
Abstract
Background
Chronic neck pain is a prevalent source of disability worldwide, and existing reviews report limited certainty due to heterogeneous methodologies and outdated trials.
Objective
To update and strengthen the evidence on the effectiveness and safety of cupping therapy for chronic neck pain by incorporating recent high-quality randomized controlled trials (RCTs).
Methods
In accordance with PRISMA 2020 and PROSPERO registration (CRD42025633104), major databases were searched through January 2025 for RCTs comparing various cupping modalities to control interventions in adults with chronic neck pain (≥3 months). Primary outcomes were pain intensity (Visual Analogue Scale, VAS/ Numeric Rating Scale, NRS) and functional disability (NDI); secondary outcomes included quality of life, range of motion, and adverse events.
Results
Nine RCTs involving 401 participants met inclusion criteria. Meta-analysis revealed that cupping significantly reduced pain intensity (Cohen's d = 1.17; 95% CI 0.26–2.09; p = 0.002) and produced consistent functional improvements (Cohen's d = 0.77; 95% CI 0.63–0.91; p < 0.001; I2 = 0%). Secondary outcomes favored cupping, with enhanced quality of life and range of motion. No serious adverse events were reported.
Conclusion
Cupping therapy provides consistent, clinically meaningful improvements in functional disability and significant pain relief for adults with chronic neck pain, within an overall evidence base that is stronger for function than for pain and is tempered by methodological limitations in several included trials. This updated synthesis elevates the evidence base, supporting cupping as a function-enhancing adjunct in multidisciplinary management and guiding its integration into clinical practice.
Introduction
Chronic neck pain ranks among the most prevalent causes of disability globally. According to the 2021 Global Burden of Disease report, approximately 203 million individuals were affected in 2020, and the number is expected to reach about 269 million by 2050, largely as a result of population expansion and increased life expectancy. 1 The global age-standardized rate of years lived with disability is 244 per 100,000, with prevalence notably higher among females than males. 2 This represents a substantial and growing global health burden, underscoring the urgent need for effective and safe treatments.3,4
Conservative management strategies, while widely recommended, often provide only modest and temporary relief. 5 Long-term pharmacological therapies such as non-steroidal anti-inflammatory drugs (NSAIDs) and opioids are associated with significant risks, including gastrointestinal complications, cardiovascular events, and dependence.6,7 These limitations highlight the importance of complementary and non-pharmacological therapies.8,9
Cupping therapy, a suction-based intervention rooted in traditional medicine, has gained interest as an adjunctive treatment for musculoskeletal pain. 1 Proposed neurophysiological mechanisms include enhanced local microcirculation, as demonstrated by increases in skin blood flow and temperature after cupping, modulation of inflammatory and oxidative stress pathways, and nociceptive modulation via segmental and descending inhibitory control.10,11 Experimental and clinical studies have reported increased muscle oxygenation and skin blood flow following cupping, as well as changes in inflammatory cytokines and activation of diffuse noxious inhibitory control, which together may contribute to reduced pain and improved function. 12 Its safety profile is generally favorable, with mild adverse effects such as bruising and transient discomfort. 13
Previous systematic reviews and meta-analyses (2018–2021) found short-term benefits of cupping on pain and function but graded the certainty of evidence as low-to-moderate due to small sample sizes, heterogeneity, and risk of bias. 14 Since 2018, several additional randomized controlled trials with improved methodological features and more detailed reporting have been published, but their findings have not yet been integrated into a comprehensive quantitative synthesis focused specifically on chronic neck pain. This gap limits clinicians’ ability to appraise the current totality of evidence and to understand how newer trials affect estimates of benefit, heterogeneity, and certainty of evidence.
This systematic review and meta-analysis, prospectively registered in PROSPERO (ID: CRD42025633104), aims to synthesize and quantitatively pool randomized controlled trial evidence on the effectiveness and safety of cupping therapy for chronic neck pain, with a primary focus on pain intensity and functional disability outcomes. In addition, we aim to appraise the certainty of the evidence using GRADE and the risk of bias using RoB 2.0. A meta-analysis is warranted at this stage because several randomized trials have been published since earlier reviews, allowing more precise pooled estimates, exploration of heterogeneity, and an updated assessment of the clinical relevance and robustness of cupping therapy as an adjunct in chronic neck pain management
Methods
Protocol and registration
This systematic review was registered prospectively in PROSPERO:CRD42025633104. The review followed PRISMA 2020 guidelines. 15 The full PRISMA checklist is provided in Appendix 1.
This systematic review initially considered a broad spectrum of study designs, including randomized controlled trials (RCTs), quasi-experimental investigations, cohort studies, and case–control studies, to maximize the comprehensiveness of our search. Following the application of our predefined eligibility criteria, only RCTs were retained for both qualitative and quantitative synthesis. The review focused exclusively on adult participants aged 18 years or older who had experienced chronic neck pain for at least three months; trials enrolling individuals with neck pain attributable to malignancy, systemic disease, infection, or acute trauma were excluded. Interventions of interest comprised various forms of cupping therapy, namely wet, dry, moving, fire, and pneumatic techniques—either as standalone treatments or as add-on therapies (i.e., cupping plus control versus control alone). Comparator groups included sham or placebo cupping, no treatment, usual care, physiotherapy, exercise regimens, transcutaneous electrical nerve stimulation (TENS), and other conservative modalities. The primary outcomes assessed were pain intensity, measured by the Visual Analog Scale or Numeric Rating Scale, and functional disability. Secondary outcomes encompassed pain experienced during movement, quality of life as captured by SF-36, SF-12, or EQ-5D instruments, pressure pain thresholds, range of motion, and the occurrence of adverse events. Our literature search was confined to studies published within five years prior to January 2025, with no language restrictions applied during screening; however, only full-text articles available in English were ultimately included. This review addressed the following research question: In adults with chronic neck pain (Population), does cupping therapy delivered as a standalone or adjunctive intervention (Intervention), compared with sham/placebo cupping, no treatment, usual care, or other conservative interventions (Comparison), improve pain intensity, functional disability, and related secondary outcomes (Outcome)?
Search strategy
A comprehensive literature search was conducted in the following databases up to January 2025: PubMed, Scopus, Web of Science, Embase, PEDro, CINAHL, EBSCOhost, Google Scholar, and OSF. The search strategy combined keywords and MeSH terms related to chronic neck pain (e.g., “cervical pain”) and cupping therapy (e.g., “wet cupping,” “dry cupping”). 16 The full, detailed search strategy is provided in Appendix 2.
Study selection
Three independent reviewers (R.F.E, N.A.E, O.MAE) screened titles and abstracts using Rayyan AI. 17 Full texts of potentially eligible studies were then assessed against the inclusion and exclusion criteria. All screening steps were performed independently by at least two reviewers; disagreements were resolved through discussion and, when necessary, consultation with a third reviewer.
Data extraction
Two reviewers independently extracted data using a piloted standardized form. Extracted items included study design, country, sample size, participant characteristics, intervention details (type of cupping, dose, frequency, duration), comparator interventions, outcome measures, follow-up times, and numerical results for all relevant outcomes. Any discrepancies in extracted data were resolved by consensus or by involving a third reviewer.
Risk of bias
The Cochrane Risk of Bias 2.0 (RoB 2) tool was utilized to evaluate the methodological quality of the included randomized controlled trials across five domains: (1) bias arising from the randomization process, (2) bias due to deviations from intended interventions, (3) bias due to missing outcome data, (4) bias in measurement of the outcome, and (5) bias in selection of the reported result. 18 For each domain, signalling questions were answered according to the RoB 2 guidance, and domain-level judgments were combined to yield an overall risk of bias classification (low risk of bias, some concerns, or high risk of bias). Two reviewers independently assessed risk of bias for each study, with disagreements resolved through discussion or, when needed, adjudication by a third reviewer. No assumptions were made beyond the information provided in the published reports.
Certainty of evidence (GRADE)
The certainty of evidence for the main outcomes (pain intensity and functional disability) was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach. For each outcome, we initially considered randomized controlled trial evidence as high certainty and then downgraded by one or two levels for concerns related to: (1) risk of bias (e.g., lack of blinding, incomplete outcome data), (2) inconsistency (unexplained statistical heterogeneity), (3) indirectness (differences in populations, interventions, or outcomes relative to the review question), (4) imprecision (wide confidence intervals, small total sample size, or few events), and (5) publication bias (as suggested by funnel plot asymmetry and small-study effects). Upgrading was not applicable because all included studies were randomized trials. Final ratings (high, moderate, low, or very low certainty) were determined by consensus among two reviewers, with disagreements resolved by discussion.
Data synthesis and analysis
Standardized mean differences (Cohen's d) with 95% CI were calculated. Heterogeneity were assessed by Q and I2. Fixed-effect model for I2 ≤ 50%, random-effects otherwise. 19 Meta-analysis was conducted with Meta-Essentials. Publication bias was assessed visually using funnel plots and statistically using Egger's and Begg's tests.20,21 The trim-and-fill method was applied to evaluate the potential influence of unpublished studies. Sources of heterogeneity were quantified using the I2 statistic and prediction intervals. 22 No subgroup or sensitivity analyses were prespecified.
Results
Study selection
A total of 1182 records were identified. After removal of duplicates and screening, 19 full-text articles were assessed for eligibility. Finally, 9 RCTs (401 participants) were included for qualitative and quantitative synthesis (PRISMA flowchart: Figure 1)
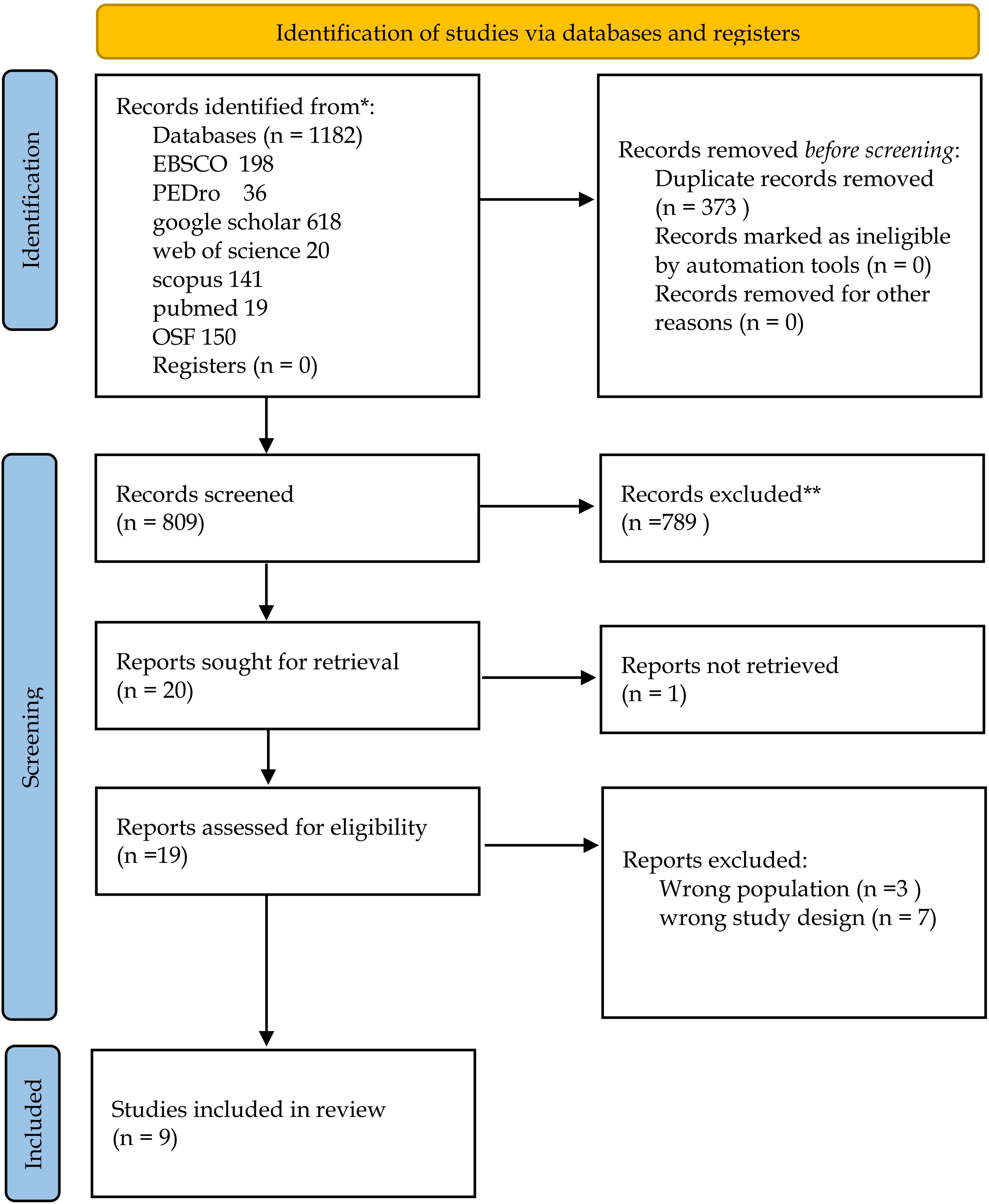
PRISMA 2020 flow diagram illustrating the identification, screening, eligibility, and inclusion of studies in the systematic review and meta-analysis.
Characteristics of included studies
Characteristics of the randomized controlled trials included in the systematic review and meta-analysis.
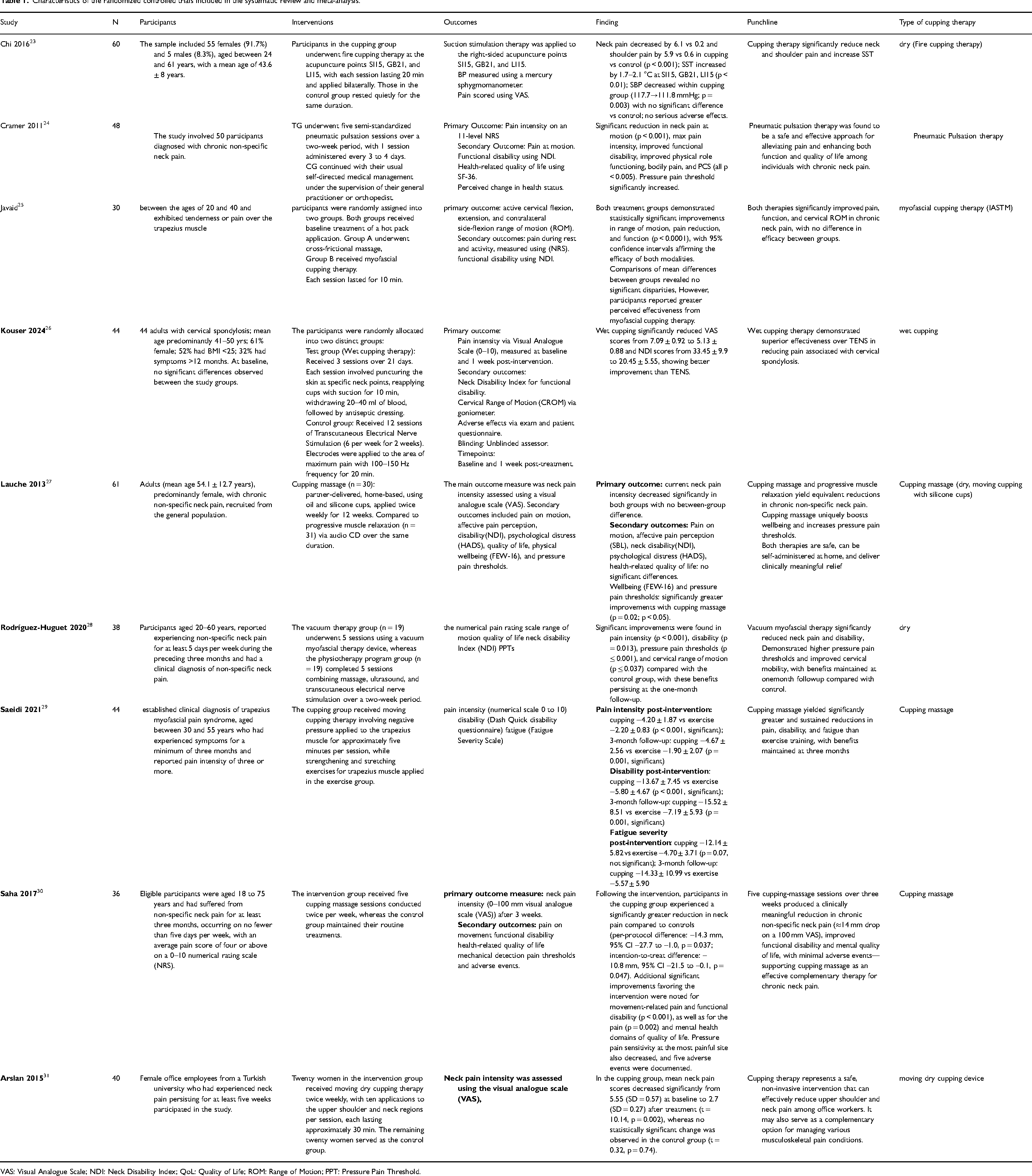
VAS: Visual Analogue Scale; NDI: Neck Disability Index; QoL: Quality of Life; ROM: Range of Motion; PPT: Pressure Pain Threshold.
Risk of bias assessment using ROB 2 tool
As illustrated in Figures 2, most studies demonstrated a low risk of bias in the randomization process (D1), with a few showing some concerns due to insufficient reporting of allocation procedures. Bias due to deviations from intended interventions (D2) and missing outcome data (D3) was generally low. The measurement of outcomes (D4) showed the highest proportion of high risk, mainly because blinding of participants and practitioners was not feasible. Some concerns were also noted in the selection of reported results (D5). In summary, seven studies were identified as having a high overall risk of bias, whereas two were judged to raise some concerns.
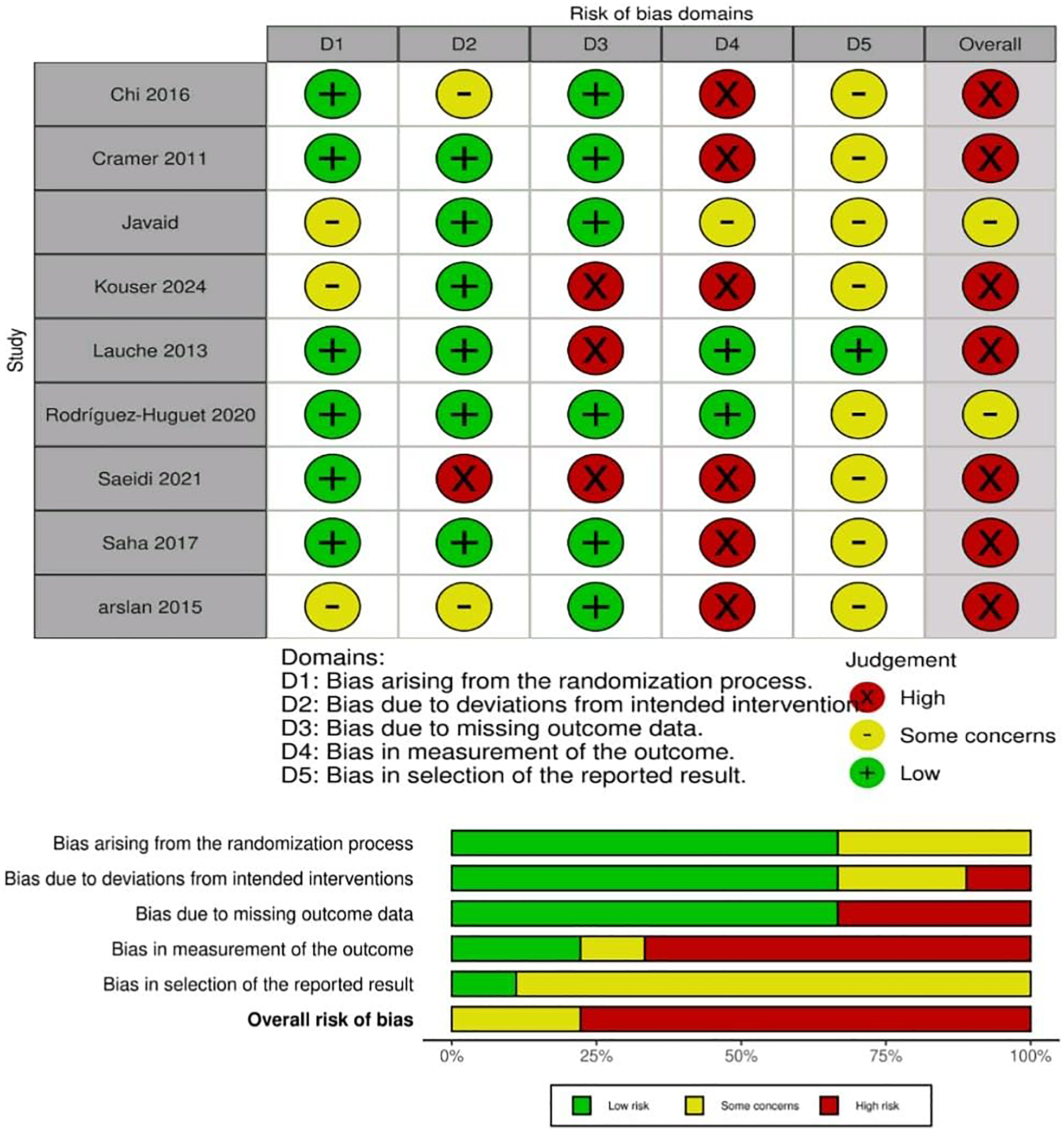
Summary of risk of bias assessment using ROB 2 tool. Green: low risk; yellow: some concerns; red: high risk.
Meta-analysis outcomes
Pain at rest
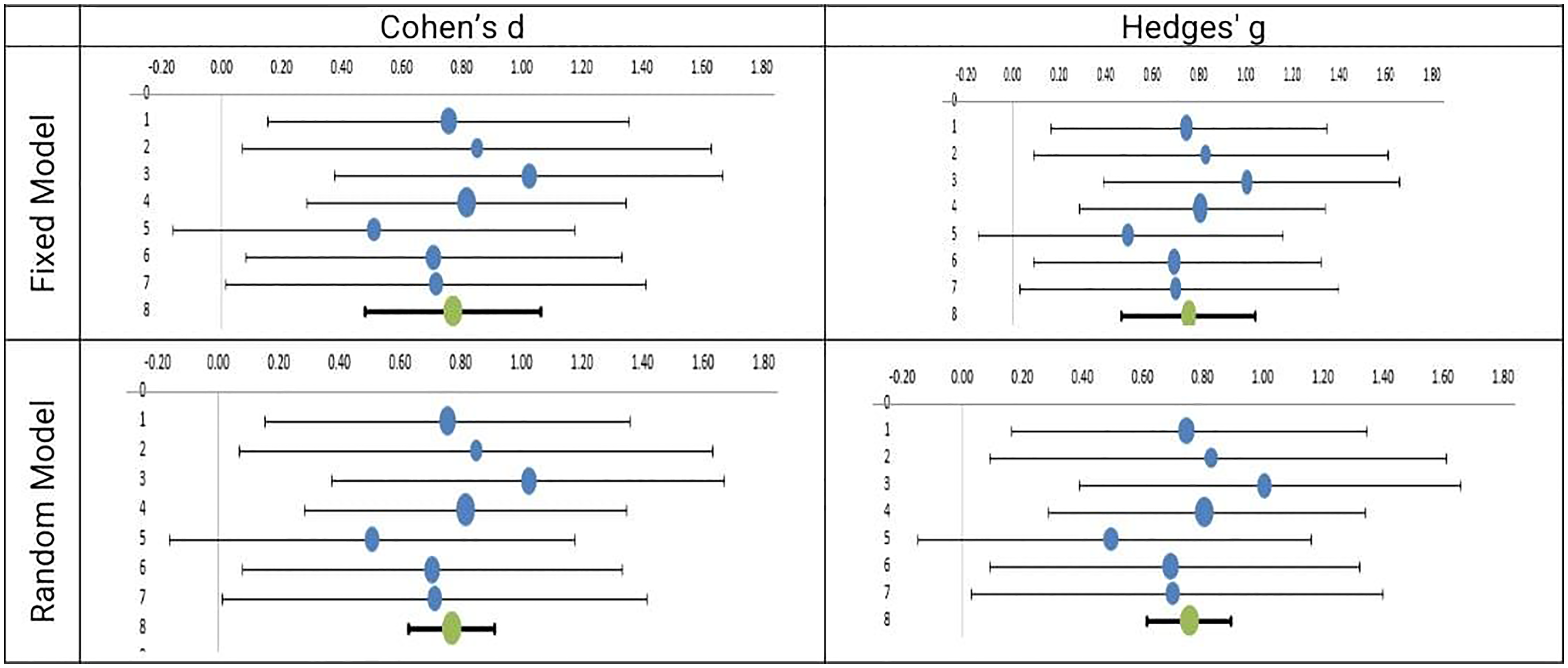
Nine RCTs with 401 participants were included in this analysis. Heterogeneity was high (I2 = 88.1%). Study-level effects ranged from very large (Chi 2016, d = 3.69) to small (Lauche 2013, d = 0.20). All studies favored cupping therapy over control. (See Table 2 and Figure 3 forest plot.)
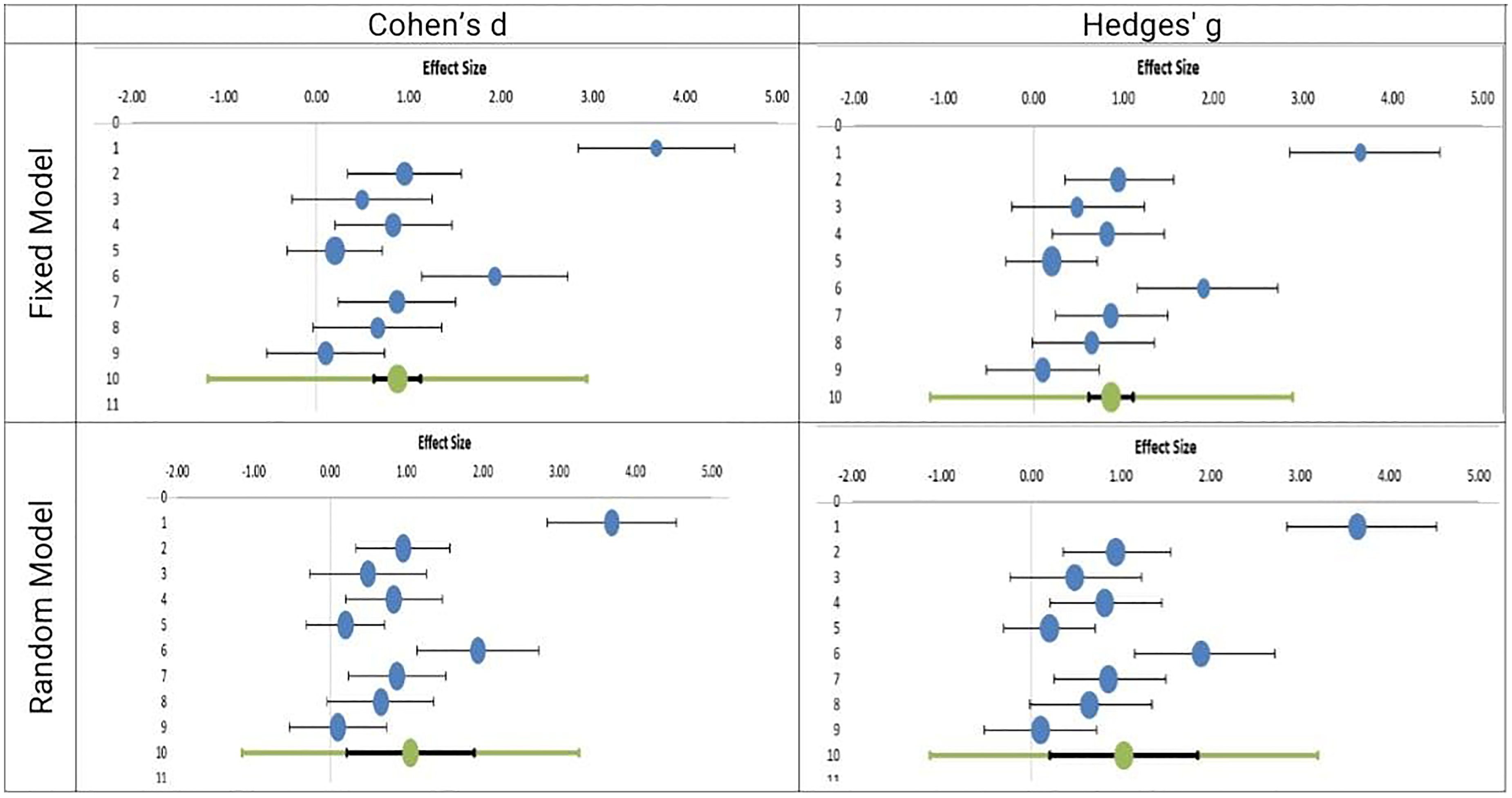
Forest plots of pain fixed and random models using both Cohen's d and hedges’g.
Summary of pain meta-analysis models and effect sizes.
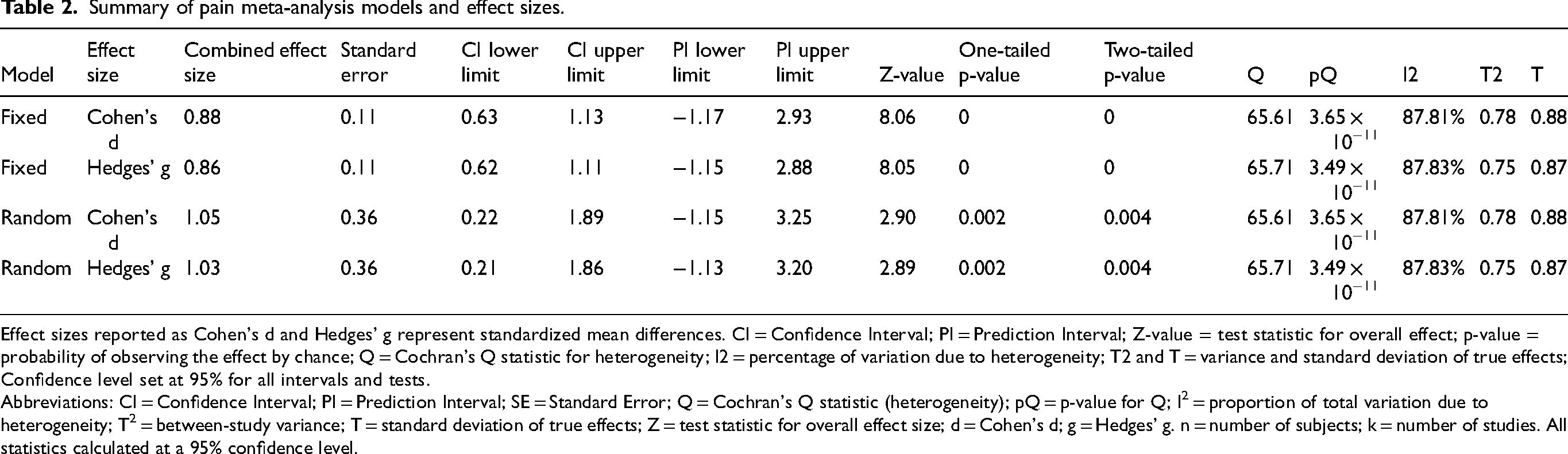
Effect sizes reported as Cohen's d and Hedges’ g represent standardized mean differences. CI = Confidence Interval; PI = Prediction Interval; Z-value = test statistic for overall effect; p-value = probability of observing the effect by chance; Q = Cochran's Q statistic for heterogeneity; I2 = percentage of variation due to heterogeneity; T2 and T = variance and standard deviation of true effects; Confidence level set at 95% for all intervals and tests.
Abbreviations: CI = Confidence Interval; PI = Prediction Interval; SE = Standard Error; Q = Cochran's Q statistic (heterogeneity); pQ = p-value for Q; I2 = proportion of total variation due to heterogeneity; T2 = between-study variance; T = standard deviation of true effects; Z = test statistic for overall effect size; d = Cohen's d; g = Hedges’ g. n = number of subjects; k = number of studies. All statistics calculated at a 95% confidence level.
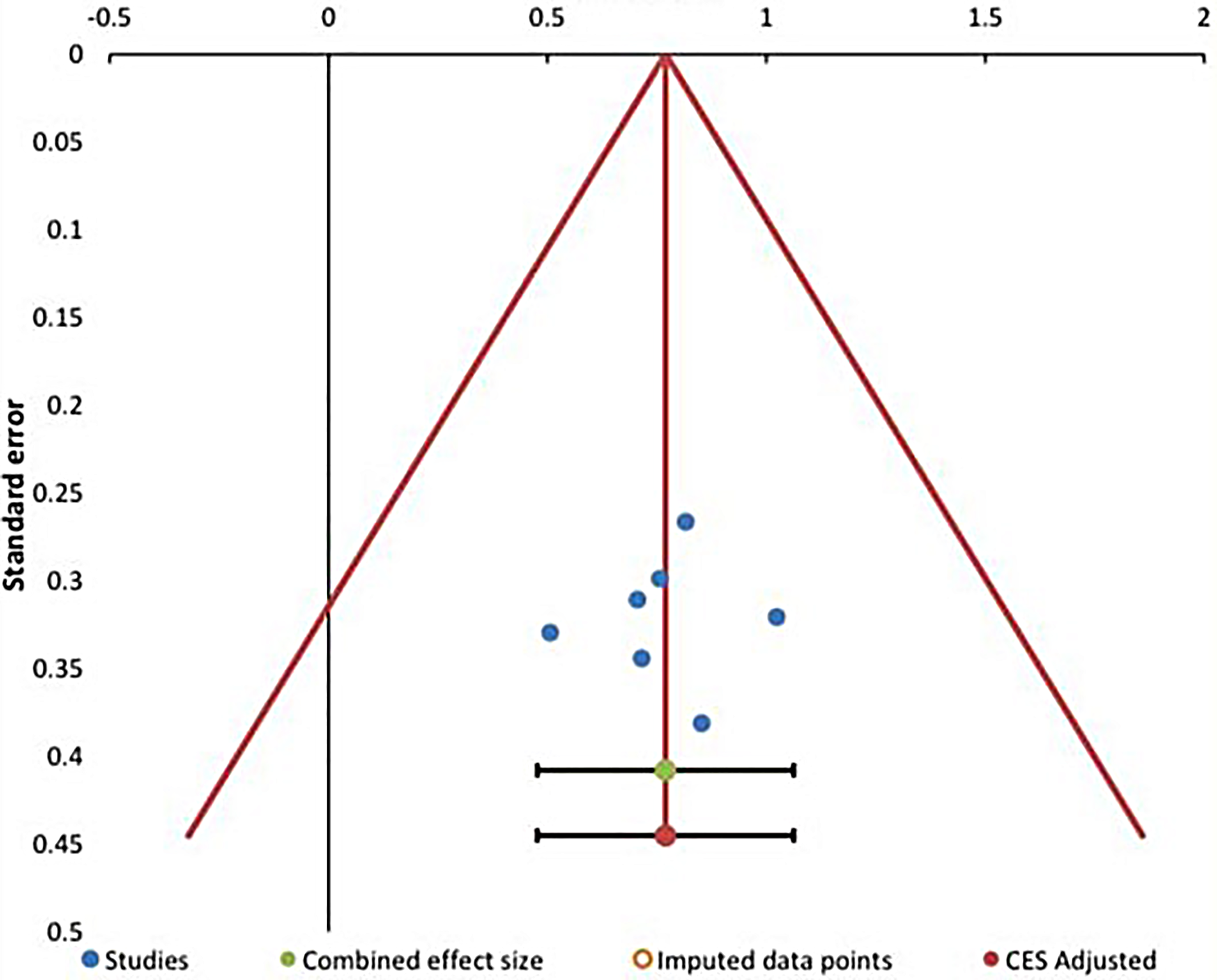
The pain results bias analysis reveals that Egger's regression test indicates significant asymmetry suggestive of potential publication bias, with an intercept of 14.47 (p = 0.018) and a notably negative slope, though the upper limit of the slope's confidence interval is not estimable. The Begg & Mazumdar rank correlation test, however, shows a non-significant result (Kendall's Tau a = 0.33, p = 0.211), suggesting weaker evidence for bias. Failsafe tests provide mixed findings: Rosenthal's Failsafe-N is 252 with a high overall Z-score (8.85), indicating that many studies would be needed to nullify the observed effect; Gleser & Olkin estimate 13 unpublished studies; Orwin's approach returns a failsafe-N of 0, reflecting high fragility under their criterion; and Fisher's method gives a very large failsafe-N (1493) and a significant chi-square test (p < 0.001), all together suggesting that while there is statistical evidence of some publication bias, the core findings remain robust against hypothetical unpublished studies. Visual inspection of the funnel plot (Figure 4) further supports the presence of asymmetry consistent with potential small-study effects.
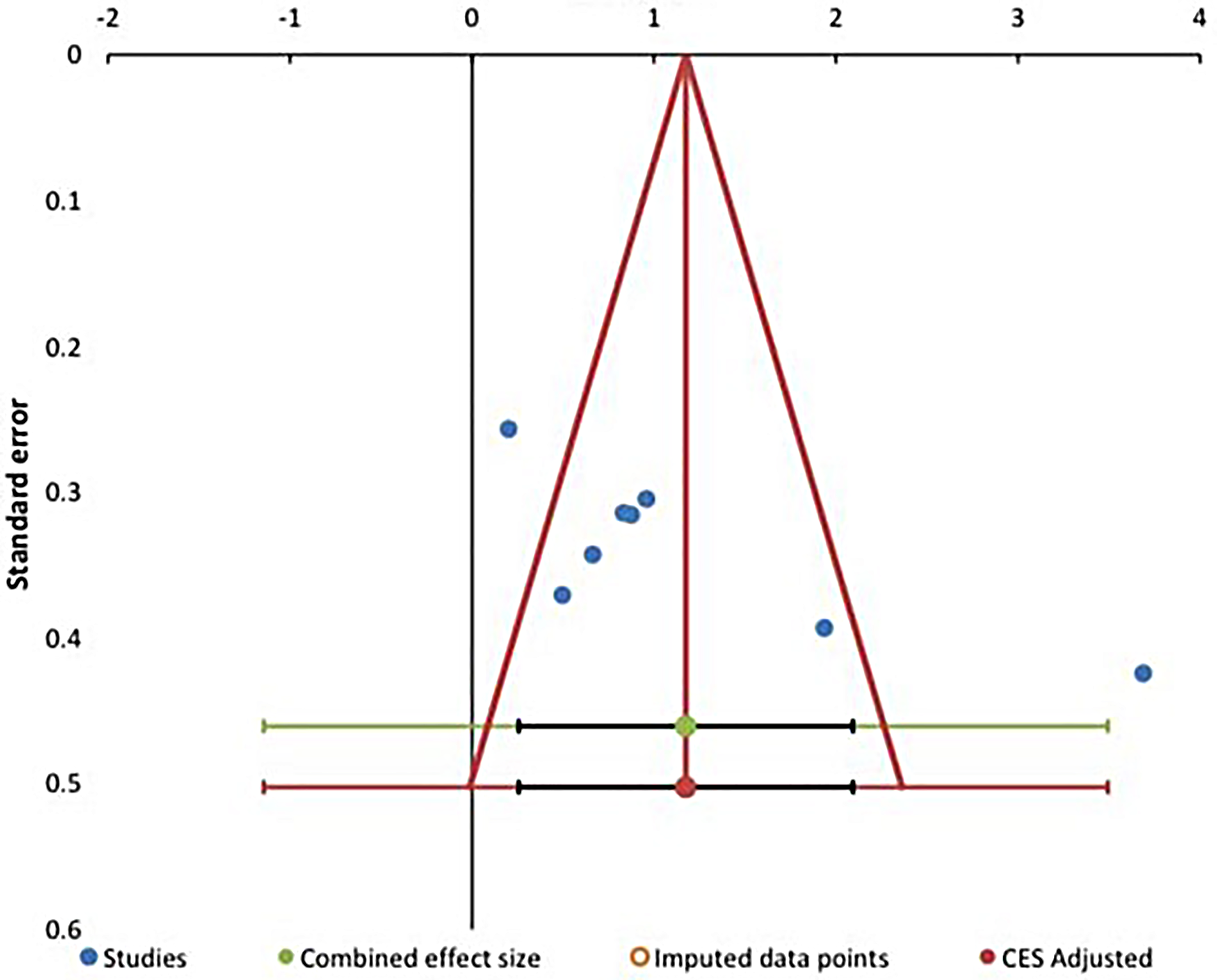
Funnel plot of pain intensity outcomes assessing potential publication bias. Effect sizes (Cohen's d) are plotted against their standard errors.
Disability
Disability represents a critical, patient-centered outcome in chronic neck pain management, as it directly reflects functional limitations in daily activities and overall quality of life. In this meta-analysis, disability was primarily evaluated using the Neck Disability Index (NDI), a validated and widely applied instrument that quantifies the impact of neck pain on daily functions such as personal care, lifting, reading, work, driving, and sleep. Since functional restoration is a fundamental objective of therapeutic interventions for chronic neck pain, assessing disability outcomes provides valuable insight into the clinical relevance of cupping therapy beyond pain reduction. The following analysis presents the pooled effects of cupping interventions on disability outcomes across the included randomized controlled trials (See Table 3 and Figure 5 forest plot).
Forest plots of neck disability Index and random models using both Cohen's d and hedges’g.
Summary of neck disability Index meta-analysis models and effect sizes.
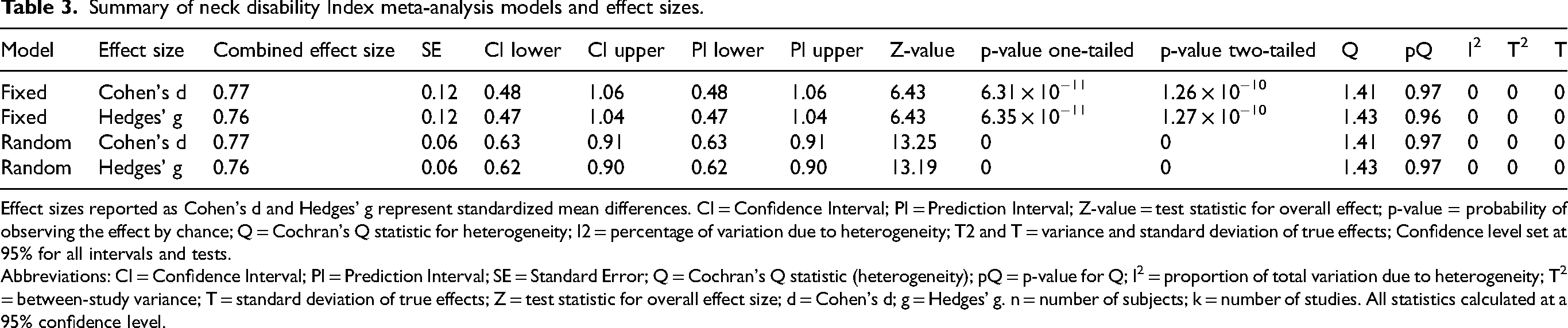
Effect sizes reported as Cohen's d and Hedges’ g represent standardized mean differences. CI = Confidence Interval; PI = Prediction Interval; Z-value = test statistic for overall effect; p-value = probability of observing the effect by chance; Q = Cochran's Q statistic for heterogeneity; I2 = percentage of variation due to heterogeneity; T2 and T = variance and standard deviation of true effects; Confidence level set at 95% for all intervals and tests.
Abbreviations: CI = Confidence Interval; PI = Prediction Interval; SE = Standard Error; Q = Cochran's Q statistic (heterogeneity); pQ = p-value for Q; I2 = proportion of total variation due to heterogeneity; T2 = between-study variance; T = standard deviation of true effects; Z = test statistic for overall effect size; d = Cohen's d; g = Hedges’ g. n = number of subjects; k = number of studies. All statistics calculated at a 95% confidence level.
The disability publication bias analysis for this set of results suggests minimal evidence of publication bias. Egger's regression shows a non-significant intercept (−0.31, p = 0.877) and slope (0.87, p = 0.877), with confidence intervals crossing zero, indicating no substantial small-study effects or asymmetry. Similarly, Begg & Mazumdar's test is non-significant (Kendall's Tau a = -0.05, p = 0.881), reinforcing the lack of detectable bias. Among the failsafe tests, Rosenthal's Failsafe-N is 99 with a high overall Z-score (6.39), while Gleser & Olkin estimate 90 unpublished studies would be needed to nullify the findings. Orwin's criterion demonstrates extreme fragility (Failsafe-N = 0), and Fisher's method yields a lower failsafe-N of 70 but a significant chi-square (p < 0.001). Taken together, these results indicate that the body of evidence appears generally robust with little indication of publication bias, although the Orwin and Fisher tests suggest that the statistical significance may be sensitive to a small number of hypothetical null studies (Table 4). Visual inspection of the funnel plot (Figure 6) does not demonstrate appreciable asymmetry and is consistent with the non-significant results of Egger's and Begg's tests.
Funnel plot of neck disability Index outcomes assessing potential publication bias. Effect sizes (Cohen's d) are plotted against their standard errors.
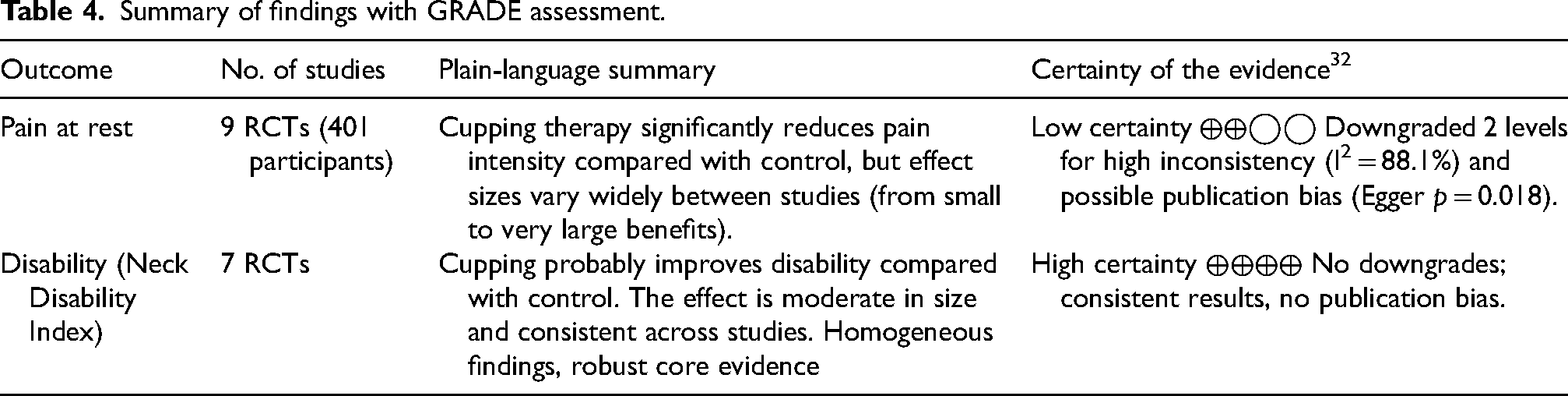
Summary of findings with GRADE assessment.
Certainty of evidence 32
For
For
Within the GRADE framework, we considered downgrading for risk of bias due to the limited feasibility of blinding; however, because the disability outcome is less susceptible to expectation effects than pain, the effect estimates were consistent across studies, and there was no evidence of publication bias, we judged that an additional downgrade was not warranted and retained a high certainty rating for disability.
Secondary outcomes
For
Discussion
Cupping therapy demonstrated consistent functional benefits across the included trials, reinforcing its applicability as a supportive intervention in the management of chronic neck pain.34,35 The uniformity of disability improvements across diverse treatment formats suggests that functional recovery is not strictly dependent on suction intensity, modality type, or delivery context, but rather reflects an accumulated adaptation in neuromuscular tolerance, movement confidence, and task engagement.36,37 Unlike pain perception, which is inherently subjective and influenced by expectation, comparator strength, and treatment ritual, disability outcomes tend to capture more enduring behavioral and motor improvements, making them more stable indicators of therapeutic efficacy. 38 In our pooled analyses, disability outcomes were derived from a larger proportion of studies with consistent direction of effect and low statistical heterogeneity, which supports a more confident interpretation of functional gains, whereas pain estimates were more heterogeneous and more susceptible to risk-of-bias influences. 14 This distinction between functional consistency and perceptual variability highlights an important clinical consideration: while analgesic relief is desirable, it is the restoration of activity tolerance and movement willingness that ultimately determines long-term rehabilitation success. 37 Within this context, cupping appears to function not merely as a passive pain-relieving modality but as a readiness-enhancing catalyst that facilitates engagement in subsequent active care. 39 By reducing discomfort enough to lower movement fear while concurrently reinforcing sensory resilience, cupping may serve as an effective transition point between symptom relief and active rehabilitation.
The considerable heterogeneity observed in pain outcomes (I2 = 88%) likely stems from the broad methodological variability among the included trials.40,41 Studies such as Chi et al. 23 and Rodríguez-Huguet et al. 28 illustrate the two extremes of this spectrum—from brief, manually delivered fire cupping with minimal parameter control to digitally regulated, multi-session vacuum protocols ensuring precise and reproducible dosing. The remaining trials occupied intermediate positions along this continuum, reflecting gradual differences in treatment standardization and dose that likely dispersed the pain effect sizes. Consistent with this interpretation, a subgroup analysis by control group type further suggested that the degree of comparator activity influenced pain outcomes. Trials using passive controls generally reported larger benefits, likely reflecting the greater therapeutic contrast with no-treatment conditions, whereas those with active comparators showed more modest effects.42,43 Together, these patterns indicate that both variability in intervention methodology and control group intensity plausibly contributed to the substantial heterogeneity observed in the pooled analysis. 44 Despite this heterogeneity, all trials demonstrated pain improvement to some extent, indicating that analgesia is a consistent qualitative outcome of cupping, even if its magnitude varies depending on implementation context.45,46 It is also noteworthy that some of the very large standardized effect sizes for pain arose from small, unblinded trials with minimal parameter control, in which expectation effects and regression to the mean may have amplified apparent treatment benefits; consequently, these extreme values should be interpreted cautiously and are unlikely to reflect typical, reproducible clinical effects in routine practice.
In addition to these findings, methodological quality deserves consideration. Risk of bias assessment using the ROB 2 tool 47 revealed that most studies had some methodological concerns, particularly in domains related to blinding of participants and outcome measurement—an expected limitation given the tactile and visible nature of cupping therapy. 12 Although seven studies were rated at high overall risk, the influence of this bias is somewhat mitigated by the consistent direction of disability improvement across all trials, suggesting that functional benefits were not solely perception-driven. Nevertheless, performance and detection bias may have inflated subjective pain estimates, contributing to the observed heterogeneity. Accordingly, our conclusions emphasize disability improvements as moderately to highly certain within the GRADE framework, while pain relief is interpreted more cautiously as promising but low-to-moderate certainty evidence that requires confirmation in larger, better-blinded trials. 47
Publication bias was also explored to assess potential overrepresentation of positive findings. Funnel plot asymmetry and Egger's regression (p = 0.018) indicated possible small-study effects in pain outcomes, whereas disability results showed no significant asymmetry (p = 0.877). This suggests that while some unpublished or negative pain studies may exist, their absence would not fully overturn the observed results. The robustness of the disability data, supported by consistent findings and high GRADE certainty, 32 reinforces the stability of the functional outcomes despite moderate bias concerns for pain.
Beyond pain and disability, several studies also documented improvements in secondary domains such as pressure pain thresholds, cervical range of motion, and vitality-related well-being, supporting the hypothesis that cupping exerts both peripheral and central effects rather than acting solely as a superficial circulatory stimulant.11,39 However, it is important to note that these mechanistic interpretations are largely hypothesis-generating and are only indirectly supported by the included RCTs, which were primarily designed to assess clinical outcomes rather than underlying physiological pathways. As such, the proposed contributions of microcirculatory enhancement, inflammatory modulation, and activation of descending inhibitory control should be interpreted as plausible explanatory models rather than definitive, trial-proven mechanisms. 14 Mechanistic theories propose contributions from enhanced local blood flow, modulation of inflammatory mediators, and activation of descending inhibitory control, which together could explain the observed convergence of sensory relief and functional restoration.48,49 From a clinical perspective, these multidimensional benefits, coupled with low cost, broad accessibility, and compatibility with both clinical and community-based implementation, make cupping a viable candidate for integration within multidisciplinary care frameworks. 38 Instead of being implemented on its own, its optimal role appears to lie in serving as a facilitating component that reduces resistance to movement and accelerates readiness for active rehabilitation strategies such as exercise and manual therapy. 5 This positioning aligns with contemporary models of musculoskeletal care, which prioritize graded exposure and engagement rather than passive symptom masking. 36
However, interpretation of these findings should acknowledge certain limitations. Pain outcomes showed substantial heterogeneity, likely reflecting methodological variability across studies.40,44 Because no subgroup or sensitivity analyses were prespecified and the limited number of trials and variable reporting precluded robust post-hoc subgroup modeling (e.g., by cupping modality, comparator type, or treatment dose), this heterogeneity could not be fully explored quantitatively and therefore constrains the interpretability of the pooled pain estimates. In contrast, disability outcomes were homogeneous and consistent across trials, which strengthens confidence in that finding. While other limitations related to blinding, heterogeneity of analgesic effects, sample size, and short follow-up warrant cautious interpretation for long-term pain relief and rare harms, In addition, mechanistic inferences in this review remain indirect, as none of the included trials were primarily powered or designed to formally test physiological pathways. 23 At the same time, this review has several strengths, including a comprehensive multi-database search strategy, prospective PROSPERO registration, adherence to PRISMA 2020, use of the RoB 2 tool for risk-of-bias assessment, and application of the GRADE approach to rate the certainty of evidence. the current evidence base justifies the use of cupping as a practical, low-cost adjunct within multidisciplinary management,41,45 pending larger and longer trials to optimize protocols and confirm durability of benefit. Future research should prioritize standardized reporting frameworks, incorporate attention-matched control conditions where feasible, and extend observation beyond immediate post-treatment phases. Despite these limitations, the overall pattern of evidence positions cupping is not as a curative monotherapy but as a function-enhancing adjunct with meaningful utility in conservative management.34,38 By reliably improving disability and likely contributing to analgesic relief across both passive and active comparators, it offers a pragmatic, scalable option for clinicians seeking to bridge the gap between symptom reduction and movement re-engagement. Within this transitional role, its integration alongside exercise, education, or manual interventions appears not only reasonable but strategically aligned with modern rehabilitation principles emphasizing progression from passive relief toward active restoration.
Conclusion
In Cupping therapy delivers consistent, clinically meaningful improvements in functional disability (I2 = 0%) and significant reductions in pain intensity for adults with chronic neck pain, all within a favorable safety profile. By integrating the most recent high-quality RCTs,14,27,28,30 this review elevates the evidence base, confirming cupping as a function-enhancing adjunct in multidisciplinary chronic neck pain management. These findings support its incorporation into clinical guidelines to bridge symptom relief with active rehabilitation, while Future studies should emphasize long-term outcomes and sustainability of the intervention, standardized protocols, and rigorous blinding strategies to further solidify practice recommendations.
Key messages
First meta-analysis exclusively focused on cupping therapy for chronic neck pain, incorporating recent high-quality RCTs to strengthen the evidence base.
Disability improvement was remarkably consistent across all studies (I2 = 0%), demonstrating robust functional benefits regardless of cupping modality or comparator.
Pain reduction was significant but heterogeneous (I2 = 88.1%), reflecting expected variability in cupping techniques, treatment protocols, and control group intensities.
Excellent safety profile confirmed with no serious adverse events reported across 401 participants and nine trials.
Evidence base significantly elevated beyond previous reviews, providing definitive support for cupping as a function-enhancing adjunct in multidisciplinary chronic neck pain management.
Supplemental Material
sj-docx-1-bmr-10.1177_10538127261446411 - Supplemental material for Effect of cupping therapy on chronic neck pain: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-bmr-10.1177_10538127261446411 for Effect of cupping therapy on chronic neck pain: A systematic review and meta-analysis of randomized controlled trials by Ahmed AM Torad, Mona Mohamed Taha, Reda Fathi Elbosaty, Noran Abdallah Essa, Sara Alsaeed Skout, Omnia Mohamed Abdelmoneim, Salma Mohammed Dawood, Ammar M Al Abbad and Mahmoud Ewidea in Journal of Back and Musculoskeletal Rehabilitation
Supplemental Material
sj-docx-2-bmr-10.1177_10538127261446411 - Supplemental material for Effect of cupping therapy on chronic neck pain: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-2-bmr-10.1177_10538127261446411 for Effect of cupping therapy on chronic neck pain: A systematic review and meta-analysis of randomized controlled trials by Ahmed AM Torad, Mona Mohamed Taha, Reda Fathi Elbosaty, Noran Abdallah Essa, Sara Alsaeed Skout, Omnia Mohamed Abdelmoneim, Salma Mohammed Dawood, Ammar M Al Abbad and Mahmoud Ewidea in Journal of Back and Musculoskeletal Rehabilitation
Footnotes
Abbreviations
The following abbreviations are used in this manuscript:
Acknowledgments
We sincerely thank Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2026R209), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia for supporting this project.
ORCID iDs
Informed consent statement
Patient consent for publication was not required as this study did not involve direct patient participation.
Author contributions
Conceptualization, AAMT, and RFE; methodology, RFE, NAE, and AAMT; software, MMT; validation, AAMT, NAE, MMT, and ME; formal analysis, NAE and MMT; investigation, SAS, OMAE., and SMD; resources, RFE; data curation, NAE, SAS, OMAE., and SMD; writing—original draft preparation, NAE, SAS, OMAE., SMD, and MMT; writing—review and editing, AAMT, RFE, MMT, AMAA, and ME; visualization, SMD; supervision, AAMT and ME; project administration, RFE, and MMT; funding acquisition. All authors have read and agreed to the published version of the manuscript. All authors fulfill the ICMJE authorship criteria, have approved the final manuscript, and agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2026R209), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the original publications as cited within the manuscript. All included studies are fully referenced.
Disclaimer/Publisher's Note
The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
Institutional review board statement
This systematic review was prospectively registered in the International Prospective Register of Systematic Reviews, ID: CRD42025633104. Ethics approval was not required for this study as it is a systematic review and meta-analysis of previously published and publicly available data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.