
Abstract
Background
Low back pain is a global health challenge that requires constant progress to aid its management. Currently, artificial intelligence, as a major technological shift, has entered medicine to guide and improve management, and it is slowly being used for low back pain. With the growing number of studies, there is a lack of a summary of them.
Objective
The objective of this study is to investigate the effectiveness of artificial intelligence-based interventions in improving pain and functional outcomes among adults with low back pain when compared to standard interventions.
Methods
A comprehensive search of PubMed, Scopus, and Web of Science was conducted. Intervention groups received artificial intelligence-based interventions, while control groups received standard interventions for low back pain. After data extraction, assessment of risk of bias was done, and then a meta-analysis was performed.
Results
Five studies met the inclusion criteria and were included in the systematic review, and four of them in the meta-analysis. Artificial intelligence-based interventions demonstrated lower pain scores (p = 0.001) and lower disability scores (p = 0.02) at endpoints than controls. Review of the studies revealed either significant or no improvement in the quality of recovery and psychological factors between the groups.
Conclusion
Based on the existing evidence, artificial intelligence-guided interventions, when compared to standard interventions, may improve pain and disability in adults with low back pain. But further research is necessary to establish its clinical relevance and future use.
Introduction
Lower back pain (LBP) is described as the pain between the lower edge of the ribs and the buttocks that can last for a short term (acute) or a long term (chronic). It can be caused by several factors, such as medical conditions, spinal problems, or pain radiating from another part of the body. LBP has been reported to have affected nearly 619 million people globally in 2020, and it is estimated that the number of cases will increase to 843 million cases by 2050. 1 LBP can affect any age group and is driven largely by population expansion and ageing; it is now the leading cause of disability worldwide, affecting quality of life and work productivity. This makes LBP a global health issue that requires constant progress in its management to reduce its burden. We have seen major evolutionary shifts in the management of LBP, such as advising patients to remain active rather than having bed rest, emphasis on non-pharmacological interventions, judicious use of medications, and advancements in interventional techniques. It is important to use these different treatment modalities on an evidence-based basis to provide a patient-centered care. 2
Driven by breakthroughs, Artificial Intelligence (AI) is the current foundation that has surged to shift science and technology. In the field of medicine, it is improving human expertise across diagnosis, treatment, and research, leading to increased efficiency and personalized care. In LBP, AI has been used to guide exercise therapy through real-time feedback, tailor rehabilitation intensity or content based on user progress, analyze biomechanical or kinematic data for posture correction, and predict treatment response or risk of chronicity. 3 Despite a growing number of studies, no comprehensive synthesis currently summarizes the effectiveness of AI-based interventions for LBP. Existing reviews often combine AI with general digital health or focus only on diagnostic applications, but not on treatment outcomes. There is a heterogeneity in the AI methods utilized and the clinical endpoints that need to be evaluated, making it unclear which approaches are truly effective. A systematic review with meta-analysis is needed to quantify the effectiveness of these AI-based interventions for LBP and compare them with the existing conventional treatment approaches. The objective of this review is to investigate the effectiveness of AI-based interventions in improving pain and functional outcomes among adults with LBP compared with standard or non-AI management.
Materials and methods
We followed the 2020 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement and the methodological guidance outlined in the Cochrane Handbook for Systematic Reviews of Interventions (version 6.5, 2024).4,5 Additionally, our protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the identifier CRD420251174515.
Inclusion and exclusion criteria
Eligibility was defined using this eligibility framework:
Population: Adults (≥ 18 years) with acute, subacute, or chronic LBP. Intervention: AI-based therapeutic or rehabilitative systems (machine-learning or deep-learning algorithms) used for treatment delivery, personalization, or feedback (e.g., AI-guided exercise programs, adaptive telerehabilitation, or self-management applications). Comparator: Conventional physiotherapy, standard care, or non-AI digital interventions. Outcome: LBP treatment outcomes. Studies focused solely on diagnostic or prognostic applications of AI were not eligible. Study design: Randomized controlled trials (RCTs). Notably, trial outcomes were not used to determine eligibility for included trials.
6
Non-randomized, quasi-randomized, observational, or single-arm non-comparative studies and protocols without extractable outcome data were excluded.
Literature search and study selection
Three biomedical databases, PubMed, Scopus, and Web of Science, were systematically searched through October 16, 2025, with no language, regional, or publication date restrictions. Search terms combined MeSH and free-text keywords for “Lower Back Pain” AND “Artificial Intelligence.” The complete search syntax for each database is presented in Supplementary Material 1.
All retrieved records were merged and uploaded into Rayyan, a validated systematic review software used for screening. 7 Duplicate records were identified and removed using Rayyan's built-in AI tool. The remaining records were then screened. Screening was carried out in two stages: first, titles and abstracts were reviewed to exclude irrelevant papers; second, full texts of potentially eligible studies were assessed. Each record was initially screened by one reviewer, and the results were cross-checked by an independent reviewer, who made the final decision. Disagreements were resolved through consensus. Studies that did not meet the predefined population or intervention criteria were excluded.
Data extraction
Extraction process
For each included study, detailed data were extracted using a standardized, pre-designed Google spreadsheet and organized into three structured sheets:
Study characteristics summary: Contained the basic methodological information of each RCT, including study ID, aim/objective, country of origin, design, setting, sample size, type of AI application, intervention protocol, inclusion and exclusion criteria, primary and secondary outcomes, follow-up points, and reported conflicts of interest. Baseline characteristics and outcome findings: Presented population and arm level data, such as group allocation, number of participants, mean age and BMI, proportion of female participants, baseline pain duration, baseline disability, and pain intensity, and summarized primary and secondary outcome findings. Risk of bias domain assessment: Recorded reviewers’ decisions for each bias domain across studies, with justifications for all ratings.
Extraction notes
Given the fast-paced, commercially driven nature of AI development in healthcare, we identified funding sources and conflicts of interest as key domains for extraction. 8 Each study was examined for disclosures related to financial sponsorship, industry involvement, or author affiliations with companies developing or promoting AI technologies. These details were systematically recorded to help interpret potential bias and contextualize findings.
For continuous variables, means and standard deviations (SDs) were extracted whenever available. When studies reported medians and interquartile ranges (IQRs), validated statistical methods were used to estimate corresponding means and SDs to maintain consistency across datasets. 9
Primary and secondary outcomes
The primary outcomes were pain intensity and LBP-related functional disability. These outcomes were chosen based on their clinical importance and relevance to LBP research and practice.10,11 For example, the NIH Research Task Force on Chronic LBP identifies both as “essential to measure” and recommends reporting them in all studies on chronic back pain. 12 Together, pain intensity and functional disability reflect both the subjective experience of pain and its impact on daily life.
Secondary outcomes included quality of life (QoL) and psychological factors such as kinesiophobia, pain catastrophizing, and self-efficacy. Both disease-specific and general health-related QoL measures were considered. Psychological factors such as fear of movement (kinesiophobia), catastrophic thinking about pain, and confidence in managing pain (self-efficacy) represent important dimensions of patient coping and are key targets for AI-driven educational or exercise interventions. 13
Outcome measures
Pain intensity was measured using a simple Numeric Pain Rating Scale (NPRS).14,15 On this scale, participants were asked to choose a number from 0 to 10 that best described the pain they felt, with 0 meaning “no pain” and 10 meaning “the worst pain imaginable.” The NPRS can be completed by phone, interview, or self-administered as a short questionnaire. This tool is widely used in pain studies and is known to be reliable and accurate for measuring changes in pain levels. All pain scores in the included studies were recorded or converted to the same 0–10 format so results could be compared consistently in the analysis.
Disability due to LBP was measured using the Roland–Morris Disability Questionnaire (RMDQ). 16 It includes 24 simple statements describing common daily activities affected by back pain. Participants mark each statement that applies to them on that day. The total score ranges from 0 (no disability) to 24 (maximum disability), with higher scores showing greater limitation in movement or daily tasks. The RMDQ is a reliable and valid tool widely used in LBP research. 17
QoL measurements had some inconsistencies in measurement tools across studies. Researchers utilized the Short Form-12 (SF-12), the EuroQol-5 Dimension (EQ-5D), its five-level version (EQ-5D-5L), and the EuroQol visual analog scales (EQ-VAS) to measure the general health-related QoL.
Important psychological factors for this review were understudied across the included research. Kinesiophobia was reported in only two studies using the Tampa Scale of Kinesiophobia (TSK), while another study assessed a related outcome, fear-avoidant beliefs, using the Fear-Avoidance Beliefs Questionnaire (FABQ). Pain catastrophizing was examined in only one study using the Pain Catastrophizing Scale (PCS). Self-efficacy was also reported by one study using the Pain Self-Efficacy Questionnaire (PSEQ).
Assessment of risk of bias in included studies
Two independent reviewers assessed the methodological quality of all included RCTs using the Cochrane Risk of Bias (ROB) tool. 18 This approach examines potential bias across seven major domains, including how the random sequence was generated, whether allocation was properly concealed, and the degree to which participants, investigators, and outcome assessors were blinded. It also considers how incomplete data were managed, whether outcomes were selectively reported, and any additional sources of bias that could affect validity. Each study was carefully reviewed and assigned a risk rating (low, high, or unclear) for each domain based on the clarity and completeness of its reported methodology.
Evidence synthesis and statistical analysis
For the primary outcomes (pain intensity and disability), sufficient data consistency across studies (≥3 using the same measurement scale) allowed for quantitative meta-analytic synthesis. Meta-analysis was performed using Review Manager (RevMan, version 5.4; The Cochrane Collaboration). Pooled analyses were conducted under a random-effects model (DerSimonian–Laird method) to account for potential differences in study design, participant characteristics, and intervention protocols. For continuous outcomes, results were expressed as mean differences (MDs) with corresponding 95% confidence intervals (CIs).
To evaluate the robustness of pooled results and identify potential sources of heterogeneity, sensitivity analyses were conducted by sequentially excluding each study from the meta-analysis. This leave-one-out approach helped determine whether any single study disproportionately influenced the overall pooled effect or altered the direction of results. Stability of findings following exclusion was interpreted as evidence of reliable and consistent estimates.
Due to variation in measurement tools and limited reporting of secondary outcomes, these findings were synthesized narratively and summarized in tabular form.
Assessment of heterogeneity and publication bias
Statistical heterogeneity among studies was assessed using the I2 statistic and the Chi-square (χ2) test, following the recommendations of the Cochrane Handbook for Systematic Reviews of Interventions (Chapter 9). 5 An I2 value of 0–30% was interpreted as low heterogeneity, 30–50% as moderate, 50–75% as substantial, and 75–100% as considerable heterogeneity. A p-value < 0.10 from the χ2 test was considered statistically significant for heterogeneity.
Because fewer than ten studies were included, publication bias was not assessed statistically or visually. According to current methodological standards, at least ten studies are required to ensure adequate power for detecting asymmetry and small-study effects. 19
Results
Search results
Our comprehensive database search yielded a total of 177 records (Figure 1). After removing 22 duplicate entries, 155 unique studies were retained for screening. Following the title and abstract review, 126 records were excluded for not meeting the inclusion criteria. The full texts of the remaining 29 articles were then examined in detail. Of these, 19 reports were excluded for the following reasons: single-arm (non-comparative) design,20,21 different research focus (e.g., use of AI for predicting treatment response, adherence, or recurrence of pain),22–25 or not reporting LBP outcomes separately (e.g., studies combining LBP with neck or shoulder pain).26,27 We also excluded this trial, 28 which included AI in both treatment arms, which neglects our intervention and control structure in the PICOS model. A notable exclusion is this protocol for an RCT, which will be relevant when completed. 29
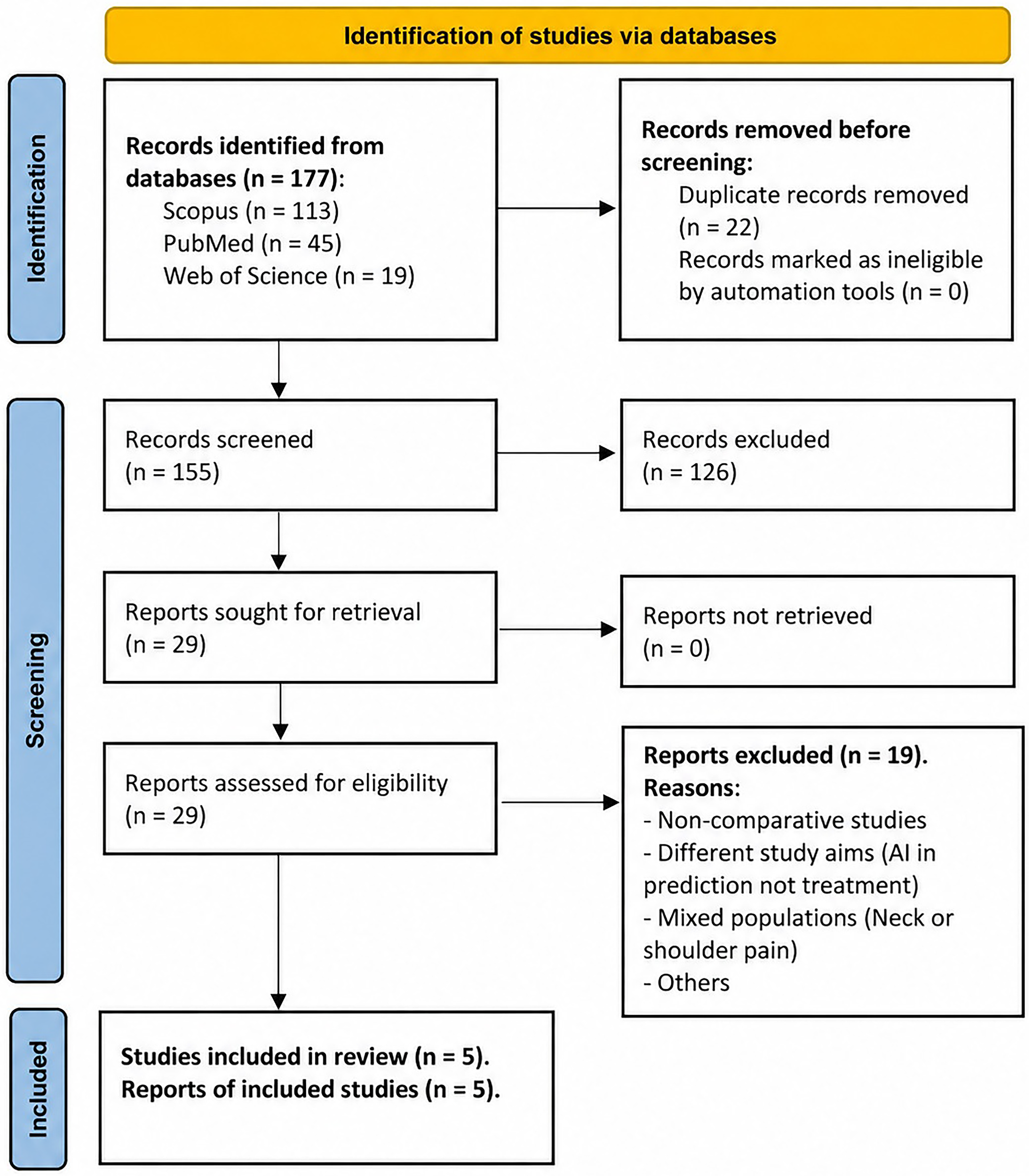
Flow diagram of the study selection process.
Ultimately, five RCTs, reported in ten related reports, met the eligibility criteria and were included in both the qualitative and quantitative analyses.30–34 The study by Sandal et al. 2021 had five secondary analyses published as distinct papers in addition to the original trial.35–39 All were identified as relevant to the review question and included in accordance with Cochrane methodological guidelines.
Study characteristics
A total of five RCTs, with 763 participants, were included in this review (Table 1). The studies were conducted across diverse countries—the United States, Japan, Korea, Denmark/Norway, and China. Intervention duration ranged from 4 to 12 weeks, except for Sandal et al., who followed participants for up to nine months. 33 All trials included patients diagnosed with LBP for more than 2 to 3 months, except Bates et al. 2023, which included self-reported patients. 30
General characteristics of the included studies evaluating AI interventions in patients with low back pain.
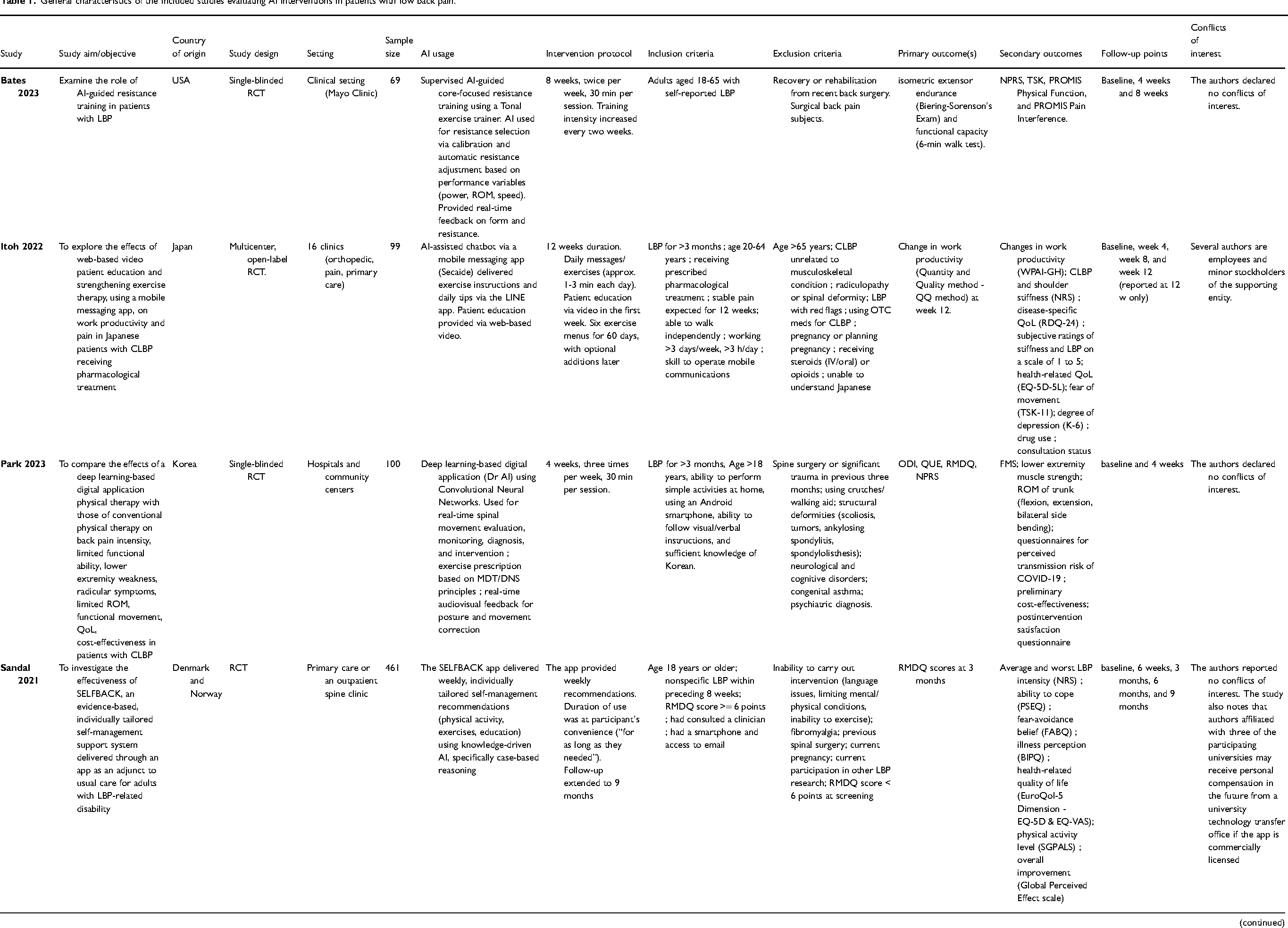
All five trials tested AI-enabled management for people with chronic or nonspecific LBP, but they differed markedly in how the technology was delivered. In two trials, participants used mobile/app-based programs that provided remote exercise guidance, education, and feedback.31,33 In two others, AI was embedded in supervised or hybrid clinical platforms that analyzed movement and tailored exercise prescriptions in real time.30,32 A fifth trial used AI-driven motion recognition within a telerehabilitation setup to guide home exercises. 34 Usual-care comparators varied by trial and included clinician advice with routine medical management, conventional in-person physiotherapy (∼3 sessions/week for 4 weeks), or standard non-AI rehabilitation (e.g., video-guided tele-rehab or clinical care only). A detailed description of the characteristics of AI-based exercise interventions and their influence on exercise prescription in the included studies is provided in Supplementary Material 2.
Participants were distributed as follows: AI-only, 361 (47.3%); active non-AI comparators, 144 (18.9%); hybrid AI + clinic, 20 (2.6%); and usual-care/no-intervention, 238 (31.2%) (Table 2). The cohort's mean age was 44.5 years (SD 14.1), with women comprising 53.9%. At entry, pain averaged 5.1/10 on the NRS (SD 2.1) and disability 10.65/24 on the RMDQ (SD 4.4), consistent with moderate baseline symptoms.
Baseline characteristics and outcome findings of included studies evaluating AI interventions in patients with low back pain.
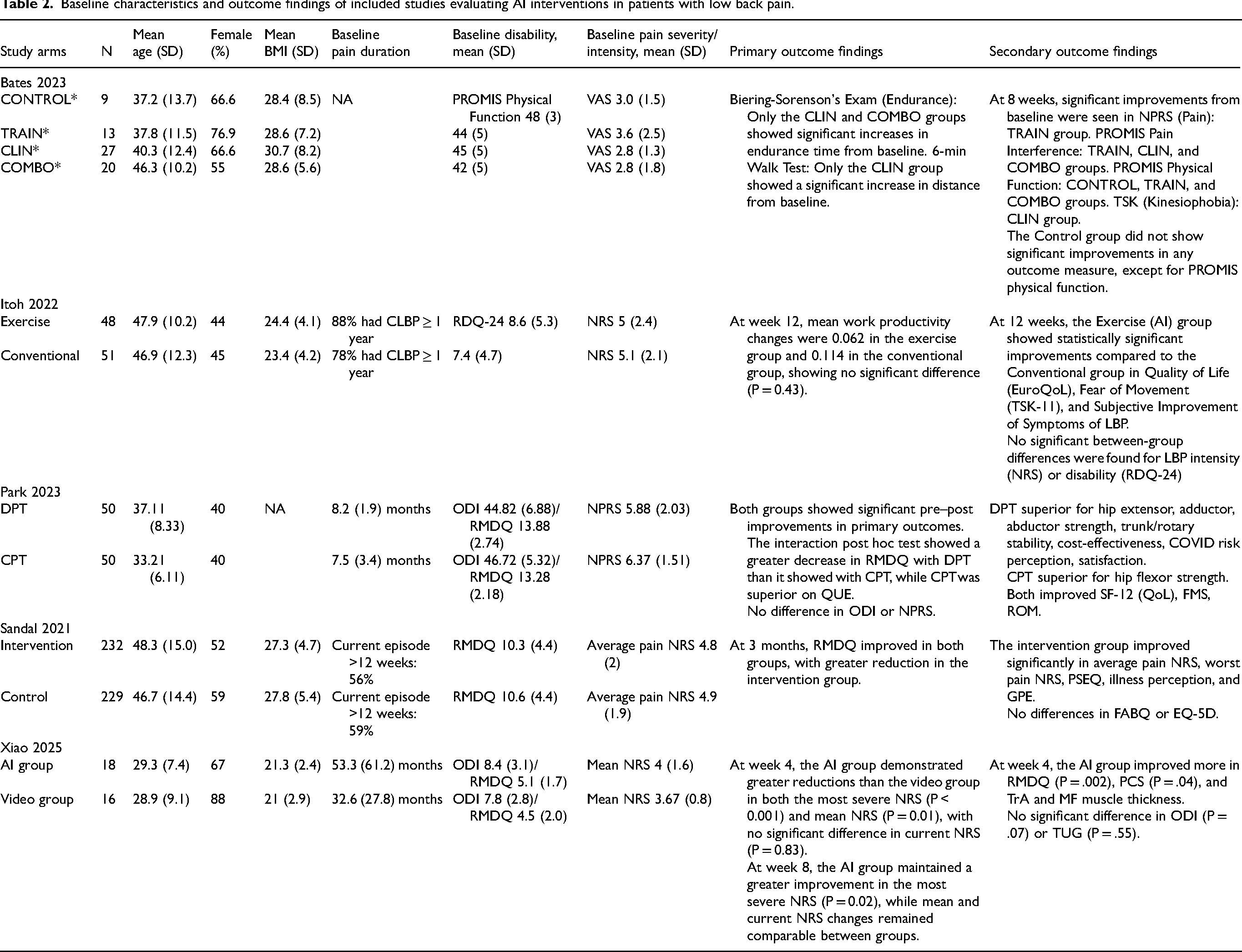
Table 1. General characteristics of the included studies evaluating AI interventions in patients with low back pain. AI = Artificial intelligence; LBP = Low back pain; CLBP = Chronic low back pain; RCT = Randomized controlled trial; ROM = Range of motion; NPRS = Numeric Pain Rating Scale; TSK = Tampa Scale of Kinesiophobia; PROMIS = Patient-Reported Outcomes Measurement Information System; QQ = Quantity and Quality method; WPAI-GH = Work Productivity and Activity Impairment–General Health; RDQ = Roland–Morris Disability Questionnaire; QoL = Quality of life; EQ-5D-5L = EuroQol 5-Dimension 5-Level; TSK-11 = Tampa Scale of Kinesiophobia-11; K-6 = Kessler Psychological Distress Scale; CNN = Convolutional Neural Network; MDT = Mechanical Diagnosis and Therapy; DNS = Dynamic Neuromuscular Stabilization; ODI = Oswestry Disability Index; QUE = Quebec Back Pain Disability Scale; RMDQ = Roland–Morris Disability Questionnaire; FMS = Functional Movement Screen; SELFBACK = Self-management support app; PSEQ = Pain Self-Efficacy Questionnaire; FABQ = Fear-Avoidance Beliefs Questionnaire; BIPQ = Brief Illness Perception Questionnaire; EQ-VAS = EuroQol Visual Analogue Scale; SGPALS = Saltin–Grimby Physical Activity Level Scale; CNSLBP = Chronic nonspecific low back pain; PCS = Pain Catastrophizing Scale; TUG = Timed Up and Go; MF = Multifidus.
Table 2. Baseline characteristics and outcome findings of included studies evaluating AI interventions in patients with low back pain. * Control (CTRL): No intervention. Training (TRAIN): Supervised moderate-intensity AI-guided core resistance training. Clinical (CLIN): Clinical care (chiropractic or physical therapy). Combined (COMBO): Clinical care plus the supervised AI-guided resistance training. AI = Artificial Intelligence; BMI = Body Mass Index; CLBP = Chronic Low Back Pain; CPT = Conventional Physical Therapy; DPT = Digital Physical Therapy; EQ-5D = EuroQol 5-Dimensions; FABQ = Fear-Avoidance Beliefs Questionnaire; FMS = Functional Movement Screen; GPE = Global Perceived Effect; LBP = Low Back Pain; MF = Multifidus; NRS = Numerical Rating Scale; ODI = Oswestry Disability Index; PCS = Pain Catastrophizing Scale; PROMIS = Patient-Reported Outcomes Measurement Information System; PSEQ = Pain Self-Efficacy Questionnaire; QoL = Quality of Life; QUE = Quebec Back Pain Disability Scale; RDQ/RMDQ = Roland-Morris Disability Questionnaire; ROM = Range of Motion; SF-12 = 12-Item Short Form Survey; TrA = Transversus Abdominis; TSK = Tampa Scale for Kinesiophobia; TUG = Timed Up and Go test; VAS = Visual Analogue Scale.
Risk of bias assessment
Overall, the included trials showed moderate methodological quality (Figures 2 and 3). Most studies demonstrated a low ROB in randomization and reporting, indicating sound study design and transparent results. However, there was a high ROB in blinding, as participants were aware of their treatment groups, and most outcomes—such as pain and disability—were self-reported subjective tools like NPRS and RMDQ. This limitation was common across all trials. In Park et al., the outcome assessor was blinded for objective measures (e.g., range of motion, strength, and functional movement screen), but primary outcomes remained self-reported, maintaining a high risk for detection bias. 32 Other domains, such as allocation concealment and attrition bias, were mostly low or unclear, reflecting minor reporting gaps rather than serious design issues.

Risk of bias assessment summary.
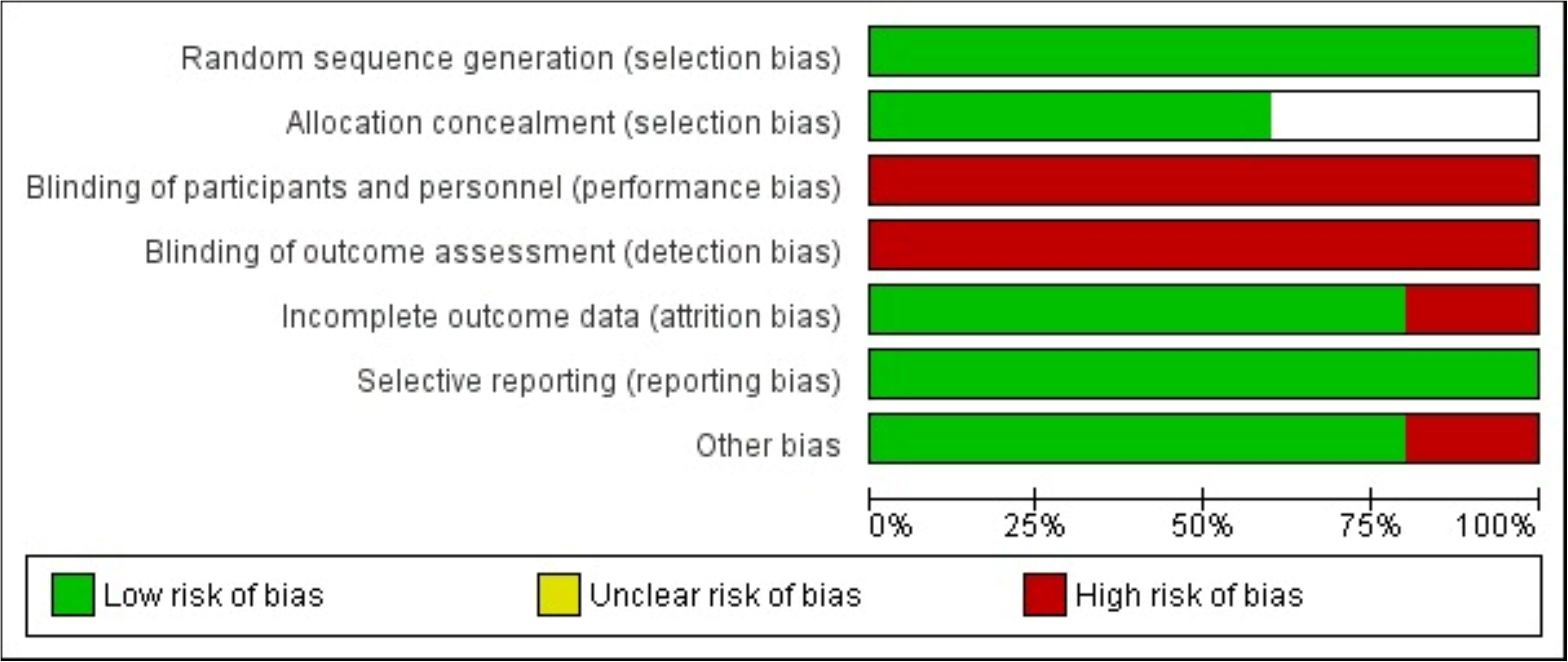
Risk of bias assessment graph.
Primary outcomes
Pain intensity (NPRS)
Endpoint timing differed across trials: 4 weeks for Park et al. (only time point reported), 8 weeks for Bates et al., 3 months for Sandal et al. (primary endpoint, rather than the 9-month follow-up), and 4 weeks for Xiao et al.
Pooling these four comparisons (AI = 313; control = 322) showed that AI-based interventions produced lower pain scores at endpoint than controls (n = 4 RCTs, MD −0.76 points; 95% CI [-1.34 to −0.17], P = 0.01) (Figure 4). Heterogeneity was moderate (I2 = 48%). In the sensitivity analysis, there was no change in direction or significance upon exclusion of each study one at a time, except when Sandal et al. was excluded; the pooled effect still favored AI but insignificantly (MD −0.66; −1.68 to 0.37) (Supplementary Material 3).
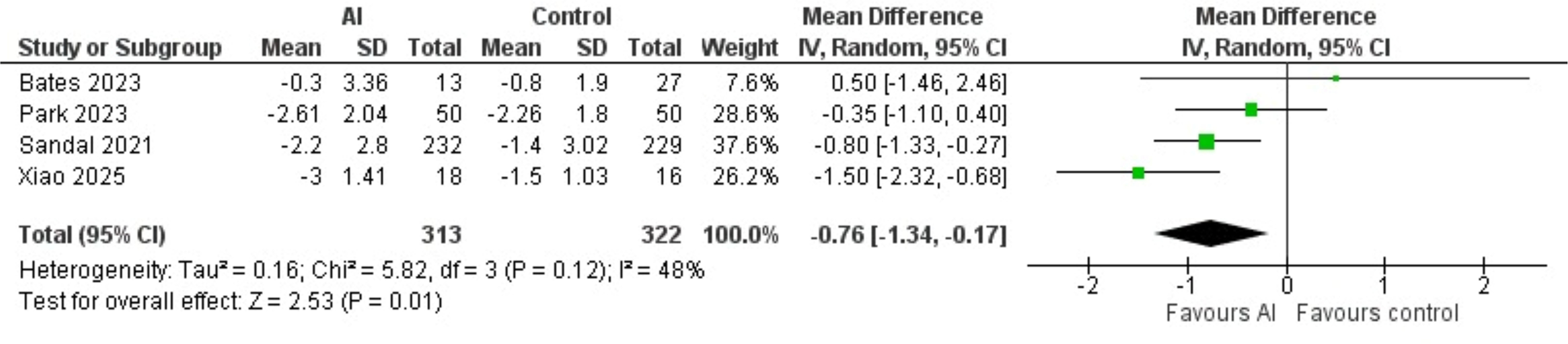
Forest plot of the mean differences between AI and non-AI-based interventions for low back pain intensity. AI = Artificial Intelligence; SD = Standard Deviation; CI = Confidence Interval.
The study by Itoh et al., the mobile-messaging trial, was not pooled in this analysis, as they reported pain intensity using the least mean square (LSM) rather than the arithmetic mean.31,40 In this trial, the adjusted change in NRS at 12 weeks did not differ between groups (LSM −1.1, standard error (SE) 0.3 in the AI arm vs. −0.7, SE 0.4 in the conventional care arm; P = 0.26). In the Sandal et al. 9-month follow-up, the AI-based group had lower average weekly pain than usual care (MD −0.69, 95% CI: [-1.07 to −0.30], P = 0.001).
Functional disability (RMDQ)
Endpoint timing varied: 4 weeks for Park et al. and Xiao et al., and 12 weeks for Sandal (primary endpoint). Pooling the three comparable trials (AI = 300; control = 358) showed lower disability at endpoint with AI (n = 3 RCTs, MD −0.88 points, 95% CI [-1.42 to −0.33], P = 0.002) (Figure 5), with no observed heterogeneity (I2 = 0%). In the sensitivity analysis, there was no change in direction or significance upon exclusion of each study one at a time.

Forest plot of the mean differences between AI and non-AI-based interventions for functional disability associated with low back pain. AI = Artificial Intelligence; SD = Standard Deviation; CI = Confidence Interval.
In the Sandal et al. 9-month follow-up, the benefit of lower disability with AI persisted at 9 months (between-group MD −0.88; 95% CI: [-1.64 to −0.11]). A larger share of participants in Xiao et al. in the intervention arm achieved ≥4-point RMDQ improvement at 3 months (52% vs 39%; adjusted odds ratio (OR) 1.76; P = 0.01).
Secondary outcomes
Quality of life
In Itoh 2022, EQ-5D-5L improved more with the AI app-based exercise program than with conventional care at 12 weeks: LS means change +0.068 vs. + 0.006; between-group difference +0.061 (95% CI 0.008 to 0.114; P = 0.03) (see also Table 2). However, in Sandal et al., EQ-5D (weighted score, −0.6 to 1.0) showed no significant difference at 3 months (MD 0.02, 95% CI: [-0.01 to 0.04]), and at 9 months (MD 0.02, 95% CI: 0.00 to 0.05 (Table 2). In Park et al., over 4 weeks, both groups improved in SF-12 form assessments: Digital Physical Therapy (DPT), the AI group, rose from 61.24 ± 6.44 to 75.20 ± 6.18 (MD +13.96), and conventional physical therapy (CPT) from 61.18 ± 4.16 to 72.14 ± 8.59 (MD +10.96), but the within-group difference was not significant (P = 0.18).
Psychological factors (kinesiophobia, self-efficacy, and pain catastrophizing)
Kinesiophobia (fear of movement or re-injury) was assessed using the TSK or TSK-11. In Itoh et al., the exercise group demonstrated a significant statistical improvement in kinesiophobia, measured by the TSK-11 score, compared with the conventional group at week 12, as the LSM difference favored the AI group by −2.8 (95% CI: [-5.5 to −0.1], P = 0.04). In Bates et al., this study measured kinesiophobia using the TSK. Only the Clinical Care (CLIN) Group showed a statistically significant decrease in TSK scores from baseline to 8 weeks (P = 0.03). In Sandal et al., this study assessed fear-avoidance using the FABQ physical activity subscale. The FABQ scores were similar between groups at both follow-ups: at 3 months (adjusted MD −0.43, 95% CI [-1.34 to 0.48]) and at 9 months (adjusted MD −0.83, 95% CI: [-1.79 to 0.13]).
Self-efficacy regarding the ability to cope despite pain was measured using PSEQ. In Sandal et al. (SELFBACK App), the AI intervention group showed a significant increase in PSEQ scores compared to the control group (usual care). At 3 months, the adjusted MD favored the intervention group by 2.52 (95% CI: 1.04 to 3.99, P = 0.001). This significant benefit in self-efficacy was sustained at 9 months (MD 3.25; 95% CI: 1.71 to 4.79.
Pain catastrophizing was also measured using PCS. In Xiao et al. (AI vs Video Telerehabilitation), the AI-assisted multimodal exercise group showed a significant improvement (decrease) in PCS scores compared to the conventional video group at week 4 (adjusted MD −3.94, 95% CI: [-7.69 to −0.19], P = 0.04).
Discussion
This systematic review and meta-analysis synthesize the emerging evidence evaluating AI-enabled non-pharmacological interventions for LBP and demonstrates that AI-based systems confer statistically significant improvements several weeks after their initiation for pain and disability compared to conventional and non-AI-driven non-pharmacological interventions. These studies investigated behavioral, exercise, and education-based interventions under AI guidance. The findings of this investigation are valuable as these rehabilitation strategies are well known as therapies for LBP treatment, but have been reported with reduced efficacy in the past due to inadequate compliance and guidance.41,42 Applying AI to these strategies can improve these shortcomings as they are able to standardize therapies, increase patient motivation through real-time feedback to allow them to engage consistently in therapies, and deliver evidence-based, patient-tailored management approaches to improve pain and thus pain-related disabilities. This enhanced care has not only demonstrated improvement in pain and disability over a short term, such as 4 weeks, but has also shown improvement over a long term, such as 9 months, as seen in these studies.30,32–34 AI used in these studies was all application-based and delivered via digital systems, and they either collected or used data that was fed to them to learn, analyze, and provide proactive and individualized intervention rather than the traditional reactive and population-based intervention, which could have had an impact to show the above effects. Although the MD values reached statistical significance in the pooled analysis of the studies for pain intensity and functional disability, the minimal clinically important difference was not applied, and hence, the clinical relevance cannot be ascertained. When the MD values of these outcomes are compared to studies that have reported values for minimally clinically important change to happen in LBP, the size effect falls below the previously established values, suggesting that the statistical benefit may not translate into clinical improvement. 43
AI and machine learning are transforming the diagnosis and management of musculoskeletal disorders. LBP is caused by multiple factors and has a biopsychosocial component to it, with the majority of LBP without an identifiable cause. In such a background, a biopsychosocial framework and machine learning algorithms can play a key role in screening and identifying risk factors to establish a key relationship between the predictors and outcomes for an individual. Bhak et al. explored multiple factors for LBP in a population and successfully built a machine learning model that was able to detect LBP based on the risk factors. 44 When compared to traditional epidemiological methods, machine learning and AI can narrow down on the optimal set of variables, thereby minimizing the risk of confounding, can identify indirect factors, and can provide personalized effects of the factors. Having better diagnostic accuracy, machine learning can be simple and cost-effective as well. Buccheri et al. in a cross-sectional study, were able to reveal this, where derivation of a simple computational equation through machine learning was able to estimate skeletal mass, which is crucial to diagnose several musculoskeletal disorders, accurately from radiological studies. 45 Beyond diagnosis, they can actively shape management through treatment selection, surgical precision, and personalized rehabilitation. Multiple studies have shown the applications and benefits of AI in musculoskeletal disorder interventions. AI has demonstrated automated anatomical structure identification, target differentiation from unnecessary structures, improved needle guidance towards the target, optimal application of therapy that improves the overall efficiency of image-guided interventions with fewer complications for musculoskeletal disorders. 46 A pooled analysis of strategies for rehabilitation for musculoskeletal disorders has demonstrated that AI-assisted strategies significantly improve rehabilitation when compared to conventional strategies by improving pain, functional outcomes, and range of motion, thereby highlighting the significance of AI in personalizing and eventually improving management in musculoskeletal disorders. 47
While it was not possible to pool all the studies to analyze for the secondary outcomes, individual investigation of the included studies revealed mixed outcomes. For quality of recovery, Itoh et al. were able to demonstrate improvement in quality of life following AI-based intervention on LBP, but Park et al. and Sandal et al. did not demonstrate any significant difference when compared with the conventional mode of interventions.31–33 Quality of recovery summarizes patients’ subjective experience to the interventions they receive. Although we cannot draw a conclusion, depending on the AI technology and the population that is studied, its influence on the quality of recovery can be variable. With digital health having demonstrated its efficacy on chronic LBP by improving quality of life in the past, the potential of AI that uses computerized forms of technology and its influence on quality of recovery in LBP patients should not be disregarded and may need further investigation. 48 Similarly for psychological outcomes, Bates et al. did not show any difference for kinesiophobia, but Itoh et al., Sandal et al. and Xiao et al. were able to demonstrate improvement in patient's fear, confidence in performing daily activities, negative cognitive and emotional responses to pain following AI based intervention when compared to usual care that could last between 4 weeks and 9 months.30,31,33,34 Since the frequency and duration of AI-guided interventions have been shown to influence these psychological outcomes, it will be useful to investigate these interventions at increased frequency and duration to determine their actual effect on these psychological outcomes both over the short term and long term. 49
As the management tools for LBP keep evolving, several noninvasive treatment modalities for LBP have emerged as they offer a safer, more sustainable alternative to surgery and medications such as opioids. Virtual reality is one such noninvasive treatment technology that combines distraction from pain, reduction of fear of movement, and teaching of self-regulation through immersive experience to treat LBP. Li et al. in a systematic analysis demonstrated that virtual reality can reduce pain, pain-related fear, and disability related to LBP when compared to conventional treatments or placebo. 50 Metaverse, the sustained version of virtual reality that shifts the immersive experience from an isolated to a persistent one has also demonstrated a reduction in disability and improvement in rehabilitation in LBP.51,52 But their effects were seen only during the immediate period after the intervention, with no difference over a short-term period. This can be due to the fact that virtual reality is primarily a delivery tool for immersive therapy that can be affected by other variable factors related to LBP. But AI, when incorporated with management techniques for LBP, becomes an optimization tool that includes other variable factors to personalize and adjust treatment plans for effective management.
This study exhibits that AI for LBP may be used as an augmentation technology rather than a therapeutic one to improve pain and disability associated with it. This intervention does not treat pain via biological pathways, but it may optimize the reinforcement of exercise as a therapy for LBP through precision and a real-time decision mode that cannot be achieved in standard clinical models. Optimization of its use can expand the durability of its benefit on a long-term basis, especially for the quality of recovery and psychological outcomes that are associated with it.
However, there are several limitations. A primary limitation of this meta-analysis is the small number of eligible studies, which reflects the nascent state of AI in LBP research and restricts our ability to come to definitive conclusions or perform robust subgroup analyses. There is a heterogeneity in the AI architectures used in the studies included in this investigation, with no uniform algorithm or outcomes. With the number of studies being small, there is a risk of disproportionate estimation and less opportunity for subgroup analysis, as it would be statistically invalid. High heterogeneity can lead to a model that can give equal weightage to all studies regardless of their size, hence a small study can have a large impact on the pooled result. Not all the studies were able to be included for all the outcomes due to either uneven or missing data in them. But a sensitivity analysis was done for the primary outcomes to determine that there was no change in significance upon exclusion of each study one at a time, except for Sandal et al., for pain intensity. Methodologically, most studies exhibited a high risk of bias in blinding domains for performance and detection. Hence, the reliability of these findings can be compromised, and as a consequence, the generalizability of these results should be approached with caution. This reflects the challenge of using and reporting technology-mediated interventions and their related outcomes, and hence the inability to infer on dose–response relationships of AI on LBP that could have contributed to small-sized gains as reported in the studies. In the background of a few available studies, overestimation of the effect size is possible as well. But with the risk of selection, attrition, and reporting bias being low, the data can still be considered for analysis and interpretation. While we acknowledge the limited number of studies and risk of bias, this meta-analysis still represents a rigorous synthesis of evidence that is currently available as randomized controlled trials in this field, and these findings provide an insight into gaps that must be addressed in future research. Since the reporting was variable and limited for secondary outcomes in the studies, an analysis was not possible, establishing a void in its interpretation. Besides these limitations, AI in general intersects with diversity concerns such as digital literacy, socioeconomic access, and cultural differences. 53 These warrant the need for targeted investigations to study specific AI tools on different LBP populations for defined outcomes, from a proof-of-concept efficacy trial concept to implementation science. AI-guided rehabilitation in LBP has demonstrated cost-effectiveness when compared to traditional rehabilitation with clinical visits, but without a difference over the long term. 54 Hence, future research should also include effectiveness-cost-utility designs to confirm its cost benefits to support reimbursement pathways.
Conclusion
In summary, AI-guided non-pharmacological exercise-based interventions may improve pain and disability in adults with LBP, likely through behavioral rehabilitation and optimization of delivery of these interventions. But these findings come in the background of certain limitations that justify the need for rigorous research on AI-assisted LBP management from an experimental to a clinical pathway to help establish their clinical relevance and guide the future of AI use in LBP.
Supplemental Material
sj-docx-1-bmr-10.1177_10538127261464781 - Supplemental material for The effectiveness of artificial intelligence-based interventions on treatment outcomes for low back pain: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-1-bmr-10.1177_10538127261464781 for The effectiveness of artificial intelligence-based interventions on treatment outcomes for low back pain: A systematic review and meta-analysis of randomized controlled trials by Kumaran Ramanujam, Samyr Carneiro, Mohamed Mohsen Helal and Vendhan Ramanujam in Journal of Back and Musculoskeletal Rehabilitation
Supplemental Material
sj-docx-2-bmr-10.1177_10538127261464781 - Supplemental material for The effectiveness of artificial intelligence-based interventions on treatment outcomes for low back pain: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-2-bmr-10.1177_10538127261464781 for The effectiveness of artificial intelligence-based interventions on treatment outcomes for low back pain: A systematic review and meta-analysis of randomized controlled trials by Kumaran Ramanujam, Samyr Carneiro, Mohamed Mohsen Helal and Vendhan Ramanujam in Journal of Back and Musculoskeletal Rehabilitation
Supplemental Material
sj-docx-3-bmr-10.1177_10538127261464781 - Supplemental material for The effectiveness of artificial intelligence-based interventions on treatment outcomes for low back pain: A systematic review and meta-analysis of randomized controlled trials
Supplemental material, sj-docx-3-bmr-10.1177_10538127261464781 for The effectiveness of artificial intelligence-based interventions on treatment outcomes for low back pain: A systematic review and meta-analysis of randomized controlled trials by Kumaran Ramanujam, Samyr Carneiro, Mohamed Mohsen Helal and Vendhan Ramanujam in Journal of Back and Musculoskeletal Rehabilitation
Footnotes
Acknowledgements
None
Ethical approval
This study has been registered with PROSPERO (registration number: CRD420251174515).
Informed consent
Not applicable.
Author contributions
Kumaran Ramanujam, Samyr Carneiro: Writing – original draft, review and editing. Mohamed Mohsen Helal – Data curation, formal analysis, investigation, methodology. Vendhan Ramanujam: Conceptualization, investigation, methodology, supervision, validation, writing - reviewing and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The datasets collected during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.