
Abstract
Background and Purpose
Upper limb motor impairment after stroke is a leading cause of long-term disability. This single-center pilot randomized controlled trial (RCT) evaluated the safety, feasibility, and preliminary efficacy of intermittent theta-burst stimulation (iTBS) combined with task-oriented training (TOT) for upper limb rehabilitation. iTBS, a non-invasive brain stimulation technique, may enhance recovery when paired with task-oriented training (TOT), particularly in the subacute phase of heightened neuroplasticity.
Methods
Twenty-nine patients with subacute stroke were randomized into three groups: (1) iTBS + TOT (n = 10), (2) sham iTBS + TOT (n = 9), and (3) traditional physiotherapy (n = 10). All underwent a 4-week intervention. Primary outcomes were safety and feasibility. Secondary outcomes included motor impairment (Fugl-Meyer Assessment for Upper Extremity, FMA-UE), functional independence (Modified Barthel Index, MBI), and neurological deficit (National Institutes of Health Stroke Scale, NIHSS), assessed at baseline, week 2, and week 4.
Results
Twenty-nine participants completed the trial without any adverse events, and one participant from Group 2 discontinued early due to discharge. At week 4, the iTBS + TOT group showed greater improvements in FMA-UE (22.9 points vs. 3.6 and 10.2; p = 0.013; p = 0.013), NIHSS (3.0 vs 6.6; p = 0.009), and MBI (90.7 vs 51.4; p < 0.001) compared with controls, indicating potential functional benefits.
Conclusions
This exploratory pilot RCT suggests that combining iTBS with TOT is safe and feasible, with preliminary evidence supporting its potential to improve upper limb recovery in subacute stroke. However, these findings should be interpreted with caution and validated in larger, adequately powered trials.
Introduction
According to recent reports, there were an estimated 93.8 million prevalent cases of stroke globally in 2021. 1 Stroke remains a leading cause of long-term disability, particularly affecting upper limb (UL) function, with 55% to 75% of survivors experiencing persistent motor impairments three to six months post-stroke.2–4 In recent years, rehabilitation strategies have increasingly emphasized early intervention and the incorporation of highly engaging, task-specific motor activities to enhance recovery outcomes.5,6 Beyond conventional motor rehabilitation, an effective strategy to promote motor recovery is to balance the inhibitory and excitatory processes. During the early stages following stroke, various reorganization processes occur in both the affected and unaffected hemispheres, and these changes are closely linked to motor outcomes. 7 In recent decades, non-invasive brain stimulation (NIBS) has garnered attention for its potential to improve functional recovery in neurological disorders, such as stroke. 8 Despite these advances, meaningful recovery of upper limb function remains a challenge, as motor improvements often plateau after the first few month's post-stroke, following a critical recovery window.9,10 The present study focused on patients in the subacute phase of stroke recovery, typically defined as 1 week to 6 months post-stroke, a period characterized by heightened neuroplasticity, spontaneous neurological recovery, and increased responsiveness to rehabilitation interventions, 11 highlighting the need for effective approaches to enhance functional recovery during this window.
Repetitive transcranial magnetic stimulation (rTMS), a non-invasive brain stimulation technique, has been increasingly recognized as a promising intervention for enhancing motor performance in the affected upper limb of stroke patients. Although its precise mechanisms are not yet fully understood, rTMS is generally believed to improve functional outcomes by modulating motor cortical excitability and promoting neural network reorganization. 12 Importantly, rTMS is thought to facilitate an environment conducive to neuroplasticity rather than directly driving skill acquisition. Consequently, prior studies have suggested that combining rTMS with conventional rehabilitation produces greater motor improvements than rTMS alone.13,14 This has led to the growing use of rTMS in conjunction with behavioral motor interventions to maximize recovery. Intermittent theta-burst stimulation (iTBS), a patterned and time-efficient form of rTMS, has emerged as a potentially more effective alternative, offering similar or enhanced efficacy in modulating brain activity while requiring shorter stimulation durations.15,16
On the other hand, Task-oriented training (TOT) is a rehabilitation approach designed to help individuals develop effective control strategies for performing meaningful tasks in real-world settings. 17 Its core principles include intensive and repetitive practice of functional movements, progressive task difficulty, and the use of timely, positive feedback to reinforce learning.18,19 Systematic reviews have demonstrated that TOT can improve arm-hand function and enhance health-related quality of life among stroke survivors with upper limb impairments.20,21 However, most existing evidence has been derived from studies involving individuals in the chronic phase of stroke recovery. 22 Research investigating the effectiveness of TOT in the subacute phase remains limited, with inconsistencies in intervention protocols and outcome measures. 23
Considering these limitations and the recognized potential of NIBS to enhance neuroplasticity, there is growing interest in integrating modalities such as iTBS with TOT to amplify rehabilitation outcomes, particularly in the subacute stage when the brain is most responsive to intervention. Specifically, administering TOT immediately following iTBS capitalizes on the stimulation-induced transient enhancement of cortical excitability, which facilitates long-term potentiation (LTP)-like synaptic plasticity via N-methyl-D-aspartate receptor-dependent mechanisms, thereby promoting Hebbian associative strengthening during motor practice and optimizing motor learning. 24
Recent systematic reviews have highlighted the synergistic potential of combining NIBS with task-specific motor training to facilitate functional recovery and promote neuroplasticity.25,26
To address this gap, we conducted a single-center pilot randomized controlled trial to explore the feasibility, safety, and preliminary efficacy of combining iTBS with TOT on upper-limb motor function in individuals with subacute stroke.
Methods
Trial design
This study used a single-blind, pilot randomized controlled trial design. Participants were randomly assigned to one of three groups (1:1:1 ratio) using a computer-generated sequence prepared and executed by an independent researcher who was not involved in treatment or outcome assessment. Outcome assessors, licensed occupational therapists, were blinded to group assignments. Although blinding of participants was not possible for all groups due to the nature of the interventions, participants in groups 1 and 2 were blinded to whether they received real or sham iTBS.
The study adhered to the ethical principles outlined in the Declaration of Helsinki and was approved by the Ethical Review Committee of the Second Affiliated Hospital of Chongqing Medical University, China (Approval No. 2024[57]). All participants provided written informed consent. This trial is registered with the Chinese Clinical Trial Registry (ChiCTR2200066978) and follows the Consolidated Standards of Reporting Trials (CONSORT) reporting recommendations. 27 The current study reports findings from the first sub-study of the larger registered trial.
Participants
Participants were recruited from the Rehabilitation Medicine Department at the second affiliated hospital of Chongqing Medical University, China, between September 2023 and November 2024. The inclusion criteria were as follows: 1) first-ever unilateral ischemic or hemorrhagic stroke affecting the middle cerebral artery, confirmed by computed tomography (CT) or magnetic resonance imaging (MRI), and with stroke onset between 1 to 6 months before enrollment; 2) age between 18 and 80 years; and 3) ability to provide written informed consent and comprehend study instructions. Exclusion criteria included: 1) significant cerebral infarction or hemorrhage in the frontal and/or temporal lobes; 2) major cardiovascular or respiratory illnesses, pregnancy, or unrelated neurological conditions, and severe orthopedic impairments affecting limb function; 3) history of cancer; 4) recent use of medications that affect cortical excitability (e.g., sedatives, antidepressants), a history of seizures, dementia, cognitive impairment, or neurodegenerative disorders; and 5) the presence of implanted devices (e.g., pacemakers or metallic objects in the head) that are contraindicated for transcranial magnetic stimulation or MRI. A CONSORT diagram illustrating randomization, treatment procedures, and group allocation is presented in Figure 1.
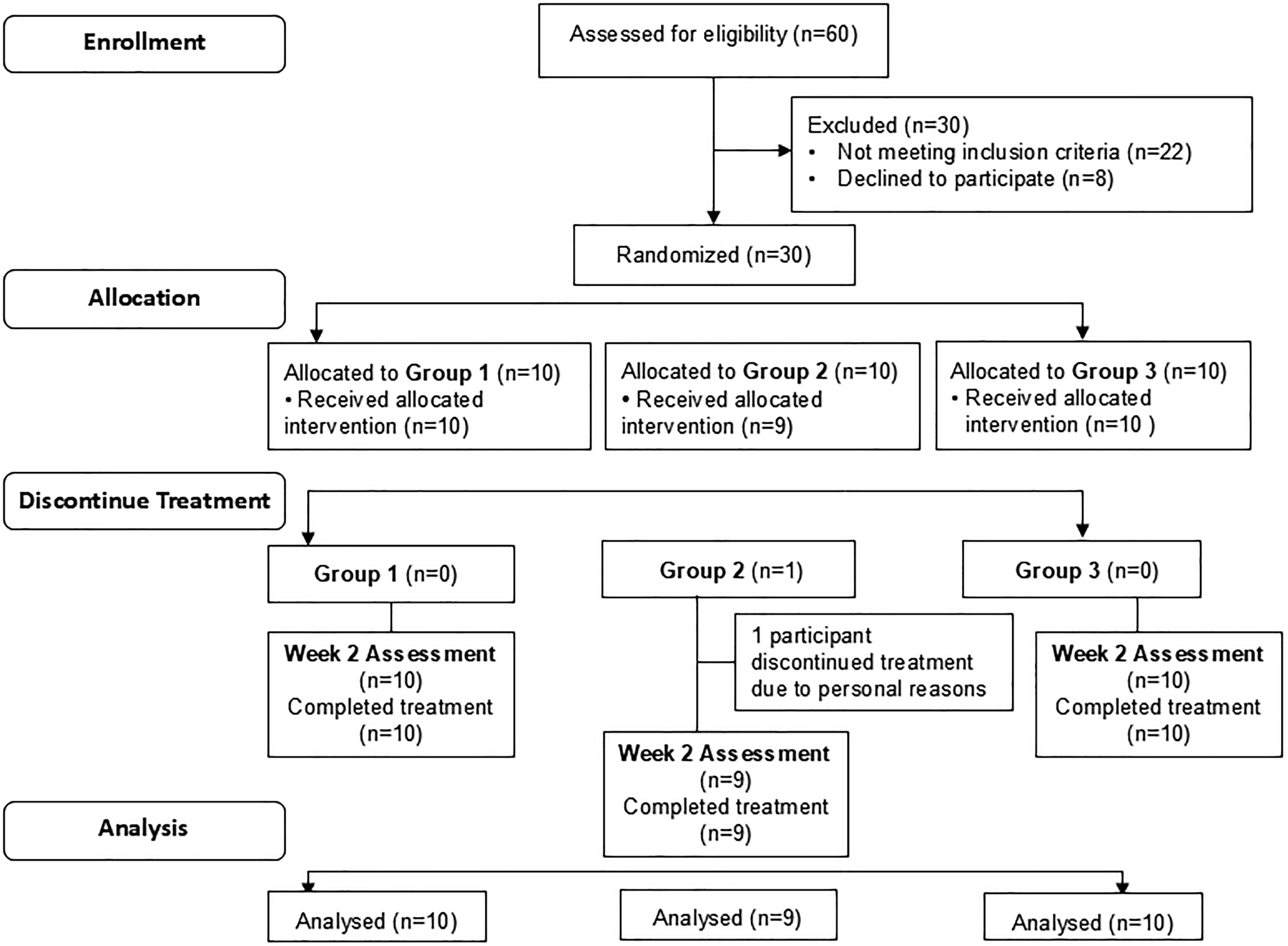
CONSORT flow diagram showing enrollment, randomization, allocation, discontinuation, and analysis of participants.
Treatment and group allocation
Each group followed a hospital-based, tailored training program. The program consisted of 45-min sessions, delivered daily for four weeks, and totaled 21 h of training. All interventions were administered by licensed physiotherapists with a minimum of 3 years of clinical experience in neurorehabilitation and prior training in task-oriented therapy and transcranial magnetic stimulation procedures. The therapists were blinded to treatment outcomes. Each session began with the application of either real or sham to the ipsilesional M1, immediately followed by task-oriented training. Participants in 1) Group 1 (iTBS + TOT) received iTBS in combination with task-oriented training; 2) Group 2 (Sham iTBS + TOT) received sham iTBS combined with task-oriented training; and Group 3 (Exercise Group) received traditional physical therapy.
iTBS protocol
We employed the original iTBS protocol, as described by Huang et al., which consists of triplet 50 Hz bursts delivered at 5 Hz intervals (i.e., 2 s on, 8 s off), for 190 s, totaling 600 pulses once daily for four weeks. Stimulation was administered using a figure-of-eight, fluid-cooled coil (inner diameter: 40 mm; outer diameter: 90 mm) connected to a transcranial magnetic stimulator (M-100 Ultimate, Yingchi, Shenzhen Yingchi Technology Co., Ltd, Shenzhen, China). 28 iTBS was delivered at the 80% individual resting motor threshold (RMT). 29 The RMT was defined as the minimum stimulation intensity over the motor hotspot that elicited an MEP of ≥50 μV in at least 5 out of 10 consecutive trials recorded from the contralateral first dorsal interosseous (FDI) muscle. The motor hotspot was identified as the scalp location eliciting the most robust and consistent MEPs from the contralateral FDI. To maintain consistency and reliability in stimulation intensity across participants, RMT was determined unilaterally, following commonly adopted procedures in stroke neuromodulation studies.30,31 Sham iTBS was administered by tilting the coil 90 degrees off the scalp, with one wing of the coil touching the scalp. 32 By doing this, the induced electrical current flow in the cortex can be largely minimized. 33 Figure 2 demonstrates a practical evaluation of finding a motor hotspot.

Practical evaluation of finding the motor hotspot.
Task-oriented training
In the TOT program, participants performed four out of six functional tasks tailored to their individual preferences. Task selection was guided by each participant's baseline motor function, observed movement capabilities, and Fugl-Meyer upper extremity scores. Therapists collaborated with participants to select tasks that were both meaningful and appropriately challenging.
Task difficulty was progressively increased throughout the intervention using motor control principles and standardized strategies outlined in the Upper Extremity Task-Specific Training Manual by a previous study. 34 Specific progression methods included increasing the required range of motion, adding resistance (e.g., weights to the object or limb), modifying the size or pliability of objects, and advancing from gross to fine motor tasks involving object manipulation. 35 All treating therapists were oriented to these progression strategies before study initiation to ensure consistency in intervention delivery across participants.
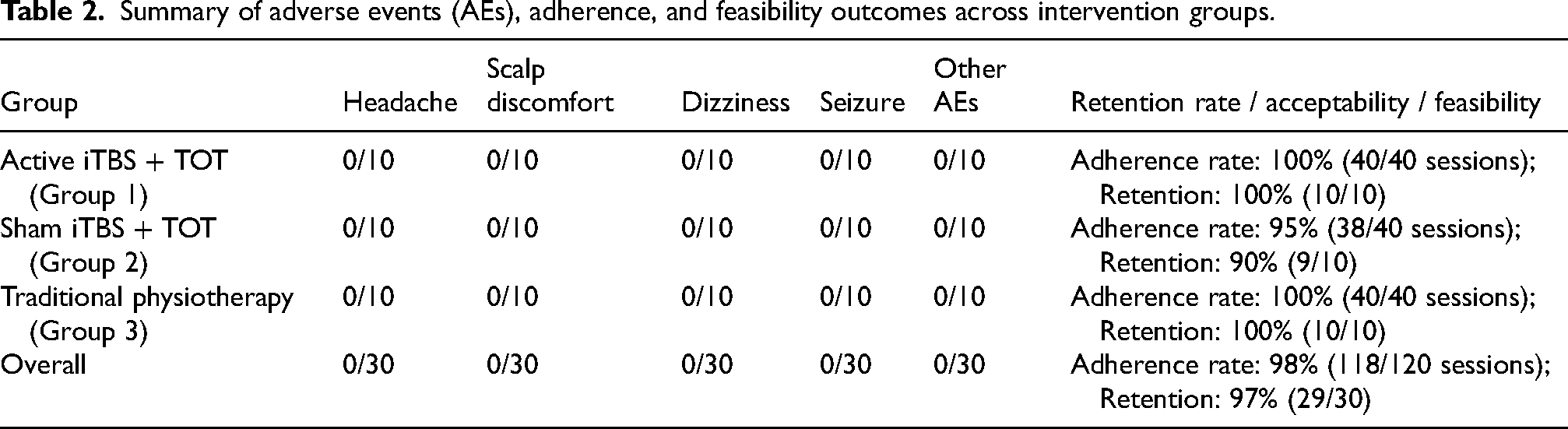
The tasks included: drinking from a glass, lifting a glass of water to a 90° angle with an extended elbow, transferring five small colored beads from a table into a box, wiping a table while keeping the elbow extended, grasping and releasing a 6 cm diameter tennis ball, and combing hair. Each 45-min session began with a 10-min warm-up, followed by 35 min of task practice, with a 2.5-min break every 15 min of continuous training. Before each session, tasks were demonstrated using the participants’ unaffected upper limb to ensure proper execution. 35
Physical therapists provided multimodal feedback, including verbal, visual, and proprioceptive cues, along with hands-on assistance to ensure accurate task execution. The training adhered to established rehabilitation principles, such as “use it to improve it,” “specificity,” “repetition,” “importance,” and “intensity". 18 Tools used in task-oriented training are shown in Figure 3.

Tools used for task-oriented training.
Traditional physiotherapy
Participants in Group 3 received traditional physiotherapy focused solely on the upper limb for 45 min each day. In the standard rehabilitation program, all participants followed a structured physical therapy regimen that reflected routine clinical practice within the hospital. This included a combination of passive and active range of motion exercises for all joints, weight-bearing activities, and supportive reaction training to improve postural control. Reaching tasks were used to enhance upper limb coordination and mobility, while grasping, holding, and releasing exercises aimed to strengthen fine motor skills. Additionally, upper limb activities of daily living (ADLs) were incorporated to promote functional independence. Therapists also integrated functional reaching, grasp-and-release exercises, and training in upper limb ADLs such as grooming, self-feeding, and dressing to support independence. Participants received daily physical therapy sessions over four weeks, ensuring a consistent and comprehensive rehabilitation approach. 36
While no neuromodulation or task-specific repletion protocols were used in this group, the therapeutic approach followed standard neurorehabilitation principles and was informed by elements of the Bobath concept, Rood techniques, and functional task-based training commonly applied in traditional stroke rehabilitation. 37 All sessions were supervised by a licensed physical therapist and delivered once daily for four weeks.
Outcome measures
Primary outcomes included feasibility and safety. Secondary outcomes included preliminary clinical measures to assess trends in motor and functional recovery. These comprised the Fugl-Meyer Assessment for Upper Extremity (FMA-UE), Modified Barthel Index (MBI), and NIH Stroke Scale (NIHSS), administered at baseline, week 2, and week 4. All assessments were conducted by a licensed occupational therapist blinded to group allocation.
Feasibility and safety
Feasibility was evaluated using predefined metrics to assess the practicality of conducting a larger-scale trial. Recruitment success was calculated as the proportion of eligible participants enrolled within the planned timeframe, with a predefined threshold of ≥70%. Of the 60 individuals assessed for eligibility, 22 did not meet the inclusion criteria and 8 declined participation, resulting in 30 enrolled participants (50% recruitment rate). Retention was defined as the percentage of randomized participants who completed the full intervention and all follow-up assessments without dropout, targeting ≥80%; this criterion was exceeded, with 29 of 30 participants (97%) completing the study. Assessment completion was defined as the proportion of scheduled evaluations (baseline, week 2, and any interim measures) fully administered and recorded per participant, with a goal of ≥90%, which was achieved for all retained participants (100%).
Adherence was quantified as the percentage of scheduled treatment sessions attended and completed, with a predefined threshold of ≥85% across groups. Overall adherence was high, with 98% of all sessions completed (Group 1: 100% [40/40 sessions]; Group 2: 95% [38/40 sessions]; Group 3: 100% [40/40 sessions]). At the participant level, 29 of 30 individuals (96.7%) completed the full intervention, with one discontinuation in Group 2 due to personal reasons.
Adverse events (AEs) were predefined as any undesirable experiences occurring during or after stimulation, including headache, scalp discomfort, dizziness, or seizure. Safety was systematically monitored throughout the study at each session through participant self-reports and non-leading therapist queries, following Good Clinical Practice (GCP) 38 and established safety guidelines for non-invasive brain stimulation. 39
Fugl-Meyer assessment- upper extremity (FMA-UE)
The FMA-UE is an impairment index designed to assess motor recovery of the UE after stroke. The UE section of the FMA consists of 33 items. Scores are summed with a maximum potential score of 66 points. 40 The FMA-UE has proven to exhibit strong test-retest reliability and reliable inter-rater and intra-rater assessments. There is substantial documentation supporting its content validity in both acute and subacute populations.41–44 Additionally, the minimal clinically important difference (MCID) for the FMA is approximately a 12.4-point improvement on average. 45 In our study, an increase in the FMA score indicates an improvement in patients’ motor function.
Modified Barthel Index (MBI)
The Barthel Index measures the ability to perform daily activities, with the highest possible score of 100. This score is based on 10 tasks, including personal hygiene, bathing, self-feeding, using the toilet, climbing stairs, dressing, managing bowel control, controlling bladder function, walking, and transferring between locations. A higher score indicates better performance in activities of daily living. The Barthel Index is recognized as a quick and dependable tool for assessing mobility and daily living activities, showing consistent accuracy regardless of the assessor's skill level. 46 Additionally, the MCID for the Modified Barthel Index is roughly a 1.85-point improvement on average. 47 In our research, an increase in the MBI score reflects an enhancement in patients’ daily living capabilities.
National Institutes of Health Stroke Scale (NIHSS)
The National Institutes of Health Stroke Scale (NIHSS) is a widely used and standardized tool for evaluating neurological deficits related to stroke. It offers a reliable, valid, and easily administered bedside assessment, making it essential for large multi-center clinical trials. The NIHSS measures various aspects, including the level of consciousness, language function, neglect, visual fields, eye movements, facial symmetry, motor strength, sensation, and coordination. This comprehensive evaluation provides a thorough understanding of neurological impairment.48,49 Each item is scored 0 to 2 or 0 to 3, with a total score ranging from 0 to 42; higher scores indicate more severe nerve damage. 50
Statistical methods
We performed data analysis using SPSS version 27.0 (IBM Corporation, Armonk, NY, USA). Categorical variables were displayed as frequencies and compared with chi-square tests. Normality of continuous data was evaluated using the Shapiro–Wilk test, along with skewness, kurtosis, Q–Q plots, and histograms. For outcomes that met parametric assumptions (NIHSS and MBI at 4 weeks), between-group comparisons were conducted using analysis of covariance (ANCOVA), adjusting for baseline scores and time since stroke onset to account for potential baseline differences in recovery potential. These results are reported as least-squares means (LSMEANS) with 95% confidence intervals (CIs) as partial η2 was calculated as a measure of effect size.
For outcomes violating normality assumptions (FMA scores), the Kruskal-Wallis test was used for between-group comparisons at 4 weeks. Post-hoc comparisons were conducted using Mann–Whitney U tests with Bonferroni correction for three pairwise tests (adjusted α = 0.017). Epsilon squared (ε2) and Cliff's delta (δ, with 95% CIs) were reported as effect sizes. To assess within-group changes across time points (Pre, Week 2, Week 4), the Friedman test was applied. Where significant, post-hoc Wilcoxon signed-rank tests with Bonferroni correction (α = 0.017) were used to examine specific time-point differences. 51 Effect sizes were expressed as rank-biserial correlations (rB). Statistical significance was set at p < 0.05.
Results
Characteristics at baseline
A total of 30 participants were enrolled, and 29 (97%) completed the 4-week intervention. Baseline demographic and clinical characteristics are presented in Table 1. The three groups were comparable in terms of age (p = 0.31), sex distribution (p = 0.75), FMA-UE (p = 0.61), MBI (p = 0.67), NIHSS scores (p = 0.36), and motor evoked potentials (MEPs; p = 0.90). Time since the stroke onset differed significantly between groups (p = 0.03), with Group 2 having the shortest duration (43 ± 29.56 days) compared to Group 1 (69 ± 46.12 days) and Group 3 (81 ± 39.65 days). Other stroke-related variables, including site of stimulation (p = 0.65), side of lesion (p = 0.88), and stroke type (ischemic vs. hemorrhagic), did not show statistically significant differences. Subcortical stroke was the most frequent lesion type in all groups. The distribution of vascular risk factors was also comparable across groups (p = 0.09), though four participants in Group 2 had no identified risk factors.
Baseline characteristics of participants.
Values are represented as mean and standard deviation (SD) for continous variables and number of participants for categorical variables. L/R (Left/Right),FMA-UE (Fugl-Meyer Assessment-Upper Extremity), MBI (Modified Barthel index), NIHSS (National Institutes of Health and Stroke Scale)
Feasibility and safety
All predefined feasibility criteria were successfully met. Recruitment, retention, assessment completion, and adherence rates exceeded the prespecified thresholds, indicating good feasibility of the trial procedures. Adherence across groups was high (overall 98%), with only one discontinuation due to personal reasons. No adverse events were reported during or after stimulation sessions (Table 2).
Summary of adverse events (AEs), adherence, and feasibility outcomes across intervention groups.
Adjusted group comparisons for clinical outcomes at week 4
At week 4, significant between-group differences were observed across all three outcome measures (Table 3).
Between-group comparison of FMA-UE, NIHSS, and MBI outcomes.
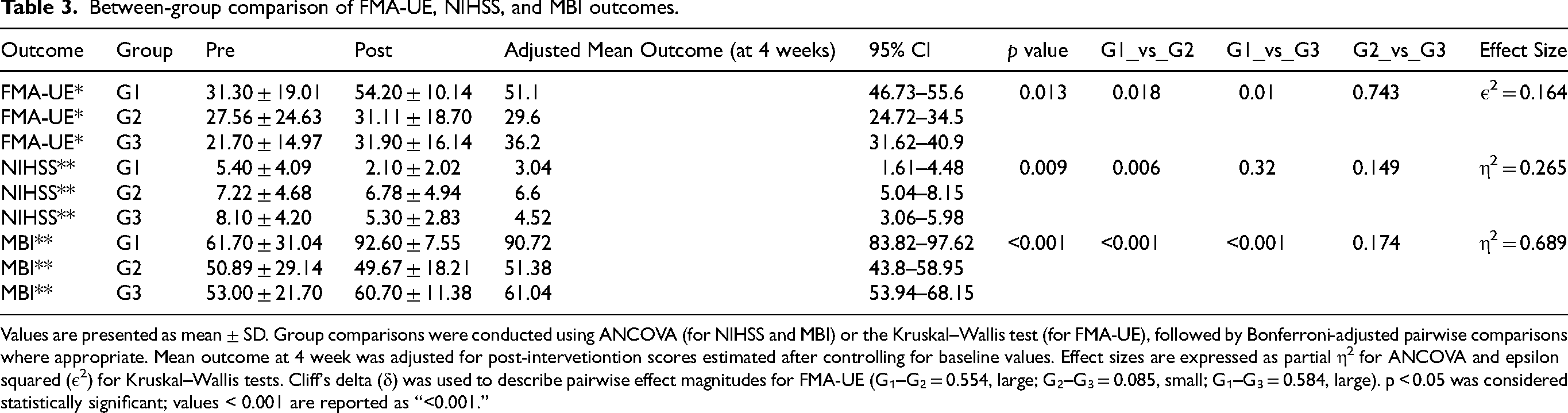
Values are presented as mean ± SD. Group comparisons were conducted using ANCOVA (for NIHSS and MBI) or the Kruskal–Wallis test (for FMA-UE), followed by Bonferroni-adjusted pairwise comparisons where appropriate. Mean outcome at 4 week was adjusted for post-intervetiontion scores estimated after controlling for baseline values. Effect sizes are expressed as partial η2 for ANCOVA and epsilon squared (ε2) for Kruskal–Wallis tests. Cliff's delta (δ) was used to describe pairwise effect magnitudes for FMA-UE (G₁–G₂ = 0.554, large; G₂–G₃ = 0.085, small; G₁–G₃ = 0.584, large). p < 0.05 was considered statistically significant; values < 0.001 are reported as “<0.001.”
For the Fugl-Meyer Assessment of the Upper Extremity (FMA-UE), the Kruskal–Wallis test revealed a statistically significant difference among the three groups (H = 8.68, p = 0.013). Post hoc comparisons using Mann–Whitney U tests with Bonferroni correction indicated that Group 1 (iTBS + TOT) demonstrated significantly higher FMA-UE scores (22.9 points), compared to both Group 2 (3.6 points, p = 0.016) and Group 3 (10.2 points, p = 0.009), while no significant difference was found between Groups 2 and 3 (p = 0.712). The magnitude of between-group differences, expressed as Cliff's delta (δ), indicated large effects favoring Group 1.
For the NIH Stroke Scale (NIHSS), analysis of covariance (ANCOVA) adjusted for baseline NIHSS and time since stroke onset revealed a significant group effect at week 4 (p = 0.009). Group 1 had a significantly lower adjusted mean NIHSS score (3.04; 95% CI: 1.61–4.48) compared to Group 2 (6.60; 95% CI: 5.04–8.15; p = 0.007). The difference between Group 1 and Group 3 (4.52; 95% CI: 3.06–5.98) was not statistically significant (p = 0.192), nor was the difference between Groups 2 and 3 (p = 0.459). The partial η2 effect size was 0.32, suggesting a large effect of treatment on NIHSS improvement.
Similarly, ANCOVA for the Modified Barthel Index (MBI), adjusted for baseline MBI and stroke duration, revealed a significant group effect (p < 0.001). Group 1 showed the highest adjusted mean MBI score (90.72; 95% CI: 83.82–97.62), which was significantly greater than both Group 2 (51.38; 95% CI: 43.80–58.95; p < 0.001) and Group 3 (61.04; 95% CI: 53.94–68.15; p < 0.001). The difference between Groups 2 and 3 was not statistically significant (p = 0.229). The corresponding partial η2 value of 0.41 indicated a large treatment effect on functional independence.
To account for the baseline difference in time since stroke onset, an additional sensitivity analysis was performed with stroke duration included as a covariate. The results remained consistent with the main findings, suggesting that the observed group differences were not substantially influenced by variation in stroke chronicity.
Within-group changes in the outcomes across different time points
All three groups demonstrated within-group improvements in FMA-UE scores over time (Table 4). In Group 1 (iTBS + TOT), the Friedman test revealed a significant overall change (p < 0.001). Post hoc comparisons showed significant improvement from baseline to week 4 (p < 0.001, r₍B₎ = 0.89) and from week 2 to week 4 (p = 0.018, r₍B₎ = 0.89, while the change from baseline to week 2 was not significant (p = 0.028, r₍B₎ = 0.84).
Within-group comparison of FMA-UE, NIHSS, and MBI across time points.
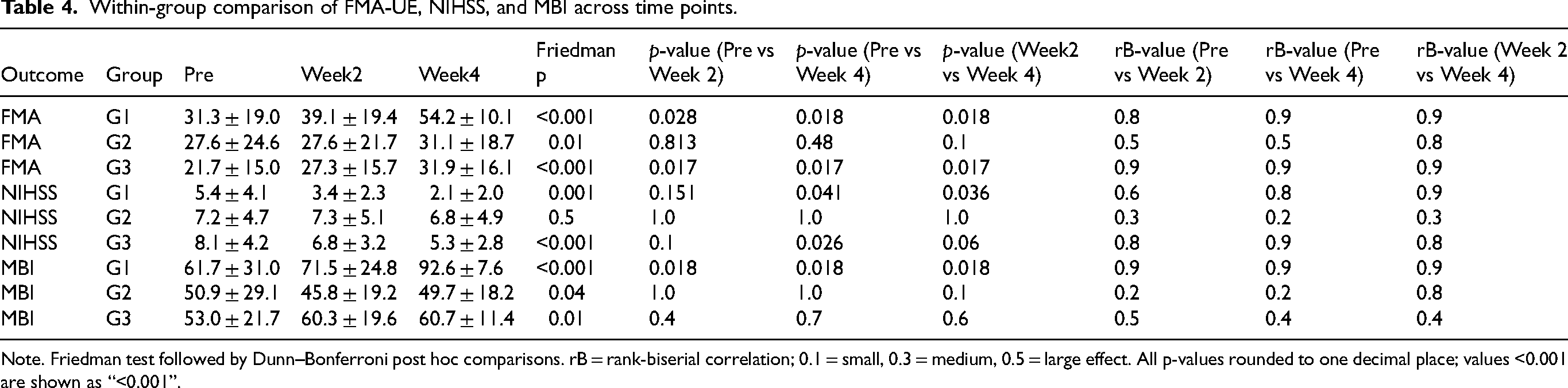
Note. Friedman test followed by Dunn–Bonferroni post hoc comparisons. rB = rank-biserial correlation; 0.1 = small, 0.3 = medium, 0.5 = large effect. All p-values rounded to one decimal place; values <0.001 are shown as “<0.001”.
Group 2 (sham iTBS + TOT) also showed a significant overall improvement (p = 0.010), with a modest increase from baseline to week 4 (p = 0.48, r₍B₎ = 0.54), while other time-point comparisons were not significant (p = 0.81 and p = 0.11). Group 3 (traditional physiotherapy) demonstrated a significant overall change (p < 0.001), but only the comparison from baseline to week 4 reached statistical significance (p = 0.017, r₍B₎ = 0.89). The changes from baseline to week 2 and week 2 to week 4 were not significant after adjustment (p = 0.076 for both).
For NIHSS scores, Group 1 exhibited a significant reduction over time (p = 0.001), with a significant decline from baseline to week 4 (p = 0.041, r₍B₎ = 0.85) and from week 2 to week 4 (p = 0.036, r₍B₎ = 0.86), whereas the change from baseline to week 2 was not significant (p = 0.151, r₍B₎ = 0.64). Group 2 showed no significant change across time points (Friedman p = 0.499; all pairwise p = 1.0, r₍ B ₎ = 0.24–0.31). In contrast, Group 3 showed a significant overall reduction (p < 0.001), driven by a significant change from baseline to week 4 (p = 0.026, r₍B₎ = 0.88)), while other comparisons were not significant (p = 0.10 and p = 0.06).
In the MBI, Group 1 showed a significant overall improvement over time (p < 0.001), with a statistically significant increase from baseline to week 2 (p = 0.018, r₍B₎ = 0.9) and from baseline to week 4 (p = 0.018, r₍B₎ = 0.9), as well as from week 2 to week 4 (p = 0.018, r₍B₎ = 0.9). Group 2 demonstrated a modest overall change (p = 0.044), but only the change from week 2 to week 4 approached significance (p = 0.1, r₍B₎ = 0.8); other pairwise comparisons were not significant (p = 1.0, r₍B₎ = 0.2). Group 3 showed a significant overall change (p = 0.018), with improvement from baseline to week 4 (p = 0.016); comparisons across other intervals were not statistically significant.
Discussion
This exploratory pilot randomized controlled trial primarily evaluated the safety, feasibility, and preliminary efficacy of combining intermittent theta-burst stimulation (iTBS) with task-oriented training (TOT) in individuals with subacute stroke. The intervention was well tolerated, with no adverse events reported. Of the 30 participants enrolled, 29 (97%) completed the 4-week intervention, demonstrating high retention, while adherence to scheduled sessions exceeded 98%, supporting the intervention's feasibility. Preliminary findings suggest that the combined intervention may contribute to improved upper limb motor recovery and functional independence; however, larger, adequately powered randomized trials are required to confirm efficacy.
Participants receiving active iTBS paired with TOT (Group 1) showed greater improvements across several domains. They exhibited notable gains in motor impairment as measured by the FMA-UE, attained near-functional independence in activities of daily living MBI (mean score 90.7), and demonstrated reduced neurological deficits as assessed by the NIHSS relative to the sham iTBS + TOT group (Group 2). Compared to traditional physiotherapy alone (Group 3), Group 1 also showed greater improvements in motor function and daily living activities, though the difference in NIHSS scores between Groups 1 (3.0) and 3 (4.5) did not reach statistical significance. Three key observations emerge from these findings. First, the 22.9-point increase in FMA-UE observed in Group 1 exceeded the established minimal clinically important difference (MCID) of 12.4 points, suggesting potential clinical relevance that merits confirmation in larger trials. Second, the superiority of Group 1 over both Groups 2 and 3 highlights the likely contribution of active neuromodulation, supported by the non-significant difference between Groups 2 and 3 in FMA-UE scores. Third, the substantial improvement in functional independence (MBI) underscores the practical significance of this combined intervention in enhancing patients’ quality of life.
The observed treatment effects in the iTBS + TOT group may reflect synergistic neuroplastic mechanisms. The proposed mechanism is that iTBS primes the ipsilesional motor cortex for subsequent motor learning by transiently increasing cortical excitability and rebalancing interhemispheric inhibition. 52 This induces a metaplastic state, lowering the threshold for synaptic modification. 53 The temporal coupling of iTBS with task-oriented training is critical, as it harnesses this period of heightened excitability to enhance activity-dependent plasticity. During this window, synchronous activation of motor circuits through targeted practice facilitates Hebbian strengthening of cortico-motor connections, mirroring the principles of paired associative stimulation.54,55 However, the absence of neurophysiological measures in this study precludes confirmation of these mechanisms.
Notably, our protocol specifically targeted the subacute phase (1–6 months post-stroke), a period characterized by heightened endogenous neuroplasticity.
56
This strategic timing contrasts with most prior iTBS studies conducted in chronic stroke populations,57,58 and may explain the accelerated recovery trajectory in Group 1. The shorter mean post-stroke duration in Group 2 (43 days vs. 69 days in Group 1) presents an intriguing observation; while this subgroup might theoretically possess greater spontaneous recovery potential, their FMA-UE improvements were modest and statistically indistinguishable from traditional physiotherapy in Group 3. Furthermore, within-group analyses revealed only minimal significant gains in group 2 beyond the baseline to week 4. Within-group analyses revealed minimal gains in Group 2 beyond baseline to week 4, suggesting that sham neuromodulation combined with TOT may not add meaningful benefit in the early subacute phase. Spontaneous neurological recovery is a common occurrence in this population and cannot be disregarded. In the absence of neurophysiological data, any interpretations regarding cortical mechanisms remain uncertain. The lack of significant difference between the sham iTBS + TOT and physiotherapy groups may be due to the absence of cortical priming with sham stimulation, leaving both groups to benefit mainly from repetitive motor practice rather than neuromodulation-induced plasticity. Additionally, potential placebo or expectancy effects should be considered when interpreting the results. Previous work has shown that sham non-invasive brain stimulation can induce measurable behavioral changes, likely due to participants’ expectations of benefit and enhanced clinical engagement during therapy59,60 While such factors may have partly contributed to improvements observed across groups, assessor blinding and the consistently greater gains in the active iTBS + TOT group suggest that these effects alone cannot account for the observed outcomes
Our results resonate with emerging evidence on neuromodulation-enhanced rehabilitation. Studies combining iTBS with functional electrical stimulation, 36 virtual reality-based cycling, 61 or using it as a priming tool before therapy. 62 A recent trial reported improved upper limb function in subacute stroke patients receiving iTBS combined with conventional therapy. 63 While the cited systematic review includes a limited number of studies, three of which focus on the subacute phase, most of the studies address spasticity rather than motor recovery. 64 Broader evidence supports early intervention during this neuroplastic window. These findings highlight the subacute phase as an opportunity for integrating neuromodulation with task-specific training; however, further targeted research is required to clarify the efficacy and optimal protocols of iTBS in this population.
The combined iTBS and TOT protocol demonstrated high feasibility and tolerability in this pilot study. Daily stimulation sessions required minimal time (≈3 min) and were seamlessly incorporated into standard rehabilitation without disrupting therapeutic schedules. Given the widespread availability of the required equipment, this approach holds significant translational potential for clinical implementation. Although the observed improvements in functional independence are encouraging, these findings must be interpreted cautiously due to the limited sample size. Nevertheless, the results provide preliminary evidence supporting the safety, feasibility, and potential efficacy of this combined neuromodulatory and task-oriented intervention, justifying further investigation in larger, controlled trials.
Several methodological constraints must be acknowledged. The single-center design, while advantageous for protocol standardization, may limit the generalizability across clinical settings. There was also a significant difference in time since stroke onset between groups, which could have influenced recovery potential; this was addressed in the analysis using ANCOVA, adjusting for baseline scores and stroke duration, with partial η2 reported as a measure of effect size. Patients in the traditional physiotherapy group (Group 3) were not blinded to the treatment allocation, which may have introduced expectation bias or placebo-related effects; however, outcome assessors remained blinded, reducing the risk of measurement bias. The short 4-week intervention period limits evaluation of long-term treatment effects, and the absence of neurophysiological assessments, such as longitudinal motor-evoked potentials, fMRI, or EEG, precluded direct examination of corticospinal excitability changes, constraining mechanistic interpretation. Additionally, MBI scores approached the upper limit in some participants, indicating near independence; potential ceiling effects may have limited the ability to detect further functional improvements. Although this pilot study primarily aimed to determine feasibility, future research should incorporate larger, multicenter samples, extended follow-up, and physiological measures to provide more insights into underlying mechanisms and the durability of treatment effects.
Conclusions
This pilot randomized controlled trial provides preliminary evidence that combining iTBS with TOT is a safe and feasible intervention for upper limb rehabilitation in individuals with subacute stroke. While the combined approach demonstrated potential to enhance motor recovery and improve functional independence, these findings should be interpreted as exploratory and preliminary, given the limited sample size. The results are insufficient to establish definitive efficacy supporting the need for larger, well-powered randomized controlled trials with extended follow-up and comprehensive neurophysiological evaluations to validate efficacy and clarify mechanisms of action.
Footnotes
Acknowledgments
The author gratefully acknowledges Aamir Raoof Memon for his assistance with the data analysis.
Ethical approval and informed consent
The study adhered to the ethical principles outlined in the Declaration of Helsinki and was approved by the Ethical Review Committee of the Second Affiliated Hospital of Chongqing Medical University, China (Approval No. 2024[57]).
Author contributions
Conceptualization: RF, YLH, AZ; Methodology: RF, YF, YZ; Formal analysis: RF; Project administration: YLH, BT, AZ; Writing – original draft: RF; Writing – review and editing: RF, BT Approval of final manuscript: all authors.
Funding
This work was supported by the Joint Funds for the innovation of science and Technology, Fujian province (2021Y9130), China Postdoctoral Science Foundation (2024M763909), the Special Funding for Postdoctoral Research Projects in Chongqing (2023CQBSHTB3155), and the Natural Science Foundation of Chongqing (CSTB2024NSCQ-MSX0197, CSTB2024TIAD-GPX0030).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data from this research are confidential, as participants signed an informed consent form ensuring the confidentiality of their information.