
Abstract
Background
Long COVID patients report various cognitive and affective symptoms that are poorly understood.
Objective
This study analyzed cognitive and affective performance in 208 Long COVID patients pre and post psychoeducational rehabilitation using a standardized screening test of higher cerebral functions. Identifying persistent difficulties may help guide future rehabilitation efforts.
Methods
The sample was comprised by a subset of 208 who completed psychoeducational rehabilitation from 614 Long COVID patients seeking rehabilitation. Performance on specific items was analyzed and compared to a reference sample of 114 educationally matched normal functioning adults.
Results
Detailed item analyses in 208 patients revealed persistent difficulties in the efficiency of learning and memory, affective expression, and the ability to accurately predict verbal memory performance compared to a reference sample. Long COVID patients showed variable performance deficits on attention, visual-spatial problem solving and memory measures. Language and related functions were consistently at a level commensurate with normally functioning individuals.
Conclusions
Persistent cognitive and affective impairments were identified in Long COVID patients post-rehabilitation. Future programs should aim on to improve the efficiency of learning and memory, enhance the range of affective expression, and improve self-awareness of functional capacities. Rehabilitation should consider the multifactorial causes of these neuropsychological symptoms.
Keywords
Introduction
Long-COVID is defined as a clinical condition in which patients with a history of probable or confirmed SARS-CoV-2 infection report symptoms that develop at the time of the initial infection or up to three months later, which persist for at least two months and cannot be explained by alternative diagnostics. The symptoms may develop after the initial recovery from acute SARS-CoV-2 infection or be due to persistence of the original illness. They may fluctuate or even reappear over time, and generally impact day-to-day functioning (Soriano et al., 2022; World Health Organization, 2021).
A meta-analysis by Premraj et al. (2022) reported that fatigue, cognitive dysfunction (brain fog, memory issues, attention disorder) and sleep disturbances appeared to be key features of post-COVID-19 syndrome. Sleep disturbances, anxiety, and depression were common and increased significantly in prevalence over time. There is a growing body of literature on the cognitive and neuropsychiatric implications of the post-acute stage of SARS-CoV-2 (Ferrucci et al., 2022; Velichkovsky et al., 2023; Zeng et al., 2023), and COVID's impact on patients’ work functions and quality of life (Miskowiak et al. 2022; Siegelman, 2020). The literature, however, is still unclear as to nature of the varied cognitive and affective symptoms reported by these patients (Meagher, 2023). Clearly a biopsychosocial approach to understanding the complex symptoms reported by Long COVID patients is necessary (Klinkhammer et al., 2024; Thurner & Stengel, 2023).
The rehabilitation literature on Long COVID patients often applies traditional interventions when treating physical symptoms such as fatigue, dyspnea, and musculoskeletal impairments (Chuang et al., 2024; Fugazzaro et al., 2022), but interventions for cognitive impairments are much less understood (De Luca et al., 2022; Mathern et al., 2022; Sacks-Zimmerman et al., 2023).
We previously reported that in a large sample (N = 614) of long COVID patients, their total BNI Screen for Higher Cerebral Functions (BNIS) score was significantly below average compared to a reference group (i.e., a mean of −1.25 Z score). It was also noted that as a group, they performed below average on composite or aggregate subtests scores sampling memory and affect expression/perception (Braga et al., 2022). We further noted there was no relationship found between severity of COVID-19 symptoms and the patients' neuropsychological test performance. The same was true for their self-reported emotional state. That is, their self-reported levels of anxiety and depression were not related to severity of neuropsychological test performance (Braga et al., 2022).
We also subsequently reported that in a subsample of the original 614 long COVID patients (N = 208) who underwent a psychoeducational rehabilitation program, 54% showed improvement in the BNIS total z-score cut-off value (z score < −1), while 33% did not improve and remained below average in their overall level of performance (Braga et al., 2023). Patients who subjectively reported a deduction in their cognitive symptoms showed clear improvement in their neuropsychological test performance with a moderate size effect (Cohen's d = 0.43).This was not observed in patients who reported no symptom reduction. Interestingly, improvement was related to the educational level of the patient (patients with higher education did better) and the level of self-reported depression (i.e., lower depression was associated with normal levels of performance). These findings suggest that multiple factors may contribute to the resolution of cognitive and affective symptoms reported by Long COVID patients.
It is important therefore to have a more in-depth understanding of the frequent performance failures on specific neuropsychological test items in Long COVID patients to help guide future psychoeducational programs.
We therefore conducted an item-by-item analysis on Long COVID patients' performance on the BNIS before and after undergoing psychoeducational rehabilitation. We identified the percentage (i.e., relative frequency) of performance failures before and after treatment to help clarify which neuropsychological features of their performance were most resistant to change given our initial rehabilitation efforts. We are aware that from a statistical point of view the reliability of a finding is influenced by the number of items used to measure a certain construct or behavioral domain (Guilford, 1956). However, clinicians must be vigilant of specific behavioral limitations that repeatedly occur and are resistant to change when developing a rehabilitation program (Prigatano, 1986). It is for this reason that we undertook this approach to data analysis.
We also conducted an individual case analysis of overall consistency levels of neuropsychological performance because this patient group also does not exhibit a consistent pattern of progressive improvement with time.
Methods
Participants
Six hundred and fourteen (614) patients with a diagnosis of SARS-Cov-2 infection, confirmed by positive Polymerase Chain Reaction (PCR) test that detects viral RNA, were initially referred to the long COVID program at the SARAH Network of Rehabilitation Hospitals (Federal District, Brazil) from April 2021 to January 2022 for treatment of cognitive and affective complaints (Braga et al., 2022). Two hundred and eight (208) of these patients were reevaluated 17 months after participating in the rehabilitation program, from August 2022 to June 2023, as previously reported (Braga et al., 2023). This current study focuses primarily on the later subgroup of patients.
Both studies were approved by the SARAH Network Ethics in Research Committee (CAAE 53956921.2.0000.0022). Written informed consent was obtained from all participants.
Materials
An interview protocol helped identify the cognitive and affective complaints reported by the patients and gather socio-demographic, academic/professional, psychological and daily-life information. The Portuguese translation of BNIS was then administered to these individuals to assess their neuropsychological test performance (Braga et al., 2022; Braga et al., 2023). The Portuguese translation and standardization study of the BNIS was completed 4 years prior to the outbreak of the COVID-19 epidemic.
The BNIS (Prigatano et al., 1995; Prigatano et al., 2018) broadly and reliably assesses disorders of higher integrative mental functions. The BNIS was specifically developed to evaluate patients with known or suspected brain disorders and to briefly but reliably evaluate both their cognitive and affective status. It comprises 50 items for evaluation of six functions (or subscales): speech/language, attention/concentration, orientation, visuospatial problem solving and memory. In addition, it asks the patients to generate affect in their tone of voice when reading a sentence and to correctly identify three facial affects. It presents the patients with a humorous, or at least incongruent, stimulus to determine if the examiner can provoke a smile or laughter in the patients. Finally, it asks the patients to predict how many of three words they can recall after a 5–10-min distraction. This single item is intended to assess the patients’ awareness of any limitations in their memory capacity. In addition to providing subtest scores in each of these domains, an overall level of performance score is calculated. In normally functioning individuals, the test typically takes between 12–15 min to complete (Prigatano et al., 2013).
Procedure
The patients were evaluated and reevaluated in person by the same experienced, licensed neuropsychologists. The amount of time between the two evaluations ranged from eight to 25 months (M = 16.7, SD = 3.5).
Summary of the Rehabilitation Program
The SARAH Network's psychoeducational rehabilitation program lasts four consecutive weeks, with weekly two-hours group meetings that can be attended virtually or in-person, depending on the patient's availability. A maximum of 12 participants is allowed for each group. The rehabilitation program has a psychoeducational focus on cognition and emotion, providing information on cognitive functions and strategies to compensate for and manage neuropsychological deficits. Patients learn to be more proactive in problem solving and in regaining control of their lives, while also receiving emotional support in safe spaces designed for empathy and connection (Rogers, 1995; Rogers, 2012). Each meeting has a specific theme: (i) Long COVID and cognition; (ii) Executive functions; (iii) Attention and memory; and (iv) “This is how the mind works, let's use it to our advantage”. Also presented are strategies for dealing with anxiety, including information about the benefits of daily relaxation, meditation, and mindfulness practices. The sessions involve presentations, discussions, and practical strategies for coping with the cognitive and emotional consequences of Long COVID. Participants receive an illustrated guide with instructions on cognitive rehabilitation, including compensatory strategies to improve functioning at work, school, home, and in the community (for more details see Braga et al., 2023).
Statistical Analysis
We ran descriptive statistical analyses for the age ranges, gender and educational levels of subjects in the original larger sample of 614 Long COVID patients, as well as the subsample of those who underwent the psychoeducational rehabilitation program. We calculated the distribution of the BNIS Total Scores for both the larger sample and the subsample of rehabilitation participants.
For the subsample of 208 patients, we calculated the percentage (%) of subjects who passed each BNIS test item (i.e., a score of 1, 2, 3 or 4 depending on the item) at the time of admission and then again upon discharge from the psychoeducational rehabilitation program. The percentage of the Long COVID patients who successfully passed a given test item was compared to the percentage of individuals with a similar educational level who passed the same test item in the standardization study. Educational level was previously shown to correlate highly with test performance in the Brazilian normative group (Prigatano et al., 2018). Next, we identified the items that revealed at least a 10-percentage point improvement from pre to post treatment. A 10-percentage point difference was arbitrarily set as potentially identifying a clinically relevant change in the exploratory investigation. We then compared the percentage of those who successfully completed a specific test item in the Long COVID subsample of 208 patients with the reference sample of 114 normal functioning individuals, matched by age and education level.
Total BNIS (raw) Score for each individual was classified as “Average” or “Normal” (Z score between −1 and +1); Mildly Impaired (mean score was equal to a Z score of < −1, but equal to or less than a Z score of −1.5); Moderate to Severe Impairment (mean Z score greater than −1.5 from the average mean performance given the person's age and educational level). The number of people classified in these three groups before and after rehabilitation was calculated.
Statistical inference analyses included Spearman's correlation coefficient, Chi-square test for independence, and McNemar's chi-squared test for related samples. Additionally, Cramer's V was used as a measure of effect size for the Chi-square test.
All analyses were performed with R version 4.4.1.
Results
How Representative was the Subsample of Rehabilitation Long COVID Patients to the Initial Larger Assessment Sample?
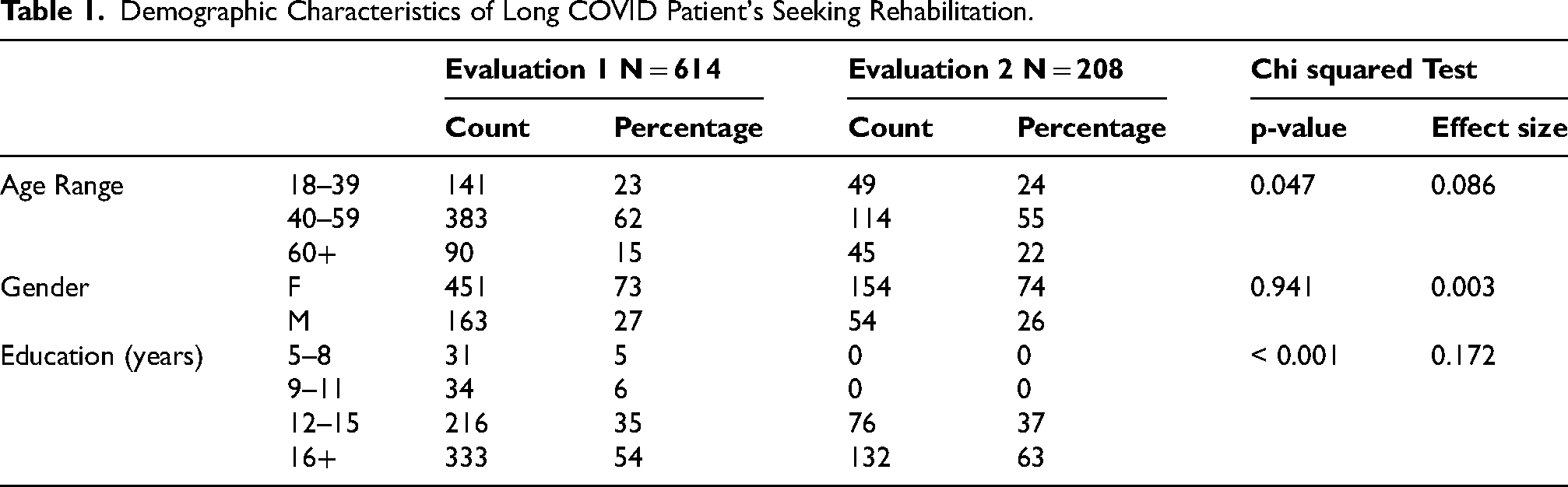
Table 1 compares the demographic features of the entire sample of 614 Long COVID patients to the subsample of the 208 patients who received the rehabilitation. There were no differences in terms of gender, but the psychoeducational rehabilitation program participants tended to be slightly older with 12 years of education or higher. The effect sizes were 0.09 and 0.17, respectively.
Demographic Characteristics of Long COVID Patient's Seeking Rehabilitation.
The level of neuropsychological test performance, as indicated by the Total (raw) BNIS score, showed a similar distribution compared to the larger sample of 614 patients and the subsample of 208 patients (Figure 1). The psychoeducational rehabilitation subsample of patients appears representative of the larger initial assessment sample. In both samples, there is a very large range of levels of performance. Scores range from severely impaired to above average levels of functioning.
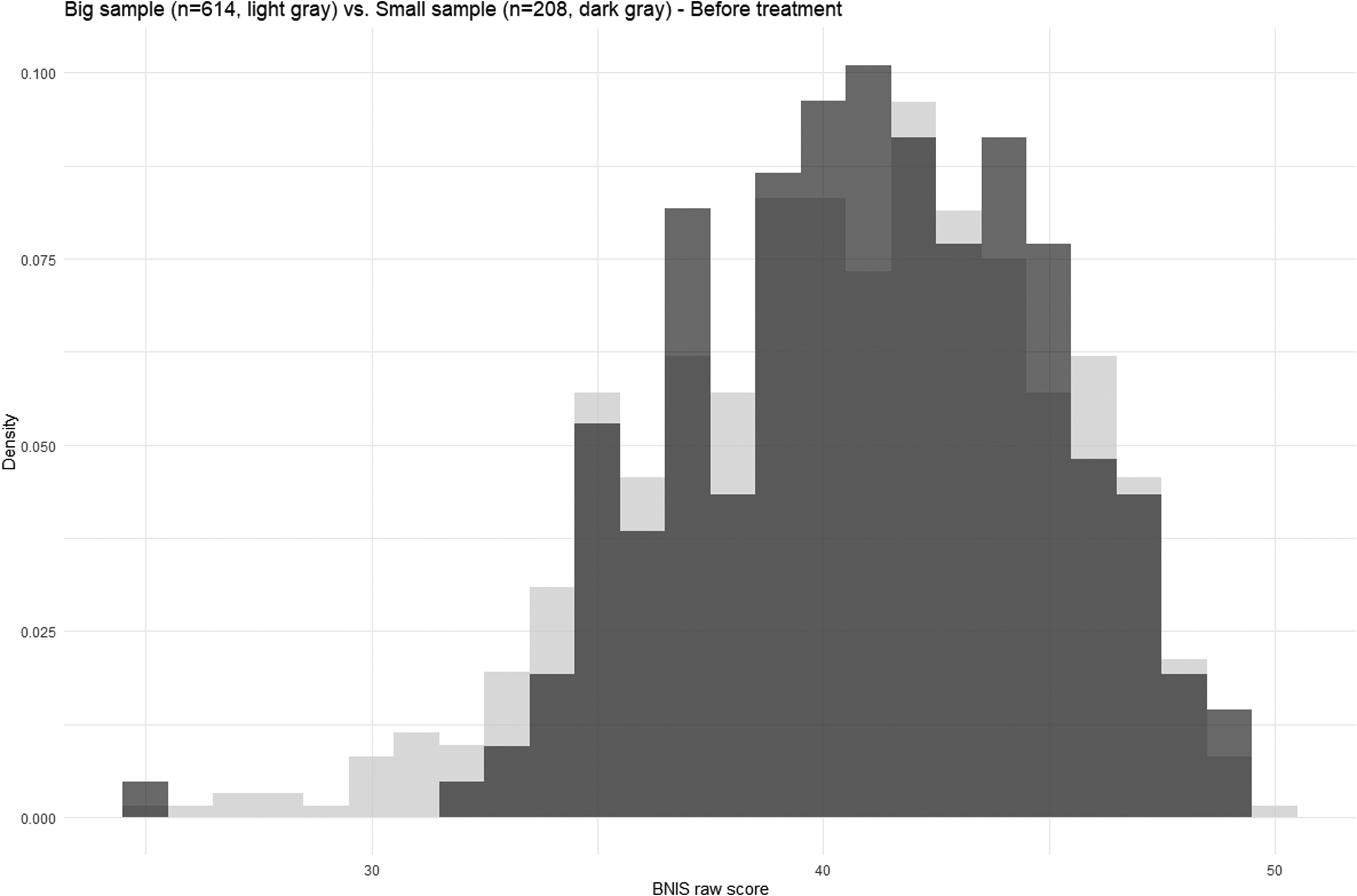
BNIS (total raw scores) histograms of the full sample (n = 614) and the smaller sample undergoing psychoeducational rehabilitation (n = 208).
Item-by-Item Analysis of Neuropsychological Test Performance Pre and Post Psychoeducational Rehabilitation
Table 2 provides an item-by-item analysis of test performance on the BNIS pre and post psychoeducational rehabilitation interventions for the 208 Long COVID patients. For purposes of comparison, the percentage of normally functioning and educationally matched individuals who successfully completed the various test items is also listed. These 114 individuals were a part of the standardization study using a Portuguese translation of the BNIS in a Brazilian study.
Item-by-Item Analysis of Performance on the BNI Screen for Higher Cerebral Functioning In Long COVID Patients (n = 208) Pre- and Post-Psychoeducational Rehabilitation compared with Normally Functioning Age and Education Matched Adults Reference Sample (n = 114
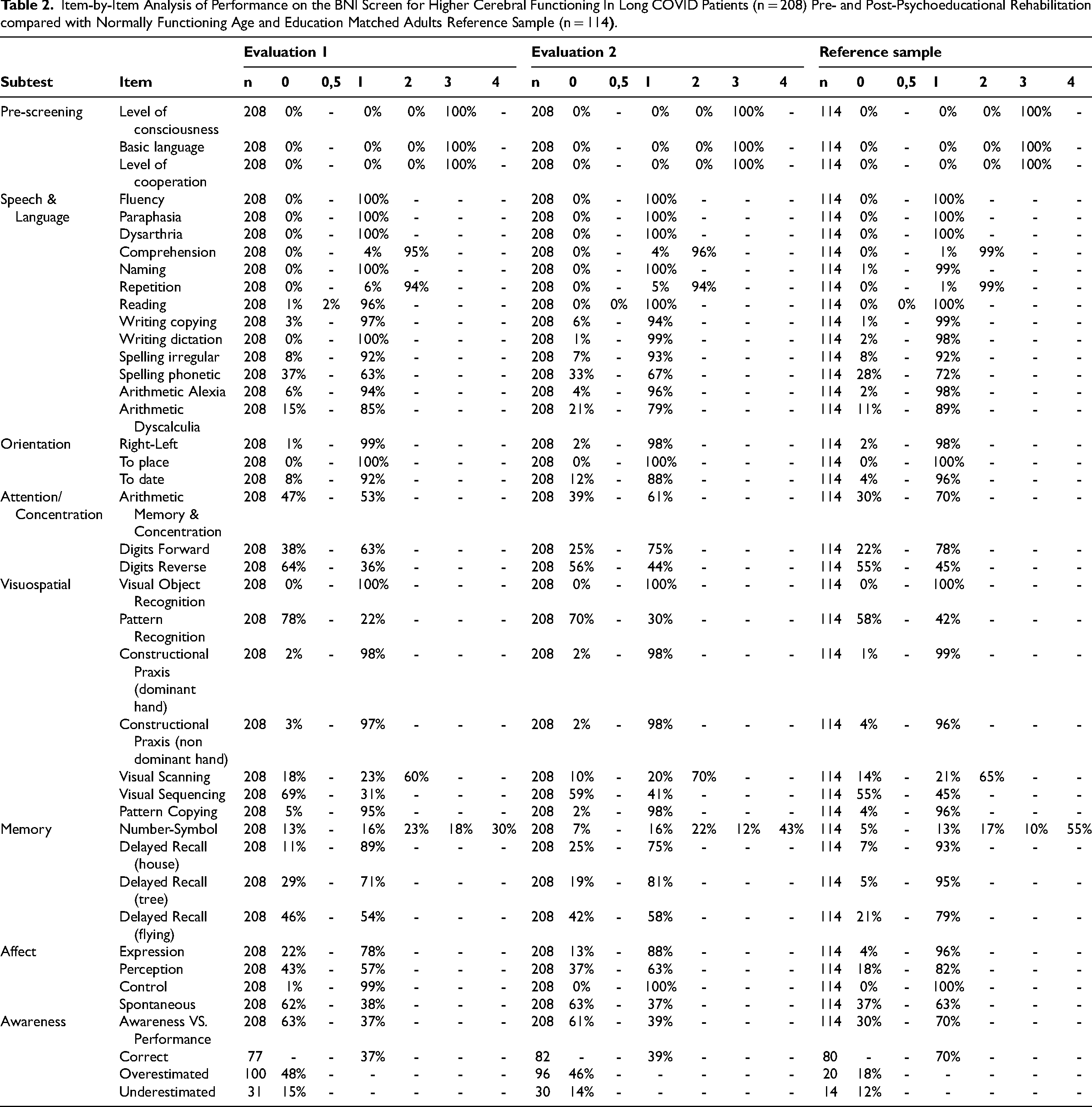
The Long COVID patients performed the language tasks without difficulty both pre and post rehabilitation. The percentage of individuals passing each of the items is nearly identical to what was observed in normally functioning individuals (Table 2). There was no item in which there was a 10-percentage point increase in the number of individuals who improved their level of performance on these items.
The vast majority of Long COVID patients exhibited no difficulties successfully performing items dealing with time and space orientation. The percentage of individuals successfully performing each item is again comparable to the percentages who passed these items when standardizing this test (Table 2). We found no evidence of changes when we compared pre- and post-rehabilitation performance.
Long COVID patients initially appeared to show relative difficulties performing attention and concentration tasks that involved doing a mental arithmetic task (53%) and repeating 5 digits in the forward direction (63%) prior to the rehabilitation program. The percentage of those passing these items, however, was similar to what was observed in the standardization study of the BNIS in Brazil (Table 2). Post rehabilitation there was an increase of 12 percentage points in the number of people who successfully completed the task of repeating 5 digits in the forward direction (improvement from 63% to 75%).
Long COVID patients had difficulty performing some, but not all, visuospatial tasks. When first asked to solve a visual scanning task, 60% were able to complete it before treatment and 70% after treatment. The percentage of individuals with 12 years of education in the normative sample who passed this test was 65%.
However, on a more demanding pattern recognition task, only 22% initially passed this item and 30% passed it post-rehabilitation. In the normative sample, 42% of individuals with 12 years of education successfully passed this item (Table 2).
Long COVID patients initially had difficulty remembering a series of number symbol associations. Prior to rehabilitation, only 30% of the patients could recall all four of the associations presented to them. At the end of rehabilitation, 43% of the participants attained this perfect score. In the standardization study, 55% of participants with at least 12 years of education achieved a perfect score of 4 out 4 items correct.
We did not find a consistent pattern of positive change following psychoeducational rehabilitation in the item involving delayed recall of three words. There was a 10-percentage point improvement on only one of the three words participants were asked to recall. On another word (of the original 3) there was a 14-percentage point decline. It is interesting to note that the most difficult of the three words to recall (i.e., flying) was only successfully recalled in 54% of Long COVID patients before rehabilitation and 58% post rehabilitation. In the standardization study, 79% of those with at least 12 years of education were able to recall that word after a delay (Table 2). Inefficiencies in learning and memory were frequent in Long COVID patients.
Long COVID patients had relative difficulty with the perception and expression of affect, but only verbal expression of affect showed a 10 percentage-points difference post treatment. Prior to the psychoeducational rehabilitation, 78% of the participants could generate a tone of happiness and anger when reading a sentence. Post treatment the percentage increases to 88%. In the standardization study, 96% of individuals with 12 years or more education could successfully perform this task (Table 2). Eight-two (82%) of normal functioning individuals successfully perceived facial affect in the standardization sample. By the end of treatment, only 63% of Long COVID patients could successfully complete this task item (Table 2).
In addition, prior to the rehabilitation, only 38% of Long COVID patients passed the spontaneous affect item and this did not change post rehabilitation (i.e., 37%). However, 63% of the healthy controls in the standardization sample who had 12 years or more of education passed this item.
Finally, there was no pre- versus post-change on the Awareness/Perception item in which the individual is asked to predict the number of words they can recall after a delay. Less than 40% of Long COVID patients were able to make an accurate prediction (Table 2). In contrast, 70% of individuals with at least 12 years of education could accurately predict their performance level in the initial standardization study (Prigatano et al., 2018).
In summary, specific item analyses revealed that Long COVID patients showed variable difficulties with attention/concentration, visual attention/visual problem solving, and memory. They consistently had a lower performance on items dealing with expression and perception of affect. As a group, they had substantial difficulties accurately predicting how many of three words they could recall after a distraction. They were less efficient in learning and memory.
The increased group performance on many of these items resulted in a positive shift in the BNIS Total (raw) scores pre to post rehabilitation (Figure 2). There was a strong positive correlation between the level of initial performance on the BNIS total score and the post rehabilitation scores (rho = + 0.69, p < 0.001).
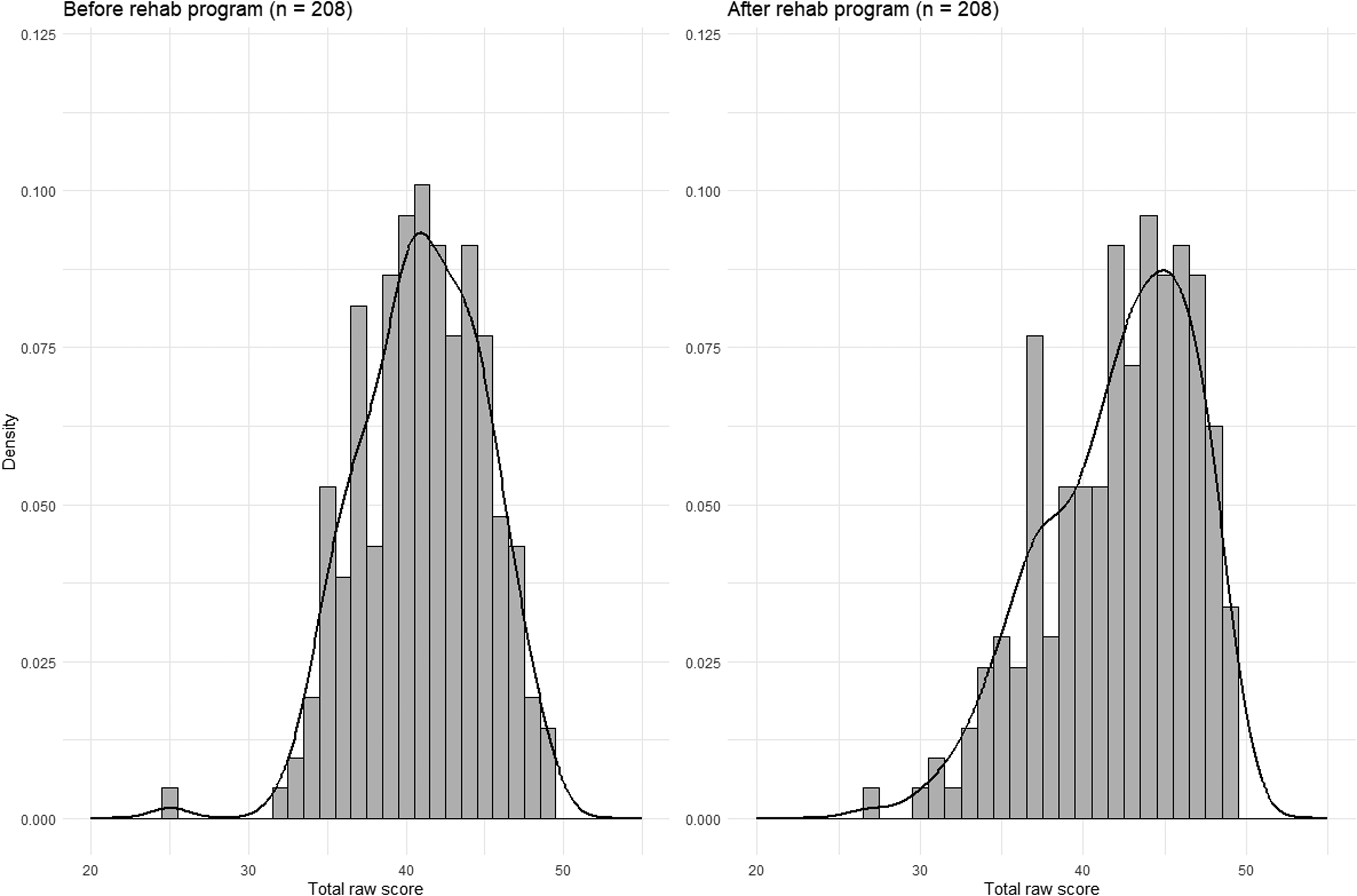
BNIS (total raw scores) histograms before and after psychoeducational rehabilitation (n = 208).
Individual Case Analysis of Performance Levels on the BNIS Pre and Post Psychoeducational Rehabilitation
We classified the patients' performance level on the BNIS at both time periods as falling within the “average range”, “mildly impaired” and “moderately to severely impaired”. Table 3 illustrates that 87 of the 208 Long COVID patients (41.8%) had average levels of test performance pre and post treatment. Many patients who initially performed in the moderate/severe impairment range had average scores post rehabilitation (i.e., 40 out of 86 or 46.5%) suggesting a clinically positive change for a subsample of Long COVID patients undergoing psychoeducational rehabilitation. Yet a few patients showed a decline in their overall performance. Of the 96 long COVID who initially presented with average levels of performance as reflected by their BNIS total score, 9 or 9.4% performed in the moderate/severe level of performance. There were no unique features of this subgroup. This later finding highlights the potential of the fluctuating neuropsychological status of some patients with Long COVID which remains poorly understood.
Contingency Table and McNemar Test* for BNIS test Performance Levels Pre- and Post- Psychoeducational Rehabilitation.
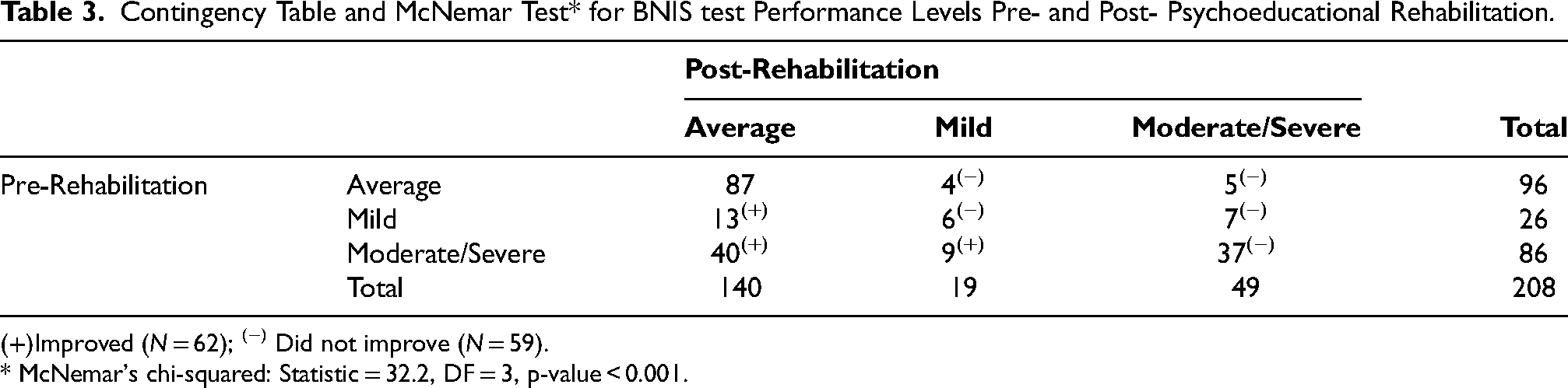
Improved (N = 62); (−) Did not improve (N = 59).
* McNemar's chi-squared: Statistic = 32.2, DF = 3, p-value < 0.001.
Discussion
The primary aim of our study was to provide a more detailed description of the neuropsychological test performance observed in Long COVID patients with cognitive and affective complaints who underwent a psychoeducational rehabilitation program. The focus of the study was to identify the frequency of specific performance successes versus failures in Long COVID patients on the BNIS. The goal of such a descriptive analysis was to help the clinician guide future psychoeducational activities for this group of patients.
After assuring that our subsample of 208 long COVID patients were comparable to the large initial sample of 614 patients, we conducted an item-by-item analysis of both pre and post neuropsychological test performance and compared to a sample of 114 normally functioning Brazilian individuals tested on average 4 years prior to the outbreak of the COVID-19 pandemic.
Performance on specific items of the BNIS revealed that long COVID patients consistently demonstrated variable difficulties performing tasks that involve attention/concentration, visuospatial attention and problem solving, and memory. Their efficiency in learning, however, was compromised. This is perhaps best reflected in the performance on the number/symbol association learning and memory test item. The patient is allowed to study it for up to three minutes and write down anything that might help them remember the associations (but they are told at the time of testing they cannot refer to what they wrote down). Recalling all associations produces a perfect score on this item. Fifty-five (55%) of the normal functioning standardization sample who had 12 years of education or higher achieved this score. In contrast, only 30% of Long COVID patients performed at this level prior to rehabilitation.
A second finding is that Long COVID patients frequently had difficulty verbally expressing affect when asked to say a sentence first in a happy tone and then in an angry tone. Nine-six (96%) percent of the standardization sample that had at least 12 years of education could successfully perform this task in contrast to the 78% of Long COVID patients prior to rehabilitation. Related to this observation was the finding that an item designed to stimulate a smile or laughter produced that response in 63% of the standardization sample who had at least 12 years of education, but in only 38% of Long COVID patients when first presented this task. The percentage passing this item did not change post rehabilitation (i.e., 37%). A disturbance in emotional expression was frequently observed in the Long COVID patients in our sample.
In everyday life, adults must make realistic judgements about their abilities when taking on responsibilities. It is perhaps one marker of effective adult problem solving. It is also striking that Long COVID patients had notable difficulty on the test item that samples their ability to predict their verbal memory performance. Seventy (70%) of normally functioning Brazilian adults with 12 years of education could successfully perform this task. In contrast, only 37% of Long COVID patients could do this before rehabilitation and continued to have notable difficulty doing it after rehabilitation (i.e., 39%). While many factors can contribute to such prediction errors, one possibility is that they have reduced awareness or insight into their actual abilities. This may be one of the most important areas to focus on in future rehabilitation efforts. Having the patients become vigilant (and realistic) about their actual abilities may greatly aid their psychosocial adjustments.
Reductions in the efficiency of new learning, problems making realistic judgments about one's memory capabilities, and difficulties expressing emotions can, of course, be related to many different factors. The findings obtained using the BNIS are, however, compatible with reports in the literature that emphasize subtle yet important impairments in broadly defined “executive functions” (Daroische et al., 2021; Velichkovsky et al., 2023). Alméria et al. (2020) chose a group of subtests to create a neuropsychological battery specific to this population. Lower scores were seen in the memory, attention, verbal fluency, working memory, mental flexibility, and phonetic fluency domains. The present findings also suggest that tests aimed at assessing the person's ability to express and perceive emotions should be included.
Our findings are also compatible with other reports in the literature. Not all long COVID patients perform below average on existing varying neuropsychological tests (Cipolli et al., 2023; Julide et al., 2024; Zeng et al., 2023). It is striking that nearly one half of this sample of Long COVID patients (96 out of 208 patients or 46.2%) had average performance levels when entering a rehabilitation program aimed at improving their self-reported cognitive difficulties. Average levels of performance should not always be interpreted as “normal” levels of performance for individuals who may have functioned above average prior to contracting any illness that may affect the central nervous system. Nevertheless, a fairly large portion of the Long COVID patients in our study did not demonstrate an overall level of neuropsychological performance suggestive of underlying brain dysfunction.
We also observed that in a very small number of individuals (9 out of 96) there is an actual substantial worsening of neuropsychological test performance post rehabilitation. Fluctuating symptoms have been reported in some Long COVID patients (World Health Organization, 2021). Following these individuals over time may provide further insight into the multifactorial nature of neuropsychological characteristics of Long COVID patients.
The underlying biological mechanisms for Long COVID remain unclear. Initially, research focused on understanding the mechanisms of acute infection and on developing effective treatment. A literature review by Serrano-Castro et al., (2020) suggested that SARS-CoV-2 is a neuroinvasive virus, able to trigger an avalanche of cytokines, with lasting effects on specific populations. It was noted that the hippocampus was especially vulnerable to coronavirus infections, thereby increasing the probability of post-infection memory impairment and accelerated degenerative diseases, such as Alzheimer's (Ritchie et al., 2020). Other studies suggest a strong immune response to a SARS-CoV-2 infection and psychological stressors associated with the pandemic that may cause chronic inflammatory processes in the body. It's also been suggested that neuroinflammation and associated nervous system disorders might contribute significantly to the etiopathogenesis of depressive states (Dąbrowska et al., 2021). A review by Sarubbo et al. (2022) concluded that, for now, the mechanisms of arrival in the brain seem to be related to disruptions in the blood-brain barrier (BBB), together with the nervous or axonal transport of the virus through the trigeminal nerve, vagus nerve or brain-gut axis. The study by Greene et al. (2024) suggested that sustained systemic inflammation and persistent localized blood-brain barrier dysfunction are key features of “brain fog” associated with long COVID. Cognitive disorders associated with mild forms of infection may be linked to hypometabolic lesions of the brain, which are likely linked to neuroinflammation (Hugon et al., 2022). These findings further reinforce the need for rehabilitation to expand its interventions to include activities that reduce neuroinflammation. This would include a wide range of potential activities such as behavioral methods for reducing anxiety (i.e., relaxation training) and instituting important dietary changes known to reduce inflammation.
The improvement in BNIS performance after rehabilitation may be related to the psychoeducational program (Braga et al., 2023). The program focused on both cognition and emotion, providing information on cognitive functions and strategies to compensate for and manage neuropsychological deficits. The use of metacognitive and compensatory strategies has proven effective in cognitive rehabilitation by promoting self-regulation, self-awareness, and patient adaptation to challenging contexts (Cicerone et al., 2011; Fleming & Ownsworth, 2006). Thus, the adoption of strategies learned in the program appears to have benefited tasks involving memory, planning, and problem-solving, even though some tasks remained below the standardization sample scores. However, tasks aimed at affect expression did not show improvement following the intervention. Although Braga et al. (2023) demonstrated a reduction in anxiety levels in this sample, addressing affective disturbances remains a challenge.
Limitations of the Present Study
When faced with having to evaluate large numbers of Long COVID patients seeking rehabilitation services for neuropsychological symptoms, extensive neuropsychological testing is impractical. Thus, the present study had to limit neuropsychological testing to a single screening instrument. More detailed neuropsychological assessments would provide greater confidence in the findings we reported, including a clearer understanding of affective performance. This major limitation of the study, however, was imposed by the realities of patient care for a large number of individuals. It provides only a “starting point” for planning further interventions focused on cognitive and behavioral functions in Long COVID patients.
A second potential limitation that might be raised by some neuropsychologists was the failure to include performance validity testing (PVTs) when conducting the BNI Screen. It has been estimated that between 8 to 9% of Long COVID patients fail PVTs in the United States (Considine et al., 2024). This study was done in Brazil. We acknowledge that there can be incentives to overstate one's cognitive and/or behavioral adjustment difficulties, but in the context of the cultural setting in which this study occurred it seems relatively unlikely. Many of these patients were working when undergoing psychoeducational orientation rehabilitation and were not seeking disability or financial support (Braga et al., 2022; Braga et al., 2023). We do note that over 40% of the study sample had average mean scores on the BNI Screen but were reporting neuropsychological impairments for which they were seeking treatment/rehabilitation. In keeping with a biopsychosocial model of this disease, we recognize that for some Long COVID patients there may be non-neurological factors contributing to their reported symptoms. However, the present findings are unique insofar as they demonstrate a very wide range impairment levels, yet highlight specific neuropsychological test performance failures. Those failures include both cognitive and affective domains of functioning. In this regard, we proposed that the BNI Screen for Higher Cerebral Functions may be especially useful in assessing this diverse patient group when planning neuropsychological rehabilitation.
Conclusion
Long COVID patients, who complain of residual cognitive and affective symptoms, do not always demonstrate such disturbances when undergoing screening of their neuropsychological functions. A psychoeducational program incorporating metacognitive and compensatory strategies led to a slight improvement in these patients’ performance. However, our investigation of 208 Long COVID patients pre and post a psychoeducational rehabilitation program reveals consistent difficulties in the efficient learning and memory, affect expression and accuracy of prediction of their verbal memory performance. These domains of functioning appear to be important areas to address when attempting to help individuals reduce their symptoms via rehabilitation interventions. This study is, however, only a “starting point” for planning cognitive and behavioral interventions for patients with Long COVID. Individual analysis of the patient's medical, psychological, and social conditions may help determine the more important aspects of the biopsychosocial model to focus on in the rehabilitation of specific Long COVID patients.
Footnotes
Acknowledgements
The authors would like to acknowledge the participation of Andrea Suhet Moreira, Maria Eloá Moreira da Silva Martins Pereira, Andrea Simoes Serra Serio, Virgínia da Silva Carneiro, Luciana de Figueiredo Pereira Freitas, Olinda Paula Azevedo, and Isabela Vollstedt Bastos.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors of this manuscript declare that they have no relevant financial or personal relationships with individuals or commercial interests (entities producing, marketing, re-selling, or distributing health care goods or services consumed by, or used on, patients) that could inappropriately influence or bias their work.