
Abstract
Background
The of upper extremity closed kinetic chain exercise combined with biofeedback requires evidence-based guidelines to elucidate its impact on the proprioception, muscle strength, and function of stroke patients.
Objective
The aim of this study is to compare the effects of upper extremity closed kinetic chain exercise combined with biofeedback on the proprioception, muscle strength, and function of stroke patients.
Methods
The 24 stroke patients were randomly divided into two groups: the upper extremity closed kinetic chain exercise combined with biofeedback group (UCKCBG; n = 11) and the control group (CG; n = 13). Training was conducted five times a week for four weeks. Outcome measures included the Thumb Localization Test (TLT), Medical Research Council Score (MRC), Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST), and Fugl-Meyer Assessment (FMA).
Results
The result showed that the UCKCBG demonstrated significant effects on TLT, MRC, CKCUEST, and FMA compared to the CG (p < 0.05).
Conclusion
This study showed that repetitive upper extremity closed kinetic chain exercise with biofeedback can be considered as a training method in clinical practice for stroke patients with decreased proprioceptive sensation, muscle strength, stability, and upper limb function
Introduction
Stroke is the second leading cause of death worldwide, accounting for 11.8% of all causes of death, with approximately 17 million new cases occurring annually (Yang et al., 2023). Stroke occurs when blood supply to the brain is interrupted or when there is brain hemorrhage, leading to motor impairments (Sharp et al., 1997). Generally, about 30–48% of stroke survivors experience proprioceptive deficits in the upper limbs post-stroke (Rand, 2018). Among the various disabilities associated with stroke, upper limb dysfunction is one of the most common sequelae (Tendulkar et al., 2017).
70% of stroke survivors face problems in activities of daily living such as personal hygiene, eating, and dressing due to upper limb dysfunction (Meadmore et al., 2014), posing a significant barrier to their societal reintegration. Therefore, restoring upper limb function is a crucial goal of rehabilitation therapy for stroke survivors (Hayward et al., 2010).
Proprioception plays a vital role in optimizing joint stability and function, enhancing postural control, movement, and muscle stabilization-related cognitive awareness (Rogol et al., 1998). Closed kinetic chain exercises for the upper limbs have been reported to enhance proprioception, joint stability, and muscle strength. Immediate feedback has been shown to improve adherence to instructions (Pontillo et al., 2007), and recent studies suggest that combining physiotherapist education with novel biofeedback techniques is more efficient than physiotherapist education alone (Hershko et al., 2008).
Biofeedback therapy provides stroke survivors with an opportunity to recalibrate proprioception, input correct sensory information, and learn self-control over various physiological responses (Huang et al., 2006). Improvements in proprioception help enhance balance ability (Jeong & Chung, 2024). Biofeedback is crucial for optimizing human motor function as it involves the nervous system detecting both sensory and motor signals (Yoon et al., 2011). Visual biofeedback specifically influences neuromuscular control during specific tasks, thereby promoting selective muscle activation. Various biofeedback interventions, such as sensory augmentation devices like smart windows and visual biofeedback using motion quantification devices, have been reported in stimulating proprioception (He et al., 2022). Furthermore, Proprioception training using mirrors is effective in improving joint position sense, muscle strength, and motor function (Gedrime et al., 2018).
Despite the effectiveness of biofeedback therapy in stimulating proprioception, its clinical application is hindered by environmental factors and cost. Laser-based biofeedback therapy offers portability and clinical feasibility (Yoon et al., 2011), enhancing correct movements and promoting effective motor function (Langer et al., 2020). Additionally, wearable devices designed to expand the scope of treatment and enhance treatment voluntariness by providing feedback have been developed (Reinkensmeyer & Boninger, 2012).
Combined therapies are more effective than individual therapy techniques, there is limited research on the combined effects of biofeedback therapy and closed kinetic chain exercises on proprioception, muscle strength, and motor function, especially focusing on upper limb proprioceptive therapy for stroke survivors (Gliga et al., 2022). Therefore, this study aims to investigate the effects of upper extremity closed kinetic chain exercises combined with biofeedback therapy on proprioception, muscle strength, stability, and function in stroke survivors and compare them with conventional physiotherapy.
Methods
Participants
This study targeted 24 patients hospitalized at W Rehabilitation Hospital in Seongnam City, and the treatment was conducted from September 5 to October 2, 2023. The selection criteria for the study subjects were as follows: individuals diagnosed with stroke (cerebral infarction or cerebral hemorrhage) by neurologists and specialists in rehabilitation medicine, those with a Mini Mental State Examination-Korean version score of 21 or higher indicating communicative ability, and those with a Modified Ashworth Scale score of less than 2. The sample size of this study was determined through statistical evaluation using G*Power Version 3.1.9.7. The primary analysis method, independent samples t-test, was used with a statistical power of 60% and a significance level (α) of 0.05. Considering a dropout rate, a total of 24 participants were determined as the minimum sample size. The final study subjects comprised 25 individuals who initially expressed voluntary willingness to participate.
The exclusion criteria for the study subjects were individuals with neurological disorders other than stroke, cardiovascular diseases, visual impairment or visual field defects, and those who had recently participated in experiments similar to this study.
Participants were provided detailed explanations about the study before treatment and were informed of their right to withdraw at any time. They voluntarily agreed to participate by signing informed consent forms. This study was conducted with approval from the Research Ethics Committee of Sahmyook University (approval number: 2023-06-018-006). The research registered with the Clinical Research Information Center complies with the World Health Organization International Clinical Trials Registry Platform (WHO-ICTRP) guidelines (Registration Number: KCT0009737).
Study Procedure
The general characteristics of the 25 eligible participants who met the selection criteria were evaluated before the experiment, and gender, age, weight, and height were confirmed through measurements with the consent of the participants and their guardians. Research subjects who initially expressed their intention to voluntarily participate were randomly classified into an experimental group and a control group that performed closed chain exercise combined with biofeedback using the www.randomizer.org site. For both groups, each training was performed 20 times in total, 30 min per session, 5 times a week for 4 weeks (Figure 1).
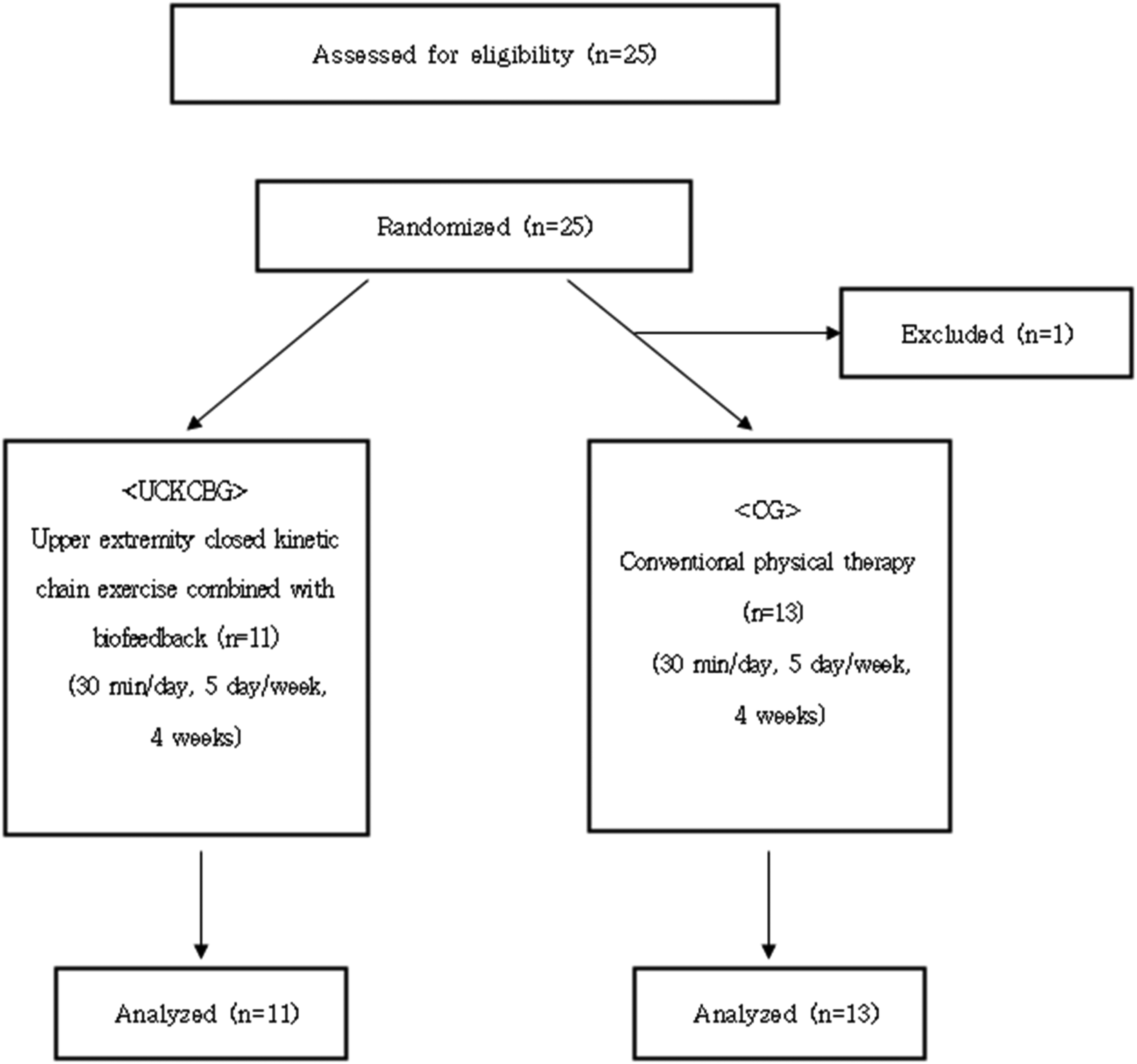
Experimental diagram.
The experimental group wore a shoulder mount strap equipped with a laser pointer (Figure 2), shined the laser pointer on the target board placed between both arms, and performed closed chain movements starting from the center and moving forward, right, left, and downward. Before starting the exercise, the distance traveled in the four directions of the experimental group was checked with a score, and the distance was measured every week during exercise to set the exercise intensity. The intensity of the exercise was set based on success 8 times or more by adding 1 point to the existing distance, and if the exercise was not successful, the exercise was performed so that it could move as much as the initial score. The exercises were performed in three different positions: First, standing with feet 40 cm away from a wall, facing it, with arms bent at 90 degrees and touching the wall (Figure 3). Second, using a Bobath table with the thigh of the experimental group elevated to 2/3 height, leaning with both hands while bending the shoulder joint 30 degrees, ensuring the palm is in a straight line with the upper arm (Figure 4). Third, in a quadruped position with the shoulder and hip joints bent at 90 degrees (Figure 5). Each position involved repeating the exercise movements 10 times, with a 2-min rest between positions to prevent muscle fatigue.

Shoulder mount strap equipped with a laser pointer.

Wall-supported standing position.

Leaning on both arms on the bobath table.
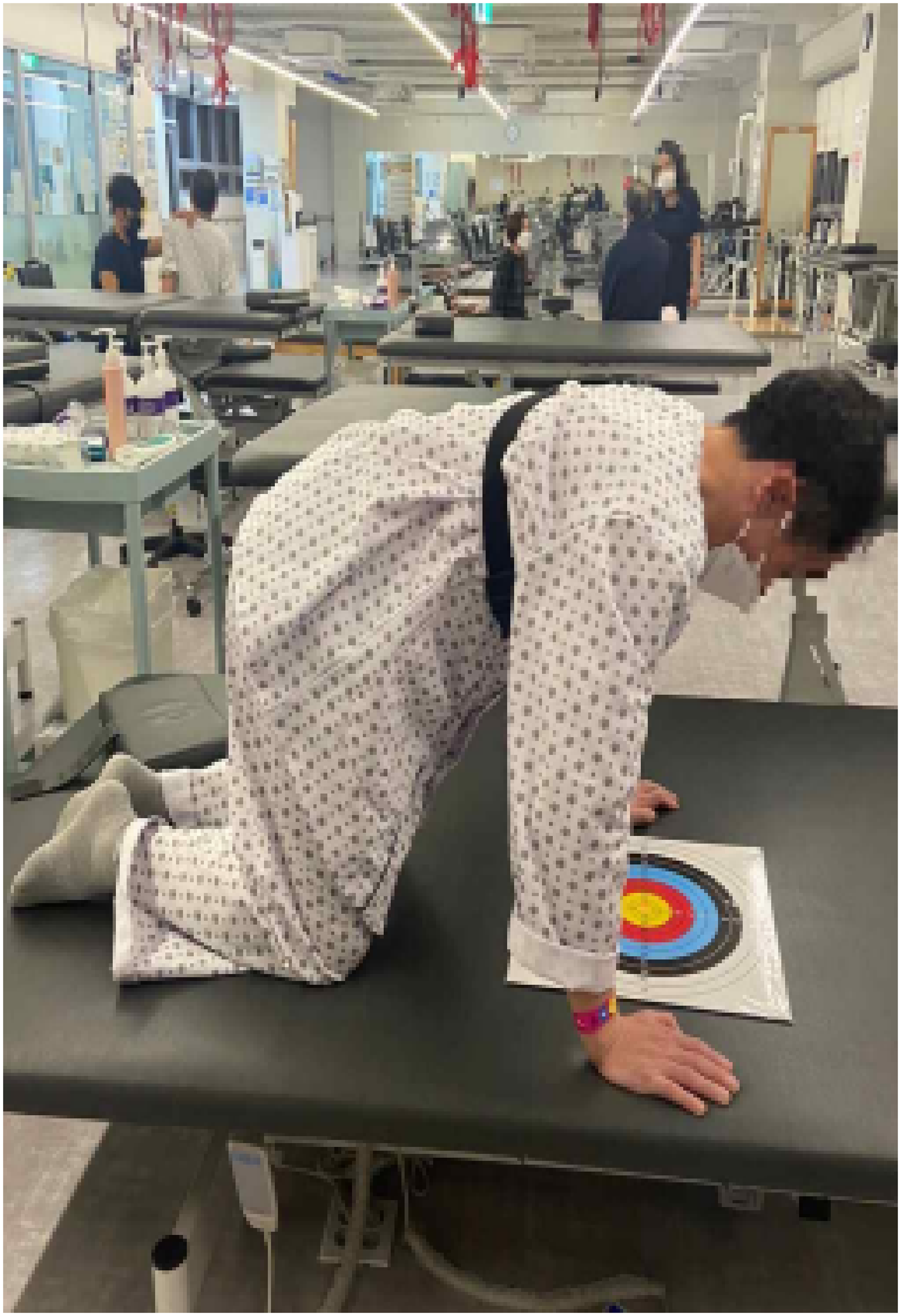
Quadruped position.
The control group received Bobath's neurodevelopmental therapy, proprioceptive neuromuscular stimulation, joint range of motion exercises, stretching, and upper and lower extremity muscle strengthening exercises as treatment according to the central nervous system development process performed one-on-one between a physical therapist and a patient. To prevent contamination in the control group, the treating therapists were not informed about the specific details of the study.
Outcome Measures
This study measured the results using clinical tests showing high reliability, validity, and sensitivity. Thumb Localizing Test(TLT) was used to evaluate the proprioceptibility of the shoulder joint, Medical Research Council Score(MRC) was used to evaluate muscle strength, Closed Kinetic Chain Upper Extremity Stability Test (CKCUST) was used to evaluate stability, and Fugl Meyer Assessment(FMA) was used to evaluate functional ability.
Thumb Localizing Test
TLT is widely used in the evaluation of proprioceptive sensory perception in stroke patients and is a test for “arm positioning.” It is clinically useful in that it can be used to examine invisible perceptual defects using exercise tasks and can be easily performed on the patient's bed (Otaka et al., 2020). It is a 4-point scale and consists of 0 point (finger grip correctly), 1 point (finger thumb is missed at first but corrected immediately), 2 points (facilitated by finding the thumb from the arm or wrist, or moving the fixed thumb), and 3 points (facilitated thumb cannot be located) (Rand, 2018), and is performed in four areas: proximal and distal areas of shoulder level and navel level. Reliability between test-retest of thumb-finding test is ICC = 0.83 (proximal area at the navel level)/0.80 (distal area at the navel level)/0.77 (proximal area at the shoulder level)/0.80 (distal area at the shoulder level), and reliability between evaluators is ICC = 0.83 (proximal area at the navel level)/0.90 (distal area at the navel level)/0.80 (proximal area at the shoulder level)/0.87 (distal area at the shoulder level) (Suda et al., 2021).
Medical Research Council Score
The MRC scale, which is a frequency strength assessment, is a total 25-point scale that calculates the sum of scores by evaluating the flexor, extensor, horizontal abductor, and horizontal adductor muscles of the paralyzed shoulder joint as 0 points (no contraction), 1 point (showing signs of contraction), 2 points (active movement with gravity removed), 3 points (active movement against gravity), 4 points (active movement against gravity and resistance), and 5 points (normal) (Compston, 2010). The test-retest reliability is r = .84∼.96 and the reliability between evaluators is r = .70∼.96 (Gregson et al., 2000).
Closed Kinetic Chain Upper Extremity Stability Test
CKCUEST is an assessment that provides scores for the work performance of the upper extremities in sports or clinical settings. The test measures the number of times a subject performs a push-up posture, has a distance of 36 inches between both arms, and can touch the back of the hand of his or her supporting hand with a hand that does not support weight, and has a 45-s break between measurements (Weon et al., 2021). In this study, a deformed motion with the knee touching the floor was performed in stroke patients, and the test-retest reliability of the closed chain upper body stability test was ICC > 0.75 and the reliability between evaluators was ICC > 0.75 (Tucci et al., 2014).
Fugl Meyer Assessment
FMA was designed to quantitatively evaluate the degree of functional recovery of stroke patients based on the stage of recovery of motor function after stroke (Fugl-meyer et al., 1975), and each item is divided into a 3-point scale that 0 points cannot be performed, 1 point can be partially performed, and 2 points can be fully performed (Lee et al., 2004). There are six items that can evaluate the upper and lower extremities, balance, sensation, and pain, and the total score of the upper limb evaluation items is 66 points, consisting of 18 items of shoulder, elbow, and lower arm, 5 items of wrist, 7 items of hand, and 3 items of upper limb coordination. FMA test-retest reliability is r = .86–.99 and the reliability between evaluators is r = .70–.99 (Sanford et al., 1993).
Statistical Analysis
All statistical analyses in this study were performed using SPSS 19.0 (SPSS Inc, Chicago, USA) to analyze specific variables. Difficulty in identifying subjects meeting the selection criteria led to a small sample size. Therefore, after conducting a Shapiro-Wilk test and confirming non-normal distribution, non-parametric tests were used. Sociodemographic variables of subjects were analyzed using means and standard deviations, while homogeneity between groups and differences in post-treatment changes were assessed using the Mann-Whitney U test. Changes within groups before and after treatment were analyzed using the Wilcoxon Signed-Rank test. The significance level (α) for all statistical tests was set at 0.05.
Results
This study targeted stroke patients and compared an experimental group, UCKCBG, which performed closed-chain upper limb exercises with biofeedback, against a control group (CG). Both groups showed homogeneity in general characteristics such as gender, age, height, weight (Table 1), and medical characteristics including diagnosis, onset duration, MMSE-K score, and MAS score (Table 2). There was no significant differences in the baseline value among the two groups (Table 3).
General Characteristics of Subjects. (n = 24)
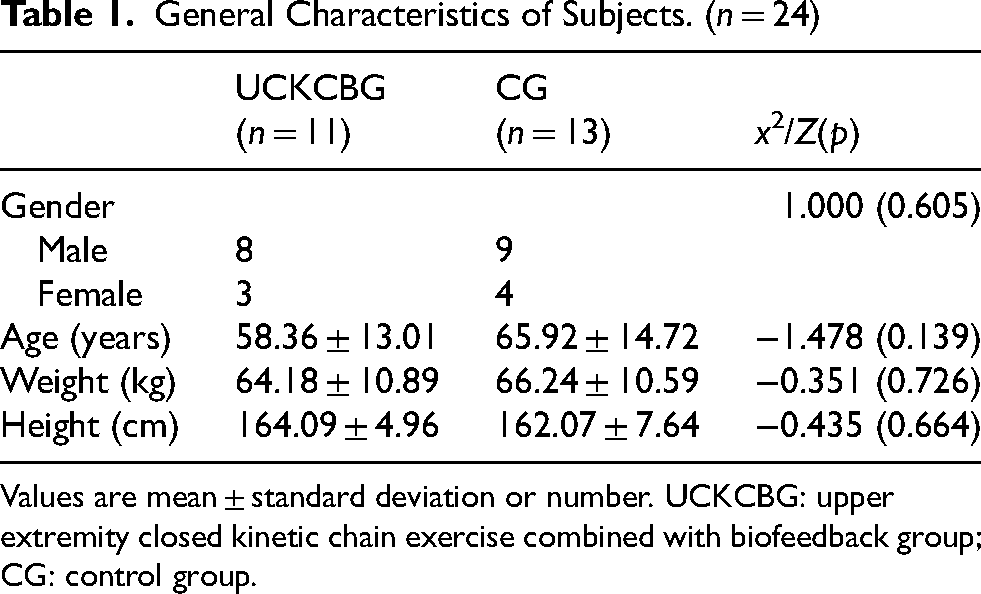
Values are mean ± standard deviation or number. UCKCBG: upper extremity closed kinetic chain exercise combined with biofeedback group; CG: control group.
Medical Characteristics of Subjects. (n = 24)
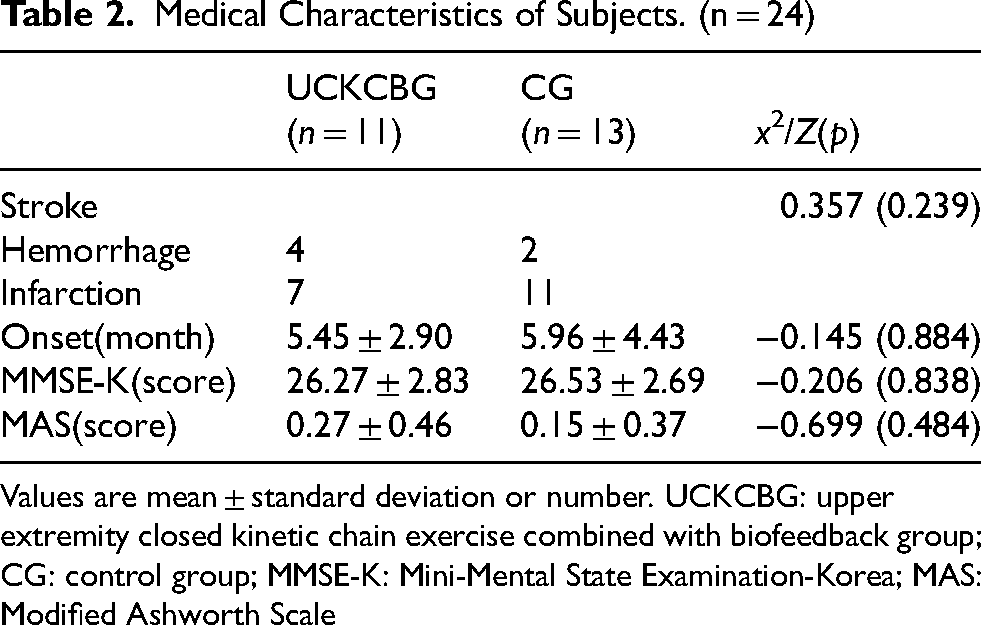
Values are mean ± standard deviation or number. UCKCBG: upper extremity closed kinetic chain exercise combined with biofeedback group; CG: control group; MMSE-K: Mini-Mental State Examination-Korea; MAS: Modified Ashworth Scale
Homogeneity Test for Measurement Items Across Subjects. (n = 24)
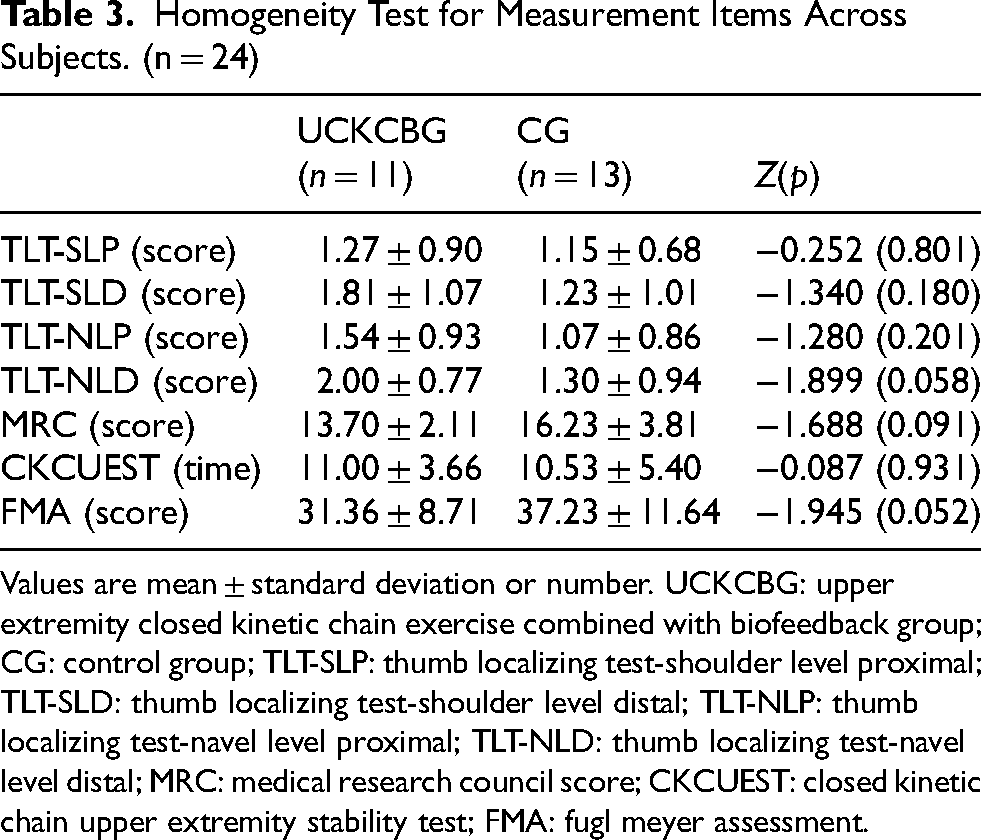
Values are mean ± standard deviation or number. UCKCBG: upper extremity closed kinetic chain exercise combined with biofeedback group; CG: control group; TLT-SLP: thumb localizing test-shoulder level proximal; TLT-SLD: thumb localizing test-shoulder level distal; TLT-NLP: thumb localizing test-navel level proximal; TLT-NLD: thumb localizing test-navel level distal; MRC: medical research council score; CKCUEST: closed kinetic chain upper extremity stability test; FMA: fugl meyer assessment.
Changes in proprioceptive sensory perception were evaluated using TLT. The results for the proximal area at the navel level and distal area at the navel level are shown in Tables 4–7 respectively. According to Tables 6 and 7, UCKCBG demonstrated significant improvements compared to CG after training (p < 0.05).
Comparison of Proprioception Abilities Measured by the TLT Proximal Area at the Shoulder Level. (n = 24)
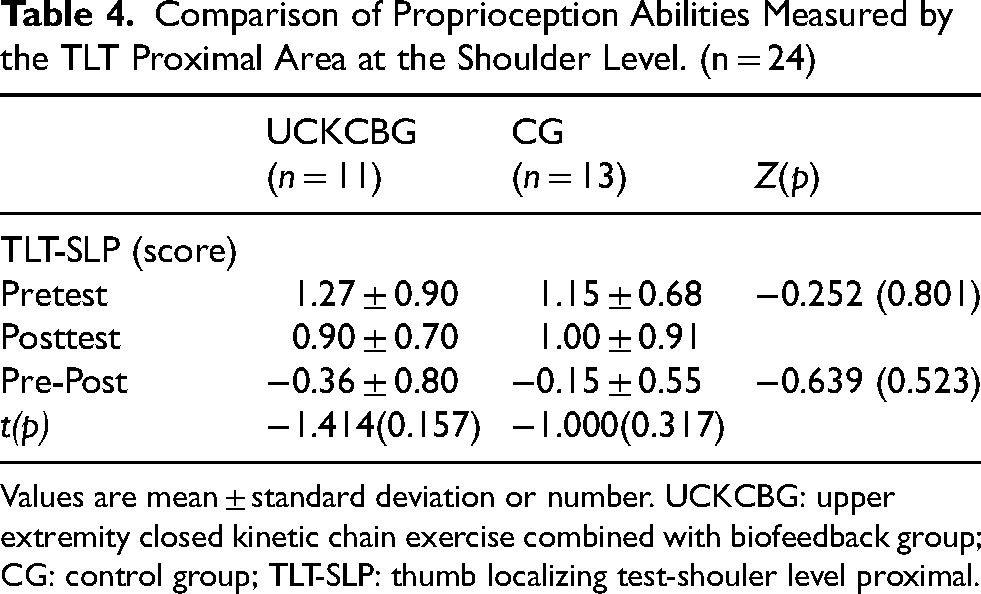
Values are mean ± standard deviation or number. UCKCBG: upper extremity closed kinetic chain exercise combined with biofeedback group; CG: control group; TLT-SLP: thumb localizing test-shouler level proximal.
Comparison of Proprioception Abilities Measured by the TLT Distal Area at the Shoulder Level. (n = 24)
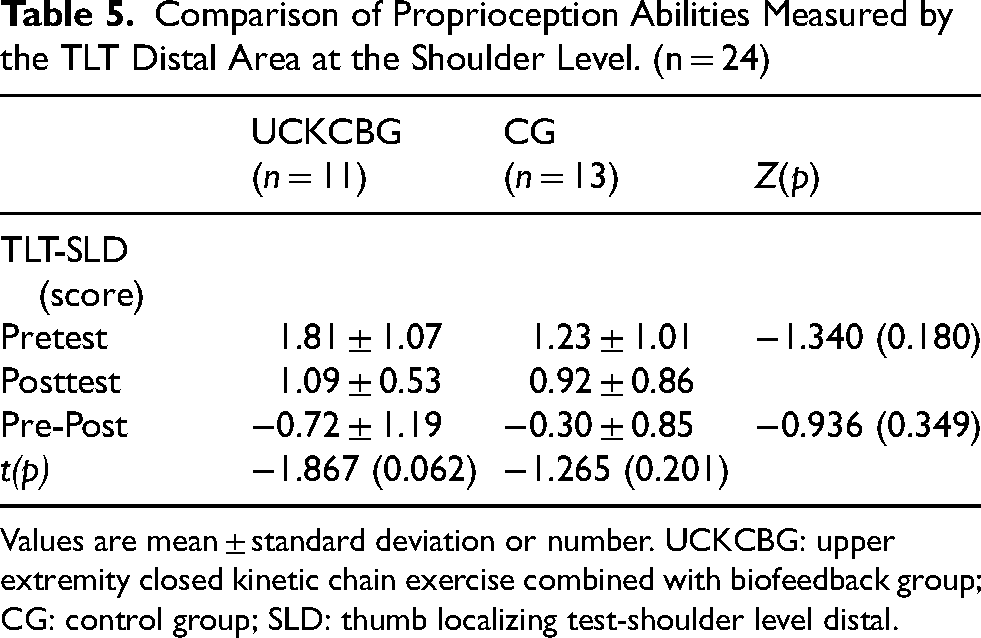
Values are mean ± standard deviation or number. UCKCBG: upper extremity closed kinetic chain exercise combined with biofeedback group; CG: control group; SLD: thumb localizing test-shoulder level distal.
Comparison of Proprioception Abilities Measured by the TLT Proximal Area at the Navel Level. (n = 24)
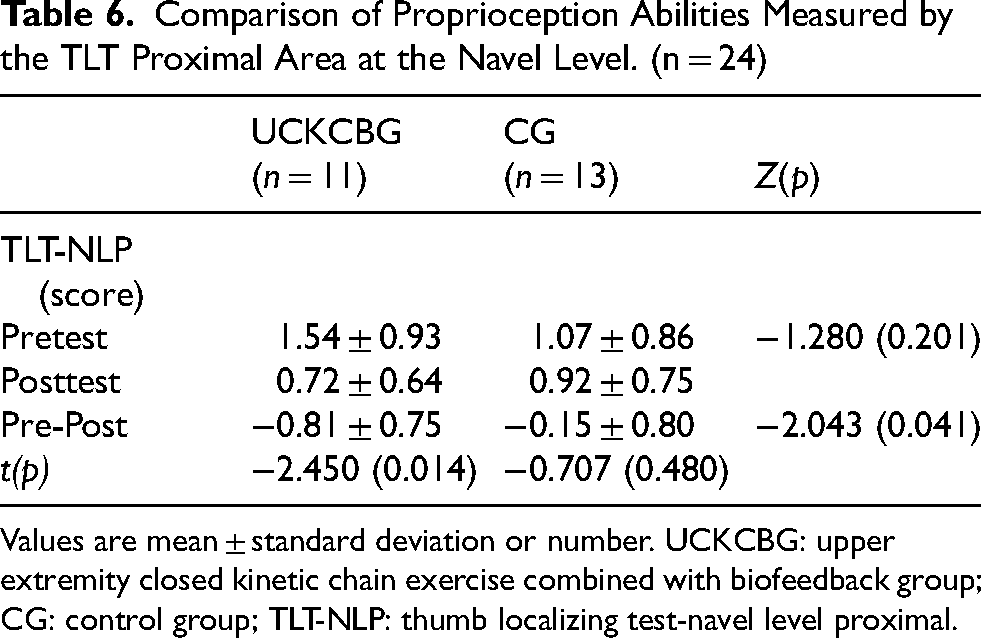
Values are mean ± standard deviation or number. UCKCBG: upper extremity closed kinetic chain exercise combined with biofeedback group; CG: control group; TLT-NLP: thumb localizing test-navel level proximal.
Comparison of Proprioception Abilities Measured by the TLT Distal Area at the Navel Level. (n = 24)
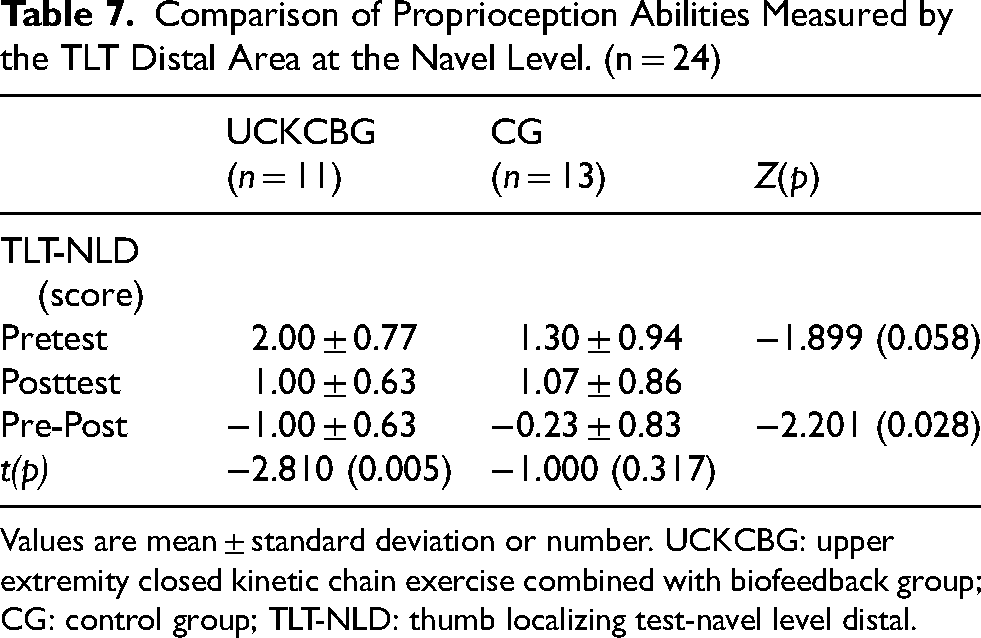
Values are mean ± standard deviation or number. UCKCBG: upper extremity closed kinetic chain exercise combined with biofeedback group; CG: control group; TLT-NLD: thumb localizing test-navel level distal.
Changes in muscle strength were assessed using MRC. The results are presented in Table 8. According to Table 8, both UCKCBG and CG showed significant increases after training, with UCKCBG showing a significant improvement compared to CG (p < 0.05).
Comparison of Strength Abilities Measured by the MRC. (n = 24)
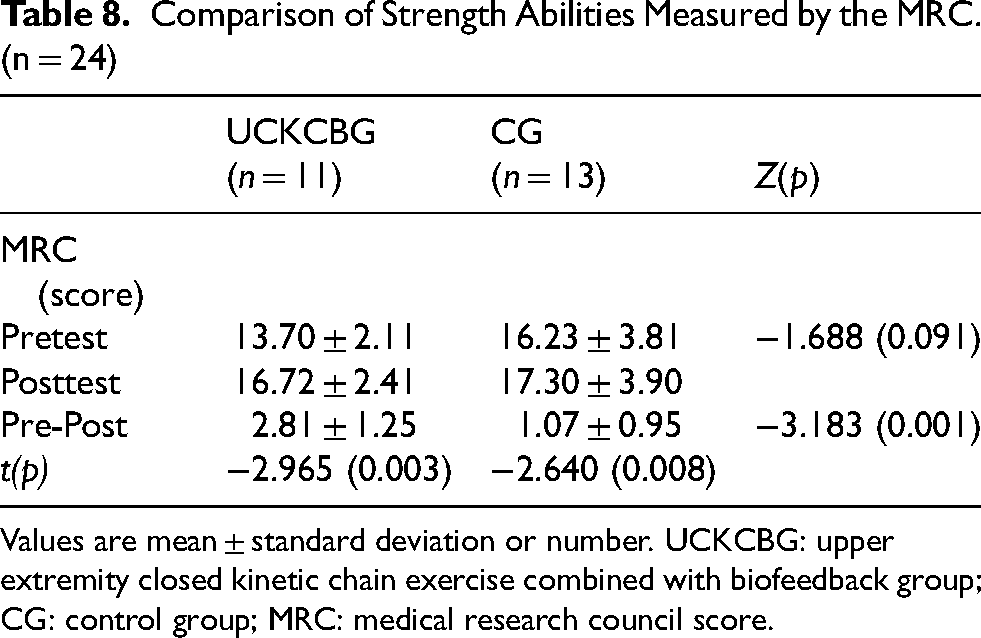
Values are mean ± standard deviation or number. UCKCBG: upper extremity closed kinetic chain exercise combined with biofeedback group; CG: control group; MRC: medical research council score.
Changes in stability were evaluated using CKCUEST. The results are presented in Table 9. Both UCKCBG and CG showed significant improvements after training, with UCKCBG showing a significant improvement compared to CG (p < 0.05).
Comparison of Stability Abilities Measured by the CKCUEST. (n = 24)
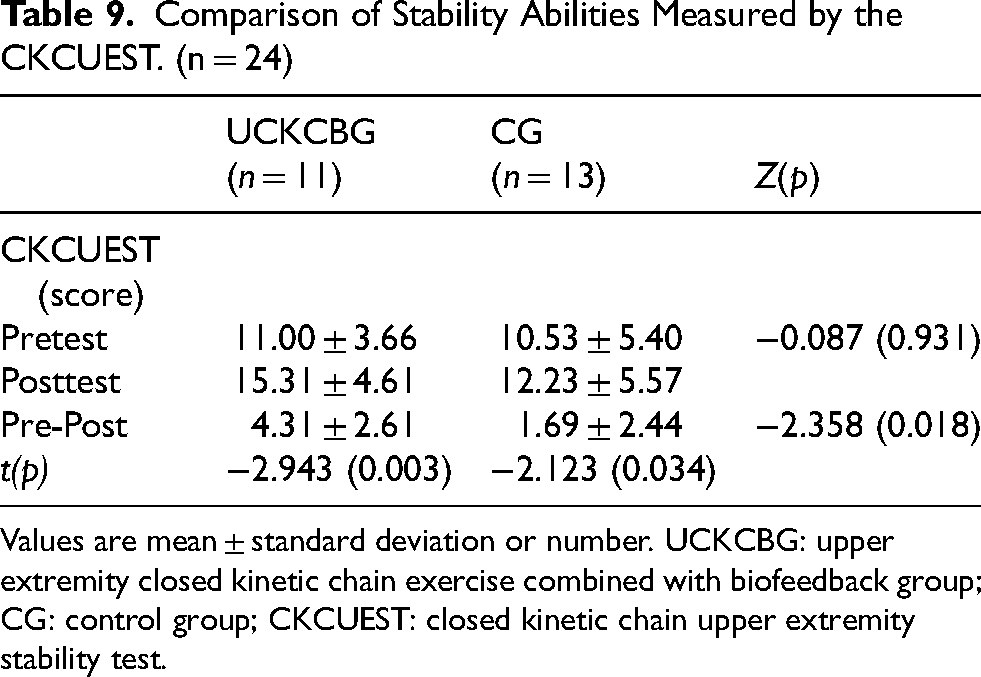
Values are mean ± standard deviation or number. UCKCBG: upper extremity closed kinetic chain exercise combined with biofeedback group; CG: control group; CKCUEST: closed kinetic chain upper extremity stability test.
Changes in upper limb function were assessed using FMA, with results shown in Table 10. UCKCBG showed a significant increase after training (p < 0.05), while CG showed no significant difference before and after training.
Comparison of Function Abilities Measured by the FMA. (n = 24)
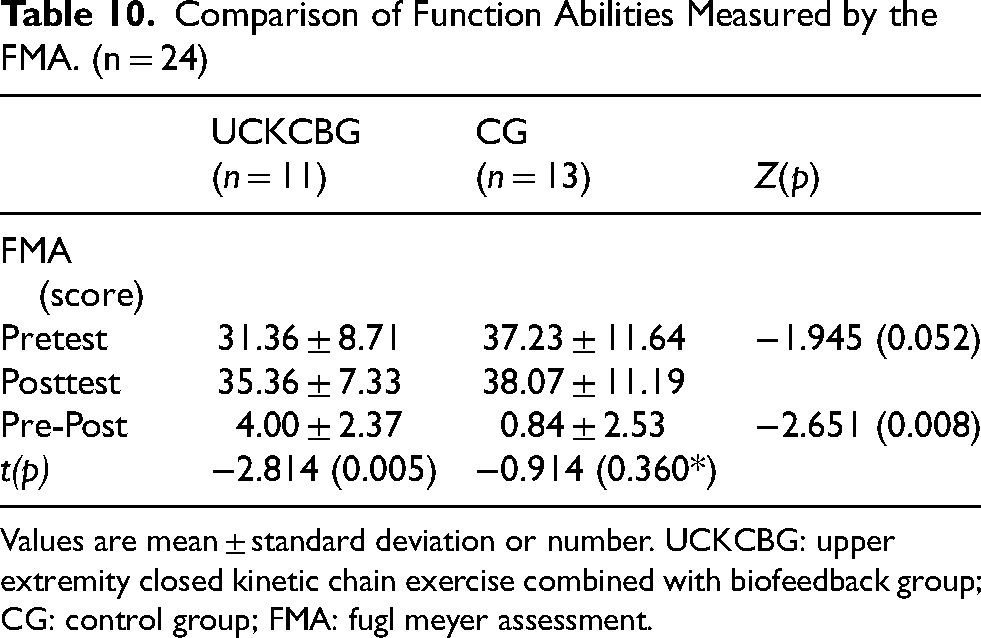
Values are mean ± standard deviation or number. UCKCBG: upper extremity closed kinetic chain exercise combined with biofeedback group; CG: control group; FMA: fugl meyer assessment.
Discussion
This study evaluated the effects of biofeedback-assisted closed chain upper limb exercises on proprioception, muscle strength, stability, and upper limb function in stroke patients. The study found significant improvements in these parameters compared to control exercises. Stroke commonly results in impaired somatosensory function and motor control of the upper limb, causing difficulties in activities of daily living such as personal hygiene, eating, and dressing (Meadmore et al., 2014), which are significant barriers to social reintegration. Therefore, the restoration of upper limb function is a crucial goal in stroke rehabilitation (Hayward et al., 2010).
Approximately 30–48% of stroke survivors experience deficits in proprioception of the upper limb post-stroke (Rand, 2018), highlighting the importance of proprioceptive exercises to optimize joint stability, enhance cognitive awareness related to posture, movements, and muscle stabilization (Rogol et al., 1998). It has been reported that intensive and repetitive sensory retraining programs using biofeedback can improve sensory deficits following stroke (He et al., 2022). Closed chain exercises replicate functional movements within the body, stimulate proprioception comprehensively, and are considered an effective rehabilitation approach when proprioception is impaired (Ghiasi & Akbari, 2007). To assess proprioception, the Two-point Discrimination Test (TLT) was used in this study. Both experimental and control groups showed statistically significant improvements in the supraumbilical region after treatment (p < 0.05), with the experimental group demonstrating superior outcomes (p < 0.05). The exercise involved in biofeedback-assisted closed chain upper limb exercises enhanced proprioception by increasing sensory input to the joints through strong pressure (Park & Kim, 2017) and improving movement accuracy through immediate visual feedback (Yoon et al., 2011). Thus, biofeedback-assisted closed chain upper limb exercises were found to enhance proprioception in stroke patients.
Muscle strength refers to the ability of muscles to generate force during segmental or whole-body acceleration or deceleration. Stroke affects the ability of muscles to generate force, which in turn affects movement acceleration or deceleration (Bohannon, 2007). Post-stroke muscle weakness is one of the factors limiting functional recovery (Park et al., 2013). Exercises using biofeedback increase average firing rates of nerves, the number of motor units activated, and synchronous activation of motor units, thereby increasing muscle strength (Anwer et al., 2011). Closed chain exercises promote joint stabilization by enhancing neuromuscular facilitation and increasing co-activation of muscles, making them beneficial for enhancing muscle strength in patients with acute muscle weakness (Andrade et al., 2011). To measure muscle strength, the Medical Research Council (MRC) scale was used in this study. Both experimental and control groups showed statistically significant effects (p < 0.05), with the experimental group demonstrating a significant increase compared to the control group (p < 0.05). Biofeedback-assisted closed chain upper limb exercises influenced muscle strength by gradually increasing shoulder muscle activity through arm movements involving the unaffected arm (Uhl et al., 2003), thus inducing muscle contraction and enhancing physiological changes and muscle hypertrophy (Kiper et al., 2015).
Upper limb function refers to the ability to perform actions such as grasping objects or reaching towards targets. Upper limb strength and sensory function are closely related, and their changes affect upper limb function (Lee et al., 2013). Functional impairment following stroke is due to impaired proprioception, muscle strength, muscle endurance, and joint stability (Park et al., 2013). In this study, the Fugl-Meyer Assessment (FMA) was used to measure upper limb function, and the experimental group showed significant improvements post-treatment (p < 0.05), with significant differences observed between the groups (p < 0.05). Biofeedback provides information about the body's condition, supports patients in improving their body functions (Parel et al., 2023), and exercises involving biofeedback are essential for improving the function of the impaired upper limb (He et al., 2022). Closed chain exercises establish early shoulder joint stability to provide a stable foundation for functional activities (Rogol et al., 1998), making them a crucial strategy for enhancing shoulder muscle activation and improving functional activities (Reistetter et al., 2009).
Restoring upper limb function is a crucial goal of rehabilitation for stroke patients’ daily activities and social reintegration (Hayward et al., 2010). Biofeedback-assisted closed chain upper limb exercises have been effective in enhancing proprioception, muscle strength, stability, and improving functional activities (Dilek et al., 2016). This study, like previous studies, suggests that biofeedback-assisted closed chain upper limb exercises show significant differences in proprioception, muscle strength, stability, and function of the upper limb. It is suggested that improvements in proprioception and muscle strength during closed chain exercises increase weight shift to the paralyzed side, and stability improvement has a significant impact on upper limb function. Therefore, it was found that there was an effect on proprioception, muscle strength, and function.
Limitations of this study include the difficulty in recruiting an adequate number of participants who met the criteria for upper limb function, leading to a small sample size. The study was conducted with hospitalized patients from a single region, making generalization challenging. Additionally, the variety of positions in closed chain upper limb exercises was limited, and there was no follow-up assessment after the study to determine the sustainability of the effects. Future research should aim to recruit a larger number of participants who meet specific criteria for upper limb function and include a variety of closed chain exercise positions. This would allow for a more accurate assessment of the effects of biofeedback-assisted closed chain upper limb exercises on improving proprioception, muscle strength, stability, and function in stroke rehabilitation.
Conclusion
This study was conducted to investigate the effects of closed-chain upper limb exercises with biofeedback on proprioceptive sensory perception, muscle strength, and upper limb function in stroke patients. The results of the study demonstrated that closed-chain upper limb exercises with biofeedback showed significant improvements in proprioceptive sensory perception, muscle strength, and function of the upper limb compared to conventional physical therapy.
It was confirmed that closed-chain upper limb exercises with biofeedback are effective in enhancing proprioceptive sensory perception, muscle strength, and function of the upper limb. Therefore, incorporating closed-chain upper limb exercises with biofeedback into rehabilitation therapy for stroke patients, who often face challenges in upper limb function recovery, could be considered as a therapeutic approach to increase proprioceptive sensory perception, muscle strength, and function of the upper limb.
Footnotes
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Statement
This study complies with the Declaration of Helsinki and was performed according to the Bioethics Committee of Sahmyook University (Approval Number: 2023-06-018-006). Registered with the Clinical Research Information Service, this study adheres to the World Health Organization International Clinical Trials Registry Platform (WHO-ICTRP) guidelines (registration number: KCT0009737).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.