
Abstract
Introduction
Hip osteoarthritis is a degenerative joint disease that significantly impacts quality of life. When conservative treatments fail, total hip arthroplasty becomes necessary to alleviate pain and improve mobility. Rehabilitation plays a crucial role in functional improvement after hip surgery, as it contributes to full motor recovery. However, traditional face-to-face rehabilitation can present several challenges. Telerehabilitation is an emerging approach, using e-Health tools to allow patients to perform exercises remotely. This technique could enhance accessibility, reduce costs, and increase adherence to rehabilitation programs, but it has yet to be fully investigated in terms of beneficial effects.
Materials and methods
This review was conducted following the preferred reporting items for systematic reviews and meta-analysis (PRISMA) statement guidelines. The scientific articles were identified through the PubMed, Google Scholar, Scopus and Cochrane Library databases. A qualitative assessment of the selected studies was performed using the modified Oxford quality scoring system. Five studies were included in this review. The risk of bias was evaluated using the Cochrane Collaboration tool. The protocol was registered at PROSPERO (n◦ CRD42025643872).
Results
The review found that telerehabilitation is not inferior to traditional methods in improving functional outcomes and quality of life. Challenges include methodological differences, demographic variations, and the lack of long-term data.
Conclusions
The review suggests future research should focus on long-term outcomes, including older patients, to better understand telerehabilitation effectiveness in hip replacement rehabilitation.
Keywords
Introduction
Epidemiology
Hip osteoarthritis (OA) is a degenerative disease that affects hip joint. It has been observed that in 2024 cases of OA continue to increase globally, affecting approximately 7.6% of the global population, 1 making it the seventh-ranked cause of years lived with disability (YLD) for adults aged 70 years and older. 2 Compared with 2020, cases of hip OA are projected to increase by 78,6% by 2050. 2
Pathophysiology and clinical presentation
Hip OA occurs with the progressive wear of the cartilage that lines the acetabulum of the pelvis and the head of the femur, the formation of osteophytes on the joint margins, the sclerosis of the subchondral bone and, in more advanced cases, the appearance of geodes. 3 Clinically, it presents with pain from mechanical loading, limitation of joint movements, 4 morning stiffness and, in the advanced stages, weakness of the abductor and flexor-extensor muscles of the hip.5-7
When the symptoms of hip OA become disabling and conservative treatments – such as drugs, infiltrations and physiotherapy8,9- are no longer effective, the patient's quality of life can be significantly compromised, making it necessary to proceed to a total hip arthroplasty (THA). 10
Role of surgery
The goal of surgery is to restore joint function, eliminating pain and improving mobility. 11 The main indications include constant pain, even at rest, difficulty walking, and severe limitations in daily activities. 12
Role of rehabilitation
The rehabilitation programs that follow surgery plays a fundamental role in the recovery process. 13 During this phase, specific interventions and therapeutic protocols are implemented which include therapeutic exercises, functional activities and recovery of walking. 14 Through targeted exercises, the patient learns to use the new joint correctly, improves coordination and strengthens the hip muscles, 15 minimizing the risk of complications. 16
Rationale for telerehabilitation
Telerehabilitation (TR) represents a new frontier in the field of rehabilitation,17,18 including that for hip replacement. 19 It is an approach that allows the patient to perform exercises at home, under the supervision of a physiotherapist or physician, with technological devices such as tablets, smartphones, computers and motion sensors. Thanks to video calls, 20 dedicated apps 21 and advanced technologies, 22 the physiotherapist can monitor the patient's progress, correct and customize the exercises and, in the case of synchronous systems, offer real-time support with immediate feedback. 23
This approach has the potential to improve patient adherence to the rehabilitation program. 24
In the comparison with traditional rehabilitation, TR in hip replacement management could be justified by several benefits for patients and healthcare professionals. 19 These may include greater accessibility to care, the possibility of guaranteeing continuity of treatment even in situations that would make it difficult to physically go to an outpatient service, the reduction of transport costs and less time for patients, family members and healthcare professionals. 25
Robust scientific evidence is needed to support the integration of telerehabilitation into current rehabilitation pathways, in order to demonstrate its potential to achieve clinical outcomes equivalent to traditional rehabilitation—such as recovery of mobility, reduction of pain, and improvement in quality of life—while providing a valid and innovative alternative to conventional methods and optimizing treatment processes, including reductions in both in-hospital and out-of-hospital stay times.
However, a significant gap still exists in the scientific literature regarding the efficacy and applicability of TR, especially in post-surgical rehabilitation protocols for hip arthroplasty. This gap is largely attributed to several factors: the variability in study designs, differences in technology platforms, the limited number of high-quality randomized trials, scarcity of long-term follow-up data, heterogeneity of interventions, and insufficient information on cost-effectiveness.
Although the available evidence suggests that TR can be as effective as conventional methods, significant variability in the quality and methodology of the studies has hindered the ability to draw definitive conclusions. 26
Aim of the study
The aim of this systematic review is to synthesize the available evidence on the use of telerehabilitation (TR) in post-surgical rehabilitation following hip arthroplasty, evaluating its impact on functional outcomes, health-related quality of life, patient satisfaction, and adherence to rehabilitation programs.
Materials and methods
Data sources, search strategy and study selection
This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement guidelines. 27 The protocol was registered at PROSPERO (no CRD42025643872). The scientific articles were identified through PubMed, Google Scholar, Scopus and Cochrane Library databases, using the Medical Subject Headings (MeSH) as applicable. The eligible studies were identified by using the following Boolean search syntax: “(telerehabilitation OR telemedicine OR telehealth OR “tele health” OR “tele rehabilitation” OR “tele medicine” OR eHealth OR digital OR mobile OR smartphone OR app OR virtual) AND (“hip surgery” OR “hip prothesis” OR “hip replacement” OR “hip arthroplasty”) AND (exercise OR “therapeutic exercise” OR “exercise-based rehabilitation” OR physiotherapy OR “physical therapy”)”. Afterward, the following filters were activated—text availability: full text; species: humans; languages: English. The search syntax used for the PubMed database was a mix of MeSH database and Boolean search syntax. The references of the articles were manually examined to find the more relevant publications.
The literature search was conducted from database inception to January 10, 2025, with no restrictions on publication year. Once potential articles were selected, they were further filtered based on specific criteria for inclusion or exclusion.
Inclusion and exclusion criteria
Inclusion criteria: Patients aged >18 years undergoing hip prosthesis; Randomized Control Trials (RCT); Studies using TR after primary total hip arthroplasty; Studies comparing both supervised and unsupervised TR with traditional exercise-based rehabilitation.
PICO framework: population (patients undergoing total hip arthroplasty), intervention (telerehabilitation), comparison (conventional or standard rehabilitation), and outcomes (functional recovery and related clinical measures).
Exclusion criteria: Conference abstracts, study protocols, case reports, case series; Studies describing a digital intervention delivered exclusively through telephone calls or gaming strategies to maintain consistency with our focus on technology-supported telerehabilitation; Reviews and meta-analyses; Trials on telerehabilitation for patients with hip or knee osteoarthritis or knee replacement, as the scope of this review is limited to telerehabilitation in patients following hip replacement.
Data extraction and outcome measures
Two reviewers, working in different locations, independently selected and manually examined the extracted studies to identify the eligible ones according to specific inclusion and exclusion criteria identified at the initial stage. They independently assessed each title, abstract, and full-text article. Disagreements were resolved by consensus consulting two other experienced investigators. The information was obtained from each study by including the type of intervention and population characteristics (study design, sample, outcomes and results).
Quality assessment
A qualitative assessment was performed on the selected studies using the Modified Oxford Quality Scoring System, also known as the Modified Jadad Score. 28 The Modified Jadad Score is a four-question scale that evaluates the randomization and concealment of treatment allocation groups, withdrawal and dropout rates, adherence to inclusion and exclusion criteria, and the clarity in describing statistical methods within the studies under analysis. Each aspect was independently assessed by the two investigators previously mentioned. The Modified Jadad score ranges from 0 to 5, with each question having a binary response (yes—1 point; no—0 points). 29 A higher score indicates better study quality. Studies with a Modified Jadad score of >3 points were considered high quality, those with a score of 2–3 points were considered moderate quality, and those with a score of <2 points were deemed low quality. The Modified Jadad Score has shown the best evidence for validity and reliability in quality assessment within this fiels. 26
Risk of bias assessment
The risk of bias for all included studies was evaluated based on the six domains outlined by the Cochrane Collaboration tool. 30 These six domains are (1) selection bias due to random sequence generation and allocation concealment; (2) performance bias, with blinding of participants and personnel as a possible source of bias; (3) detection bias due to blinding of the outcome assessment; (4) attrition bias, evaluating possible incomplete outcome data; (5) reporting bias due to selective outcome reporting; and (6) other bias, evaluating any important concerns about bias not covered in the other domains. Each domain was judged as “low risk of bias” (“green”), “high risk of bias” (“red”), or “unclear risk of bias” (“yellow”). This systematic review follows the Cochrane Collaboration criteria for evaluating all the studies included. 30 All reviewers were trained in using the Cochrane Collaboration tool. Finally, the authors’ judgments on each risk of bias item were presented both as percentages and as a summary across all included studies, using the Risk of Bias visualization tool. 31
Results
Identification of studies
The studies were identified through a search of four databases (Pubmed, Google Scholar, Scopus and Cochrane Library). At the end of the selection process, 4.539 articles were extracted. These articles were identified by searching for studies of likely relevance to the review. Duplicates were eliminated (n = 160). Thus, all the titles and abstracts were selected, removing review articles, meta-analyses, case reports, letters, editorials, systematic reviews and meta-analysis, cadaveric studies, conference meetings, and studies without accuracy and safety evaluations and subsequently, the full text of the remaining 47 articles was assessed to verify their eligibility. Forty-two articles were excluded because they were either not relevant to the research question or had an inappropriate study design. Finally, five research articles were included (Figure 1).
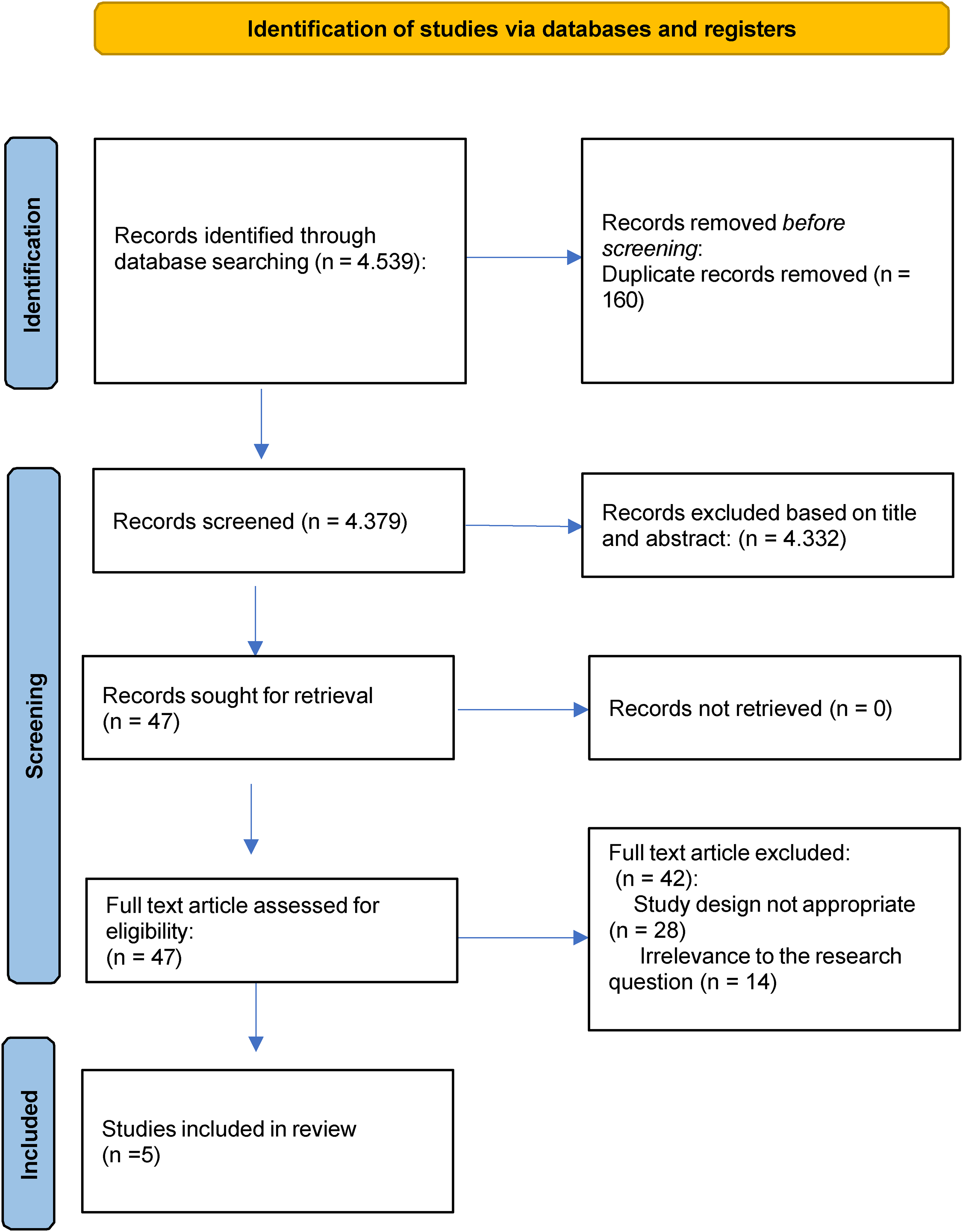
Study selection and eligibility screening flow according to PRISMA guidelines.
Characteristics of the included studies
Table 1 shows the characteristics of the included studies retrieved from the systematic review.
Summary characteristics of the selected studies.
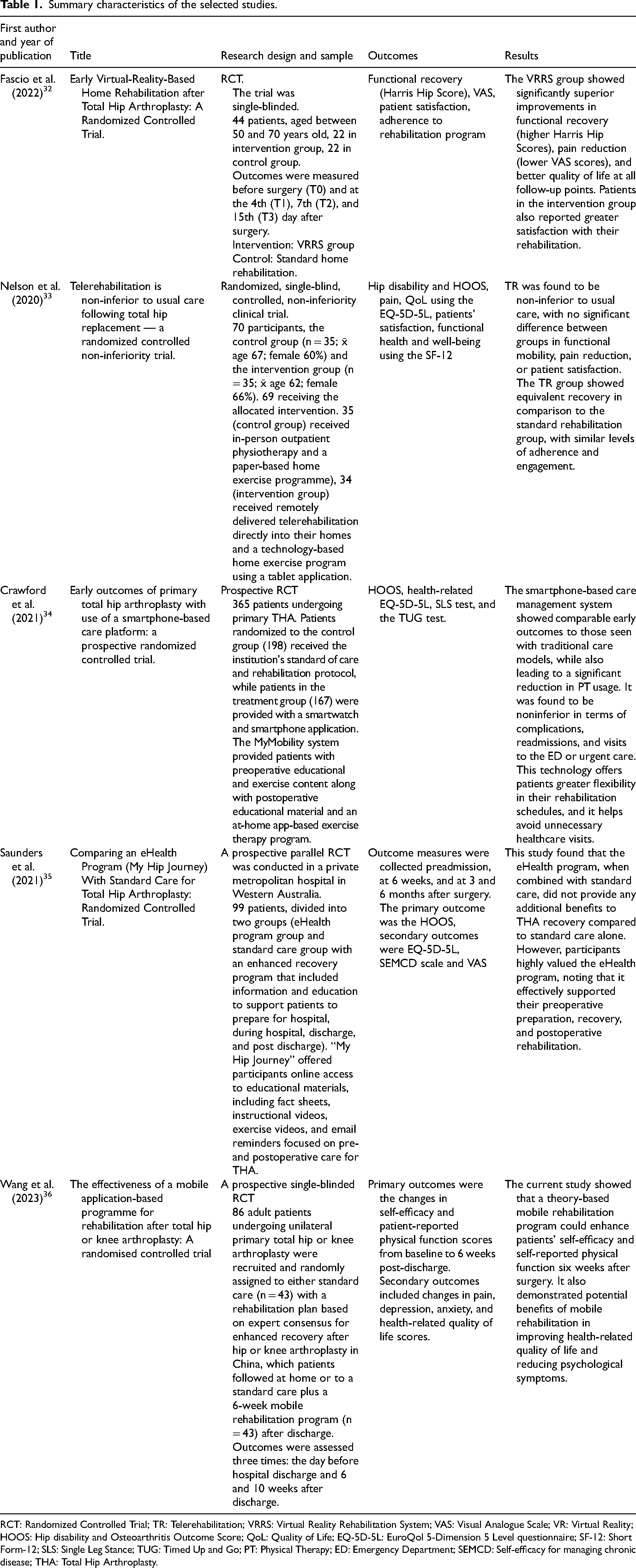
RCT: Randomized Controlled Trial; TR: Telerehabilitation; VRRS: Virtual Reality Rehabilitation System; VAS: Visual Analogue Scale; VR: Virtual Reality; HOOS: Hip disability and Osteoarthritis Outcome Score; QoL: Quality of Life; EQ-5D-5L: EuroQol 5-Dimension 5 Level questionnaire; SF-12: Short Form-12; SLS: Single Leg Stance; TUG: Timed Up and Go; PT: Physical Therapy; ED: Emergency Department; SEMCD: Self-efficacy for managing chronic disease; THA: Total Hip Arthroplasty.
Sample size, a brief summary about the research design and outcomes, as well as results were analyzed in all of the five studies. They focus on the potential benefits of TR in THA.
Assessment of methodology and quality of the studies
The methodological quality of the included studies was assessed using the Modified Jadad Score, as shown in Table 2. In this systematic review, all the studies were categorized as having moderate quality (scores 3 to 4).32–36
The modified version of Jadad quality scale.
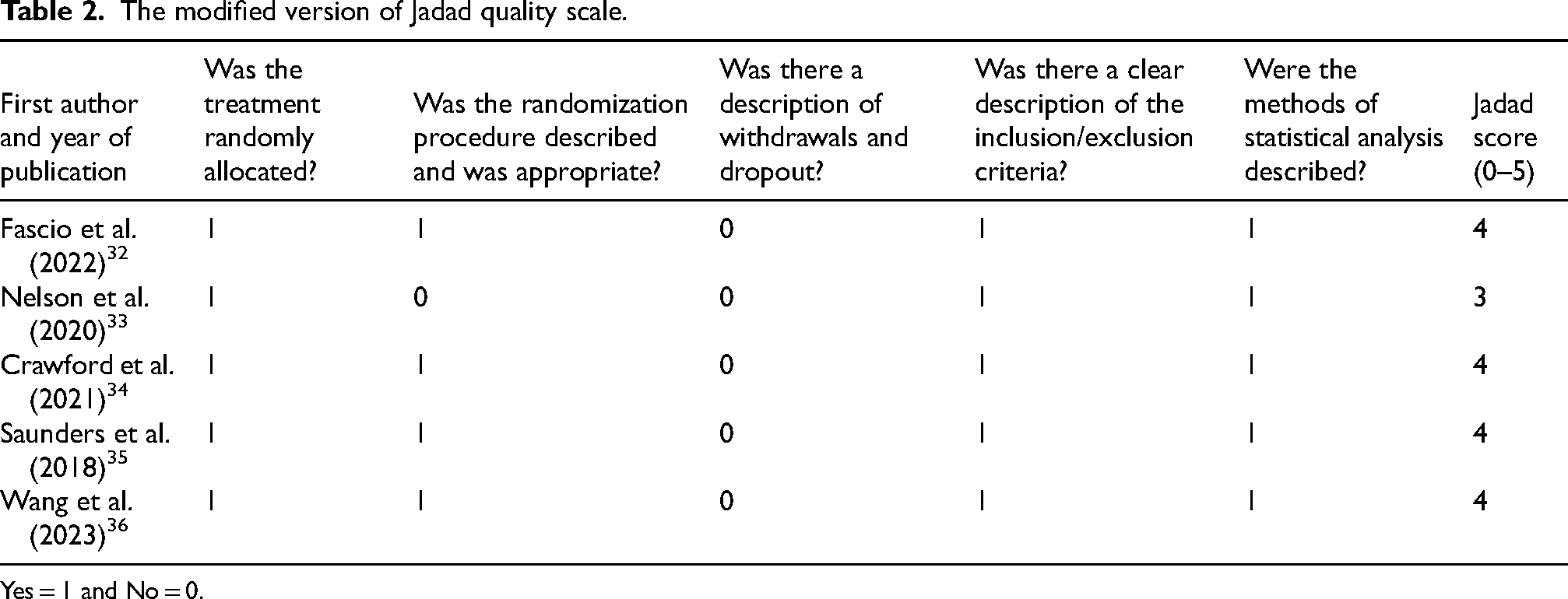
Yes = 1 and No = 0.
Evaluation of risk of bias
The risk of bias graph is reported in Figure 2. The overall level of risk of bias in all the studies selected in this systematic review showed some concerns about the deviations from the intended intervention (performance bias), the blinding of the outcome assessment (detection bias), the incomplete measurement of the outcome data (attrition bias). More specifically, 40% of the studies highlighted some concerns, 20% highlighted high risk of bias, while 40% of them had a low risk of bias. The risk of bias of the included studies was assessed independently by two reviewers, and any discrepancies were resolved through discussion or by consulting a third reviewer.
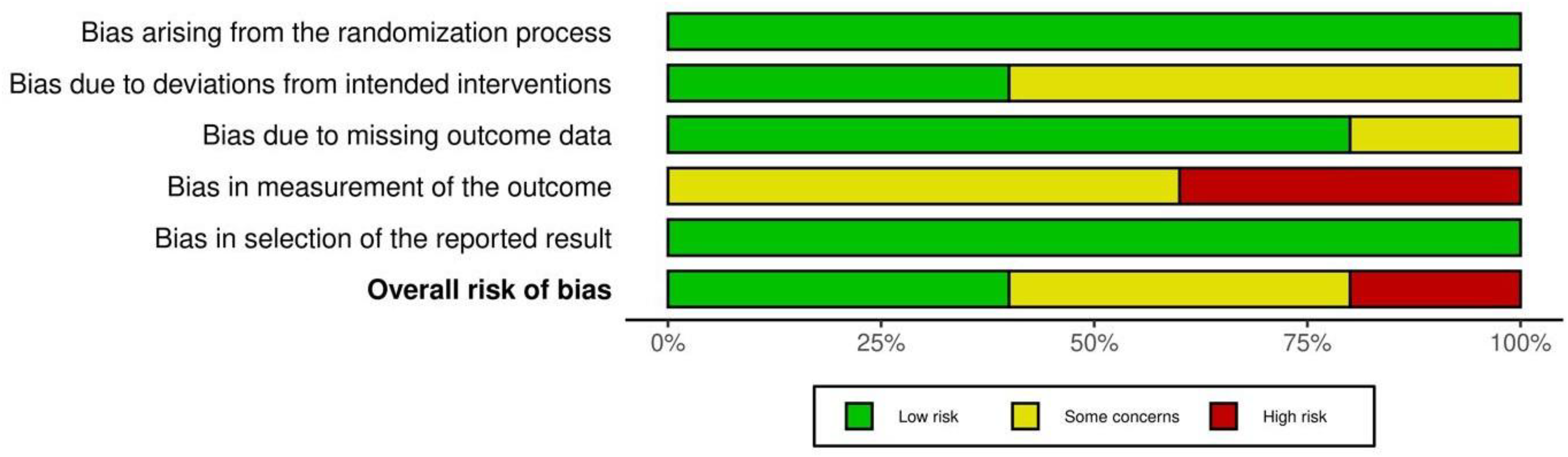
Risk of bias graph: review of the authors’ judgments about each risk of bias item presented as percentages across all the included studies.
A risk of bias summary is reported in Figure 3. It reveals that two out of the five studies presented a low risk of bias,32,33 one of them presented high risk of bias 34 and two of them presented some concerns.35,36 Conversely, two of the five studies showed a low risk of bias due to deviations from the intended intervention.32,33 Moreover, four studies had a low risk of bias in terms of missing outcome data.32,33,35,36 Two studies revealed a high risk of bias in the outcomes measurement.34,35 Lastly, all of five studies presented a low risk of bias in the selection of the reported results.32–36
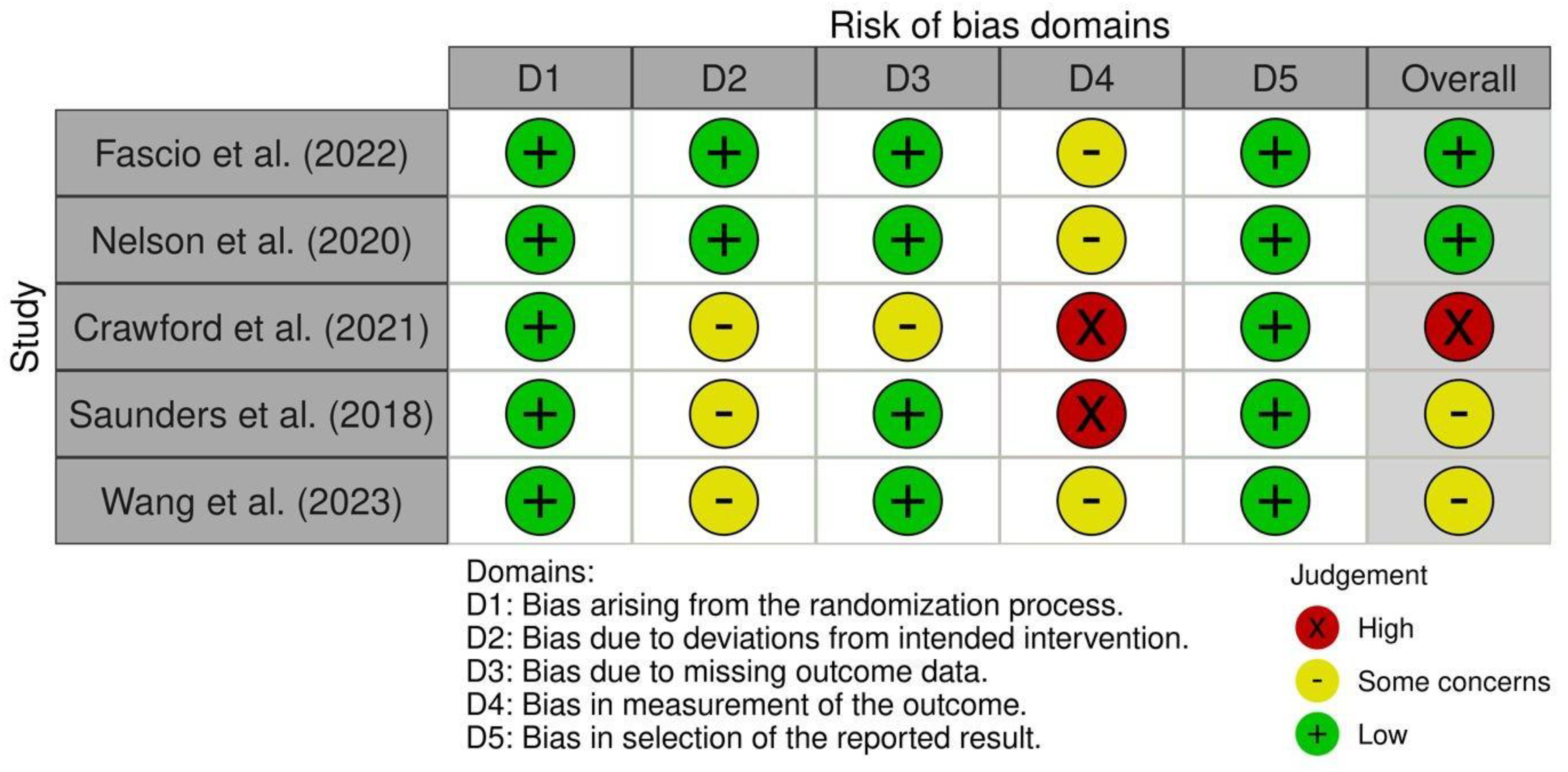
Risk of bias summary.
The risk of bias scores for each study was determined by evaluating how well each addressed key methodological areas. Fascio et al. 32 and Nelson et al. 33 showed a low risk of bias for performance bias due to their effective intervention monitoring. Crawford et al. 34 had a high risk of bias due to deviations in the intervention, while Saunders et al. 35 raised concerns about adherence to the eHealth program. For detection bias, Fascio et al., 32 Nelson et al., 33 Saunders et al. 35 and Wang et al. 36 had a low risk thanks to blinding, while Crawford et al. 34 had a high risk due to potential errors from digital platform use. Regarding attrition bias, four32,33,35,36 studies demonstrated a low risk by managing missing data well, while Crawford et al. 34 raised concerns due to participant dropout. All studies had a low risk of reporting bias as they reported all pre-specified outcomes transparently.
Discussion
This systematic review evaluates the effectiveness and applicability of TR in patients undergoing THA, examining innovative approaches such as digital platforms, virtual reality, smartphone applications and tablet-based systems. The included studies compare these methodologies with traditional in-person rehabilitation programs, with the aim of providing useful recommendations for daily clinical practice. A significant contribution that emerged is the growing role of TR in ensuring accessibility, personalization and reduction of healthcare costs, while maintaining functional outcomes comparable to or even superior to standard care.
Methodological differences and limitations
The analyzed studies presented methodological heterogeneity in various aspects, including technologies used, population and duration of follow-up.
Technologies
The use of different technologies across studies, such as advanced VRRS (an advanced telerehabilitation system providing interactive exercises with real-time feedback) by Fascio et al., 32 simpler platforms like iPads and apps used by Saunders et al. 35 and Nelson et al. 33 or smartwatch and a smartphone app (mymobility) used by Crawford et al., 34 complicates direct comparisons. Similarly, Wang et al. 36 used a mobile application-based programme for rehabilitation, which may offer advantages in patient accessibility, but its effectiveness can be influenced by the level of technological literacy.
The differences between technologies may influence patient challenge of determining a “one-size-fits-all” solution and suggests that the choice of technology should be tailored to the specific needs and preferences of the patient's population.
Population and bias
Population characteristics such as age and technological literacy may introduce biases. The younger participants (mean age 62 vs. 67 years; p = 0.03) in the study of Nelson et al., 33 who had a significantly lower mean age than the control group, could potentially be more comfortable with and more likely to adhere to digital interventions. Similarly, Saunders et al. 35 acknowledge that participants already had internet access and devices, which could affect the applicability of their findings to populations without such resources. Crawford et al. 34 report a significant difference in age between groups (p = 0.007), with a possible impact on technology adherence. These factors suggest that TR might not be equally effective or accessible for older adults or those with limited technology access. Such age-related differences may introduce confounding, potentially affecting the internal validity of the studies and limiting the generalizability of the findings to broader patient populations.
Duration of follow-up
Fascio et al. 32 evaluated outcomes at 15 days post-operatively, Nelson et al. 33 and Saunders et al. 35 included 6-month follow-up, and Crawford et al. 34 limited follow-ups to 90 days. The variation in follow-up durations between the studies, ranging from 15 days to 6 months, further complicates the ability to assess the long-term benefits of TR. Wang et al., 36 focused on short-term outcomes and did not extend follow-up beyond 6 months. The lack of long-term outcome measures in most of the studies indicates that more research is needed to understand the sustained effects of TR over time, especially as outcomes may differ significantly in the longer term.
Comparison of outcome measures
Comparison of functional and quality of life outcomes across studies indicates that TR is non-inferior to traditional rehabilitation, although it is important to note that, although improvements in functional independence and quality of life were observed in all studies, the magnitude of improvement did not consistently favor one method over the other. For example, Fascio et al. 32 found no significant differences between the VRRS group and the control group in the HOOS JR score at 15 days post-operatively (p > 0.05), nor in the FIM and Barthel index (measures of functional independence).
Saunders et al. 35 found that the eHealth My Hip Journey program (n = 50) did not differ from usual care (n = 49) in improving the HOOS, EQ-5D-5L quality of life or SEMCD score at 6 months (p > 0.05).
Nelson et al. 33 confirmed the non-inferiority of TR (iPad + app) compared to in-person physiotherapy (n = 35 per group), with non-significant differences in HOOS QOL score at 6 weeks (Δ = 2 points; 95% CI: −10 to 13; p = 0.92).
The study by Crawford et al. 34 showed a 21.4% reduction in the use of postoperative physiotherapy (p = 0.001) without compromising clinical outcomes (HOOS JR, TUG test).
The findings of Wang et al. 36 add to the growing evidence that mobile rehabilitation programs can be a valuable alternative to traditional rehabilitation methods, providing similar functional outcomes while potentially offering greater convenience for patients, suggesting that TR maintains clinical efficacy, while reducing logistical barriers (e.g., transportation).
Benefits in perceived satisfaction
The studies explored patients’ perceived satisfaction with TR through various metrics, and while the results were not directly comparable due to differences in assessment methods, general trends emerged. Three of the five study groups adopted different metrics to assess satisfaction, limiting direct comparisons but highlighting cross-sectional benefits.
Fascio et al. 32 used the Global Perceived Effect, with a significantly higher score in the VRRS group (4.76 vs. 3.96; p < 0.001) compared to control. In particular, participants perceived the exercise booklet as useful for the recovery after THA, while the experimental group considered the TR system very helpful for their post-surgery functional recovery.
Nelson et al. 33 used a health care satisfaction questionnaire (14 items) in both groups. The only difference between the groups was for the item ‘my therapy session was easy to attend’ in which the intervention group scored higher on “ease of participation": 95/100 in the teleheab group vs. 86/100 in the control (p = 0.017).
Saunders et al. 35 measured the satisfaction levels with a satisfaction survey administered electronically 6 weeks after surgery to all participants, but no statistically significant difference in the satisfaction levels between the intervention and control groups was noted. In the intervention group, an additional survey had also been admnisistered, in wich the majority felt that the “application was easy to use” (35/37, 95%). Furthermore, Wang et al. 36 evaluated patient satisfaction with their mobile application-based rehabilitation program and found positive feedback, with patients reporting high levels of satisfaction with the usability and accessibility of the mobile app.
Crawford et al. 34 did not include specific parameters for perceived satisfaction, focusing instead on adherence and clinical outcomes.
This is a limitation, as satisfaction is an important determinant of the overall success of a rehabilitation program. Future studies could benefit from incorporating more comprehensive satisfaction measures to understand how patients experience TR.
Adherence
Crawford et al. 34 state that 84.5% of patients with high mobility program adherence were able to evade supplemental physical therapy, thus showing the application's potential to assist patients with undertaking rehabilitation tasks and avoiding further interventions. Telerehabilitation patients had higher program adherence according to Nelson et al. 33 (86% vs. 74%; p = 0.048), possibly due to motivational automated prompts the system offered. These results demonstrate the capability of TR to positively influence adherence and thus to potentially improve rehabilitation outcomes in patients with limited ability to attend regular in-person rehabilitation sessions. Safety Although the studies were not primarily directed at the assessment of safety, the absence of serious adverse events related to the incorporated technologies was reported. TR interventions risk profiles were similar to standard care, thus these technologies could safely be incorporated in THA rehabilitation.
Safety
Although the studies were not primarily directed at the assessment of safety, the absence of serious adverse events related to the incorporated technologies was reported. TR interventions risk profiles were similar to standard care, thus these technologies could safely be incorporated in THA rehabilitation. It is necessary to be
cautious as most constituants are young and may not reflect older patients or those with comorbidities with potential barriers to the use of digital tools, similarly to what happens for other musculoskeletal disorders. 37 Therefore, the safety and feasibility of TR with these populations are worthy of further investigation.
Limitations and challenges
Despite the promising results, several challenges remain in the widespread implementation of TR for patients undergoing THA. One significant issue is the heterogeneity of tools and technologies used across studies, ranging from advanced virtual reality systems to simple mobile applications. This diversity complicates the establishment of standardized protocols and makes it difficult to determine the most effective technological solution for TR. Similarly, with specific reference to the comparison with traditional rehabilitation, the selected studies are heterogeneous in terms of techniques and approaches, although all are based on therapeutic exercises performed in the context of usual care.
Furthermore, the lack of long-term data remains a major limitation, as most studies focus on short-term outcomes (≤6 months). Recognizing the rehabilitation and recovery from a THA is likely to be prolonged, understanding the prolonged effects of TR on recovery is pertinent to its implementation. A lack of long-term evidence, as well as differences in methodologies, technologies, and participant characteristics, hinders the establishment of TR protocols that may be in some way universal. A further limitation is that the bulk of the studies included young, tech-savvy participants, thereby restricting the generalisability of the findings in older and more comorb,nded patients, who may also have their own barriers to the effective utilization of TR. To date, the literature has not reported serious adverse events related to TR; however, the available evidence on safety remains limited. Nonetheless, some relative and absolute contraindications to TR need to be stated in order for TR to be safely and efficiently made available to a broad variety of TR patients. Addressing these challenges will be essential in optimizing TR protocols to make them accessible, effective, and relevant for diverse patient populations. Future research should prioritize the inclusion of older adults and those with comorbidities, as well as the analysis of long-term outcomes, to achieve a more comprehensive understanding of the role and potential of TR in the context of THA.
Conclusion
In conclusion, this systematic review highlighted the growing role of TR in patients undergoing THA, demonstrating that innovative technologies such as digital platforms, virtual reality, could be useful in improving functional outcomes and quality of life. Despite methodological heterogeneity across the analyzed studies and the limited availability of long-term data, the evidence supports the non-inferiority of TR compared to traditional rehabilitation, and in some cases, it may offer additional benefits such as reduced healthcare costs and increased accessibility, while maintaining comparable clinical outcomes. Future research priorities should focus on long-term outcomes, cost-effectiveness analyses, older patient populations, and standardized intervention protocols to further clarify the effectiveness of TR in this population.
Disclaimer/Publisher's note
The statements and opinions expressed in this article are solely those of the authors and do not necessarily reflect the official position of the journal, the publisher, or the editors. The publisher and editors disclaim any responsibility for injuries or damages resulting from the use of information contained herein.
Footnotes
Abbreviations
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The original contributions presented in the study are included in the article and further inquiries can be directed to the corresponding author.