cm) and L3 (1.03 ± 0.46 cm). Despite these trends, it did not achieve statistical significance (p = 0.127 and p = 0.372). Similarly, MRI classifications showed minor variations, with extrusion cases exhibiting the highest muscle thickness, but the differences were not statistically significant (p = 0.769).
Differences of Piriformis muscle thickness across onset, radicular involvement, and MRI findings.
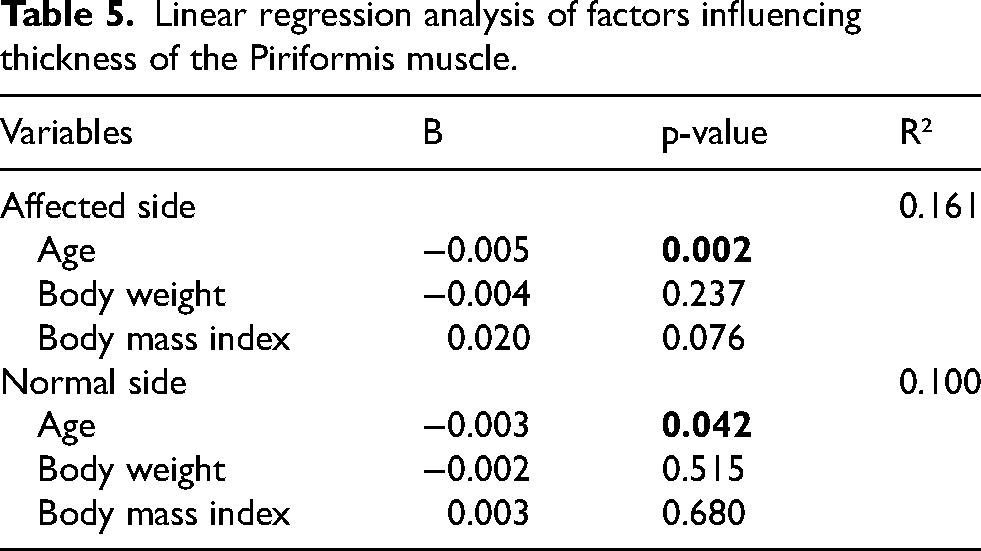
Logistic regression analysis revealed that age was the only significant variable influencing piriformis muscle thickness on both the affected and normal sides. On the affected side, age demonstrated a significant negative association (B = −0.005, p = 0.002), explaining 16.1% of the variance (R² = 0.161). Similarly, on the normal side, age showed a significant negative relationship (B = −0.003, p = 0.042), with the model accounting for 10% of the variance (R² = 0.100). These results indicate that age is a critical factor affecting piriformis muscle thickness (Table 5).
Linear regression analysis of factors influencing thickness of the Piriformis muscle.
Discussion
Lumbar disc herniation and piriformis syndrome are two distinct medical conditions frequently confused due to their overlapping symptomatology which makes accurate diagnosis challenging. The co-occurrence of these conditions has been reported in various case studies, with piriformis syndrome occasionally identified as a complication of LDH, particularly in patients who have undergone interventions such as artificial disc replacement surgery.9–12 This coexistence highlights the importance of thorough clinical evaluation, as both conditions can contribute to lower back pain and radiating leg pain. Although the co-occurrence of LDH and piriformis syndrome has been well-documented, no studies have yet objectively explored and investigated the correlation between these two conditions. Prior research has indicated that hypertrophy of the piriformis muscle, characterized by increased thickness measurable through ultrasound imaging, serves as a key diagnostic marker for piriformis syndrome. 23 Despite these findings, the potential association between nerve root irritation due to herniated discs and piriformis muscle thickening remains unexplored. Therefore, the present study aimed to address this clinical gap by investigating whether herniated nucleus pulposus may contribute to increased thickness of the piriformis muscle. This study demonstrated a mean age of 54.39 years, with a predominance of male patients, indicating that LDH primarily affects middle-aged individuals. These findings align with previous studies suggesting that age-related degenerative changes and occupational factors contribute to the higher prevalence of LDH in this demographic.24,25
Our study identified a significant increase in piriformis muscle thickness on the side affected by herniated disc compared to the unaffected side (1.17 ± 0.22 cm vs. 0.93 ± 0.18 cm, p < 0.05). This finding highlights the potential role of the piriformis muscle in adapting to the underlying pathology associated with LDH, such as spasms and thickening. The underlying mechanisms linking disc herniation to piriformis muscle thickening involve a complex interplay of mechanical and inflammatory factors. Mechanical nerve compression in herniated nucleus pulposus induces neuronal apoptosis in dorsal root ganglion neurons, thereby stimulating the release of proinflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) and neuropeptides. This process further alters the surrounding tissue adjacent to the nerve, causing an increase in vascular permeability, oedema, and further recruitment of proinflammatory cytokines, resulting in altered neuromuscular functions and muscle spasms, including the piriformis muscle as a compensatory pathological response.14,26,27 In addition, the inflammatory processes and responses can extend to adjacent tissues, including the epineurium and perineurium, critical components of the fascial system, leading to structural and functional alterations.28,29 These changes disrupt the release of collagen and hyaluronic acid, resulting in fascial densification, reduced mobility, and increased mechanical tension. 30 Another proposed theory is that herniated nucleus pulposus can significantly disrupt postural alignment, thereby contributing to lumbopelvic instability.31,32 These structural changes may further exacerbate piriformis muscle thickening by altering its mechanical properties. The piriformis muscle plays an essential role in maintaining proper postural alignment and stability during static and dynamic positions in incoordination with other hip muscles.8,33 Therefore, lumbopelvic instability in patients with LDH may lead to compensatory increased tension within the piriformis muscles, as an adaptive mechanism to mitigate the instability, therefore contributing to its hypertrophy and increased thickness. Additionally, several studies have reported on the occurrence of neurogenic muscular hypertrophy due to compressive radiculopathy. In cases of compressive radiculopathy, the peripheral muscle fibers innervated by affected nerves exhibit abnormal continuous chronic electroactivity, leading to overstimulation and subsequent hypertrophy, which serves as an adaptive response to ongoing neural dysfunction.34,35
In the present study, several factors were identified as influencing piriformis muscle thickness in patients with LDH including age, weight, body mass index (BMI), nerve root involvement, and symptom onset. Among these variables, age exhibited a significant negative correlation with piriformis muscle thickness on both the affected (r = −0.308, p = 0.001) and unaffected sides (r = 0.252, p = 0.009), indicating that older patients tend to have thinner piriformis muscles. Furthermore, age was identified as a significant predictor in the multivariate linear regression analysis, which examined the influence of age, body weight, and body mass index on piriformis muscle thickness. This finding aligns with previous studies that have demonstrated similar patterns of muscle degeneration in spinal pathologies. For example, Tian et al. reported that lumbar muscle degeneration was significantly correlated with age in patients with lumbar disc herniation, highlighting that aging contributes to muscle changes in spinal pathologies. 36 Similarly, Kalichman et al. reviewed evidence showing that muscle degeneration, including increased fat infiltration, is often bilateral and multilevel among patients with lumbar disc herniation, even in cases with single nerve root irritation. 37 However, due to the broad age range in this study, it remains challenging to differentiate between age-related atrophic changes and the effects of underlying conditions such as radiculopathy or LDH. In contrast, weight (r = 0.218, p = 0.024) and BMI (r = 0.192, p = 0.047) were positively correlated with muscle thickness. This suggests that increased body mass and weight lead to greater mechanical loads on the lumbopelvic region, resulting in compensatory thickening of the muscles. This finding is consistent with previous study which have reported a positive association between high BMI and piriformis thickness22,38 Furthermore, Bejia et al. suggested that elevated BMI amplifies systemic inflammatory responses, thereby aggravating nerve irritation and contributing to sciatica. 39
Our study further analyzed the association between onset, level of radicular involvement, and severity of disc bulging. Notable differences in piriformis muscle thickness were observed, with greater thickening in cases of LDH affecting the L5 and S1 roots (S1: 1.24 ± 0.23 cm, L5: 1.17 ± 0.22 cm) compared to those affecting the L3 and L4 roots (L4: 1.08 ± 0.12 cm, L3: 1.03 ± 0.46 cm). Although these differences were not statistically significant, this observed difference in muscle thickness may be explained by two factors: the anatomical proximity of the L5 and S1 nerve roots to the piriformis muscle, which facilitates the spread of inflammation and the primary innervation of the piriformis muscle by the S1 and S2 nerve roots, with partial contribution from L5.40,41 Among cases of acute-phase LDH, the piriformis muscle exhibited greater thickening (1.22 ± 0.23 cm) compared to chronic-phase cases (1.15 ± 0.21 cm), although this difference was not statistically significant (p = 0.328). The increased muscle thickness in the acute phase is primarily attributed to an inflammatory response, which induces muscle spasms and thickening via the activation of pro-inflammatory cytokines such as TNF-α. These early changes represent compensatory and inflammatory adaptations. Conversely, thinner piriformis muscles in chronic-phase cases are likely a result of muscle atrophy due to prolonged denervation and diminished muscle activity. As inflammation subsides over time, the transition from adaptive thickening to degenerative changes, including fibrosis and atrophy, occurs, reflecting the long-term effects of reduced neural input and muscle utilization.42–44
The clinical implications of piriformis muscle thickening remain an important consideration. Increased muscle thickness may contribute to myofascial pain, altered biomechanics, and sciatic nerve irritation, potentially exacerbating radicular symptoms in LDH patients. Given these implications, integrating ultrasound evaluation of the piriformis muscle into routine clinical assessments could provide valuable insights into musculoskeletal adaptations in LDH. Regular monitoring of piriformis thickness via ultrasound may help guide rehabilitation strategies, preventing muscle hypertrophy and improve functional outcomes.
This study has several limitations. Firstly, its cross-sectional design prevented the assessment of whether piriformis muscle thickening is reversible following successful therapeutic intervention for LDH. Further longitudinal studies with extended follow-up are required to assess this asymmetry's development as a muscular adaption and its potential reversibility following treatment. Secondly, we did not measure the functional impact of muscle thickening because it did not include a quantitative muscle strength evaluation. Thirdly, while a diagnostic cutoff of piriformis muscle thickness of 0.995 cm has been established for diagnosing piriformis syndrome using ultrasound, 23 this study discovered increased piriformis muscle thickness among patients with LDH. This suggests that LDH may influence muscle thickness measures and potentially impair the accuracy of the existing diagnostic threshold. Therefore, future research should focus on refining and adjusting the optimal diagnostic cutoff values, taking into account the potential influence of LDH-related muscle changes, to enhance the accuracy of diagnostic values for piriformis syndrome diagnosis in individuals with concomitant lumbar pathology such as LDH. Additionally, the inherent operator dependency of ultrasound, may introduce variability in measurement standardization, where even minor inconsistencies in probe positioning could affect accuracy despite adherence to standardized protocols. This limitation may have been further exacerbated by the reliance on a single sonologist for ultrasound assessments. Incorporating multiple sonologists in the evaluation process could enhance the reliability of measurements and mitigate inter-operator variability. Lastly, while this study found a significant association between lumbar disc herniation (LDH) and piriformis muscle thickening, correlation does not imply causation. The cross-sectional nature of this study limits the ability to establish a causal relationship, and prospective studies incorporating additional variables are needed to explore the underlying mechanisms linking LDH to piriformis muscle thickening.
Conclusion
In conclusion, this study found that individuals with lumbar disc herniation exhibit a statistically significant increase in piriformis muscle thickness on the affected side compared to the unaffected side. These findings indicate that both mechanical compression and inflammatory processes associated with LDH may contribute to adaptive structural changes in the piriformis muscle. Consequently, we suggest that a detailed and comprehensive assessment and evaluation must be conducted to rule out or facilitate the early diagnosis of piriformis syndrome in patients with concomitant conditions such as LDH.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.