
Abstract
Background
Body awareness is an important protective factor that helps individuals cope with negative situations and learn from positive movement experiences. Therefore, tools that assess postural habits and awareness are of great importance.
Objective
This study aims to examine the validity and reliability of the Postural Habits and Awareness Scale (PHAS) in individuals with chronic low back pain.
Methods
The study was prospectively designed, and face-to-face assessments were performed. The PHAS, Fremantle Back Awareness Questionnaire (FBAQ), and Oswestry Disability Index (ODI) were used as assessment parameters. All assessments except the PHAS were conducted only once, while the PHAS was repeated 7–10 days after the initial assessment for retest analyses.
Results
Confirmatory factor analysis showed that the model had an acceptable fit with the data (CMIN/df = 1.46, RMSEA = 0.056, CFI = 0.92, GFI = 0.90). The scale's internal consistency was assessed using Cronbach's alpha, which was found to be α = 0.721 for the total scale. Test–retest reliability was evaluated using the Intraclass Correlation Coefficient (ICC) for the subdimensions and the total score. The ICC values were 0.878, 0.629, 0.739, and 0.844 for the subdimensions, respectively, and 0.877 for the total score.
Conclusion
In this study, the scale demonstrated satisfactory results in terms of both construct validity and reliability. The analysis findings indicate that the scale has a multidimensional structure consistent with the theoretical framework and shows an acceptable fit with the data. Overall, the scale is considered sufficiently valid and reliable, and it is an effective tool for assessing postural habits and awareness.
Introduction
Low back pain is a widespread clinical presentation that can occur at any time in a person's life, regardless of age, and limits activity. 1 Approximately 80% of adults have experienced back pain at least once in their lives. 2 In particular, prolonging pain into the chronic period causes changes in neuromuscular activity.3,4 As a result of changing neuromuscular activity, the mechanical behavior of the muscles is affected, resulting in postural changes, more pain, and avoidance behavior.5,6
Natural anatomical alignment minimizes the stress load on the joint surfaces.7,8 To achieve this, the individual must first have high body awareness. Body awareness is a concept that focuses on recognizing normal or abnormal processes in the body. 9 As body awareness develops in an individual, it is expected that there will be increased breath control, mental control, emotional control, coordination, improvement in muscle and joint movements, and improved response predictions due to changes in the body.10–12 Postural awareness is one of the components of body awareness, and it is defined as the conscious awareness of an individual's posture by processing the proprioceptive signals received from the periphery by the central nervous system.13,14 Awareness can be affected by many physical, physiological, emotional, and environmental factors as well as postural habits.15,16 Poor postural habits, in particular, cause body asymmetry. 17 Self-report tools are used in the literature to measure body awareness such as the Body Awareness Questionnaire, the Fremantle Waist Awareness Questionnaire, and the Frankfurt Body Concept Scale. 18 The only questionnaire that can evaluate postural awareness and habits is the postural habits and awareness scale (PHAS) developed by Bayar et al. 17 This scale was first developed in a study conducted on healthy individuals and was later used to evaluate different age, clinical condition and occupational groups.19–22
The reason for assessing PHAS in individuals with chronic low back pain is that postural habits and postural awareness are significantly impaired in this patient group due to neuromuscular changes.13,23 Individuals with chronic low back pain often experience motor control disorders, irregular muscle activation patterns, and changes in postural strategies due to prolonged pain. 24 This leads to the development of incorrect postural habits and decreased awareness. Therefore, it is important to assess these parameters not only in individuals with postural abnormalities but also in individuals with clinical conditions that affect postural awareness. Postural awareness and habits that are disrupted at the neuromuscular level in individuals with chronic low back pain need to be evaluated. 25 Because awareness of the body against negative situations and positive activity experiences learned can protect in many cases. For this reason, the importance of tools that assess awareness of body posture is high. This study examines the validity and reliability of the Postural Habits and Awareness Scale (PHAS), which assesses postural habits and awareness, in patients with chronic low back pain in Turkey.
Methods
Study design, ethics, and sample size
This methodological study was approved by the Karadeniz Technical University Health Sciences Scientific Research Ethics Committee (ID: 2024/110, Date: 06.09.2024). The convenience sampling method was used in the selection. Participants were selected from patients who applied to the hospital's physical medicine and rehabilitation clinic, where the study was conducted, and met the inclusion criteria. The required sample size for a 19-item instrument would be approximately 95–190 participants. 20 We enrolled 146 participants, which lies within this recommended range and is adequate for validity and reliability analyses.
Participants
All participants were informed verbally and in writing about the study. Then, written consent was obtained stating that they participated in the study voluntarily. Inclusion criteria for the study were: (1) being between the ages of 18 and 65, (2) being diagnosed with mechanical low back pain lasting longer than three months, and (3) having a pain intensity of at least 3/10 according to the Visual Analog Scale. Those with cardiac, respiratory, or kidney diseases, those with infectious diseases in the spinal cord, those who have undergone spinal surgery or a history of spinal fractures, those with rheumatological problems, those with neurological deficits, pregnant women, and those with oncological diseases were not included in the study.
Assessments
The same researcher performed all assessments in a private room using a face-to-face interview method. All assessments except PHAS were performed once. PHAS was repeated 7–10 days after the first assessment for re-test measurements. To avoid any treatment-related changes between measurements, the initial assessment was performed on the examination day, and the second assessment was performed on the first day the participants would start their physiotherapy sessions. Until the retest period, the patients were not given an exercise program, and medical treatments prescribed by the doctor were not interfered with.
Statistical analysis
The data were analyzed using IBM SPSS Statistics (version 22). Statistical significance was set at p < 0.05. The Kolmogorov–Smirnov test was employed to assess conformity to a normal distribution. The data for continuous variables were given as mean and standard deviation, while categorical variables were expressed as frequency and percentage. Cronbach's alpha coefficient was calculated to determine internal consistency. A coefficient greater than 0.70 indicates high internal consistency. 24 An intraclass correlation coefficient (ICC) calculation was made using test-retest results. If the ICC of <0.40 is poor reliability, 0.40–0.59 is moderate, 0.60–0.79 is acceptable, and ≥0.80 indicates outstanding. 25 The structural validity of the PHAS was assessed by confirmatory factor analysis (CFA). Model fit values were taken as basis. CFA was conducted with AMOS (version 22). We assessed model fit via χ2/df, GFI, AGFI, CFI, TFI, and RMSEA, and determined structural validity according to conventional threshold values. 26 Convergent validity was investigated by correlating PHAS scores with the FBAQ and by calculating AVE and CR based on CFA factor loadings. Acceptable convergence was defined a priori as AVE ≥ 0.50 and CR ≥ 0.70, consistent with conventional guidelines. 27 The absolute value of the correlation coefficient was interpreted as: 0.10–0.29 (small), 0.30–0.49 (moderate), and ≥0.50 (strong). 28 Moreover, the standard error of measurement (SEM) was calculated to determine the precision of individual scores and to quantify potential measurement error. SEM was derived using the formula SEM = SD × √(1 − r), where SD represents the standard deviation of the baseline scores and r denotes the intraclass correlation coefficient. To identify the smallest detectable change that exceeds measurement error, the minimum detectable change at the 95% confidence level (MDC95) was computed using the formula MDC95 = SEM × 1.96 × √2. 29
Results
Participant characteristics
A total of 146 participants were included in the study (Figure 1). The mean age was 44.54 ± 12.49 years, and the mean BMI was 26.70 ± 3.85 kg/m2. The average pain intensity during the past week was 5.31 ± 2.40 on the VAS, and the mean disease duration was 15.41 ± 17.30 months. Of all participants, 71.2% were female and 28.8% were male. According to the Oswestry Disability Index, 21.9% of participants had minimal disability, 57.5% had moderate disability, and 20.6% had severe disability (Table 1).
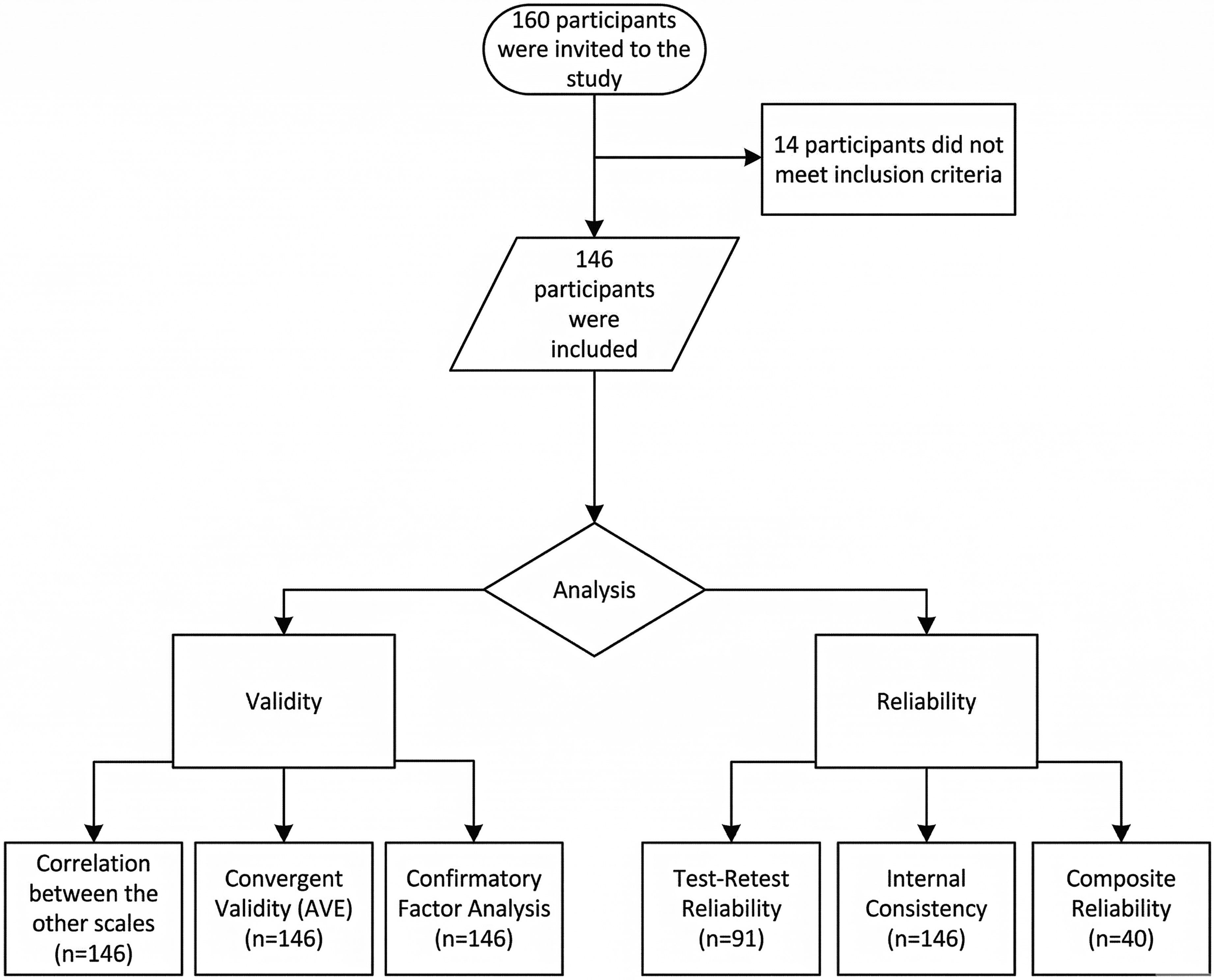
Flow chart of participants.
Descriptive statistics (n = 146).
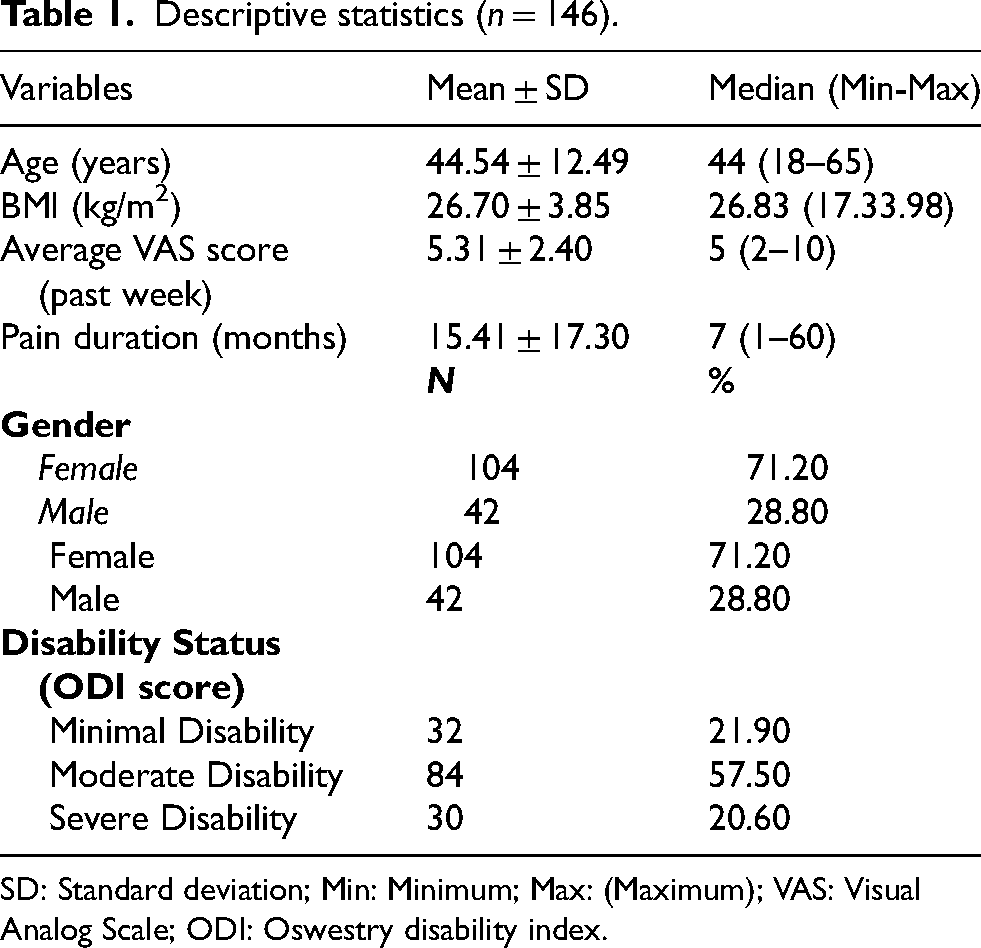
SD: Standard deviation; Min: Minimum; Max: (Maximum); VAS: Visual Analog Scale; ODI: Oswestry disability index.
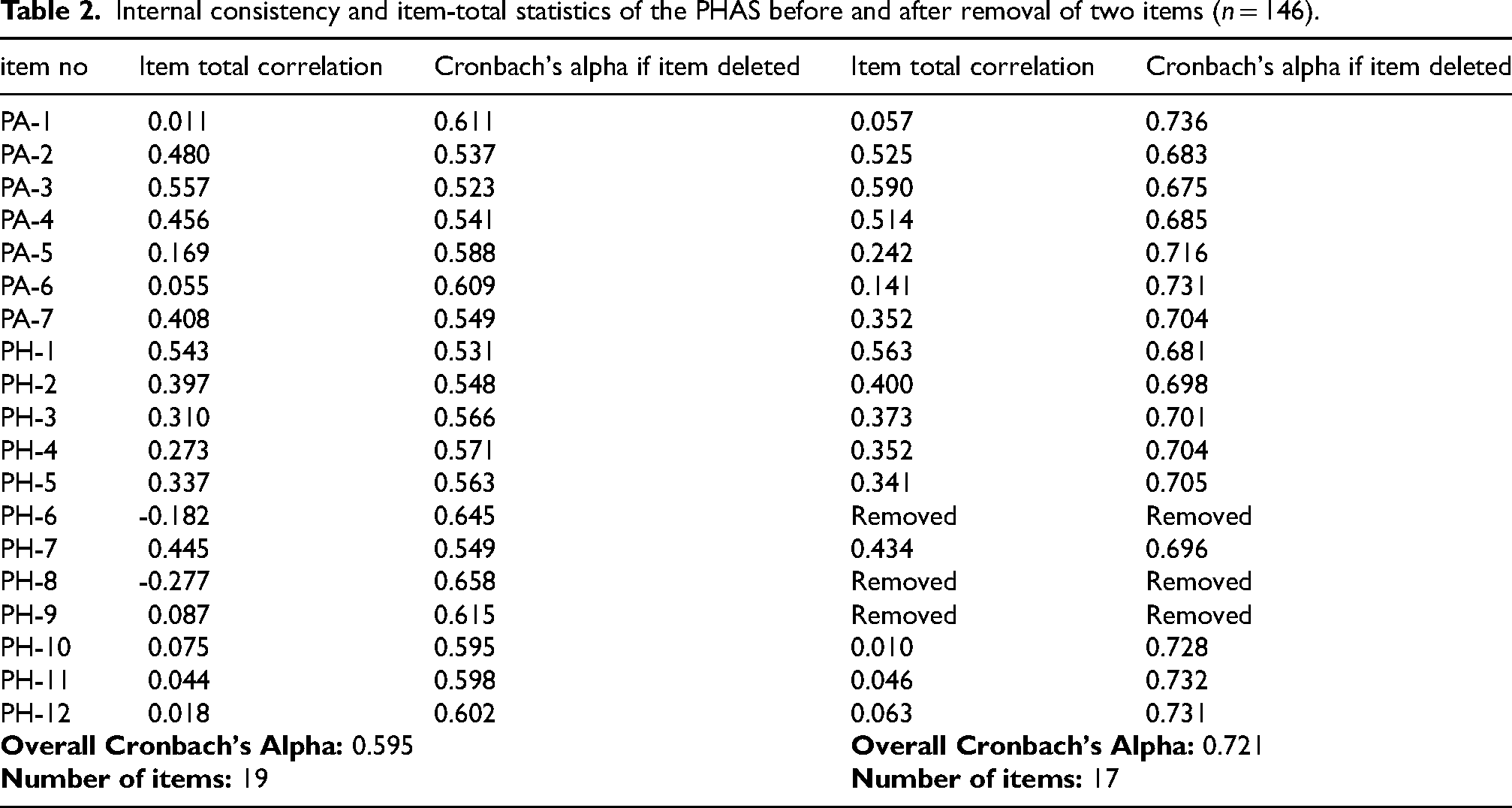
Internal consistency and item-total statistics of the PHAS before and after removal of two items (n = 146).
Test-Retest reliability.
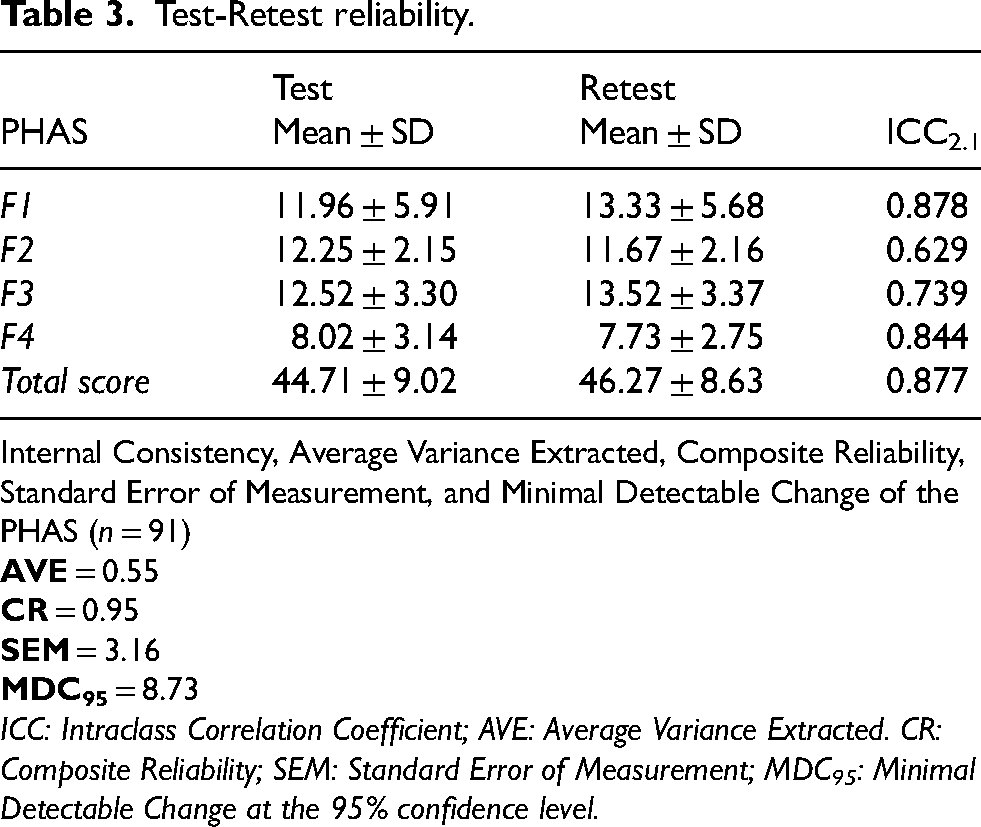
Internal Consistency, Average Variance Extracted, Composite Reliability, Standard Error of Measurement, and Minimal Detectable Change of the PHAS (n = 91)
ICC: Intraclass Correlation Coefficient; AVE: Average Variance Extracted. CR: Composite Reliability; SEM: Standard Error of Measurement; MDC95: Minimal Detectable Change at the 95% confidence level.
Reliability
Validity
Construct validity
Construct validity of the PHAS was examined CFA. The results indicated an acceptable model fit to the data, with the following fit indices: CMIN/DF = 1.46, GFI = 0.90, AGFI = 0.85, TLI = 0.90, CFI = 0.92, and RMSEA = 0.056. These values demonstrate that the hypothesized factor structure adequately represents the observed data, supporting the construct validity of the scale. The path diagram of the PHAS is shown in Figure 2.
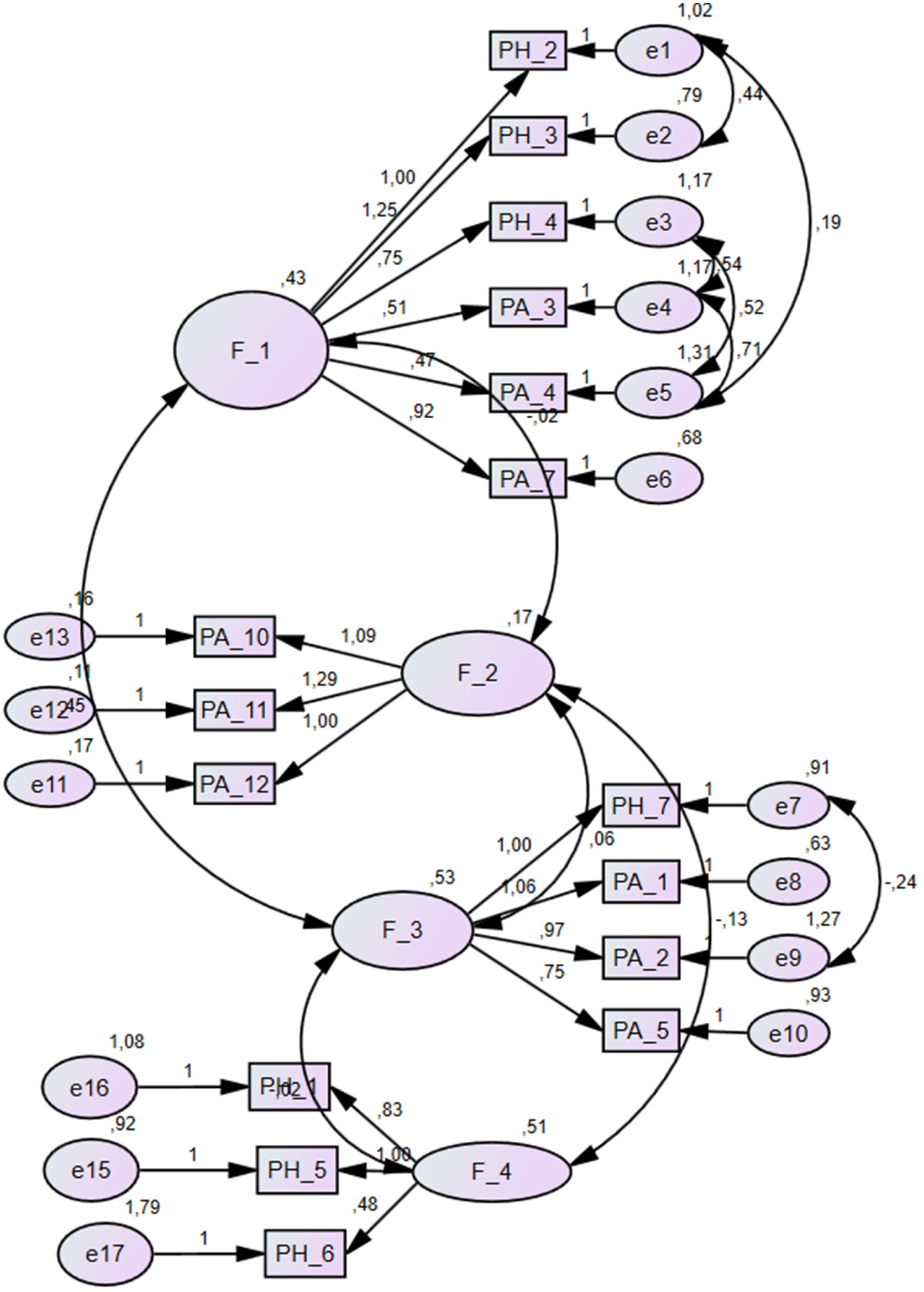
Path diagram of the PHAS.
Convergent validity
Convergent validity of the PHAS was evaluated through correlation analyses with the Fremantle Back Awareness Questionnaire (FBAQ) across different disability levels determined by the Oswestry Disability Index (ODI) and in the total sample (Table 4). In the overall sample, a significant negative correlation was observed between PHAS and FBAQ total scores (r = −0.300, p = 0.002), indicating that lower postural and functional awareness was associated with poorer back awareness, as theoretically expected.
Correlation between PHAS total score and FBAQ total score by ODI-based disability groups and the total sample
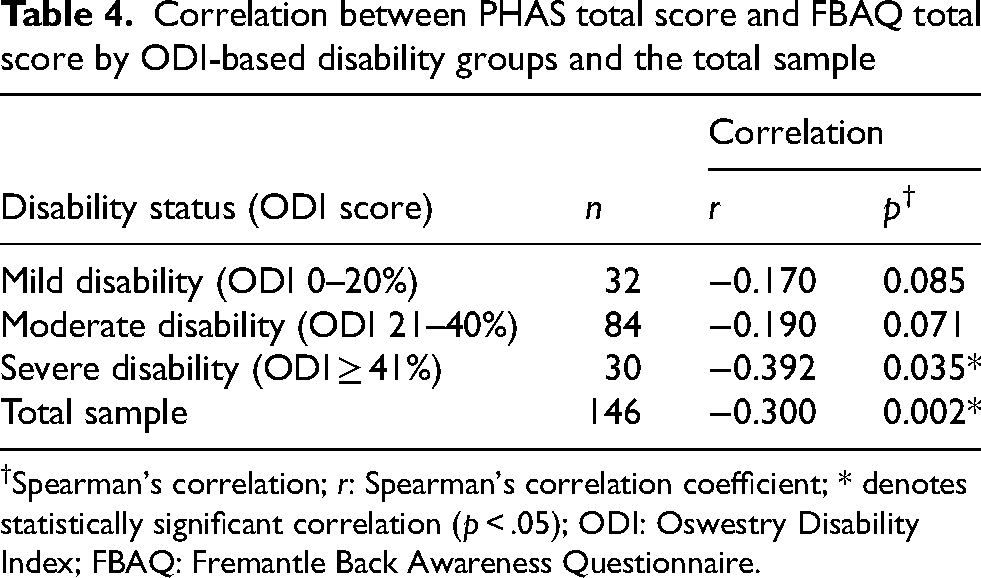
Spearman's correlation; r: Spearman's correlation coefficient; * denotes statistically significant correlation (p < .05); ODI: Oswestry Disability Index; FBAQ: Fremantle Back Awareness Questionnaire.
When examined by disability subgroups, the correlation was strongest and statistically significant in participants with severe disability (r = −0.392, p = 0.035), while no significant correlations were found in the mild (r = −0.170, p = 0.085) or moderate (r = −0.190, p = 0.071) disability groups. The stronger association in the severe disability group suggests that individuals with greater functional limitations tend to exhibit both reduced postural awareness and disturbed back perception.
These findings support the convergent validity of the PHAS, demonstrating its theoretical consistency with another measure assessing body and back awareness (FBAQ).
Discussion
This study investigated the psychometric properties of the Postural Habits and Awareness Scale (PHAS) in individuals with chronic low back pain (CLBP). Although the PHAS was originally developed and validated by Bayar et al. 17 for use in healthy adults, its applicability to populations with musculoskeletal disorders had not yet been established. The present findings demonstrated that the Turkish PHAS is a valid and reliable tool for assessing postural habits and awareness in individuals with CLBP.
In the original study, the PHAS showed acceptable internal consistency, with Cronbach's alpha coefficients between 0.619 and 0.832 for the four subscales and 0.73 for the total 19-item scale. 17 In the current study, internal consistency for the 16-item version was acceptable (α = 0.721) after the removal of three items that demonstrated low item–total correlations. After the removal of three items with low item–total correlations, the internal consistency of the PHAS improved to an acceptable level. Similar methodological refinements are common when scales are adapted or validated in clinical populations.30,31 In individuals with chronic low back pain, factors such as pain intensity, fear of movement, and altered proprioceptive processing can influence how respondents interpret posture-related statements, potentially affecting item correlations and response patterns. Previous studies have demonstrated that chronic low back pain is accompanied by impaired proprioceptive accuracy, disrupted body schema, and movement-related fear, all of which can alter body perception and motor control.32,33 Therefore, the refinement performed in this study may reflect not measurement error, but the necessary adaptation of the scale to the perceptual and behavioral characteristics of individuals with chronic low back pain.
Test–retest reliability analyses also revealed moderate to excellent stability (ICC = 0.629–0.878), supporting the reproducibility of the PHAS in this sample. These results are consistent with the original study, in which test–retest reliability was high (r = 0.905). 17 The current SEM and MDC95 values indicated that a change exceeding 8.73 points represents a real and clinically meaningful difference, confirming the instrument's precision for monitoring postural awareness changes over time.
The confirmatory factor analysis revealed a good model fit (CFI = 0.92, RMSEA = 0.056, χ2/df = 1.46), supporting the four-factor structure proposed by Bayar et al. 17 These findings demonstrate that the underlying construct of postural habits and awareness remains stable when applied to individuals with CLBP. Chronic pain is known to alter postural control, proprioception, and body schema representation, leading to maladaptive postural strategies.32–34 The acceptable model fit observed here suggests that the PHAS can adequately capture these dimensions even in the presence of such clinical changes.
A significant negative correlation between PHAS and the Fremantle Back Awareness Questionnaire (FBAQ) total scores (r = −0.300, p = 0.002) confirmed the theoretical relationship between postural and back awareness. Both instruments assess perceptual and cognitive aspects of body representation, and their inverse relationship reflects that decreased postural awareness is associated with impaired back awareness. This significant correlation observed among participants with severe disability supports the view that as functional limitation increases, both postural awareness and body perception deteriorate. This aligns with previous research reporting disrupted body schema and decreased proprioceptive acuity in chronic pain conditions.32,33,35 Evidence suggests that body perception distortions become more pronounced as clinical severity increases in individuals with chronic low back pain (CLBP).32,33 In the original psychometric work on lumbar-specific self-perception, FreBAQ scores in patients with CLBP were associated with both pain intensity and disability level. 33 Moreover, studies on postural control have shown that CLBP is accompanied by greater postural sway during quiet standing, with larger effects when pain intensity is higher and when sensory conditions are challenged (e.g., visual deprivation), which is consistent with reduced proprioceptive acuity and protective movement strategies.34,35 Accordingly, in our sample, the PHAS–FBAQ relationship may have been attenuated in the mild and moderate disability groups due to less pronounced (or more heterogeneous) perceptual distortions and possible range restriction of questionnaire scores. In contrast, among severely disabled patients, reduced postural awareness/habits (PHAS) and impaired lumbar perception (FBAQ) may co-occur more consistently, resulting in a stronger correlation.
The present findings extend the utility of the PHAS beyond healthy populations to individuals with chronic musculoskeletal pain. The ability to quantify postural awareness and habits provides clinicians with valuable information to identify maladaptive postural behaviors contributing to pain persistence. Interventions focusing on postural retraining, sensorimotor re-education, or mindful movement could benefit from using the PHAS to evaluate changes in postural awareness as part of rehabilitation outcomes. Moreover, the PHAS complements other self-report measures such as the FBAQ and the Oswestry Disability Index, enabling a more comprehensive assessment of physical and perceptual aspects of chronic low back pain.
This study has several limitations. The sample included only individuals with chronic low back pain, which may limit generalizability to other musculoskeletal or neurological conditions. In addition, responsiveness to treatment and sensitivity to clinical change were not evaluated. Moreover, although three items (PH-6, PH-8, and PH-9) were removed due to low/negative corrected item–total correlations during internal consistency analysis, item deletion may have implications for content coverage; however, a formal post-deletion content validity reassessment (e.g., expert panel review) was not conducted. Also, it was not recorded whether the patients used medication prescribed by the doctor until the retest period. Future research should investigate the scale's longitudinal responsiveness, compare PHAS scores across different diagnostic groups, and explore its relationship with objective postural control and proprioceptive measures.
Conclusion
In conclusion, the Postural Habits and Awareness Scale, originally developed for healthy individuals, demonstrated acceptable reliability and validity in patients with chronic low back pain. The PHAS is therefore a clinically applicable, self-reported tool for evaluating postural habits and awareness in this population and may assist clinicians and researchers in developing targeted interventions aimed at improving postural control and body awareness.
Footnotes
Acknowledgements
Not applicable.
Ethical approval and informed consent statement
The study was approved by the Karadeniz Technical University Health Sciences Scientific Research Ethics Committee (ID: 2024/110, Date: 06.09.2024). Also, all patients were informed verbally and in writing about the study. Written consent was obtained for participation in the study.
Author contributions
Design: E.Ş., A.T
Data collection: E.Ş., E.S.B
Data analysis and interpretation: E.Ş., E.M
Drafting the Article: E.Ş., E.S.B., E.M., A.T.
Critical revision of the article: E.Ş., E.S.B., E.M., A.T.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the results of our study are available from the corresponding author upon reasonable request. The data are not publicly available due to ethical or privacy restrictions.