
Abstract
Background
The combination of speech and language therapy (SLT) with acupuncture, electroacupuncture, and non-invasive brain stimulation is commonly used in clinical practice and scientific research for post-stroke aphasia (PSA).
Objective
This study assesses the therapeutic effectiveness of SLT-based combination therapies in improving language function in patients with PSA.
Methods
PubMed, CBM, Embase, Web of Science, Cochrane Library, China National Knowledge Infrastructure (CNKI), Wan Fang Data and Chinese Scientific Journals Database (VIP) were searched through 2 December, 2024. This study included randomized controlled trials (RCTs) that compared the influence of SLT-based combination treatments and controls on language function in patients with PSA. The meta-analysis was conducted using random effects NMA.
Results
A total of 66 studies were included. The NMA assessing the effectiveness of various interventions for improving speech, repetition, and listening comprehension skills following SLT revealed that combined therapies generally outperformed SLT alone. For speaking skills, SLT + Electroacupuncture demonstrated the highest likelihood of improvement (SUCRA = 84.6). For repetition scores, SLT + Electroacupuncture was effective (SUCRA = 92.0). In listening comprehension, SLT + tDCS showed the greatest potential for improvement (SUCRA = 89.8).
Conclusions
The results revealed that any type of SLT-based combination intervention was more effective than SLT alone.
Keywords
Introduction
Stroke is one of the leading causes of death and disability worldwide. Approximately 20% to 40% of stroke patients are diagnosed with aphasia (Engelter et al., 2006; Flowers et al., 2016; Lazar & Boehme, 2017) and 20% of stroke patients experience long-term language impairment (Breitenstein et al., 2017). Its low recovery rate seriously affects the reintegration of patients into society (Sul et al., 2019). Difficulties in communicating with the outside world led to a decline in quality of life and impose a serious burden on society and families. SLT is one of the most effective measures for treating aphasia after stroke (Tsouli et al., 2009).
A Cochrane review suggested that long-term speech-language therapy (SLT) could improve the language function of patients with post-stroke aphasia (PSA) (Brady et al., 2016). However, traditional SLT has a limited effect on PSA (Zhang et al., 2018). Other additional therapy was necessary for not all patients who received intensive SLT (Brady et al., 2018). At present, SLT-based combination therapies for PSA mainly include acupuncture, electroacupuncture, transcranial Direct Current Stimulation (tDCS), and repetitive Transcranial Magnetic Stimulation (rTMS).
In this context, it was difficult to determine the superiority of the different combination treatment interventions with individual RCTs or even pairwise meta-analysis, as these studies were often designed to compare one combined treatment with data from SLT control groups. There are currently meta-analyses of the efficacy of acupuncture, electroacupuncture, rTMS, or tDCS on PSA (Elsner et al., 2020; Liang et al., 2022; Shi et al., 2022; Tang et al., 2019; Zhang et al., 2019; Zhang et al., 2021a, 2021b). In addition, there have been studies comparing the effectiveness of different non-invasive brain stimulation for aphasia (Ding et al., 2022), and there have been studies comparing the effectiveness of different acupuncture interventions (Liang et al., 2022). However, no meta-analysis has emphasized the combination with SLT, and no comparison has been made between the combination of acupuncture, electroacupuncture, rTMS, or tDCS with SLT.
As a branch of traditional meta-analysis, network meta-analysis (NMA) has matured theoretical support and could be used for indirect comparisons of therapeutic effects (Jinatongthai et al., 2017; Lu & Ades, 2004). Also called mixed treatment comparisons or multiple treatment comparison meta-analysis. NMA expands the scope of a conventional pairwise analysis by simultaneously analysing both direct and indirect evidence from different studies, allowing for estimation of the relative effectiveness among all interventions and rank ordering of the interventions, even where comparisons of two interventions are lacking (Bafeta et al., 2014).
To date, no systematic review has pooled the effects of different SLT-based combination therapies on the outcomes of AQ, naming, repetition, listening comprehension, and speaking. Therefore, this study aimed to conduct an NMA of RCTs (1) to assess the comparative efficacy of different SLT-based combination therapies on outcomes of general language function and different language dimensions, and (2) to determine the specific therapeutic schedules for different dimensions of language.
Methods
Registration
The program has been registered on PROPERO under the registration number CRD42022343595.
Qualification Criteria
According to the PICO principle, the specific inclusion and exclusion criteria are shown in Appendix Table A1.
Data Sources and Retrieval Strategy
Studies were obtained from PubMed, CBM, Embase, Web of Science, Cochrane Library, China National Knowledge Infrastructure (CNKI), Wan Fang Data, and Chinese Scientific Journals Database (VIP). The databases were retrieved by combining the subject words with keywords. Using PubMed as an example, the search strategy is shown in Appendix Table A2. For example, the search for “stroke” (Simon et al., 2016) and “aphasia” was conducted. The search strategy was adapted for the other databases and adjusted appropriately according to the different grammatical rules of different databases. In addition to the above databases, the reference lists of the included articles were browsed for articles that met the inclusion criteria.
Study Selection
EndNoteX9 was used to manage the retrieved studies. The study selection process was divided into two steps and completed by two researchers. Preliminary screening: Eliminate repeated and unqualified studies by reading the titles and abstracts. Rescreening: Reading through the full text and selecting the studies according to the inclusion and exclusion criteria.
Data Extraction
The following data were collected from the included studies: (1) author, (2) year of publication, (3) country, (4) study period, (5) sample size, (6) mean age, (7) aphasia type, (8) AQ and the results of different language dimensions, such as naming, repetition, listening comprehension, and speaking, (9) details of the combination treatment protocol, (10) outcome assessment tools.
Risk of Bias of Individual Studies
Two researchers independently assessed the quality of the included RCTs by utilizing the Cochrane risk of bias (ROB) assessment tool. As specified by the Cochrane Handbook V.5.1.0, the following seven domains were considered: (1) randomized sequence generation, (2) allocation concealment, (3) blinding of participants and researchers, (4) blinding of outcome assessment, (5) incomplete outcome data, (6) selective reporting and (7) other bias. Each domain was rated as high-risk, low-risk, or unclear-risk of bias as appropriate. The trials were categorized into three levels of ROB by the number of components for which a high ROB potentially existed: high risk (five or more), moderate risk (three or four), and low risk (two or less).
Data Analysis
First, the included literature was qualitatively described, and combination therapy was divided into the following categories: (1) SLT, (2) SLT + Acupuncture, (3) SLT + Electroacupuncture, (4) SLT + Sham Acupuncture, (5) SLT + rTMS, (6) SLT + Sham rTMS, (7) SLT + tDCS, and (8) SLT + Sham tDCS.
When a study had multiple intervention arms and defined all similar arms as constituting the same combination intervention (e.g., receiving rTMS on the right pars triangularis of the posterior inferior frontal gyrus versus receiving rTMS on the right posterior superior temporal gyrus), the data from different intervention groups were pooled.
In accordance with current Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) NMA guidelines (Hutton et al., 2015), we performed pairwise meta-analyses in RevMan 5.4.1, calculated I-squared (I2) measures and visually inspected the forest plots to assess statistical heterogeneity, and STATA software (Version 16.0) was used to command ‘mvmeta’ and ‘network’ to perform multivariate NMA. The data were standardized due to between-study heterogeneity, and a random effects NMA was performed to calculate pooled estimates and 95% CIs. The mean and standard deviation of the difference were used as the indices of the curative effect to analyse the results.
The geometry of the network characterized the relation and precision of direct comparisons. In terms of the type of intervention, different types of SLT combined treatments were compared with a particular control intervention. The geometry of the network was assessed by generating network graphs (Salanti et al., 2011). The network graph is a visualization of network relationships between different interventions. Every node in the graph represents one kind of intervention measures, and the size of the node indicates the intervention measures of sample size, with a larger point indicating a larger sample size. A solid line between two nodes indicates a direct connection, and a thicker solid line indicates more evidence. Indirect comparative evidence of the two unconnected nodes could be discussed according to the network relationship. This network meta-analysis was conducted according to a frequentist approach with weighted least squares based on multivariate regression with random effects. This approach could enable adequate consideration of multiple-arm studies and include restricted maximum-likelihood estimation (White et al., 2012).
The response rate of different SLT combined treatments is denoted by SUCRA (Kodama et al., 2018). While the SUCRA can be usefully re-expressed as the percentage of effectiveness of the SLT combined interventions, such scores should be interpreted cautiously unless there are actual clinically meaningful differences between interventions (Chaimani et al., 2017). The presence of bias was checked due to small-scale studies, which may have led to publication bias in the NMA. A network funnel plot was generated and visually inspected using the criterion of symmetry (Trinquart et al., 2012).
Results
Study Selection
As shown in Figure 1, 2114 unique records were screened, and 266 full text articles were assessed for eligibility, the specific reasons for excluded literature can be found in Appendix Table A3. Sixty-six trials with 4607 participants were included in this NAM and detailed citations can be found in Appendix Table A4 and A5.
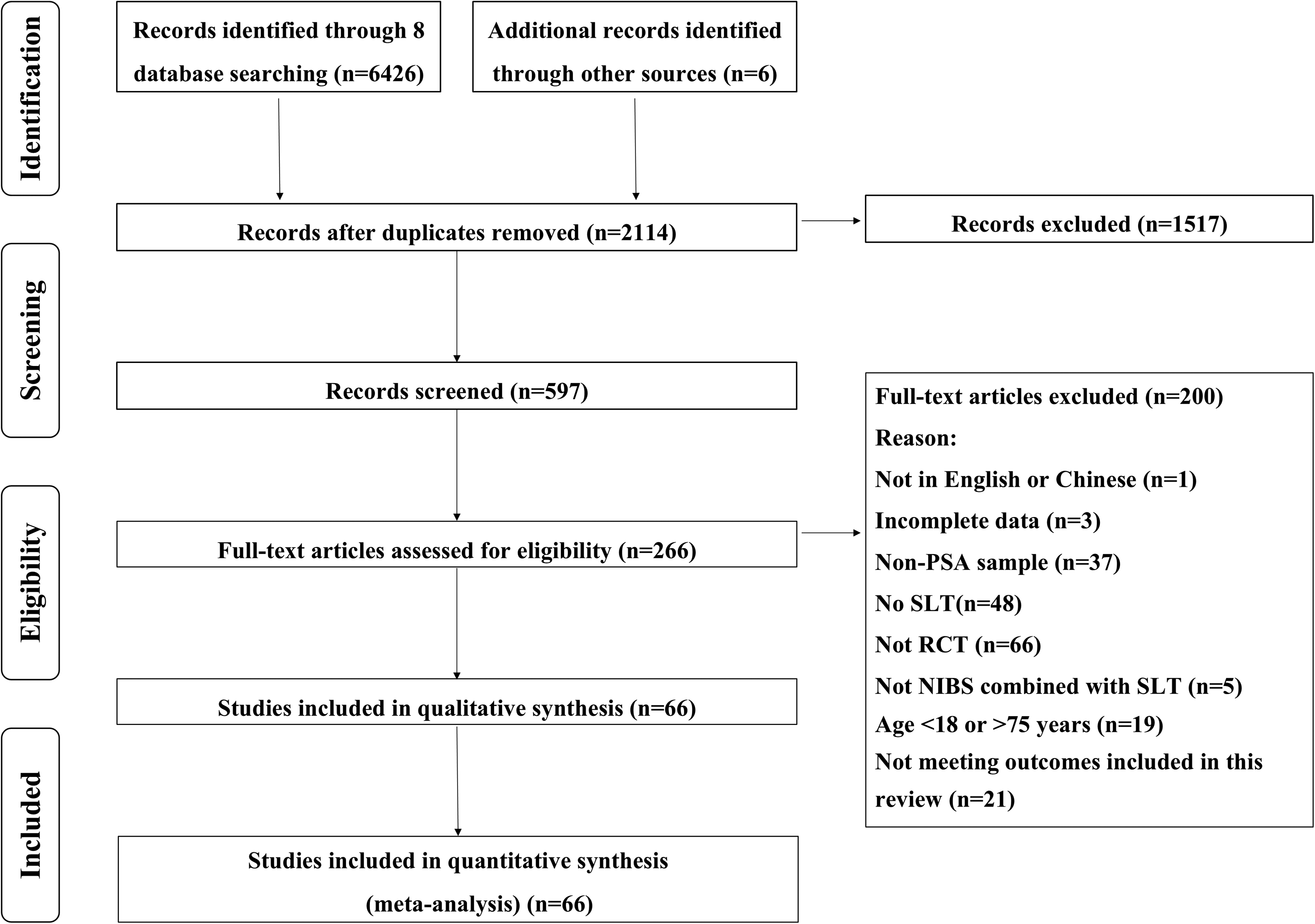
Literature incorporation flowchart.
Study Characteristics
The characteristics of the included studies are presented in Appendix Table A4.
In terms of combination therapy, 2043 participants were included in the simple SLT therapy group, 1214 participants were included in the SLT + Acupuncture group, 415 participants were included in the SLT + Electroacupuncture group, 578 participants were included in the SLT + rTMS group, 136 participants were included in the SLT + tDCS group, 57 participants were included in the SLT + Sham Acupuncture group, 148 participants were included in the SLT + Sham rTMS group, and 10 participants were included in the SLT + Sham tDCS group. The mean length of the different interventions was 38.35days. Further details relating to the different interventions are re-ported in Appendix Table A4.
For baseline demographics, the mean AQ score (42.21[SD:19.88] (Ying et al., 2016)) included 2045 subjects, the naming score (22.17[SD:19.96]) included 2189 subjects, the repetition score (23.72[SD:18.97]) included 3027 subjects, the listening comprehension score (57.94[SD:60.81]) included 3329 subjects, and the speaking score (9.56[SD:7.11]) included 2520 subjects.
In relation to the outcome measures reported, the AQ was measured preintervention and postintervention in 32 of the 66 studies (48.49%). In terms of other different language dimension outcomes, naming scores were reported in 34 (51.52%) studies, repetition scores were reported in 45 (68.18%) studies, listening comprehension were reported in 49 (74.24%) studies, and speaking scores were reported in 40 (60.61%) studies.
All of the studies were RCTs. The sample sizes of the included studies ranged from 18 to 160. The mean (SD) sample size was 70. The age of participants ranged from 18 to 75 years. Sixty-one studies, including 4234 subjects, reported an average age of (58.4[SD:8.58]). The time since stroke ranged from 14 to 360 days. A comprehensive summary of the characteristics of the included trials examining different SLT-based combined treatments for improving language function can be found in Appendix Table A4.
Results of ROB Assessment
Details of the ROB assessment in each study included are provided in Appendix Table A6. Overall, 8 articles were judged to have a low ROB, 45 to have a moderate ROB, and the remaining 13 to have a high ROB.
Network Meta-Analysis
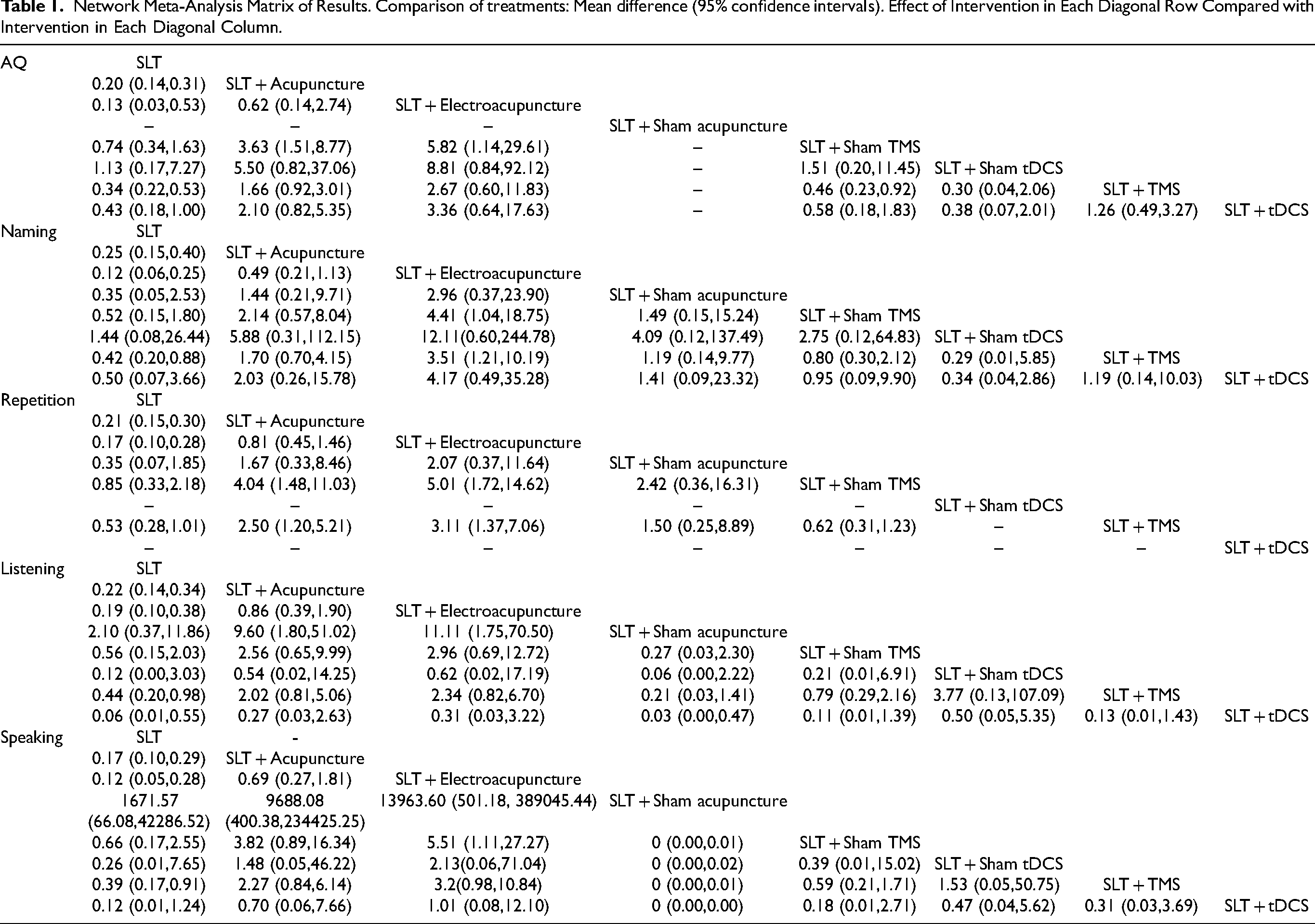
Five measures of language function, AQ score, naming score, repetition score, listening comprehension and speaking score, were included in the NMA. The pre-post data for all outcomes included in the NMA are displayed in Appendix Table A7. NMA maps of the studies examining the efficacy of different combination therapies on the AQ, Naming, Repetition, Listening comprehension and Speaking scores, are illustrated in Figure 2. The size of the nodes indicates the number of participants in that intervention type, and the thickness of lines between interventions indicates the number of studies included in that com-parison. The complete matrix of the results is shown in Table 1. The ranks of the exercise interventions are shown in Table 2 and were based on their likelihood of having the desired effect on the outcome being measured.
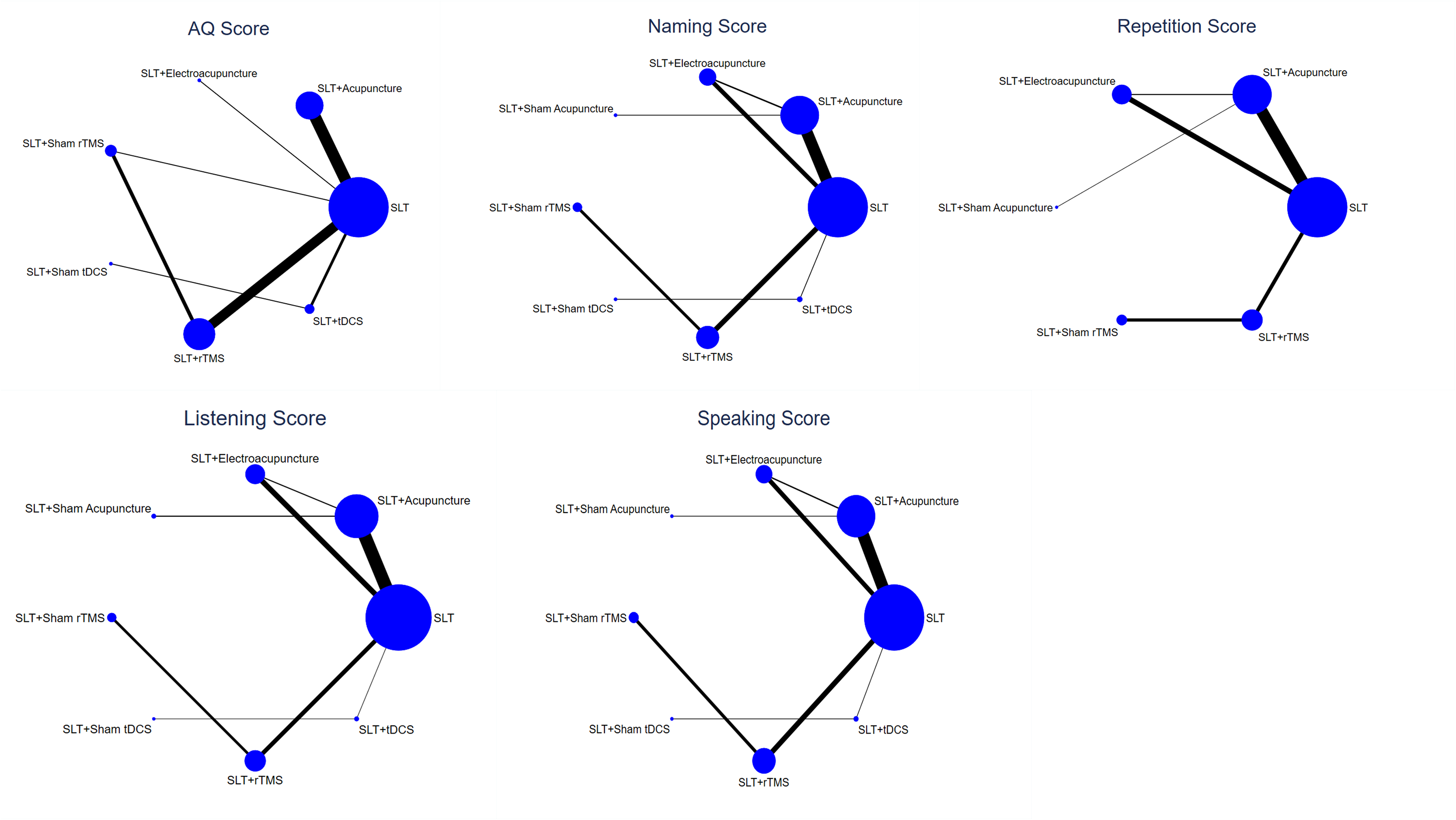
Network meta-analysis maps.
Network Meta-Analysis Matrix of Results. Comparison of treatments: Mean difference (95% confidence intervals). Effect of Intervention in Each Diagonal Row Compared with Intervention in Each Diagonal Column.
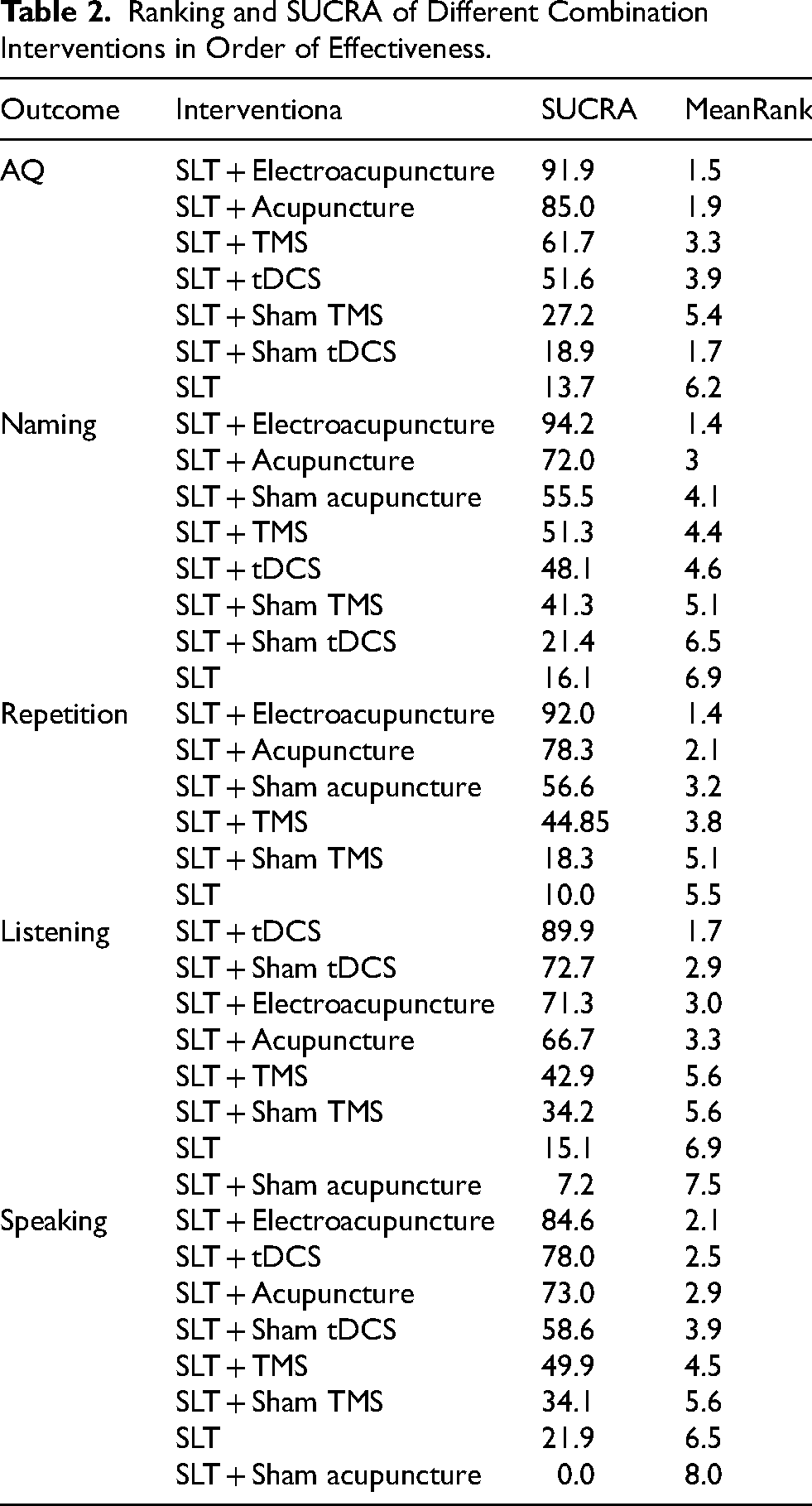
Ranking and SUCRA of Different Combination Interventions in Order of Effectiveness.
Aphasia Quotient
Thirty-two studies, with 2045 participants and seven intervention categories contributed to the NMA assessing the AQ. The complete matrix is illustrated in Table 1. All combination therapies (SLT + Acupuncture: 0.20[CI = 0.14,0.31]; SLT + Electroacupuncture: 0.13[CI = 0.03,0.53]; SLT + Sham rTMS: 0.74[CI = 0.34,1.63]; SLT + Sham tDCS: 1.13[CI = 0.17,7.27]; SLT + rTMS: 0.34[CI = 0.22,0.53]; and SLT + tDCS: 0.43[CI = 0.18,1.00]) were more effective at improving the AQ score than SLT alone (Table 1). The ranking of the different combination interventions based on their likelihood of being the best or worst for improving the AQ score. SLT + Electroacupuncture had the highest likelihood of improving the AQ score in both the direct and indirect comparisons (SUCRA = 91.9) (Table 2).
Naming
Thirty-four studies, with 2189 participants and eight intervention categories con-tributed to the NMA assessing naming scores. The complete matrix is illustrated in Table 1. All combination therapies (SLT + Acupuncture: 0.25[CI = 0.15,0.40]; SLT + Electroacupuncture: 0.12[CI = 0.06,0.25]; SLT + Sham Acupuncture: 0.35[CI = 0.05,2.53]; SLT + Sham rTMS: 0.52[CI = 0.15,1.80]; SLT + Sham tDCS: 1.44[CI = 0.08,26.44]; SLT + rTMS: 0.42[CI = 0.20,0.88]; and SLT + tDCS: 0.50 [CI = 0.07,3.66]) were more effective at improving naming scores than SLT alone (Table 1). The ranking of the different combination interventions based on their likelihood of being the best or worst for im-proving naming scores. The SLT + Electroacupuncture group had the highest likelihood of improving naming scores according to both direct and indirect comparisons (SUCRA = 94.2) (Table 2).
Repetition
Forty-four studies, with 3009 participants and seven intervention categories con-tributed to the NMA assessing repetition scores. The complete matrix was illustrated in Table 1. All combination therapies (SLT + Acupuncture: 0.21[CI = 0.15,0.30]; SLT + Electroacupuncture: 0.17[CI = 0.10,0.28]; SLT + Sham Acupuncture: 0.35[CI = 0.07,1.85]; SLT + Sham rTMS: 0.85[CI = 0.33,2.18]; and SLT + rTMS: 0.53[CI = 0.28,1.01]) were more effective at improving the repetition score than SLT alone (Table 1). The ranking of the different combination interventions based on their likelihood of being the best or worst for improving the repetition score. The SLT + Electroacupuncture group had the highest likelihood of improving the repetition score according to both the direct and indirect comparisons (SUCRA = 92.0) (Table 2).
Listening Comprehension
Forty-nine studies and one study (Zhao et al., 2021) were not included because they could not form a closed loop with other studies, with 3329 participants and eight intervention categories contributing to the NMA assessing listening comprehension score. The complete matrix was illustrated in Table 1. All combination therapies (SLT + Acupuncture: 0.22[CI = 0.14,0.34]; SLT + Electroacupuncture: 0.19[CI = 0.10,0.38]; SLT + Sham Acupuncture: 2.10[CI = 0.37,11.86]; SLT + Sham rTMS: 0.56[CI = 0.15,2.03]; SLT + Sham tDCS: 0.12[CI = 0.00,3.03]; SLT + rTMS: 0.44[CI = 0.20,0.98]; and SLT + tDCS: 0.06[CI = 0.01,0.55]) were more effective at improving listening comprehension scores than SLT alone (Table 1). The ranking of the different combination interventions based on their likelihood of being the best or worst for improving the listening comprehension score. SLT + tDCS had the highest likelihood of improving listening comprehension scores according to both direct and indirect comparisons (SUCRA = 89.8) (Table 2).
Speaking
Forty studies, with 2520 participants and seven intervention categories, contributed to the NMA assessing speaking scores. The complete matrix is illustrated in Table 1. All combination therapies (SLT + Acupuncture: 0.17[CI = 0.10,0.29]; SLT + Electroacupuncture: 0.12[CI = 0.05,0.28]; SLT + Sham Acupuncture: 1671.57[CI = 66.08,42286.52]; SLT + Sham rTMS: 0.66[CI = 0.17,2.55]; SLT + Sham tDCS: 0.26[CI = 0.01,7.65]; SLT + rTMS: 0.39[CI = 0.17,0.91]; and SLT + tDCS: 0.12[CI = 0.1,1.24]) were more effective at improving speaking scores than SLT alone (Table 1). The ranking of the different combination interventions based on their likelihood of being the best or worst for improving speaking scores. The SLT + Electroacupuncture group had the highest likelihood of improving speaking scores according to both the direct and indirect comparisons (SUCRA = 84.6) (Table 2).
Meta-Analysis Results
Aphasia Types
In these 66 studies, 12 reported AQ scores in patients with specific types of aphasia, with 8 studies focusing on Broca's aphasia and 4 on non-fluent aphasia (see Figure 3). Among these, 9 studies used SLT + rTMS, and 3 studies used SLT + acupuncture. This study aimed to explore whether there were differences in therapeutic effects between SLT combined with NIBS and SLT alone, depending on the type of aphasia. The meta-analysis revealed that, compared to SLT alone, SLT combined with NIBS significantly improved overall language abilities (AQ scores) in patients with specific aphasia types (MD = 12.29, [CI = 7.65, 16.94], p < 0.00001). In subgroup analysis, non-fluent aphasia patients receiving SLT + rTMS showed a significantly greater improvement in language abilities compared to those treated with SLT alone (MD = 14.04, [CI = 11.52, 16.56], p < 0.00001). In Broca's aphasia patients, SLT combined with NIBS (including rTMS and acupuncture combined with SLT) was significantly more effective than SLT alone (MD = 11.56, [CI = 5.49, 17.64], p = 0.0002).
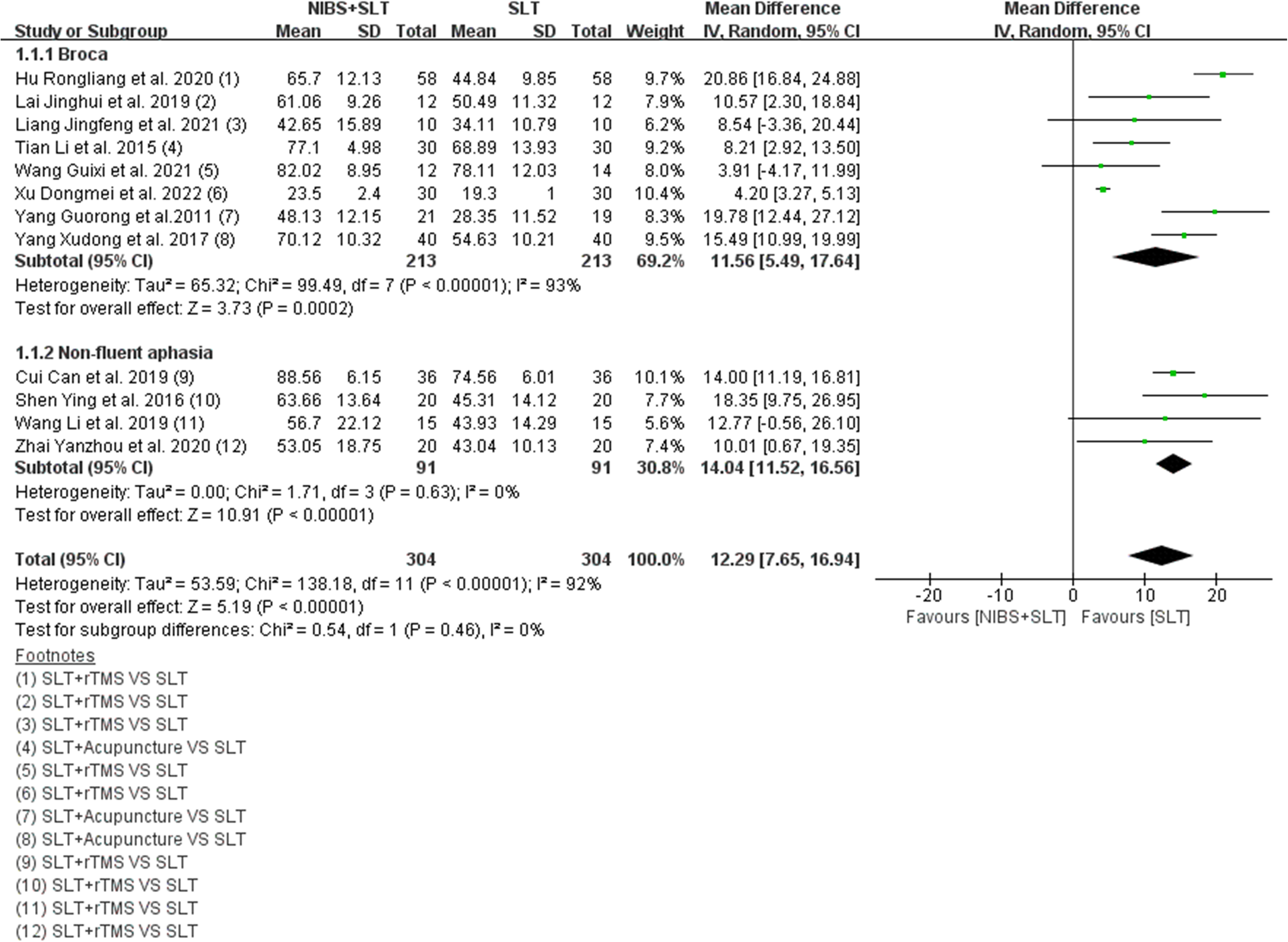
Differences in efficacy of SLT + NIBS versus SLT alone on AQ scores for specific aphasia types.
For other language function dimensions, patients with specific types of aphasia treated with SLT combined with NIBS exhibited significantly better outcomes than those treated with SLT alone. Detailed results can be found in the forest plot in Appendix Figure A1.
Specific Language Functions
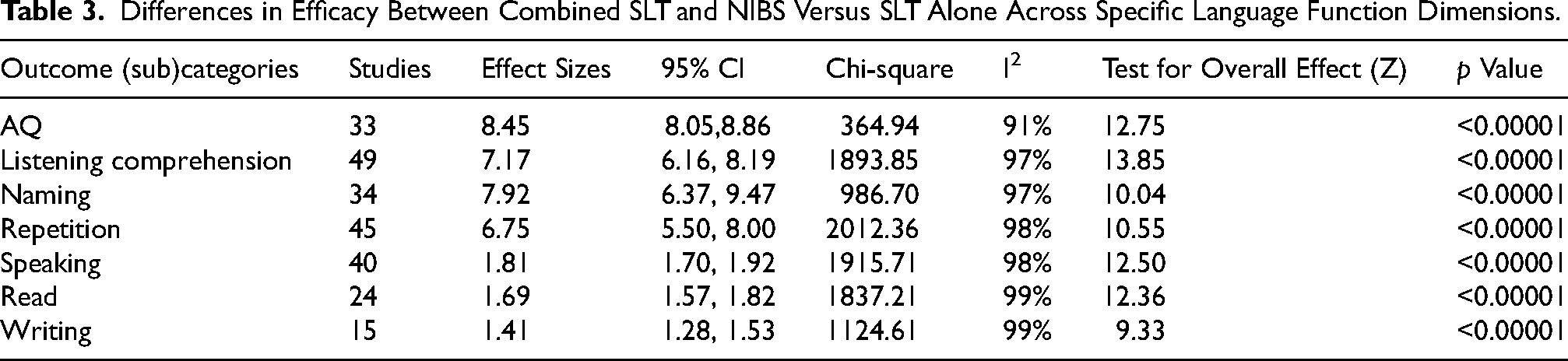
Compared to SLT alone, the combination of NIBS and SLT significantly improved outcomes in PSA (MD = 7.51, [CI = 7.07, 7.95], p < 0.00001). This improvement was particularly notable in AQ score (MD = 8.48, [CI = 8.05, 8.86], p < 0.00001), naming (MD = 7.92, [CI = 6.37, 9.47], p < 0.00001), listening comprehension (MD = 7.17, [CI = 6.16, 8.19], p < 0.00001), and repetition (MD = 6.75, [CI = 5.50, 8.00], p < 0.00001). Detailed results are presented in Table 3 and Appendix Figure A2.
Differences in Efficacy Between Combined SLT and NIBS Versus SLT Alone Across Specific Language Function Dimensions.
Results of Additional Analyses
The presence of bias was checked due to small-scale studies, which may have led to publication bias in the NMA. A network funnel plot was generated (Appendix Figure A3), and the data were visually inspected using the criterion of symmetry. To some extent, the consistency of the included studies was reflected.
Discussion
In the present study, the available data regarding the impact of various combination therapies on individuals living with PSA has been systematically analysed. In contrast to most meta-analyses that focus solely on the effects of a single combination therapy, our approach included direct and indirect evidences from 66 randomized controlled trials (RCTs) involving more than 4607 adults diagnosed with PSA and comparing eight different intervention arms.
Previous studies in the field of PSA have proposed a range of therapeutic approaches aimed at improving language function. These include various non-invasive brain stimulation (NIBS) techniques such as tDCS (Bonilha et al., 2024), rTMS (Wang et al., 2023), acupuncture (Li et al., 2024), electroacupuncture (Shi et al., 2022), as well as SLT (Berker et al., 1986; Breitenstein et al., 2017) alone. Electroacupuncture as an extended technique of acupuncture, has both the effects of traditional acupuncture and the functions of modern electrotherapy and is widely used as a complementary therapy for patients with PSA (Huang et al., 2020). However, the optimal approach remains unclear, necessitating a systematic evaluation of their relative effectiveness, especially in combination.
The most frequently utilized post-stroke language assessment scales in the included studies were the Western Aphasia Battery (WAB), the Boston Diagnostic Aphasia Examination (BDAE), and the Aphasia Battery for Communication (ABC). Of these, the WAB assesses naming, repetition, listening comprehension, and speaking skills to produce a key AQ score that is below the 93.5 cutoff for a diagnosis of aphasia, with lower scores reflecting a more severe language impairment (Kertesz, 2020). Furthermore, BDAE provides quantitative criteria for categorization and severity of aphasia through a detailed scale of 0 to 5, with higher scores indicating less severe impairments (Liu et al., 2023). The ABC is designed for Chinese speakers and provides a thorough assessment of oral expression, comprehension, reading, and writing (Pei et al., 2023). Each domain is scored out of 100, with higher scores indicate better language functioning. The combination of these tools enabled the researcher to conduct a comprehensive and in-depth assessment of the intervention's efficacy.
This study revealed that any SLT-based combination therapy was more effective than SLT alone, which is similar to the findings of a recent meta-analysis (Zhang et al., 2021c) which showed that, compared to the SLT group, acupuncture combined with SLT could improve BDAE level and ABC scores in patient with PSA. In addition, several software programs, such as the CNN-based model (Mahmoud et al., 2023), have been used to assess speech severity levels to help quantify the severity of speech disorders in patients with PSA. However, despite progress in assessment tools, specific and widely accepted guidelines for the treatment of conditions such as aphasia are lacking.
This study main findings indicate that in subjects with PSA, the combined intervention of SLT + Electroacupuncture is promising for improving AQ, naming, as well as repetition score. Out of the eight combination interventions investigated, SLT alone appeared to have the least effect on language function. The SUCRA ranking suggested that, when prescribing interventions to potentially improve the AQ score, SLT + Electroacupuncture and SLT + Acupuncture may be the top two combination interventions for this population. In addition, a subgroup analysis of this study for a specific population found that for Broca's aphasia patients, SLT + electroacupuncture, SLT + acupuncture, SLT + rTMS, and SLT + tDCS treatments significantly improved listening comprehension, repetition, and naming abilities. As for patients with non-fluent aphasia, SLT + rTMS treatment was expected to improve listening comprehension, repetition and naming abilities. In terms of listening comprehension scores, SLT + tDCS showed potential for significant improvement, which was different from a recent report (Ding et al., 2022) showing that dual and anodal tDCS outperformed rTMS for naming and repetition, but Low-Frequency (LF)-rTMS was the most prioritized NIBS mode for alleviating global severity. This could be related to the focus of this NMA on combination therapies based on SLT, instead of ranking the efficacy of different NIBS modes for post-stroke aphasia.
Further analysis revealed significant differences in the effectiveness of various interventions across specific language function dimensions. Compared to SLT alone, combined SLT therapies demonstrated greater efficacy in improving auditory comprehension, naming, and repetition abilities (Junshuang et al., 2018; Ying et al., 2016; Zhaoying et al., 2019). However, the results did not indicate a distinct advantage regarding speech production and auditory comprehension. This discrepancy may stem from the study's primary focus on evaluating therapeutic outcomes rather than exploring the underlying neural mechanisms of speech production and auditory comprehension. Considering that these language functions involve more complex brain network activities, future research should integrate neuroimaging data to comprehensively elucidate the mechanistic effects of interventions on different dimensions of language functions.
From the traditional Chinese medicine (TCM) point of view, acupuncture has the function of dredging the meridians and collaterals (Wei et al., 2020), to improve the language function of PSA patients. From a neuropsychological perspective, acupuncture specifically enhances the functional connections between the cognitive brain network of the language-dominant hemisphere and the surrounding adjacent brain regions in healthy elderly people (Chung et al., 2019). The activity of the peripheral brain area at the site of stroke injury is enhanced (Li et al., 2017), neuroplasticity is modulated in stroke patients, and brain regions associated with language are activated (Hull et al., 2009; Zhang et al., 2021a). One article (Chang et al., 2017) pointed out that language-related brain areas were activated by acupuncture including the frontal, temporal, parietal, occipital lobes, insula, precuneus, and other wide range of brain function areas as shown by MRI. Hence, it is reasonable to suggest that compared with other joint intervention modes, SLT + Electroacupuncture and SLT + Acupuncture improve the AQ, naming, repetition, and speaking better.
Current stroke guidelines recommend that brain stimulation may be considered as an adjunctive experimental therapy to behavioral SLT (Zhang et al., 2020), but acupuncture is recommended only for post-stroke paralysis, dysphagia, depression, and dysarthria (Chiaramonte & Vecchio, 2021) and not for aphasia (Winstein et al., 2016). However, the clinical practice of acupuncture for PSA has received increasing attention worldwide. The results of the present NMA showed the beneficial effect of SLT + Electroacupuncture and SLT + Acupuncture on PSA, which was superior to that of other SLT-based combination therapies.
Strengths and Limitations
This study had several strengths and weaknesses. This review was systematic and exhaustive. A considerable sample size of adults living with PSA (n = 4607) was included, thus providing the power to detect statistically significant mean differences. Only RCTs, the gold standard for evaluating the effectiveness of the interventions were included. The use of the AQ as the outcome measure in the NMA also strengthened this study as it was considered to be a common and accepted indicator for evaluating language functions. Furthermore, this study exclusively included Chinese and English literature to ensure accurate interpretation and high-quality analysis while minimizing potential biases arising from translation. The National Institutes of Health (NIH) recognized the scientific validity of acupuncture during a landmark hearing in 1997, marking a significant milestone in the global acceptance of Chinese acupuncture. To ensure the study incorporates the most current and scientifically rigorous information, literature published since 1997 was included in the analysis.
In this paper, a network meta-analysis was conducted to investigate the effects of SLT combined with acupuncture, electroacupuncture, and other physical stimulation treatments on overall language function and different language dimensions in patients with PSA. The effect of therapy on the language function of PSA patients has been frequently evaluated in former meta-analysis. There was no systematic meta-analysis of the efficacy of combination regimens, nor was there any comparison of efficacy differences for language function and different language dimensions between different combination regimens.
Our review shares a number of limitations with the studies on which it is based. The first limitation was heterogeneity in the quality of the included studies. Allocation concealment (87.88%; n = 58), blinding of participants and researchers (93.94%; n = 62), and blinding of outcome assessment (86.36%; n = 57) were the main sources of risk of bias in the included studies. The included studies were conducted in the cultural setting of acupuncture as a traditional and familiar intervention in the healthcare system. Therefore, the results may not represent the potential effects of these interventions on all populations of the world. More studies in populations from other cultural backgrounds are necessary.
The second limitation was the absence of subgroup analysis for stroke duration, or treatment course due to the insufficient number of studies post-grouping for analysis, which could introduce potential bias. Although efforts were made to minimize heterogeneity through strict inclusion and exclusion criteria, the study populations differed in several aspects, including country of recruitment and the ratio of male to female participants. Despite the fact that most of the included studies used SLT interventions at a frequency of 30 min 5 times a week (51.56%; n = 34), there was more variation in the duration and frequency of the interventions. In the subgroup analysis of aphasia types, due to the insufficient number of studies on other aphasia types, only Broca's aphasia and non-fluent aphasia were analysed. However, there was considerable heterogeneity in the analysis, highlighting the need for further exploration of clinical differences across studies. Therefore, potential sources of clinical heterogeneity should be considered in future studies.
The third limitation was that the number of studies was unevenly distributed among the different types of SLT-based combination therapies, leading to limited sample sizes for the SLT + Sham Acupuncture, SLT + tDCS, and SLT + Sham tDCS studies. In the analysis of repetition, only one study compared the impact of SLT + tDCS and SLT + Sham tDCS on this result, and it could not form a closed loop with other studies, therefore, it was not included in the analysis of the impact on repetition.
Conclusion
Despite its limitations, this NMA provided valuable information for the clinical application of SLT-based combination therapies in the management of PSA. In patients with PSA, SLT alone did not demonstrate the same level of improvement in language function as SLT-based combination therapies. Based on the current and available evidence, our review suggests that a combination of SLT + Electroacupuncture may potentially enhance clinically significant improvements in AQ, naming, repetition, and speaking among patients with PSA. Similarly, a combination of SLT + tDCS potentially improves listening comprehension skills among patients with PSA.
In conclusion, this study aimed to demonstrate the efficacy of SLT-based combination therapies for PSA. It is hoped that the results of this study will provide clinicians with further insight into SLT-based combination therapies, and provide solid evidence for future research on the mechanisms of PSA. Furthermore, this study offers an interdisciplinary overview of stroke aphasia, with the objective of furnishing robust evidence for future research in this field.
Supplemental Material
sj-docx-1-nre-10.1177_10538135241312600 - Supplemental material for Speech and language therapy plus electroacupuncture or non-invasive brain stimulation for post-stroke aphasia: a systematic review and network meta-analysis
Supplemental material, sj-docx-1-nre-10.1177_10538135241312600 for Speech and language therapy plus electroacupuncture or non-invasive brain stimulation for post-stroke aphasia: a systematic review and network meta-analysis by Lanlan Zhang, Bingbing Lin, Yunshi Huang, Mengxue Wang, Jinglei Ni, Jian Song and Jia Huang in NeuroRehabilitation
Footnotes
Abbreviations
Ethics Statement
This study, as a literature review, is exempt from Institutional Review Board approval.
Author Contributions
LZ and JH conceived the study, initiated the design, and revised the manuscript. LZ, YH, MW, JN and JS participated in the design and drafted the manuscript. BL and JH revised the important parts of this manuscript critically. YH participated in the later revision of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science Foundation of China grant number [No. 82074512].
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.