
Abstract
Background
Cervical radiculopathy (CR) is a neurological disorder with unilateral motor and sensory deficits. This study examines its bilateral impact on upper extremity function across different nerve root levels to inform rehabilitation approaches.
Objective
The aim of this study is to examine bilateral sensorimotor dysfunctions in patients with cervical radiculopathy.
Methods
Forty-two patients (mean age 44.4 ± 11.05 years; 34 women, 8 men) with C4–5, C5–6, or C6–7 CR and 16 controls (mean age 42.2 ± 15.5 years; 9 women, 7 men) with non-specific neck pain participated. Evaluations included pain (VAS), neck disability (NDI), upper extremity functionality (DASH), muscle strength measurements, sensory function, hand performance, kinesiophobia (TAMPA) and emotional status (Beck Inventory).
Results
All radiculopathy groups showed significant bilateral muscle weakness (5–12%) in upper extremities and reduced lateral pinch strength compared to controls (p < 0.05). Sensory deficits were severe, with C5 and C6 groups showing 46% reduction in light touch sensation and C7 group exhibiting 80% reduction, with decreased vibration sensation. The C7 group demonstrated the most severe impairments. Psychological assessment revealed kinesiophobia in all groups, with radiculopathy groups showing moderate anxiety compared to mild anxiety in controls, and mild depressive symptoms across all groups.
Conclusions
Unilateral cervical radiculopathy leads to significant bilateral sensorimotor impairments, with severity varying by nerve root level. Findings emphasize the need for comprehensive bilateral assessment and rehabilitation programs addressing both affected and unaffected limbs.
Keywords
Introduction
Cervical radiculopathy (CR), a neurological disorder affecting approximately 83 per 100,000 individuals annually, is characterized by motor and sensory deficits along specific nerve root distributions. 1 Most prevalent in individuals during their fourth and fifth decades of life. 1 CR significantly impairs upper extremity function, impacting daily activities and quality of life. C7 nerve root involvement is most common, followed by C6 and C8. 2 CR typically presents unilaterally with arm pain, paresthesia, and muscle weakness, distributed according to the involved nerve root(s). 3 Symptoms can manifest in proximal segments (shoulder, elbow) or distal segments (wrist and hand). 4 This multifaceted condition can cause a range of motor deficits and sensory disturbances across multiple upper extremity segments, potentially leading to significant functional impairments. 5
While numerous studies have investigated motor and sensory function in individuals with CR at various levels6,7 a comprehensive understanding of its impact on the entire upper extremity remains incomplete. Some research has focused primarily on the cervical region,8,9 while others have specifically targeted upper extremity symptoms.10,11 Although some studies have adopted more holistic approaches encompassing both cervical and upper extremity symptoms,12,13 there remains a limited understanding of the interplay between proximal and distal upper extremity segments and their inter-segmental interactions in CR. Therefore, to fully understand the impact of CR on upper extremity function, a comprehensive evaluation of sensorimotor deficits across both proximal and distal segments is essential.
This study aimed to comprehensively investigate the extent of sensorimotor dysfunction in affected and unaffected upper extremities in patients with unilateral CR at three specific levels: C4–5, C5–6, and C6–7. These groups were compared to each other and a group with non-spesific neck pain (NSNP), a prevalent non-nerve root condition. Considering the potential impact of unilateral problems on the contralateral side, this study investigated sensorimotor involvement bilaterally in all groups. This integrated approach may provide clinicians with valuable insights for assessing CR, leading to more targeted and effective rehabilitation strategies and improved treatment outcomes. The hypotheses of this study are as follows:
Patients with unilateral cervical radiculopathy will exhibit significant sensorimotor deficits in both the affected and unaffected upper extremities compared to individuals with non-specific neck pain (NSNP). The severity of sensorimotor deficits will vary depending on the specific nerve root involved (C5, C6, or C7). The bilateral sensorimotor impairments observed in patients with cervical radiculopathy will significantly correlate with reduced upper extremity functionality (as measured by DASH scores) and increased psychological impacts (as measured by kinesiophobia, depression and anxiety scales).
Method
Study design
This study was conducted in a prospective cross-sectional design between August 2022 and April 2023 to investigate sensorimotor dysfunction in the upper extremities of patients with CR. Participants were recruited from the X Hospital. Patients with a history of neck pain lasting at least three months were eligible for inclusion in this study. The study group consisted of individuals aged 18 to 65 years diagnosed with CR, confirmed by medical history, physical examination, and MRI findings, exhibiting radicular symptoms corresponding to the affected cervical level. Participants were divided into three subgroups based on the affected cervical level: C4–5 (C5), C5–6 (C6), and C6–7 (C7). A control group presenting mechanical neck pain was included. Exclusion criteria were systemic or neurological disorders (excluding CR), previous spinal surgery, acute trauma, fracture, malignancy, osteoporosis, rheumatic disease, or ongoing pharmacological treatment for chronic neck pain.
CR diagnosis was based on criteria established by Rubinstein et al. 13 : radicular pain and/or neurological deficits, limited cervical spine movement, and positive provocation tests. Patients presenting at the institution were screened for eligibility by a physiatrist, based on clinical examination. Patients with positive clinical findings were subsequently referred for MRI. MRI scans were performed and interpreted by a radiologist specializing in musculoskeletal imaging. Within two weeks, the patients were seen by the physiatrist, who reviewed the clinical findings in conjunction with the MRI results to confirm the diagnosis of cervical radiculopathy.The level of radiculopathy was determined using the dermatome map, a widely used tool in clinical practice that delineates the dermatome areas innervated by each cervical nerve root. 14 The dermatome mapping procedure involved identifying and marking areas of pain, numbness, or tingling in the patient's upper extremity on the dermatome map to determine the corresponding nerve root dermatome. The corresponding nerve root dermatome was then determined. In cases of overlapping dermatome areas, the dermatome with the most severe symptoms was designated as the primary affected level. This information, combined with MRI and physical examination findings, guided the final radiculopathy level determination, consistent with the methodology employed by Tong et al. 15
Sample size calculation
G*Power (version 3.1.9.4, Heinrich-Heine-Universität Düsseldorf, Germany) was used for the sample size calculation. 16 G*Power (version 3.1.9.7, Heinrich-Heine-Universität Düsseldorf, Germany) was used for the sample size calculation. Our primary outcome measures were motor assessments (muscle strength and grip strength) and sensory assessments (Semmes-Weinstein monofilament test and vibration test). Based on the study by Joghataei et al., 17 which reported an effect size of Cohen's d ≈ 1.04 for grip strength improvement after 5 treatment sessions, we conducted an a priori power analysis. This effect size was converted to f = 0.5 for the one-way ANOVA statistics. With a Type I error rate of 5% (α = 0.05) and statistical power of 80% (1-β = 0.80), a minimum of 48 participants were required. Sample size was adjusted upward to compensate for possible participant withdrawal. A total of 58 participants were enrolled: 13 in the C5 group, 13 in the C6 group, 16 in the C7 group, and 16 in the control group.
Measurements
Demographic and clinical characteristics, including age, gender, body mass index, affected side, dominant side, education level, and symptom duration, were recorded for each participant. All bilateral measurements were conducted under standardized conditions (e.g., controlled temperature, consistent positioning).
Pain assessment
Pain intensity was assessed using a 10-cm Visual Analog Scale (VAS), with 0 indicating no pain and 10 indicating unbearable pain. Participants were asked to mark their pain levels at rest, during activity, and at night.
Neck disability status
The patient-reported neck disability was measured using the Neck Disability Index (NDI). 18 Patients’ ratings on 10 items, including pain intensity, personal care, lifting, sleeping, driving, recreation, headaches, concentration, reading, and work, were summed to a total score expressed as a percentage, with a higher score indicating a higher degree of disability.
Muscle strength measurement
Isometric muscle strength of the proximal upper extremities was measured using a digital dynamometer (Lafayette Manual Muscle Testing System, Model 01165, Lafayette Instrument Company, Lafayette, IN, USA). Participants were seated in a standardized position. Isometric muscle strength of both proximal (shoulder flexors, extensors, abductors, elbow flexors, and extensors) and distal upper extremities (wrist flexion, extension, supination, and pronation) was assessed using a digital dynamometer (Lafayette Manual Muscle Testing System, Model 01165, Lafayette Instrument Company, Lafayette, IN, USA) following standardized testing protocols. 19 Participants were seated in a standardized position to ensure accurate measurement of each specific muscle group. Measurements were performed in triplicate with a 30-s rest period between each repetition. The highest value from the three trials was recorded as the maximum strength in kilograms.
The strength of intrinsic hand muscles was evaluated using manual muscle testing. A 0–5 scoring system was employed, with 0 representing no muscle contraction and 5 representing normal strength. The average of three measurements was recorded for each muscle group.
Grip and pinch strength measurements
Grip strength was assessed using a Jamar hand dynamometer (Jamar Hydraulic Hand Dynamometer, Model SH5001, Saehan Corporation, Masan, South Korea) according to the standardized position and protocol recommended by the American Society of Hand Therapists. 20 Lateral, tip, and tripod pinch strengths were evaluated with a pinchmeter (Baseline Pinch Gauge, Model 12–0201, Fabrication Enterprises Inc., White Plains, NY, USA). For both assessments, participants were seated with their shoulders adducted and neutrally rotated, elbows flexed to 90°, and forearms and wrists in a neutral position. Participants were instructed to squeeze the dynamometer for 3–5 s with maximal effort. Three trials were performed for each hand, alternating between affected and unaffected sides, with a 30-s rest period between trials. The average of the three trials was recorded in kilograms. Participants received detailed instructions and completed a trial for each grip type prior to the assessment.
Sensory evaluation
Light touch sensation was assessed bilaterally using the Semmes-Weinstein monofilament test kit (North Coast Medical Inc., Gilroy, CA, USA). The assessment followed standardized protocols as described in recent clinical studies. 21 Monofilaments were applied sequentially, starting with the 2.83 filament, to the following locations on each hand: thumb, index finger, and little finger. 15 Each monofilament was applied at a 90-degree with sufficient pressure to bend it for 1–1.5 s, three times at each location. Participants responded “yes” when they felt the stimulus. A threshold was considered achieved when the patient correctly identified at least seven out of ten applications. Results were classified as normal (1.65–2.83), diminished light touch (3.22–3.61), diminished protective sensation (3.84–4.31), loss of protective sensation (4.56–6.65), and unmeasurable sensation (above 6.65).
Vibration was evaluated using a 128 Hz tuning fork. The assessment was performed at the radial and ulnar styloid processes, as these bony prominences provide reliable anatomical landmarks for evaluating the distal effects of cervical nerve roots. 22 Vibration testing is particularly relevant as it assesses large-diameter myelinated Aβ fibers, which are often affected in the early stages of nerve root compression. 23 Participants were seated comfortably with forearms supported and wrists in a neutral position. Following a practice trial, the tuning fork was applied to each styloid process three times. Participants indicated when the vibration was first perceived and when it was no longer perceived. The duration of perceived vibration was recorded for each trial, and the average duration was calculated. A minimum of 30 s was allowed between measurements to prevent sensory adaptation. Results were classified as normal, diminished, or absent based on age-normalized reference values.
The Moberg Pick-Up Test (MPUT) evaluated functional sensation, assessing tactile discrimination and fine motor control within the context of daily living activities. 24 This test is relevant to cervical radiculopathy assessment as it provides valuable insight into sensory deficits and potential motor impairments affecting hand function. Participants were seated with forearms supported and wrists neutral. They transferred twelve small metal objects between containers using their thumb and index finger, first with eyes open and then with eyes closed. This two-stage protocol assesses both stereognosis and hand function, which gives information about tactile discrimination and fine motor control. 25 The test was repeated three times per hand, and the average completion time for each phase was recorded, after a practice trial.
Upper extremity functional level
Upper extremity functional level was evaluated using the Disabilities of the Arm, Shoulder, and Hand questionnaire, a standardized 30-item self-report measure widely validated for assessing upper extremity symptoms and activity limitations. 26 Each item is scored from 1 (no disability) to 5 (most severe disability), with total scores ranging from 0 to 100. Higher scores indicate greater disability.
Emotional status
Beck Depression Scale (BDS) and Beck Anxiety Scale (BAS) were used to assess depression and anxiety levels, with higher scores indicating more severe depression or anxiety. 27 Although these scales measure related constructs, they capture different psychological aspects: The Beck Depression Inventory specifically measures depressive symptoms such as negative mood, pessimism, and anhedonia, whereas the Beck Anxiety Inventory focuses on physical and cognitive symptoms of anxiety such as nervousness, fear, and somatic complaints. The use of both scales allowed for a more comprehensive assessment of participants’ emotional state. The Tampa Scale of Kinesiophobia was used to assess fear of movement. 28 Higher scores indicate a greater fear of movement.
Statistical analysis
After data collection by TE, the data analysis was performed by an independent statistician, who was blinded to the study groups. Statistical analyses were performed using SPSS (Statistical Package for Social Sciences) for Windows, version 22.0. The normality of the data distribution was tested using the Kolmogorov-Smirnov test. Descriptive statistics were presented with number, median and interquartile range, percentage, mean and standard deviation. One-way ANOVA with post-hoc Scheffe test was used to compare quantitative continuous data between independent groups. For within-group analysis, paired samples t-test and repeated measures ANOVA were used for normally distributed variables, while Kruskal-Wallis H test was performed for between-group comparisons of non-normally distributed variables. Statistical significance was set at p < 0.05.
Results
This study included 42 participants with CR and 16 participants with NSNP. Participants with CR were categorized into three subgroups based on the affected cervical level: C4–5 (n = 13), C5–6 (n = 13), and C6–7 (n = 16). The study flow chart is presented in Figure 1. Patients with CR had an average age of 44.4 ± 11.1 years and a BMI of 25.43 ± 4.1, and NSNP had an average age of 42.2 ± 15.5 years and a BMI of 24.6 ± 3.9.
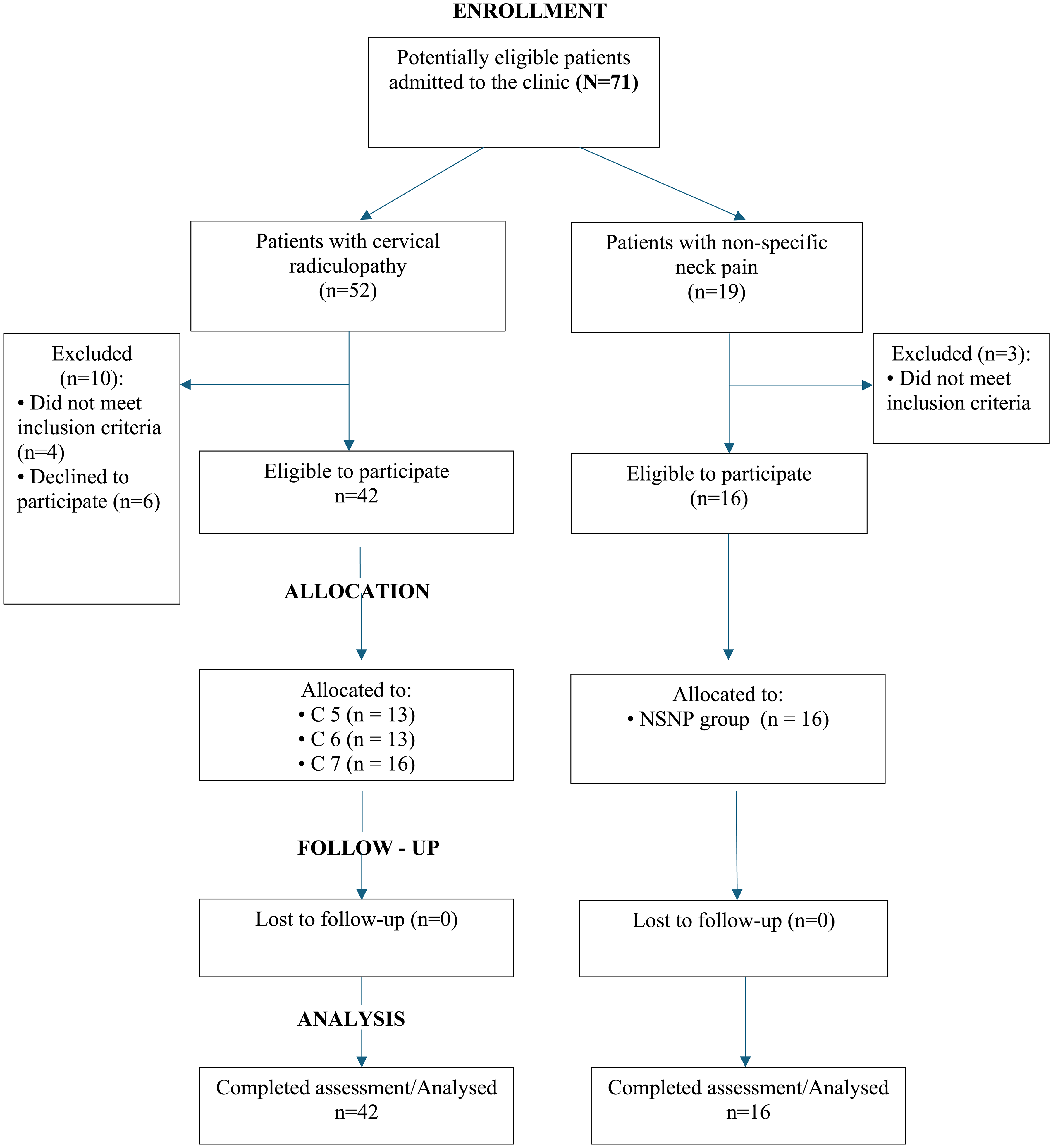
Flow-chart of the study.
There were no statistically significant differences between groups regarding age, BMI, sex, affected side, or dominant side. In the radiculopathy group, 8 participants (19.0%) were male and 34 (81.0%) were female. In the NSNP group, 7 participants (43.8%) were male and 9 (56.2%) were female. Regarding the affected side, 20 participants (47.6%) in the radiculopathy group and 8 (50.0%) in the NSNP group had right-side involvement, while 22 (52.4%) in the radiculopathy group and 8 (50.0%) in the NSNP group had left-side involvement. In the radiculopathy group, 41 participants (97.6%) were right-hand dominant and 1 (2.4%) was left-hand dominant. All participants (100.0%) in the NSNP group were right-hand dominant.
There were no significant differences in pain severity and NDI between groups (p > 0.05) (Table 1). DASH symptom (F = 4.876; p = 0.005) and DASH work (F = 3.933; p = 0.013) scores differed significantly between groups. The C7 group demonstrated worse functional status compared to the other groups. The presence of high kinesiophobia scores (>37) in all groups indicates the presence of fear of movement in these patients (Table 1). Anxiety scores of 16 or higher in the radiculopathy groups indicate moderate anxiety, while mild anxiety symptoms were reported in the NSNP group. Mild depressive symptoms were reported in all groups (Table 1).
Comparison between CR and NSNP groups regarding pain, neck disability, upper extremity disability and emotional status.
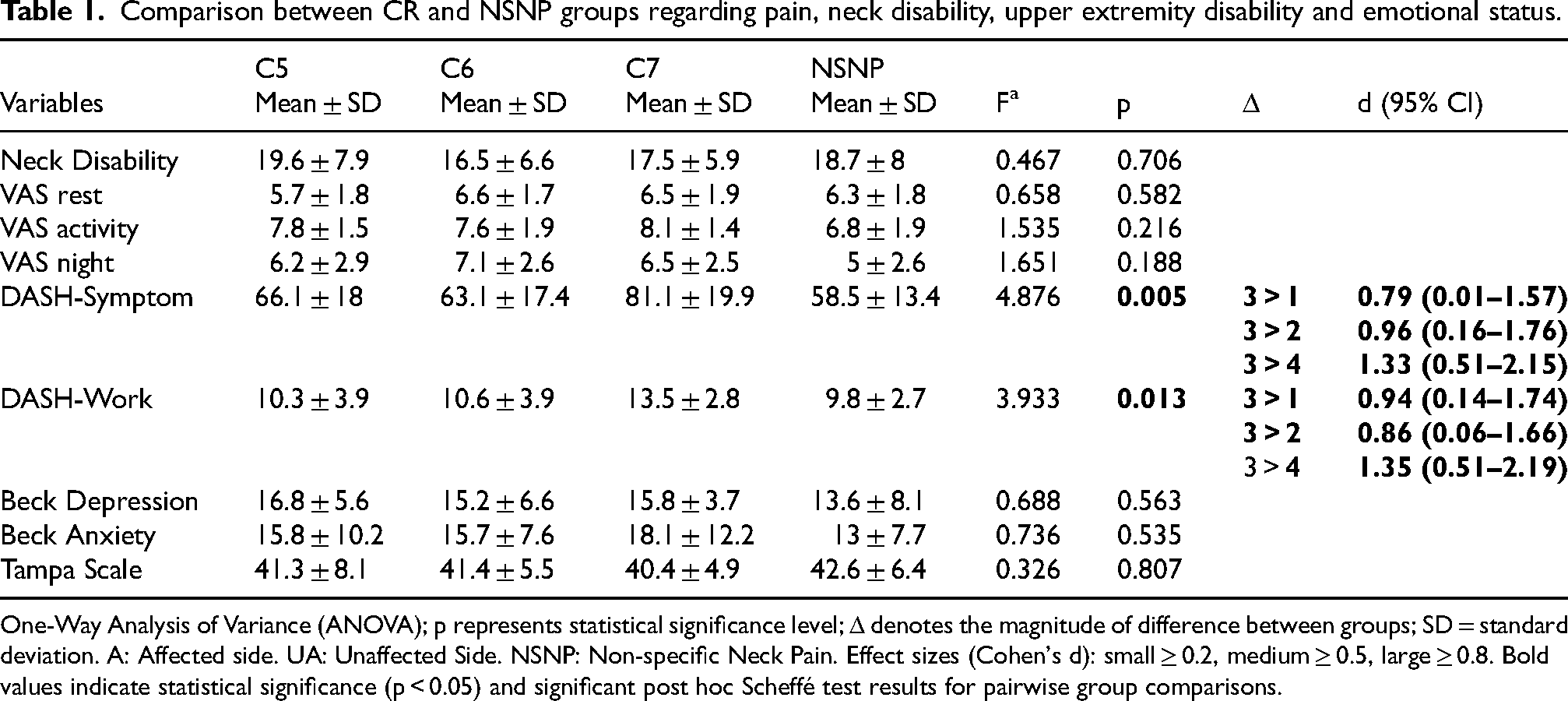
One-Way Analysis of Variance (ANOVA); p represents statistical significance level; Δ denotes the magnitude of difference between groups; SD = standard deviation. A: Affected side. UA: Unaffected Side. NSNP: Non-specific Neck Pain. Effect sizes (Cohen's d): small ≥ 0.2, medium ≥ 0.5, large ≥ 0.8. Bold values indicate statistical significance (p < 0.05) and significant post hoc Scheffé test results for pairwise group comparisons.
Affected-side elbow flexor strength (F(3, 54) = 6.914; p = 0.001 < 0.05), extensor strength (F(3, 54) = 3.400; p = 0.024) and non-affected side elbow flexor strength (F(3, 54) = 5695; p = 0002) showed significant differences between groups. Patients in the NSNP group demonstrated greater strength than those in the C5, C6, and C7 groups (Table 2). Affected-side wrist flexor (F(3, 54) = 6.914; p = 0.001), wrist extensor (F(3, 54) = 3.256; p = 0.029), pronator (F(3, 54) = 2.964, p = 0.040) and supinator (F(3, 54) = 3.651, p = 0.018) muscle strengths differed significantly between groups. Patients in the radiculopathy groups exhibited lower strength compared to the NSNP group. Unaffected-side pronator and supinator muscle strength showed significant differences between groups (pronator: F(3, 54) = 3.447, p = 0.023; supinator: F(3, 54) = 2.858, p = 0.045). The C7 group had lower supinator strength compared to the NSNP group. All radiculopathy groups demonstrated lower pronator strength compared to the NSNP group (p < 0.05). The weakness of the forearm and wrist muscles was 5–7% compared to the NSNP group (Table 2).
Comparison between CR and NSNP groups regarding shoulder. elbow and wrist muscle strengths.
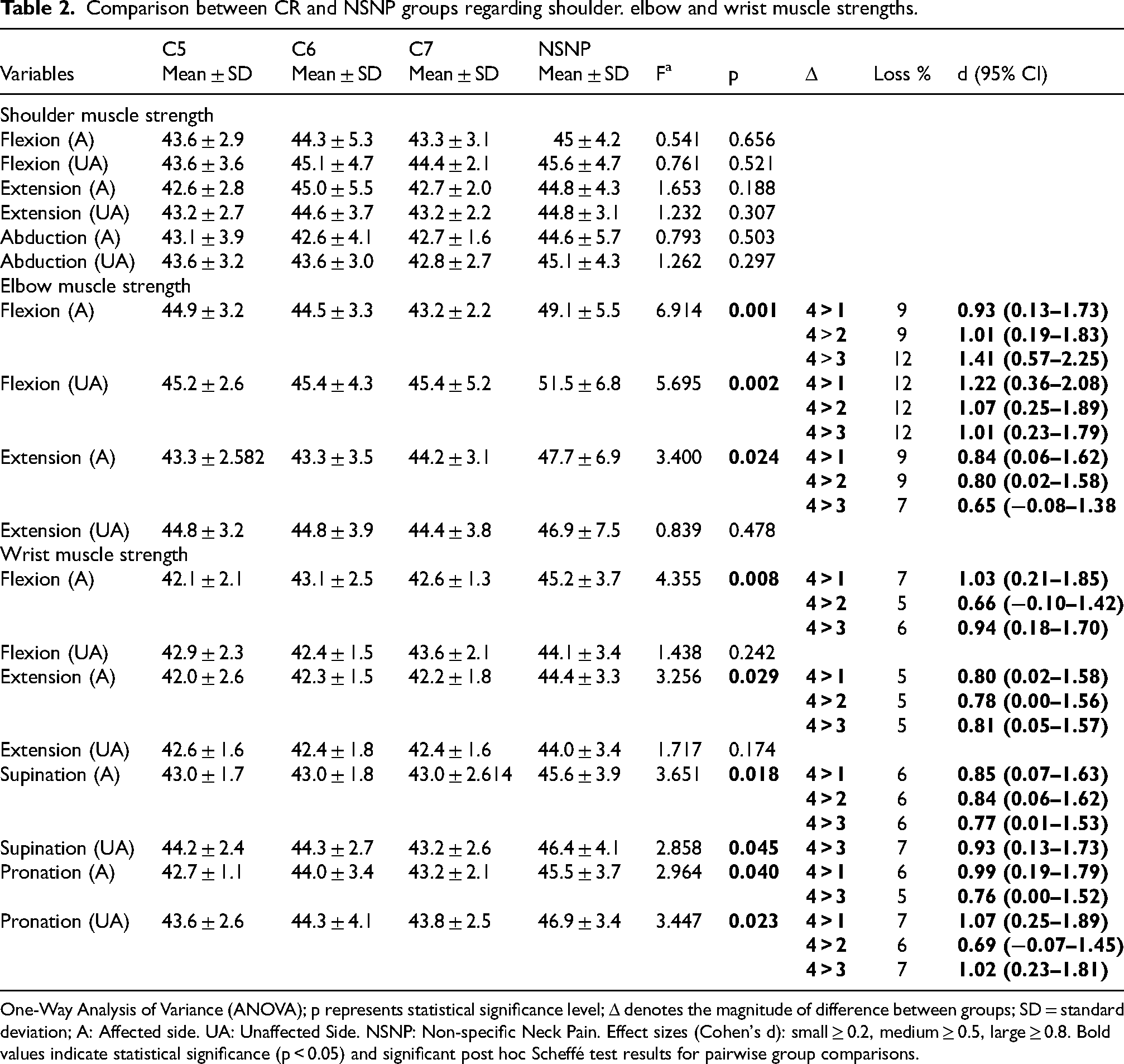
One-Way Analysis of Variance (ANOVA); p represents statistical significance level; Δ denotes the magnitude of difference between groups; SD = standard deviation; A: Affected side. UA: Unaffected Side. NSNP: Non-specific Neck Pain. Effect sizes (Cohen's d): small ≥ 0.2, medium ≥ 0.5, large ≥ 0.8. Bold values indicate statistical significance (p < 0.05) and significant post hoc Scheffé test results for pairwise group comparisons.
A significant difference was observed in affected-side thumb flexor (H(3)= 20,54; p = 0.000), extensor (H(3)= 16,33; p = 0.001), abductor (H(3)= 17,49; p = 0.001), adductor (H(3) = 12,09; p = 0.007) and opposition (H(3) = 14,13; p = 0.003) muscle strength between groups (Table 3). All radiculopathy groups had lower thumb strength compared to NSNP group. There were significant differences between groups in unaffected-side thumb flexor (H(3)= 13,98; p = 0.003), extensor (H(3)= 14,77; p = 0002), abductor (H(3)= 13,37; p = 0.004), adductor (H(3)= 15,53; p = 0.001) and opposition (H(3)= 10,43; p = 0.015) strength. All radiculopathy groups had lower flexor, extensor and abductor muscle strength compared to NSNP group, and C6 and C7 groups exhibited lower adductor and opposition strength compared to NSNP group (Table 3).
Comparison between CR and NSNP groups regarding hand muscle strengths.
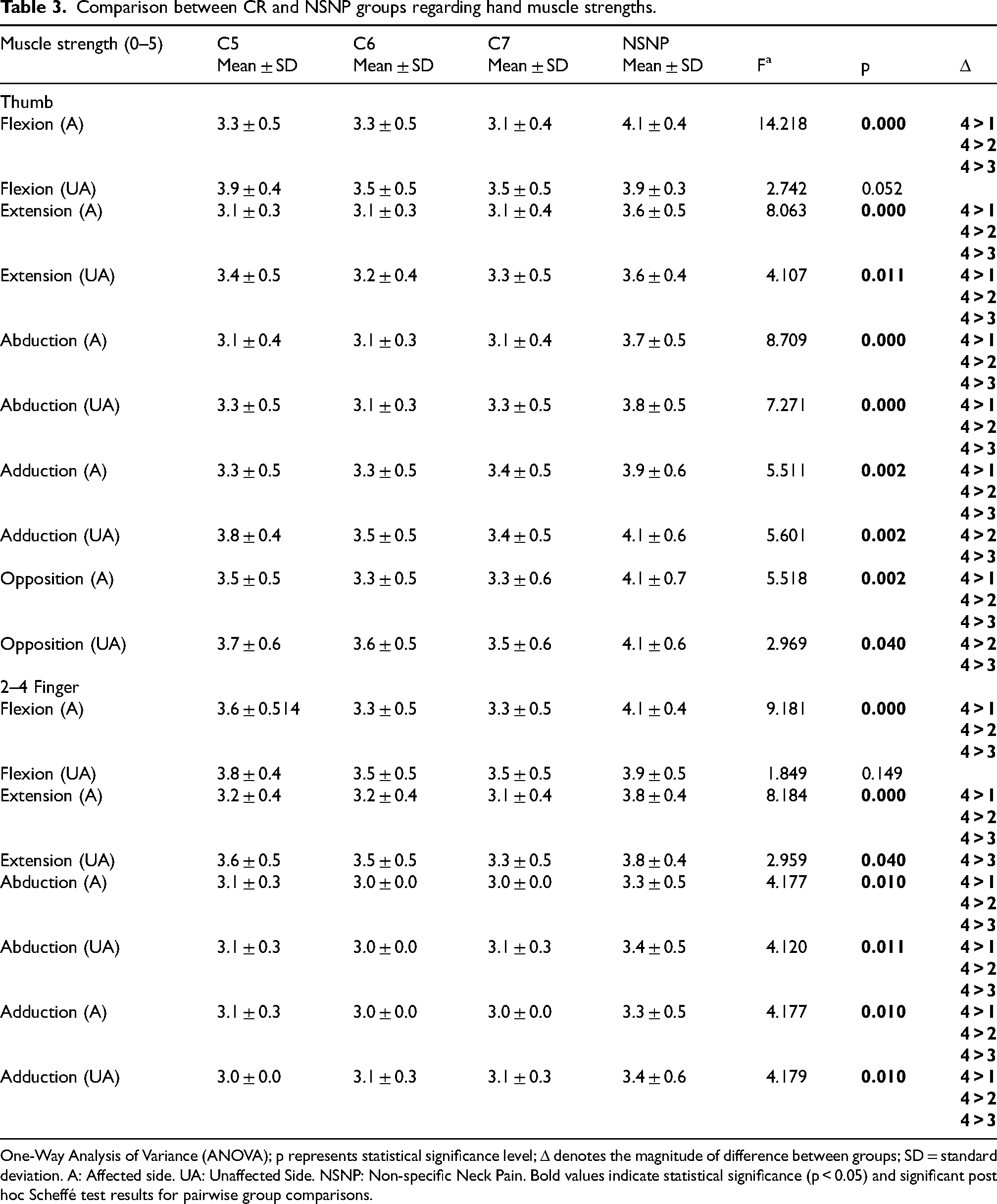
One-Way Analysis of Variance (ANOVA); p represents statistical significance level; Δ denotes the magnitude of difference between groups; SD = standard deviation. A: Affected side. UA: Unaffected Side. NSNP: Non-specific Neck Pain. Bold values indicate statistical significance (p < 0.05) and significant post hoc Scheffé test results for pairwise group comparisons.
Significant differences were observed between groups in affected-side finger flexor (H(3)= 14,79; p = 0.002), extensor (H(3)= 17,01; p = 0.001), abductor (H(3)= 11,19; p = 0.011) and adductor (H(3)= 16,99; p = 0001) strength (Table 3). All radiculopathy groups demonstrated lower extensor and abductor muscle strength, while C6 and C7 groups also showed lower flexor and adductor muscle strength compared to NSNP group. Unaffected-side finger flexor (H(3)= 9,08; p = 0028), and adductor (H(3)= 10,24; p = 0.017) strength also showed significant between-group differences. The NSNP group had greater flexor strength compared to the C6 and C7 group, and greater adductor strength compared to all radiculopathy groups (Table 3).
Affected-side lateral pinch grip strength (F = 3.029; p = 0.037) differed significantly between groups, with the NSNP group demonstrating greater strength than the radiculopathy groups (Table 4). Unaffected-side palmar pinch grip strength (F = 2.939; p = 0.041) also showed between-group differences, with the NSNP group exhibiting greater strength compared to the C6 and C7 groups (Table 4).
Comparison between CR and NSNP groups regarding grip and pinch strengths.
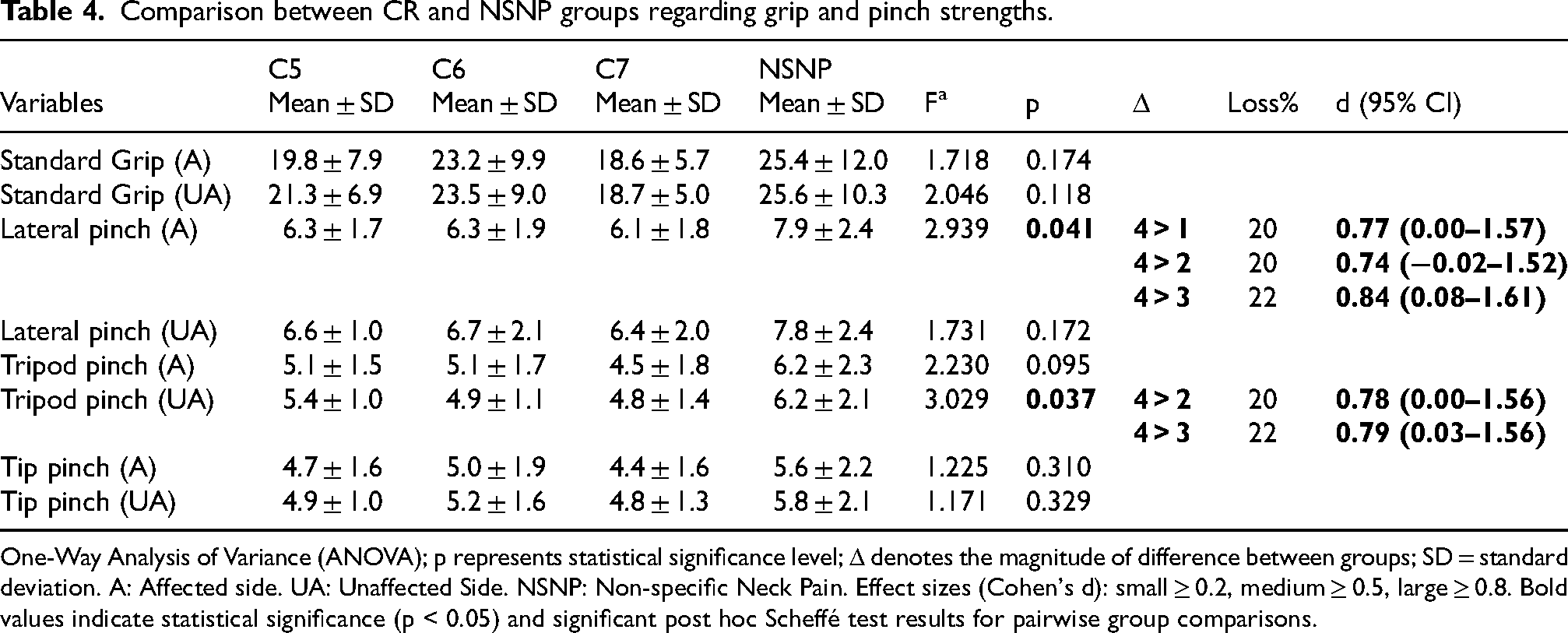
One-Way Analysis of Variance (ANOVA); p represents statistical significance level; Δ denotes the magnitude of difference between groups; SD = standard deviation. A: Affected side. UA: Unaffected Side. NSNP: Non-specific Neck Pain. Effect sizes (Cohen's d): small ≥ 0.2, medium ≥ 0.5, large ≥ 0.8. Bold values indicate statistical significance (p < 0.05) and significant post hoc Scheffé test results for pairwise group comparisons.
Sensory testing revealed a 46% reduction in light touch sensation in the C5 and C6 groups, while an 80% reduction was seen in the C7 radiculopathy group (Table 5). The C5 and C6 radiculopathy groups demonstrated twice the sensory loss compared to the NSNP group. Sensory loss was also found in the unaffected limb, with the C7 group showing twice the deficit compared to the other groups (Table 5). Vibration sensation at the affected-side radial styloid differed significantly between groups (F = 4.239; p = 0.009) (Table 6). Radiculopathy groups had shorter vibration sensation durations compared to the NSNP group. Similar findings were observed for the unaffected side (F = 2.858; p = 0.045), with C6 and C7 groups showing shorter durations than the NSNP group.
Light touch/pressure sensation loss in the CR and NSNP groups.

Comparison between CR and NSNP groups regarding vibration sense and hand dexterity.
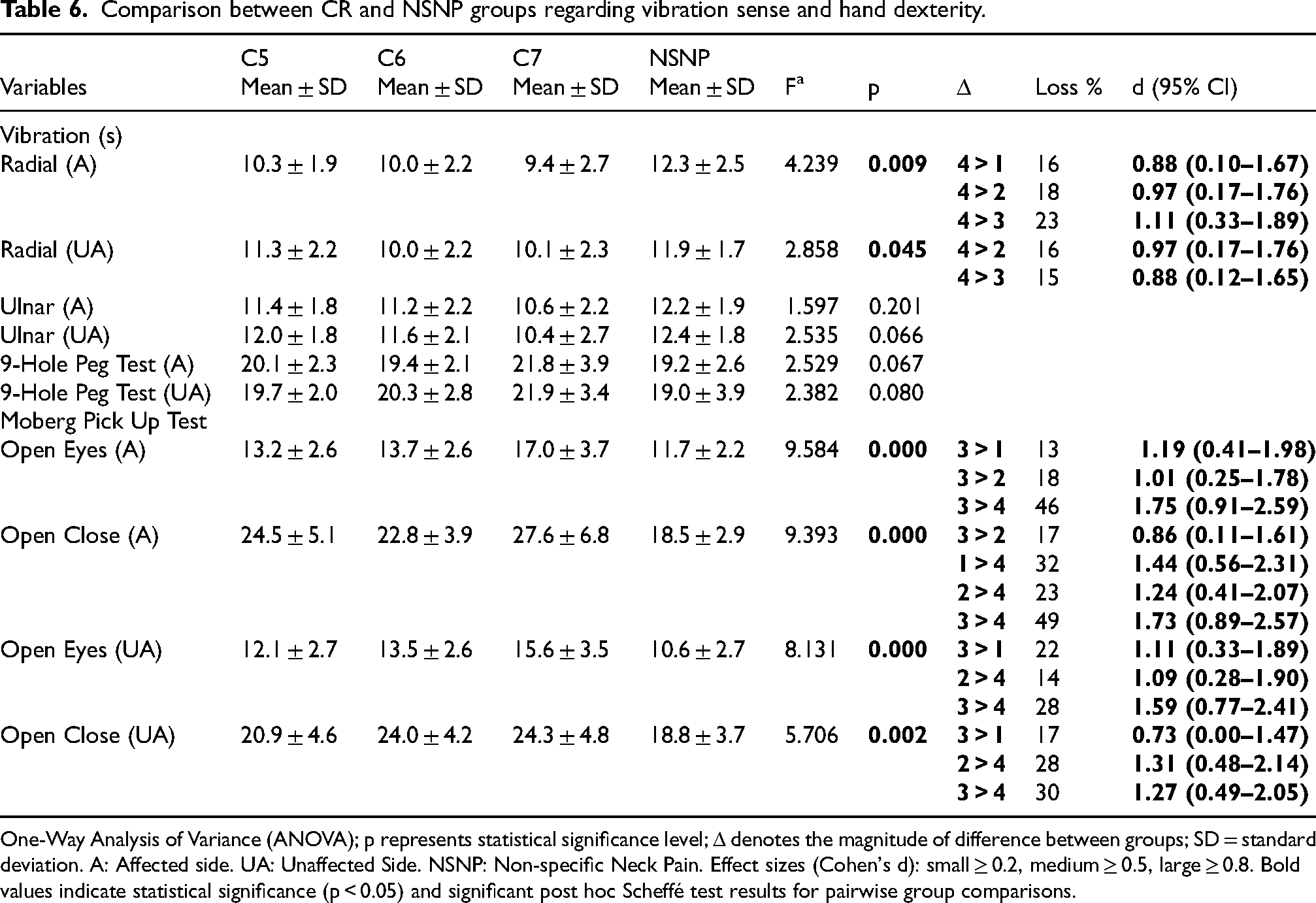
One-Way Analysis of Variance (ANOVA); p represents statistical significance level; Δ denotes the magnitude of difference between groups; SD = standard deviation. A: Affected side. UA: Unaffected Side. NSNP: Non-specific Neck Pain. Effect sizes (Cohen's d): small ≥ 0.2, medium ≥ 0.5, large ≥ 0.8. Bold values indicate statistical significance (p < 0.05) and significant post hoc Scheffé test results for pairwise group comparisons.
No significant between-group differences were found in hand dexterity test results. Affected-side Moberg pick-up test times, both with eyes open (F = 9.584; p = 0.001) and eyes closed (F = 9.393; p = 0.001), differed significantly between groups (Table 6). The C7 group had longer completion times with eyes open compared to other groups. With eyes closed, all radiculopathy groups had longer completion times than the NSNP group. Unaffected-side Moberg pick-up test times also showed significant between-group differences with eyes open (F = 8.131; p = 0.001) and eyes closed (F = 9.393; p = 0.001). With eyes open, the C7 group had longer times than the C5 and NSNP groups, and the C5 group had longer times than the C6 group. With eyes closed, the C7 group had longer times than the C5 and NSNP groups, and the C6 group had longer times than the NSNP group (F = 5.706, p = 0.002).
Discussion
This study investigated sensorimotor changes in upper extremities bilaterally in C5- C7 cervical radiculopathy. The study highlights the presence of significant differences in motor strength, sensory function and overall upper extremity functionality at different levels of radiculopathy. Motor deficits, including weakness of the elbow, wrist and finger muscles, were observed at all levels of CR. Sensory deficits were also prominent, with the C5 and C6 groups showing twice the deficit of the NSNP group and the C7 showing four times the sensory loss. In addition, the C7 group demonstrated the worst hand performance and upper extremity functionality. The substantial sensorymotor deficits in the unaffected extremity in patients with CR emphasize the complex and wide-ranging bilateral effects of CR.
When assessing sensorimotor deficits in cervical radiculopathy, it is important to consider the possible influence of demographic variables such as age and gender and concomitant conditions such as systemic diseases that may impair sensorimotor function. The lack of statistically significant differences in demographic factors between the groups in this study minimizes potential confounding variables. Age-related changes affect upper extremity function, with individuals over 50 having a higher sensory perception threshold and lower motor skills. 29 The average age of patients with CR in the present study is consistent with previous studies, as the age range of 40–50 years represents the period in which degenerative disk disease and CR are most commonly observed. 30 Epidemiologic studies have also shown that women have a higher risk of developing CR despite geographical differences. 31 The gender distribution in the current study showed a female predominance in the CR group. The differences in gender predisposition to CR between studies suggest that prevalence rates vary and may be influenced by the characteristics of the study population1,2 In addition, patients with comorbidities were excluded from the current study, as comorbidities such as diabetes, peripheral neuropathy and inflammatory rheumatic diseases can directly affect peripheral nerve conduction, which can lead to misleading results in sensorimotor tests.
Proximal and distal muscle weakness has been documented in cervical radiculopathies.6,32 In the present study, elbow, wrist, thumb, and finger strength were significantly weaker in the radiculopathy groups compared to the NSNP group. Furthermore, consistent with reports of bilateral electrophysiological changes in unilateral cervical radiculopathies, 33 we observed decreased strength in the unaffected limb of all radiculopathy groups compared to the NSNPgroup. Notably, most patients are unaware of these motor weaknesses. This bilateral upper extremity involvement has two key implications. Firstly, using the unaffected extremity as a control in unilateral cases may introduce bias. Secondly, comprehensive bilateral assessment is crucial for effective physiotherapy planning. The observed hand muscle weakness even in C6 radiculopathy challenges traditional understanding and suggests broader neurophysiological consequences of nerve root compression. These effects are not uniformly distributed, with more pronounced and bilateral weakness distally, particularly in the hands. It's important to consider that the presence of motor or sensory deficits doesn't necessarily confirm pathology. Overlapping or intersegmental spinal roots and anastomoses of peripheral nerves can contribute to these findings. 34
The strength of the intrinsic hand muscles is critical for functional hand activities, especially those requiring dexterity, such as handwriting. 35 Distal muscle weakness can be observed in cervical radiculopathy.6,7 Measurement of isolated intrinsic hand muscle strength can be a valuable tool for monitoring the progress of physiotherapy interventions. In this study, a manual muscle test was performed. However, future studies could incorporate objective measurements using instruments such as the Rotterdam Intrinsic Hand Myometer, a validated and reliable tool for assessing individual intrinsic hand muscle strength. 36 Distal intrinsic muscle weakness in the groups with radiculopathy could also contribute to decreased lateral and palmar pinch strength in these individuals, as the contribution of intrinsic muscles to pinch strength is known. 36 This reduced pinch strength in individuals with radiculopathy could have a negative impact on fine motor skills and thus upper extremity functionality. Considering the correlation between pinch strength and DASH scores in healthy individuals, 37 targeted exercises to strengthen specific muscles are recommended for individuals with cervical radiculopathy. Bilateral broader involvement suggests that rehabilitation programs should incorporate bilateral assessment and treatment strategies that address both sides of the body. This more comprehensive approach may be necessary to address the complex and often bilateral nature of muscle weakness in cervical radiculopathy.
Non-specific neck pain has been shown to have a significant impact on upper limb function. 38 Although the relationship between neck pain and upper limb disability is not fully understood, several possible explanations were presented in the study by Alreni et al. 39 One proposed mechanism is the direct mechanical connection between the neck and the upper lextremity. Due to this musculoskeletal connection, increased loads or repetitive movements of the upper extremity may stress these structures and possibly cause pain or protective muscle spasms in the neck, while neck pain itself may lead to reduced upper extremity function due to pain provocation. 40 Reduced activity due to pain could lead to deconditioning characterized by decreased strength and endurance of the muscles in the neck and upper extremities, which can then lead to compensatory movements and increased strain on cervical structures. 41
The DASH is widely used to assess upper extremity function in various musculoskeletal disorders and can be used in patients with single or multiple disorders of the shoulder, arm and hand. 26 The DASH has shown acceptable validity and responsiveness in patients with non-traumatic neck complaints as well as shoulder, arm, and hand problems. In this study, DASH scores ranged from a low score of 59 in the NSNP group to a high score of 81 in the C7 group. Healthy adults between the ages of 40 and 49 usually achieve scores between 9 and 11. 42 The significantly higher DASH scores in the groups, especially in the C7 group, indicate a significant impairment of upper extremity function.
The literature on upper extremity function in individuals with cervical radiculopathy is limited, and studies often lack specific grouping by cervical root level, making it difficult to draw definitive conclusions about root-specific impairments. Daliri et al. reported an average DASH score of 50 in individuals with cervical radiculopathy. 43 The greater impairment observed in our C7 group could be due to the effects on hand dexterity. The poorer Moberg test scores in this group, reflecting impairment in functional sensation, indicate greater difficulty in activities of daily living, a finding consistent with the observed association between DASH and MPUT in hand disorders. 44 Therefore, incorporating exercises to improve functional sensation and hand dexterity into physiotherapy programs for patients with C7 radiculopathy may be critical for improving performance in activities of daily living. Considering the increased sensory deficits observed in all radiculopathy groups, particularly in the C7 group (80%), it is also recommended to integrate bilateral sensory training into treatment programs.
Emotional state has been shown to have an impact on disability in musculoskeletal disorders. In particular, anxiety and depression have been associated with poorer upper extremity function in individuals with cervical radiculopathy. 43 In this study, moderate levels of anxiety was observed in the groups with radiculopathy, while mild anxiety was observed in the NSNP group. Mild depressive symptoms were present in all groups. This suggests that a patient's emotional state may contribute to upper extremity dysfunction. Kinesiophobia may further exacerbate this problem by reducing activity levels, potentially worsening both upper extremity impairment and emotional well-being.
The results of this study have important clinical implications for the rehabilitation of cervical radiculopathy. First, the observed bilateral sensorimotor deficits suggest that assessment protocols should evaluate both extremities, as using the contralateral side as a baseline may lead to assessment bias. These findings are consistent with evidence showing that seemingly unilateral pathologies often manifest bilaterally due to neurophysiological mechanisms such as cross-cortical disinhibition and maladaptive neuroplasticity. 45 Therefore, examination of only the symptomatic side may provide incomplete clinical data. A comprehensive approach requires bilateral assessment and the inclusion of both extremities in therapeutic interventions. Rehabilitation programs should also incorporate level-specific considerations to address the neurological segments involved in cervical radiculopathy to improve treatment efficacy and functional outcomes. Second, the level-specific differences in sensorimotor impairments suggest that rehabilitation programs should be tailored to the affected nerve root. The muscle weakness and decreased pinch strength at all levels of radiculopathy suggest that targeted strengthening of intrinsic hand muscles should be included in rehabilitation protocols. 32 Second, the level-specific differences in sensorimotor impairments suggest that rehabilitation programs should be tailored to the affected nerve root. For example, in C7 radiculopathy, where more pronounced sensory deficits and manual dexterity impairments have been observed, sensory discrimination and fine motor coordination training may improve functional outcomes. 7 In addition to sensorimotor impairments, these patients exhibited lower emotional status, including moderate anxiety and significant kinesiophobia. This emphasizes the importance of integrating psychological interventions into the rehabilitation framework and is consistent with previous research on psychological factors and upper extremity disability in cervical radiculopathy. 46
This study had some limitations. The study design has inherent limitations. Cross-sectional studies are limited in their ability to demonstrate causality, which makes it difficult to determine the direction of relationships between variables. Longitudinal studies are better suited to understand changes over time and the potential impact of interventions. In addition, unequal group size can lead to bias and affect the generalizability of results. Future studies should aim for balanced group sizes to ensure more accurate comparisons. Finally, the lack of a control group consisting of individuals without neck pain limits the scope of our conclusions. The inclusion of such a group would have provided a valuable basis for comparison and allowed a more comprehensive assessment of sensorimotor function in individuals with neck pain compared to healthy controls.
Footnotes
Ethical considerations
Ethical approval was obtained from the Non-Interventional Clinical Research Ethics Committee of Hacettepe University (application number 2021/15-03). The procedures followed were in accordance with the Helsinki Declaration of 1975, as revised in 1983.
Informed consent
Written informed consent was obtained from all participants after the study procedures were explained.
Author contributions
Tuba Eren: Investigation, Methodology, Resources, Data Curation, Visualization, Writing – original draft, Writing – review & editing. Çiğdem Ayhan Kuru: Project administration, Methodology, Supervision, Conceptualization, Writing – review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.