
Abstract
Objectives
No previous studies have investigated the relationship between body perception disturbance (BPD) and functional outcomes in patients who underwent lumbar spinal surgery. This study prospectively investigated temporal changes in BPD and its relationship with postoperative pain and disability in patients who underwent surgery for lumbar spinal stenosis.
Methods
In this prospective observational study, a total of ninety patients who underwent lumbar spinal surgery at our institution between September 2023 and July 2024 were included. BPD, pain intensity, and disability were assessed by using Fremantle Back Awareness Questionnaire, Visual Analog Scale, and Oswestry Disabilty Index at three time points: preoperatively, at discharge, and 3 months postoperatively.
Results
The results showed a significant decrease in BPD from the preoperative period to 3 months postoperatively (p < 0.05). However, no significant association was observed between BPD and the postoperative pain intensity or disability. Furthermore, high preoperative BPD levels had no significant impact on postoperative outcomes at 3 months.
Conclusions
The results of this study suggest that BPD significantly improves postoperatively, and that the effects of preoperative BPD on pain and disability are limited. Further studies with extended follow-up periods and the consideration of psychosocial factors are needed to fully understand the long-term effects of BPD on postoperative outcomes.
Introduction
Lumbar spinal stenosis (LSS) affects 3.65 million individuals aged 40–79 in Japan, with a 10% prevalence among those aged 70–79. 1 In severe cases, surgical treatment makes LSS a leading cause of spinal surgery in older adults. 2 However, approximately one-third of patients are dissatisfied with the results of surgery. 3 Dissatisfaction often arises from persistent residual symptoms like lower limb pain and numbness. 4 Hara et al. reported that 27 (30.3%) of 89 patients with LSS who underwent lumbar decompression surgery continued to experience lower limb pain and numbness. 5 Urgent evidence is needed for effective rehabilitation to address residual symptoms, including chronic postsurgical pain.6,7
Recently, a multifaceted approach based on a biopsychosocial model 8 has been proposed for low back pain (LBP), emphasizing the need to address not only the sensory aspects of pain, the traditional focus of treatment, but also its emotional and cognitive aspects. 9 Regarding the emotional aspect of pain, psychosocial factors such as pain catastrophizing and kinesiophobia have been reported to be strongly associated with chronic pain 9 and chronic LBP (CLBP), 10 leading to the proposition that body perception disturbance (BPD) is one of the factors within the cognitive aspects of pain.11,12 Body perception refers to the ability to accurately perceive and recognize body parts and movements. 13 It has been suggested that pain-induced neuroplastic changes lead to contraction of the brain's body representation area, which in turn results in the deterioration of body image.14,15 Reductions in body image and tactile acuity at the affected site have been observed in patients with CLBP. 16 Additionally, the effectiveness of sensorimotor retraining approaches aimed at improving body image and addressing cortical reorganization, 17 a cause of CLBP, has also been reported. Wand et al. developed the Fremantle Back Awareness Questionnaire (FreBAQ) to assess BPD in patients with LBP. 11 It has been shown to be reliable and valid, with reported associations with pain intensity, disability, pain catastrophizing, and duration of the disease. 11
In a previous study investigating the impact of BPD on CLBP, Yamashita et al. reported that BPD was more associated with the chronicity of LBP than with actual postural abnormalities, 18 based on a comparison between patients with cerebral palsy and those with CLBP. Additionally, in patients with CLBP, the severity of pain itself does not directly cause disability, but BPD mediates the relationship between pain and disability. 19 This indicates BPD's involvement in the chronicity of LBP and the development of disability. However, these studies were conducted in patients with nonspecific CLBP on conservative therapy, and our literature search revealed no prospective studies that investigated the relationship between BPD and functional outcomes in patients who underwent lumbar spinal surgery. While previous studies have reported the impact of anxiety, depression, and pain catastrophizing on postoperative outcomes, 2 as well as the effectiveness of cognitive-behavioral therapy, 20 the influence of BPD on the chronification of LBP and functional prognosis remains inadequately studied. 21 Therefore, the purpose of this study was to elucidate temporal changes in BPD in postoperative patients with LSS and explore their relationship with postoperative pain and disability. We hypothesized that body perception disturbance (BPD) would decrease postoperatively and that preoperative BPD levels might influence postoperative pain and disability.
Materials and methods
Study design
This is a single-institutional prospective cohort study
Participants
Participants were patients diagnosed with LSS at our hospital who underwent surgical treatment between September 2023 and July 2024, and recruited consecutively during preoperative assessments at our hospital.
Inclusion Criteria: (1) ages ≥40 years and (2) cases that could be continuously followed up for evaluation until 3 months postoperatively.
Exclusion Criteria: (1) individuals who had difficulty completing the questionnaire or had incomplete responses due to cognitive problems, and (2) cases involving fixation of more than five vertebrae. This was performed to exclude cases of corrective fixation. Additionally, patients with red flag conditions, such as malignancy or vertebral fractures, and those with a history of previous lumbar surgery were excluded to reduce potential confounding factors that could influence postoperative outcomes.
Radiological diagnosis based on MRI and surgical findings confirmed the type of stenosis. Of the 90 patients analyzed, 78 patients (86.7%) had central canal stenosis, 37 patients (41.1%) had foraminal stenosis, and 32 patients (35.6%) had both types. Fusion procedures were more frequently selected in cases with multilevel stenosis or when foraminal stenosis was prominent on imaging, as these conditions were considered to indicate greater mechanical instability or advanced degeneration.
Although conservative treatment history was not systematically collected as a study variable, retrospective review of medical records revealed that more than 90% of participants had received some form of conservative management prior to surgery. This included pharmacological treatment (e.g., NSAIDs) and/or non-pharmacological interventions such as nerve root blocks. These findings are consistent with standard clinical practice, where surgical intervention for lumbar spinal stenosis is typically reserved for patients with insufficient response to conservative treatment or those with progressive symptoms.
Procedure and ethical considerations
The evaluation time points for the outcome measurements were assessments on the day before surgery, at discharge, and at 3 months postoperatively (Figure 1). Selection bias was minimized by recruiting consecutive patients meeting eligibility criteria, and recall bias was reduced by using validated questionnaires for all assessments. Participants were recruited during preoperative assessments. In accordance with the Declaration of Helsinki, the purpose and details of the study were explained to the participants using an explanatory document. Those who agreed to participate signed a consent form indicating their voluntary participation. This study was approved by the Research Ethics Committee of the Tokyo Metropolitan University Arakawa (Approval Number: 23053), which included approval for obtaining written and verbal informed consent from all participants.
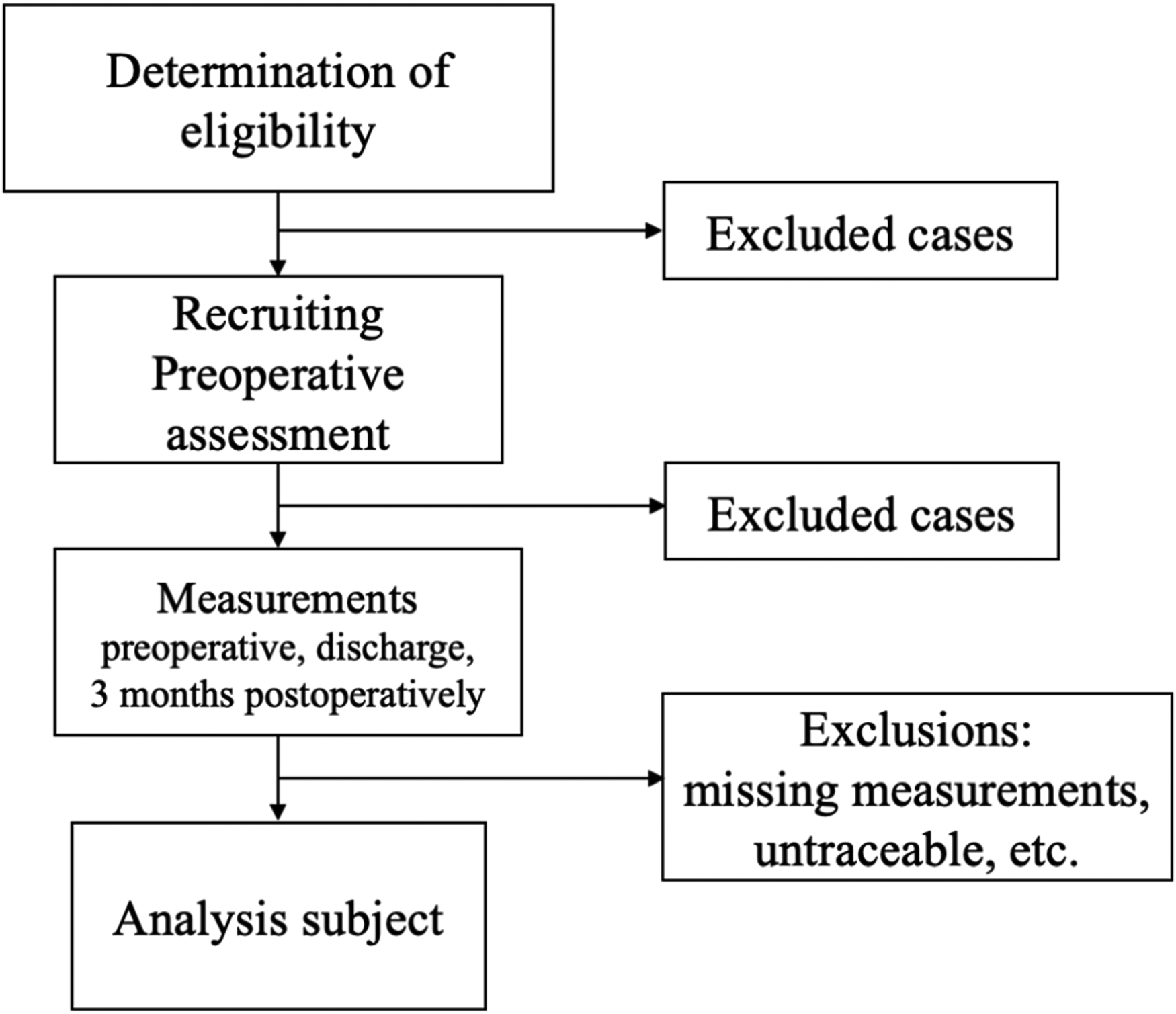
Study flow.
Outcome measurements
Primary Outcomes: Japanese version of the FreBAQ, Visual Analog Scale (VAS) for LBP and lower limb pain intensity, and the Japanese version of the Oswestry Disability Index (ODI).
FreBAQ
FreBAQ is a questionnaire that can assess BPD. 11 The Japanese version was developed by Nishigami et al., and its validity and reliability have been confirmed. 19 The questionnaire consists of nine items related to neglect-like symptoms, proprioception, and body image, scored on a 5-point Likert scale (0–4), with higher scores indicating greater BPD. Although no cutoff values or severity classifications have been reported, the average score for patients with CLBP who visited orthopedic clinics in Japan is reported to be 11.7 ± 6.4, with a median of 10. 19
VAS
The VAS is evaluated on a horizontal line on paper, with the left end (0 mm) representing “no pain (or numbness)” and the right end (100 mm) representing “the worst pain (or numbness) imaginable." 22 The patients were asked to mark the point corresponding to their symptom intensity, and the distance from the left end to the marked point was quantified as the symptom intensity.
ODI
The ODI is widely used internationally to evaluate disabilities specific to LBP. 23 Thus, the reliability and validity of the method have been confirmed. The questionnaire consists of 10 items assessing activities of daily living impaired by LBP, each scored on a 6-point Likert scale (0–5).
Secondary outcome
Patient demographic information (sex, age, height, weight, and body mass index [BMI])
Duration of disease, hospital stay duration, surgical procedure, and number of fixed vertebrae
All secondary outcomes were obtained from the medical records. Disease duration was defined as the number of days from the onset of symptoms to the evaluation date and was categorized as <1 month, 1–3 months, 3–6 months, and >6 months, measured on an ordinal scale. The duration of the hospital stay was measured from the date of surgery to the date of discharge. Surgical procedures were categorized as either decompression or fusion. The procedures included in this study were lumbar laminectomy, microendoscopic laminectomy, full endoscopic laminectomy for decompression, posterior lumbar interbody fusion, transforaminal lumbar interbody fusion, lateral lumbar interbody fusion, and posterolateral fusion for fusion.
Statistical analysis
Longitudinal changes in BPD
The longitudinal changes in the FreBAQ from preoperative period to 3 months postoperatively were assessed using the Mixed-effects Model for Repeated Measures (MMRM), a type of linear mixed model used to analyze incomplete longitudinal measurement data. Multiple comparisons were performed using Tukey's method if significant differences were observed.
Relationship between BPD, pain, and disability
The relationships between the 3-month postoperative VAS score and ODI with each measurement item were evaluated using an Linear Mixed Model (LMM), which adjusted for covariates and examined the interaction effects. The objective variables were the 3-month postoperative VAS and ODI, which included age, sex, BMI, surgical procedure, number of fixed vertebrae, disease duration, preoperative VAS (LBP and leg pain), preoperative ODI, and preoperative FreBAQ scores, with participant's ID included as a random effect. An LMM was employed to examine the relationship between preoperative BPD and postoperative pain/disability while adjusting for potential confounders. Patient ID was included as a random effect to account for individual-level variability, while fixed effects included demographic factors, surgical details, and preoperative clinical scores.
A complete case analysis was performed, and participants with missing data for primary outcome measures were excluded from the final analysis. Of the 136 patients initially enrolled, 36 were excluded from the final analysis due to missing data on primary outcome measures, such as incomplete responses to the FreBAQ, VAS, or ODI at one or more of the three evaluation time points. As a result, a total of 90 participants were included in the complete case analysis. This approach was chosen because the proportion of missing data was moderate and assumed to be missing at random (MAR). Complete case analysis is a commonly used and accepted method in clinical research when the risk of systematic bias is low and the sample size remains sufficient for statistical power. Therefore, we considered this approach appropriate for maintaining consistency and validity in our statistical analyses. All statistical analyses were performed using the SPSS ver. 27 (IBM, NY, USA) with a significance level of 5%.
Sample size
The sample size was calculated using the G*Power ver. 3.1 (Faul, University, Kiel, Germany). To test the differences in repeated measures with an effect size of η² = 0.25, an α error of 0.05, a power of 0.8, and three measurement points, the required sample size was 28 cases.
Additionally, the independent variables included in the LMM regression model were age, sex, BMI, surgical procedure, disease duration, number of fixed vertebrae, preoperative ODI, preoperative VAS (LBP or leg pain), and preoperative FreBAQ score, totaling nine variables. Assuming that 10 cases per independent variable would be needed for LMM regression analysis, a total of 90 cases were considered necessary; therefore, the target sample size was set at 90 cases. In this study, we also considered the possibility of patient dropout and, thus, set a study period that would allow us to obtain the required number of cases.
Results
Participants
Figure 2 shows a flowchart of this study. During the study period, 136 patients underwent surgical treatment for LSS at our hospital. One patient aged <40 years, nine patients who underwent fixation on more than five vertebrae, and 36 patients who were untraceable for follow-up were excluded, leaving 90 patients for analysis. The demographic data of the participants is shown in Table 1. Missing data were most commonly observed in incomplete questionnaires.
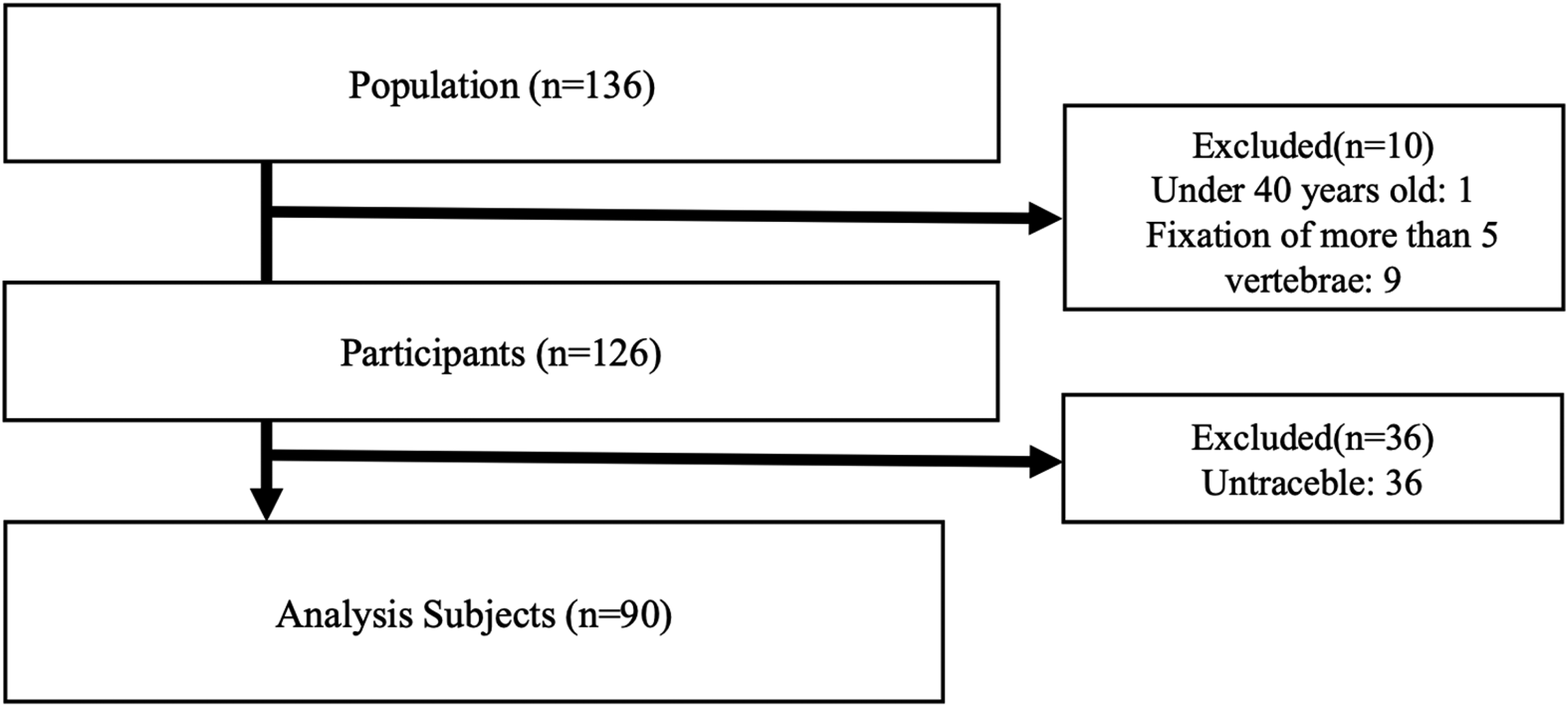
Flowchart of patient selection.
Demographic data.
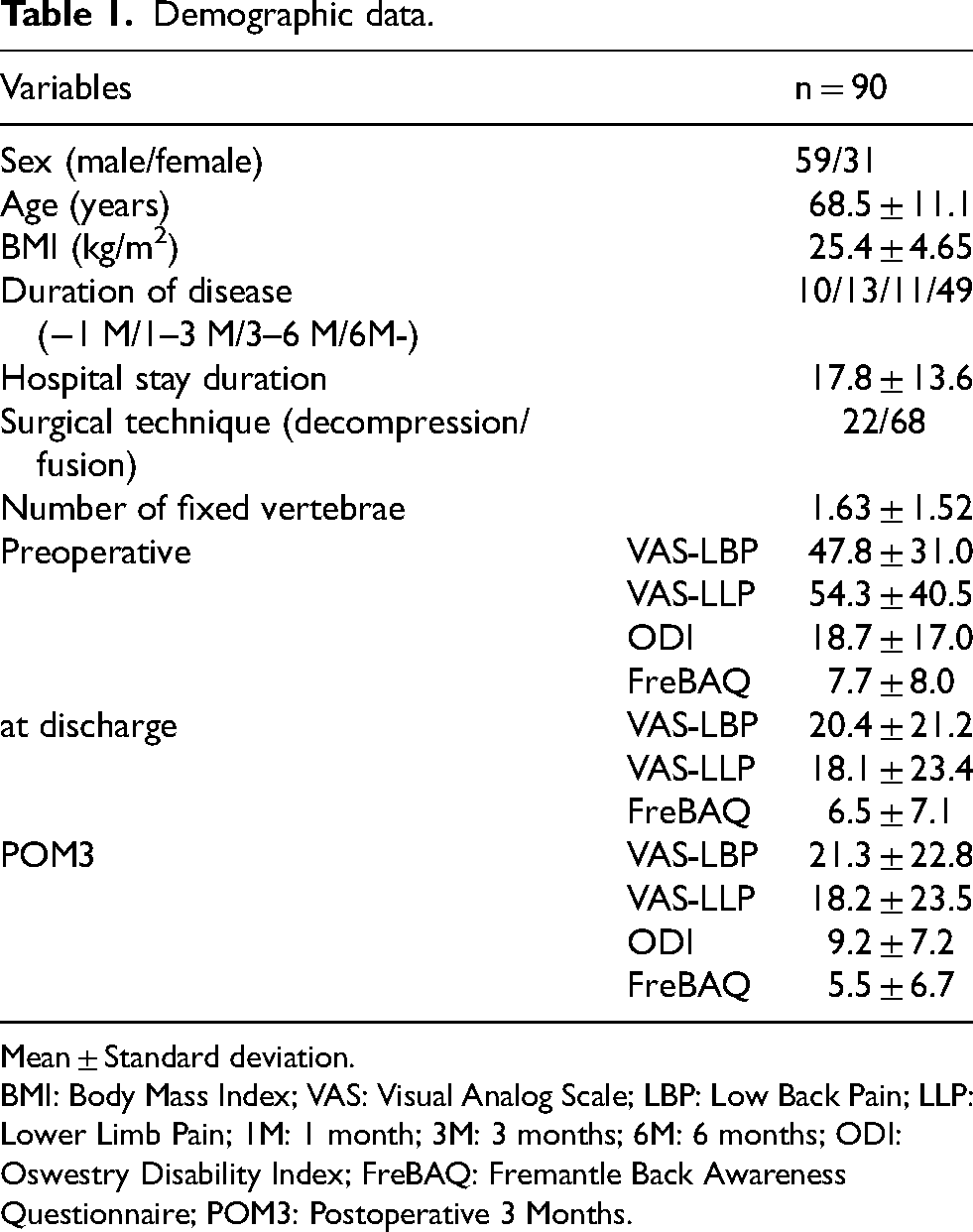
Mean ± Standard deviation.
BMI: Body Mass Index; VAS: Visual Analog Scale; LBP: Low Back Pain; LLP: Lower Limb Pain; 1M: 1 month; 3M: 3 months; 6M: 6 months; ODI: Oswestry Disability Index; FreBAQ: Fremantle Back Awareness Questionnaire; POM3: Postoperative 3 Months.
Comparison between fusion and decompression groups
We compared the baseline characteristics between patients who underwent decompression surgery alone (n = 22) and those who received fusion surgery (n = 68). Patients in the fusion group were significantly older than those in the decompression group (mean age: 70.1 ± 9.4 vs. 63.7 ± 12.8 years, p = 0.003). The preoperative FreBAQ scores were also significantly higher in the fusion group (8.9 ± 8.6 vs. 4.9 ± 6.4, p = 0.009). However, there were no significant differences between the two groups in terms of preoperative ODI (p = 0.89), VAS for low back pain (p = 0.65), or VAS for leg pain (p = 0.74). No significant differences were found in sex, BMI, or disease duration.
Longitudinal changes in FreBAQ
According to the MMRM results on the longitudinal changes in FreBAQ, there were significant differences among the three groups classified by evaluation timepoints: 7.7 ± 8.0 for preoperative, 6.5 ± 7.1 for discharge, and 5.5 ± 6.7 for 3 months postoperative (p < 0.05) (Table 2). Post hoc tests revealed that the preoperative FreBAQ scores were significantly higher than those at 3 months postoperatively (p < 0.05) (Table 2, Figure 3). No significant differences were observed between the FreBAQ scores at discharge and those preoperatively or 3 months postoperatively (Table 2, Figure 3).
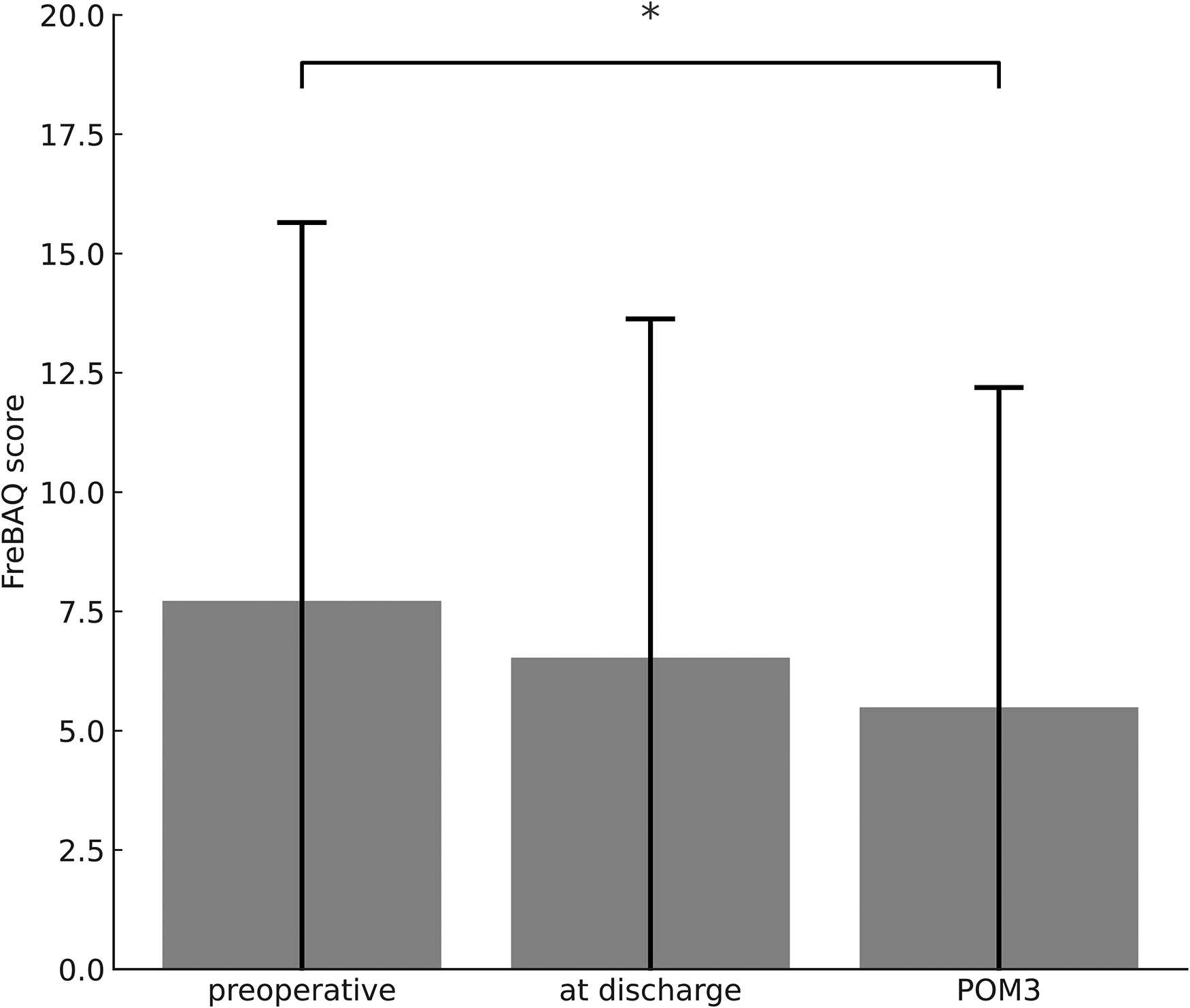
Temporal changes in FreBAQ scores. POM3: Postoperative 3 Months *: Statistically significant
Mixed model repeated measures and the post hoc analysis by Tukey method for FreBAQ.
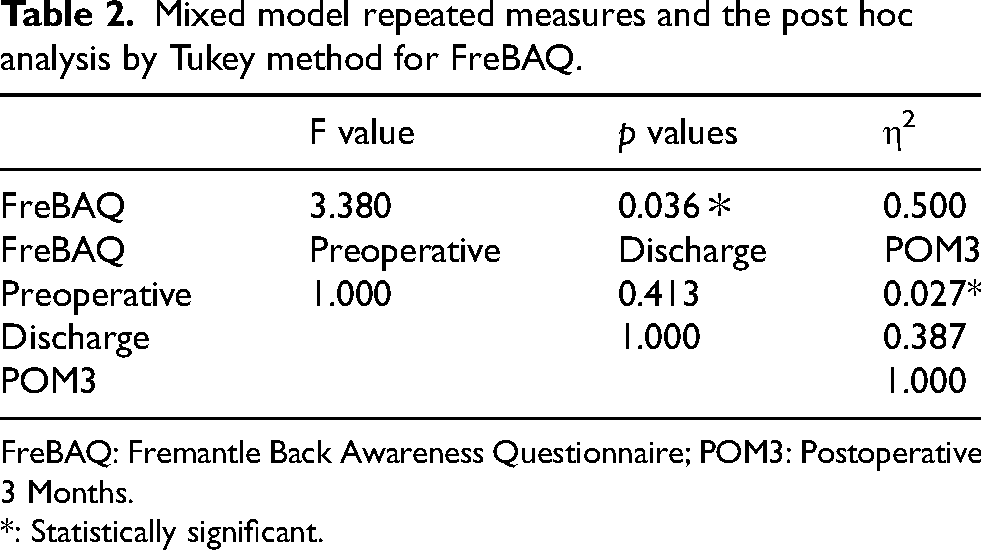
FreBAQ: Fremantle Back Awareness Questionnaire; POM3: Postoperative 3 Months.
*: Statistically significant.
Relationship between FreBAQ, LBP and leg pain VAS, and ODI
The LMM results showed a significant association between the 3-month postoperative LBP VAS score and the preoperative ODI (coefficient = 0.671, 95% CI: 0.200–1.142, p < 0.05) (Table 3). No significant associations were found between the 3-month postoperative leg pain VAS scores and other factors (p > 0.05) (Table 4). A significant association was observed between the 3-month postoperative and preoperative ODI scores (coefficient = 0.280, 95% CI: 0.148–0.411, p < 0.05) (Table 5).
The result of LMM analysis for 3-month postoperative low back pain VAS.
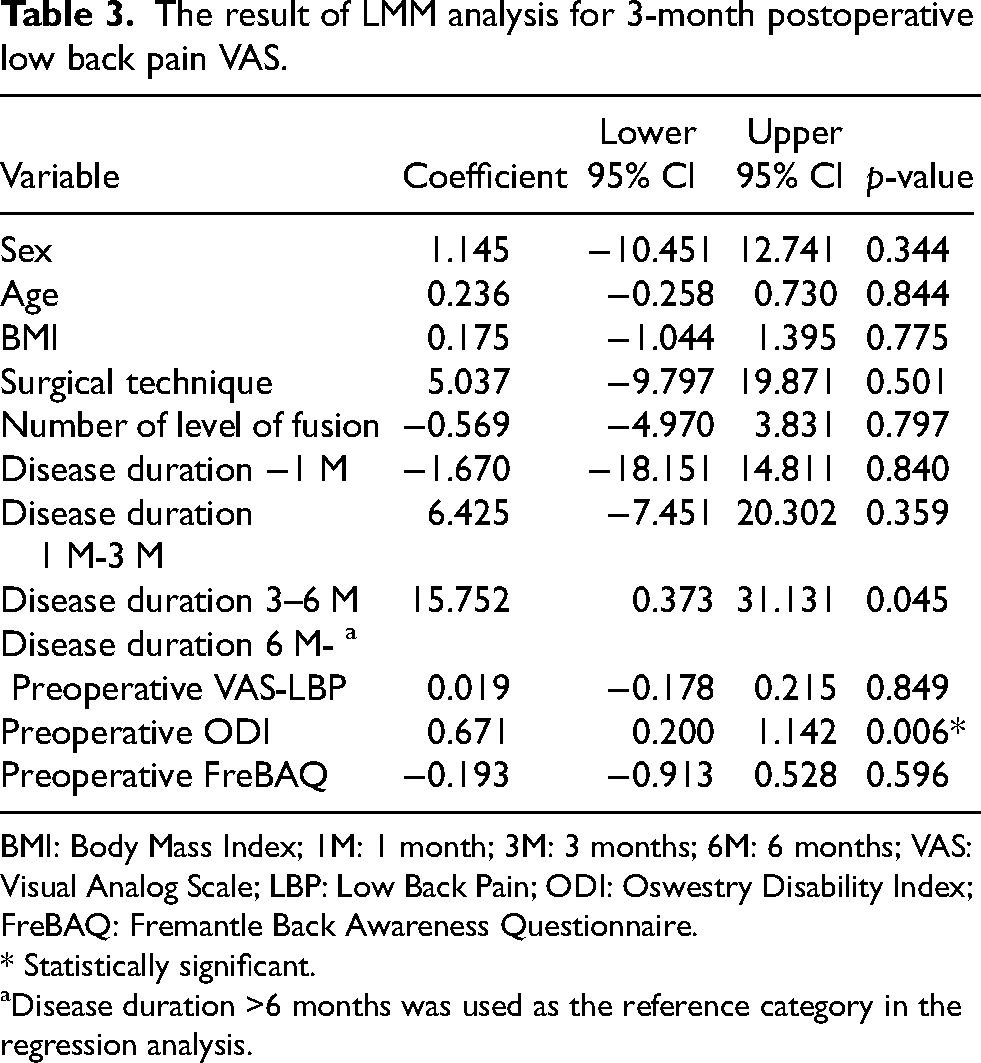
BMI: Body Mass Index; 1M: 1 month; 3M: 3 months; 6M: 6 months; VAS: Visual Analog Scale; LBP: Low Back Pain; ODI: Oswestry Disability Index; FreBAQ: Fremantle Back Awareness Questionnaire.
* Statistically significant.
Disease duration >6 months was used as the reference category in the regression analysis.
The result of LMM analysis for 3-month postoperative lower limb pain VAS.
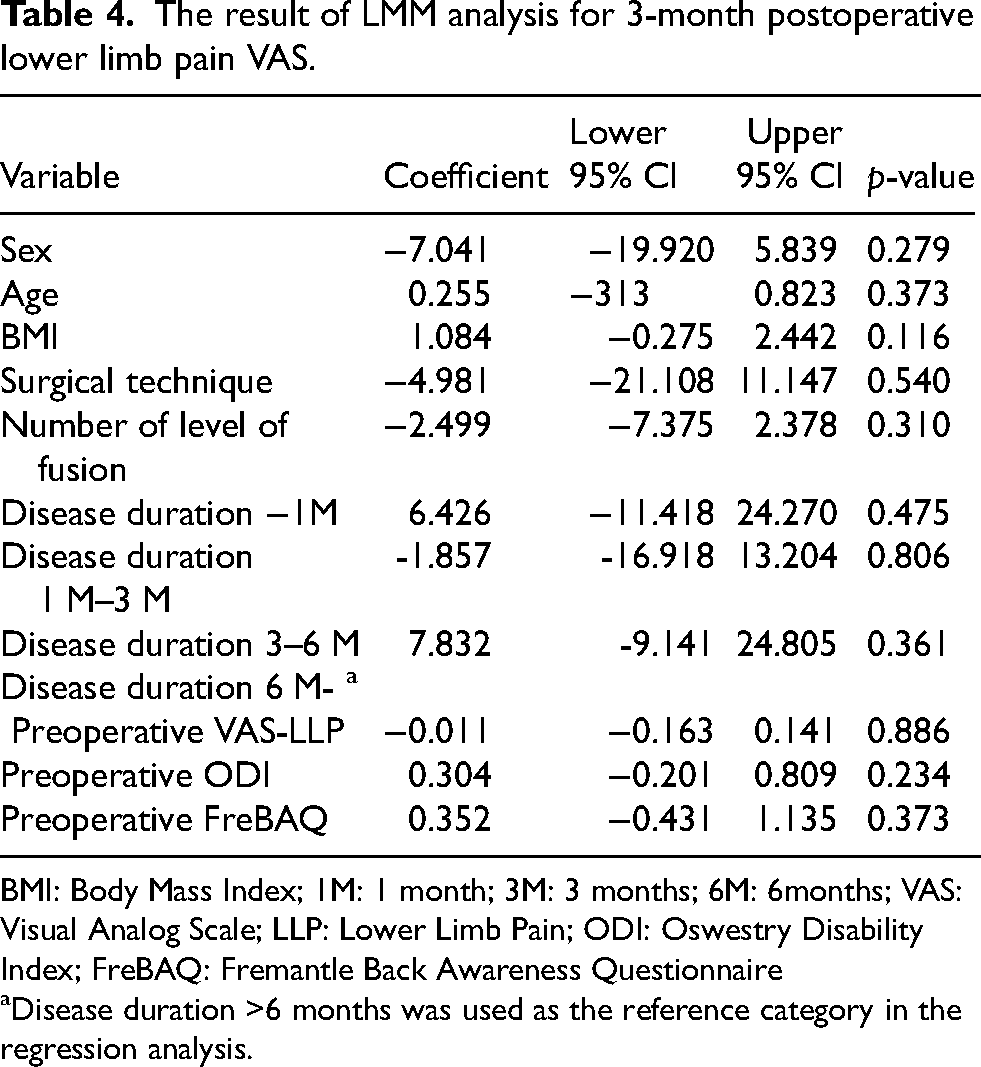
BMI: Body Mass Index; 1M: 1 month; 3M: 3 months; 6M: 6months; VAS: Visual Analog Scale; LLP: Lower Limb Pain; ODI: Oswestry Disability Index; FreBAQ: Fremantle Back Awareness Questionnaire
Disease duration >6 months was used as the reference category in the regression analysis.
The result of LMM analysis for 3-month postoperative ODI.
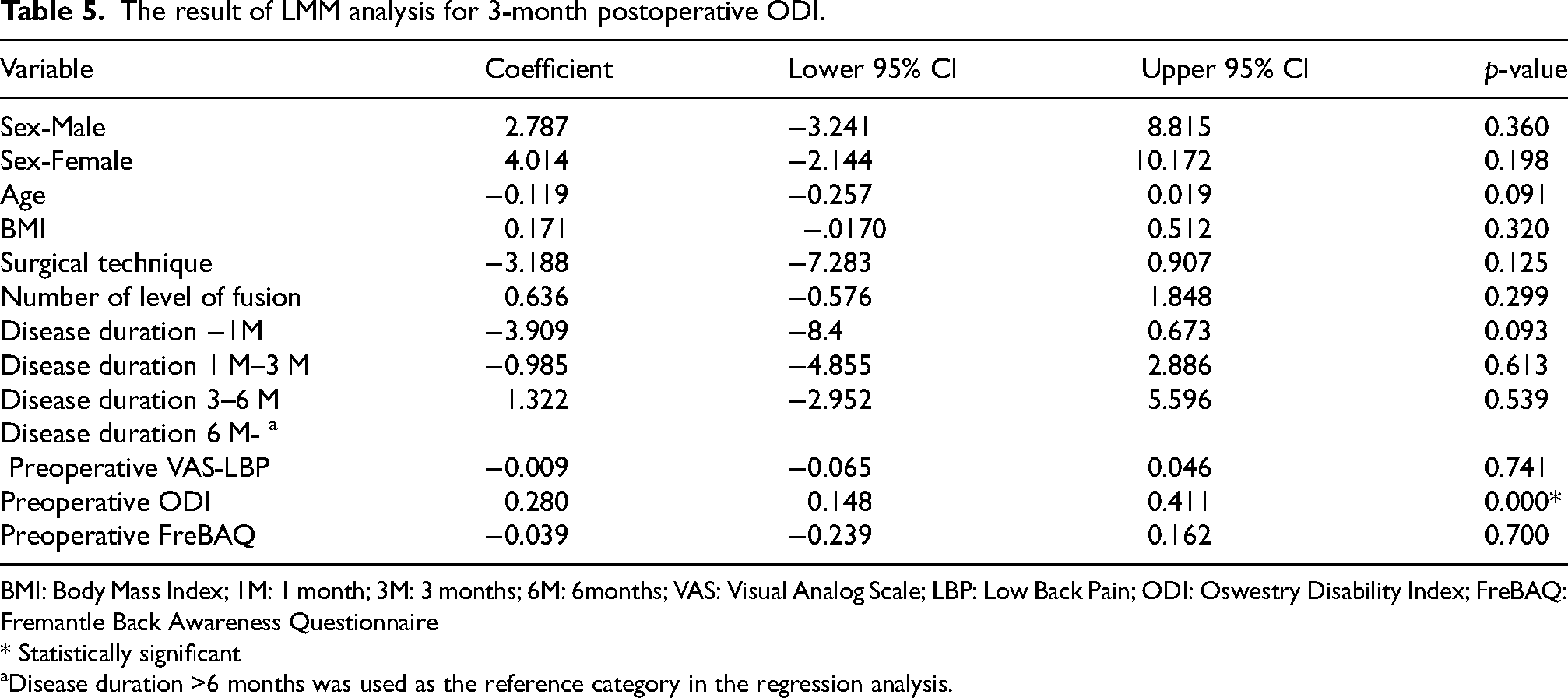
BMI: Body Mass Index; 1M: 1 month; 3M: 3 months; 6M: 6months; VAS: Visual Analog Scale; LBP: Low Back Pain; ODI: Oswestry Disability Index; FreBAQ: Fremantle Back Awareness Questionnaire
* Statistically significant
Disease duration >6 months was used as the reference category in the regression analysis.
Discussion
This study prospectively investigated longitudinal changes in BPD in patients after surgery for LSS and their impact on postoperative pain and disability. The results showed that BPD significantly decreased at 3 months postoperatively compared to preoperative levels. Additionally, preoperative BPD was not significantly associated with pain intensity or disability 3 months postoperatively.
Our study is the first to investigate the longitudinal changes in BPD and their impact on postoperative functional outcomes in patients undergoing LSS. The relationship between pain intensity and BPD may have influenced the observed decrease in BPD from preoperative to 3 months postoperative levels. Wand et al. have suggested that BPD is associated with pain intensity and disability. 12 Therefore, we hypothesized that the reduction in BPD may have been driven by the pain-relieving effects of surgery24,25 and the natural course of postoperative recovery, leading to decreased pain intensity and improved disability. Caneiro et al. reported a longitudinal association between pain intensity and disability and cognitive-emotional factors of pain, 26 and the results of this study were consistent with those of previous studies. Hence, the longitudinal changes in BPD observed in this study may have been influenced by the changes in pain intensity and disability over time. Although the specific mechanisms underlying the postoperative decrease in BPD cannot be fully elucidated from the results of this study alone, Sundermann et al. suggested that chronic pain can alter body image owing to unpleasant sensory and emotional experiences associated with pain. 27 Furthermore, recent studies on pain and cortical plasticity suggest that cortical plasticity associated with chronic pain can be improved through interventions such as feedback to brain regions altered by somatosensory pain memory and pharmacological therapies that prevent or treat the formation of maladaptive memories. 28 Therefore, it is conceivable that the improvement in BPD observed in this study may be due to the reorganization of the somatosensory cortex 14 and somatic perception, which had been impaired by pain, following postoperative pain relief.
Regarding the impact of BPD on pain intensity and disability, Wand et al. reported that the FreBAQ was associated with pain intensity and disability in a study involving patients with CLBP. 12 However, the results of the present study differ from those of previous studies. The reasons for the difference may be the characteristics of the participants, the multifaceted nature of pain, and the mechanism of pain chronicity. While the previous study included patients with CLBP who received conservative therapy, this study included patients with postoperative LSS. Since this study investigated the impact of preoperative BPD on postoperative pain intensity and disability, it likely reflects the influence of the postoperative course. In addition, the relatively high proportion of fusion surgeries and the lower preoperative ODI scores observed in our cohort may reflect the clinical characteristics of our institution, which is a specialized spine surgery center. At such facilities, surgical intervention may be considered even for patients with relatively mild disability when imaging findings, such as central canal or foraminal stenosis, indicate the potential for future symptom progression. This institutional tendency has been similarly reported in previous studies, where lumbar spinal stenosis patients with comparable baseline ODI values underwent surgical treatment despite relatively low disability levels. 29 Therefore, we believe that the clinical profile of our cohort is consistent with that of similar surgical populations in comparable healthcare settings, supporting the applicability of our findings within this context. Furthermore, it has been demonstrated that the emotional and cognitive aspects of pain do not directly influence pain itself but rather act as indirect mediators.30,31 For instance, mechanisms have been proposed whereby anxiety, depression, and pain catastrophizing related to pain enhance central sensitization, 30 ultimately worsening pain perception and disability. Pain catastrophizing amplifies psychological stress and fear, which in turn increases pain sensitivity and delays recovery.
Regarding the impact of factors other than BPD on pain intensity and disability, previous studies have identified several risk factors for persistent postoperative pain, including preoperative pain intensity, walking distance, physical activity level, comorbid medical conditions such as hypertension and diabetes, and psychosocial factors.32–34 In this study, the only factor significantly associated with LBP and disability at 3 months postoperatively was the preoperative ODI. This finding is consistent with previous research reporting that higher preoperative disability is associated with higher postoperative pain and disability. 33 These results suggest that focusing on patients with LSS from the preoperative period to 3 months postoperatively provides valuable insights into the specific management of persistent pain and disability after surgery, which differs from conservative CLBP.
Concerning the lack of an impact of BPD on pain and disability at 3 months postoperatively, Caneiro et al. also supported the longitudinal changes in pain intensity, disability, and other pain-related factors. 26 However, they reported that the factors most strongly associated with changes in disability varied among individual cases, highlighting the importance of individualization. 26 Additionally, Marcuzzi et al. found that in patients with CLBP, there was a significant change in mechanical pain sensitivity compared to the control group, 35 suggesting that enhanced mechanical sensitivity may contribute to the progression of CLBP. There has been increasing awareness of the necessity of subgrouping in the management of LBP, 36 and it has also been reported that not all patients with CLBP experience sensorimotor incongruence, 37 indicating the importance of further subgrouping and individualization. Therefore, further large-scale and detailed investigations are required to clarify the relationships among BPD, postoperative pain, and disability.
This study had some limitations. First, the limited study period of 3-month follow-up was a constraint. This study evaluated only short-term longitudinal changes, potentially missing evaluations of chronic pain, disability changes, and risk of recurrence. Second, the physical findings were not evaluated in this study. By enabling these assessments, the mechanisms related to temporal changes in BPD and their relationships with functional outcomes can be more clearly elucidated. Therefore, the limited impact of preoperative BPD on pain intensity and disability cannot be discussed in this study. Third, we did not systematically collect data on whether participants had received conservative treatment prior to surgery. However, it is generally understood that surgical intervention for lumbar spinal stenosis is typically indicated in patients with severe or progressive symptoms, or in those who do not respond to conservative management. Therefore, we assume that the majority of our participants either had already undergone non-surgical treatment without sufficient relief or presented with symptoms severe enough to warrant surgical intervention at the time of diagnosis. Fourth, some follow-up data were missing. The main reasons for this data loss included emergency discharge and failure to attend follow-up visits; however, it should be noted that the outcomes of these cases were not taken into consideration. Fifth, since this was a single-center study, findings may not be generalizable to other populations with different surgical practices. Finally, the study did not include psychosocial factors. Although this study adjusted for key confounding variables using an LMM, unmeasured confounders may still exist. In particular, psychological factors such as pain catastrophizing, depression, and social support, which have been shown to influence postoperative outcomes, were not included in the analysis. Future studies should incorporate these psychosocial variables to improve the robustness of the findings. Recognizing these limitations, future studies should involve larger-scale and longer-term investigations as well as a more detailed evaluation of other factors, including psychosocial factors.
Despite the single-center nature of our study, the demographic characteristics and surgical profiles were similar to those reported in previous multicenter studies, supporting some degree of external validity. Nonetheless, validation in more diverse clinical settings is warranted. From a clinical standpoint, routine assessment of BPD using FreBAQ prior to surgery may help identify patients at risk of altered postoperative recovery patterns, thereby enabling early intervention through sensorimotor retraining or cognitive rehabilitation.
Conclusion
This longitudinal study investigated the impact of BPD on pain and disability in patients after surgery for LSS. It was found that preoperative BPD significantly decreased at 3 months postoperatively. The direct impact of preoperative BPD on pain and disability reduction 3 months postoperatively is limited. These results suggest that BPD does not necessarily affect postoperative pain or disability in all patients. However, because surgical treatment may contribute to the improvement of BPD itself, it is necessary to consider the research methods and subgroups involved in the chronicity of postoperative pain and individualized approaches. Therefore, future research should further investigate the mechanisms underlying postoperative improvement in BPD and its long-term effects.
Footnotes
Acknowledgements
We would like to thank Editage for English language editing.
Ethical approval and informed consent statements
In accordance with the Declaration of Helsinki, the purpose and details of the study were explained to the participants using an explanatory document. Those who agreed to participate signed a consent form indicating their voluntary participation. This study was approved by the Research Ethics Committee of the Tokyo Metropolitan University Arakawa (Approval Number: 23053).
Consent to participate
Informed consent to participate in this study was obtained both verbally and in writing from all participants.
Author contribution
Conceptualization: YK, AE, RY, TT, HK; Methodology: YK, AE, KK ; Formal analysis and investigation: YK, AE, KK, RF; Writing – original draft preparation: YK; Writing – review and editing: AE, KK, RF, SO, RY, TT, HK; Supervision: AE, SO, HK.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.