
Abstract
Background
The improvement following arthroscopic rotator cuff repair (ARCR) is associated with biopsychosocial factors, including emotional well-being, health beliefs, and patient engagement.
Objective
This prospective study aimed to investigate the relationship between musculoskeletal health literacy (MHL) and physical and psychological outcomes in patients with ARCR.
Methods
A total of 44 patients were divided into two groups: low (n = 24) and high (n = 20) MHL using the Turkish Health Literacy Scale-32. The patients received a standardized rehabilitation program composed of 30 treatment sessions (five days per week) lasting between 45 and 60 min. The primary outcomes included pain (Visual Analog Scale) and disability-function (Shoulder Pain and Disability Index and The Disabilities of the Arm, Shoulder and Hand Questionnaire). Secondary outcomes included pain catastrophizing (Pain Catastrophizing Scale-PCS), anxiety/depression (Hospital Anxiety and Depression Scale), kinesiophobia (Tampa-Scale of Kinesiophobia-TSK), and quality of life (12-Item Short-Form Health Survey). The outcomes were assessed pre- and post-treatment.
Results
Both MHL groups showed significant improvements in pain, disability, and function over time (p < 0.001), with no group-by-time interaction for physical outcomes. However, higher MHL was associated with greater improvements in PCS (p = 0.029) and TSK scores (p = 0.041), indicating significant group-by-time interactions for psychological outcomes.
Conclusion
Higher MHL was associated with improved psychological outcomes, but not physical outcomes, after ARCR. The MHL may be more strongly related to psychological adaptation rather than physical recovery. Interventions targeting MHL may have the potential to influence rehabilitation outcomes. Further randomized trials are required to assess the clinical benefits of MHL-targeted educational interventions in terms of causality.
Introduction
Health literacy refers to the mental and social skills required to access and understand printed or electronic resources related to health. 1 Individuals interpret and evaluate the information they access and communicate effectively with health professionals using qualitative and quantitative data. 2 In addition to having knowledge about healthy living, disease pathologies, factors that facilitate treatment processes, they are also capable of interacting effectively with people with different disease backgrounds.3,4
Individuals need to take greater responsibility to achieve optimal treatment outcomes and effectively utilize healthcare resources in musculoskeletal disorders.5,6 Limited musculoskeletal health literacy (MHL) could increase the burden on healthcare services by hindering access to and understanding medical information and achieving optimal treatment in patients with shoulder problems.7–9 Low levels of MHL have been reported to be associated with worse patient-reported baseline assessment results in non-traumatic shoulder pain. 8 Similarly, inadequate MHL levels have been associated with higher symptom severity and functional disability following shoulder surgery. 9 Low MHL levels could delay patients’ return to activity, work, and sports by reducing adherence to treatment instructions. 10
Although arthroscopic rotator cuff repair is an effective procedure for reducing pain and disability in shoulder patients with rotator cuff tears, healing is influenced by a wide range of psychosocial factors, including emotional well-being, health beliefs, and patient engagement, in addition to physical variables.11,12 Postoperative rehabilitation following ARCR requires adherence to a structured and progressive program, including periods of immobilization, gradual restoration of movement, and active participation in exercise-based therapy. 11 In this context, MHL may be relevant to recovery, as it could influence patients’ understanding of rehabilitation goals, adherence to prescribed exercises, and interpretation of postoperative symptoms.7–10 Patients with limited MHL may be more likely to misinterpret pain signals, develop maladaptive beliefs, and exhibit fear-avoidance behaviours, which may negatively influence rehabilitation engagement.7–10
Many patients seek online medical information following shoulder arthroscopy; however, it remains unclear whether clinical outcomes differ according to how effectively this information is understood and applied. Therefore, this study aimed to examine the associations between MHL levels and physical and psychological outcome variables in patients after ARCR. We hypothesized that higher MHL levels would be associated with better clinical outcomes.
Material and methods
This prospective, longitudinal observational study included patients treated with ARCR by a single orthopedic surgeon (HÇB) between June 2023 and May 2025. Forty-four individuals who underwent ARCR were referred to the physiotherapy clinic and evaluated pre- and post-rehabilitation by a physiotherapist (MİK) with 10 years of clinical experience. A local ethics committee approved this study. Informed consents were obtained from all participants. The study adhered to STROBE guidelines.
Patient selection
Patients aged 18 to 65 years with a confirmed diagnosis of full-thickness rotator cuff tear (<3 cm), based on magnetic resonance imaging and clinical tests, who underwent ARCR with standardized surgical techniques and were fluent in Turkish were included.13,14
Patients were excluded from the study protocol if they had a neurological or systemic inflammatory problem, comorbidities affecting shoulder function, disc herniation, partial RCT, and a history of frozen shoulder.13,14 These exclusion criteria were applied to reduce potential confounding factors that could independently influence postoperative pain, tendon healing, shoulder function, or psychological responses during rehabilitation.
Postoperative rehabilitation protocol
All patients used an immobilization sling for six weeks postoperatively and participated in a standardized supervised rehabilitation program conducted by the same physiotherapist (CK), who has 9 years of ARCR experience. The program consisted of 30 sessions (5 days/week, 45–60 min each) over six weeks, including strength training, joint mobilizations, stretching, perturbation, sensorimotor, and motor control exercises to restore shoulder neuromuscular control.15,16 A detailed rehabilitation program was reported in the previous study. 17 Patient education was integrated into the program. Patient education was delivered as a standardized component of the rehabilitation program and included verbal information regarding postoperative precautions, pain management, exercise rationale, and expected recovery progression. Educational content was not formally individualized according to health literacy level, and no structured written materials were provided. Patients were instructed to avoid additional treatments for shoulder pain during the study period.
Outcome measures
MHL was assessed at the beginning of the rehabilitation period (6th postoperative week), concurrently with baseline outcome measures. MHL was assessed using the Turkish Health Literacy Scale-32 (THLS-32), a validated instrument measuring two dimensions (health care; disease prevention and health promotion) and four information processing skills (accessing, understanding, appraising, applying) related to health information. 18 Scores range from 0 to 50, with higher scores indicating better health literacy. Categories are: insufficient (0–25), problematic-limited (>25–33), adequate (>33–42), and excellent (>42–50) health literacy.
Due to the relatively small sample size and uneven distribution across the four original categories, MHL levels were dichotomized to improve statistical stability and interpretability; however, this approach may reduce sensitivity to detect potential dose-response relationships and may result in loss of information:
Low MHL: Combined “insufficient” (0–25) and “problematic-limited” (>25–33) THLS-32 scores, High MHL: Combined “adequate” (>33–42) and “excellent” (>42–50) scores. This grouping approach is consistent with previous literature and helps address small subgroup sizes in the original four-category structure.
Demographic characteristics of the participants were recorded. Baseline assessments were performed postoperatively at the initiation of the supervised rehabilitation program (6th week after surgery). Post-treatment assessments were conducted immediately after completion of the six-week rehabilitation protocol (12th week after surgery). Visual analog scale (VAS) was used to assess pre- and post-treatment pain severity. 19 Shoulder Pain and Disability Index (SPADI) and The Disabilities of the Arm, Shoulder and Hand (DASH) Questionnaire were used to assess function.20,21 Following reliable, valid, and culturally adapted patient reported outcome measurements in terms of catastrophizing, anxiety, depression, kinesiophobia, and quality of life were also used: Pain Catastrophizing Scale (PCS), 22 Hospital Anxiety and Depression Scale (HADS), 23 Tampa-Scale of Kinesiophobia (TSK), 24 and 12-Item Short-Form Health Survey (SF-12). 25
Sample size
The variable used to estimate the sample size was the change in DASH. According to van Kampen et al., the minimal clinically important difference for DASH in patients with RCT is 12.4 points. 26 In a pilot study, the baseline DASH standard deviation was 25.92. It was determined that 44 participants were required for a prospective study with 80% power and α = 0.05 and an effect size of 0.47. Sample size calculation was based on the primary physical outcome (DASH). However, psychological outcomes were secondary and may be underpowered to detect small to moderate effects. Therefore, findings related to psychological measures should be interpreted cautiously.
Statistical analysis
Statistical Package for the Social Sciences 22.0 program for Windows was used. Counts and proportions were used for descriptive statistics of continuous and categorical data, respectively. Baseline demographic comparisons among MHL groups were performed using independent samples t-test or Mann-Whitney U test based on normal distributions, and χ2 was used for categorical variables. Post-treatment within-group comparisons were performed using paired samples t-tests or Wilcoxon test, while pre-treatment between-group clinical comparisons were conducted using independent samples t-tests or Mann-Whitney U tests, depending on the normality of the distribution. To evaluate changes over time and differences between MHL groups, a 2 (time: pre-treatment vs. post-treatment) × 2 (groups: Low MHL vs High MHL) repeated measures ANOVA in mixed design with Bonferroni post-hoc test was conducted for each outcome. The partial eta-squared (η2p) was calculated to classify effect size based on previously reported cut-offs. 27 The level of significance was set at p < 0.05. Due to the limited sample size, adjusted models including covariates such as sex and baseline psychological scores were not performed, as this could result in model overfitting and unstable estimates. Therefore, results should be interpreted with caution regarding potential confounding effects.
Results
The study population included 44 patients divided into two MHL groups: low MHL (n = 24; mean age 54.71 ± 10.69 years; 19 female; 27.59 ± 4.16 kg/m2 BMI) and high MHL (n = 20; mean age 52.40 ± 9.63 years; 11 female; 25.48 ± 6.78 kg/m2 BMI). Demographics and participant characteristics are presented in Table 1. Groups were similar in terms of participant characteristics, except for sex distribution (p = 0.044), with a higher proportion of females in the low MHL group.
Participant characteristics.
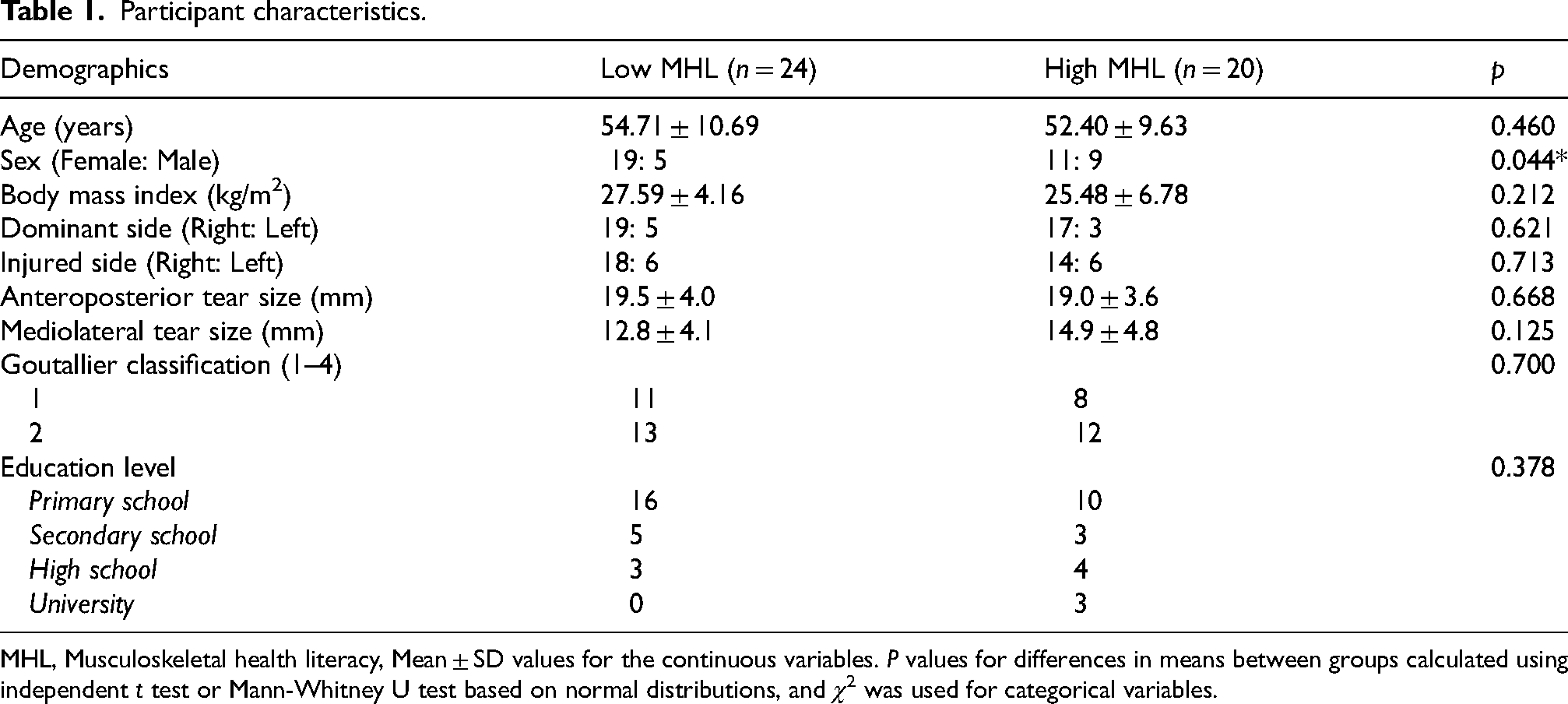
MHL, Musculoskeletal health literacy, Mean ± SD values for the continuous variables. P values for differences in means between groups calculated using independent t test or Mann-Whitney U test based on normal distributions, and χ2 was used for categorical variables.
Primary outcomes
Both low and high MHL groups demonstrated significant improvements over time in all primary physical outcomes, including pain (VAS rest, activity, night), DASH, and SPADI scores (p1 < 0.001 for all within-group comparisons). The baseline comparison of the groups revealed no statistically significant differences (p2 > 0.05). Significant main effects of time were observed across all physical measures (p3 < 0.001, η2p ranging from 0.45 to 0.87), indicating overall improvement regardless of MHL level (Table 2). No significant group-by-time interactions were found for any physical outcomes (p3 > 0.05), suggesting that the extent of improvement did not differ between low and high MHL groups.
Comparison of the physical outcome measurements between and within the groups.
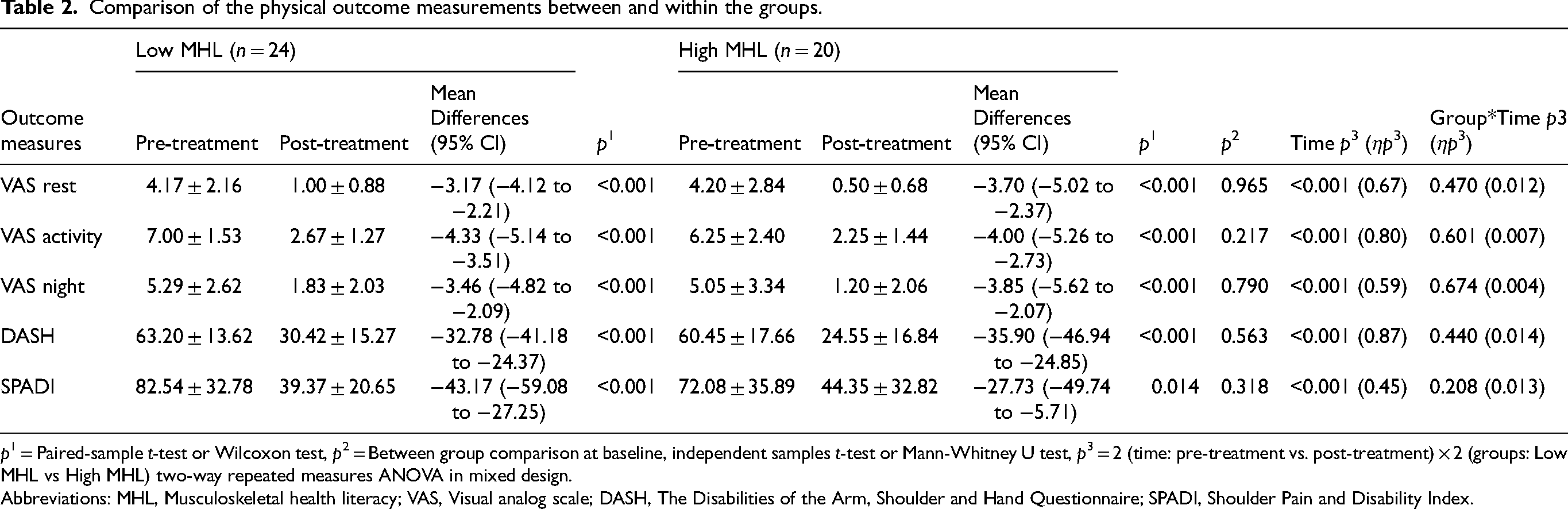
p1 = Paired-sample t-test or Wilcoxon test, p2 = Between group comparison at baseline, independent samples t-test or Mann-Whitney U test, p3 = 2 (time: pre-treatment vs. post-treatment) × 2 (groups: Low MHL vs High MHL) two-way repeated measures ANOVA in mixed design.
Abbreviations: MHL, Musculoskeletal health literacy; VAS, Visual analog scale; DASH, The Disabilities of the Arm, Shoulder and Hand Questionnaire; SPADI, Shoulder Pain and Disability Index.
Secondary outcomes
MHL groups with similar pre-treatment baseline values (p2 = 0.857) demonstrated significant improvements in PCS scores following treatment (low MHL: p1 = 0.008; high MHL: p1 < 0.001). A significant group-by-time interaction was detected (p3 = 0.029, η2p = 0.108), with the high MHL group exhibiting a greater improvement in catastrophizing compared to the low MHL group (Table 3, Figure 1).
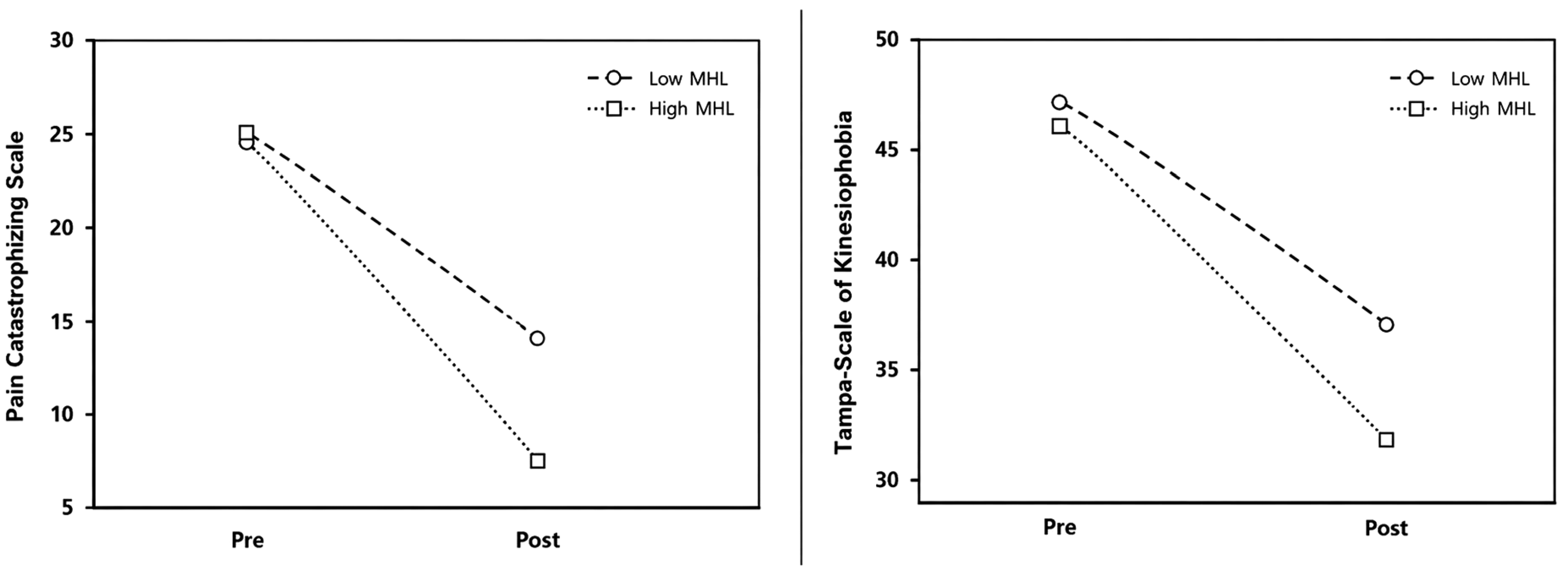
The changes in pain catastrophizing and kinesiophobia in terms of time-dependent variation and group*time interactions.
Comparison of the psychological outcome measurements between and within the groups.
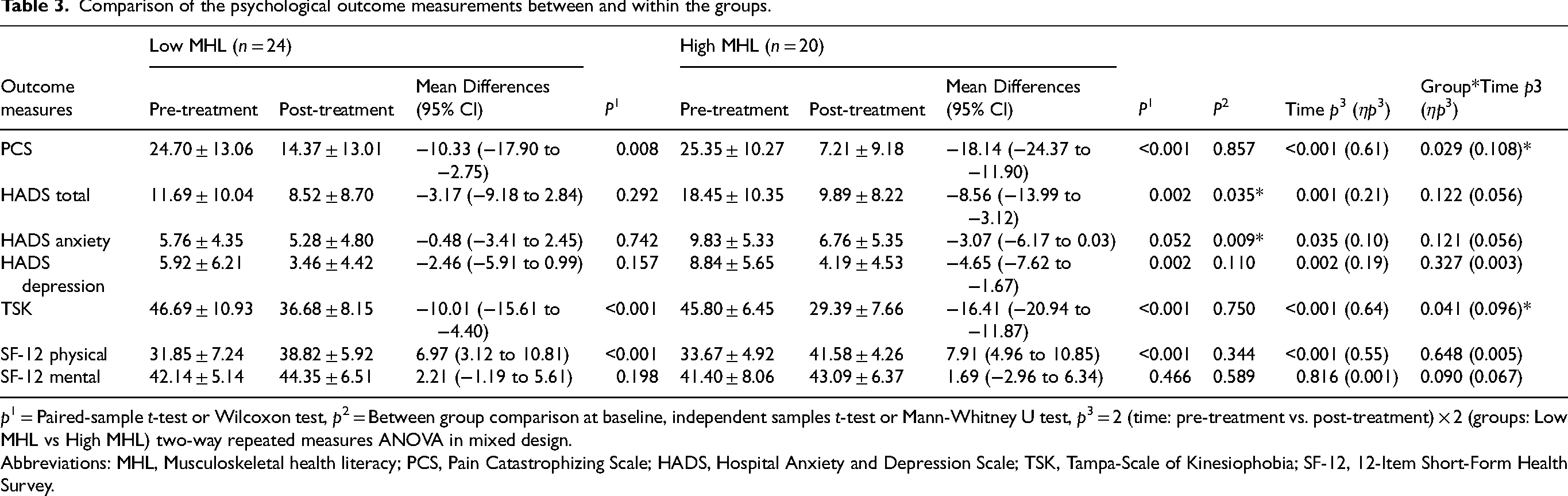
p1 = Paired-sample t-test or Wilcoxon test, p2 = Between group comparison at baseline, independent samples t-test or Mann-Whitney U test, p3 = 2 (time: pre-treatment vs. post-treatment) × 2 (groups: Low MHL vs High MHL) two-way repeated measures ANOVA in mixed design.
Abbreviations: MHL, Musculoskeletal health literacy; PCS, Pain Catastrophizing Scale; HADS, Hospital Anxiety and Depression Scale; TSK, Tampa-Scale of Kinesiophobia; SF-12, 12-Item Short-Form Health Survey.
In addition to the difference in baseline HADS total (p2 = 0.035) and HADS anxiety (p2 = 0.009) scores, the high MHL group demonstrated significant improvement in total HADS scores (p1 = 0.002), primarily due to improvements in depression subscale scores (p1 = 0.002). The low MHL group did not show significant changes in HADS total or subscale scores (p1 > 0.05). No significant group-by-time interactions were found for HADS measures (p3 > 0.05, Table 3). Baseline differences should be considered when interpreting between-group comparisons.
MHL groups with similar pre-treatment baseline values (p2 = 0.750) demonstrated significant improvements in TSK scores following treatment (p1 < 0.001 for both). A significant group-by-time interaction (p3 = 0.041, η2p = 0.096) indicated that the high MHL group achieved greater improvements in kinesiophobia compared to the low MHL group (Table 3, Figure 1).
Both groups with similar pre-treatment baseline values (p2 = 0.344–0.589) demonstrated significant improvements in SF-12 physical component scores following treatment (p1 < 0.001). No significant changes were observed in SF-12 mental component scores within or between groups (p1 > 0.05 for both). No significant group-by-time interactions were identified for either SF-12 component (p3 > 0.05 for both).
Discussion
The aim of this prospective study was to examine the associations between MHL levels and both physical and psychological outcomes in patients following ARCR. While both low and high MHL groups showed significant improvements in pain, disability, and physical function following a standardized rehabilitation program, MHL level was not associated with the physical outcomes. However, higher MHL was associated with greater improvements in psychological outcomes, specifically pain catastrophizing and kinesiophobia, both of which are regarded within literature as indicators of poor rehabilitation adherence and long-term outcomes. These findings suggest that MHL may be associated with differences in maladaptive psychological responses after ARCR. To the best of our knowledge, this is the first study to specifically demonstrate that higher MHL is associated with reduced pain catastrophizing and kinesiophobia in patients after ARCR.
Kim et al. conducted a review of the literature and identified a lack of studies in the field of orthopaedic surgery using appropriate designs and validated measures of health literacy. 28 They stated that the relationship between health literacy and the outcomes of orthopaedic patients has yet to be fully explained. 28 To the best of our knowledge, the relationship between MHL, postoperative catastrophizing, and kinesiophobia have not been examined in patients with ARCR. Although previous studies have indicated an association between limited MHL and suboptimal preoperative symptoms, as well as diminished comprehension of postoperative care instructions,7,9,29 none have specifically examined its relationship with these significant psychological variables. The present study addresses this gap in the literature by demonstrating that MHL was associated with cognitive-emotional domains, such as pain catastrophizing and fear-avoidance beliefs, rather than directly influencing pain intensity or functional recovery following surgery.
It is suggested that MHL should be considered in the treatment of chronic pain and its associated maladaptive thoughts. Miller-Matero et al. conducted a study to examine the relationship between health literacy, pain and psychological functioning. 30 They found that individuals with higher health literacy levels were more likely to demonstrate reduced depressive symptoms and increased pain acceptance following the intervention, compared to those with lower levels. Moreover, individuals with lower health literacy may not benefit as much from standard psychological interventions for symptom management. 30 A similar relationship between health literacy, pain catastrophizing, and clinical outcomes has been demonstrated in cases of chronic pelvic pain, 31 chronic low back pain 32 etc. Patients often experience a long and painful period after arthroscopy. This period is characterized by decreased mental well-being, decreased range of motion, deterioration in daily physical activities, and negative thoughts.31,32 Therefore, tackling maladaptive thoughts could be a major predictor of postoperative outcomes after ARCR.
Gruson et al. 33 and Lans et al.34,35 reported that health literacy has multidimensional effects, including coping mechanisms and behavioural patterns developed during the disease process. According to the results of the present study, the association of a high MHL level with better pain catastrophizing scores could be explained by the patient's possibly better coping skills, better adherence to treatment guidelines, and better psychological adaptation to surgical and rehabilitation processes. It has been reported that interventions such as cognitive-behavioural approaches and pain neuroscience education could be effective against psychological parameters such as pain catastrophizing and kinesiophobia in post-ARCR rehabilitation processes.36–39 Pain neuroscience training targets maladaptive thoughts related to pain neurophysiology and beliefs about pain, while MHL provides the opportunity to have a broad understanding of the whole prognosis, including pre-disease.28,34,36 Integrating MHL assessment into the assessment and treatment phases may help identify patients who have the potential to obtain low scores in terms of psychological variables in the post-ARCR rehabilitation period. However, research is required to determine whether modifying MHL leads to improved postoperative psychological outcomes.
Catastrophizing and kinesiophobia are cognitive-emotional factors that could potentially limit the efficacy of rehabilitation by sustaining fear-avoidance behaviours and negative pain perceptions. Patients with higher MHL appear to be better able to comprehend their diagnosis, surgical process, and rehabilitation objectives, facilitating adaptive coping and reducing fear-driven behaviours.28,33 Bittencourt et al. reported that patients with low health literacy exhibited higher levels of pain severity compared to other groups of patients with musculoskeletal pain. The group demonstrating adequate health literacy exhibited a lower level of kinesiophobia in comparison with their controls. 40 It has been demonstrated that increasing the health literacy of patients with low literacy is associated with a decrease in kinesiophobia. 41 Keessen et al. reported that patients with higher levels of kinesiophobia frequently lack comprehension of medical information and misinterpret body signals. This has been associated with poor health literacy and low educational level. 42 Huang et al. explained the association between high health literacy and low kinesiophobia with better access to and understanding of disease-related information and better post-operative rehabilitation compliance. 43 In accordance with literature, the present findings provide an in-depth perspective on the level of health literacy that may be associated with improving pain catastrophizing and kinesiophobia in patients following ARCR. However, given the number of outcomes and statistical comparisons performed, the possibility of type I error cannot be excluded. The observed significant interactions for PCS and TSK should therefore be interpreted cautiously, particularly as these were secondary outcomes and the study may have been underpowered to detect smaller effects. Our findings may partly reflect pre-existing psychosocial differences rather than MHL level.
Patients with limited health literacy may experience difficulties accessing and appropriately acting on medical information, thereby putting them at increased risk of unfavorable clinical outcomes. 7 Puzzitiello et al. proposed that patients with shoulder arthroplasty often have limited health literacy, which is associated with increased preoperative severity of symptoms and disability. 9 However, this study was in retrospective design and did not include the effect of MHL level on clinical outcomes following rehabilitation. Grison et al. found that patients with limited MHL demonstrated worse patient-reported outcomes at baseline compared to those with adequate MHL in the setting of non-traumatic shoulder pain. 8 We examined the associations between MHL levels and clinical outcomes in ARCR, a topic which has not been the focus of the studies mentioned. While our findings are in line with prior research, they enhance our understanding of the association between health literacy and clinical outcomes. The findings of this study suggest that intervening in adjustable factors may positively impact clinical outcomes. This provides a noteworthy contribution to both health literacy and health behavior change literature.
In our study, we found no difference in physical measurement variables when comparing them according to the MHL levels of patients. This could be explained by the fact that physical variables are less patient-dependent than psychosocial variables, and the application of standardized rehabilitation programs and the integrity of surgical repair. However, variables such as pain catastrophizing and kinesiophobia are directly associated with patients’ perceptions, understanding and fear-avoidance behaviors related to pain and movement.28,33 Patients with a high MHL may find it easier to cooperate with the treatment process by understanding the treatment expectations applied to them and interpreting medical information.
Limitations of the study
The results should be read carefully, as the relatively small sample size in our study may limit the generalizability of the findings, especially in terms of psychological variables. Psychological outcomes were secondary and the study may have been underpowered to detect small-to-moderate effects. Sex distribution differed significantly between groups, with a higher proportion of females in the low MHL group, which may have influenced psychological outcomes, as sex-related differences in pain perception and coping strategies have been reported. In addition, baseline differences in HADS scores suggest that pre-existing psychological status may have contributed to observed changes. Therefore, the associations between MHL and psychological outcomes should be interpreted with caution. Another limitation is the lack of longitudinal assessment of changes in MHL levels over time. Given the observational design, causal inferences could not be drawn from these findings. In addition, as the results were evaluated during the early rehabilitation period (6–12 weeks postoperatively), and ARCR recovery is a long-term process, future studies should include medium- and long-term follow-ups. Furthermore, dichotomization of MHL may have resulted in loss of information and limited the ability to explore dose-response relationships. Future studies using adjusted models (e.g., ANCOVA or mixed-effects models) are needed to better account for potential confounding variables. Sensitivity analyses using alternative categorizations or continuous MHL scores were not performed due to sample size limitations. In addition, biological and individual factors such as genetic predisposition, tissue healing capacity, and pain sensitivity were not evaluated and may also influence postoperative recovery. Finally, since this is a single-center study, it is recommended that the external validity of the results be tested.
Conclusion
In conclusion, higher MHL levels were associated with better improvement in pain catastrophizing and kinesiophobia scores in ARCR patients. However, physical measurement parameters such as pain and disability were not found to be associated. The MHL level may be more strongly related to psychological adaptation rather than physical recovery. Interventions targeting MHL may be relevant in rehabilitation processes; however, further randomized controlled studies are required to determine causal effects. Our findings may be important for clinicians working in shoulder rehabilitation, as they highlight the importance of MHL levels.
Supplemental Material
sj-docx-1-bmr-10.1177_10538127261463354 - Supplemental material for Associations between musculoskeletal health literacy and changes in pain catastrophizing and kinesiophobia after arthroscopic rotator cuff repair: A prospective study
Supplemental material, sj-docx-1-bmr-10.1177_10538127261463354 for Associations between musculoskeletal health literacy and changes in pain catastrophizing and kinesiophobia after arthroscopic rotator cuff repair: A prospective study by Caner Kararti, Fatih Ozyurt, Muhammed İhsan Kodak, Hakki Çağdaş, İsmail Özsoy, Gülşah Özsoy and Abdulhamit Tayfur in Journal of Back and Musculoskeletal Rehabilitation
Footnotes
List of abbreviations
Acknowledgements
Not applicable.
Ethics approval and consent to participate
A local ethics committee approved this study. Informed consents were obtained from all participants.
Author contributions
CK: Writing, review, editing, supervision, methodology, treatment program, analysis, conceptualization. FÖ: Writing, review, editing, methodology, analysis, conceptualization. MİK: Writing, review, editing, supervision, methodology, assessment, analysis, conceptualization. HÇB: Writing, review, editing, supervision, methodology, diagnosis, analysis, conceptualization. İÖ: Writing, review, editing, supervision, methodology, analysis, conceptualization. GÖ: Writing, review, editing, supervision, methodology, analysis, conceptualization. AT: Writing, review, editing, supervision, methodology, analysis, conceptualization.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was approved by Selçuk University Medical Faculty Clinical Research Ethics Committee (2023/602).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.