
Abstract
Shoulder pain is highly prevalent and may persist despite conservative care, leading to functional limitation and substantial healthcare burden. Percutaneous peripheral nerve stimulation (PNS) has emerged as a targeted neuromodulation strategy; however, randomized evidence remains heterogeneous across stimulation parameters and clinical presentations. This systematic review followed PRISMA 2020 guidelines and was registered in PROSPERO (CRD420251247712). PubMed, Scopus, Embase, and Web of Science were searched (December 2015–December 2025; English language). Randomized controlled trials (RCTs) evaluating percutaneous PNS-related interventions for postoperative shoulder pain, chronic shoulder pain, supraspinatus tendinopathy, upper trapezius myofascial pain, and cervical-related shoulder pain were included. The search identified 2189 records; after removal of 723 duplicates, 1466 titles and abstracts were screened and 54 full texts assessed. Ten RCTs met eligibility criteria. Postoperative trials demonstrated clinically meaningful pain reductions and opioid-sparing effects with ultrasound-guided brachial plexus PNS compared with sham stimulation. In supraspinatus tendinopathy, multimodal programs integrating PNS with eccentric exercise and percutaneous electrolysis yielded superior improvements in pain and disability compared with conventional rehabilitation. For upper trapezius myofascial pain, intramuscular and percutaneous stimulation protocols produced short-term improvements in pain and mechanical sensitivity. Cervical neuromuscular stimulation trials also demonstrated significant benefits in pain and range of motion. Overall risk of bias was moderate to high, with the majority of trials rated as low risk and the remainder as having some concerns. Current RCT evidence supports percutaneous PNS as a safe and clinically relevant intervention for shoulder pain, particularly in postoperative analgesia and chronic tendinopathy when integrated into rehabilitation programs. However, substantial variability in stimulation dosimetry highlights the need for protocol standardization in future trials.
Introduction
Shoulder pain is among the most prevalent musculoskeletal complaints encountered in orthopedic and rehabilitation practice, affecting individuals across all age groups and imposing a substantial burden on function, quality of life, and healthcare systems. 1 Common clinical presentations include postoperative pain following rotator cuff repair, supraspinatus tendinopathy, upper trapezius myofascial pain, and chronic cervicobrachial syndromes.2,3 Although a wide range of conservative and pharmacological treatments is available, a considerable proportion of patients experience persistent pain, functional impairment, and prolonged recovery, underscoring the need for more effective and safer non-surgical interventions.
The pathophysiology of shoulder pain is multifactorial, involving the interaction of peripheral tissue injury, altered neuromuscular control, and maladaptive neural processing. Injury or overload of rotator cuff tendons, periarticular bursae, the glenohumeral capsule, or scapular stabilizing muscles activates peripheral nociceptors and promotes the release of inflammatory mediators, leading to peripheral sensitization and pain amplification.4,5 With symptom persistence, alterations in motor control commonly emerge, including reflex inhibition of the supraspinatus muscle and compensatory overactivation of the upper trapezius, contributing to scapular dyskinesis and increased mechanical stress on sensitized structures. 6
In chronic conditions, central sensitization plays an increasingly prominent role, characterized by enhanced nociceptive signaling at the spinal level, expansion of receptive fields, and impaired descending inhibitory control. 7 These neurophysiological changes help explain why shoulder pain frequently persists beyond tissue healing and is often accompanied by weakness, impaired proprioception, and functional limitation. Consequently, shoulder pain should be viewed as a complex and multidimensional condition that extends beyond isolated structural pathology.
Percutaneous peripheral nerve stimulation (PNS) has emerged as a promising therapeutic option for the management of musculoskeletal and neuropathic pain. In this review, PNS is used as an umbrella term for percutaneous neuromodulation approaches targeting peripheral nerves or motor points. Percutaneous electrical nerve stimulation (PENS) refers to percutaneous stimulation delivered near a named nerve, typically under anatomical or ultrasound guidance. Intramuscular electrical stimulation refers to percutaneous stimulation delivered within the muscle to target motor points or trigger point regions.
Common stimulation parameters reported in the literature include frequencies ranging from 2 to 100 Hz, pulse widths between 50 and 400 µs, and amplitudes adjusted to elicit comfortable sensory or motor responses without inducing excessive discomfort. In clinical practice, PNS has been widely applied for neuropathic pain, chronic low back pain, postoperative analgesia, and refractory musculoskeletal conditions. Expected treatment outcomes include reduction in pain intensity, improvement in functional capacity, decreased opioid consumption in postoperative settings, and modulation of central sensitization mechanisms in chronic conditions. These physiological and clinical characteristics distinguish percutaneous PNS from superficial electrotherapeutic modalities and underscore its growing role in pain management. 7 Ultrasound-guided stimulation of the brachial plexus, suprascapular, or axillary nerves, as well as intramuscular stimulation of myofascial trigger points, has demonstrated encouraging results in clinical trials, with improvements in pain intensity, function, and postoperative recovery.8–10
From a mechanistic perspective, PNS primarily activates large-diameter afferent fibers, reducing nociceptive transmission through segmental spinal mechanisms and facilitating descending inhibitory pathways. 11 Additionally, peripheral effects on motor unit recruitment and neuromuscular coordination may contribute to improved shoulder biomechanics and functional recovery. 12 These combined effects offer a plausible explanation for the rapid analgesia and sustained clinical benefits reported in several trials. 13
Despite increasing interest in PNS, considerable heterogeneity remains across stimulation protocols, treatment duration, patient populations, and comparator interventions, limiting the generalizability of individual study findings. 14 Moreover, it remains unclear whether the therapeutic effects of PNS differ between acute postoperative conditions, chronic shoulder pain, and tendinopathic disorders, or whether specific patient subgroups derive greater benefit.15,16 Therefore, a systematic and up-to-date synthesis of randomized evidence is warranted to clarify the clinical role of PNS in shoulder pain management.
Accordingly, this systematic review aimed to evaluate the effects of PNS on pain intensity, functional outcomes, and neuromuscular recovery in adults with shoulder pain or upper trapezius myofascial pain, encompassing postoperative, chronic, and tendinopathic conditions. The review was conducted in accordance with PRISMA 2020 guidelines and seeks to provide clinically relevant evidence to inform orthopedic practice and future research.
Methods
Study design
This systematic review examined the effects of percutaneous peripheral nerve stimulation (PNS) on pain intensity, functional outcomes, and neuromuscular recovery in adults with shoulder pain or upper trapezius myofascial pain. The review followed the PRISMA 2020 guidelines and was prospectively registered in PROSPERO (CRD420251247712).
Eligibility criteria
Eligibility criteria were defined using the PICO framework:
Population: Adults (≥18 years) with acute postoperative shoulder pain, chronic shoulder pain, supraspinatus tendinopathy, hemiplegic shoulder pain, or upper trapezius myofascial pain. Studies involving pediatric populations, surgical PNS implants, or mixed samples without extractable shoulder-specific data were excluded.
Intervention: Percutaneous peripheral nerve stimulation (PNS), including ultrasound-guided electrical stimulation of suprascapular, axillary, or brachial plexus nerves; intramuscular electrical stimulation of upper trapezius trigger points; percutaneous neuromodulation protocols (2–150 Hz); multimodal interventions combining PNS with exercise, dry needling, or electrolysis. Both short-duration (single session to 4-week) and extended (60-day) protocols were eligible.
Comparison: Sham stimulation, placebo PNS, conventional physiotherapy, other electrotherapies, standard postoperative care, or no intervention.
Primary Outcomes: Pain intensity and functional disability (DASH/SPADI); Secondary Outcomes: Opioid consumption, ROM, PPT, adverse events.
Study design
Randomized controlled trials (sham-controlled or active comparator) were included. Case reports informed mechanistic plausibility but were not used for effect synthesis.
Information sources
Electronic searches were conducted in PubMed, Scopus, Embase, and Web of Science, covering the period from December 2015 to December 2025. The search was restricted to randomized controlled trials published in peer-reviewed journals and indexed in these databases. Only studies published in English were considered.
In addition to database searches, reference lists of included studies and relevant reviews were manually screened to identify potentially eligible trials. Forward citation tracking was performed using Scopus to ensure comprehensive coverage of indexed RCTs.
Grey literature sources and clinical trial registries were not systematically searched, as the objective of this review was to synthesize completed, fully reported randomized controlled trials suitable for formal methodological appraisal.
Search strategy
The search used MeSH and free-text terms related to PNS and shoulder pain.
A representative PubMed strategy included: (“percutaneous nerve stimulation” OR “percutaneous electrical nerve stimulation” OR “PENS” OR “peripheral nerve stimulation”) AND (“shoulder pain” OR “suprascapular nerve” OR “rotator cuff” OR “myofascial pain” OR “upper trapezius”) AND (“randomized controlled trial” OR “sham” OR “placebo”)
Search strategies were adapted for EMBASE (Emtree terms) and Scopus. Full strategies are available upon request.
Study selection
All records were imported into Rayyan for duplicate removal and screening.
Two independent reviewers (G.S.P and M.L.S.) with clinical and research experience in musculoskeletal rehabilitation and neuromodulation conducted study selection and quality assessment. Both reviewers have prior experience in systematic reviews and clinical application of percutaneous electrotherapy techniques. Screening and eligibility assessment were conducted using predefined inclusion and exclusion criteria derived from the PICO framework. Risk-of-bias assessment was performed using the Cochrane RoB 2 tool. Disagreements between reviewers were resolved through structured discussion and re-examination of eligibility criteria. As consensus was reached in all cases, involvement of a third independent arbitrator was not required.
A PRISMA 2020 flow diagram summarizes the selection process (Figure 1).
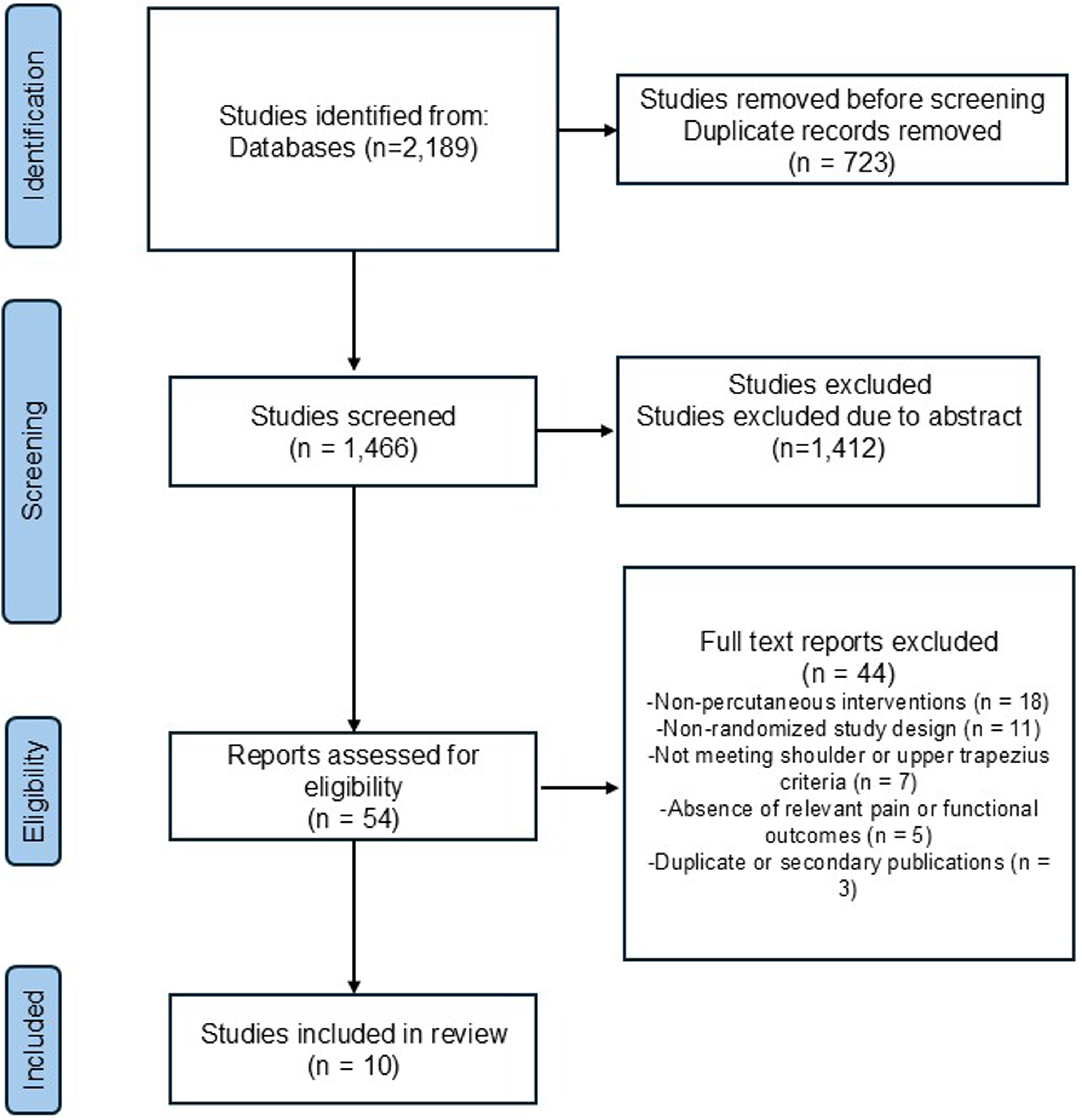
PRISMA 2020 flow diagram of study selection.
Data extraction
Two reviewers independently extracted data using a standardized form, including: study metadata (year, country, design, sample size); participant characteristics (diagnosis, chronicity, demographics); PNS protocol (target nerve, stimulation frequency, duration, guidance technique); comparator details; pain outcomes (values, effect sizes, time points); functional/ROM outcomes; opioid consumption outcomes; adverse events and device-related issues; follow-up duration (immediate to long-term, up to 5 years); where data were unclear or incomplete, study authors were contacted.
In addition to clinical condition, studies were descriptively stratified according to follow-up duration (immediate: ≤1 week; short-term: >1 week to 3 months; long-term: >3 months), use of ultrasound guidance for percutaneous electrode placement, and rehabilitation stage (acute/postoperative phase versus chronic presentations). Given the heterogeneity in protocols and outcome reporting, these stratifications were applied narratively to facilitate interpretability rather than for quantitative subgroup analysis.
Risk of bias and certainty assessment
The Cochrane Risk of Bias 2.0 (RoB 2) tool was applied to all randomized controlled trials, assessing domains of randomization, deviations from intended interventions, missing outcome data, measurement of outcomes, and selective reporting. Most studies used double-blind designs; blinding was less consistent in chronic pain trials due to treatment duration. ROBVIS was used for graphical visualization.
In addition to risk-of-bias assessment using the Cochrane RoB 2 tool, the overall certainty of evidence for each clinical condition was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework. Certainty ratings were determined for key outcomes (pain intensity, functional outcomes) within each clinical subgroup (postoperative shoulder pain, nonspecific chronic shoulder pain, supraspinatus tendinopathy, upper trapezius myofascial pain, and cervical-related shoulder symptoms).
The GRADE approach considers five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Evidence was categorized as high, moderate, low, or very low certainty. Downgrading decisions were made based on subgroup-level assessment of these domains, taking into account sample size, heterogeneity of interventions, and methodological limitations.
Data synthesis
Due to heterogeneity in treatment protocols and outcomes, results were synthesized narratively. Studies were grouped by clinical condition (postoperative shoulder pain, supraspinatus tendinopathy, chronic shoulder pain, upper trapezius myofascial pain, and cervical-related shoulder pain). Intervention characteristics were extracted in accordance with key Template for Intervention Description and Replication (TIDieR) domains (provider, setting, procedural guidance, stimulation parameters, tailoring, and adherence monitoring) to enhance reproducibility. Quantitative pooling was not feasible.
Results
Study selection and characteristics
The systematic search yielded 2189 records. After removal of 723 duplicates, 1466 titles and abstracts were screened for eligibility. Of these, 1412 were excluded for not meeting inclusion criteria, leaving 54 full-text articles for detailed assessment.
Following strict alignment with the PROSPERO-registered intervention criteria (percutaneous peripheral nerve stimulation or intramuscular percutaneous electrical stimulation), 10 randomized controlled trials met all eligibility criteria and were included in the final analysis (Figure 1).
The included trials investigated percutaneous neuromodulation across several shoulder-related conditions, including postoperative pain following rotator cuff repair, supraspinatus tendinopathy, chronic shoulder pain, upper trapezius myofascial pain, and cervical spondylosis involving the shoulder girdle.
Sample sizes ranged from 16 to 124 participants. Interventions targeted the brachial plexus, suprascapular nerve, axillary nerve, cervical nerve roots, or upper trapezius muscle. Stimulation frequencies ranged from 2 to 150 Hz, and treatment duration varied from single-session protocols to 60-day continuous stimulation programs. Sham-controlled designs predominated. Detailed characteristics of the included trials are presented in Table 1.
Characteristics of the included randomized controlled trials evaluating percutaneous peripheral nerve stimulation for shoulder and upper trapezius pain.
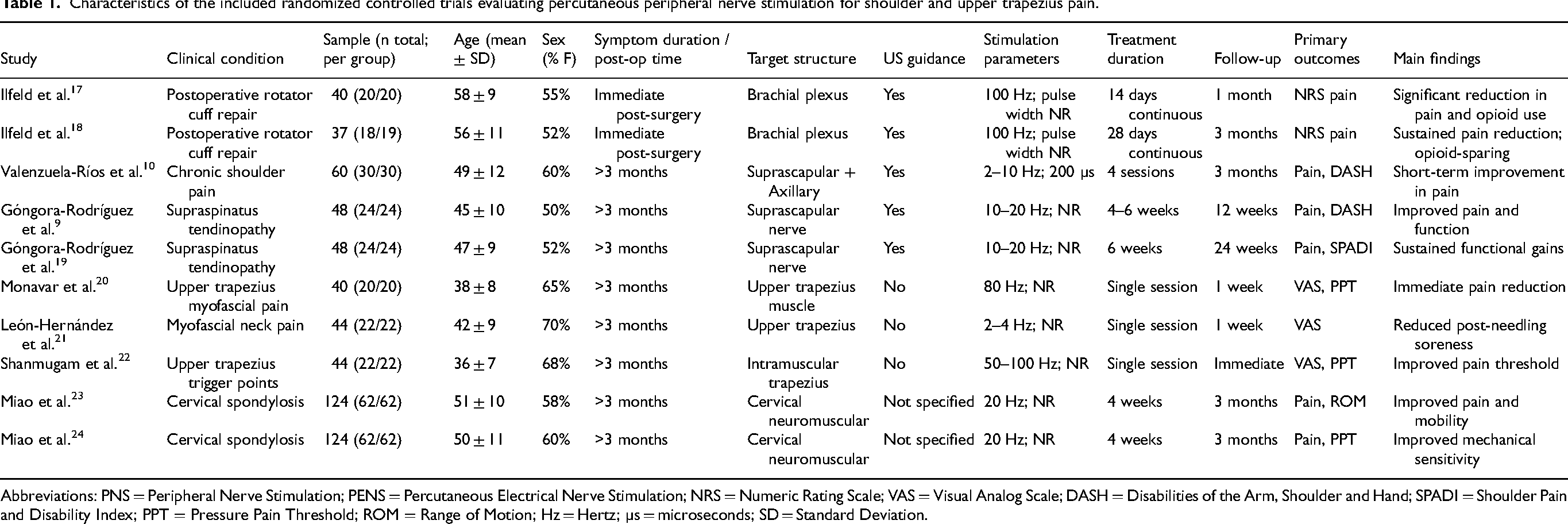
Abbreviations: PNS = Peripheral Nerve Stimulation; PENS = Percutaneous Electrical Nerve Stimulation; NRS = Numeric Rating Scale; VAS = Visual Analog Scale; DASH = Disabilities of the Arm, Shoulder and Hand; SPADI = Shoulder Pain and Disability Index; PPT = Pressure Pain Threshold; ROM = Range of Motion; Hz = Hertz; µs = microseconds; SD = Standard Deviation.
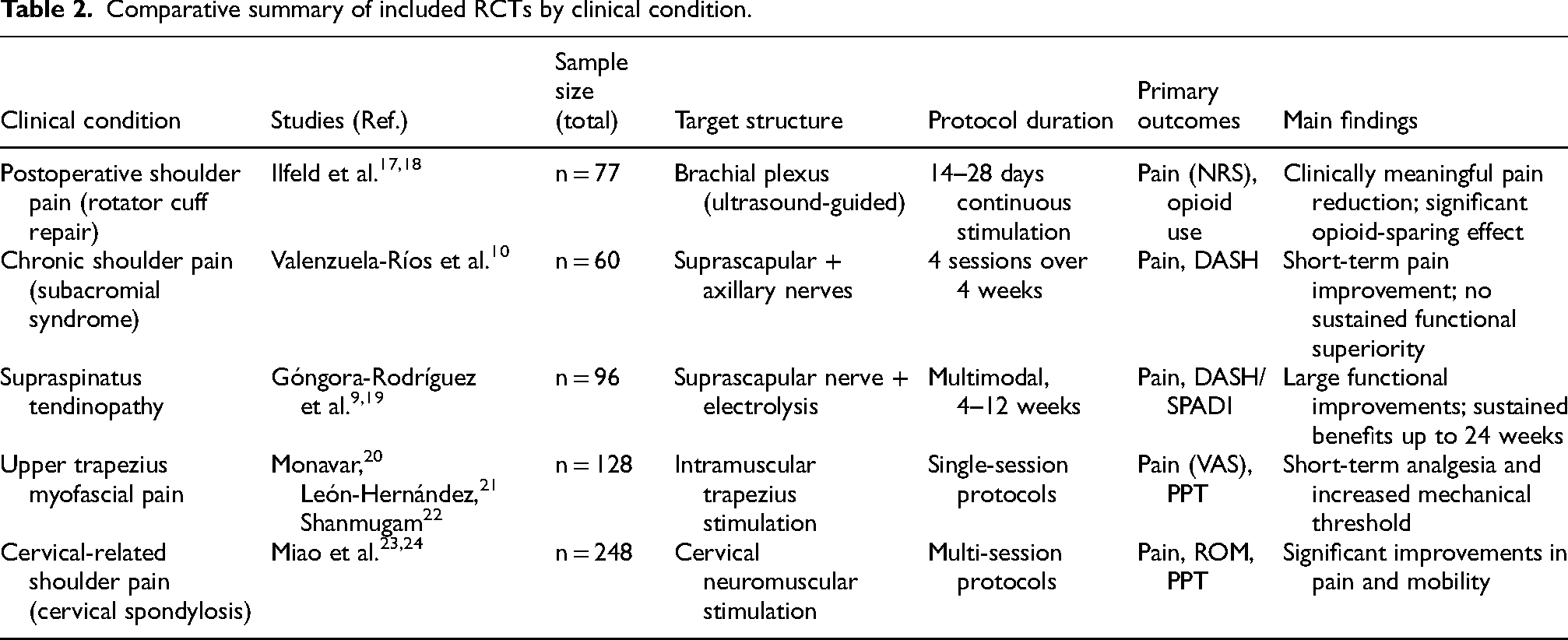
A structured comparison of studies according to clinical condition, target structures, and primary outcomes is presented in Table 2.
Comparative summary of included RCTs by clinical condition.
Postoperative shoulder pain
Two randomized controlled trials by Ilfeld et al. evaluated ultrasound-guided percutaneous peripheral nerve stimulation of the brachial plexus following rotator cuff repair.17,18 In the proof-of-concept trial, patients receiving active PNS demonstrated markedly lower postoperative pain scores (median NRS 0.8 vs 3.2) and substantially reduced opioid consumption compared with sham stimulation. 17 These findings were replicated in a larger pragmatic effectiveness trial, where active PNS resulted in significantly lower pain scores (1.1 ± 1.1 vs 3.1 ± 1.7) and reduced opioid requirements during the early postoperative period. 18
Collectively, these trials provide strong evidence that percutaneous PNS produces rapid, clinically meaningful analgesia and opioid-sparing effects after rotator cuff repair.
Chronic shoulder pain
Valenzuela-Rios et al. 10 evaluated four sessions of ultrasound-guided percutaneous electrical nerve stimulation (PENS) targeting the suprascapular and axillary nerves. Short-term improvements in pain were observed at one month; however, differences were not maintained at three months, and no significant superiority was found in disability outcomes compared with exercise alone.
This suggests that limited-session PENS protocols may provide transient analgesia but may require repeated or prolonged application to achieve durable functional benefits.
Supraspinatus tendinopathy
Two high-quality RCTs by Góngora-Rodríguez et al.9,19 evaluated multimodal rehabilitation programs combining percutaneous PNS with percutaneous electrolysis and eccentric exercise. In both studies, participants receiving the PNS-based protocol demonstrated significantly greater improvements in pain and disability (DASH and SPADI) compared with conventional electrotherapy-based rehabilitation. Clinical success rates approached 80%, and improvements were sustained at 12- and 24-week follow-up.
These findings support the integration of percutaneous PNS into multimodal rehabilitation for chronic tendinopathic shoulder disorders.
Upper trapezius myofascial pain
Three RCTs investigated intramuscular or percutaneous stimulation for upper trapezius myofascial pain. Monavar et al. 20 demonstrated that intramuscular electrical stimulation significantly reduced VAS pain scores and increased pressure pain threshold compared with placebo, with effects sustained for at least one week. León-Hernández et al. 21 showed that combining dry needling with percutaneous electrical nerve stimulation reduced post-needling soreness and improved pain outcomes compared with dry needling alone.
Shanmugam et al. 22 reported significant reductions in pain and improvements in pressure pain threshold with intramuscular stimulation, independent of electrode placement configuration.
Across studies, percutaneous stimulation consistently produced short-term improvements in pain intensity and mechanical sensitivity in myofascial trigger point syndromes.
Cervical spondylosis with shoulder involvement
Two RCTs by Miao et al.23,24 evaluated percutaneous neuromuscular electrical stimulation in patients with cervical spondylosis involving upper trapezius activation and shoulder-related symptoms.
Both trials demonstrated significant improvements in pain intensity, cervical range of motion, and pressure pain thresholds compared with sham stimulation. Although the primary pathology was cervical, shoulder girdle symptoms and muscle activation patterns were directly addressed.
These studies suggest that percutaneous neuromodulation targeting cervical segments may beneficially modulate shoulder-related pain when segmental mechanisms are involved.
Safety across RCTs
Across the 10 included RCTs, percutaneous PNS demonstrated a favorable safety profile. Reported adverse events were mild and transient, including temporary soreness, minor discomfort, and localized irritation.
No serious adverse events—such as infection, neurological injury, or persistent deficits—were reported. Continuous brachial plexus stimulation studies reported no major lead-related complications within trial duration.
Overall, the evidence supports percutaneous PNS as a safe and well-tolerated intervention in shoulder-related pain conditions.
Risk of bias
Overall, the methodological quality of the included trials was moderate to high.
Seven studies were judged to have an overall low risk of bias,9,10,17–19,22,24 while three studies were rated as having some concerns.20,21,23 No trial was classified as having a high overall risk of bias.
Regarding the randomization process, most trials adequately described random sequence generation and allocation concealment, particularly the sham-controlled neuromodulation studies. However, some trials provided limited detail on allocation concealment procedures, leading to “some concerns” in this domain.
In the domain of deviations from intended interventions, all included studies were judged to be at low risk of bias. Sham-controlled designs were frequently employed—especially in postoperative brachial plexus stimulation17,18 and cervical neuromuscular stimulation trials23,24—supporting appropriate participant and personnel blinding.
Missing outcome data were minimal across studies. Attrition rates were low and balanced between intervention and control groups, and analyses were generally conducted according to prespecified protocols.
Measurement of outcomes was considered low risk in most trials. Validated and standardized instruments were consistently used, including the Numeric Rating Scale (NRS),17,18 Visual Analog Scale (VAS),20–22 the Disabilities of the Arm, Shoulder and Hand (DASH),9,19 the Shoulder Pain and Disability Index (SPADI), 19 pressure pain threshold (PPT),20,22 and range-of-motion assessments.23,24 Outcome assessor blinding was reported in the majority of sham-controlled trials.9,17,18,24
With respect to selection of the reported result, most studies were judged to be at low risk. Nevertheless, some concerns were identified in trials lacking publicly available protocols or clear prespecification of primary outcomes,20,21 which may increase the possibility of selective reporting.
Figure 2 presents the updated ROBVIS summary, illustrating domain-specific and overall risk-of-bias judgments across the ten included percutaneous stimulation trials.
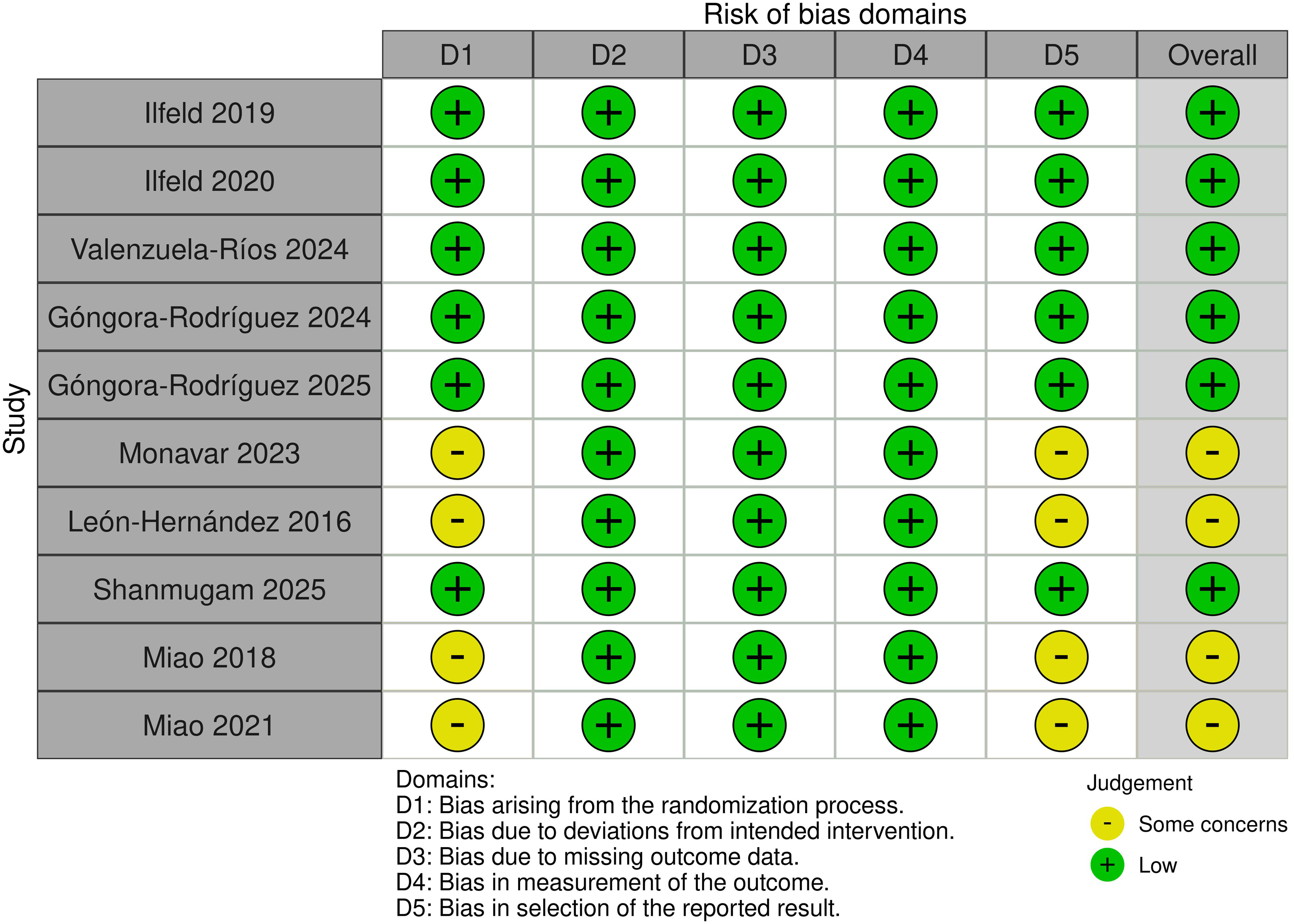
Risk-of-bias assessment of included randomized controlled trials using the Cochrane RoB 2 tool.
Certainty of evidence
Certainty of evidence was assessed using the GRADE framework and is summarized in Table 3.
GRADE certainty of evidence by clinical condition.
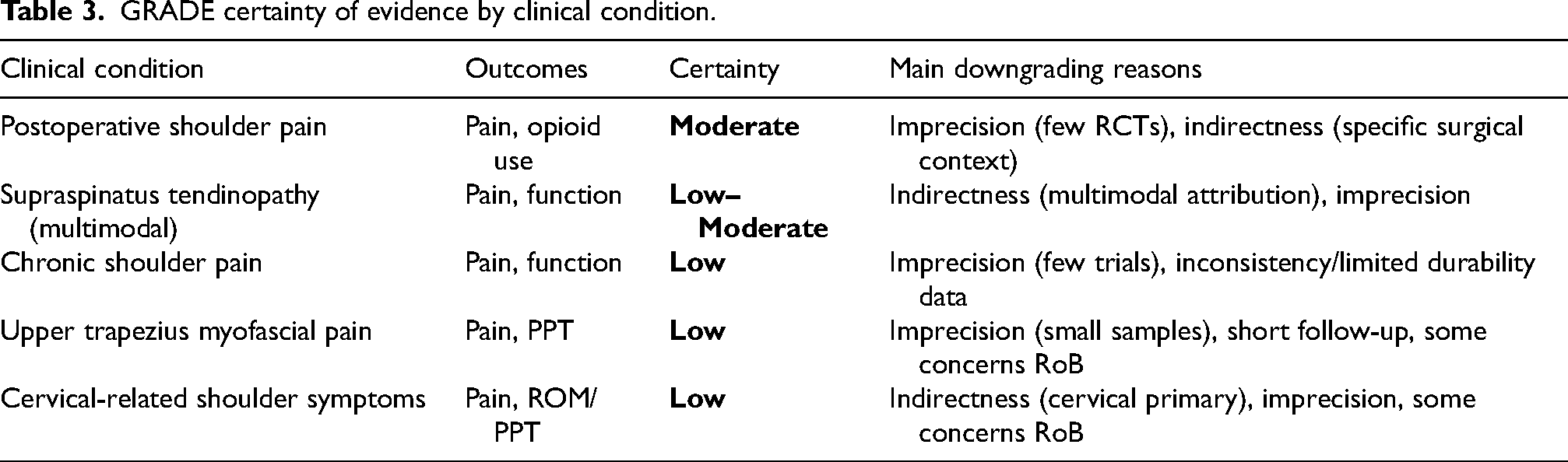
For postoperative shoulder pain, certainty was rated as moderate, primarily downgraded due to imprecision related to the limited number of trials despite consistent effect direction and magnitude.
For supraspinatus tendinopathy, certainty was rated as low to moderate, downgraded for indirectness given the multimodal nature of interventions and limited isolation of PNS-specific effects.
For nonspecific chronic shoulder pain, certainty was rated as low, due to imprecision and limited durability data.
For upper trapezius myofascial pain and cervical-related shoulder symptoms, certainty was also rated as low, primarily downgraded for imprecision (small sample sizes), short follow-up duration, and some concerns in risk-of-bias assessments.
Discussion
The findings of this systematic review indicate that PNS, including PENS and intramuscular electrical stimulation, produces clinically meaningful improvements in shoulder-related pain conditions. Across postoperative pain, supraspinatus tendinopathy, myofascial pain syndromes, and cervical-related shoulder pain, percutaneous neuromodulation demonstrated consistent analgesic effects, with several trials also reporting functional gains and opioid-sparing benefits.
The strongest evidence emerged in the postoperative setting. The randomized trials by Ilfeld et al.17,18 demonstrated substantial reductions in pain intensity and opioid consumption following rotator cuff repair when percutaneous brachial plexus stimulation was applied. The magnitude of analgesia observed in these trials exceeded established minimal clinically important differences (MCID) for pain reduction and was sustained throughout the early recovery phase. These findings suggest that direct modulation of shoulder-related neural structures may attenuate acute nociceptive drive and reduce reliance on opioid analgesia after surgery.
In supraspinatus tendinopathy, the trials by Góngora-Rodríguez et al.9,19 showed that combining percutaneous PNS with eccentric exercise and percutaneous electrolysis resulted in superior improvements in pain and disability (DASH/SPADI) compared with conventional rehabilitation strategies. Importantly, the improvements in disability exceeded commonly accepted MCID thresholds (10–15 points for DASH), supporting clinical relevance. These results reinforce the concept that percutaneous neuromodulation may enhance the effectiveness of structured rehabilitation programs rather than serving as an isolated modality. Because these trials did not include an isolated PNS-only arm, the specific causal contribution of PNS cannot be fully separated from the effects of exercise-based rehabilitation and electrolysis. The results support the clinical effectiveness of the integrated program, but attribution to PNS alone remains limited.
In upper trapezius myofascial pain, intramuscular and percutaneous stimulation approaches20–22 consistently produced short-term reductions in pain intensity and increases in pressure pain threshold. While the analgesic effects were robust in the immediate or short-term period, long-term durability was less consistently reported. This suggests that repeated sessions or integration within broader neuromuscular retraining programs may be required to achieve sustained benefit in myofascial syndromes. However, durability beyond short follow-up windows is unclear. Current evidence supports single-session protocols as producing short-term benefits, while repeated-session schedules should be viewed as a plausible strategy that requires direct testing in adequately powered RCTs with longer follow-up.
The cervical neuromuscular stimulation trials by Miao et al.23,24 demonstrated significant improvements in pain, range of motion, and mechanical sensitivity in patients with cervical spondylosis presenting with shoulder-related symptoms. These findings highlight the importance of segmental and proximal neural contributions to shoulder pain and suggest that percutaneous stimulation may exert therapeutic effects through modulation of cervical spinal circuits influencing scapulothoracic musculature.
In contrast, within the subgroup of nonspecific chronic shoulder pain (excluding postoperative, tendinopathic, and clearly cervical-driven presentations), the available evidence should be interpreted as exploratory. The limited number of eligible RCTs and variability in stimulation dose, treatment duration, and follow-up preclude firm clinical recommendations for this population. Trial characteristics that may influence durability include total treatment exposure (number of sessions), anatomical targeting precision, and the use of procedural guidance (e.g., ultrasound).
From a mechanistic perspective, percutaneous stimulation differs from surface-level electrotherapies by positioning the electrode in close proximity to target nerves or motor points. This facilitates activation of large-diameter afferent fibers and may enhance segmental inhibitory mechanisms and descending pain modulation pathways.11–16 Such mechanisms likely contribute to the sustained analgesia observed in postoperative and tendinopathic conditions. Additionally, intramuscular stimulation may influence local motor unit recruitment and reduce abnormal muscle hyperactivity, particularly in myofascial pain states. However, proposed links to broader central sensitization reversal and long-term neuroplastic changes should be interpreted as plausible hypotheses, as direct mechanistic measurements were not consistently included in the RCTs reviewed.
A major methodological limitation identified across the included trials is the lack of standardized dosimetry parameters. Considerable heterogeneity was observed in stimulation frequency (ranging from 2 to 150 Hz), pulse duration, treatment duration (single session to 60 days), and duty cycles (on/off patterns). Few studies provided a clear physiological rationale for parameter selection, and none directly compared different frequency or timing protocols within the same population.
Direct comparison of durability across chronic shoulder pain trials is limited because eligible RCT evidence is sparse and protocols are not directly comparable. Limited-session protocols may yield transient analgesia, while durability likely depends on cumulative dose, targeting precision, and integration with progressive rehabilitation. This remains a key research gap.
Considerable variability was observed in follow-up duration across trials. Postoperative brachial plexus PNS trials demonstrated immediate and short-term analgesic effects,17,18 whereas supraspinatus tendinopathy studies reported sustained improvements extending beyond three months.9,19 In contrast, most intramuscular trapezius stimulation trials assessed only immediate or short-term outcomes,20–22 limiting conclusions regarding durability.
Another relevant methodological factor concerns the use of ultrasound guidance. Trials employing ultrasound-guided electrode placement10,17,18 likely achieved greater anatomical precision, which may partly explain the magnitude and consistency of analgesic effects observed in these studies. In contrast, protocols without imaging guidance may introduce variability in target accuracy, potentially influencing reproducibility.11,14
Finally, the included populations differed according to rehabilitation stage. Postoperative trials reflect acute-phase neuromodulation, whereas tendinopathy and cervical spondylosis studies represent chronic presentations. Chronic shoulder conditions are frequently associated with central sensitization mechanisms,6,7 which may alter responsiveness to neuromodulatory interventions. Mechanistic reviews of peripheral nerve stimulation further suggest that stimulation effects may differ depending on the chronicity of nociceptive input.11,12 This distinction should be considered in protocol design and future subgroup analyses.
Although postoperative trials consistently demonstrate superiority of percutaneous PNS over sham with clinically meaningful analgesia and opioid-sparing effects,17,18 the current evidence base remains limited to a small number of RCTs and specific surgical contexts. Therefore, we classify percutaneous PNS as a promising and clinically relevant non-pharmacological option, rather than a universal standard of care.14,15 Patient-level predictors of response have not been formally established; however, candidates most likely to benefit may include individuals with higher early postoperative pain burden, higher opioid requirement/risk, and those requiring effective analgesia to facilitate early mobilization. Established risk models in postoperative pain suggest that baseline pain intensity, analgesic consumption, and psychosocial factors influence recovery trajectories.25–27 Future trials should prospectively evaluate these predictors in the context of percutaneous PNS.
Standardized reporting of stimulation parameters—including frequency (Hz), pulse width, amplitude, treatment duration, number of sessions, and on/off cycles—is essential for reproducibility in musculoskeletal rehabilitation research. The absence of consensus regarding optimal dosimetry remains one of the principal methodological drawbacks in the use of percutaneous electrotherapy modalities. Without comparative dose-response trials, it remains unclear whether low-frequency protocols (e.g., 2 Hz) produce superior segmental analgesia, or whether higher-frequency paradigms provide more sustained neuromodulatory effects.15,22
Future randomized trials should incorporate factorial or dose-comparison designs to identify optimal stimulation parameters for specific shoulder pathologies. Establishing standardized dosimetry frameworks would substantially improve clinical translation and guideline development.
Although the PICO framework was clearly defined, the included populations were clinically heterogeneous, encompassing postoperative shoulder pain, chronic subacromial pain, supraspinatus tendinopathy, upper trapezius myofascial pain, and cervical spondylosis with shoulder-related symptoms. This heterogeneity justifies the use of narrative synthesis and limits direct comparability across trials. In particular, cervical spondylosis studies may involve segmental or radicular mechanisms contributing to shoulder pain, potentially differing from purely glenohumeral or tendinopathic conditions. Although all included trials reported shoulder-related outcomes, mixed or cervicobrachial presentations may introduce variability in treatment response. Future trials should adopt more homogeneous diagnostic criteria to enhance comparability and enable quantitative synthesis.
Beyond statistical significance, clinical relevance was interpreted using established MCID thresholds. For pain intensity measured by VAS/NRS, a reduction of approximately 1.4–2.0 points is commonly considered clinically meaningful. For functional disability, MCID thresholds of approximately 10–15 points for DASH are frequently used. Postoperative PNS trials reported pain reductions that exceed typical pain MCID thresholds, and tendinopathy trials reported functional improvements consistent with clinically meaningful change.
Another methodological aspect relevant to reproducibility concerns the reporting of intervention details according to the TIDieR framework. 28 Although most included trials adequately described stimulation frequency, anatomical target, and session duration, reporting was less consistent regarding provider expertise, setting characteristics, intensity progression, tailoring strategies, and adherence monitoring. 29
Ultrasound-guided studies generally provided clearer descriptions of electrode placement and procedural precision, whereas non-guided protocols often lacked detailed information on localization methods.17,30 Furthermore, few trials explicitly described whether stimulation intensity was progressively adjusted or how treatment fidelity was monitored across sessions. Incomplete reporting of these domains may limit reproducibility and comparability across trials. Future randomized studies evaluating percutaneous peripheral nerve stimulation should adopt structured reporting consistent with TIDieR recommendations to enhance transparency, standardization, and clinical translation in musculoskeletal rehabilitation.
Certainty of evidence varied across clinical conditions according to GRADE assessment. Postoperative shoulder pain demonstrated moderate certainty, reflecting consistent direction of effect despite limited trial numbers. In contrast, evidence for supraspinatus tendinopathy was rated as low to moderate due to indirectness related to multimodal intervention designs. Certainty for nonspecific chronic shoulder pain, myofascial pain, and cervical-related presentations was low, primarily due to imprecision, short follow-up durations, and methodological heterogeneity. These ratings underscore that while the overall direction of effect favors percutaneous PNS in selected contexts, confidence in durability and generalizability remains condition-specific.
This review has several limitations. First, the search strategy was restricted to published randomized controlled trials indexed in major bibliographic databases, and grey literature sources as well as clinical trial registries were not systematically searched. In addition, several included RCTs were small, which raises concern for small-study effects, where effect sizes may be inflated compared with larger pragmatic trials. Although this approach ensured inclusion of peer-reviewed studies with complete methodological reporting suitable for formal risk-of-bias assessment, it may increase the risk of publication bias.
When restricting interpretation to trials judged as low risk of bias, confidence remains strongest for postoperative analgesia17,18 and supraspinatus tendinopathy multimodal programs.9,19 In contrast, certainty for myofascial and cervical-related conditions decreases because a larger proportion of studies in these subgroups were rated as having some concerns and had shorter follow-up, limiting durability conclusions. Overall, the direction of effects remains similar, but certainty is reduced for chronic myofascial/cervical presentations.
Second, only studies published in English were included, potentially introducing language bias. Third, heterogeneity in stimulation parameters and outcome measures precluded quantitative meta-analysis and limits direct comparison across studies. Sources of heterogeneity included differences in patient populations (postoperative, tendinopathic, myofascial, cervical-related), variation in stimulation parameters (frequency, pulse width, duration, guidance technique), diversity of comparators (sham, exercise-based rehabilitation), and variability in outcome measures and follow-up duration. These factors precluded meaningful pooling of effect sizes and justified a structured narrative synthesis approach.
Finally, although most trials reported statistically significant improvements, long-term follow-up beyond six months was limited, particularly outside the postoperative setting. Additional high-quality RCTs with extended follow-up periods are needed to determine durability of analgesic and functional effects.
Overall, the evidence synthesized in this review supports percutaneous PNS/PENS as a safe and clinically relevant intervention for shoulder pain, particularly in postoperative analgesia and chronic tendinopathy when integrated into multimodal rehabilitation programs. The benefits appear most pronounced in conditions involving deeper neural structures or segmental mechanisms. However, optimization of stimulation parameters and standardization of treatment protocols remain critical priorities for future research.
Footnotes
Acknowledgments
The authors thank the members of the Laboratory of Neuroscience, Neuromodulation and Pain Studies (LANNED/UNIFAL-MG) for their support in data screening and critical discussions during the development of this review. We also acknowledge the authors of the original studies included in this review for their contributions to the field.
Ethical approval and informed consent
Ethical approval and informed consent were not required for this study, as it is a systematic review of previously published studies and does not involve direct interaction with human participants or access to identifiable personal data.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data generated or analyzed during this study are included in this published article and its supplementary materials. Additional information is available from the corresponding author upon reasonable request.