
Abstract
Background
Repetitive transcranial magnetic stimulation (rTMS) has shown potential in rehabilitating patients with incomplete spinal cord injury (iSCI). However, the evidence is mainly based on small-scale studies with varying protocols.
Objective
To summarize the impact of rTMS on motor function deficits in individuals with iSCI and identify optimal stimulation parameters through a meta-analysis.
Methods
A systematic literature search was conducted in multiple databases from inception to July 31, 2024. Randomized controlled trials investigating rTMS effects on motor function in iSCI were included. Study quality was assessed using the RoB 2 and PEDro scale. RESULTS: Eleven studies with 345 participants were included. rTMS applied at 100–110% of resting motor threshold (SMD = 0.81, P = 0.0005), with over 15 stimulation sessions (SMD = 0.66, P = 0.04) and a cumulative pulse count of 1800 (SMD = 0.50, P = 0.04), significantly enhanced motor function recovery in iSCI patients. Four studies reported mild, transient adverse effects in 11 patients.
Conclusion
rTMS may enhance motor function in iSCI patients with certain parameters. However, given study limitations, conclusions should be viewed as exploratory.
Keywords
Introduction
Spinal Cord Injury (SCI) is characterized by damage to the spinal cord from traumatic or non-traumatic causes, potentially leading to temporary or permanent functional impairments (Ahuja et al., 2017). Globally, annual SCI incidence rates vary from approximately 10.04 to 83 per million (Karsy & Hawryluk, 2019). Following SCI, individuals may experience reduced motor and sensory functions, autonomic dysfunction, and neurogenic pain, leading to significant physiological, social, and vocational impacts on patients and their families (Dietz & Fouad, 2014). In scenarios where incomplete spinal cord injury (iSCI) occurs, there is potential for some functional recovery as several cortical, subcortical, and spinal circuits are intact, with some fibers being undamaged (Raineteau & Schwab, 2001). Research indicates that motor function recovery is considered the most critical need within a decade after iSCI (Lo et al., 2016). Motor function impairments following SCI encompass a series of impairments, including but not limited to changes in muscle strength, muscle tone, motor control, coordination, and flexibility (Cieza et al., 2010). These deficits are a key focus in SCI rehabilitation, especially in patients with iSCI. Thus, identifying methods to expedite motor function recovery post-iSCI is a major challenge in rehabilitation medicine. The current clinical treatment for iSCI primarily involves a comprehensive approach that includes respiratory and mobility training, physical and occupational therapy, decompression surgery, anti-inflammatory drugs, and stem cell transplantation, among others (Anjum et al., 2020; Harvey, 2016; Jendelova, 2018). However, approximately 40–50% of patients continue to experience long-term or even lifelong motor function impairments (Hornby et al., 2020).
Repetitive Transcranial Magnetic Stimulation (rTMS) is a non-invasive technique for brain stimulation. It employs a magnetic coil to generate rapidly changing magnetic fields that pass through the skull, inducing electric currents in specific cortical areas. Depending on the stimulation parameters, rTMS can either facilitate or suppress neuronal activity in targeted brain regions (Hallett, 2007). Commonly, single-pulse transcranial magnetic stimulation (TMS) is used in examining cerebral functionality, while rTMS is applied to provoke changes in neural activity (Klomjai et al., 2015). rTMS effects are often sustained after the stimulation phase, and is broadly agreed that these could affect the result from the processes of neural adaptability, especially through long-term potentiation (LTP) and long-term depression (LTD) (Hoogendam et al., 2010; Suppa et al., 2016). Documented benefits of rTMS include its integration into clinical treatments for stroke, Parkinson's disease, epilepsy, pain, depression, cognitive disorders, and sleep disturbances (Lefaucheur et al., 2014, 2020). Recently, TMS has been increasingly used to evaluate and treat motor impairments after iSCI (Wang et al., 2023). As a diagnostic tool, TMS helps in identifying residual corticospinal connections and neural recovery post-SCI (Squair et al., 2016). Moreover, leveraging the principles of reshaping neural pathways and enhancing neuroplasticity, rTMS has been used to examine motor function enhancement among individuals diagnosed with iSCI (Krogh et al., 2022a). However, small sample sizes and variable protocols in studies(Lefaucheur et al., 2020; Schoisswohl et al., 2019) weaken the data quality on rTMS for post-iSCI motor recovery in practice.
Recently, reviews have been conducted on rTMS stimulation protocols (Brihmat et al., 2022); however, the absence of quality assessment and heterogeneity analysis in the included literature could pose a considerable risk of publication bias. Furthermore, standardized rTMS protocols encompass a range of parameters (Hallett, 2007; Klomjai et al., 2015), including stimulation frequency, intensity, coil type, number of pulses, and treatments per session, which influence therapeutic outcomes and safety. This diversity complicates the identification of the optimal stimulation protocol. Moreover, given the widely recognized variability in outcomes (Schoisswohl et al., 2019), it is challenging to establish a standardized protocol for optimal stimulation parameters.
This meta-analysis examined the effects of various rTMS protocols on motor function recovery in patients with SCI. The study aimed to identify effective parameters while recognizing their efficacy may vary with individual characteristics and clinical contexts. The objective of this study is to identify effective parameters for improving motor function in patients with iSCI, synthesize evidence, and guide their clinical application.
Methods
Data Sources and Study Selection
This review adhered to the protocols specified in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Page et al., 2021). It is registered with the International Prospective Register of Systematic Reviews (PROSPERO) (registration number: CRD42023495022).
A pair of independent investigators searched databases including PubMed, Embase, Cochrane Library, Web of Science, and CNKI from their inception until July 2024. The detailed search strategies are shown in electronic Suppl. File 1.
The studies were chosen according to the following eligibility criteria: (1) Study Type: Randomized controlled trials (RCTs). (2) Participants: Patients with motor function impairment following iSCI. (3) Intervention Measures: The control group received either a placebo or conventional rehabilitation training, while the experimental group underwent rTMS treatment in addition to the control group's interventions. (4) Outcome Measures: Extractable data presented as means and standard deviations, used to evaluate limb motor function. The exclusion criteria were as follows: (1) Studies not aimed at improving motor function impairment; (2) Insufficient or unusable data after contacting the corresponding author; (3) Articles with poor methodological quality, defined as those scoring ≤3 on the PEDro scale.
Data Extraction
Two researchers independently gathered data from the selected papers: the first author's name, number of participants, age, sex, duration of illness, severity of spinal cord injury, rTMS intervention parameters, and outcome measures. For each study, we extracted the mean differences and standard deviations of the between-group (rTMS vs. control) changes from baseline to post-treatment for each outcome measure. The researchers extracted data from each study and assessed its suitability for study inclusion. Disagreements in data extraction or inclusion decisions were resolved through consultation with a third contributor.
Quality Assessment of Included Studies
The quality of the included RCTs was independently evaluated by two reviewers using both the revised Cochrane risk-of-bias tool for randomized trials (RoB 2) (Sterne et al., 2019) and the PEDro scale (Cashin & McAuley, 2020). The RoB 2 assessed: randomization process, outcome data completeness, allocation concealment, outcome measurement accuracy, selective reporting, and other biases. The studies were classified as ‘low risk’, ‘high risk’, or ‘some concerns’. The PEDro scale categorized studies as “good” (6+), “fair” (4–5), or “poor” (≤3). Studies with a score of ≤3 on the PEDro scale were excluded from our analysis. Any disagreements between reviewers were first addressed through discussion and, if unresolved, by a third independent adjudicator.
Statistical Analysis
Statistical analyses were conducted with RevMan 5.4 (Cochrane Collaboration, London, UK). The analyses calculated the effect sizes by the mean and standard deviation differences post-rTMS between the experimental and control groups. The standardized mean difference (SMD) for each outcome measure in every study was calculated along with 95% confidence intervals (CI). The magnitude of effect sizes was classified as small (SMD < 0.4), medium (0.4 ≤ SMD ≤ 0.69), or large (SMD > 0.70) (Higgins, 2008).
We assessed heterogeneity with the I2 statistic (Higgins et al., 2003). Sensitivity assessments were performed when I2 was over 50% and P < 0.05 to determine the impact of individual studies on the overall estimate. Funnel plots assessed publication bias for subgroups with over 10 studies. A P-value < 0.05 was considered significant.
Results
Literature Screening Process and Results
The initial search yielded 2,049 articles. After removing duplicates using EndNote 21 software (Clarivate, Philadelphia, USA) and the abstracts were screened according the inclusion and exclusion criteria. This process ultimately resulted in the inclusion of 11 articles for meta-analysis. Figure 1 presents the flowchart of the study selection process.
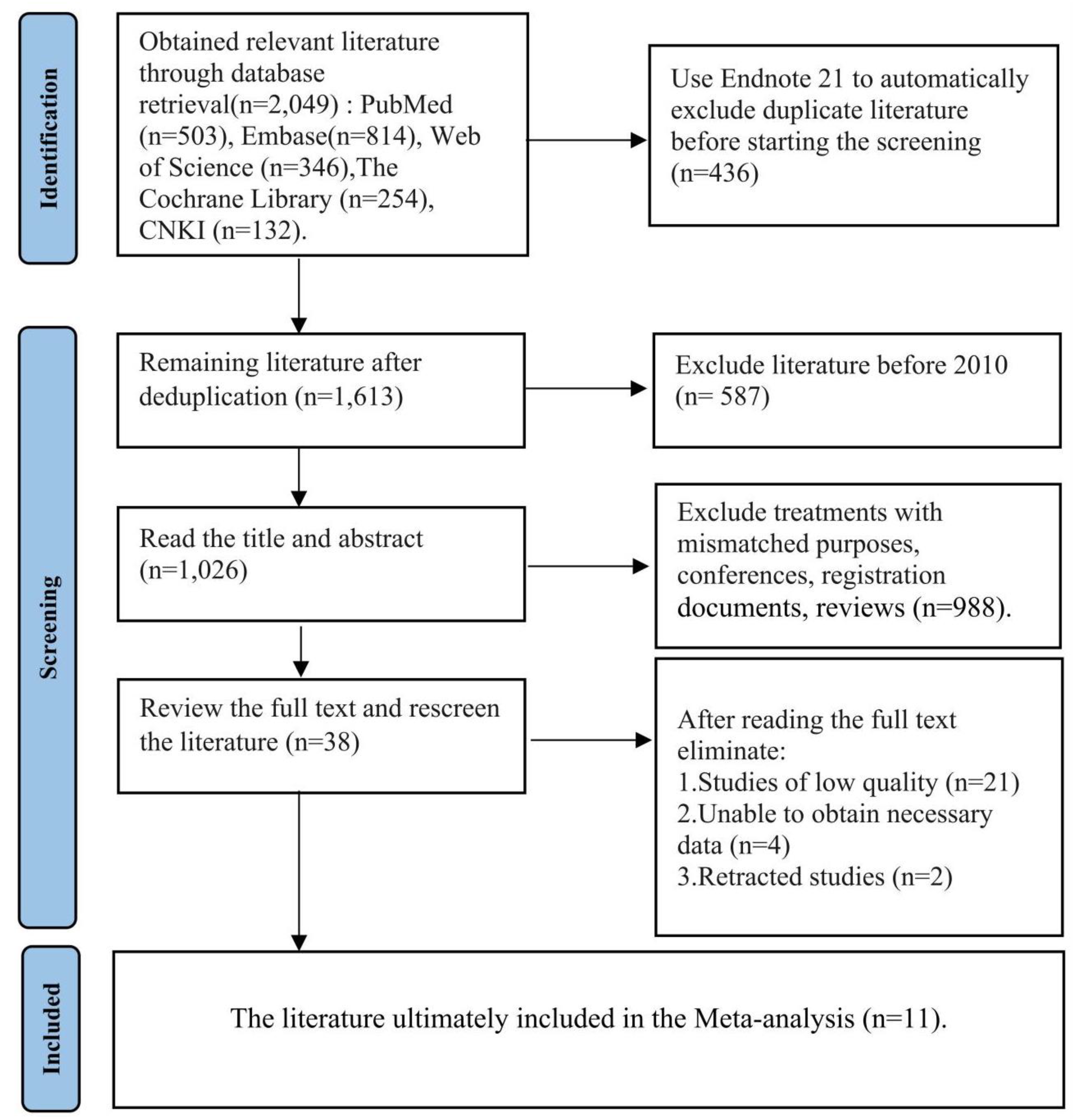
Flow chart of literature screening.
Characteristics of Studies
A total of 11 RCTs (Benito et al., 2012; Feng et al., 2023; Gomes-Osman & Field-Fote, 2015; Kesikburun et al., 2023; Krogh et al., 2022b; Kumru et al., 2010, 2016; Liang et al., 2021; Sun et al., 2019; Wang et al., 2016; Wincek et al., 2021) were included, comprising 345 patients with incomplete spinal cord injuries. This group was divided into 187 participants who received TMS and 178 participants in the control groups. Most of the included RCTs were parallel controlled trials, with three studies being crossover trials (Benito et al., 2012; Gomes-Osman & Field-Fote, 2015; Kumru et al., 2010). In the crossover trials, the rTMS protocol sequences were randomized and balanced across participants. The mean age of the participants was 40.45 (12.88) years, mostly with American Spinal Injury Association Impairment Scale (AIS) classifications C and D. Regarding adverse effects, four studies noted transient mild discomfort post-rTMS (Krogh et al., 2022a; Kumru et al., 2010; Sun et al., 2019; Wang et al., 2016). Specifically, eight cases (2%, 8/345) of temporary facial muscle spasms were reported and two patients (1%, 2/345) experienced mild scalp discomfort or headache after the first treatment (Krogh et al., 2022a; Kumru et al., 2010). Additionally, one patient experienced a seizure after treatment (Krogh et al., 2022a). (Table 1)
Characteristics of the Included Literature.
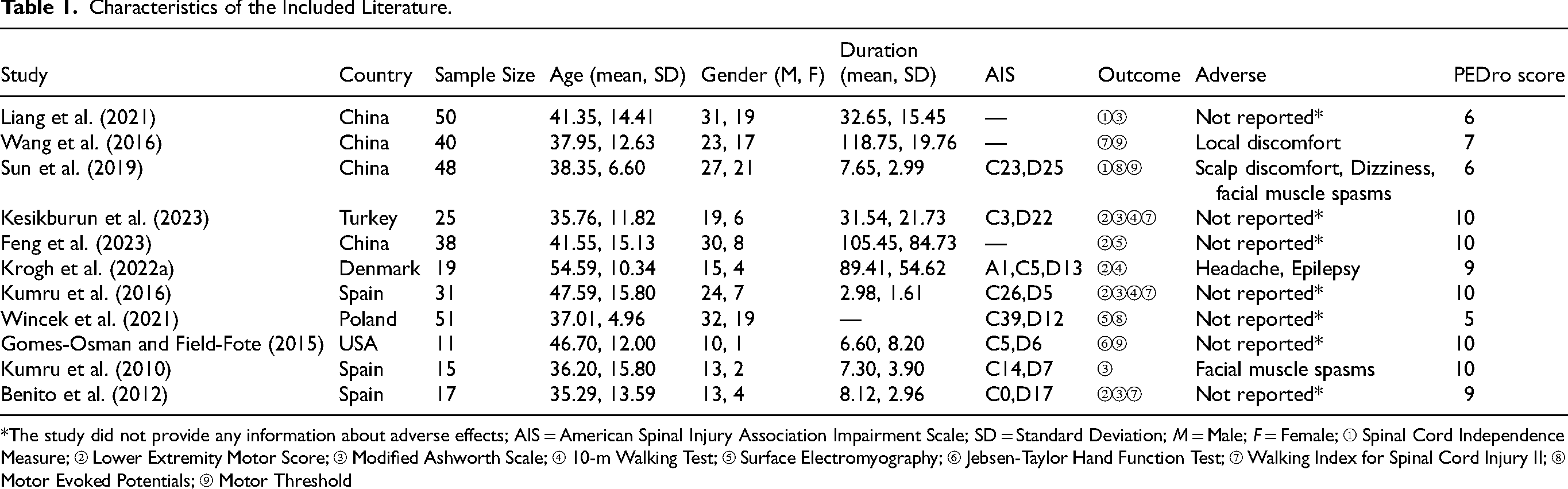
*The study did not provide any information about adverse effects; AIS = American Spinal Injury Association Impairment Scale; SD = Standard Deviation; M = Male; F = Female; ① Spinal Cord Independence Measure; ② Lower Extremity Motor Score; ③ Modified Ashworth Scale; ④ 10-m Walking Test; ⑤ Surface Electromyography; ⑥ Jebsen-Taylor Hand Function Test; ⑦ Walking Index for Spinal Cord Injury II; ⑧ Motor Evoked Potentials; ⑨ Motor Threshold
The frequency of rTMS application varied from 9 to 20 Hz, with intensities ranging from 70% to 110% of the resting motor threshold (RMT). The number of pulses ranged from 600 to 1800. One study utilized Theta Burst stimulation (Feng et al., 2023), a potent form of rTMS. Detailed information regarding the stimulation protocols is presented in Table 2
Stimulation Protocol for Repetitive Transcranial Magnetic Stimulation.
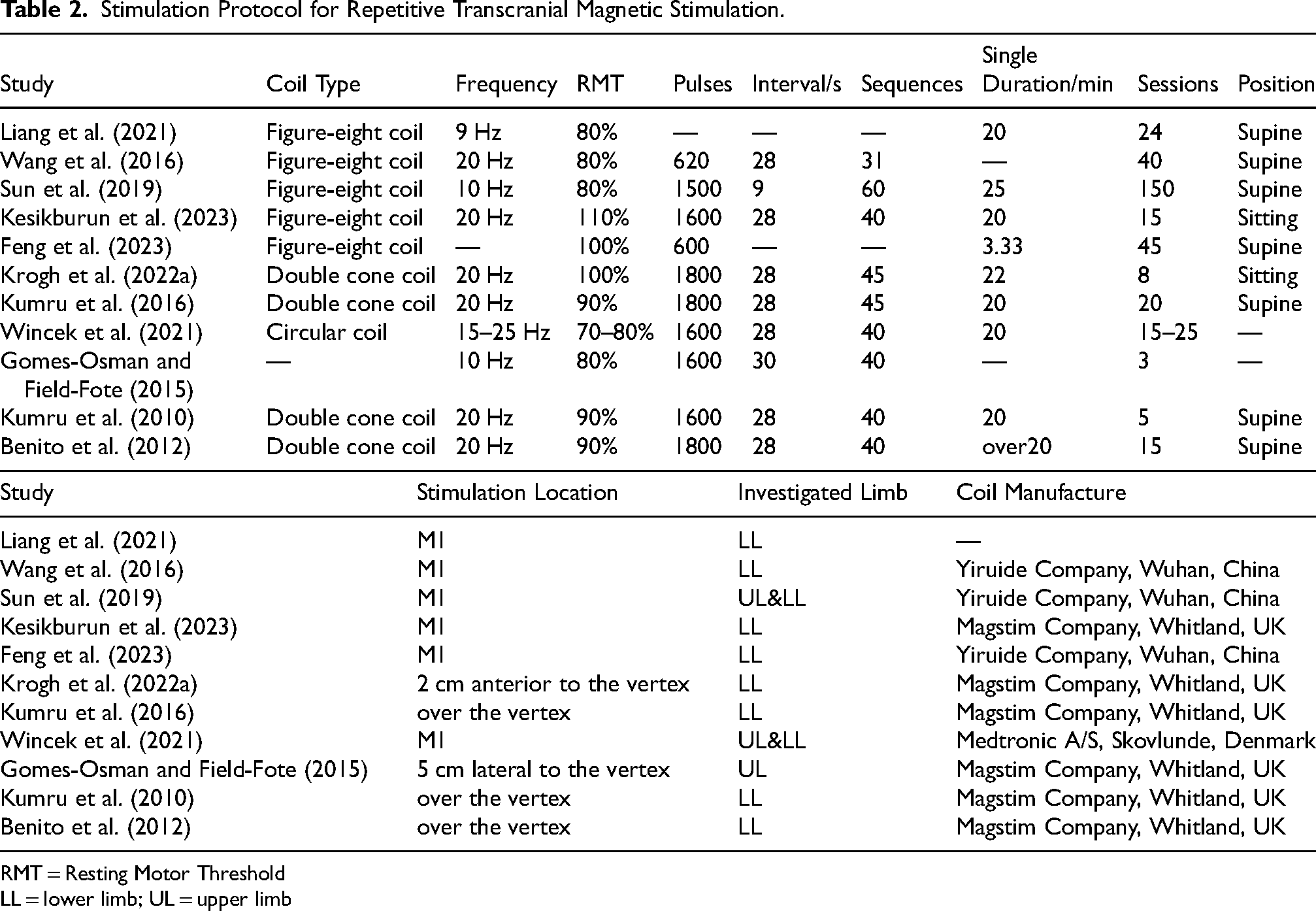
RMT = Resting Motor Threshold
LL = lower limb; UL = upper limb
Quality Assessment Results
Using the PEDro scale for procedural and descriptive evaluation, a high standard of methodological rigor was generally observed. The studies had a median PEDro score of 9 (range: 5–10). (Table 1
The assessment using the RoB 2 tool indicated that eight studies had low risk of bias (Benito et al., 2012; Feng et al., 2023; Kesikburun et al., 2023; Krogh et al., 2022b; Kumru et al., 2016; Liang et al., 2021; Sun et al., 2019; Wang et al., 2016), two studies had some concerns (Gomes-Osman & Field-Fote, 2015; Kumru et al., 2010), and one study had a high risk of bias (Wincek et al., 2021). (Figure 2)
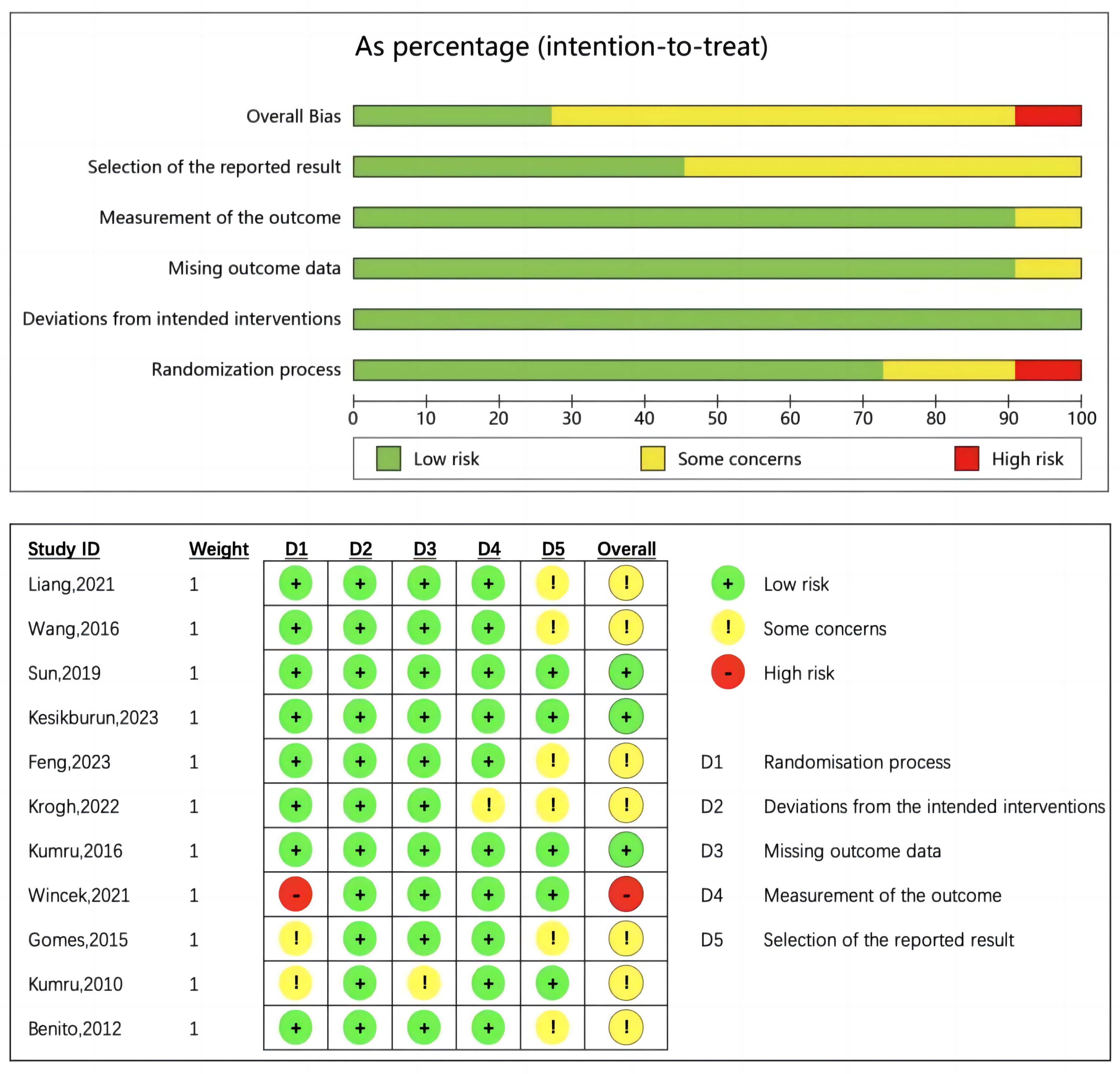
Quality evaluation results and evaluation summary of the included literatur.
Effect of Intervention Measures
Motor function
Ten of the included studies (Benito et al., 2012; Feng et al., 2023; Gomes-Osman & Field-Fote, 2015; Kesikburun et al., 2023; Krogh et al., 2022b; Kumru et al., 2010, 2016; Liang et al., 2021; Sun et al., 2019; Wang et al., 2016) evaluated limb motor function recovery post-rTMS, as shown in Table 1. The assessment tools used included the Spinal Cord Independence Measure III (SCIM III), Lower Extremity Motor Score (LEMS), Modified Ashworth Scale (MAS), 10-Meter Walking Test (10MWT), Surface Electromyography (sEMG), and the Jebsen-Taylor Hand Function Test (JTT), among others. The results demonstrated that rTMS significantly improved motor function in patients with iSCI compared to the control group, with a medium effect size (SMD = 0.43, 95% CI: 0.20 to 0.66, p = 0.0002). (Figure 3)
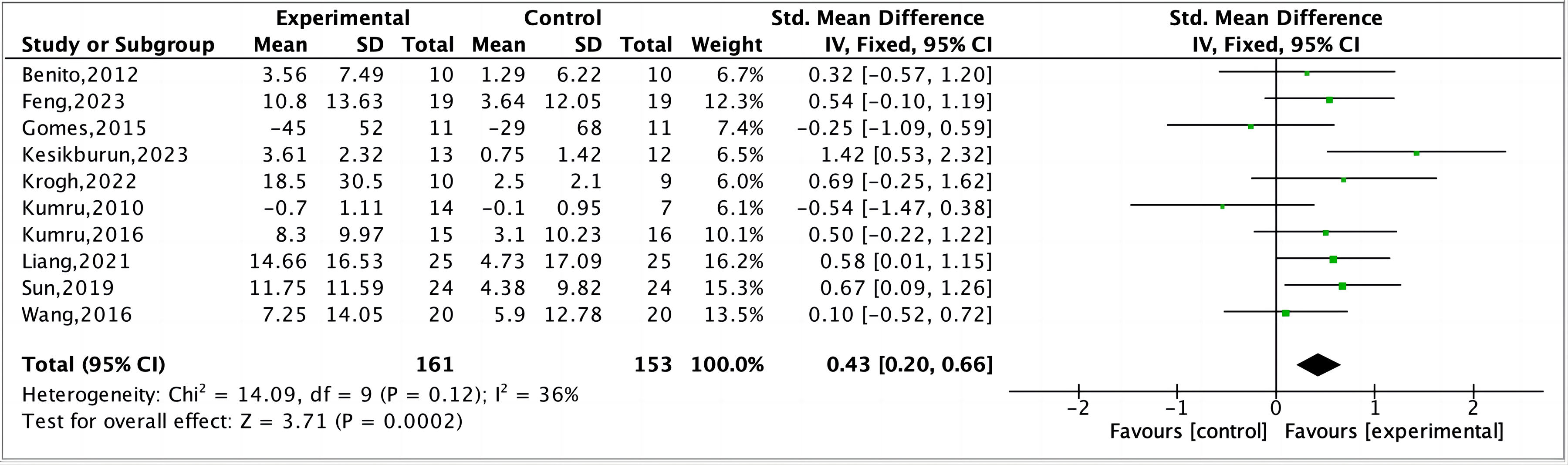
Forest map of the meta-analysis of motor function by rTMS.
Impact of Stimulation Parameters on Motor Function
Stimulation Frequency
Among the 10 articles (Benito et al., 2012; Kesikburun et al., 2023; Krogh et al., 2022b; Kumru et al., 2010, 2016; Liang et al., 2021; Sun et al., 2019; Wang et al., 2016; Wincek et al., 2021) that reported specific stimulation frequencies, the analysis for the 15–25 Hz range demonstrated a non-significant effect with a small effect size estimation (SMD = 0.27, 95% CI: −0.18–0.73, P = 0.24). For frequencies of 9–10 Hz, the analysis also showed a non-significant effect (SMD = 0.42, 95% CI: −0.08–0.91, P = 0.10). No significant differences were found between subgroups before and after sensitivity analysis. (Figure 4)
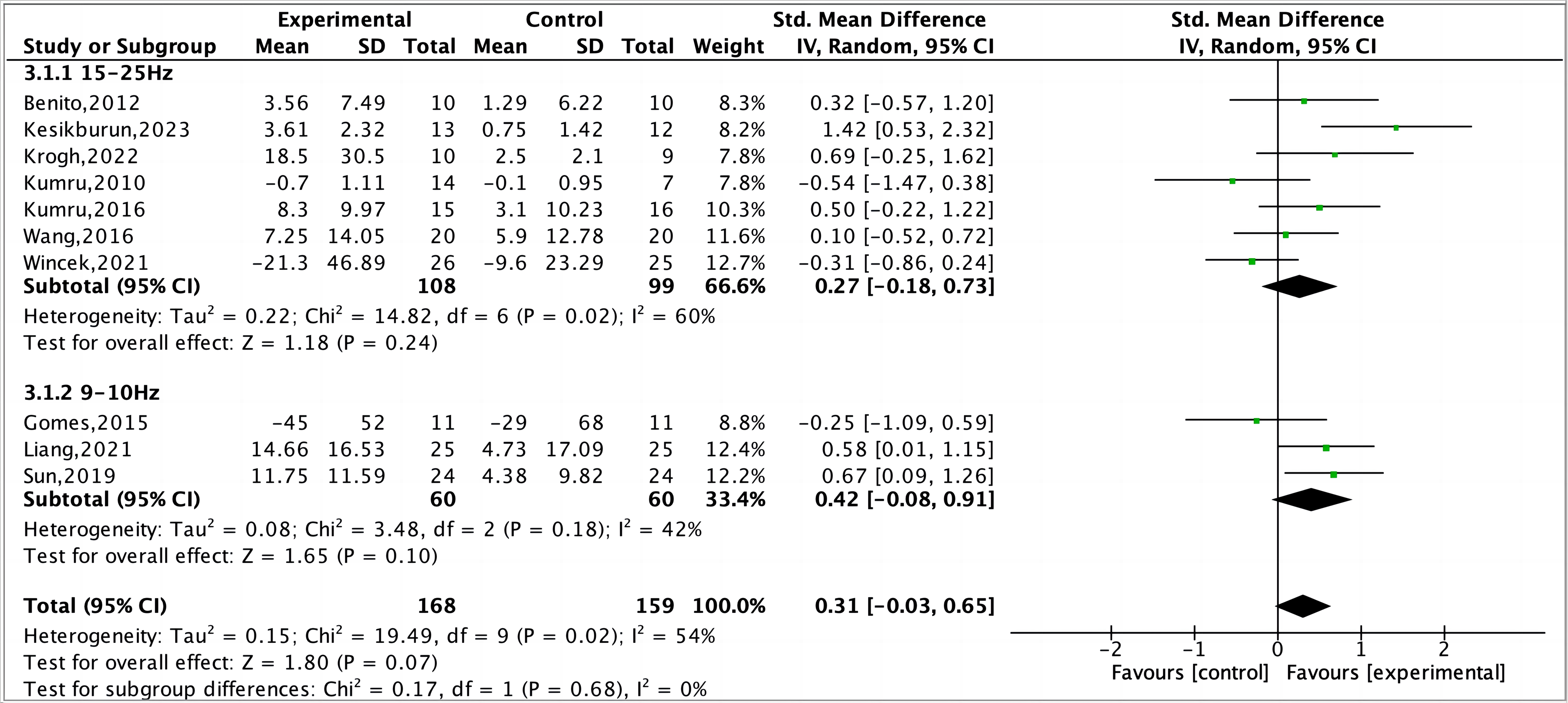
Forest plot of the meta-analysis of the effects of frequency on recovery of motor function.
Stimulation Intensity
When analyzing all included studies at stimulation intensities below 90% RMT, the pooled results were non-significant (SMD = 0.18, 95% CI: −0.23–0.60, P = 0.38). At 90–100% RMT intensities, the results were also non-significant (SMD = 0.14, 95% CI: −0.47–0.75, P = 0.65). Above 100% RMT, the analysis indicated significant effects with a large effect size (SMD = 0.83, 95% CI: 0.3–1.35, P = 0.002). Sensitivity analysis excluding two studies (Liang et al., 2021; Sun et al., 2019) below 90% RMT showed a non-significant outcome (SMD = −0.15, 95% CI: −0.52–0.22, P = 0.42), and differences between subgroups became statistically significant (I2 = 77.9%, P = 0.01). (Figure 5)
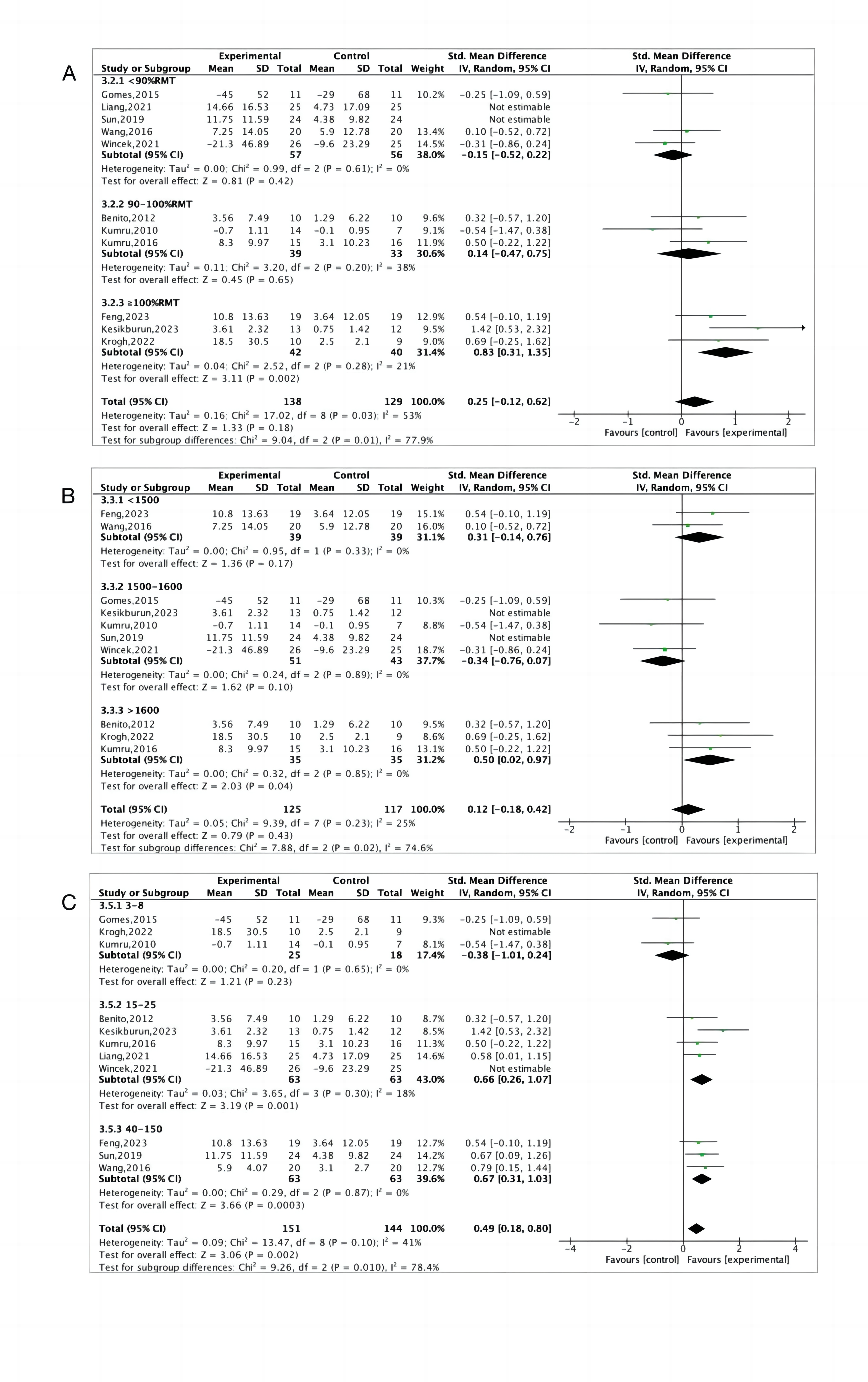
Meta-analysis results for intensity (A), number of sessions (B) and number of pulses (C).
Stimulation Sessions
Upon analyzing all included studies, those with 3–8 sessions showed a non-significant effect (SMD = −0.38, 95% CI: −1.01–0.24, P = 0.23). For 15–25 sessions, the results were significant with a medium effect size (SMD = 0.66, 95% CI: 0.26–1.07, P = 0.001). The 40–150 session group also yielded significant outcomes with a medium effect size (SMD = 0.67, 95% CI: 0.31–1.03, P = 0.0003). Post-exclusion of one study (Wincek et al., 2021), the 15–25 session group's effect size remained stable and significant. Removing two studies (Krogh et al., 2022a; Wincek et al., 2021) revealed a significant subgroup difference (I2 = 78.4%, P = 0.01). (Figure 5)
Pulse Number
Among 10 articles (Benito et al., 2012; Feng et al., 2023; Kesikburun et al., 2023; Krogh et al., 2022b; Kumru et al., 2010, 2016; Liang et al., 2021; Sun et al., 2019; Wang et al., 2016; Wincek et al., 2021) specifying pulse numbers, the meta-analysis for studies with fewer than 1500 pulses showed an SMD that was not significant (SMD = 0.31, 95% CI: −0.14–0.76, P = 0.17). For studies administering 1500–1600 pulses, the analysis yielded a non-significant SMD (SMD = −0.34, 95% CI: −0.76–0.07, P = 0.10). Studies administering over 1600 pulses showed significant results with a medium effect size (SMD = 0.50, 95% CI: 0.02–0.97, P = 0.04). Excluding two studies (Kesikburun et al., 2023; Sun et al., 2019) from the 1500–1600 pulse category revealed significant subgroup differences (I2 = 74.6%, P = 0.02). (Figure 5)
Coil Type
Ten studies (Benito et al., 2012; Feng et al., 2023; Kesikburun et al., 2023; Krogh et al., 2022b; Kumru et al., 2010, 2016; Liang et al., 2021; Sun et al., 2019; Wang et al., 2016; Wincek et al., 2021) specified coil types. Meta-analysis with a figure-of-eight coil showed a medium effect size (SMD = 0.60, 95% CI: 0.25–0.95, P = 0.0008). For the double-cone coil, the analysis resulted in a small effect size (SMD = 0.27, 95% CI: −0.24–0.77, P = 0.30). Sensitivity analyses indicated no significant differences between coil types (P = 0.29). (Figure 6)
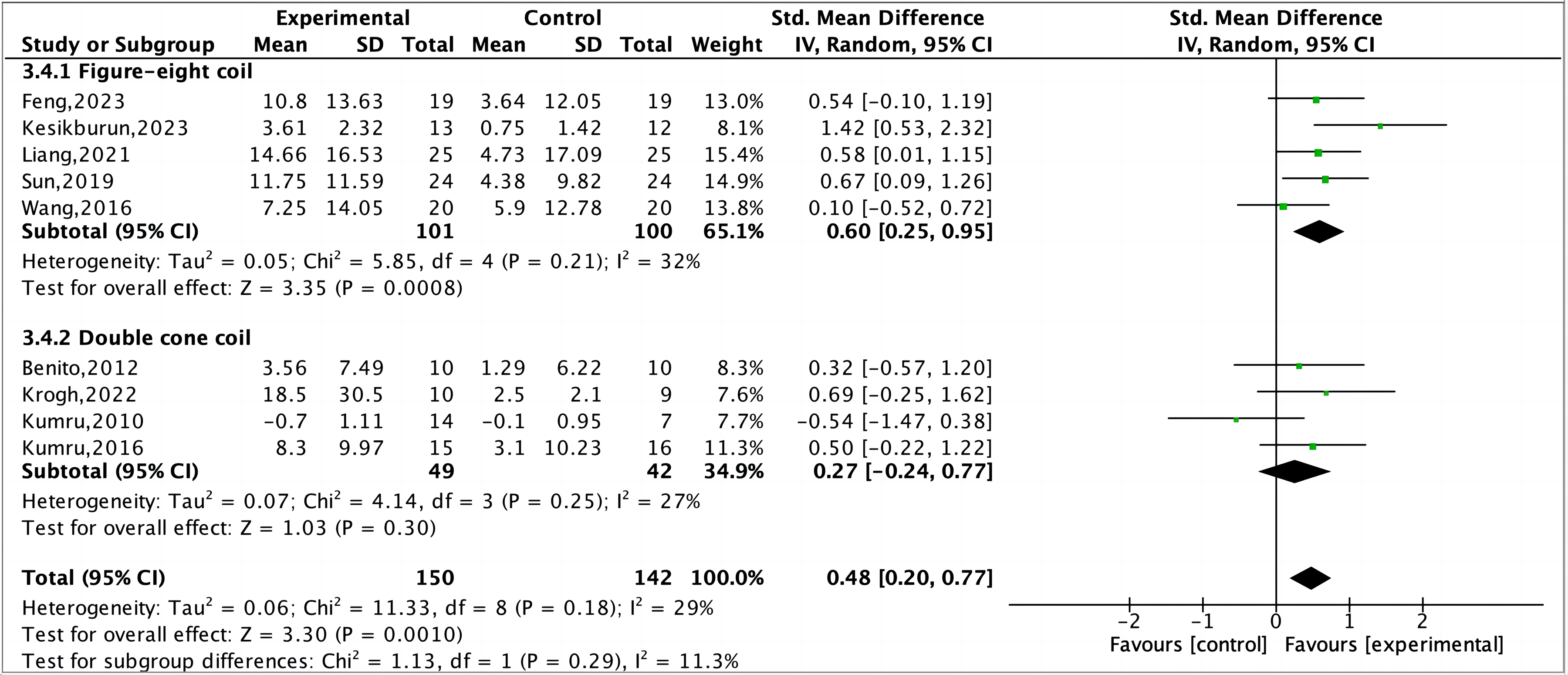
Forest plot of the meta-analysis of the effects of coil type on recovery of motor function.
Publication Bias
Funnel plot analysis was conducted on the included studies using RevMan 5.4 software, with the studies segmented into subgroups based on the number of pulses, the number of stimulation sessions, and stimulation intensity. No obvious asymmetry was observed in any of the funnel plots. (Figure 7)
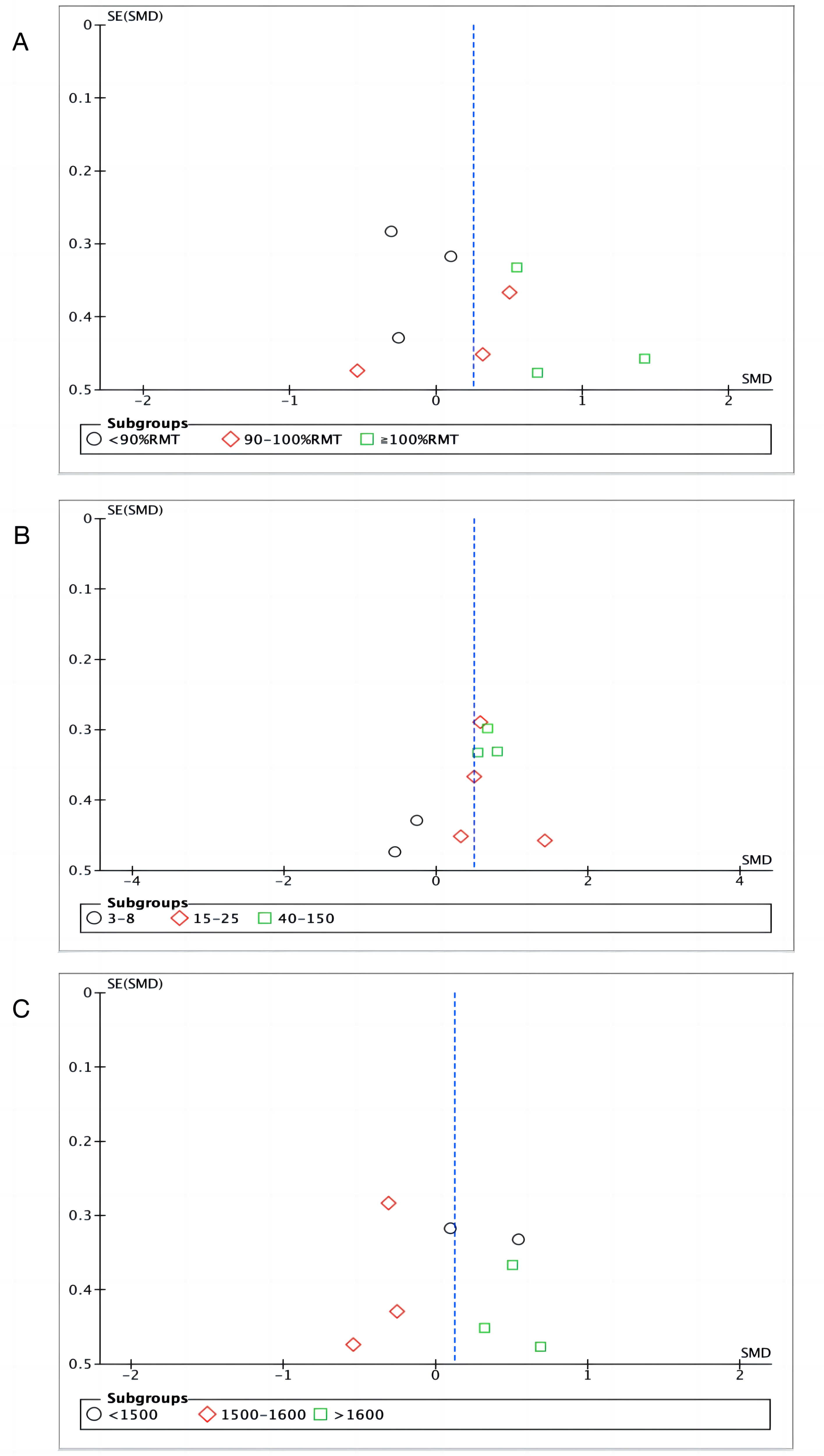
Funnel plot of publication bias. (A) Funnel plot of publication bias for the effect of intensity on motor function; (B) Funnel plot of publication bias for the effect of sessions number on motor function; (C) Funnel plot of publication bias for the effect of pulse number on motor function.
Discussion
After an iSCI, neurons within the spinal cord may undergo structural damage or necrosis, leading to varying degrees of motor function impairment, which significantly affects the quality of life of patients (Chen et al., 2023). Previous meta-analyses suggested that rTMS possesses some clinical efficacy in treating motor function impairments caused by iSCI (Gao et al., 2018), although the total of investigations encompassed was limited. This meta-analysis provides further evidence that rTMS may enhance motor function in patients with iSCI, thereby linking outcomes to particular stimulation settings. Specifically, favorable results are associated with 100–110% RMT intensities, 15 or more sessions, and a pulse count of 1800, suggesting these parameters may play an important role in motor recovery after iSCI.
SCI is accompanied by cell death, inflammation, hypoxia, and neural circuit changes, leading to corticospinal excitability (CSE) dysregulation (Ahuja et al., 2017). Some of the articles included in this study (Sun et al., 2019; Wang et al., 2016; Wincek et al., 2021) demonstrated that rTMS improves CSE in patients with iSCI; however, although one of the studies (Gomes-Osman & Field-Fote, 2015) found rTMS improved motor function in iSCI patients, it did not significantly enhance CSE. The precise modes of operation for rTMS remain incompletely comprehended and require further research. Most researchers believe that the observed effects are attributable to mechanisms of neuronal plasticity, specifically LTP and LTD (Hallett, 2007; Hoogendam et al., 2010; Klomjai et al., 2015). Studies have also demonstrated that rTMS can diminish intracortical inhibition (Hiscock et al., 2008); notably, in patients with iSCI who exhibit improved motor function, a decrease in cortical inhibition has been observed (Nardone et al., 2015). Therapeutic outcomes from rTMS may also stem from enhanced neural stem/progenitor cells (NSPCs) growth, increased brain-derived neurotrophic factor, neuronal excitability, and cerebral blood flow modulation (Lee et al., 2015). These mechanisms potentially elucidate improvements in motor function impairments seen in patients with iSCI following rTMS treatment.
The stimulation frequency is widely acknowledged as the principal element affecting rTMS's impact on cortical arousal (Pell et al., 2011). It is commonly held that stimulations at low frequencies (LF, < 1 Hz) exert a dampening effect on CSE, while stimulations at high frequencies (HF, > 5 Hz) induce an excitatory effect (Simonetta-Moreau, 2014). This could account for the predominantly beneficial outcomes observed within the investigations included this comprehensive review. The HF stimulation's excitatory effects might boost cortical stimuli transmission, thus improving corticospinal interactions and potentially facilitating neuronal reorganization and new synaptic formation at the SCI site (Gunduz et al., 2017). Ruimeng et al. discovered that HF rTMS notably enhanced lower extremity motor capabilities among individuals diagnosed with iSCI (Duan et al., 2021), aligning with the findings of numerous studies cited in this paper (Benito et al., 2012; Krogh et al., 2022a; Kesikburun et al., 2023; Wincek et al., 2021). Thomson et al. noted that LF could result in a decrease in cerebral cortical blood oxygen saturation (HbO) (Thomson et al., 2012). LF rTMS is linked to diminished neural activity (Fitzgerald et al., 2006), and this reduction in neural activity could lead to a decreased demand for oxygenated blood, consequently leading to a reduction in HbO. In this meta-analysis, rTMS at 9–25 Hz was found to enhance CSE and clinical outcomes in patients with iSCI. However, combined data analysis showed no significant difference in outcomes between the high (9–10 Hz) and very high (15–25 Hz) frequency rTMS, even after sensitivity analysis. The effect of increased rTMS frequency on therapeutic outcomes is still unclear.
The efficacy of rTMS is influenced by stimulus intensity (Lang et al., 2006). The accepted safe range for rTMS intensity is 90–130% of the MT (Rossi et al., 2009, 2021). In this study, the included studies administered rTMS at intensities from 70% to 110% of the RMT. A recent meta-analysis showed that RMT and active motor threshold (AMT), the lowest intensities eliciting motor evoked potentials in resting and active muscles, respectively, do not significantly influence treatment effectiveness when used as intensity benchmarks (Xiang et al., 2019). This meta-analysis suggests, particularly after the exclusion of two studies (Liang et al., 2021; Sun et al., 2019), that rTMS at 100–110% RMT could be associated with improved outcomes, aligning with findings from earlier research (Kim & Lee, 2020). Heterogeneity in results may stem from varied outcome measures and measurement techniques. Caution is warranted given the limited number of studies and possible variability from diverse measurement methods. Several studies have suggested that higher-intensity rTMS may bolster the activation of longitudinal spinal neurons and spread stimuli over a larger cortical area, thus accelerating the corticospinal-motor neuronal linkage's spatiotemporal summation effect (Rossini et al., 2015). Additionally, increased rTMS intensity correlates with deeper stimulation, as the induced electric field reaches further into the brain, engaging more extensive neural networks (Lang et al., 2006; Lefaucheur, 2019). The deep location of the functional representation area of the lower limb muscles within the brain's interhemispheric fissure (Groppa et al., 2012) may also contribute to the observed efficacy of rTMS at 100–110% RMT for treating motor dysfunction in patients with iSCI.
Pulse quantity is crucial for determining rTMS's post-effects (Brihmat et al., 2022). rTMS may have enduring effects on the brain and could alter neural plasticity (Klomjai et al., 2015). The underlying processes responsible for the post-effects of rTMS are similar to the mechanisms of LTP and LTD seen in animal studies (Hoogendam et al., 2010; Klomjai et al., 2015; Suppa et al., 2016). Research has shown that repetitive presynaptic stimulation of incoming fibers can lead to LTP or LTD in synaptic activity (Simonetta-Moreau, 2014; Yu et al., 2024). Moreover, the post-effects of rTMS are additionally affected by the duration of the stimulation and the stimulation frequency (Klomjai et al., 2015; Pell et al., 2011).
More pulses typically mean longer stimulation. Research suggests that rTMS can restore the damaged central nervous system and promote growth in NSPCs, with peak cell viability at 1500 pulses; however, NSPCs apoptosis rates surge when the pulse count hits 3000 (Zhao et al., 2020). Yu et al. reported that more pulses do not always result in better outcomes, noting a peak effect at a certain threshold (Yu et al., 2024). A review showed that 70% of studies used > 1600 pulses, mostly with positive outcomes (Brihmat et al., 2022), consistent with this study's findings. The results of the meta-analysis, after excluding two studies (Kesikburun et al., 2023; Sun et al., 2019), revealed that the effects of rTMS might be more pronounced with 1800 pulses. Sun et al. (2019) and Kesikburun et al. (2023) used SCIMIII and LEMS to measure outcomes, where increases in scores indicate functional improvement. Conversely, other measures in these studies suggested improvement with score decreases, potentially contributing to heterogeneity.
The type of coil dictates the stimulation area (Lefaucheur, 2019), and enhancing the specificity and depth of TMS can render its effects more adaptable and selective (Gomez et al., 2018). Optimizing stimulation involves balancing depth, focus, and energy, making the selection of the right coil type critical. Transcranial magnetic coils can be either single (circular) or dual (figure-8, double cone) (Lefaucheur, 2019). The initial TMS systems used circular coils for their ease of manufacture (Barker et al., 1985), generating broad electric fields. This maximally stimulates the area of the brain beneath the coil's perimeter but lacks the precision to target specific cortical areas accurately (Deng et al., 2013). The figure-8 coil, which allows for deeper penetration, has been used to target the interhemispheric fissure's deep areas, activating lower limb function and pelvic muscles (Gomez et al., 2018; Klomjai et al., 2015). The double-cone coil penetrates deeper but is less focused than the figure-8 coil (Deng et al., 2013; Gomez et al., 2018). However, some studies indicate the double-cone coil's broader reach may be beneficial in patients with SCI. The subgroup analysis in this meta-analysis demonstrated no statistically significant variance between the groups using the double-cone and figure-8 coils. This may be related to the excitation locus and the positioning of the coil alignment (Klomjai et al., 2015). Designing the coil to better balance stimulation depth, focus, and energy for optimal effects is a key issue that researchers are currently addressing.
Session count is a key determinant of rTMS efficacy; clinicians require objective evidence for session selection. Studies have also indicated that prolonged rTMS treatment may improve motor skills by increasing cortical excitability through sustained neural activity (Rajak et al., 2019). However, an increase in the number of sessions does not automatically translate to improved therapeutic outcomes. Recent studies have also indicated that there are no significant motor function differences between 20 and 30 sessions after 6 weeks of therapy (Lv et al., 2023). With prolonged treatment, a bidirectional equilibrium may emerge, potentially decreasing the opposite hemisphere's motor cortex responsiveness and the facilitatory impact of rTMS (Tang et al., 2022). After excluding two studies (Krogh et al., 2022a; Wincek et al., 2021), it was observed that treatment regimens involving more than 15 sessions of stimulation yielded better therapeutic effects. Although there is a trend towards improved outcomes as the number of stimulation sessions increases beyond 40, the upper limit for the optimal number of sessions is yet to be determined. Krogh et al. (2022a) and Wincek et al. (2021) selected the 10 MWT and sEMG, respectively, as indicators to evaluate improvements in motor function, which differ from the findings of most of the studies that indicated the use of the LEMS as the evaluation result. The primary source of heterogeneity may stem from the differing content and methods of measurement used in these outcome indicators.
Nevertheless, this study has some limitations: (1) A small number of original articles were included, with low-quality and erroneous data studies excluded, ultimately resulting in only 11 studies being incorporated; (2) Due to insufficient data, intervention parameters were analyzed only for number of pulses, frequency, intensity, coil type, and number of stimulation sessions; (3) Some intervention parameters involved a small number of samples, which may reduce the reliability of the evidence; (4) Due to the limitations of the included studies, we were unable to perform stratified or subgroup analyses on factors that might influence the magnitude of treatment effects, such as assessment scales, disease duration, investigated limb, and SCI segments; (5) Although this study aimed to identify optimal rTMS parameters, variations in equipment may lead to a lack of standardization in device-specific settings, potentially influencing the evaluation of therapeutic effects; (6) Reporting of adverse events was inconsistent across the included studies, with some omitting this information entirely.
Collectively, the outcomes of this meta-analysis provide further supporting evidence for the potential clinical efficacy of rTMS in treating motor functional impairments caused by iSCI, and to the best of our understanding, this is the first study to systematically analyze the optimal parameters for rTMS treatment of motor functional impairments in iSCI. The analysis revealed that rTMS treatment of motor functional impairments in patients with iSCI is significant when the stimulation intensity is between 100–110% RMT, the number of stimulation sessions was also more than 15, and the number of pulses was 1800. This suggests that under specific stimulation intensities, number of stimulation sessions, and pulse counts, rTMS may maximize the promotion of neural plasticity, thereby aiding in the recovery of motor functions. This finding provides a basis for clinicians in the selection of intervention parameters when applying rTMS treatment for iSCI, helping to optimize treatment effects, reduce treatment duration, and potentially lower treatment costs. Despite the robust evidence, the conclusion was tempered by limitations, including small sample sizes, varied study designs, and inconsistent stimulation parameters. Future studies should address these issues through larger, well designed RCTs and refined rTMS treatment parameters, while also emphasizing rigorous monitoring of adverse effects to further enhance the safety profile of rTMS in iSCI treatment.
Supplemental Material
sj-docx-1-nre-10.1177_10538135251325435 - Supplemental material for Optimal Parameter Analysis of Repetitive Transcranial Magnetic Stimulation on Motor Function in Patients with Incomplete Spinal Cord Injury: A Meta-Analysis
Supplemental material, sj-docx-1-nre-10.1177_10538135251325435 for Optimal Parameter Analysis of Repetitive Transcranial Magnetic Stimulation on Motor Function in Patients with Incomplete Spinal Cord Injury: A Meta-Analysis by Yu Liang, Liyun Xue, Saoying Yang, Chen Wang and Xifang Liu in NeuroRehabilitation
Footnotes
Acknowledgments
The authors have no acknowledgments.
Contribution
Yu Liang: methodology, validation, formal analysis, investigation, data curation, writing-original draft, writing-reviewing and editing, project administration. Liyun Xue and Saoying Yang: methodology, investigation, writing-reviewing and editing. Chen Wang: conceptualization, methodology and validation. Xifang Liu: conceptualization, methodology, validation, investigation, writing-reviewing and editing.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.