
Abstract
Background
Posterior condylar offset (PCO) is a crucial knee anatomic parameter closely linked with joint function. Its restoration during posterior-stabilized total knee arthroplasty (TKA) draws wide research attention. Most studies focus on the impact of the PCO alterations on soft tissue balance and postoperative function, while relevant contributing factors remain poorly investigated.
Objective
To explore PCO variation after posterior-stabilized TKA and analyze potential influencing factors contributing to such changes.
Methods
From November 2020 to November 2021, 146 consecutive participants with a diagnosis of severe knee osteoarthritis were enrolled for this prospective study. All participants underwent primary posterior-stabilized TKA utilizing 3D-printed patient-specific instrumentation. Perioperative clinical variables and radiographic parameters were assessed, and the osteotomy thickness in the posterior femoral condyle was quantified during the TKA procedure.
Results
A total of 134 participants (17 males and 117 females) were recruited in this prospective study, including 72 patients (53.7%) with changes of PCO after TKA < 3 mm in group 1, and 62 patients (46.3%) with changes of PCO after TKA ≥ 3 mm in group 2. The demographic characteristics, clinical scores, and radiographic measurements of the two groups were comparable before TKA. In general, postoperative PCO was considerably reduced compared with preoperative PCO (29.77 ± 3.52 mm vs. 27.67 ± 2.99 mm, p < 0.001). Postoperative PCO reduction was noted in 99 patients (73.9%). The correlation analysis indicated a relatively weak positive relationship between PCO variation and the osteotomy of posterior lateral femoral condyle (r = 0.282, p = 0.004). Moreover, radiographic evaluation revealed that patients in group 1 had a smaller preoperative posterior tibial slope (PTS, p < 0.001) and a smaller PTS change (p = 0.002) after TKA.
Conclusion
PCO tends to decrease after posterior-stabilized TKA. The osteotomy in posterior lateral femoral condyle may potentially serve as a direct influencing factor for such reduction. The preoperative PTS and a greater PTS change were found to be indirect influencing factors associated with PCO variability in posterior-stabilized TKA. These imply that the anatomical morphology in posterior femoral condyle should not be sacrificed for the pursuit of uniform femoral and tibial osteotomy concepts.
Introduction
Total knee arthroplasty (TKA) is a prevalent and effective surgical procedure for advanced and severe arthritis. Although clearly beneficial to joint functional recovery, it definitely causes knee biomechanical changes, and leads to a series of postoperative complications. Three-dimensional (3D)-printed patient-specific instrumentation (PSI) enables customized osteotomy based on preoperative CT data, potentially improving accuracy and alignment.1–4 Utilizing reconstructed 3D imaging, surgeons can plan femoral and tibial osteotomies and implant positions to match individual anatomy.5–8 However, the prostheses ultimately implanted in this study were standard, non-customized implants, which may impact the final ideal restoration of posterior condylar offset (PCO).
Posterior condylar offset (PCO) refers to the vertical distance between the peak of posterior condyle and the line tangential to the posterior cortex (Figure 1). The restoration of PCO, as well as its impact on clinical outcome and range of movement (ROM), remains a key research hotspot in posterior-stabilized TKA. From a clinical standpoint, even small changes in PCO have meaningful consequences: a reduction of 1 mm could lead to a decrease in knee flexion ranging from 3.3 to 6.2 degrees. 9 Excessive osteotomy in posterior femoral condyle during TKA, which results in a significant decrease in PCO, may cause impingement at the posterior margin of femur and tibial plateau.10,11 A significant alteration in PCO may also result in quadriceps weakness and an increase in posterior cruciate ligament tension, consequently impacting the stability and functionality of the knee joint following TKA. 12 Furthermore, PCO variation serves as a crucial factor affecting patient satisfaction following total knee arthroplasty (TKA). Substantial PCO deviation compromises patient satisfaction and overall postoperative experience.13,14 However, current implant design concept often prevent precise PCO restoration when using conventional instrumentation from various manufacturers in TKA. 15 Therefore, clarifying PCO variability and exploring its related direct and indirect factors are critical for restoring or minimizing the morphology variation in posterior femoral condyle during posterior-stabilized TKA.
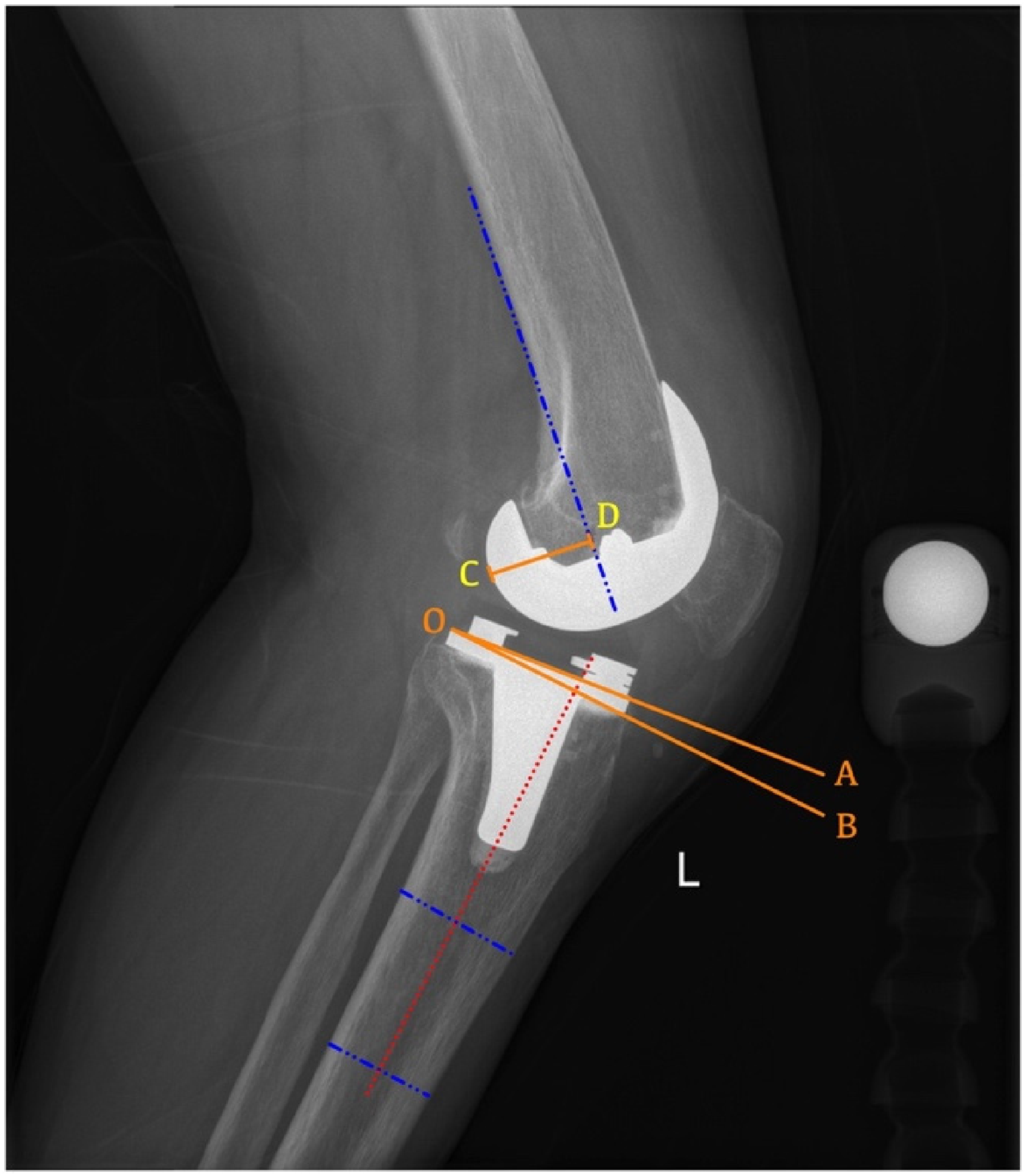
Radiographic assessment of lateral view following posterior-stabilized TKA. A radiographic example illustrates the posterior tibial slope measurements using the proximal anatomic axis (the angle formed by lines OA and OB) and the posterior condylar offset (CD, the vertical distance between the peak of posterior condyle and the line tangential to the posterior cortex).
Nevertheless, most existing studies have focused on the consequences of PCO change (e.g., soft tissue balance, joint function), while few have systematically explored the underlying factors driving PCO variability. This constitutes a clear knowledge gap. Therefore, this study aimed to address two key questions: (1) Does the PCO alter following TKA? (2) What factors, both direct and indirect, may contribute to the variability observed in PCO?
Patients and methods
Study design
In this prospective study, we enrolled 146 consecutive patients with a diagnosis of varus knee osteoarthritis who underwent primary posterior-stabilized TKA at our hospital from November 2020 to November 2021.
This was an exploratory, real-world study without clinical trial registration or randomization.
This study was a purely observational, real-world study, the osteotomy amount in the posterior femoral condyle during TKA was determined according to the standard design protocols of 3D-printed patient-specific instrumentation. It should be noted that the non-randomized nature of the study might have resulted in selection bias, although there were no statistical differences in the general characteristics (demographic data, clinical scores, and radiographic parameters) of participants at baseline between the two groups. The detailed design protocols are described in the surgical intervention section below. Meanwhile, this study was reported in accordance with the STROBE statement for observational studies.
The present study was conducted in accordance with the 2013 Declaration of Helsinki (seventh revision) and approved by the Ethical Review Board at Peking University International Hospital (No. 2020-036(BMR), dated August 27, 2020). Written informed consent was obtained from all participants.
Patients were excluded if they had a history of prior surgery on the affected knee, post-traumatic arthritis, knee valgus deformities, or insufficient image quality. All patients were scheduled for unilateral TKA. Out of 146 patients, 1 patient who underwent high tibial osteotomy procedure, 6 patients with valgus knees, and 5 patients with insufficient imaging quality were not included in the scope of this study (Figure 2). Ultimately, 134 patients (17 males and 117 females, 134 knees) were recruited in this study. Participants’ average age was 68.0 ± 6.0 years, ranging from 54 to 81 years, and their mean body mass index (BMI) was 27.1 ± 3.7 kg/m2, spanning from 18.0 to 38.0 kg/m2.
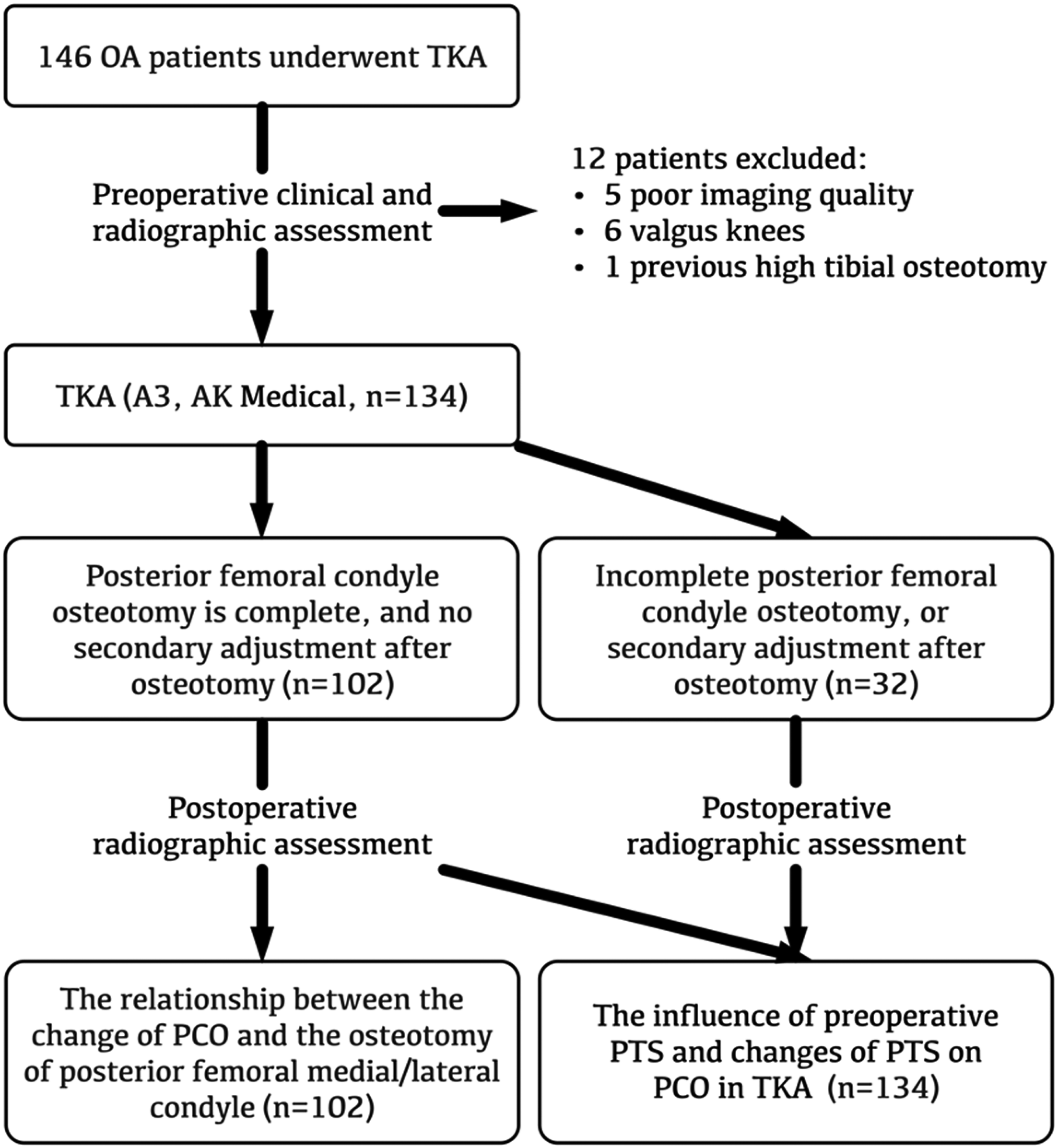
Flow diagram of patients’ selection and exclusion.
Surgical intervention
All procedures were conducted by a single experienced surgeon. All participants (134 knees) were implanted with an A3 fixed-bearing, posterior-stabilized total knee system (Beijing AK Medical Co., Ltd, China). All procedures were performed using 3D-printed patient-specific instrumentation technique. A medial parapatellar approach was adopted for knee exposure, with minimal removal of infrapatellar fat pad and without patellar eversion. A tourniquet was routinely used for the entire surgical procedure. Tibial and femoral osteotomies were performed with 3D-printed patient-specific instrumentation according to preoperative individual design. The surgical design and intraoperative osteotomy followed the same protocols as detailed in our previous article. 16 In particular, the design protocol of 3D-printed patient-specific instrumentation for femoral osteotomy is as follows: the osteotomy amount in the posterior lateral femoral condyle was routinely 9 mm, which matches the posterior condyle thickness of the femoral prosthesis adopted in this study. Meanwhile, if an anterior femoral condyle notch existed, or a mismatch was present between the transverse width of the femoral component and the native femoral condyle, the osteotomy amount in the posterior femoral condyle would be adjusted appropriately. Adjustment of osteotomy in the posterior femoral condyle during TKA was only performed when the flexion-extension gap could not be balanced by soft tissue release. In such cases, the osteotomy in the femoral condyle, as well as the placement and size of the implants, were no longer strictly guided by the 3D-printed patient-specific instrumentation. All intraoperative adjustments (including the need for secondary recutting of the posterior condyle) were recorded prospectively. If the osteotomy of the posterior femoral condyle was adjusted, the relevant PCO data were only adopted to analyze how preoperative PTS and intraoperative PTS changes affect the variation of intraoperative PCO during TKA. These data were not applied to other analytical parts. Excluding these cases would introduce selection bias. Detailed patient grouping information is included in the scope of this study (Figure 2).
Postoperative pain management involved a combination of periarticular cocktail injection and femoral nerve block. Rehabilitation training began promptly after the surgery, led by a consistent rehabilitation team.
Clinical assessment
Preoperative and 3-month postoperative follow-up data were recorded for all enrolled patients, including demographic data (age, gender, affected side and BMI) and clinical scores namely ROM, Knee Society scores (KSS), Knee Society Function scores (KSFS), 17 and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). 18
Radiographic assessment
All patients received standardized radiographic examinations before and after TKA. The radiographic acquisition protocols were strictly consistent with those established in previous studies. 19 A full-length standing anteroposterior X-ray imaging of the entire lower extremity was obtained, with knee joint fully extended, and the tibial tubercles aligned forward to the central axis of the X-ray beam at a distance of 8 ft, and care was taken to ensure the knee was not rotated. In the lateral radiographic views, the medial and lateral femoral condyles were superimposed at around knee 30 degrees flexion. Two independent surgeons performed all radiographic measurements using the Centricity PACS system (GE Healthcare) and were blinded to patient clinical data. The analysis was based on the average of these two sets of radiographic measurements. The evaluated radiographic parameters were the posterior tibial slope (PTS) 20 and PCO 21 (Figure 1). To assess reproducibility, 20 randomly selected radiographs were re-measured by the same two surgeons after a two-week interval. Intraclass correlation coefficients (ICCs) were calculated using a two-way random effects model for absolute agreement. The intra-observer ICC was 0.856 for PCO and 0.799 for PTS; the inter-observer ICC was 0.825 for PCO and 0.782 for PTS. All ICC values indicated good to excellent reliability (ICC > 0.75).
To evaluate how well the PCO was preserved in TKA, patients were categorized into two groups according to the alterations in PCO values pre- and post-TKA: group 1 (<3 mm) and group 2 (≥3 mm). The reference threshold of 3 mm for PCO difference was established based on prior research indicating that a change of less than 3 mm in PCO is considered acceptable in TKA. 22 Of note, the average thickness of human knee articular cartilage is approximately 3 mm. Therefore, a reduction in PCO of 3 mm or more roughly corresponds to the complete loss of the cartilage layer from the posterior femoral condyle, simulating the pathological condition of advanced cartilage wear in osteoarthritis. This threshold thus carries both clinical and pathophysiological relevance.
Statistical analysis
The sample size was calculated using G*Power software (Ver. 3.1.9.6; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany) in this study. Based on previous literature, a post hoc power analysis using G*Power software indicated that a minimum sample size of 109 subjects was required to detect a significant change in PCO from pre- to post-TKA (effect size = 0.3, α = 0.05, power = 0.9). 23 In this study, a total of 146 subjects were finally enrolled. Post hoc power analysis cannot fully validate the reliability of research findings, thus the high statistical power should be interpreted with caution. For statistical analysis, Prism 9.0 software (GraphPad, San Diego, CA, USA) was employed. Continuous variables were expressed as the means ± SD. Normality of continuous variables was evaluated by Shapiro-Wilk test. Normality of continuous variables was evaluated by Shapiro-Wilk test, combined with Q-Q plots and histograms for visual inspection. Independent samples t-test was adopted for intergroup comparison of normally distributed data, and Mann-Whitney U test was used for non-normally distributed data. Categorical variables were evaluated utilizing a Fisher's exact test. Threshold for statistical significance in this study was set at p < 0.05.
Results
The general characteristics of participants prior to surgery
Of the 134 enrolled patients, 72 patients (53.7%) exhibited PCO changes of less than 3 mm after TKA in group 1, while 62 patients (46.3%) demonstrated PCO changes of 3 mm or more after TKA in group 2. The preoperative general characteristics of the participants are presented in Table 1. A comparison of preoperative demographic data, clinical scores, and radiographic parameters between the two groups showed no statistical significance (as seen in Table 1), indicating that the baseline characteristics of the two groups were comparable.
The general characteristics of patients prior to surgery
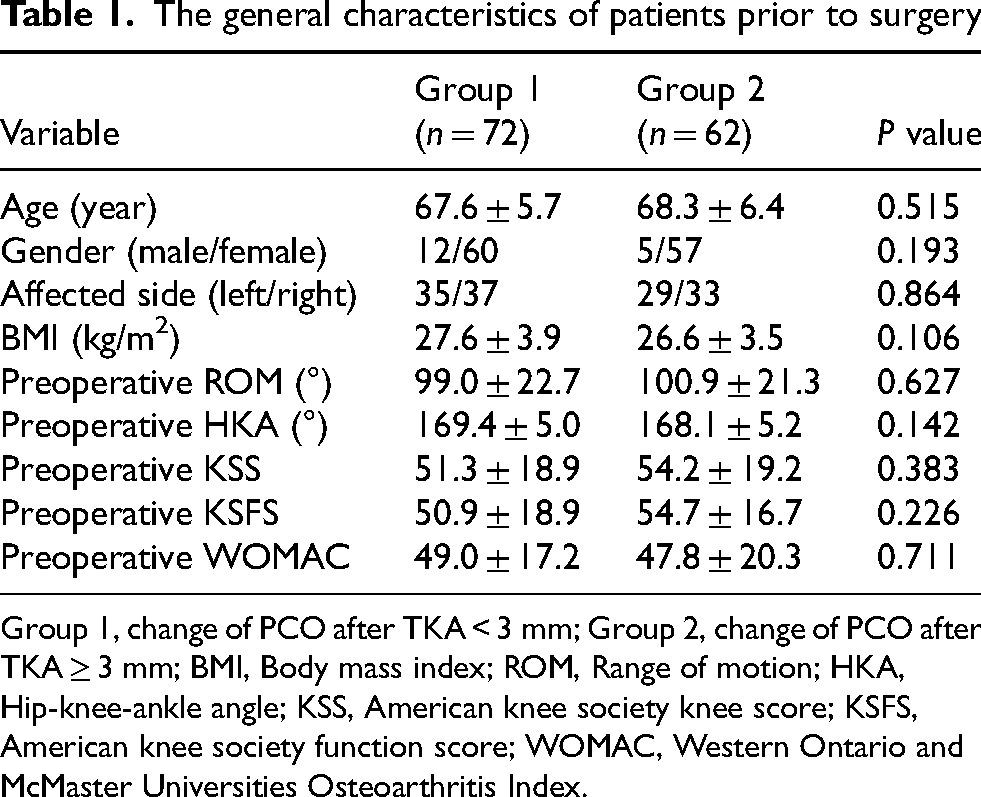
Group 1, change of PCO after TKA < 3 mm; Group 2, change of PCO after TKA ≥ 3 mm; BMI, Body mass index; ROM, Range of motion; HKA, Hip-knee-ankle angle; KSS, American knee society knee score; KSFS, American knee society function score; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
The variability of PCO in posterior-stabilized TKA
Overall, postoperative PCO was significantly reduced compared with preoperative PCO (Figure 3A). A decrease in PCO was noted in 99 patients (73.9%). Preoperative PCO was 29.77 ± 3.52 mm, which decreased to 27.67 ± 2.99 mm postoperatively (p < 0.001, Figure 3A). The mean decrease in PCO after TKA was 2.10 mm (95% confidence interval: 1.62 to 2.58 mm), with a Cohen's d of 0.74, indicating a moderate effect size. Of the 134 patients, 102 patients (76.1%) underwent complete posterior femoral condyle osteotomy during TKA. The remaining 32 patients (23.9%) failed to achieve complete posterior femoral condyle osteotomy, and needed secondary adjustment after osteotomy. Whether posterior femoral condyle osteotomy was completed at one time during TKA without secondary adjustment did not influence the variation of PCO. In brief, no statistical significance in PCO alteration was found between the two groups (Figure 3B). The change in PCO was 3.24 ± 2.84 mm in the complete osteotomy group, and 3.07 ± 2.01 mm in the incomplete osteotomy group.
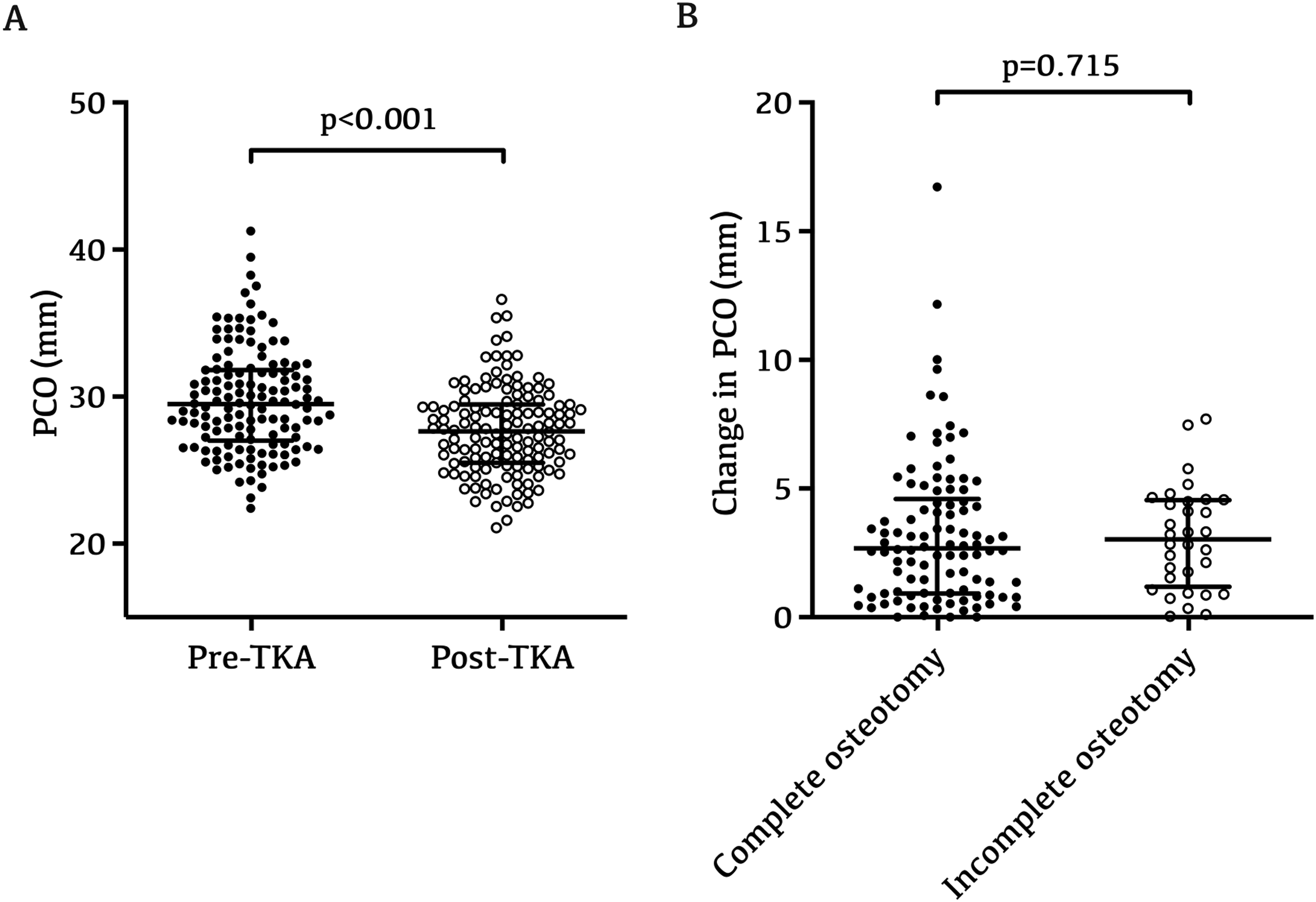
The variability of PCO in posterior-stabilized TKA. A: A comparison of the PCO pre and post-TKA (n = 134). It was observed that PCO changed significantly after TKA when compared with its preoperative physiological status (p < 0.001). Specifically, preoperative PCO was 29.77 ± 3.52 mm, and decreased to 27.67 ± 2.99 mm following TKA. B: Of the 134 patients, 102 patients (76.1%) underwent complete posterior femoral condyle osteotomy during TKA. The remaining 32 patients (23.9%) failed to achieve complete posterior femoral condyle osteotomy, and needed secondary adjustment after osteotomy. There was no statistical significance in PCO variation between complete osteotomy group (n = 102) and incomplete osteotomy group (n = 32), PCO change was 3.24 ± 2.84 mm in complete osteotomy group, and 3.07 ± 2.01 mm in incomplete osteotomy group.
The relationship between the variability of PCO and the osteotomy in posterior femoral condyle
Further analyses were conducted to examine the association between PCO changes and the osteotomy amount in posterior medial/lateral femoral condyle, which likely served as the direct factor determining postoperative PCO variation. The osteotomy change in posterior medial/lateral femoral condyle was defined as the osteotomy minus implant thickness in the posterior femoral condyle. Correlation analysis indicated a relatively weak positive association between the change of PCO and the osteotomy in posterior lateral femoral condyle (r = 0.282, p = 0.004, Figure 4A). Nevertheless, no significant correlation was found between the change of PCO and the osteotomy of posterior medial femoral condyle (r = 0.060, p = 0.547, Figure 4B).
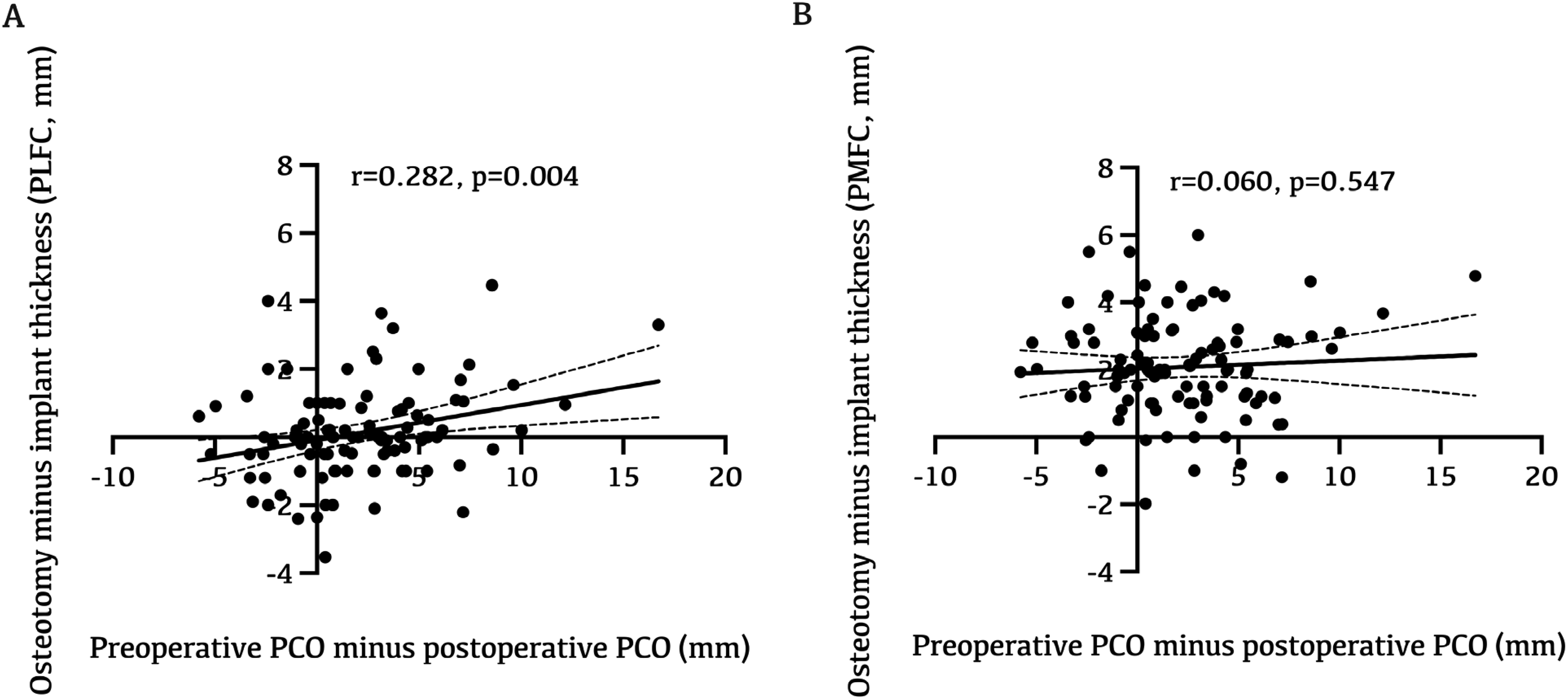
Correlation between PCO variation and posterior medial/lateral femoral condyle osteotomies. A: Correlation analysis indicated a relatively weak positive correlation between PCO change and posterior lateral femoral condyle osteotomy (n = 102, p = 0.004), which indicated that osteotomy amount of posterior lateral femoral condyle serves as an associated factor contributing to PCO variation following TKA. B: PCO change did not show a significant correlation with posterior medial femoral condyle osteotomy (n = 102, p = 0.547), which might be attributed to cartilage injury of posterior medial femoral condyle in varus knee or external rotation osteotomy in the distal femur.
The influence of preoperative PTS and changes of PTS on PCO in TKA
Similarly, 72 patients (53.7%) with postoperative PCO changes <3 mm were assigned to group 1, while 62 patients (46.3%) with postoperative PCO changes ≥3 mm were assigned to group 2. Radiographic assessment revealed that group 1 had a smaller preoperative PTS (p < 0.001, Figure 5A), which was 9.68° ± 3.00° in group 1 and 11.82° ± 3.05° in group 2. Additionally, the change in PTS was also smaller in group 1 following TKA (p = 0.002, Figure 5C), which was 5.90° ± 3.44° in group 1 and 7.90° ± 3.55° in group 2.
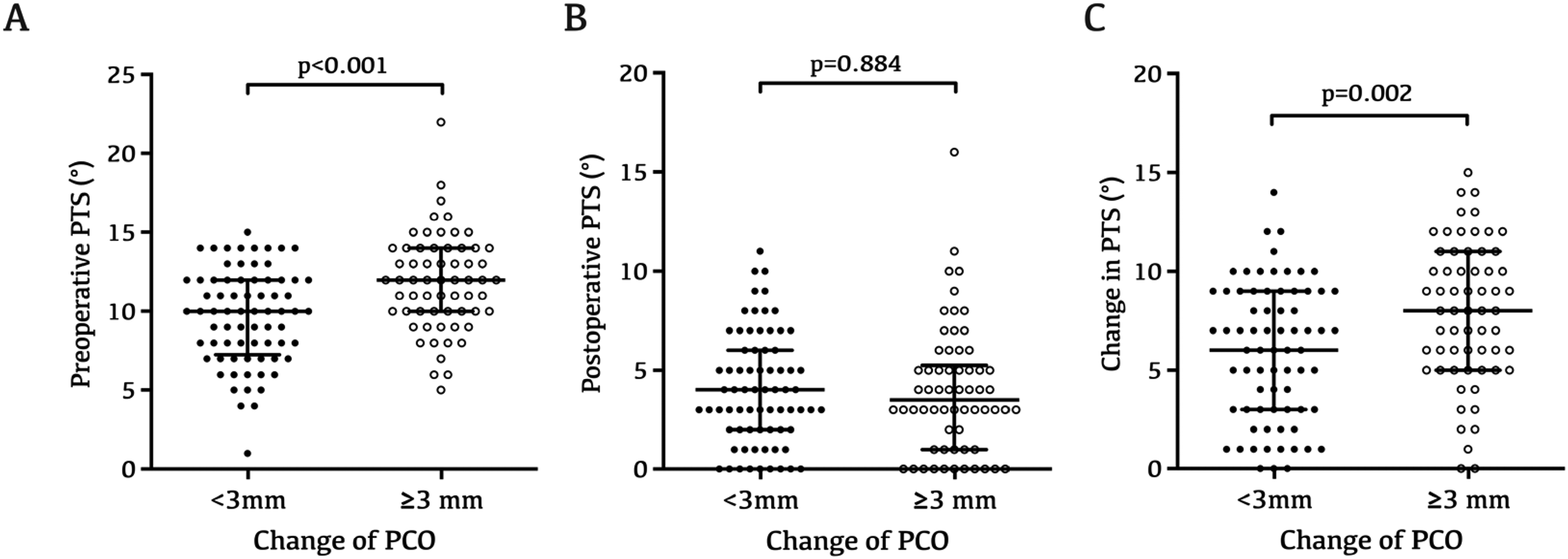
Impact of preoperative PTS, postoperative PTS and PTS changes on PCO in TKA. A: Patients in group 1 had a smaller preoperative PTS in group 1 (p < 0.001), which was 9.68° ± 3.00° (n = 72), compared with 11.82° ± 3.05° in group 2 (n = 62). B: No statistical significance was observed in postoperative PTS between the two groups (p = 0.884), which was 4.03° ± 2.81° in group 1 (n = 72), and 3.95° ± 3.22° in group 2 (n = 62). C: Patients in group 1 experienced a smaller PTS change following TKA (p = 0.002), which was 5.90° ± 3.44° in group 1 (n = 72), and 7.90° ± 3.55° in group 2 (n = 62).
Discussion
This study was designed to address two primary research questions: (1) Does PCO change after posterior-stabilized TKA? and (2) What factors, both direct and indirect, are associated with PCO variability? The principal discovery of this study was that PCO changed significantly and presented a decreasing trend after posterior-stabilized TKA. The factor most directly associated with PCO variability was posterior lateral femoral condyle osteotomy. Preoperative PTS and a greater PTS changes were also associated with PCO variability.
Numerous previous studies have demonstrated that restoration of PCO is a critical factor affecting biomechanics in posterior-stabilized TKA. Postoperative alterations in PCO affect knee biomechanical properties, including intraoperative soft tissue balance, range of motion, patellofemoral contact stress, quadriceps force, and the collateral ligaments tension.9,24,25 Multiple factors can cause PCO alterations during TKA, including modified posterior femoral condylar osteotomy for avoiding anterior femoral notching, abnormal external rotation in femoral component, improper prosthesis sizing and inaccurate osteotomy. 15 In this study, femoral and tibial osteotomy were performed with 3D-printed patient-specific instruments designed based on conventional osteotomy criteria. Hence, our result is consistent with previous studies, showing a significant alteration in PCO following TKA.
In order to investigate the factors directly and indirectly associated with morphological variations of posterior femoral condyle during posterior-stabilized TKA, we further analyzed the correlation between PCO changes and posterior medial and lateral femoral condyles osteotomies, along with PTS in TKA. This study initially revealed that there was a relatively weak correlation between the variability of PCO and the osteotomy minus implant thickness in posterior lateral femoral condyle. Nevertheless, no significant correlation was identified between the variability in PCO and the osteotomy amount in posterior medial femoral condyle. This finding may be explained by the following hypothesis: the cartilage tissue in the posterior lateral femoral condyle may be relatively intact due to the typical wear pattern of osteoarthritis in varus knees, allowing for more precise measurement of osteotomy volume without the variation caused by different degrees of cartilage degeneration seen in the posterior medial femoral condyle. Further studies are required for verification.
To prevent impingement at the posterior margin of femur and tibial plateau during TKA, it is crucial to restore the native anatomy of posterior femoral condyle, and avoid excessive osteotomy.10,11 By subtracting the actual implant thickness from the measured osteotomy thickness in posterior lateral femoral condyle, and analyzing its correlation with PCO changes, we concluded that posterior lateral femoral condyle osteotomy was the factor most directly associated with PCO alteration in TKA. Studies have indicated that a reduction in PCO by 3 mm or more can lead to a significant decrease in ROM, in contrast to those cases where the offset is restored to within 3 mm. Moreover, decreasing the PCO could also cause a paradoxical roll forward. 22 In light of these associations, it is important to prioritize the restoration of posterior femoral condyle morphology when designing 3D-printed patient-specific instruments, although this recommendation should be tested in future studies.
PTS is a crucial anatomical parameter in TKA, it is calculated from the posterior inclination at the medial tibial plateau on lateral knee X-ray imaging or computed tomography.26,27 A suitable PTS is a vital anatomical structure for maintaining anteroposterior stability, which also ensures the adequate gap to prevent tension during knee flexion. 28 Previous studies have also demonstrated that the PCO on normal knee anatomy was negatively related to the PTS. 29 In our study, to assess PCO restoration in TKA, patients were categorized into two groups: group 1 (<3 mm) and group 2 (≥3 mm). The 3 mm threshold for PCO difference was established based on prior research, which reported that a change of less than 3 mm in PCO is clinically acceptable in TKA. 22 The current study first found that patients with a change in PCO of 3 mm or more after TKA had a greater preoperative PTS, which suggested that preoperative PTS may be one of the indirect factors contributing to the variability of PCO. A possible explanation, based on existing literature indicating a negative correlation between PCO and PTS, involves the medial concavity of the tibial plateau, the firm connection between the meniscus and tibia, and the tight medial collateral ligament, which together may contribute to sagittal balance between flexion and stability. 30 However, this mechanistic interpretation remains speculative and requires further investigation. While 3D-printed patient-specific instruments can theoretically restore preoperative PTS and PCO perfectly, inherent implant design features necessitate a deliberate PCO reduction during preoperative planning to compensate for decreased PTS (lowered PTS, correspondingly lowered PCO).
Similarly, this study also found that patients with a PCO change of 3 mm or more following TKA exhibited a greater postoperative PTS alteration, which revealed that a greater PTS change may also be one of the indirect factors contributing to the variability of PCO. An increase in PCO and PTS can shift the contact point between the tibiofemoral components posteriorly, which in turn increases the quadriceps lever arm. This enhancement in movement efficiency can lead to a reduction the force required by quadriceps during knee flexion and extension, and patellofemoral contact stress. 24 However, an excessive PTS can further widen knee flexion gap, which is already enlarged due to PCL removal in posterior-stabilized TKA. If excessive PTS is allowed in TKA, it will cause knee posterior flexion instability and post-cam impingement.31,32 Integrating this study and prior evidence, we postulate that patients with a large preoperative PTS, increasing the postoperative PTS when designing 3D-printed patient-specific instruments could reduce the sacrifice of posterior femoral condyle morphology. However, this hypothesis requires validation in dedicated clinical studies. Whether it is necessary to perfectly restore preoperative PCO and PTS in TKA, is still necessary to explore and update the implant design concept. For example, custom knee implants can be used to match prosthesis geometric features with individual patient anatomy, while asymmetric prosthesis design is adopted to achieve more physiological postoperative kinematics. Previous studies have confirmed that a custom knee implant can obtain excellent coronal leg alignment, better rotational alignment and tibial component fit, and more natural knee kinematics. 33 However, due to the late appearance of custom implant designs and navigation techniques, there is no long-term follow-up result, so further follow-up is needed to confirm the advantages of these techniques in improving the durability of implant and postoperative function.
The current study also has several limitations: Firstly, despite overlapping the medial and lateral femoral condyles on lateral knee X-ray imaging as much as possible, there may still be inherent errors in the measurement of PCO and PTS. Secondly, study population was confined to an elderly demographic (54–81 years old), rather than encompassing a broader age spectrum. Consequently, these data might also have been influenced by pathological alterations associated with advanced knee arthritis. Thirdly, this study primarily evaluated PCO variability in TKA and analyzed its direct and indirect associated factors, but did not assess the potential impacts of PCO variation on functional recovery and postoperative rehabilitation. Long-term clinical follow-up is warranted to clarify whether PCO variation influences knee functional outcomes and prosthesis survival. Fourthly, a major conceptual limitation is that intraoperative adjustments (e.g., additional recutting of the posterior condyle or changes in component rotation) were allowed and not fully accounted for in the primary analysis. This introduces potential surgeon-dependent treatment heterogeneity, which may confound the observed associations with PCO change. Because intraoperative decision-making itself may be influenced by anatomical complexity or soft-tissue balance, it is difficult to disentangle whether observed PCO changes reflect preoperative factors or surgeon-driven modifications. Finally, this study was a prospective observational study, which was more inclined to a real-world study. Patients did not undergo randomization before TKA. Due to these limitations, we must approach our conclusions with caution and acknowledge the need for further randomized controlled, double-blind clinical trials with more rigorous design, which will help us to further clarify and verify the conclusions of this study.
Conclusion
This study revealed that PCO tends to decrease after posterior-stabilized TKA. A potential direct influencing factor associated with PCO variability was osteotomy of the posterior lateral femoral condyle. Preoperative PTS and a greater change in PTS are potential indirect factors contributing to PCO variability. These findings indicate that surgeons should attach importance to posterior femoral condyle morphology and individualization of preoperative planning based on PTS, rather than neglecting native anatomical features for standardized osteotomy. However, this non-randomized observational study cannot confirm causal relationships. Future rigorous randomized controlled trials are required to validate these findings and explore ways to lessen PCO variation in TKA.
Footnotes
Ethical approval
Ethical approval for this study was obtained from the Peking University International Hospital, Beijing, China (number 2020-036(BMR)).
Informed consent
All study participants provided informed consent.
Author's contributions
Junfeng Wang responsible for the conceptualization and design of the study, as well as the acquisition, analysis, and initial drafting of the manuscript. Bin Sun and Ke Zhang involved in the collation and analysis of the data. Bin Yang played a role in the study design, manuscript editing and revision.
Funding
This study was funded by the National Natural Science Foundation of China (12572364) and Peking University International Hospital Research Grant (YN2023ZD03).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.