
Abstract
Background
Neurological disorders are the leading cause of global disability. To enhance neurorehabilitation effectiveness, it is essential to consider contextual factors that influence patient outcomes and the overall experience.
Objective
This study aimed to examine the integration of contextual factors into neurorehabilitation practice among physical therapists, focusing on their frequency of use, associated beliefs, ethical considerations, and communication strategies.
Methods
A cross-sectional web-based survey was disseminated to a convenience sample of physical therapy professionals via various online platforms. The survey collected demographic data and information regarding the integration of contextual factors into neurorehabilitation practice.
Results
A total of 369 physical therapists completed the survey. Respondents reported moderate use of contextual factors (43%), with verbal communication (85%), positive attitude (82%), and physical contact (75%) the most frequently employed factors. The strongest beliefs about the influence of contextual factors on therapeutic outcomes were linked to verbal communication and optimistic behavior. No significant correlations were found between respondents’ characteristics and the use of contextual factors.
Conclusion
Physical therapists recognize the importance of contextual factors such as verbal communication, positive attitudes, and a professional approach in neurorehabilitation. Enhanced training is recommended to further integrate these factors into neurorehabilitation practice and optimize patient outcomes.
Introduction
Neurological disorders are the primary cause of global disability. The disability-adjusted life years (DALYs), which combine years of life lost and years lived with disability due to neurological conditions, have risen by 18% since 1990 (Steinmetz et al., 2024). Neurological disorders are becoming a major public health concern, with predictions indicating a significant rise in their prevalence and impact in the coming years (Feigin et al., 2020). The high prevalence of neurological disorders such as stroke, epilepsy, and Parkinson's disease presents considerable challenges for healthcare systems and individuals affected (Feigin et al., 2020). The increasing prevalence of neurological disorders highlights the rising global demand for rehabilitation services (Jesus et al., 2019). A recent systematic review indicates that these services play a crucial role in significantly reducing the global burden of disability (Cieza et al., 2020).
Neurorehabilitation focuses on facilitating recovery following nervous system injury, with the primary goal of minimizing functional deficits and enhancing patient independence (Katz & Dwyer, 2021). In this context, physical therapists play a critical role in this process, particularly by addressing motor control and learning deficits through targeted therapeutic interventions aimed at reducing impairments and enhancing functional capacity (Langhorne et al., 2011). Nevertheless, the neurorehabilitation research community has recognized that a one-size-fits-all approach is ineffective in addressing the complexities of individual patient needs (Winstein, 2018). To optimize rehabilitation outcomes, it is essential to consider contextual factors such as patient perspectives, social support, cultural beliefs, and expectations that influence the therapeutic outcome and patient experience. These factors play a crucial role in creating a supportive environment that enhances patient engagement and treatment adherence, thereby improving rehabilitation outcomes (Di Blasi et al., 2001; Mairami et al., 2020; Winstein, 2024; Zou et al., 2016).
Contextual factors are defined as “variables that are not outcomes of the study but need to be recognized (and measured) to understand the results, including potential confounders and effect modifiers” (Boers et al., 2014). These factors can influence outcomes by triggering expectations, memories, and emotions, potentially leading to placebo or nocebo effects (Palese et al., 2019). This approach aligns with the World Health Organization's (WHO) International Classification of Functioning (ICF), which promotes a broader biopsychosocial understanding of functionality by integrating biological, psychological, and social factors in patient care (World Health Organization, 2001). Several elements can be recognized as contextual factors, such as the characteristics of physical therapists (e.g., professionalism, gestures, behaviors, and appearance), patient characteristics (e.g., expectations, beliefs, and personality), the therapist-patient relationship (e.g., verbal and non-verbal communication), the treatment approach (e.g., clear diagnosis, patient-centered approach), and the therapeutic environment (e.g., interior design, equipment) (Hall et al., 2010; Rossettini et al., 2020). These contextual factors are recognized as key mediators in the rehabilitation process (Testa & Rossettini, 2016).
For patients with neurological disorders, contextual factors play a critical role in shaping pain perception and motor function, potentially leading to enhanced rehabilitation outcomes. Pain-related beliefs are also essential; individuals with spinal cord injury (SCI) and stroke who believed that activity could exacerbate their condition reported higher pain intensity and interference, whereas those who believed in a medical cure experienced reduced pain level (Adams et al., 2019; Mairami et al., 2020). Studies have shown that incorporating patient-centered approaches in rehabilitation, such as personalized exercise programs and motivational interviewing, can significantly improve motor function and overall quality of life for stroke survivors (Oyake et al., 2023). Additionally, robust social support networks correlate with better adherence to interventions and overall psychological well-being for patients with stroke and SCI (Adams et al., 2019; Mairami et al., 2020). Integrating culturally tailored rehabilitation interventions that align with patients’ beliefs and values further enhances engagement and motivation during therapy, leading to improved functional outcomes (Mairami et al., 2020). Therefore, understanding and integrating contextual factors into clinical practice is essential for delivering culturally sensitive and effective care.
Despite the growing recognition of their importance, research gaps remain regarding how physical therapists perceive and integrate these elements, particularly in neurorehabilitation. Several studies have explored contextual factors in other rehabilitation settings. For instance, Rossettini et al. (2018) conducted a cross-sectional survey among physical therapists specialized in Orthopedic Manual Therapy, revealing broad knowledge of the psychological and physiological effects of contextual factors while also highlighting those certain elements (e.g., professional reputation, specific environmental features) are underused or inconsistently applied. Many therapists also expressed a need for greater education and ethical guidance on their application. More recently, Sherriff et al. (2023) used a modified Delphi approach to assess the views of musculoskeletal practitioners, including physical therapists, and reported a strong consensus on the importance of contextual factors, particularly the therapeutic alliance, practitioner beliefs, and patient characteristics in shaping outcomes for individuals with chronic low back pain. However, practitioners reported less confidence in managing cognitive and emotional needs and noted the need for further training in psychosocial competencies. While these studies support the relevance of contextual factors, they are primarily limited to musculoskeletal or general rehabilitation settings. Therefore, this study aims to examine the integration of contextual factors into neurorehabilitation, focusing on their frequency of use, associated beliefs, ethical considerations, and communication strategies among physical therapists.
Methods
Design and Participants
This study employed a cross-sectional survey design. We recruited physical therapists who were involved in providing healthcare to individuals with neurological conditions. Students and physical therapy interns were excluded from the study. This study was conducted in accordance with the Declaration of Helsinki and approved by the College of Medicine Institutional Review Board at King Saud University Medical City (IRB No. E-21-6434). All participants provided an informed consent form prior to their participation.
According to the Saudi Commission for Health Specialties, the number of Saudi physical therapists was estimated to be 5,500 at the time of the survey (World Physiotherapy, 2021). The required sample size for this study was estimated using Daniel's formula (Daniel & Cross, 2018), with a 95% confidence interval and a 5% margin of error, resulting in a target of 360 physical therapists. To account for potential non-responses or dropouts, a larger number of therapists were invited to participate.
Survey
A self-administered, web-based questionnaire was utilized to conduct this cross-sectional study. The content of the questionnaire was adapted from a previously developed and content-validated instrument by Rossettini et al. (2018), which was designed through expert panel review and pilot testing with clinicians. The survey was administered through SurveyMonkey and consisted of two sections: Section A (sociodemographic and professional characteristics) included questions about gender, age, educational background, area of practice, and years of experience in the field. Section B (contextual factors) contained questions designed to explore various aspects of contextual factors, including the frequency of use of contextual factors, beliefs about their therapeutic effects, perceived ethical implications, communication strategies related to contextual factors, the circumstances of contextual factors’ application, potential mechanisms of action, and their therapeutic effects on various health conditions, including acute pain, chronic pain, neurological disorders, and rheumatologic disorders. The complete survey instrument is provided in Appendix A.
Data Collection
Before initiating the primary data collection, a pilot survey was administered to a group of 10 expert Saudi physical therapists to assess the survey's effectiveness. The pilot survey took about 10–15 min to complete, and feedback was gathered over a two-week period. Adjustments were subsequently made to improve the survey's style consistency, formatting, and clarity of response options. After incorporating these revisions, the finalized survey link was distributed to the physical therapists through the email lists of the Saudi Physical Therapy Association (SPTA) and the Ministry of Health (MOH). Additionally, the survey link was circulated via social media posts, and invitations were shared by physical therapists within their professional networks.
Statistical Analysis
Data from the physical therapy survey were downloaded from SurveyMonkey and imported into Excel for thorough review, focusing on accuracy and identifying any missing values. Demographic and other participant characteristics were summarized using counts (percentages) for categorical variables and means (standard deviations) for continuous variables. Frequency counts and percentages were calculated to summarize survey responses regarding the use of contextual factors, beliefs about their therapeutic effects, ethical implications, and communication strategies. For frequency of use and belief items, mean scores with 95% confidence intervals (CIs) were calculated to provide an overall measure of belief strength for each contextual factor. The relationships between participants’ characteristics and the use of contextual factors were analyzed using Cramer's V. Additionally, associations between the frequency of contextual factor use and the participants’ beliefs about these factors were examined using Spearman's correlation test, with Fisher's Z transformation applied for adjustment. All analyses were conducted using R software v4.2.2, with a significance level set at 5%.
Results
Characteristics of the Respondents
The characteristics of the respondents are shown in (Table 1). The majority of respondents were female (n = 250; 68%), with an average age of 29 ± 6 years. Most participants held a bachelor's degree (83%) and had 1 to 5 years of clinical experience (n = 267; 72%). A significant portion of the respondents worked between 31 and 45 h per week (n = 154; 42%), and over half were private practitioners (n = 201; 54%).
Sociodemographic and Professional Characteristics of Respondents (n = 369).
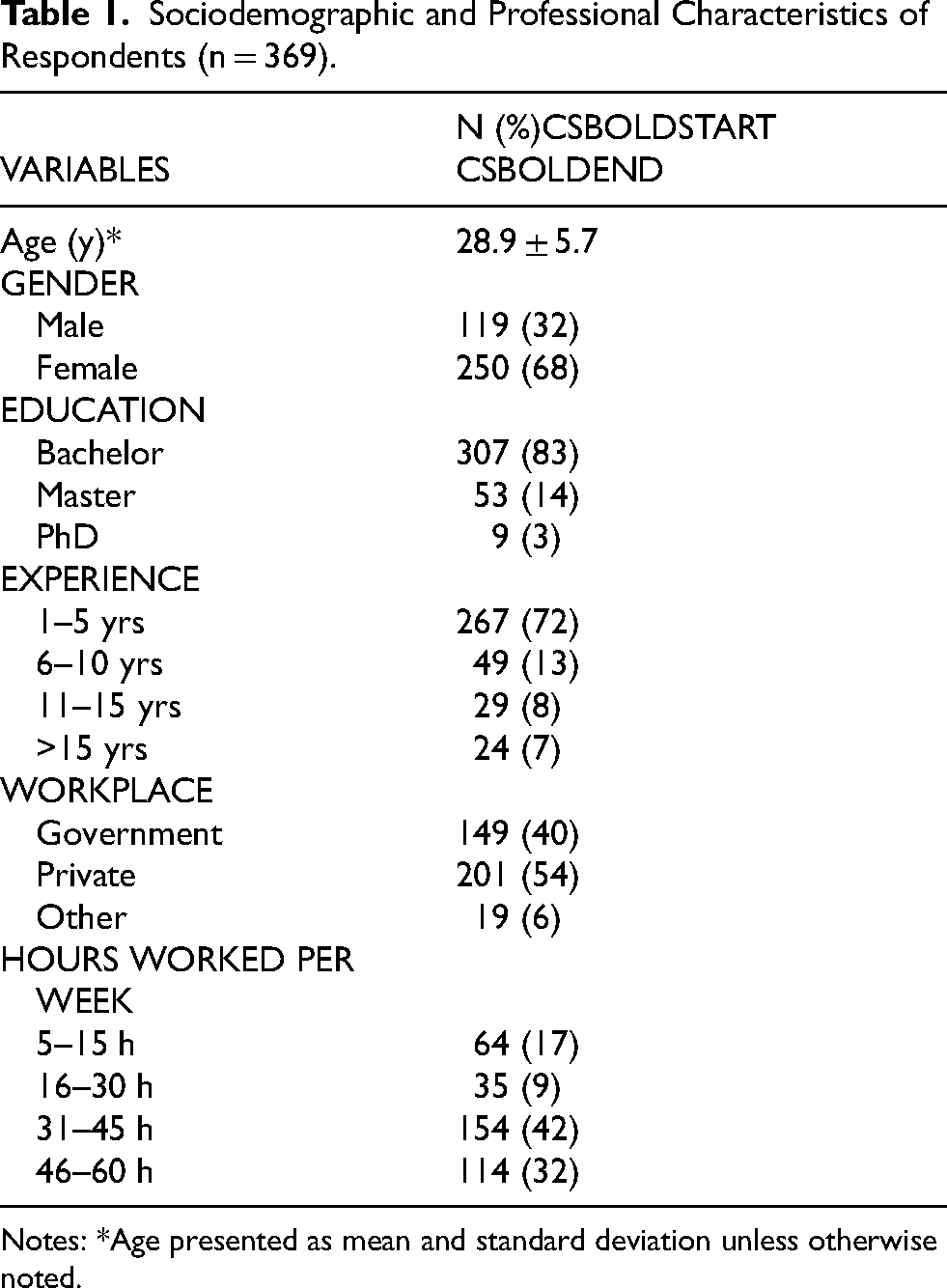
Notes: *Age presented as mean and standard deviation unless otherwise noted.
Frequency of Use of Contextual Factors
The use of contextual factors among physical therapists showed moderate use, with an overall mean frequency of 1.8 (95% CI 1.7–1.9) on a four-point Likert scale. Specifically, 43% of physical therapists reported using contextual factors ‘many times’ in their clinical practice, while 38% used them ‘often’ (n = 140), 14% ‘at least once’ (n = 51), and 6% ‘never’ (n = 21). The most frequently employed contextual factors were ‘verbal communication’ (mean = 1.3; 95% CI 1.2–1.4, daily use = 85%), ‘positive attitude and optimistic behavior’ (mean = 1.4; 95% CI 1.3–1.5, daily use = 82%), ‘professional approach to patient’ (mean = 1.6; 95% CI 1.5–1.7, daily use =75%), and ‘physical contact with the patient’ (mean = 1.5; 95% CI 1.5–1.6, daily use = 75%). In contrast, the least utilized factors were ‘professional reputation’ (daily use = 40%), ‘adequate design and environment architecture’ (daily use = 48%), and ‘comfortable setting’ (daily use = 54%). A detailed breakdown of contextual factors usage is presented in Figure 1.
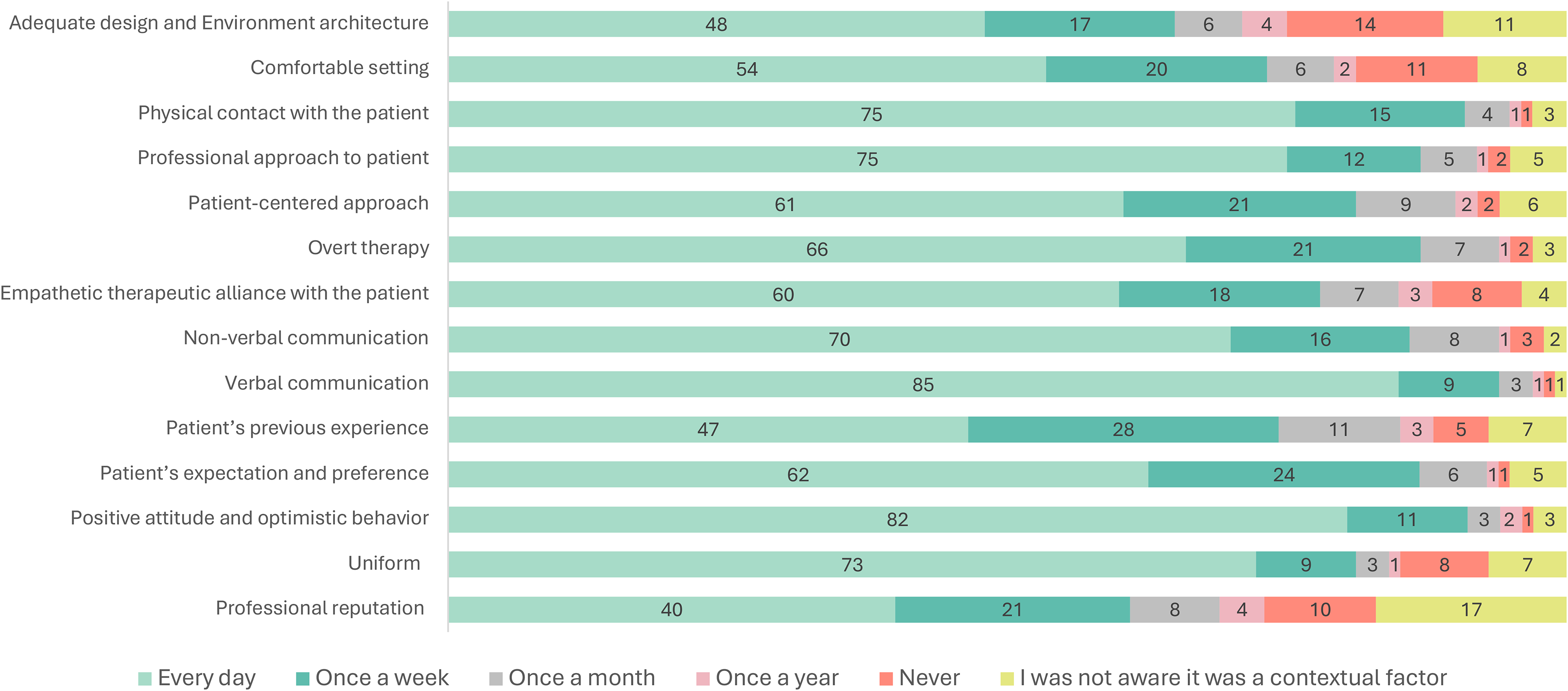
Frequency of use of Contextual Factors in Neurorehabilitation among Physical Therapists.
Beliefs about the Influence of Contextual Factors on Therapeutic Outcomes
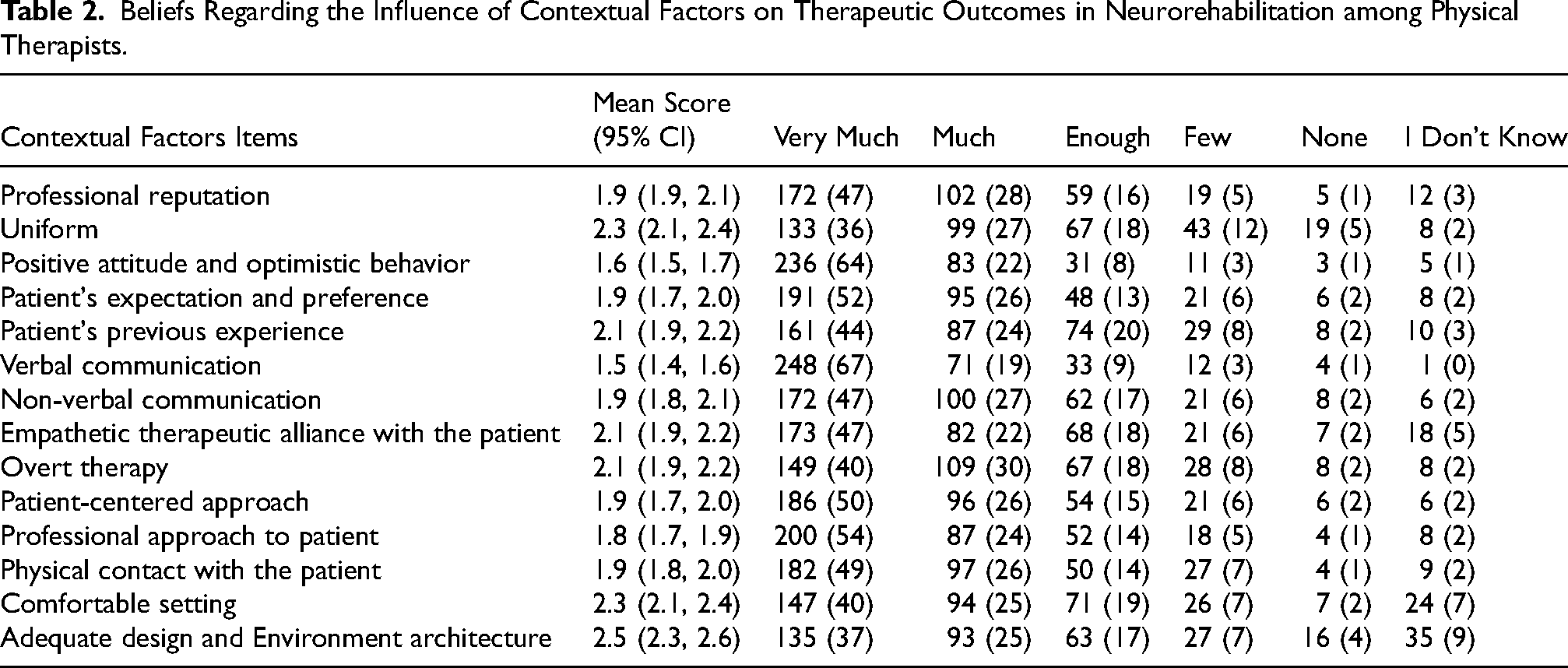
The most strongly believed contextual factors were ‘verbal communication’ (mean = 1.5; 95% CI 1.4–1.6), ‘positive attitude and optimistic behavior’ (mean = 1.6; 95% CI 1.5–1.7), and ‘professional approach to patient’ (mean = 1.8; 95% CI 1.7–1.9). The least strongly believed factors were ‘uniform’ (mean = 2.3; 95% CI 2.1–2.4), ‘comfortable setting’ (mean = 2.3; 95% CI 2.1–2.4), and ‘adequate design and environment architecture’ (mean = 2.5; 95% CI 2.3–2.6). An overall description of beliefs regarding contextual factors is provided in (Table 2).
Beliefs Regarding the Influence of Contextual Factors on Therapeutic Outcomes in Neurorehabilitation among Physical Therapists.
Therapeutic Benefits of Contextual Factors
Physical therapists most frequently reported ‘physiological and psychological’ effects as the therapeutic benefits of contextual factors, particularly in cases involving acute pain (n = 191, 52%) and neurological disorders (n = 186, 50%). The ‘psychological’ effect was predominantly noted in cases of chronic pain (n = 142; 39%). The least benefit was reported for rheumatologic disorders, with 11% (n = 42) indicating no beneficial effect. No health condition was exclusively associated with ‘physiological’ effects. A detailed report of therapeutic effects is presented in (Table 3).
Therapeutic Benefits of Contextual Factors (n = 369).

Ethical Implications of Using Contextual Factors in Neurorehabilitation
The most common response regarding the ethical acceptability of using contextual factors was that they bring ‘beneficial psychological effects’ (76%). The least selected ethical justification was ‘the other therapies are over’ (12%). Conversely, the use of contextual factors was considered ethically unacceptable when based on the notion that ‘evidence is insufficient’ (55%). The least frequent response indicating ethically unacceptable use was when ‘it undermines trust between patient and physical therapist’ (37%). Detailed results for ethical implications are illustrated in Figure 2.
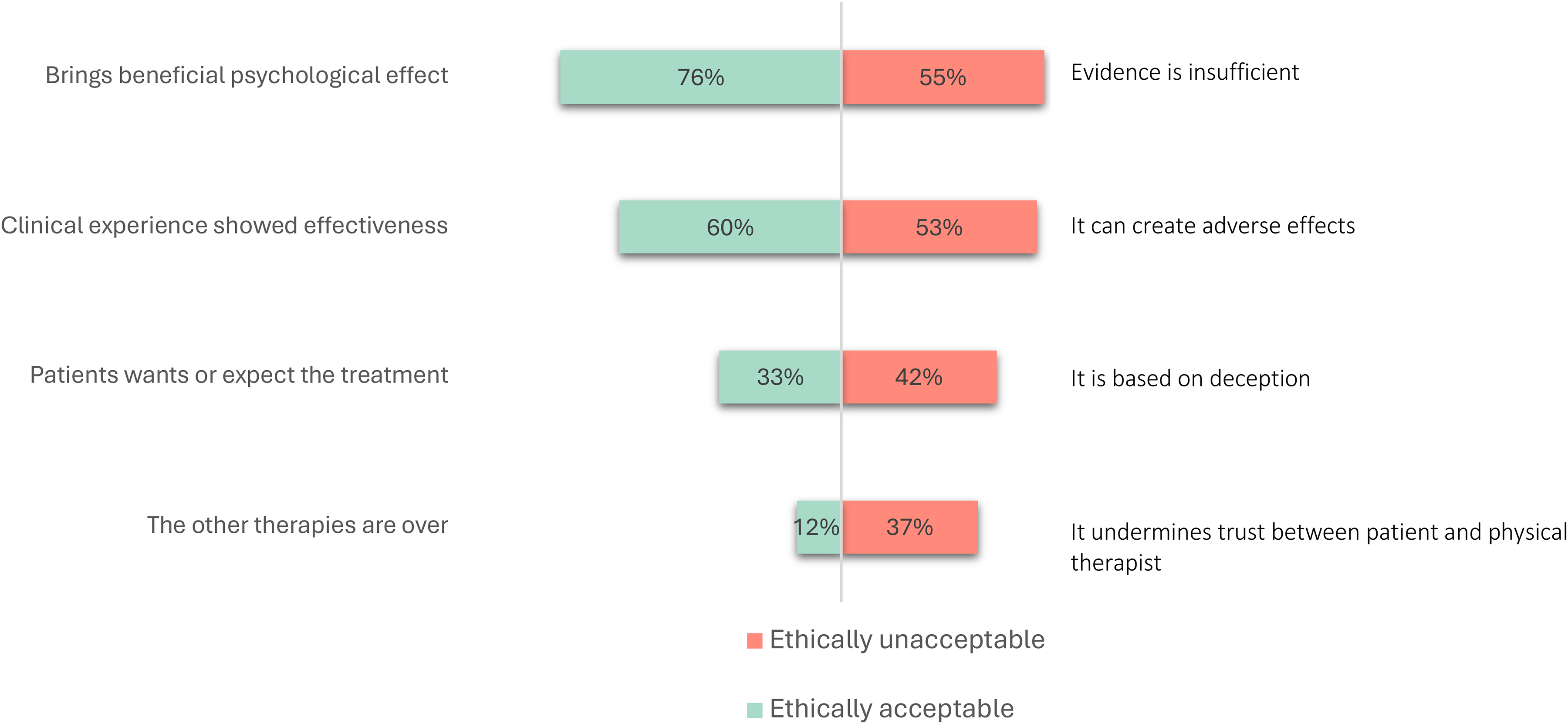
Percentages of Responses for Ethically Acceptable and Unacceptable Use of Contextual Factors in Neurorehabilitation Among Physical Therapists.
Communication of Contextual Factors to Patients
When questioned about communication of contextual factors, respondents most frequently selected the statement ‘it is a treatment that can help and will not hurt’ (48%). The least common response was ‘it is a treatment without a specific effect’ (6%). Detailed responses regarding the communication of contextual factors are presented in Figure 3.
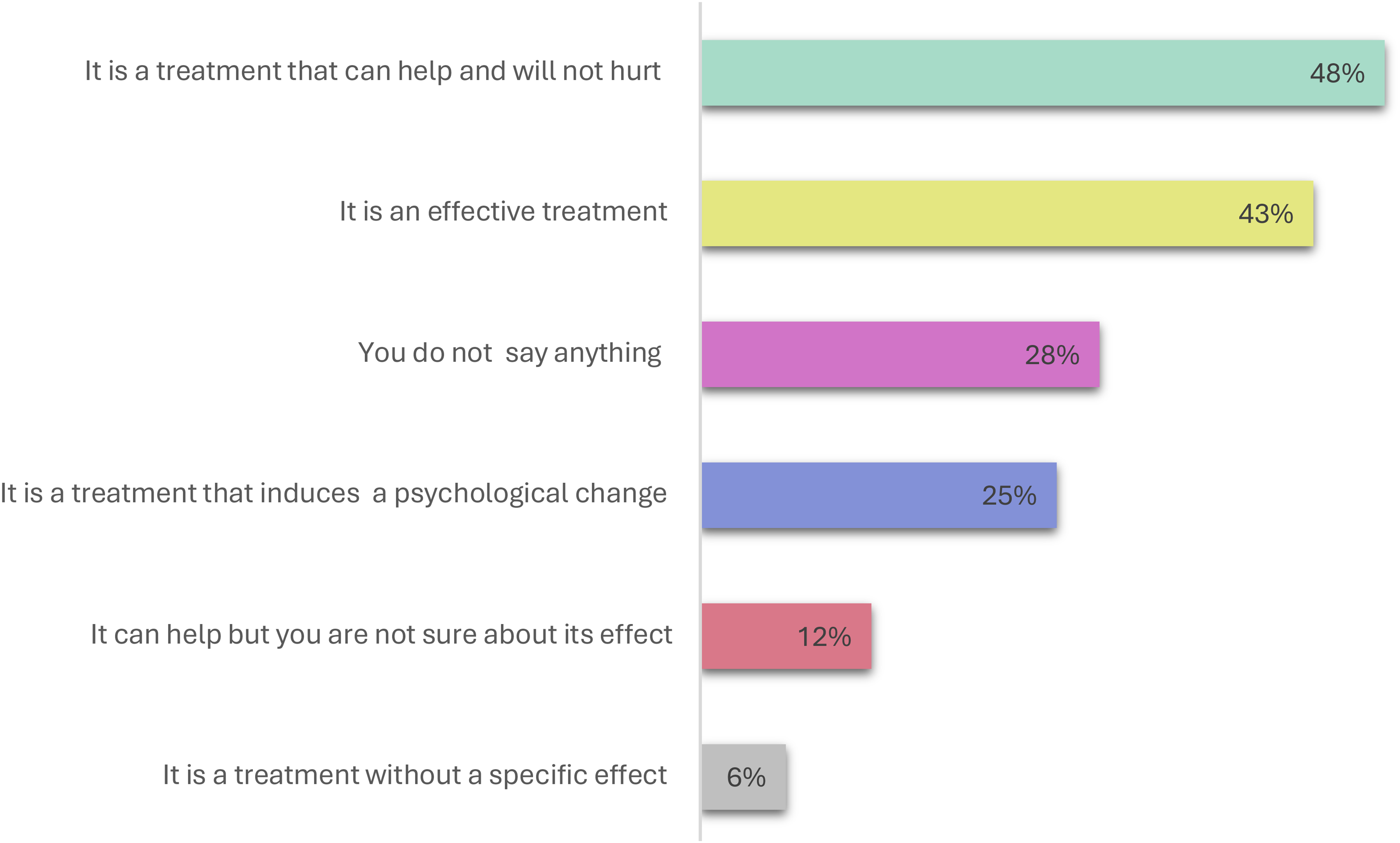
Responses on How Physical Therapists Communicate the Use of Contextual Factors to Patients in Neurorehabilitation.
Circumstances and Mechanisms for Applying Contextual Factors
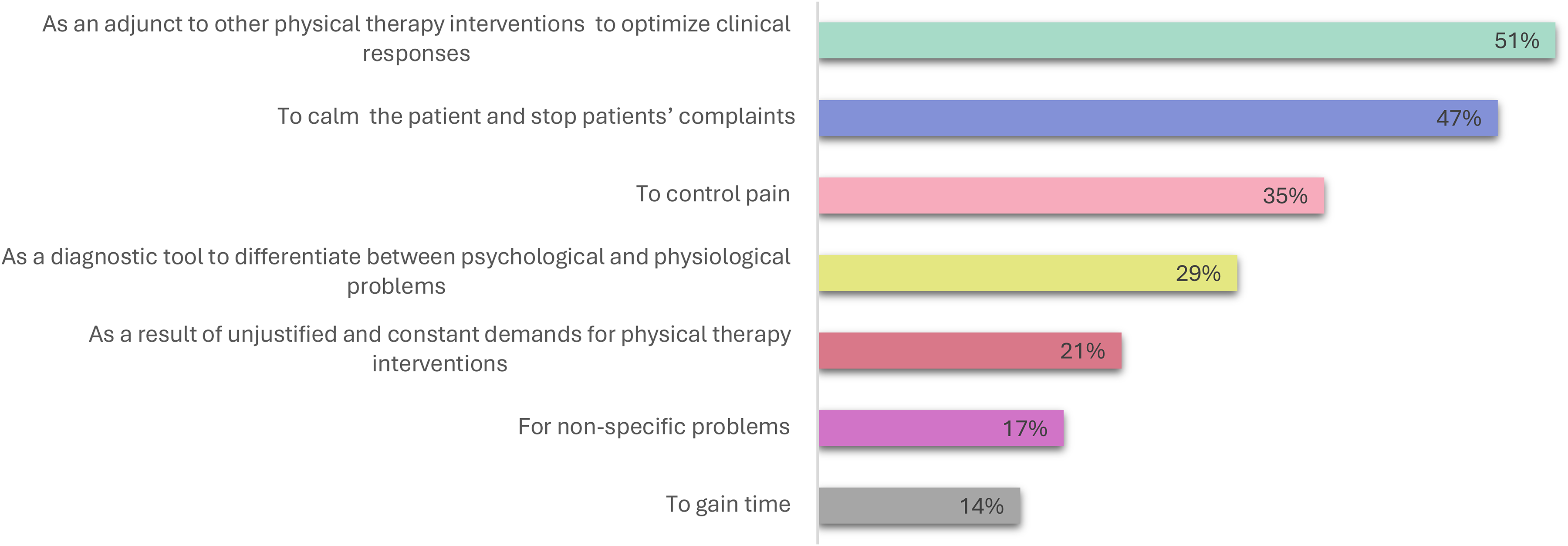
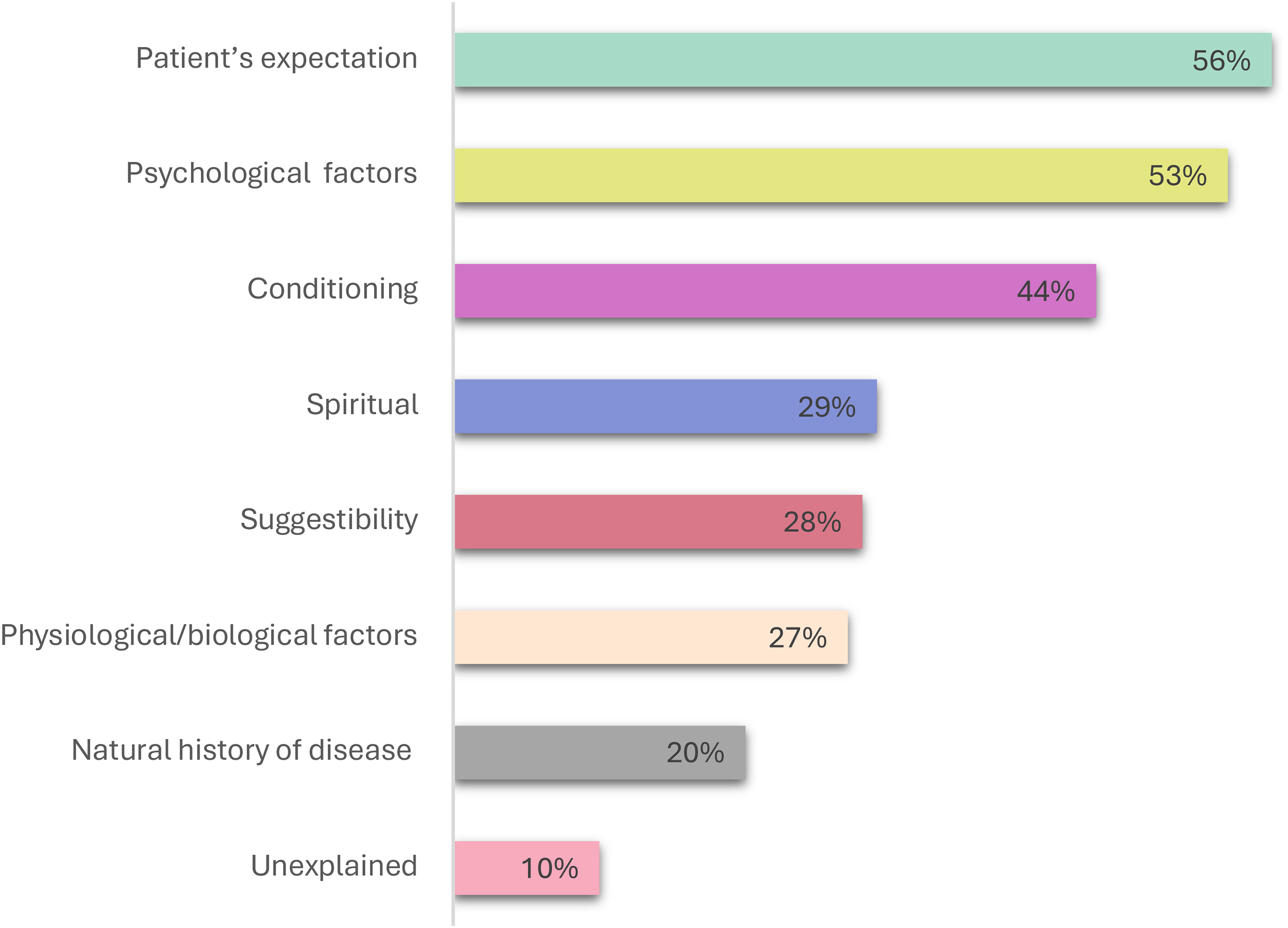
The most frequently reported circumstance for applying contextual factors was ‘as an adjunct to other physical therapy interventions to optimize clinical responses’ (51%). The least frequent circumstance was ‘to gain time’ (14%). A full presentation of circumstances of application is provided in Figure 4. Regarding the mechanism of action, the most common belief was that contextual factors work through ‘patient's expectation’ (56%), while the least selected mechanism was ‘unexplained’ (10%). Responses for mechanisms of action are presented in Figure 5.
Percentages of Responses for Communication to Patients’ Implications of Contextual Factors.
Percentage of Responses for Circumstances of Contextual Factors Application.
Correlation Between Variables
The correlation coefficients between the frequency of contextual factor use and beliefs about their impact were all weak (rs < 0.4). The weakest correlations were observed for ‘reputation’ (rs = 0.16) and ‘empathetic behavior’ (rs = 0.16). A detailed presentation of these correlations is provided in Figure 6. There were no significant correlations (Cramer's V) between the demographic characteristics and the frequency of use of contextual factors.
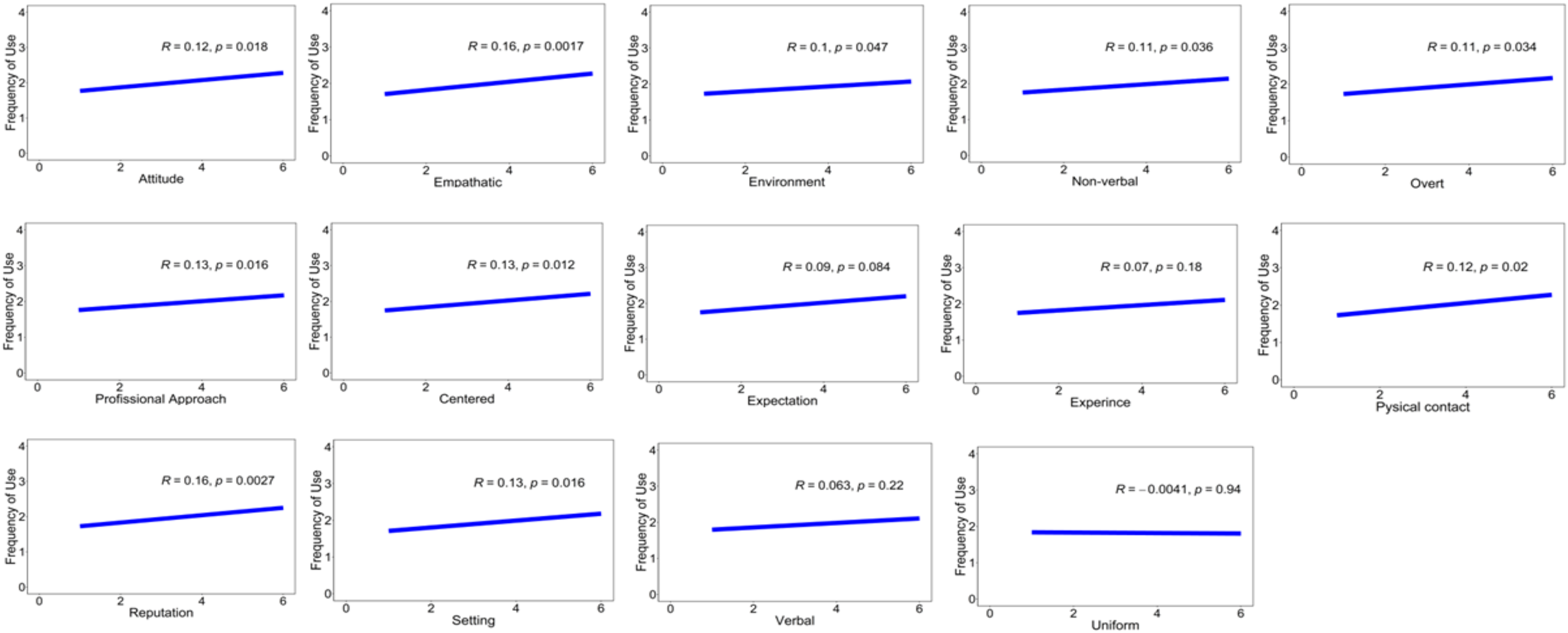
Correlation between Responses of Frequency of Use and Believes of Contextual Factors.
Discussion
The primary finding of this research indicates that physical therapists reported a moderate frequency of using contextual factors in their daily practice and expressed a strong belief in their therapeutic value. Verbal communication and maintaining a positive attitude were reported as the most frequently used contextual factors in neurorehabilitation settings. This emphasis on communication and optimism was likely rooted in the unique needs of patients with neurological conditions, who often face significant challenges related to motor function, cognition, and emotional well-being. Verbal communication in neurorehabilitation has been associated with improved patient outcomes, including better engagement in therapy and higher levels of motivation and adherence to the rehabilitation program (Danzl et al., 2012; Pinto et al., 2012). This is further supported by studies among physical therapists, which highlight the central role of communication in building therapeutic relationships and enhancing patient participation (Oyake et al., 2023; Roberts & Bucksey, 2007; Rossettini et al., 2018; Testa & Rossettini, 2016).
A positive attitude and optimistic behavior from physical therapists significantly contribute to patient outcomes, particularly in the mentally and emotionally taxing process of neurorehabilitation. A therapist's positive demeanor fosters a supportive environment, mitigating frustration and hopelessness and enhancing patient satisfaction and engagement (Pinto et al., 2012). This therapeutic relationship, characterized by empathy and encouragement, is crucial for maintaining resilience and promoting successful rehabilitation outcomes (Lange & Danielsson, 2024; Peiris et al., 2012). Establishing a positive patient-clinician communication atmosphere is also vital, as it can trigger placebo analgesic effects that enhance treatment outcomes. For instance, Knittle et al. (2012) found that interventions targeting motivation in rheumatoid arthritis patients improved self-efficacy and physical activity levels, with these gains sustained over 32 weeks, despite minimal contact time. Recent perspectives underscore that integrating such optimistic and motivational elements into physical therapy practice is more than a technique; it represents a shift in professional identity toward function-focused, psychologically informed care that empowers patients, promotes engagement, and ultimately optimizes rehabilitation outcomes (Purcell & Langridge, 2025).
The results of this study also revealed that 75% of respondents consistently employed a professional approach to patient care, reflecting their confidence in its effectiveness as a contextual factor that positively influences patient outcomes in neurorehabilitation. A professional approach, which includes clear communication, empathy, and a structured treatment plan, is essential for building trust and confidence across rehabilitation, including neurorehabilitation settings (Melin et al., 2021; Parry, 2004; Turner-Stokes et al., 2009).
Furthermore, a significant proportion of physical therapists recognized the efficacy of physical contact in neurorehabilitation. Therapeutic touch and manual guidance play crucial roles in enhancing patient engagement and facilitating motor learning, particularly for patients with neurological conditions, by reinforcing trust and emotional support. Physical contact serves as a powerful tool during clinical interactions, conveying trust, empathy, and support, which are essential for fostering a therapeutic relationship (Bishop et al., 2019; Druart et al., 2023; O'Keeffe et al., 2016). Physical contact between the patient and therapist was found to enhance the patient-therapist interaction, as reported by both physical therapists and patients (Rossettini et al., 2018). These findings underscore the importance of incorporating physical contact into neurorehabilitation practices to support patients’ emotional and physical well-being during their recovery.
Uniforms were generally less emphasized as a contextual factor by physical therapists. This finding aligns with the results of previous studies where patients perceive white coats as more professional but prefer tailored clothing for physical therapists, which may reflect the close, hands-on nature of the patient-therapist relationship (Ingram et al., 2011; Mercer et al., 2008). Evidence suggests that patients value comfort and approachability over formal attire in these settings, which can facilitate a more collaborative and trusting therapeutic relationship (Ingram et al., 2011; Mercer et al., 2008). This contrasts with the medical field, where lab coats are often regarded as both the most professional and preferred attire (Rehman et al., 2005). These differences in attire preferences may be attributed to the distinct roles and interpersonal dynamics between patients and their healthcare providers.
A majority of physical therapists believe that the use of contextual factors is ethically acceptable because they have beneficial psychological effects Additionally, 12% of physical therapists believe it is ethically acceptable to use contextual factors only when other therapies are over, raising concerns about their inappropriate use as a last resort rather than as part of an integrated, evidence-based practice. This highlights the importance of using contextual factors to complement, rather than replace, established therapies (Leplege et al., 2007). Furthermore, the prioritization of patient autonomy, particularly when patients expect or request these treatments, further underscores the need for careful ethical consideration in their application (Hufford, 2003; Jesus et al., 2022; Légaré et al., 2011).
In this study, most physical therapists recognized that the mechanism for action of contextual factors originates from patients’ expectations, combined with psychological factors such as treatment motivation and credibility. Patient expectations, defined as beliefs about the likely outcomes of a treatment, play a crucial role in influencing the effectiveness of interventions, particularly in pain management (Turner-Stokes et al., 2009; Wassinger et al., 2022). Previous studies emphasized the importance of incorporating patient expectations into the decision-making process. In stroke rehabilitation, expectations and motivation are key factors that facilitate recovery, with greater self-efficacy contributing to better outcomes (Winstein, 2018).
Approximately 50% of the physical therapists in this study characterized contextual factors as an “intervention that can help but will not harm,” reflecting the view that these factors are supplementary rather than central to patient outcomes. This perspective may stem from a limited understanding of the neurophysiological mechanisms underlying the therapeutic effects of contextual factors, which are increasingly recognized for their potential to enhance clinical outcomes in neurorehabilitation (Testa & Rossettini, 2016; Turner-Stokes et al., 2009). Although often used as adjuncts to optimize clinical responses, the potential of contextual factors as a primary therapeutic intervention appears underutilized. Practical limitations, such as time constraints, high patient volumes, and a limited number of sessions, may further limit their consistent application. A previous study on motor learning in neurorehabilitation also identified limited knowledge and time constraints at both the individual and organizational levels as key barriers to implementation among physical therapists (Almarwani & Aldawsary, 2023). These challenges underscore the need for enhanced training programs that not only strengthen therapists’ understanding with evidence-based knowledge but also empower them to integrate contextual factors more effectively into neurorehabilitation practice, ultimately optimizing patient outcomes.
This study has several limitations that should be acknowledged. First, the reliance on self-reported data introduces the potential for response bias, as participants may have interpreted or recalled their experiences inaccurately. Additionally, the specific population of surveyed physical therapists may limit the generalizability of the findings. The cross-sectional design of the study further restricts the ability to establish causal relationships. Furthermore, the study focused on physical therapists dealing with a broad range of general neurological conditions rather than specific disorders, which may limit the applicability of the findings to neurological conditions.
Conclusion
Physical therapists recognize the importance of contextual factors in neurorehabilitation and believe in their therapeutic potential, particularly in the use of verbal communication, maintaining a positive attitude, and employing a professional approach. However, many therapists perceive these factors as supplementary rather than central to patient outcomes, which may stem from a limited understanding of the neurophysiological mechanisms underlying their therapeutic effects. As a result, contextual factors are often underutilized as primary therapeutic interventions. To address this, enhanced training is recommended to better integrate these factors into practice, ultimately optimizing patient outcomes in neurorehabilitation.
Footnotes
Consent to Participate
All participants provided informed consent prior to participation.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and approved by the College of Medicine Institutional Review Board at King Saud University Medical City (IRB No. E-21-6434).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Appendix A. Survey Instrument
Dear participants,
You are invited to participate in a research survey about integrating contextual factors into neurorehabilitation among physical therapists.
Objectives: to examine the integration of contextual factors into neurorehabilitation practice among physical therapists, focusing on their frequency of use, associated beliefs, ethical considerations, and communication strategies.
The contextual factors consist of a series of relational or environmental situations that may affect the perception of patients’ pain and functional impairment. For example, words, posture, and sounds are used by physical therapists in the therapeutic setting to enhance the effectiveness of the treatment.
Target participant: Licensed Saudi Physical therapist who are involved in providing healthcare to individuals with neurological conditions.
IRB approval of Research Project No. E-21-6434.
Participation in this survey: participation is voluntary, and responses will be kept anonymous. This online survey should take about 10 min to complete. Your participation and time in completing this survey are highly appreciated.
Please make sure to click the “submitting” button after finishing the survey.
□ I voluntarily agree to participate in this research study.
How old are you? ………. Gender:
□ Male □ Female What is your highest academic degree?
□ Bachelor □ Master □ Ph.D. How many years of clinical experience do you have?
□ 1–5 yrs □ 6–10 yrs □ 11–15 yrs □ > 15 yrs What is your main work setting?
□ General hospital □ Private practice □ Other How many hours do you work per week?
□ 5–15 h □ 16–30 h □ 31–45 h □ 46–60 h
it brings beneficial psychological effects the other therapies are over the patient wants or expects this treatment clinical experience has shown their effectiveness
it is based on deception it undermines trust between patient and physical therapist evidence is insufficient it can create adverse effects
it is a treatment that can help and will not hurt it is an effective treatment you do not say anything it is a treatment without a specific effect it is a treatment that induces a psychological change it can help but you are not sure about its effect.
as a result of unjustified and constant demands for physical therapy interventions to calm the patient and stop the patient's complaints as an adjunct to other physical therapy interventions to optimize clinical responses for non-specific problems as a diagnostic tool to differentiate between psychological and to control pain to gain time
patient's expectation conditioning suggestibility natural history of disease psychological factors unexplained physiological/biological factors spiritual energies mind-body connections