
Abstract
Objective
This study aimed to investigate the associations of multi-dimensional lipid metabolism indicators, comprising serum lipid profiles and the degree of fatty infiltration in the musculoskeletal system, with bone mineral density (BMD) and bone turnover markers (BTMs), and to identify independent risk factors for the occurrence and severity of osteoporotic vertebral compression fractures (OVCFs) in postmenopausal women.
Methods
This retrospective study included a total of 133 postmenopausal women from January 2023 to July 2024. Participants were stratified by fracture status and vertebral compression severity. Clinical data, including bone and lipid metabolic indicators and BMD, were retrieved from electronic medical records and MRI reanalysis. Pearson correlation analyzed associations between lipid metabolic indicators and BTMs/BMD. Univariate and multivariate logistic regression analyses were performed to identify independent risk factors for OVCFs, with multicollinearity among variables assessed using the variance inflation factor (VIF), and ordinal logistic regression was applied to assess lipid metabolic indicators’ impact on vertebral compression severity. Statistical analyses included Student's t-test or Mann-Whitney U test for group comparisons and one-way analysis of variance (ANOVA) for multiple-group comparisons.
Result
This study included 133 participants: 34 controls, 32 with mild, 38 with moderate, and 29 with severe fractures. Age, BMI, BMD, vertebral bone quality (VBQ), the fatty infiltration ratio of the paraspinal muscles (FIR), and lipoprotein(a) [Lp(a)] differed significantly between fracture and control groups (all p < 0.05). VBQ and FIR were negatively correlated with total BMD (r = -0.466, p < 0.05; r = -0.455, p < 0.05) and positively correlated with the ratio of the fractured vertebra compressed sagittal cross-sectional area (RCSA) (r = 0.344, p < 0.05; r = 0.320, p < 0.05) and age (r = 0.615, p < 0.05; r = 0.283, p < 0.05). Univariate and multivariate regression analyses indicated that VBQ (p = 0.043; OR = 4.260, 95% CI: 1.046–17.345), FIR (p = 0.047; OR = 2.372, 95% CI: 1.010–5.572), and Lp(a) (p = 0.048; OR = 1.002, 95% CI: 1.002–1.799) were independently associated with an increased risk of OVCFs. Ordinal logistic regression confirmed VBQ (p = 0.006; OR = 3.168, 95% CI: 1.378–7.282) and FIR (p = 0.034; OR = 1.156, 95% CI: 1.009–1.325) were associated with increased fracture severity.
Conclusion
VBQ and FIR were independently associated with osteoporotic fractures in postmenopausal women and were further linked to fracture severity, suggesting their potential value in risk stratification and fracture severity assessment. Although Lp(a) showed a statistically significant association with OVCFs, the association was relatively weak, and its clinical significance requires further validation.
Keywords
Background
Postmenopausal osteoporosis (PMOP) is a metabolic bone disorder characterized by high bone turnover, primarily resulting from estrogen (E2) deficiency. Its pathological features include deterioration of bone microarchitecture and reduced bone mass. 1 These changes increase bone fragility and compromise mechanical stability, thereby significantly elevating the risk of fractures. Osteoporotic vertebral compression fractures (OVCFs), in particular, are a hallmark complication of osteoporosis. Against the backdrop of a globally aging population, the incidence of new vertebral fractures in women over 50 years of age reaches 10.7 per 1000 person-years, markedly higher than the rate of 5.7 per 1000 person-years in men. 2 OVCFs are often accompanied by persistent pain and functional limitations, substantially impairing patients’ daily activities and quality of life. In severe cases, complications such as spinal cord compression, vertebral collapse, and spinal deformities may occur, further exacerbating the healthcare burden. 3 Therefore, the accurate identification of high-risk individuals at an early stage is critical for the effective management of osteoporosis and the prevention of OVCFs.
OVCFs in postmenopausal women represent a common yet under-recognized clinical problem, characterized by difficulties in early identification and risk stratification. Currently, the diagnosis of osteoporosis is largely based on BMD assessment. However, osteoporosis is a complex multifactorial disorder involving genetic, aging-related, endocrine, immune, and gut microbiota–associated mechanisms.4,5 A proportion of postmenopausal women sustain fragility fractures even before their BMD reaches the diagnostic threshold for osteoporosis, indicating that reliance on BMD alone may be inadequate to meet the demands of precise diagnosis and risk stratification in clinical practice. 6
Accumulating evidence suggests that disordered lipid metabolism is associated with menopausal status and the development of OVCFs. Postmenopausal decline in E2 levels contributes to systemic lipid metabolic disorders through multiple mechanisms, thereby promoting ectopic adipose deposition and abnormalities in serum lipid profiles. Increased bone marrow adipose tissue (BMAT) within the vertebrae is significantly associated with trabecular bone loss and reduced spinal compressive strength. 7 Excessive accumulation of BMAT can produce lipotoxic metabolites such as palmitic acid, leading to alterations in the bone marrow microenvironment and disruption of bone metabolic homeostasis. 8 Similarly, fatty infiltration of the paraspinal muscles is a major determinant of impaired muscle strength and endurance, contributing to an increased risk of falls and fractures in postmenopausal women. This alteration represents a hallmark of paraspinal muscle degeneration.9,10 The liver is a central organ in regulating triglyceride (TG), total cholesterol (TC), and fatty acid metabolism to meet systemic energy demands. The decline in estrogen levels after menopause promotes the release of free fatty acids from adipose tissue, which are subsequently transported to the liver via the circulation, thereby enhancing lipid metabolic dysregulation. 11 Wen et al. reported that patients with OVCFs exhibited higher levels of total cholesterol and high-density lipoprotein compared to non-fracture controls. 12
Collectively, these findings suggest that dysregulated lipid metabolism may play a critical role in the pathogenesis of osteoporosis and OVCFs. The higher baseline body fat in women (approximately 27% vs. 15% in men), combined with postmenopausal hormonal changes, creates a physiological context that predisposes women to more severe lipid metabolic disturbances, thereby further accelerating bone loss. Although growing evidence has linked disordered lipid metabolism to OVCFs, existing studies have predominantly focused on circulating lipid parameters, with relatively limited investigation into ectopic fat deposition. Moreover, whether a direct link exists between circulating lipid profiles and ectopic fat accumulation remains unclear.
Objective
This study aimed to comprehensively evaluate multidimensional lipid metabolism indicators in postmenopausal women, including circulating lipid parameters and musculoskeletal fatty infiltration, and to investigate their associations with BMD, BTMs, and the severity of OVCFs. It is hoped that this study will aid in the early identification of postmenopausal women at high risk of osteoporotic vertebral compression fractures.
Methods
This was a retrospective case-control study including 99 postmenopausal women with OVCFs and 34 controls without fractures. This study was researcher-initiated and approved by Jiangsu Provincial Hospital of Chinese Medicine (YJZ202581). IRB of Affiliated Hospital of Nanjing University of Chinese Medicine (Jiangsu Province Hospital of Chinese Medicine) has approved this retrospective study and waived informed consent in accordance with the ethical principles of NHC: Measures for Guidelines on Ethical Review of Biomedical Research Involving Human Subjects (2023), WMA: Declaration of Helsinki and CIOMS: International Ethical Guidelines for Health-related Research Involving Humans.
Study population
This retrospective study enrolled female patients diagnosed with OVCFs who were admitted to the Department of Orthopedics at Jiangsu Provincial Hospital of Chinese Medicine between January 2023 and July 2024. The inclusion criteria were: (1) Women in menopause; (2) Complete medical records (including general information, BMD, MRI, BTMs and lipid profile); (3) Meeting diagnostic criteria for OVCFs 13 ; (4) Single-level thoracic or lumbar OVCFs (T11-L5); (5) Fracture site demonstrating hyperintense signal on T2-weighted fat-suppressed MRI images.
The exclusion criteria were as follows: (1) Patients with abnormal bone metabolism disorders, such as osteogenesis imperfecta, Cushing's syndrome, and osteomalacia; (2) Long-term use of medications that affect bone metabolism, such as glucocorticoids; (3) Participants who had previously enrolled in similar studies or received anti-osteoporosis drug therapy, such as alendronate sodium or teriparatide; (4) History of high-energy trauma, such as motor vehicle accidents or falls from height; (5) History of hip, spinal, or pelvic surgery.
Non-fracture controls were postmenopausal women who underwent lumbar MRI and BMD examination during the same study period. They were recruited from patients who visited our hospital for low back pain, spinal degeneration, or routine health check-up, without any history of vertebral fracture, high-energy trauma, or metabolic bone diseases. The flowchart illustrating the study population selection process is presented in Figure 1.
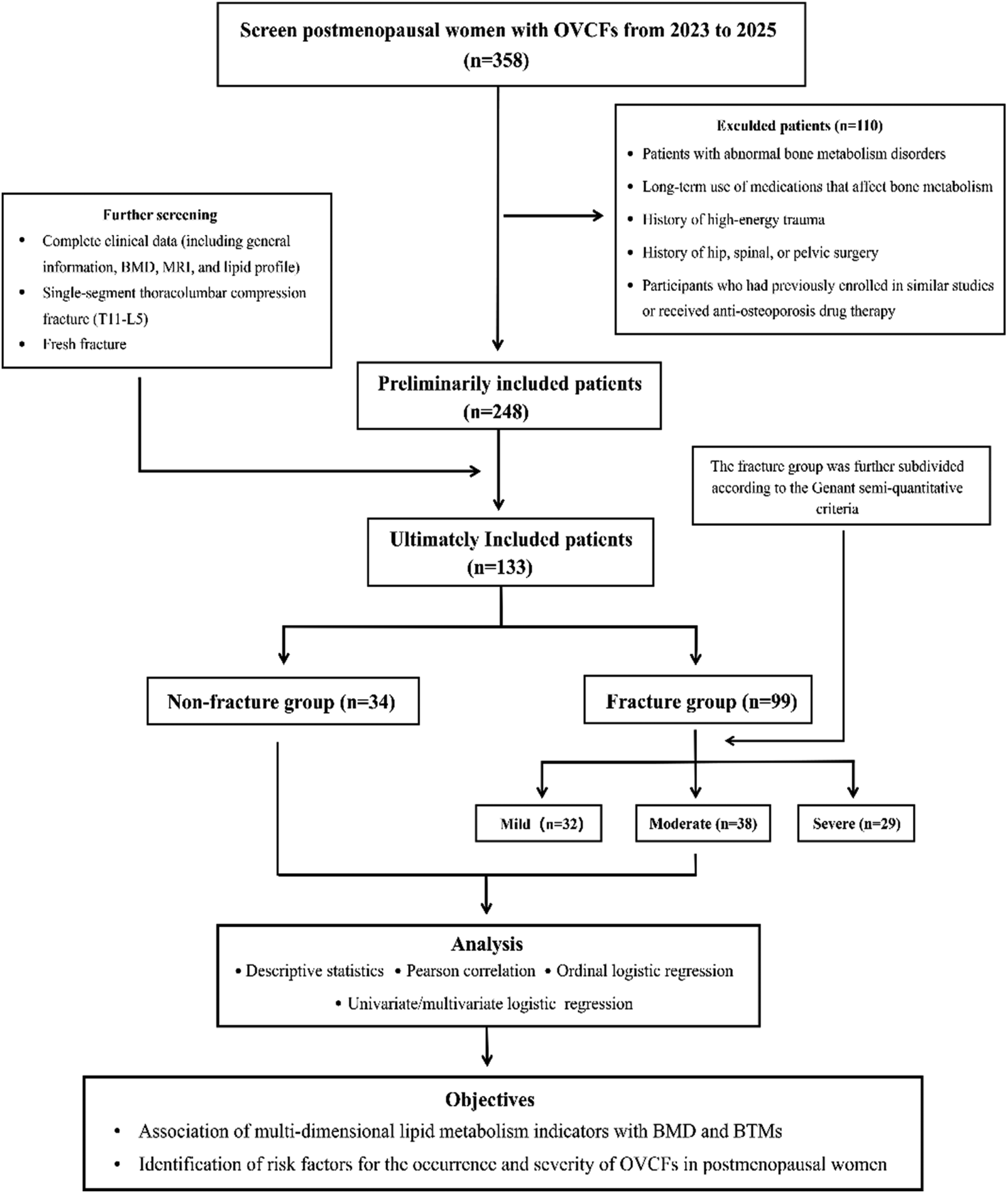
The flowchart of the study.
Lipid profiles and lumbar bone mineral density
Lipid profiles, BTMs, BMD and radiological data were extracted from the electronic medical records, with all measurements obtained during the same hospitalization period to ensure temporal consistency. Following hospitalization, blood sampling was generally performed first, with BMD and MRI examinations completed within one week. Fasting venous blood samples were collected for all laboratory analyses, which were performed using electrochemiluminescence immunoassay. The assessed lipid profiles included: TC, triglycerides, low-density lipoprotein (LDL), high-density lipoprotein (HDL), apolipoprotein A1 (ApoA1), apolipoprotein B (ApoB), apolipoprotein E (ApoE), Lp(a), and small dense LDL (sd LDL). BTMs consisted of: procollagen type I C-terminal propeptide (PICP), procollagen type I N-terminal propeptide (PINP), alkaline phosphatase (ALP), calcium, phosphorus, osteocalcin, and 25-hydroxyvitamin D [25-(OH)D]. BMD (g/cm2) for L1-L4 were measured using DXA on a Prodigy Advance system (General Electric Company, USA).
Imaging-related parameters
Images were obtained with a 1.5 T magnetic resonance scanner (Siemens, Germany), using a standard spine array coil. Imaging protocols included acquisition of axial and sagittal T1-weighted (repetition time/echo time, 450/16) and T2-weighted (repetition time/echo time, 3405/150) images (Figure 2. A-B). The data were evaluated by two radiologists with over 10 years of experience. The fracture group were classified based on the height of the anterior and posterior vertebral body on the midsagittal plane, according to the Genant Semiquantitative Criteria. The severity of OVCFs was graded as mild (approximately 20–25% reduction in anterior, middle, and/or posterior height and a reduction of area 10–20%), moderate (approximately 25–40% reduction in any height and a reduction in area 20–40%), or severe (approximately 40% reduction in any height and area) (Figure 2. C-E). 14
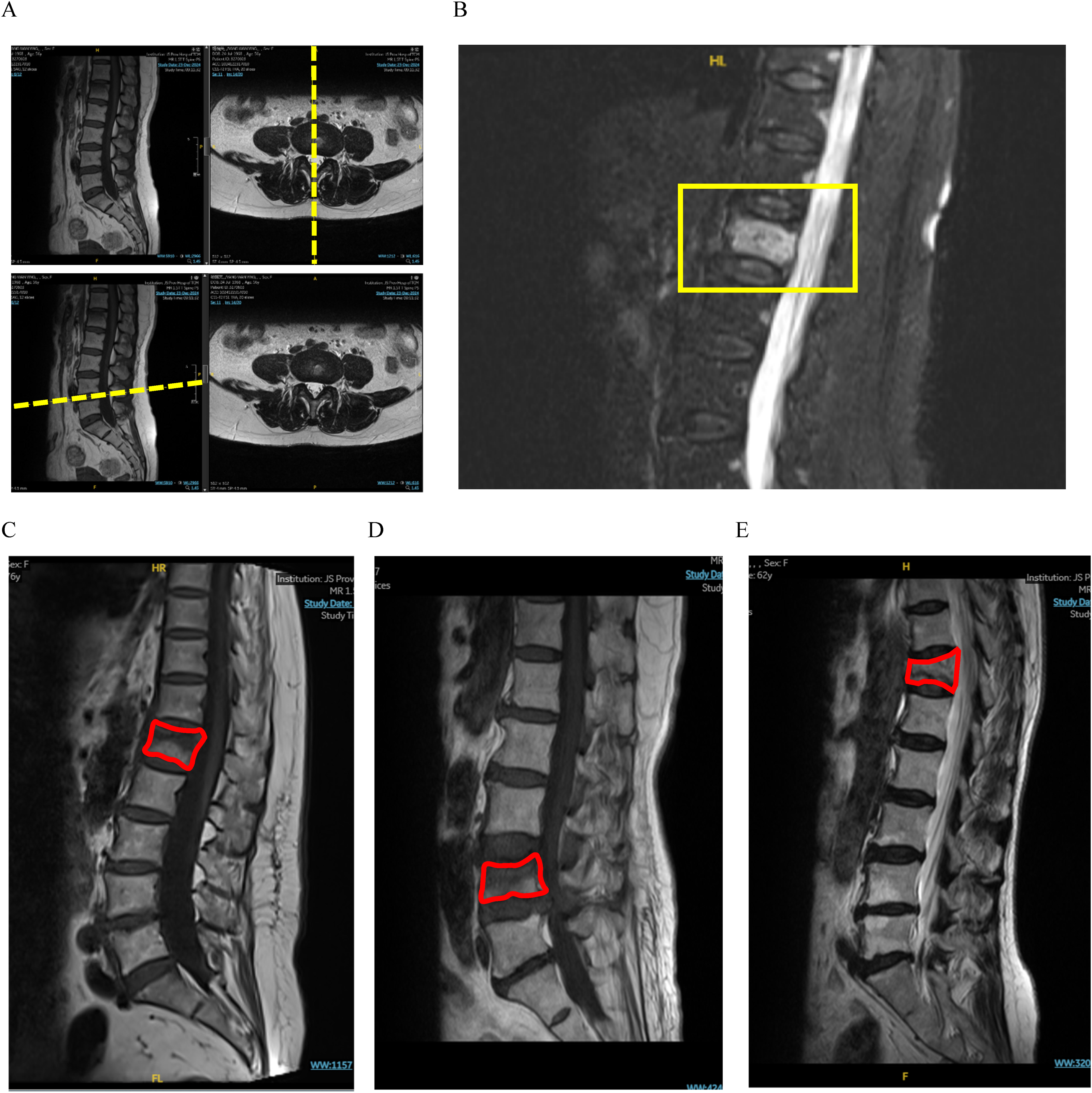
MRI assessment and representative examples of acute OVCFs with varying severity. A. Sagittal and axial localizer images illustrating the planes for quantifying vertebral compression, FIR, RCSA and VBQ; B. Sagittal T2-weighted fat-suppressed MRI revealing hyperintense signal (boxed) in vertebra, indicative of bone marrow edema and confirming an acute fracture; C-E. Representative sagittal MRI images demonstrating the grading scale: mild (C, <25% height loss), moderate (D, 25–40% height loss), and severe (E, >40% height loss). The affected vertebrae are delineated by outlines.
Fatty infiltration ratio of paraspinal muscles
Fatty infiltration parameters derived from MRI have been widely used to assess muscle quality and have demonstrated good reproducibility and reliability in previous studies.15,16 This study quantified fatty infiltration in the psoas major, erector spinae, and multifidus muscles (Figure 3-A). All measurements were performed using axial T2-weighted MRI processed with FIJI software (http://fiji.sc/Fiji). 17 The analysis followed a standardized protocol: first, the total cross-sectional area (CSA) of each muscle was obtained by manual tracing of muscular boundaries at the L4-L5 intervertebral level, using fascial planes as anatomical guides. Following this, adipose tissue was differentiated from muscle tissue using threshold segmentation techniques. After the optimal threshold for adipose tissue was manually determined, adipose tissue on axial T2-weighted MR images was converted to red to obtain the FCSA. 18 FIR was then calculated using the following formula: FIR = FCSA / CSA (Figure 3-B).
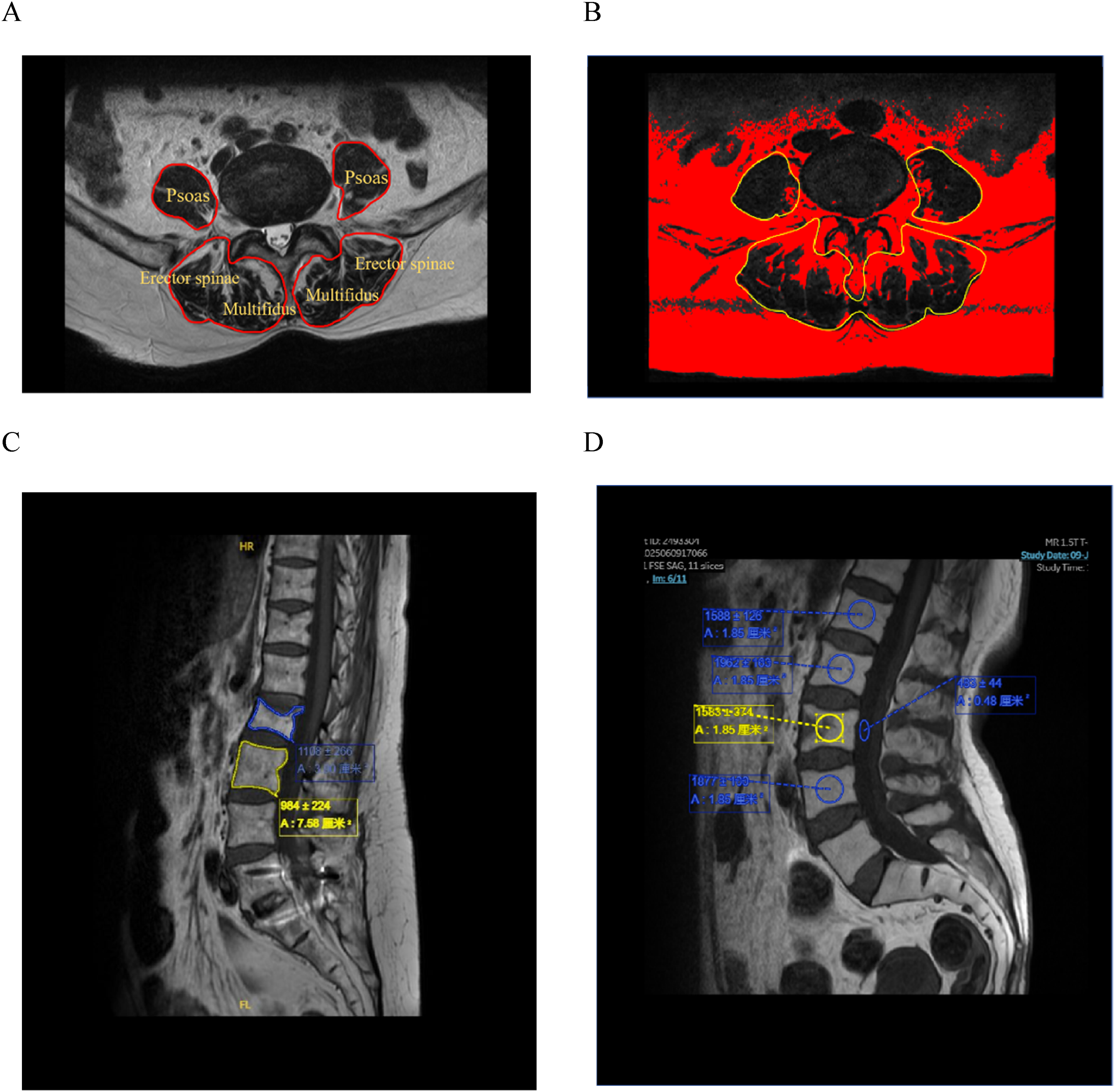
Method for analyzing the degree of fatty infiltration in paraspinal muscles and vertebral body. A. Axial T2-weighted MRI at the L4-L5 level demonstrating the distribution of paraspinal muscle, respectively: Psoas, Erector spinae, and Multifidus; B. Quantification of FIR in the paraspinal muscles using threshold segmentation techniques; C. PACS-based vertebral body outlining for RCSA calculation; D. PACS-based signal intensity analysis for VBQ score calculation.
The ratio of the fractured vertebra compressed sagittal cross-sectional area
Vertebral compression severity is traditionally evaluated based on the degree of vertebral height loss. More recently, the sagittal cross-sectional area ratio has emerged as a widely used imaging-based parameter for assessing vertebral compression, enabling more precise quantification of fracture extent, objective evaluation of compression severity, and enhanced accuracy and reliability in group stratification.19,20 This approach enables quantitative assessment of compression degree and ensures the accuracy of grouping. The axial position is located in the middle of the sagittal plane, where the sagittal T2-weighted image of the fracture site is acquired. Image analysis was conducted using ImageJ software. With the image selection tool, the boundaries of the fractured vertebra and the normal vertebra below it were manually delineated on the sagittal T2-weighted image of the fracture site. Subsequently, ROI parameters were measured, including the fracture vertebral sagittal cross-sectional area (FSCSA) and the normal vertebral sagittal cross-sectional area (NSCSA). The RCSA calculation formula is as follows: RCSA = (NSCSA - FSCSA) / NSCSA (Figure 3-C). To facilitate subsequent correlation analysis, the RCSA for the non-fracture group was standardized as the sagittal cross-sectional area of the L2 vertebra /sagittal cross-sectional area of the L3 vertebra.
Vertebral bone quality score
The VBQ score is a measure of bone quality based on MRI T1-weighted signal intensity, first proposed by Ehresman. 21 It has been validated as a reliable surrogate marker of bone quality and reflects the level of vertebral marrow fatty infiltration, with higher scores indicating greater fat content within the vertebral body. 22 VBQ score is the ratio of the median L1–L4 signal intensity (SI) and L3 cerebral spinal fluid (CSF) SI, VBQ (L1−4) Score = Median (SI L1−L4 )/SI L3 CSF. 23 All images were assessed and analyzed using PACS software. Place ROI within each vertebral body from L1 to L4 to calculate the average signal intensity within the region. ROI excludes cortical bone by placing concentric ROIs approximately 0.3 cm from the vertebral body perimeter (Figure 3-D). If a vertebral body is severely compressed, it is excluded from calculations, and the VBQ score is calculated using the remaining vertebral bodies. The signal intensity of cerebrospinal fluid (CSF) is measured at the L3 level. When this is not feasible due to obstruction (e.g, L3 spinal canal stenosis), CSF at the L2 or L4 level is used.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Sciences (version 22.0; SPSS Inc., Chicago, IL, USA). If the continuous variable followed a normal distribution, it was expressed as mean ± standard deviation, and if it did not follow a normal distribution, it was expressed as median (lower quartile, upper quartile). Intraclass correlation coefficients (ICC) were used to assess the intra-rater reliability and inter-rater reliability of VBQ, FIR, and RCSA. Variants between the control and fracture groups were analyzed using a t-test or Mann-Whiteny U test. One-way ANOVA was used for multiple-group comparisons, followed by Tukey's multiple comparisons test for post-hoc pairwise analysis. Correlation analysis employed Pearson's correlation coefficient. Univariate and multivariate logistic regression screened independent risk factors for OVCFs. VIF was used to assess multicollinearity among the variables included in the model. Ordinal logistic regression models explored the influence of lipid metabolism indicators on vertebral compression severity, using OVCFs presence as the dependent variable and lipid metabolism indicators as explanatory variables, while adjusting for confounding factors including age, BMI, and BMD. Statistical significance was set at p < 0.05.
Results
Participant characteristics
This retrospective study enrolled 133 postmenopausal women from Jiangsu Provincial Hospital of Chinese Medicine, comprising 34 control subjects without fractures and 99 patients with osteoporotic vertebral compression fractures. Table 1 presents the demographic and clinical characteristics of all participants. Given that VBQ, FIR, and RCSA measurements require manual delineation, which inherently introduces potential measurement variability, we implemented a rigorous reliability assessment. Therefore, data from 133 patients were independently measured by two physicians. The inter-rater reliability assessed by ICC, demonstrated excellent agreement: VBQ (ICC=0.928, 95% CI = 0.900–0.948), FIR (ICC=0.905, 95% CI = 0.869–0.932), and RCSA (ICC=0.840, 95% CI = 0.782–0.884). All ICC values exceeded 0.8, indicating strong measurement consistency (Figure 4).
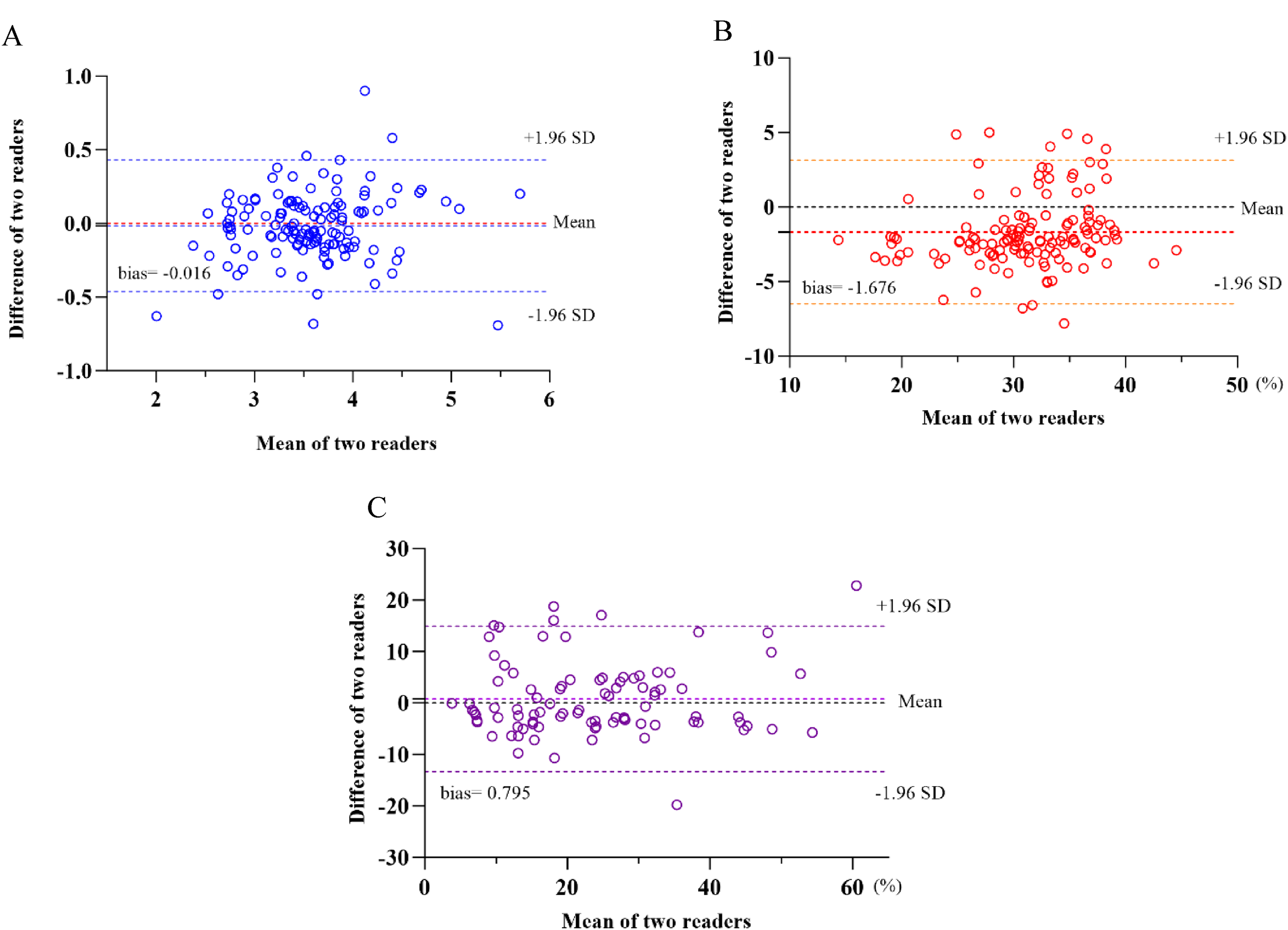
Bland-Altman plots of two readers for imaging-related parameters. A. VBQ; B. FIR; C. RCSA.
General demographic and clinical characteristics of participants.
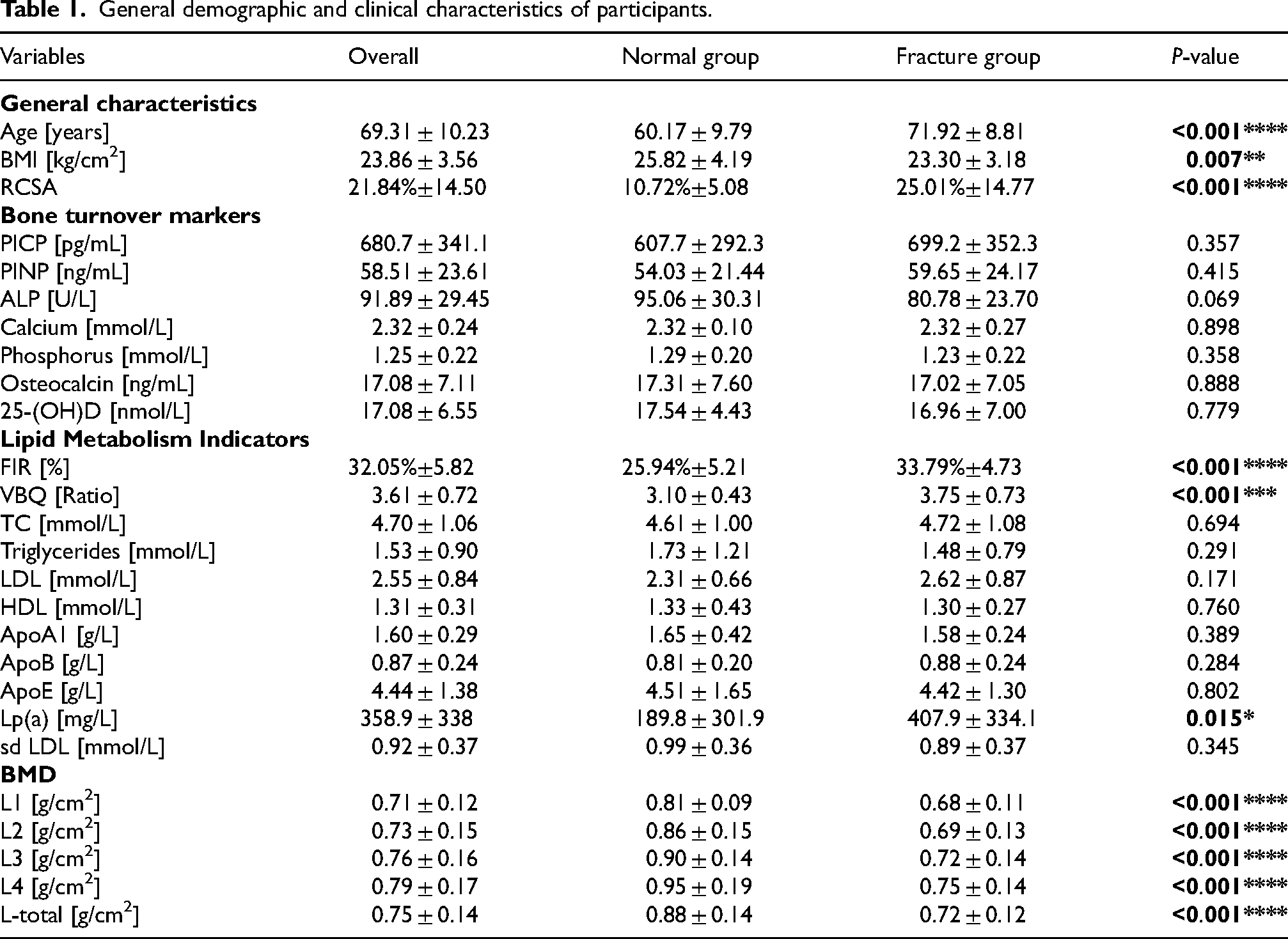
The mean age of all participants was 69.31 ± 10.23 years, ranging from 50 to 89 years. The mean BMI was 23.86 ± 3.56, ranging from 15.62 to 35.01. Significant differences were observed in both age and BMI between the fracture and control groups. Increasing age was associated with a significant increase in the incidence of osteoporotic vertebral compression fractures. Conversely, higher BMI values may represent a potential protective factor against fracture occurrence. BMD remains a critical predictor of fracture risk. Bone mineral density was generally higher in the normal group than in the fracture group, whether measured at individual vertebrae (L1-L4) or as overall bone density. Among lipid metabolism indicators and BTMs, VBQ, FIR, and Lp(a) were significantly elevated in the fracture group, while no statistically significant differences were observed in the remaining indicators (Table 1).
Correlation between lipid metabolism indicators and general characteristics, BTMs, and BMD
Pearson correlation analysis, visualized in the heatmap (Figure 5), revealed several significant associations among lipid metabolism indicators, BMD, general characteristics, and BTMs. FIR and VBQ were negatively correlated with total BMD (r = -0.466, p < 0.05; r = -0.455, p < 0.05), while positively correlated with RCSA (r = 0.344, p < 0.05; r = 0.320, p < 0.05) and age (r = 0.615, p < 0.05; r = 0.283, p < 0.05). Regarding associations between lipid metabolism indicators and BTMs, ALP showed significant positive correlations with multiple indicators, including FIR (r = 0.239, p < 0.05), TC (r = 0.250, p < 0.05), LDL (r = 0.272, p < 0.05), ApoB (r = 0.289, p < 0.05), and sd LDL (r = 0.358, p < 0.05).
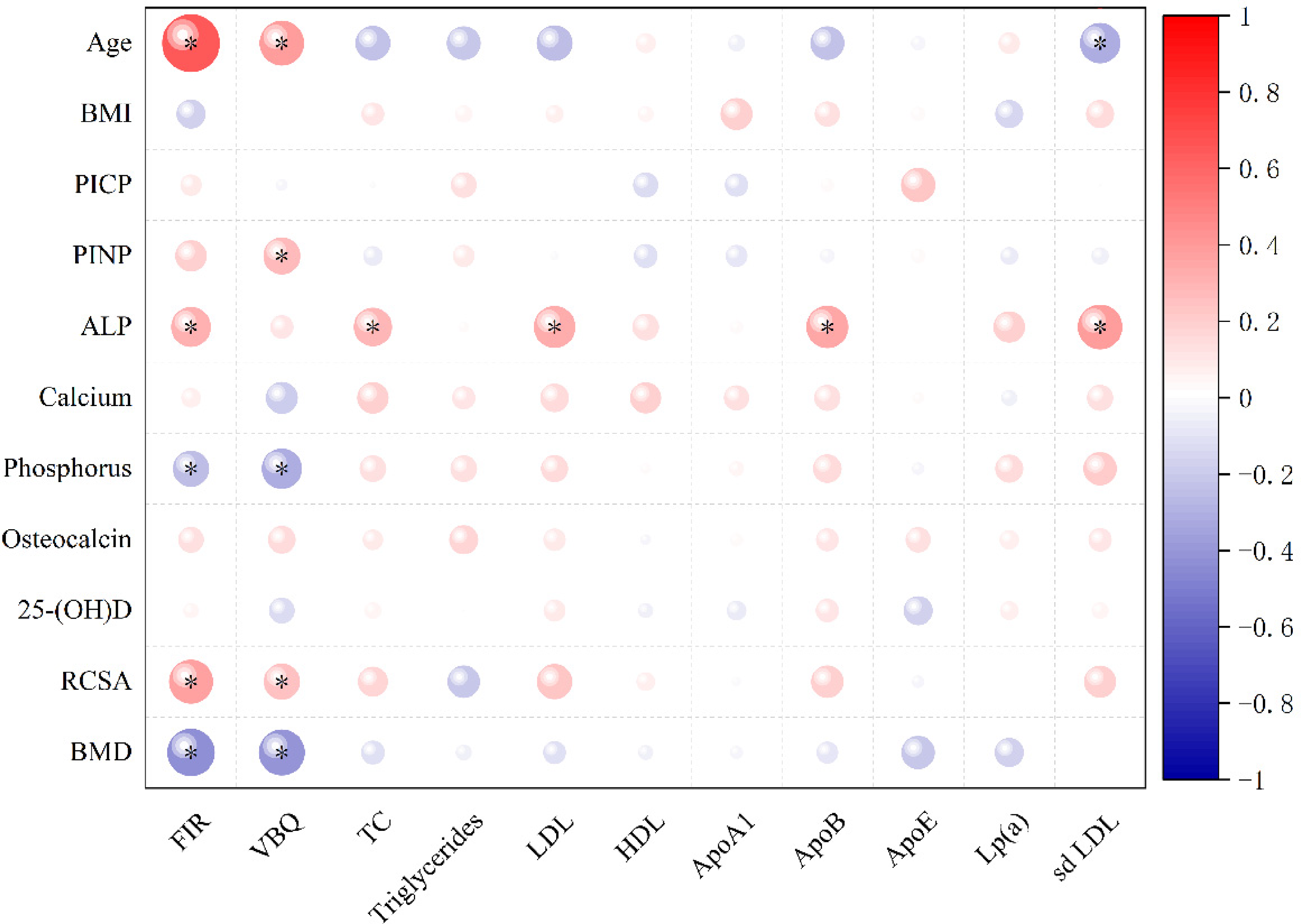
Correlation heatmap of lipid metabolism indicators with clinical characteristics, BMD, and BTMs. Note: This figure visualizes Pearson correlation coefficients.Significant correlations (p ≤ 0.05) are displayed, and the magnitude of each correlation is represented by the size of the circle, with larger circles corresponding to stronger associations.
Logistic regression analysis of lipid metabolism indicators and the occurrence of OVCFS
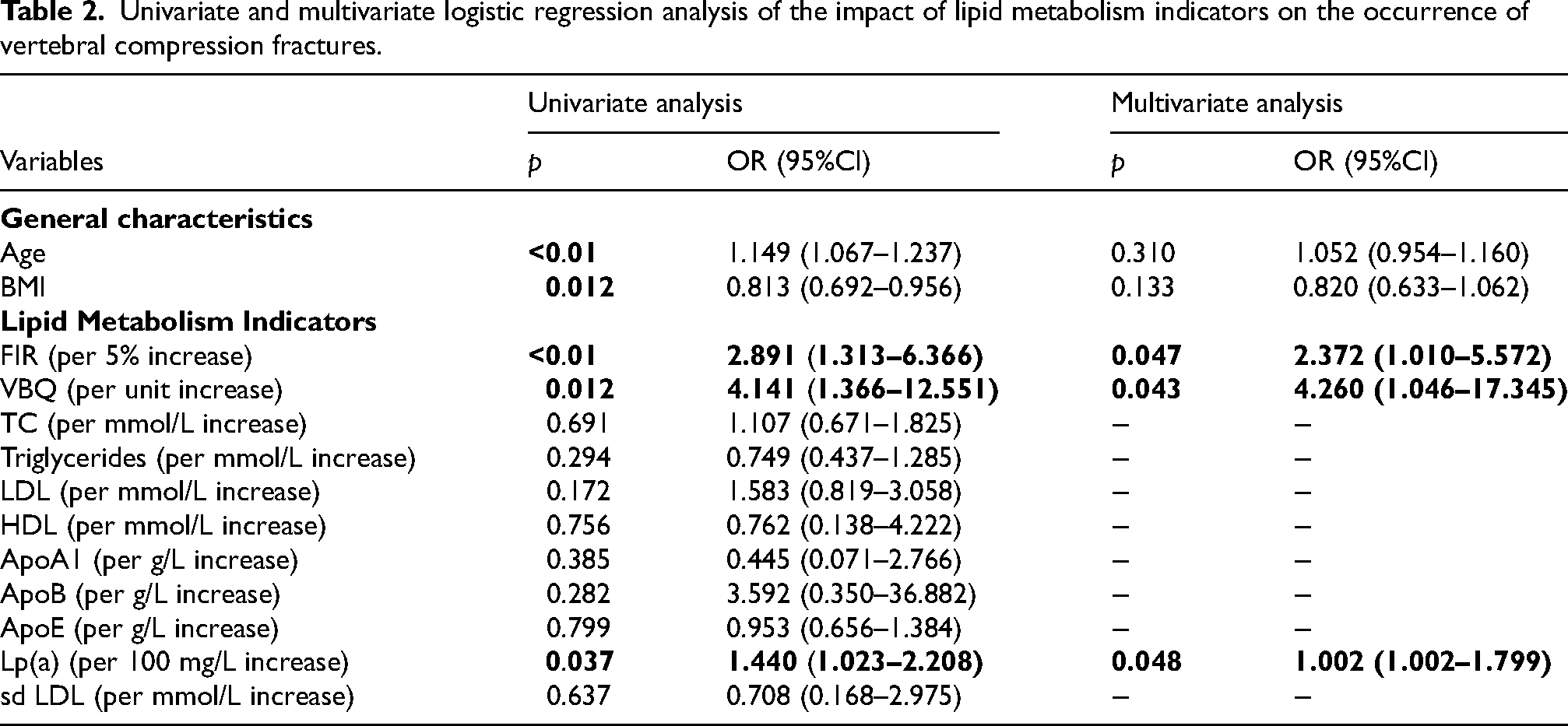
Univariate and multivariate logistic regression analyses were performed to evaluate the association between lipid metabolism indicators and OVCFs. In univariate analysis, Age (p < 0.01; OR = 1.149, 95% CI: 1.067–1.237), BMI (p = 0.012; OR = 0.813, 95% CI:0.692–0.956), FIR (p < 0.01; OR = 2.891, 95% CI: 1.313–6.366), VBQ (p = 0.012; OR = 4.141, 95% CI: 1.366–12.551), and Lp(a) (p = 0.037; OR = 1.440, 95% CI: 1.023–2.208) were significantly associated with OVCFs. Other lipid parameters, including TC, triglycerides, LDL, HDL, ApoA1, ApoB, ApoE, and sd LDL, did not demonstrate significant associations. Furthermore, collinearity diagnostics indicated that all VIFs were < 5, suggesting no significant multicollinearity among the included variables. Therefore, based on the results of the univariate analysis, variables with P < 0.05 (including age, BMI, VBQ, FIR, and Lp(a)) were entered into the multivariate logistic regression model to identify factors independently associated with the occurrence of osteoporotic vertebral compression fractures.
After adjusting for age and BMI in the multivariate analysis, FIR (p = 0.047; OR = 2.372, 95% CI: 1.010–5.572), VBQ (p = 0.043; OR = 4.260, 95% CI: 1.046–17.345), and Lp(a) (p = 0.048; OR = 1.002, 95% CI: 1.002–1.799) remained statistically significant independent predictors of OVCFs. These findings suggest that FIR, VBQ, and Lp(a) are significant lipid metabolism indicators associated with the risk of OVCFs, even after controlling for potential confounding factors. However, compared with FIR and VBQ, the association between Lp(a) and OVCFs was relatively weak (Table 2).
Univariate and multivariate logistic regression analysis of the impact of lipid metabolism indicators on the occurrence of vertebral compression fractures.
Subgroup analysis based on fracture compression severity
Based on the degree of vertebral compression, the patients were further stratified into mild, moderate, and severe compression subgroups for additional analysis (Table 3). RCSA revealed significant differences in compression area among the mild, moderate, and severe groups, indicating that the included patients demonstrated good differentiation. Analysis of variance revealed that age and BMI—which had shown significant differences in the initial analysis of fracture occurrence—were not statistically different among the compression-based subgroups. Among BTMs, PICP showed a significant difference (p = 0.011), with levels increasing progressively with compression severity. ALP also exhibited an upward trend in the moderate and severe groups, although the difference was not statistically significant (p = 0.052). Regarding lipid metabolism indicators, FIR, VBQ, and most vertebral BMD measurements remained significantly different across subgroups. Higher FIR and VBQ values, together with lower BMD, were consistently associated with more severe vertebral compression fractures. Figure 6 shows the distribution of lipid metabolism indicators across different groups.
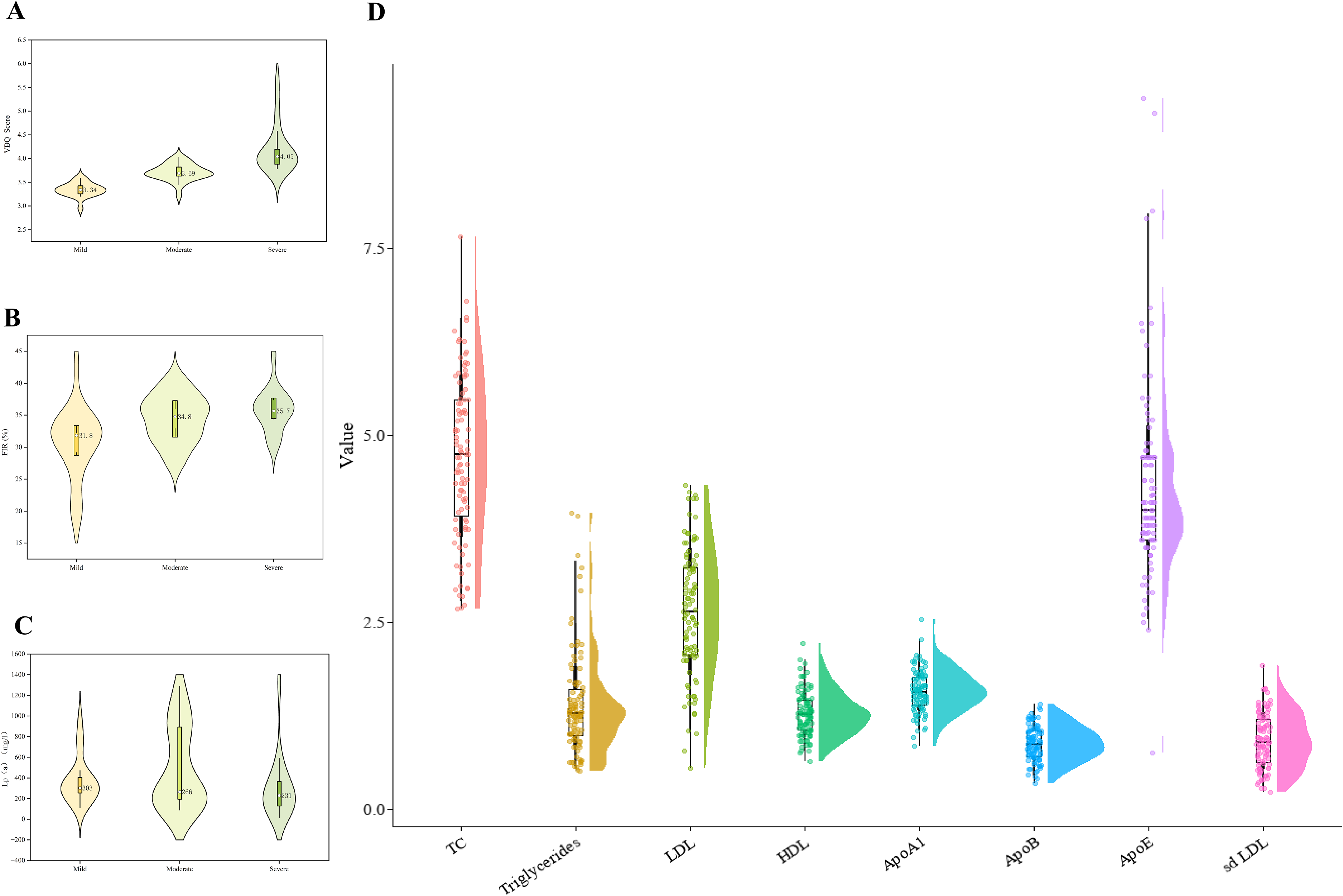
Data Distribution Chart for Lipid Metabolism Indicators. A: VBQ; B: FIR; C: Lp(a); D: TC, Triglycerides, LDL, HDL, ApoA1, ApoB, ApoE, and sd LDL.
ANOVA between patients in the mild, moderate, and severe fracture groups.
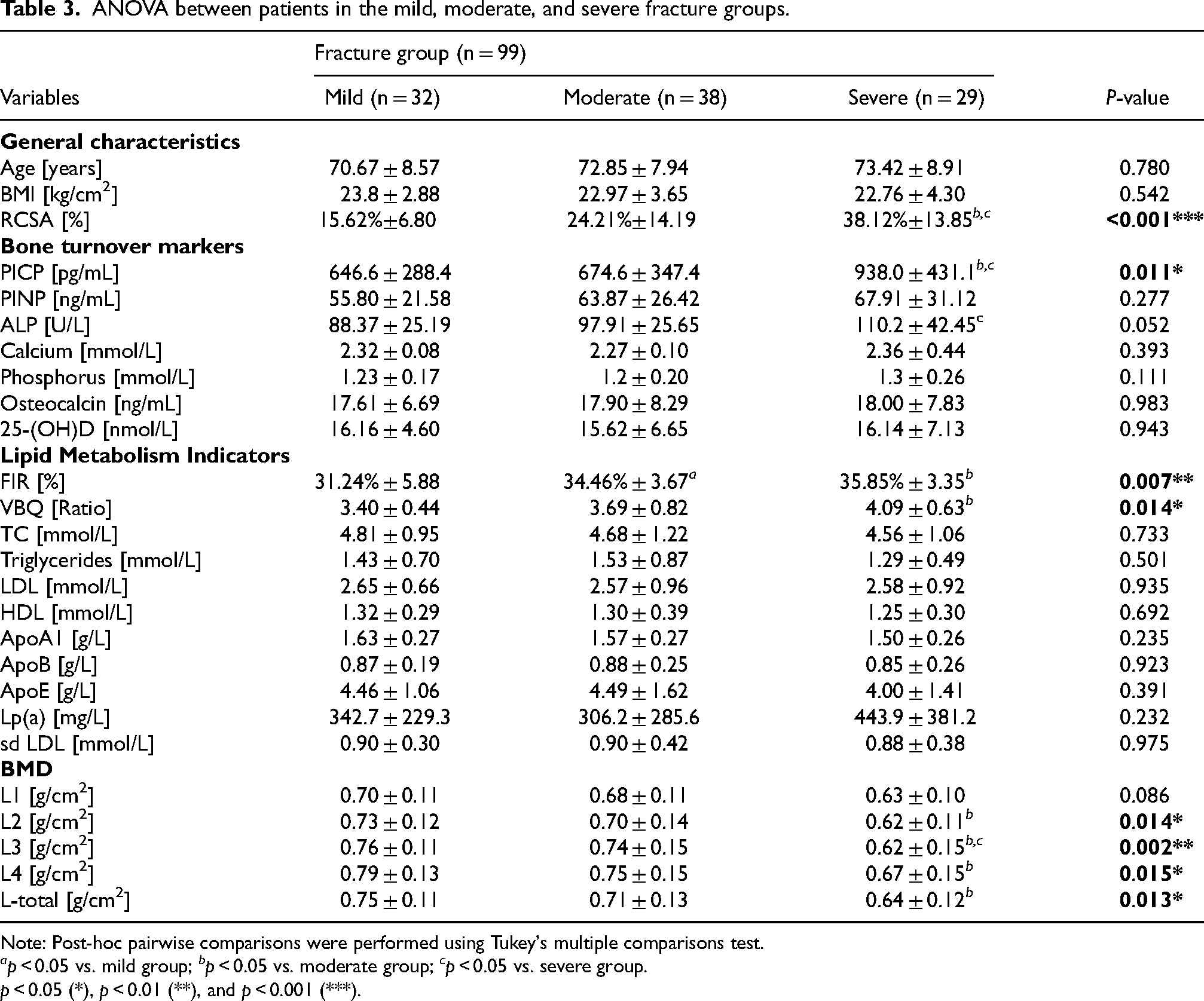
Note: Post-hoc pairwise comparisons were performed using Tukey's multiple comparisons test.
ap < 0.05 vs. mild group; bp < 0.05 vs. moderate group; cp < 0.05 vs. severe group.
p < 0.05 (*), p < 0.01 (**), and p < 0.001 (***).
Ordinal logistic regression analysis for screening lipid metabolism indicators affecting fracture compression severity
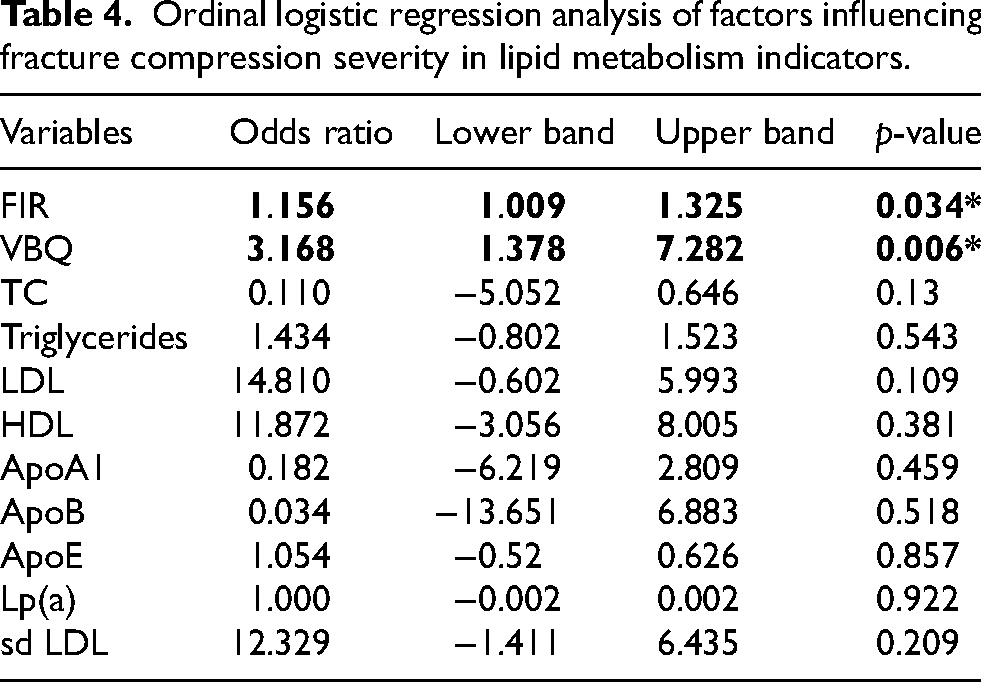
An ordinal logistic regression analysis was performed to assess the relationship between lipid metabolism indicators and vertebral compression severity (Table 4). The parallel lines test indicated no violation of the proportional odds assumption (p = 0.78), confirming the model's appropriateness for the data. The analysis revealed that FIR (OR = 1.156, 95% CI: 1.009–1.325; p = 0.034) and VBQ (OR = 3.168, 95% CI: 1.378–7.282; p = 0.006) were statistically significant risk factors associated with increased severity of vertebral compression. In contrast, other lipid-related variables did not show significant associations (all p > 0.05). These results suggest that FIR and VBQ are independently associated with the severity of vertebral compression, highlighting their potential clinical relevance in the assessment and management of vertebral fractures.
Ordinal logistic regression analysis of factors influencing fracture compression severity in lipid metabolism indicators.
Discussion
Osteoporotic vertebral compression fractures have become a major public health concern among postmenopausal women. A nationwide cross-sectional study conducted in 2021 reported that the prevalence of OVCFs among Chinese women aged 40 years and older has reached 9.7%. 24 Although current clinical guidelines recommend DXA screening for individuals aged 65 years and above, adherence remains suboptimal due to financial burden and limited accessibility in primary care settings. Moreover, DXA assessment has certain limitations in evaluating the risk of fragility fractures. 25 Lipid metabolism disorders are closely associated with accelerated bone loss, and related indicators may serve as potential predictive biomarkers for the auxiliary diagnosis of osteoporosis in PMOP. In this context, the present study systematically evaluated the associations between multidimensional lipid metabolism indicators and general clinical characteristics, BTMs, and BMD in postmenopausal women. Our findings suggest that lipid metabolic dysregulation, particularly ectopic fat deposition within the musculoskeletal system, play a critical role in the development of osteoporosis and contribute to the occurrence and progression of OVCFs.
A total of 133 postmenopausal women with OVCFs were enrolled, including 34 in the non-fracture group and 99 in the fracture group. Comparative analysis revealed significant differences between the fracture and non-fracture groups in several parameters: age, BMI, BMD, VBQ, FIR, and Lp(a) levels. Advanced age, higher VBQ, elevated FIR, and increased Lp(a) were identified as potential risk factors for vertebral compression fractures, whereas higher BMD and BMI appeared to exert protective effects. Pearson correlation analysis revealed that VBQ and FIR were significantly negatively correlated with BMD, while showing significant positive correlations with age and RCSA, suggesting that increased fatty infiltration is closely associated with bone loss and age-related degenerative changes. In contrast, the present study did not observe significant associations between circulating lipid parameters and BMD or BTMs, which is inconsistent with some previous reports. Earlier studies have suggested that lipid metabolism indicators such as TC and HDL differ significantly in patients with OVCFs and those with recurrent fractures after surgery.12,26 Several factors may account for these discrepancies. First, many previous studies were conducted in single-center settings, with differences in study populations and sample characteristics. Second, circulating lipid levels are regulated by multiple organ systems, including the liver and intestine, and primarily reflect systemic metabolic status rather than local bone microenvironmental changes. Therefore, these factors may, at least in part, explain the inconsistencies observed across different studies. Conversely, VBQ and FIR, as site-specific indicators, can more directly reflect aberrant metabolism and structural deterioration within the bone microenvironment, thereby exhibiting higher specificity in identifying fracture risk. Subsequently, univariate and multivariate logistic regression analyses were performed to identify independent risk factors for fracture among lipid metabolism indicators. After adjustment for confounding factors including age and BMI, VBQ, FIR, and Lp(a) remained independently associated with OVCFs. However, compared with FIR and VBQ, the association between Lp(a) and OVCFs was relatively weak. Currently, evidence does not support a direct association between Lp(a) levels and osteoporosis or OVCFs. Instead, elevated Lp(a) has been predominantly associated with atherosclerotic cardiovascular disease and increased all-cause mortality. 27 Within the frameworks of the “calcification paradox” and bone-vascular coupling, Lp(a) may indirectly affect vertebral fracture risk via vascular dysfunction. Through bone–vascular crosstalk, Lp(a)-related atherosclerosis and lipid metabolic disturbances may impair bone homeostasis, thereby contributing to osteoporosis progression and fracture risk. 28 Further investigations are warranted to validate these findings.
The fracture group was subsequently stratified into mild (n = 32), moderate (n = 38), and severe (n = 29) subgroups based on the Genant semi-quantitative criteria and RCSA. Among the parameters evaluated, lumbar spine BMD retained significant discriminatory power across the compression severity subgroups. In contrast, other parameters such as age, BMI, and Lp(a), which were significant in the initial group comparison, showed no significant differences in this subgroup analysis. Notably, the lipid metabolism indicators FIR and VBQ continued to demonstrate significant differences. This finding was further confirmed by ordinal logistic regression analysis targeting vertebral compression severity. These results suggest that VBQ and FIR may be implicated not only in the initial fracture occurrence but also in the progression of vertebral collapse, thereby offering a novel perspective for stratifying disease severity.
The VBQ score, derived from T1-weighted MRI signal intensity, reflects the extent of vertebral fatty infiltration and serves as an indirect biomarker of bone quality. BMAT accounts for approximately 70% of adult marrow volume and 10% of total body fat, with its content progressively increasing under conditions such as aging and postmenopausal estrogen deficiency. 29 In the present study, the mean VBQ value was 3.61 ± 0.72, which aligns with previous findings. Li et al. reported that VBQ values in postmenopausal women were significantly higher than 3.0 and exhibited a progressive increase with decreasing BMD. 23 Furthermore, studies by Özmen and Gassert have further corroborated the value of VBQ as an independent predictor of OVCFs,30,31 demonstrating that patients with osteopenia or osteoporosis exhibit significantly higher vertebral fat content compared to non-osteoporotic fracture controls.
The paraspinal muscles, serving as a key structure for maintaining dynamic spinal stability, play a critical role in the pathogenesis of spinal disorders. Muscle degeneration is primarily characterized by fatty infiltration, a process in which muscle fibers are progressively replaced by adipose tissue. Such degenerative changes may alter mechanical loading patterns and compromise the balance of the spine. Our study revealed that increased fat content in the paraspinal muscles was significantly associated with a higher risk of OVCFs and negatively correlated with lumbar BMD. Muscle and bone tissues share a common origin in mesenchymal stem cells, and this ontogenetic relationship underlies their functional interdependence, which has attracted growing interest in the association between sarcopenia and osteoporosis. Recent studies have even proposed the integrative concept of “osteosarcopenia”. A meta-analysis by Chen et al. demonstrated that patients with incident vertebral fractures exhibited significantly greater fatty infiltration in the paraspinal muscles compared to the non-fracture group (SMD: 0.768, 95% CI: 0.475–1.062), 32 and such infiltration was associated with an increased risk of vertebral refracture. Studies by Huang and Roig further confirmed that paraspinal muscle fatty infiltration was positively correlated with the severity of OVCFs in postmenopausal women, while improved muscle mass was shown to enhance bone microstructural parameters.19,33
Currently, techniques such as Dixon MRI and magnetic resonance spectroscopy (MRS) are widely used for the assessment of bone marrow fat content.34,35 However, these methods usually require specific imaging sequences and complex post-processing procedures, with relatively high demands on equipment and operator expertise, thereby limiting their routine clinical application. VBQ and FIR can be measured opportunistically from routine lumbar MRI without additional sequences. Radiology departments could integrate them into standard reporting templates to support fracture risk stratification. Therefore, VBQ and FIR demonstrate favorable clinical accessibility and application potential, particularly for large-scale population screening and routine clinical risk assessment.
Conclusion
This study demonstrated that MRI-derived VBQ and FIR were independently associated with OVCFs in postmenopausal women and may be useful for identifying individuals at high risk of fracture. In addition, both indicators showed potential clinical value in assessing the severity of vertebral compression. Although Lp(a) showed statistical significance, its association with OVCFs was relatively weaker than that of VBQ and FIR, and its clinical validity and utility still require further validation in larger-scale studies.
From a clinical application perspective, VBQ and FIR data can be obtained simultaneously without additional examinations in postmenopausal women undergoing routine lumbar MRI for low back pain or degenerative spinal disorders. Elevated levels of these indicators may help prompt further osteoporosis-related examinations, thereby facilitating early risk identification and preventive intervention.
Limitations
However, this study has several limitations. As a single-center retrospective investigation, although multiple confounding factors were adjusted for, the potential for selection bias and unmeasured confounders cannot be fully excluded. In addition, the limited sample size may affect the generalizability of our findings. Notably, due to inherent study limitations, the temporal relationship between lipid metabolism disorders and the occurrence of OVCFs cannot be established. It remains unclear whether lipid abnormalities act as predisposing factors for fracture development or represent secondary changes following fracture events.
Recommendations
Future large-scale, multicenter prospective studies are warranted to further validate the role of lipid metabolism indicators in the risk prediction and disease assessment of osteoporosis and osteoporotic fractures in postmenopausal women. On this basis, it would be valuable to develop a risk prediction model integrating lipid metabolism–related indicators, such as VBQ and FIR, to enable precise risk stratification and comprehensive management of OVCFs. It should be emphasized that the present study primarily focused on the role of lipid metabolism indicators in the occurrence and progression of osteoporotic fractures. However, fracture development is a multifactorial process; therefore, these lipid parameters should not be used as standalone predictors in clinical practice but rather interpreted in combination with other relevant factors.
Footnotes
Acknowledgements
We Acknowledge all those who participated in the revision of the manuscript.
Ethics approval and consent to participate
Institutional Review Board of Affiliated Hospital of Nanjing University of Chinese Medicine (Jiangsu Province Hospital of Chinese Medicine) has approved this retrospective study and waived informed consent in accordance with the ethical principles of NHC: Measures for Guidelines on Ethical Review of Biomedical Research Involving Human Subjects (2023), WMA: Declaration of Helsinki and CIOMS: International Ethical Guidelines for Health-related Research Involving Humans (YJZ202581).
Consent for publication
Not applicable.
Authors’ contributions
Yihua Zhu, Qian Cheng, Qitai W, and Jiaxin Liu spearheaded and supervised all the trials. Yang Guo, Lining Wang, Yong Ma designed the study and trials. Tianchi Zhang, Wumiti Taxi, Kaixuan Wang, Xi Chen, Qinfeng Zhou, and Cong Wang conducted the trials and analyzed the data. Yihua Zhu, Qian Cheng wrote and revised the manuscript. All authors reviewed and approved the final version of the manuscript, ensuring integrity and accuracy in all aspects of the work.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the the National Natural Science Foundation of China, the Natural Science Foundation of Jiangsu Province, the Natural Science Foundation of the Jiangsu Higher education Institution of China, the NATCM's Project of High-level Construction of Key TCM Disciplines, the Jiangsu CM Clinical Innovation Center of Degenerative Bone & Joint Disease (grant number No.82074458, No.82174411, No.BK20220470, No.BK20221351, No.22KJB360012, NATCM's Human Education Letter[2023]No. 85, Jiangsu science and education of traditional Chinese medicine[2021]No. 4).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical trial number
Not applicable.
Abbreviations
Osteoporotic vertebral compression fractures (OVCFs); Postmenopausal osteoporosis (PMOP); dual-energy X-ray absorptiometry (DXA); the ratio of the fractured vertebra compressed sagittal cross-sectional area (RCSA); Vertebral bone quality (VBQ); the fat infiltration ratio of the paraspinal muscles (FIR); the fracture vertebral sagittal cross-sectional area (FSCSA); lipoprotein(a) [Lp(a)]; total cholesterol (TC); Low-density lipoprotein (LDL); High-density lipoprotein (HDL); Apolipoprotein A1 (ApoA1); Apolipoprotein B (ApoB); Apolipoprotein E (ApoE); small dense LDL (sd LDL); Procollagen type I C-terminal propeptide (PICP); Procollagen type I N-terminal propeptide (PINP); alkaline phosphatase (ALP); 25-hydroxyvitamin D [25-(OH)D]; the cross-sectional area (CSA); cerebral spinal fluid (CSF); Intraclass correlation coefficients (ICC).