
Abstract
Background
Over half of spinal cord injuries result in tetraplegia, profoundly impairing daily activities (ADLs).
Objective
To evaluate biceps-to-triceps (B-T) and deltoids-to-triceps (D-T) tendon transfers, comparing their impacts on elbow extension strength and ADL independence.
Methods
Retrospective review of tendon transfers performed between 2003 and 2023 at a neurorehabilitation center. Post-surgery muscle strength was assessed using the Medical Research Council (MRC) scale and ADL independence with the motor Functional Independence Measure (mFIM). We used ANOVA to identify post-surgery associations between MRC achieved scores and performance in ADLs.
Results
A total of 34 individuals (42 arms) underwent B-T or D-T surgeries, predominantly at C5 level (66.7%) with 69.0% classified as AIS A. Post-surgery, 81% of B-T and 76.2% of D-T achieved antigravity elbow extension (MRC 3–4), with mean MRC scores of 3.2 for both groups. The B-T group, older at surgery (39.9 vs. 27.8 years) and with shorter time since injury to surgery (2.3 vs. 5.0 years), showed significant post-surgery improvements in Self-care, Transfers, Locomotion, and total mFIM. In contrast, significant associations between MRC scores and mFIM outcomes in D-T transfers involved Self-care, Sphincter control, Transfers, and total mFIM.
Conclusions
MRC scores and ADLs were positively impacted by rehabilitation tendon transfers.
Introduction
Spinal cord injury (SCI) is a major contributor to long-term disability and health loss with an annual global incidence of 40 to 80 per million population (Bae et al., 2023) and 20.6 (95% UI 18.9 to 23.6) million individuals living with SCI worldwide (Safdarian et al., 2023). The segment of the spine most susceptible to injury is the cervical spine, with key anatomical factors contributing to this increased risk, such as its greater range of motion, the relative weakness of the musculature supporting this area, and the higher mechanical vulnerability of the cervical vertebrae compared to other regions of the spine (Torlincasi & Waseem, 2023). Over 50% of SCIs are estimated to be cervical or tetraplegia (van Zyl et al., 2019). Cervical SCI constitutes a severe life-altering event, resulting in profound impairments in an individual's capacity to perform most activities of daily living (ADLs). This population mainly comprises young to middle-aged adults (20–40 years old) with active lifestyles (Bennett et al., 2022). Trauma is its most common cause, including motor vehicle accidents, falls, sports-related or diving injuries (Rief et al., 2019; Shafafy et al., 2019).
For individuals with tetraplegia, enhancing hand function has consistently been reported as the top-ranked goal over the past 20 years (Chang et al., 2012; van Zyl et al., 2019) Patients with cervical SCI have paralysis of the triceps brachii. Loss of elbow extension makes it impossible to use their hands above shoulder level for not being able to hold the elbow extended against gravity (Hentz & Leclercq, 2002). Elbow extension is a critical function for executing ADLs such as dressing, eating, wheelchair locomotion, independent transfers, and reaching objects above shoulder level (Peterson et al., 2017). Elbow extension can be restored by transferring a preserved muscle's tendon onto the paralyzed triceps brachii tendo (Fridén & Gohritz, 2015). The posterior deltoid-to-triceps (D-T) and the biceps-to-triceps (B-T) transfers are the two most common types of transfers used for elbow extension (Zlotolow et al., 2023).
The B-T transfer has been reported as superior to D-T transfer for the restoration of elbow extension in a 2023 review (Zlotolow et al., 2023), based mainly on a prospective, randomized study conducted in 2003 comparing both techniques. Eight biceps-to-triceps transfers were done along with eight deltoid-to-triceps transfers, and at the 2-year follow-up, seven of eight biceps transfers produced antigravity strength, while only one of eight deltoid transfers maintained antigravity strength with elbow extension (Mulcahey et al., 2003).
Leclercq and colleagues in 2008 remarked each of the 2 techniques as having strong advocates and opponents. They concluded that the B-T transfer by the medial route has clear advantages over Moberg's technique. Nevertheless, multiple possible causes of the inferior results were mentioned, including surgical technique or attenuation of the transfer over time (Leclercq et al., 2008).
In relation to maximum strength after elbow reconstruction, Peterson and colleagues compared voluntary activation during maximum isometric elbow extension following B-T transfer (n = 5) and D-T transfer (n = 4) concluding that individuals with a B-T transfer better activated their transferred muscle (Peterson et al., 2017).
In a reported experience conducted in 2017, Medina et al. concluded that in the 6 arms that underwent B-T transfers, full and active elbow extension against gravity at 12 months after surgery was achieved. Muscle strength assessment was done according to the scale proposed by the Medical Research Council (MRC) as in extensive related research (Medina et al., 2017).
Ledgard et al. recently reported that 65% to 75% of patients with tetraplegia would benefit from upper limb surgery, but only 14% undergo such reconstructive procedures (Ledgard & Gschwind, 2020). The reasons for explaining this underutilization are complex (Fridén & Lieber, 2019) with inadequate or lack of information and on-field experiences related to specific procedures reported as causing skepticism among patients, therapists, and rehabilitation physicians (Fridén & Gohritz, 2015). The importance of restoring abilities in ADLs, in addition to functions, was emphasized by Fridèn and Lieber in their recent review analyzing reconstructive hand surgery in tetraplegia, which also highlighted a notable scarcity of studies addressing ADLs (Fridén & Lieber, 2019).
A 2024 systematic review identified 14 studies on D-T transfers, noting several significant limitations. Firstly, the majority of these studies consist of small case series or case reports, limiting the ability to make definitive conclusions. Additionally, some studies only report mean values from manual muscle testing, which hinders detailed quantitative analysis. The variation in surgical techniques, tailored to individual patient characteristics, along with the diverse levels of injury, precludes direct comparisons within this patient group. These characteristics are common challenges in research involving patients with tetraplegia. Furthermore, the review emphasized the absence of long-term follow-up data, crucial for assessing the long-term effectiveness of these surgical interventions (Chung et al., 2024).
Therefore, in this study we aimed to: i) describe the surgical techniques of B-T and D-T transfers consistently performed in a referral neurological center in a European country by the same surgical team over the past 20 years (2003–2023) and compare their outcomes in terms of elbow extension strength; ii) compare pre and post-surgery levels of independence in ADLs for both surgical techniques, with assessments conducted between six months and one year both before and after surgery and iii) analyze the relationship between post-surgery achieved MRC scores for elbow extension strength and ADL specific items (e.g., eating, bathing, grooming) and subtotals (e.g., self-care, transfers).
Materials and Methods
Study Design
We conducted a retrospective observational cohort study analyzing post-acute patients with tetraplegia admitted to the Rehabilitation Unit of Institut Guttmann hospital in Catalonia, Spain between 2002 and 2023. This study conforms to the STROBE Guidelines (“Strengthening the Reporting of Observational Studies in Epidemiology”) (Vandenbroucke et al., 2007).
Participants and Setting
Eligible participants were adult patients (≥ 18 years at the moment of admission) with the diagnosis of cervical SCI, admitted to inpatient rehabilitation at Institut Guttmann hospital, between 2002 and 2023, who underwent either biceps to triceps or deltoids to triceps transfer surgery (between 2003 and 2023).
Pre- and post-surgery, all individuals underwent MRC grading for muscle strength of biceps, posterior deltoids, and triceps in supine. For biceps, patients were asked to flex the elbow from an extended position. For posterior deltoids, the shoulder was supported into flexion and patients were then asked to extend their shoulder backwards. Elbow extension was measured with the shoulder supported at 90 degrees of flexion, with patients extending the arm against gravity.
An MRC grade 4 of 5 or 5 of 5 posterior deltoid or biceps is required for transfer. The lesions were classified according to the International the Classification of the American Spinal Injury Association (ASIA Impairment Scale).
Those excluded from the study were patients without documented pre-surgery MRC scores of posterior deltoid (n = 3) or biceps (n = 2), those with an pre-surgery MRC lower than 4 (n = 1), those with no post-surgery elbow extension MRC (n = 2), those without documented pre-surgery functional independence in ADL assessment within six months pre-surgery (n = 2) or post-surgery (n = 4). All patients admitted at the rehabilitation unit were referred from different acute care setting hospitals (mainly from Catalonia, Spain). The rehabilitation program includes five daily hours of intensive treatment oriented towards cognitive, swallowing, behavioral and physical problems as well as training in ADLs.
Surgical Procedures
Four of the six authors of this study (JMM, LL, ADA, FD) performed all surgical transfers at Institut Guttmann hospital, leaded by author FD during the whole period under study.
The surgical technique for the D-T transfer using tibialis anterior graft has been performed at Institut Guttmann hospital since 2003. Based in the procedure described by Rothwell and Sinclair (Rothwell & Sinclairm, 1997) involves the posterior deltoid transposition with contralateral tibialis anterior tendon graft, patient in prone position, graft harvesting with 2 incisions at the level of the tibialis anterior insertion and at the myotendinous level. Posterior approach from the scapular spine to the deltoid V, localization of the posterior deltoid belly, dilaceration of the fibers and its des-insertion, respecting the insertion into the humerus of the rest of the deltoids, suture at the proximal level of the graft with the muscular belly and the fascia of the posterior deltoids, fan-shaped suture with slow-absorbing monofilament 2/0. Approach over the triceps tendon and the graft is passed to the posterior side at the subcutaneous level through the posterior region of the arm, both tendons are sutured with a Pulvertaft-type interlaced suture. Figures 1, 2 and 3 illustrate key moments from the B-T and D-T transfers conducted at Institut Guttmann hospital during the study period. Figure 1 shows the fan-shaped proximal suture of the tibialis anterior tendon graft to the belly and inferior fascia of the posterior deltoids. The end of the tibialis anterior that will be sutured to the triceps tendon can be seen at the bottom of the image
Fan-shaped proximal suture of the tibialis anterior tendon graft to the belly and inferior fascia of the posterior deltoids.

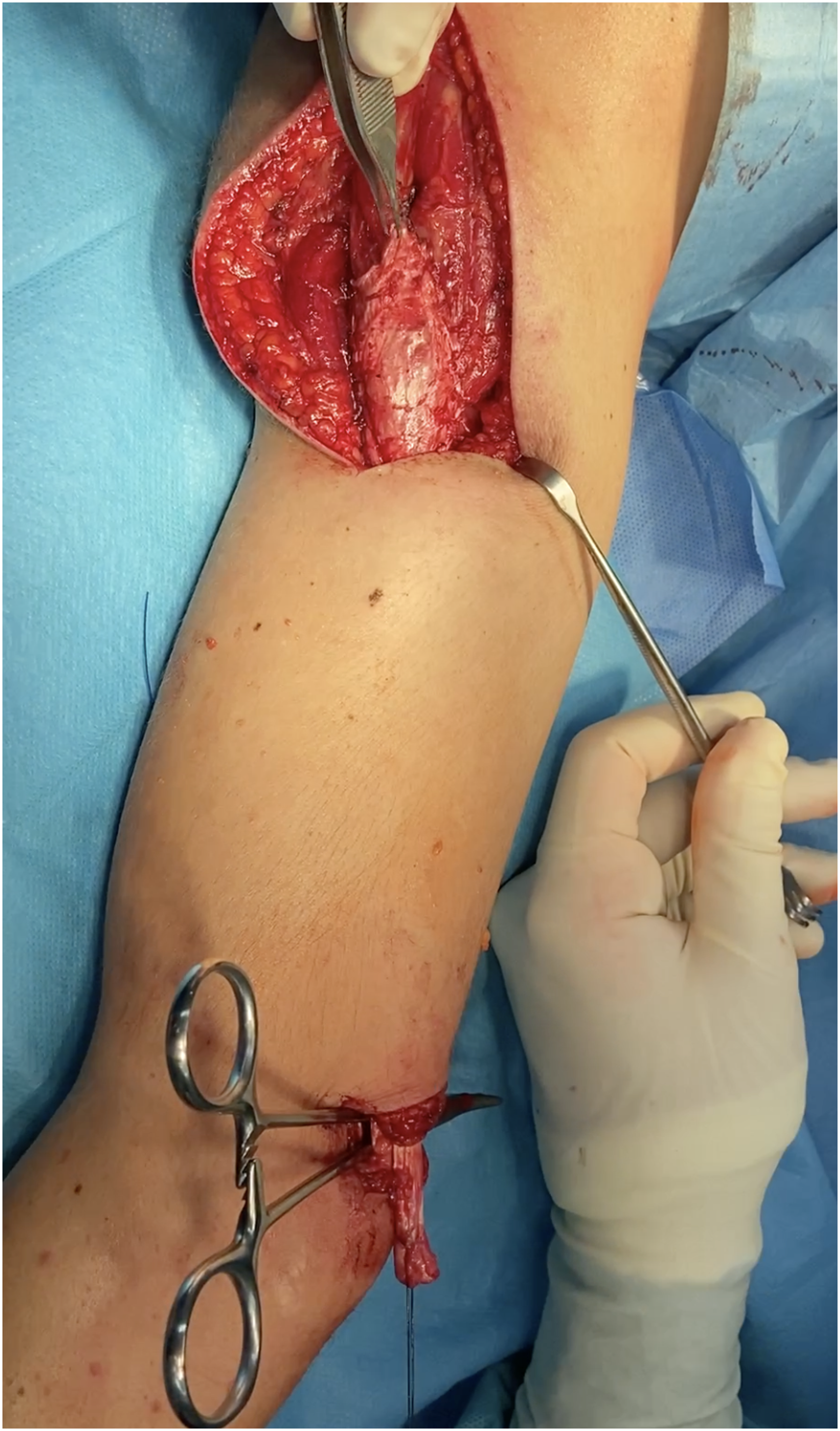
Complete elevation of the biceps, for its transfer by medial or cubital route.
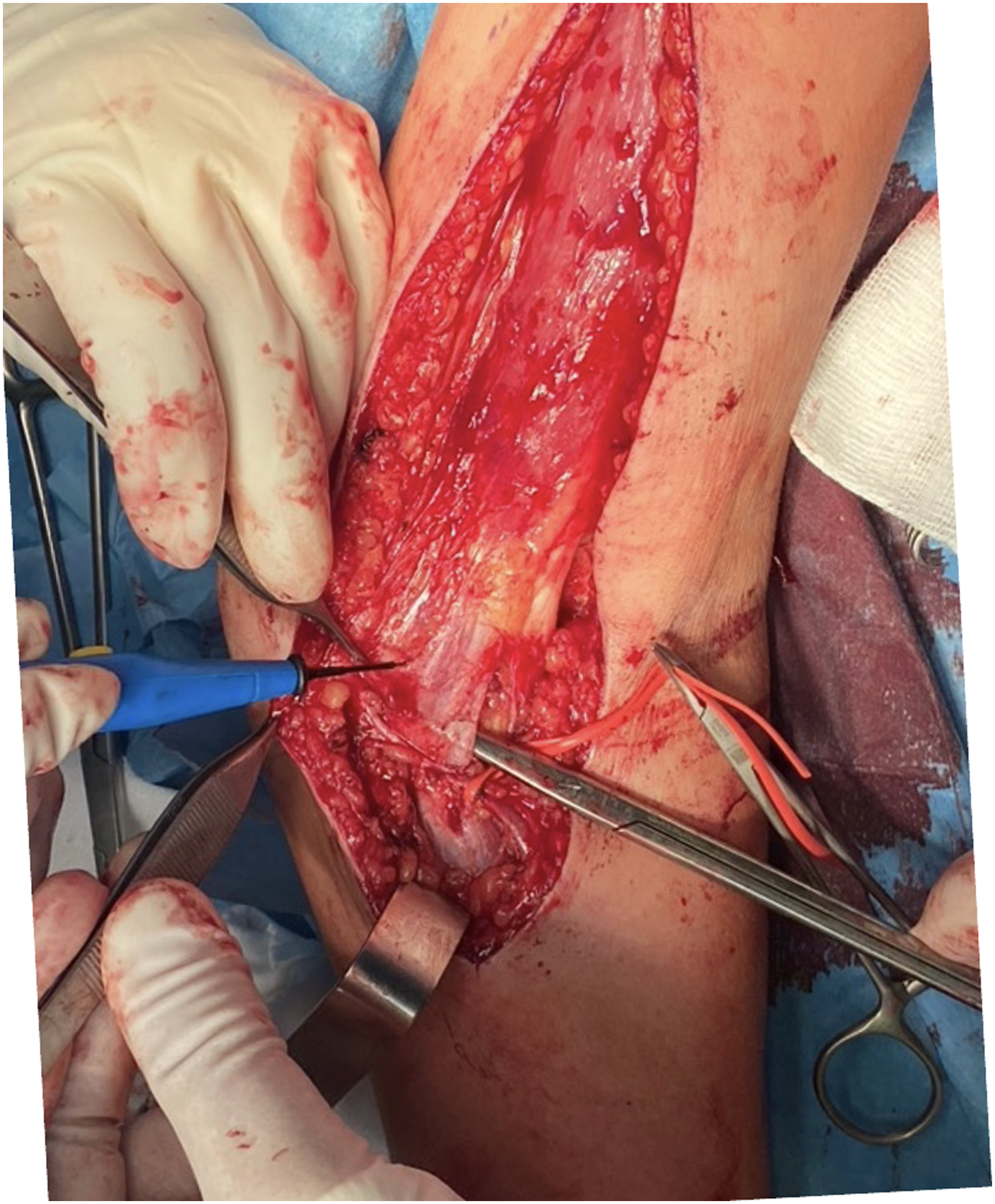
Transecting of the lacertus fibrosus.
The B-T transfer has been performed at Institut Guttmann hospital since 2011 according to Zancolli technique (Kuz et al., 1999). With the patient in the supine position, an anterior arciform incision is made in the arm and elbow. The biceps tendon is located along with its expansion, the lacertus fibrosus. This is sectioned as distally as possible. The muscle is then elevated, separating it from the brachialis and marking the upper limit of the detachment at the level of the entry of the motor branches of the musculocutaneous nerve into the biceps. An incision is made over the triceps tendon and the tendon is passed to the posterior side at the subcutaneous level through the cubital region of the arm, below the ulnar nerve to avoid compressing it. Both tendons are sutured with a Pulvertaft-type interlaced suture. Figure 2 shows the moment of complete elevation of the biceps, for its transfer by medial or cubital route, the limit of elevation is the entry into the muscle of the innervation from the musculocutaneous nerve. Figure 3 shows the moment of transecting the lacertus fibrosus.
In both techniques, if the length of the biceps tendon or the tibialis anterior graft allows it, the suture is reinforced with a bone anchor in the olecranon.
Figure 4 (top) presents the number of surgeries by natural year throughout the study period.
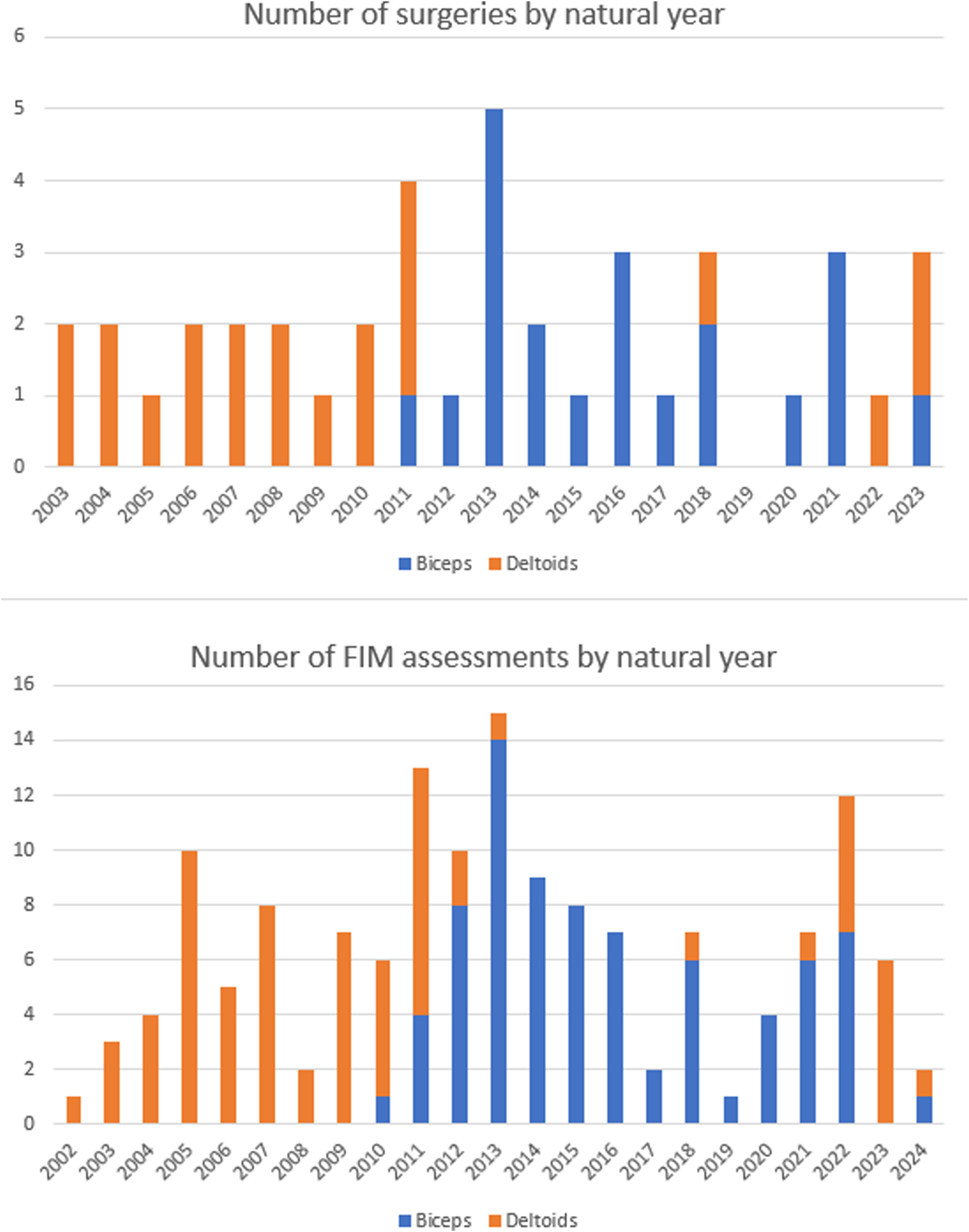
Top: total number of surgeries performed annually throughout the study period, with biceps-to-triceps (B-T) transfers and deltoids-to-triceps (D-T) transfers represented in different colors. Bottom: Total number of FIM assessments conducted annually throughout the study period, also depicted in different colors for B-T and D-T transfers.
Outcome Measures
One of the primary outcomes assessed in this study was elbow extension strength, quantified using the MRC scale. This widely accepted scale provides a standardized measure of muscle strength and has been extensively employed in related orthopedic and neurological research (Medina et al., 2017). The use of the MRC scale allows for consistent and reliable comparison of muscle strength outcomes across different studies, enhancing the validity of our findings in the context of broader clinical research.
Achievement of functional independence in ADLs is extensively measured using the Functional Independence Measure (FIM™) (Linacre et al., 1994) a widely used outcome measure of the level of assistance required for an individual with SCI to perform ADLs. Higher scores represent greater functional independence (range: 18–126). FIM ratings are presented as motor and cognition subscales. The motor subscale (range: 13–91) includes 13 items across 4 domains: sphincter control, self-care, transfer, and locomotion (Linacre et al., 1994). Details are presented in Table SM1 (Supplemental material).
We addressed potential sources of bias by implementing standardized protocols and assessment tools across all study participants. Surgical interventions, as explained above, were performed following established and consistent procedural guidelines to minimize variability in technique and outcomes. To assess patient conditions and outcomes reliably, we utilized standardized measurement scales, including the MRC, the ASIA scale for neurological status, and the FIM for independence in performing daily living activities. These tools are widely recognized for their validity and reliability in clinical assessments, ensuring that our data collection processes were uniform and could be replicated, thereby reducing the risk of measurement bias.
Statistical Analyses
Statistical analyses were performed using R-v3.5.1 (64 bits) (R Core Team, 2024). The significance level was set at p ≤ 0.05. Absolute and relative frequencies were reported for categorical variables. Non-parametric statistics with median and interquartile range (IQR), were used for non-normally distributed continuous variables. Differences between groups were analyzed with Student t-test, Mann–Whitney U-test and Chi2 test (χ2).
To evaluate the impact of surgical tendon transfers on functional outcomes, we will employ a one-way ANOVA. This statistical test is designed to compare means across multiple independent groups to determine whether any significant differences exist between them. Specifically, the independent variable in our analysis will be the post-surgery MRC scores, which categorize the degree of muscle strength recovery into different levels (e.g., 2, 3, and 4). These scores will serve as the grouping variable to assess the influence of varying degrees of muscle recovery on functional capabilities.
The dependent variables in this analysis will be the FIM items, which include discrete tasks such as Eating, Bathing, and Grooming. Each of these FIM items provides a quantifiable measure of the patients’ ability to perform ADLs, reflecting their functional independence post-surgery. By analyzing these items, we aim to identify which aspects of daily life are most impacted by the differing levels of muscle strength restoration achieved through surgical intervention. Upon finding significant differences in the one-way ANOVA, we will conduct a Tukey post-hoc test. This test is chosen for its robustness in comparing all possible pairs of group means while controlling for the family-wise error rate. The Tukey post-hoc analysis will allow us to pinpoint which specific MRC score comparisons differ significantly in terms of their impact on the different FIM items and subtotals, providing a more detailed understanding of the relationship between muscle strength recovery and functional outcomes.
In our study, we employed listwise deletion to handle missing data, ensuring that analyses were performed only on complete cases for variables where missingness occurred.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Results
Between 2003 and 2023, a total of 34 individuals with tetraplegia underwent surgical arm transfers, involving 42 arms in total. Specifically, 21 arms received B-T transfers and 21 D-T transfers. Among these patients, three had D-T transfers on both arms, while five had B-T transfers on both arms.
Of the 34 individuals who had surgery, 31 (91.2%) were male. The distribution of AIS grades demonstrated a predominance of motor complete injuries, with 69.0% classified as AIS A, 14.3% as AIS B, and 16.7% as AIS C. In terms of neurological levels, a majority of our patients were classified at the C5 level, which accounted for 66.7% of the cases, followed by C6 at 21.4% and C4 at 11.9% (Table 1).
Biceps to Triceps and Deltoids to Triceps Transfers, Demographic and Clinical Variables Comparison.
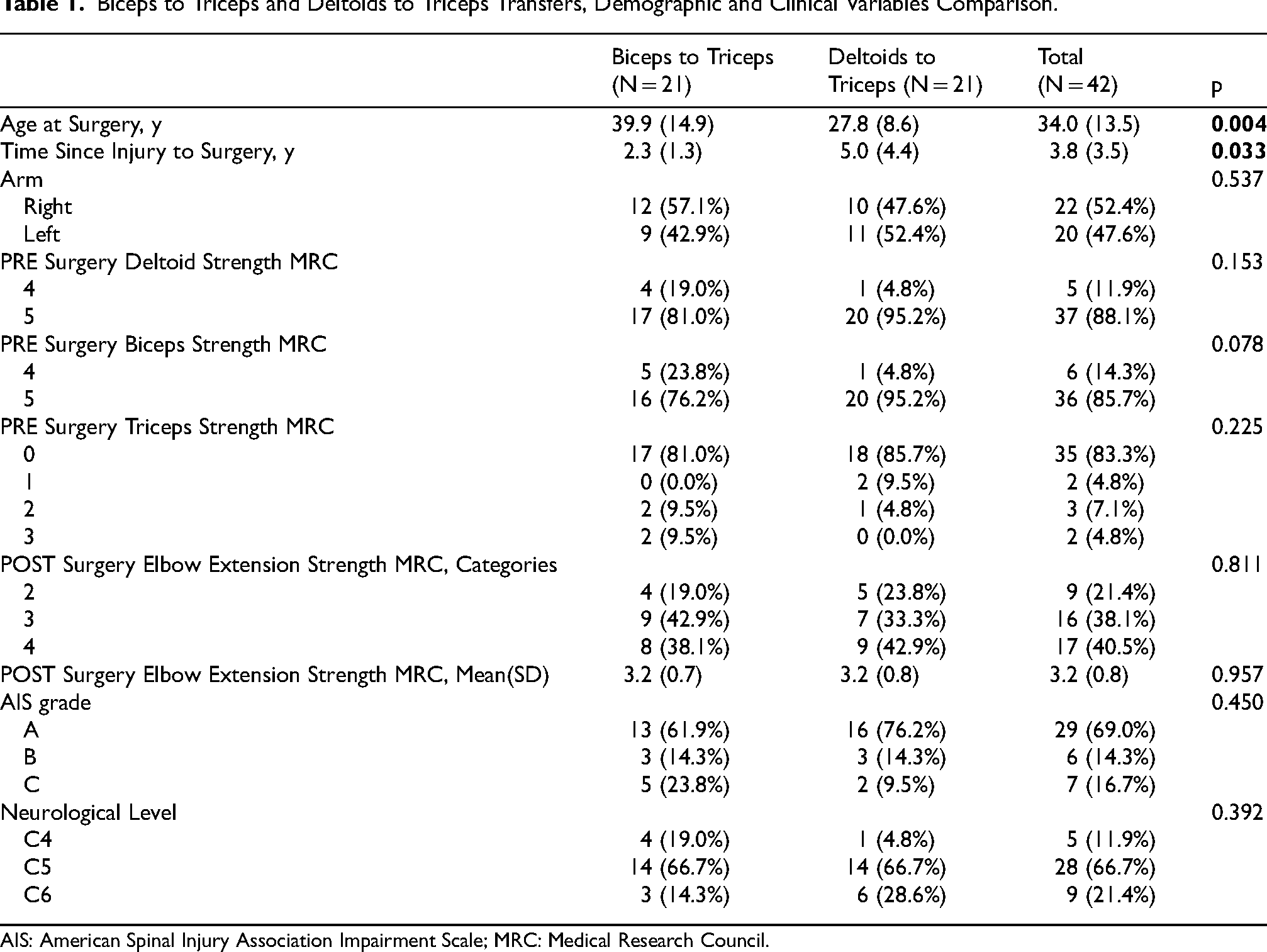
AIS: American Spinal Injury Association Impairment Scale; MRC: Medical Research Council.
Time since injury to surgery was significantly lower for B-T than for D-T transfers with 2.3 (1.3) vs 5.0 (4.4) years respectively. Meanwhile the patients’ age at surgery was significantly older for B-T than for D-T transfers with 39.9 (14.9) vs 27.8 (8.6) years respectively.
The most common cause of injury was diving accidents at the sea or swimming pools (32.4%), closely followed by traffic accidents (26.5%), sports (14.7%) work related (11.8%) and other falls (8.8%).
Muscle Strength
Thirty-seven arms (88.1%) had pre-surgery posterior deltoid strength grade 5 of 5 (17 biceps to triceps [81%] and 20 deltoid to triceps [(95.2%]). The rest (11.9%) had pre-surgery posterior deltoid strength grade 4 of 5 (4 biceps to triceps [19%] and 1 deltoid to triceps [(4.8%]).
Thirty-six arms (85.7%) had pre-surgery biceps strength grade 5 of 5 (16 biceps to biceps [76.2%] and 20 deltoid to triceps [(95.2%]). The rest (14.3%) had pre-surgery biceps strength grade 4 of 5 (5 biceps to triceps [23.8%] and 1 deltoid to triceps [(4.8%]).
No significant differences were observed at pre-surgery posterior deltoid strength either at pre-surgery biceps strength between D-T and B-T groups.
Eighty-three percent of all arms had a pre-surgery triceps strength of MRC 0 of 5 (81% B-T and 85.7% D-T). No significant differences were observed at pre-surgery triceps strength between deltoid to triceps and biceps to triceps groups.
After surgery, 78.6% of the arms (n = 33) were able to extend against gravity (MRC grade 3 of 5 or 4 of 5).
When this is categorized by surgery type, 81% (n = 17) of B-T and 76.2% (n = 16) of D-T achieved antigravity extension, with no significant differences for MRC categories between groups.
When analyzing MRC as a continuous variable, there were no statistically significant differences in post-surgery elbow extension between the B-T group and the D-T group, mean MRC was 3.2 (0.7) and 3.2 (0.8) for B-T and D-T respectively.
Pre and Post-Surgery FIM Assessments
A total of 154 FIM assessments were performed during the period under study, 50.6% of the FIM assessments (n = 78) were performed to the B-T group, meanwhile 49.4% of the FIM assessments (n = 76) were performed to the D-T group. Figure 4 (bottom) presents the number of FIM assessments performed by natural year throughout the study period.
FIM assessments were performed at follow-up visits to the hospital, therefore not all patients had the same number of FIM assessments. Nevertheless, all included patients (n = 34) had at least one pre-surgery and one post-surgery FIM assessment. The B-T group underwent 37 pre-surgery and 41 post-surgery FIM assessments. Meanwhile, the D-T group underwent 36 pre-surgery and 40 post-surgery assessments. All FIM assessments were conducted between six months and one year both before and after surgery.
Table 2 of the manuscript presents a comprehensive comparison of pre- and post-surgery FIM scores for two types of surgical interventions. For the B-T transfers, significant improvements were observed in several domains: the average FIM scores for Self-care rose from 8.18 pre-surgery to 12.87 post-surgery (p < 0.001); Transfers from 3.35 to 5.34 (p = 0.039); Locomotion from 4.35 to 6.80 (p < 0.001); and the Total Motor score increased markedly from 17.94 to 28.09 (p < 0.001). In contrast, the D-T transfers did exhibit no significant changes in any FIM category. This analysis highlights the differential impact of these two surgical techniques on independence in ADLs.
Biceps to Triceps and Deltoids to Triceps Transfers Pre and Post Surgery Fim Comparisons.
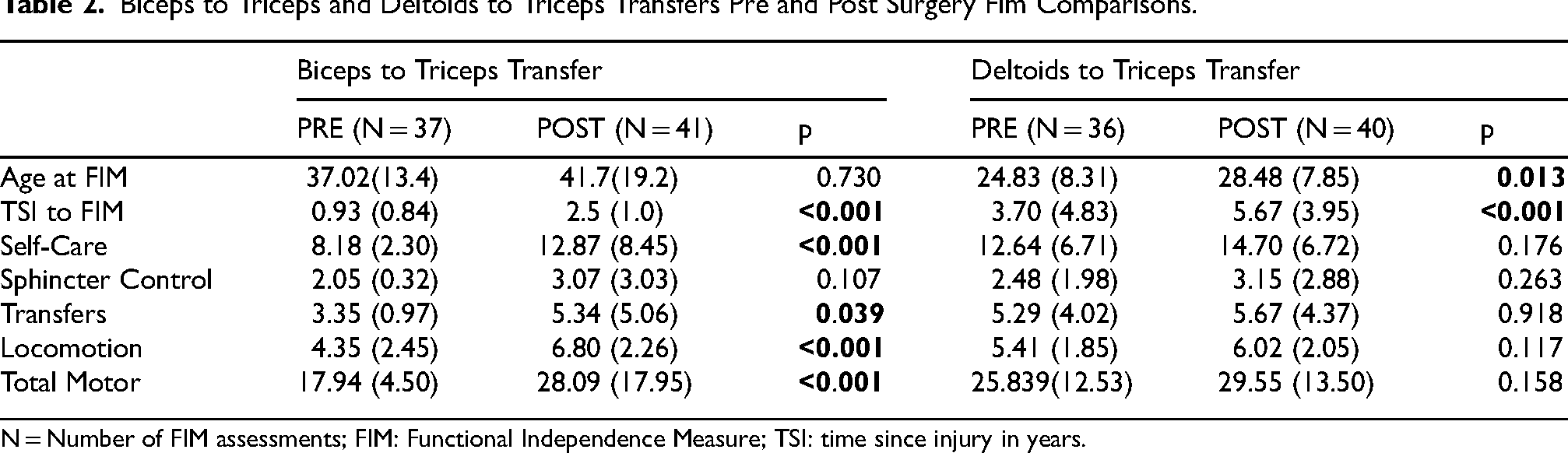
N = Number of FIM assessments; FIM: Functional Independence Measure; TSI: time since injury in years.
Effects of Post-Surgery Elbow Extension Strength on Functional Independence in ADLs
The analysis revealed distinct patterns of significance between the two types of surgical interventions. For B-T transfers, significant improvement was observed only in the ‘Eating’ item (p = 0.00035). Other items and subtotals approached significance but did not cross the conventional threshold.
Conversely, D-T transfers demonstrated a broader range of significant differences across multiple FIM items, notably in ‘Grooming’, ‘Bathing’, ‘Dress Upper Body’, ‘Dress Lower Body’, ‘Toileting’, ‘Subtotal Selfcare’, ‘Bowel Management’, ‘Subtotal Sphincter Management’, ‘Bed/Chair’, ‘Tub/Shower’, ‘Subtotal Transfers’, and ‘Total Motor’, indicating a more extensive influence of this surgical technique on functional recovery (Table 3).
ANOVA Results for the Fim Items and Subtotals for Each Surgery.
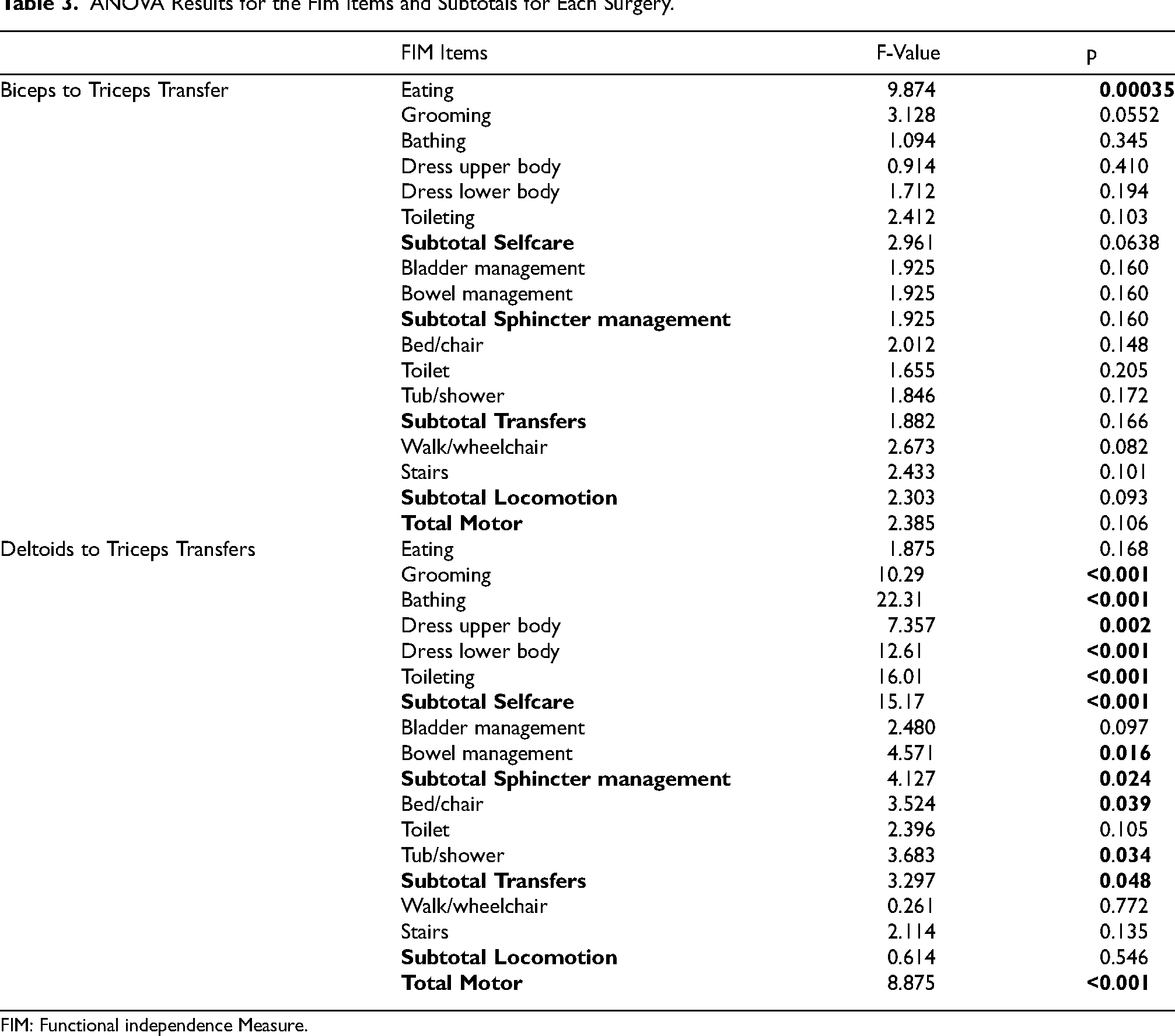
FIM: Functional independence Measure.
Table 4 provides a detailed presentation of the Tukey post-hoc comparisons for FIM items and subtotals following significant ANOVA results. The table specifically highlights the differences in FIM scores between patients with varying post-surgical Medical MRC elbow extension strength scores of 2, 3, and 4.
Tukey Post-Hoc Comparisons for Fim Items with Significant Anova Results.
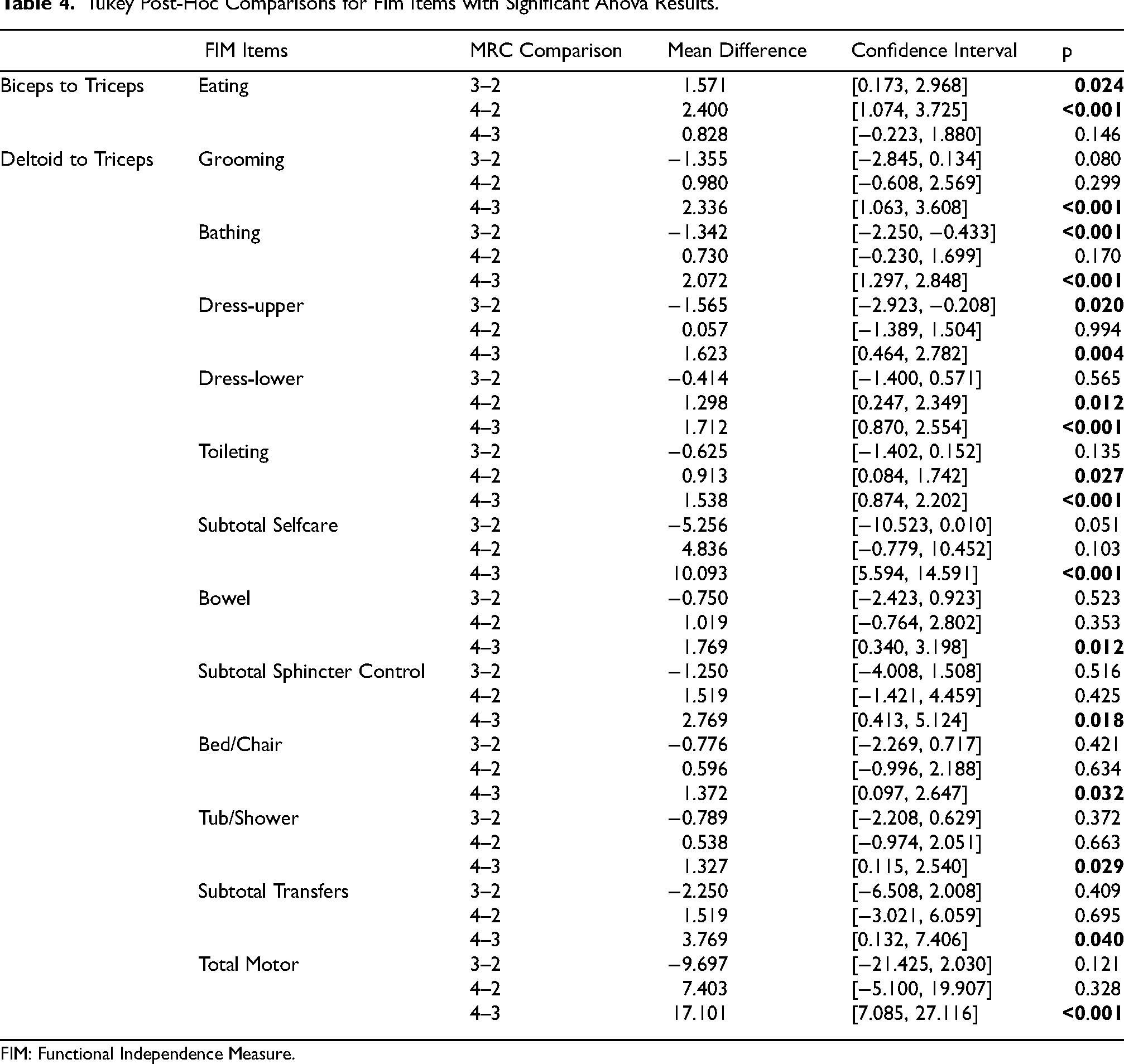
FIM: Functional Independence Measure.
For the deltoids to triceps transfer group, the most notable significant results were observed when comparing the MRC scores of 3 to 4, suggesting a more pronounced improvement in FIM scores as the muscle strength increased from moderate (3) to good (4). For example, significant improvements were recorded in items such as Grooming (p = 0.0002), Bathing (p < 0.001), Dress Upper Body (p = 0.004), Dress Lower Body (p < 0.001), Toileting (p < 0.001), and Total Motor (p < 0.001). These findings indicate a substantial enhancement in various aspects of daily functioning associated with increased muscle strength levels from 3 to 4, underscoring the potential impact of achieving higher MRC scores in enhancing independence in ADLs.
Discussion
The first aim of our study was to compare B-T and D-T tendon transfers in terms of elbow extension strength, focusing on procedures consistently performed at the same neurorehabilitation center over the past 20 years by the same surgical team. Despite differences in the time since injury to surgery and the age at surgery between the D-T and B-T groups, the outcomes in terms of post-surgery MRC grades for elbow extension strength were remarkably consistent. Both groups achieved an average MRC grade of 3.2, underscoring the efficacy of tendon transfer surgery in facilitating significant functional recovery. Our results are consistent with those reported by Hamou and cols (Hamou et al., 2009) in a systematic literature review of 201 tendon transfers for elbow extension across 14 studies, where 190 D-T transfers achieved an average MRC grade of 3.3. However, the review noted a significant imbalance, with only 11 B-T transfers conducted. In contrast, our study reported on an equal number of surgeries for both techniques.
Our study enhances the understanding of tendon transfers for elbow extension strength, particularly highlighting the predominance of C5 neurological level injuries, which constitute two-thirds of the cases examined. This focus is significant given that discussions on upper limb recovery strategies often do not concentrate so heavily on a single neurological level (Chung et al., 2024). C5 injuries, which typically preserve some shoulder function and elbow flexion, are pivotal in achieving more substantial functional gains from such surgeries. Our findings underscore their potential as optimal candidates for tendon transfers, capable of achieving meaningful functional improvements and rehabilitation milestones.
Regarding our second objective, significant improvements were observed in ADLs for patients undergoing B-T transfers, as evidenced by the comparison of pre- and post-surgery FIM scores. Notably, three of the four motor FIM subtotals—Self-care, Transfers, and Locomotion—as well as the Total Motor FIM, showed significant enhancements post-surgery only for B-T group. No pre-post differences in any FIM item (either in the motor FIM subtotal) was observed for the D-T group. This finding is particularly compelling given that B-T patients, were older at the time of post-surgery assessment (mean age of 41 years) compared to those undergoing deltoids to triceps (D-T) transfers (mean age of 28 years) and also had a shorter time since injury to surgery. The shorter interval from injury to surgical intervention in the B-T group suggests the potential benefits of earlier surgical transfers for enhancing functional outcomes.
The importance of contextualizing our results cannot be overstated. By benchmarking our findings against established standards, we can more accurately assess the effectiveness of the surgical interventions we employed. This approach provides a clearer understanding of how our outcomes compare with expected results for similar patient demographics, facilitating a more nuanced interpretation of our success and areas for potential improvement. In Table 2, the post-surgery motor FIM scores for the biceps-to-triceps (B-T) and deltoids-to-triceps (D-T) groups were 28.09 (SD = 17.95) and 29.55 (SD = 13.50), respectively. These scores slightly exceed those reported for patients with tetraplegia at C4-C6 neurological levels, according to the American Consortium for Spinal Cord Medicine (Mahanes et al., 2024) where mean motor FIM scores for patients classified as ASIA A and B at levels C4, C5, and C6 were 18, 23, and 27 points, respectively (Chan & Chan, 2005). Given that 85% of our study participants are classified as ASIA A or B, our results suggest that our surgical interventions—particularly in the context of a predominantly C5-level injury population—may be especially effective in enhancing motor function beyond typical recovery expectations.
As third objective we investigated the relationships between post-surgery MRC scores and FIM items for B-T and D-T transfers. The results revealed distinct outcomes between the two surgical approaches. For the B-T transfers, significant differences were observed only in the ‘Eating’ item, suggesting a targeted improvement in this specific function. In contrast, the D-T transfers demonstrated a broader impact, with significant associations found between the post-surgery MRC scores and three of the four motor FIM subtotals—Self-care, Sphincter control, and Transfers as well as for the Total Motor FIM score. Such results underscore the need for further research to explore these nuances in future studies, potentially guiding more refined surgical strategies and patient-specific rehabilitation programs. For example, for the D-T transfers our results suggest the need for specialized rehabilitation activities focused on enhancing eating functions in this group.
In our study, both B-T and D-T transfers demonstrated a commendable safety profile, with no major post-surgical complications reported. The majority of complications were confined to the immediate post-surgery period and were minor in nature, including wound dehiscence and hematoma formation. Additionally, some patients experienced transient fevers post-operation, a relatively common response to surgical stress. These findings are consistent with known minor complications of tendon transfer surgeries (Dunn et al., 2017), which can also include pain, swelling, and occasional infections that generally resolve with appropriate medical management. The absence of severe complications in our cohort highlights these procedures as safe options for improving upper limb function in patients with tetraplegia.
A main limitation of our study is its uni-center nature, which might restrict the generalizability of the findings across different surgical settings or geographic locations. However, this characteristic also ensures the uniformity of the procedures, as all surgeries were performed by the same team of surgeons, contributing to consistent surgical techniques and postoperative care across all cases. Despite the apparent lower number of individuals and arms treated annually in our study compared e.g., to Dunn and cols (Dunn et al., 2017), the differences are not substantial. Specifically, our study, spanning from 2003 to 2023, treated an average of approximately 1.62 individuals and 2.0 arms per year, while Dunn et al., covering 1983 to 2014, treated about 2.34 individuals and 4.25 arms annually (Dunn et al., 2017). Although our figures are slightly lower, they remain within a comparable range, suggesting that the volume of cases handled per year is similar when considering the specialized nature of these interventions.
Another notable limitation of our study is the lack of evaluation for elbow flexion strength following B-T or D-T transfers. The focus of our research was primarily on assessing the improvements in elbow extension, which is a crucial functional outcome for enhancing ADLs in patients with tetraplegia. This exclusion limits the scope of our findings to one dimension of arm function, although this was a deliberate choice to concentrate our analysis on the specific outcomes most directly influenced by the procedures undertaken. Future studies could benefit from incorporating both aspects of elbow functionality to provide a more comprehensive evaluation of surgical effectiveness and patient outcomes.
In our study, eight patients underwent tendon transfer surgeries on both arms. Specifically, five patients received B-T transfers and three patients received D-T transfers. These cases were not analyzed separately from the single-arm surgeries in our data evaluation. Future work should include a detailed analysis of these subgroups to assess the specific outcomes and challenges associated with each type of bilateral intervention.
Conclusions
In this work we compared B-T and D-T transfers in patients with tetraplegia mostly comprising C5 level (66.7% of the cases) with 69.0% of them classified as AIS A. We identified no significant differences between groups in elbow extension strength with both achieving a mean 3.2 score out of 5 in the MRC. We found that 38.1% of patients in the B-T group and 42.9% of the D-T group achieved MRC-4 respectively.
The B-T group was significantly older at surgery (39.9 (14.9) vs 27.8 (8.6)) and with shorter time since injury to surgery (2.3 (1.3) vs 5.0 (4.4)). Regarding pre-post-surgery differences in ADLs three of the four motor FIM subtotals—Self-care, Transfers, and Locomotion—as well as the Total Motor FIM, showed significant enhancements post-surgery only for B-T group. No pre-post differences in any FIM item were observed for the D-T group. Therefore, our results seem to suggest better ADL performance when surgeries performed earlier post injury.
Importantly, when comparing our outcomes with benchmarks established by the American Consortium for Spinal Cord Medicine, our post-surgery motor FIM scores for both B-T and D-T groups are in line with or slightly higher than those reported for similar patients with tetraplegia at C4-C6 neurological levels. This alignment not only validates the efficacy of our surgical interventions but also underscores their potential to exceed typical recovery expectations.
When analyzing the relationships between post-surgery MRC scores and FIM items for each type of transfer, significant associations were observed only in the ‘Eating’ item for B-T transfers. In contrast, the D-T transfers demonstrated a broader impact, with significant associations found between the post-surgery MRC scores and three of the four motor FIM subtotals—Self-care, Sphincter control, and Transfers as well as for the Total Motor FIM score. This suggests that different surgical approaches may necessitate targeted post-surgery rehabilitation activities addressing the most significantly impacted aspects.
Future research can focus on optimizing post-surgery rehabilitation strategies that target the ADLs most affected by surgical interventions. By concentrating on the specific ADLs that demonstrate the most significant associations or present the greatest challenges following surgery, tailored rehabilitation plans can be developed to effectively enhance functional recovery.
Supplemental Material
sj-docx-1-nre-10.1177_10538135241308803 - Supplemental material for Functional Independence and Elbow Strength in Tetraplegia: Analysis of Tendon Transfers
Supplemental material, sj-docx-1-nre-10.1177_10538135241308803 for Functional Independence and Elbow Strength in Tetraplegia: Analysis of Tendon Transfers by Alejandro García-Rudolph, José Manuel Mendez, Lidia Ledesma, Mark Andrew Wright, Alejandro del Arco and Frederic Dachs in NeuroRehabilitation
Supplemental Material
sj-docx-2-nre-10.1177_10538135241308803 - Supplemental material for Functional Independence and Elbow Strength in Tetraplegia: Analysis of Tendon Transfers
Supplemental material, sj-docx-2-nre-10.1177_10538135241308803 for Functional Independence and Elbow Strength in Tetraplegia: Analysis of Tendon Transfers by Alejandro García-Rudolph, José Manuel Mendez, Lidia Ledesma, Mark Andrew Wright, Alejandro del Arco and Frederic Dachs in NeuroRehabilitation
Footnotes
Acknowledgements
The authors acknowledge Olga Araujo from Institut Guttmann Documentation Department for her continuous support in accessing to related literature.
Ethics
The study follows the Declaration of Helsinki and this study was approved by the Ethics Committee of Clinical Research of Institut Guttmann hospital. The participants are anonymized and non-identifiable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.