
Abstract
Objectives
To systematically review the effects of transcranial magnetic stimulation (TMS) on post-stroke dysphagia, focusing on stimulation mode, frequency, and target region.
Methods
This systematic review followed PRISMA guidelines and was registered in PROSPERO (CRD42025631286). We systematically searched PubMed, Cochrane Central, and Embase for RCTs on TMS for post-stroke dysphagia up to December 11, 2024. Meta-analysis was conducted using Stata 16, with heterogeneity assessed via the I2 statistic. Subgroup and sensitivity analyses explored sources of heterogeneity. Risk of bias and study quality were evaluated using the Cochrane Risk of Bias 2.0 (RoB 2) tool and the Physiotherapy Evidence Database (PEDro) scale.
Results
This meta-analysis included 14 RCTs with 882 stroke patients, assessing swallowing function using the Penetration-Aspiration Scale (PAS), Standardized Swallowing Assessment (SSA), Functional Dysphagia Scale (FDS), Fiberoptic Endoscopic Dysphagia Severity Scale (FEDSS), and Functional Oral Intake Scale (FOIS). The results showed that TMS significantly improved swallowing function across all scales: PAS (MD = −1.32, 95% CI: −1.50 to −1.14, P < 0.001), SSA (MD = −1.97, 95% CI: −2.43 to −1.50, P < 0.001), FEDSS (MD = −0.65, 95% CI: −0.84 to −0.46, P < 0.001), FOIS (MD = 0.92, 95% CI: 0.72 to 1.13, P < 0.001), and FDS (MD = −5.54, 95% CI: −7.48 to −3.60, P < 0.001).
Conclusion
This meta-analysis demonstrates that TMS significantly improves swallowing function in stroke patients, with consistent effects across scales, interventions, stimulation modes, and targets. However, variability in protocols and short follow-up periods may limit the generalizability of the findings.
Introduction
Dysphagia is a common and potentially life-threatening complication of stroke, with an incidence of 51% to 55% (Cohen et al., 2016; Diéguez-Pérez & Leirós-Rodríguez, 2020). It can lead to aspiration, choking, pneumonia, and malnutrition, significantly reducing quality of life and increasing healthcare burdens (Alamer et al., 2020; Pandian et al., 2018). Damage to swallowing-related brain regions may result in oral coordination issues, impaired pharyngeal contraction, delayed laryngeal vestibule closure, and cricopharyngeal dysfunction. Meanwhile, cognitive deficits, such as impaired attention and executive dysfunction, can further weaken the planning and monitoring of swallowing movements, exacerbating primarily motor-based dysphagia and, in severe cases, constituting an independent, cognition-driven subtype of oropharyngeal dysphagia (Dehaghani et al., 2021; Takizawa et al., 2016; Terré, 2020). Eating discomfort, anxiety, and reduced social interaction further impact quality of life. Traditional rehabilitation methods, such as swallowing muscle exercises, feeding training, and vocal exercises, often rely heavily on patient cooperation, which can be challenging for those with cognitive deficits. While some stroke patients recover swallowing function within weeks, recovery varies widely (Singh & Hamdy, 2006). Neuro-regulation techniques that enhance cortical plasticity have recently gained attention as effective strategies to improve swallowing function and reduce dysphagia-related complications (Fisicaro et al., 2019; Tang et al., 2024).
In recent years, brain stimulation techniques such as transcranial magnetic stimulation (TMS) and transcranial direct current stimulation (tDCS) have emerged as potential therapies for dysphagia (Gómez-García et al., 2023; Jiao et al., 2023). TMS is a safe, non-invasive, and painless neuromodulation method that regulates cortical excitability. Depending on the frequency, TMS can be categorized into low-frequency (≤1 Hz) and high-frequency (≥5 Hz) stimulation. Low-frequency TMS suppresses overactive cortical activity to restore balance, while high-frequency TMS enhances cortical excitability. Growing evidence has explored the use of TMS in post-stroke dysphagia, particularly its ability to activate the corticobulbar pathway by targeting the swallowing motor cortex, thereby improving muscle control (Tarameshlu et al., 2019). Several studies report significant benefits of TMS on swallowing function, especially when combined with conventional rehabilitation (Liu et al., 2022; Tarameshlu et al., 2019; Yu-Lei et al., 2022). However, some studies show limited or inconsistent effects, likely due to variations in patient characteristics, stimulation parameters, timing, and study designs (Juan Du et al., 2016; Khedr & Abo-Elfetoh, 2010; Lee et al., 2015).
Previous systematic reviews have suggested that rTMS may improve post-stroke dysphagia but did not assess the efficacy of theta-burst transcranial magnetic stimulation (TBS) or thoroughly analyze the effects of rTMS parameters such as frequency and target sites (Liao et al., 2017). Additionally, whether differences in stimulation modes (e.g., rTMS vs. TBS) or parameters (e.g., frequency and target sites) significantly influence treatment outcomes is unclear. This meta-analysis integrates evidence from RCTs to evaluate the efficacy of TMS, including rTMS and TBS, in treating post-stroke dysphagia. It also explores factors affecting treatment outcomes, such as stimulation mode, frequency, and target sites, to provide robust evidence for optimizing clinical use and guiding future research directions.
Methods
This systematic review was conducted in line with the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) and is registered in PROSPERO (International Prospective Register of Systematic Reviews) under the number CRD42025631286.
Search Strategy
We searched three databases (PubMed, Embase, and Cochrane Central Register of Controlled Trials) for RCTs published up to December 11, 2024. The search strategy included three components: ①Clinical condition: deglutit*/swallow*, dysphag*, brain*/ischemi*/cerebr*/cerebell*/infarct*; ②Intervention: TMS/rTMS/TBS; ③ Study type: RCTs. Truncation using an asterisk (*) was applied to capture keyword variations. The search combined controlled vocabulary (e.g., MeSH terms) and free-text terms, with references from included studies screened for additional relevant documents. Details of the search strategy are in Supplementary Table 1. Manual searches of references in published studies were also conducted, and authors of conference-only studies were contacted for data when possible.
Inclusion and Exclusion Criteria
This study followed the PICOS framework, with inclusion criteria as follows: (i) Participants (P): Patients diagnosed with ischemic or hemorrhagic stroke confirmed by CT or MRI, and with dysphagia or oropharyngeal dysfunction verified through VFSS, with no restrictions on sex, age, or other demographics; (ii) Interventions (I): The experimental group received TMS treatment, which could be combined with identical conventional rehabilitation interventions provided to both groups; (iii) Control group (C): The control group received the same interventions as the experimental group but without TMS; (iv) Outcomes (O): Studies must report original data or sufficient information on swallowing function before and after the intervention to evaluate efficacy; (v) Study design (S): Both parallel-arm and crossover RCTs were included. Exclusion criteria included studies where dysphagia was caused by other conditions (e.g., head trauma, cancer, or infections), those not providing original data (e.g., reviews, meta-analyses, systematic reviews, letters, or conference abstracts), and case reports. This framework ensures the quality and consistency of data for assessing the effectiveness of TMS in treating post-stroke dysphagia.
Study Selection and Data Extraction
Two reviewers (C.L. and J.W.) independently evaluated studies based on the inclusion and exclusion criteria. All citations were imported into EndNote (Clarivate Analytics) for deduplication and to facilitate title/abstract screening. Titles and abstracts were initially screened in EndNote, followed by full-text review to finalize included studies. Discrepancies were resolved through discussion, with a third reviewer (Z.Y.) adjudicating if needed. Data were collected using a standardized form, including the first author's name, country, publication year, study type, intervention details, sample size, control methods, clinical outcomes, and follow-up duration. Post-treatment scores included the Penetration-Aspiration Scale (PAS), Standardized Swallowing Assessment (SSA), Functional Dysphagia Scale (FDS), Fiberoptic Endoscopic Dysphagia Severity Scale (FEDSS), and Functional Oral Intake Scale (FOIS). Baseline characteristics of the 14 included studies are presented in Table 1.
Characteristics of Included Studies in the Meta-Analysis.
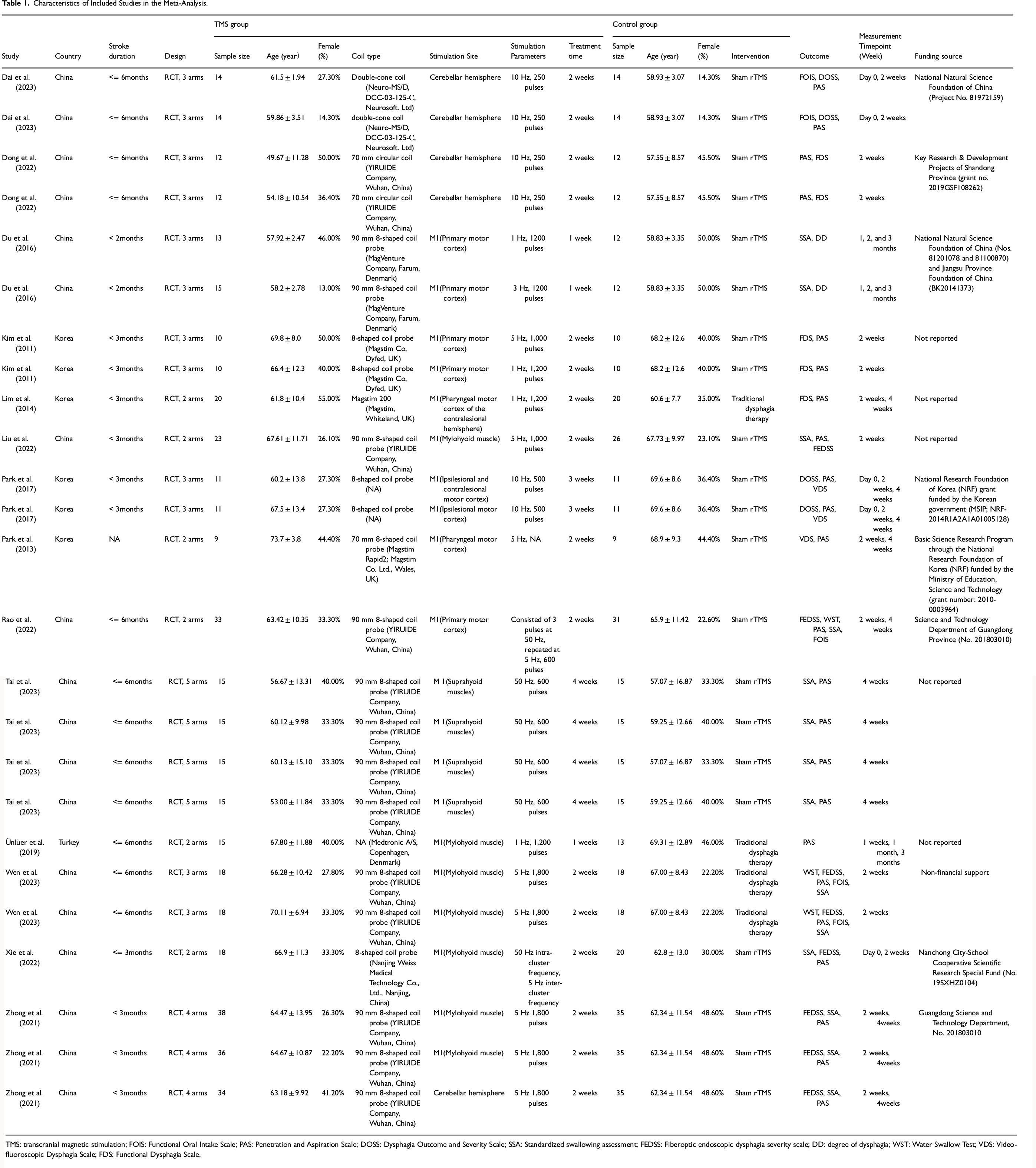
TMS: transcranial magnetic stimulation; FOIS: Functional Oral Intake Scale; PAS: Penetration and Aspiration Scale; DOSS: Dysphagia Outcome and Severity Scale; SSA: Standardized swallowing assessment; FEDSS: Fiberoptic endoscopic dysphagia severity scale; DD: degree of dysphagia; WST: Water Swallow Test; VDS: Video-fluoroscopic Dysphagia Scale; FDS: Functional Dysphagia Scale.
Mean values and standard deviations (SD) were used for the meta-analysis, extracted from published tables when available. If unavailable in tabular form, data were extracted from published figures using GetData Graph Digitizer (http://getdata-graph-digitizer.com). Two reviewers (C.L. and J.W.) independently performed all extractions, and any discrepancies were resolved by discussion or, if required, by adjudication with a third reviewer (Z.Y.).
To ensure reproducibility, inter-reviewer reliability was measured at each stage using Cohen's κ. In a pilot test on 10% of randomly selected records, C.L. and J.W. obtained κ = 0.78. Agreement was κ = 0.81 for title/abstract screening, κ = 0.84 for full-text review, and κ = 0.81 for data extraction from tables and figures. These values reflect substantial to nearly perfect concordance. Any disagreements were resolved by discussion or, if needed, by a third reviewer (Z.Y.).
Assessment of Risk of Bias
The Cochrane RoB 2 tool evaluated the risk of bias in the studies, focusing on randomization, deviations from intended interventions, missing data, outcome measurement, and result reporting. Each study's overall risk of bias was categorized based on these criteria. Two reviewers (L.W. and Y.S.) independently rated each item as high risk, some concerns, or low risk, followed by a cross-check. To supplement this, the PEDro scale was used to assess study quality. Discrepancies were resolved through consultation with a third reviewer (C.Q.).
Outcome Indicators
The primary outcomes in this study included the PAS, SSA, FDS, FEDSS, and FOIS. PAS, an 8-point scale commonly used with fiberoptic endoscopy, evaluates the severity of penetration and aspiration, with higher scores indicating more severe impairment (Borders & Brates, 2020). FOIS categorizes swallowing function into 7 levels based on safety and efficiency, with lower scores reflecting greater limitations, and is recognized for its high reliability and validity (Bakhtiyari et al., 2022). SSA, ranging from 18 to 46 points, measures swallowing dysfunction severity, with higher scores indicating worse function, and is well-suited for bedside screening (Yun et al., 2018). FEDSS, scored from 1 to 6, assesses risks associated with different food consistencies and observed penetration or aspiration during the endoscopic examination, where higher scores denote greater impairment (Jimenez-Dominguez & Manzano-Aquiahuatl, 2021). FDS provides a multidimensional assessment of swallowing function, with higher scores reflecting more severe dysfunction. These scales offer comprehensive evaluations from various perspectives, supporting the study's findings.
Certainty of Evidence Assessment
The certainty of evidence for primary outcomes was evaluated with GRADEpro GDT software (McMaster University) using the GRADE framework, which considers five domains: risk of bias, inconsistency, indirectness, imprecision, and publication bias. Evidence from randomized controlled trials started at a “high” level and was downgraded as warranted. Pooled estimates were used in GRADEpro to produce the Summary of Findings (SoF) table.
Data Synthesis and Statistical Analysis
Effect sizes for post-treatment clinical scores were calculated as standardized mean differences (SMD) with 95% confidence intervals (CI) using a Z test. Heterogeneity was assessed via Cochran's Q statistic and I2 test. A fixed-effect model was applied for low heterogeneity (Q test p > 0.05 or I2 < 50%), while a random-effect model was used for significant heterogeneity (Q test p < 0.05 or I2 > 50%). Only a very small number of crossover trials were identified, and most did not report paired data; therefore, analyses were performed using unpaired estimates, consistent with previous meta-analyses on similar topics. Subgroup analyses explored potential sources of heterogeneity. This study used fixed-effect models for analyses based on specific scales, while random-effect models were applied otherwise. Random-effect models, which assign more weight to smaller studies, often produce conservative results. Statistical analyses were performed with RevMan 5.2 (Cochrane Collaboration, Oxford, UK), ensuring consistency and accounting for variability across studies.
For studies not reporting standard deviations, we first derived SDs from the reported standard errors or 95% confidence intervals according to the Cochrane Handbook for Systematic Reviews of Interventions (Chandler et al., 2019). If neither standard errors nor confidence intervals were available, we estimated SDs from the range following Wan et al. (Wan et al., 2014). If SDs remained unavailable, we contacted the corresponding authors to request the original data.
To evaluate potential publication bias for PAS as the primary endpoint, we constructed an enhanced funnel plot using Duval & Tweedie's trim-and-fill method, iteratively estimating and imputing potentially missing studies. We judged bias by whether the imputed studies fell within the region of statistical significance and by the overall plot symmetry. Concurrently, we quantitatively assessed funnel-plot asymmetry using a regression-based Egger's intercept test and Kendall's rank correlation Begg's test.
Results
Outcomes of the Literature Search and Selection Process
A total of 529 articles were identified across three databases. After removing 122 duplicates, the remaining articles were screened by title, abstract, and full-text review, including 14 eligible studies. The detailed process is illustrated in Figure 1.
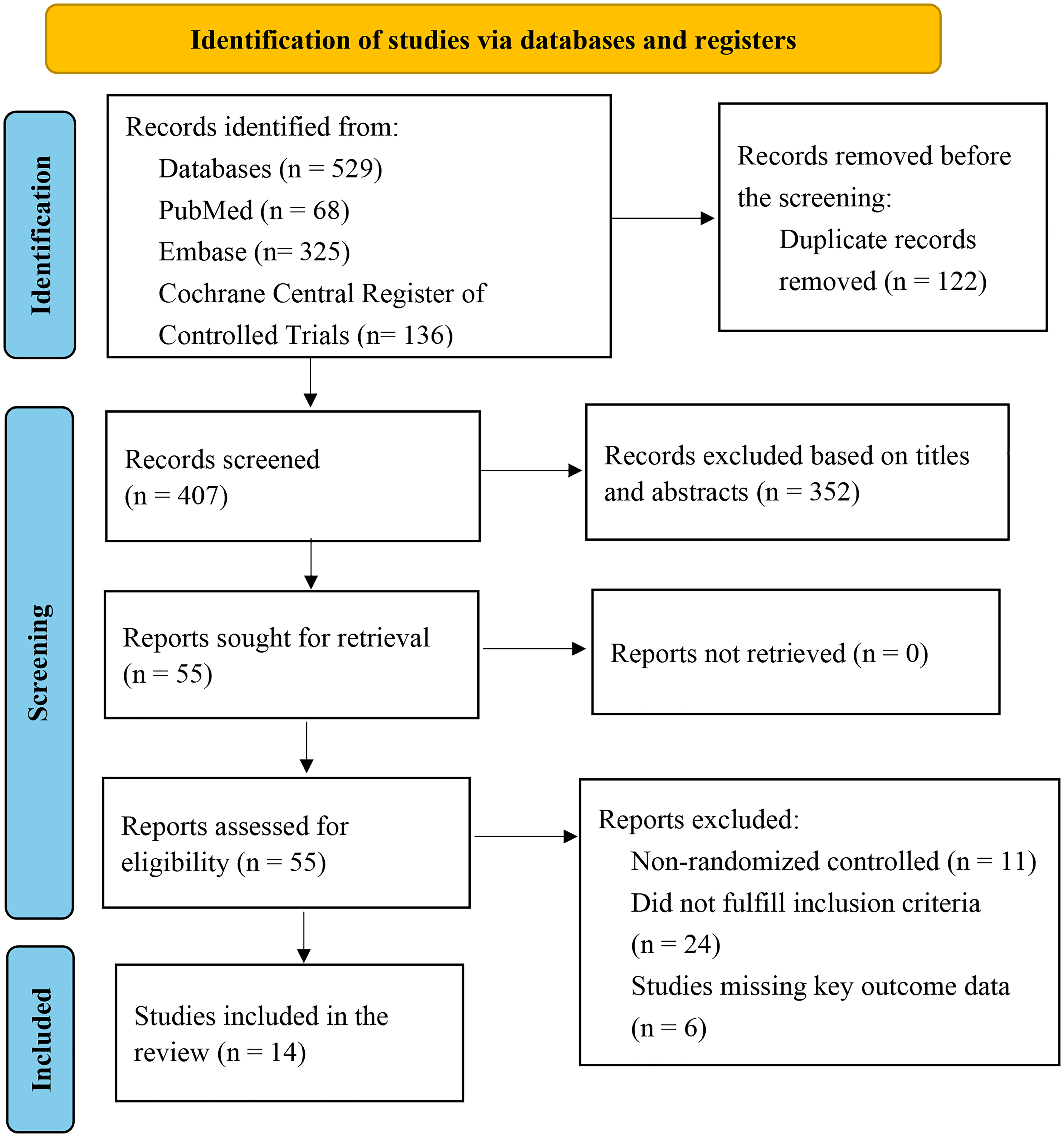
Flow Diagram of Study Selection Process.
Included Study Characteristics
This study included 14 RCTs with a total of 882 participants, published between 2011 and 2023. Of these, 9 studies were conducted in China (Dai et al., 2023; Dong et al., 2022; Du et al., 2016; Liu et al., 2022; Rao et al., 2022; Tai et al., 2023; Wen et al., 2023; Xie et al., 2022; Zhong et al., 2021), 4 in South Korea (Kim et al., 2011; Lim et al., 2014; Park et al., 2013; Park et al., 2017), and 1 in Turkey (Ünlüer et al., 2019). The experimental groups included 444 patients who received rTMS or TBS treatment, while the control groups included 438 patients who underwent conventional swallowing training or sham stimulation. Swallowing function was assessed using either the FEDSS or the Video-fluoroscopic Swallowing Study (VFSS).
In some studies, experimental groups were divided into two or more subgroups, and since there was no interference between these subgroups, they were treated as independent studies. For instance, 3 studies included unilateral and bilateral stimulation groups (Dai et al., 2023; Dong et al., 2022; Park et al., 2017), and 2 studies included low-frequency and high-frequency stimulation groups (Du et al., 2016; Lim et al., 2014). Additionally, 3 studies used TBS as the stimulation mode (Rao et al., 2022; Tai et al., 2023; Xie et al., 2022), while the rest applied rTMS. Regarding stimulation targets, 3 studies focused on the cerebellum, while others targeted the motor cortex M1 region associated with the suprahyoid muscles. In the control groups, 3 studies used conventional swallowing training alone, while the rest used sham stimulation. Sham stimulation involved positioning the coil perpendicular to the skull to block signal transmission while replicating the “clicking” sound, without providing therapeutic effects. Among the 14 included clinical trials, eight provided detailed information on their funding agencies and grant numbers; one explicitly stated it received no financial support, and five did not report any funding information. The characteristics of the included studies are summarized in Table 1.
Risk of Bias
We assessed the risk of bias for 14 RCTs using Cochrane's RoB 2 tool. Two reviewers independently evaluated Cochrane Collaboration guidelines, as shown in Figure 2. Overall, the risk of bias was low across most domains, except for some concerns related to participant data blinding.
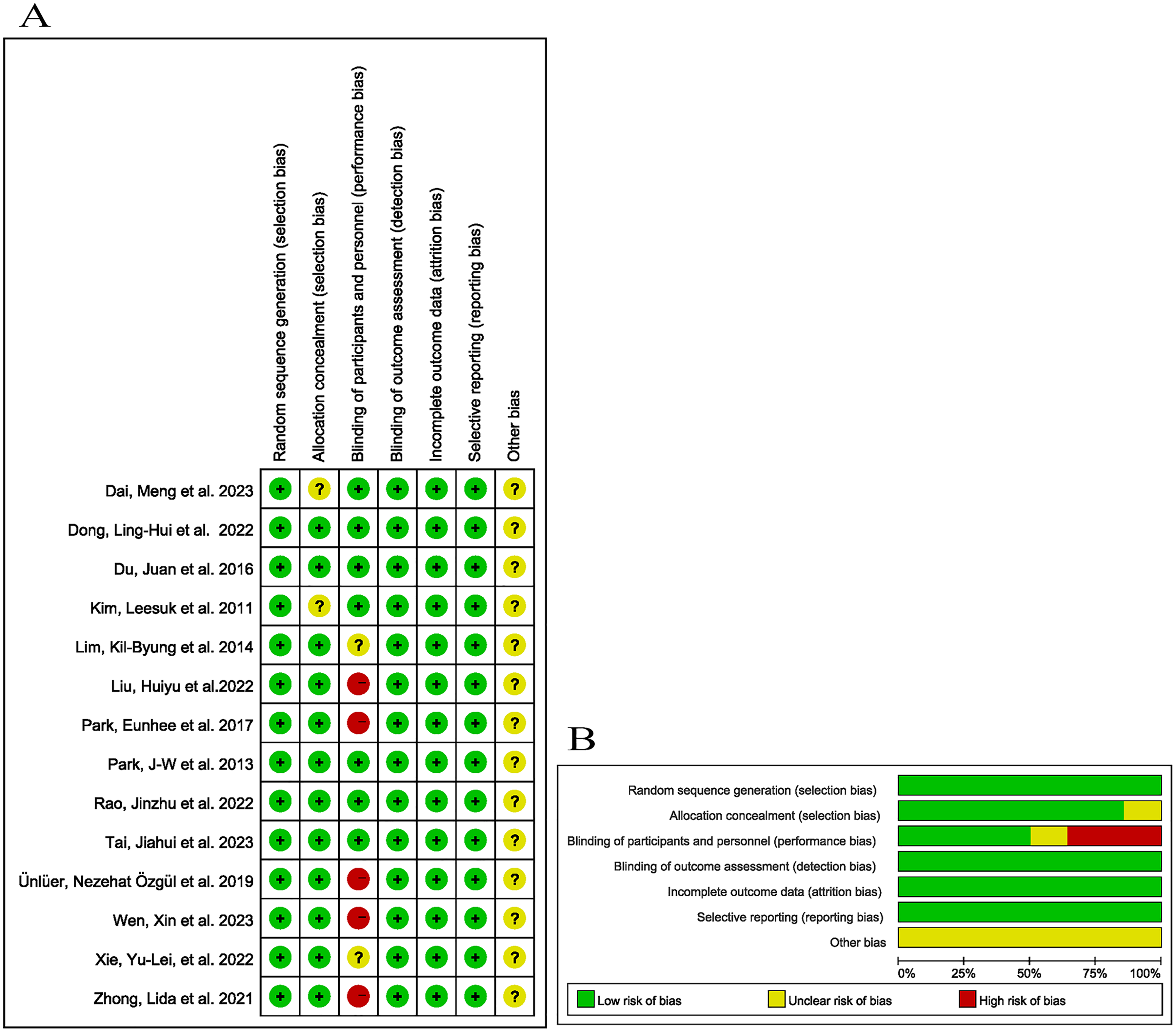
Summary and Deviation Chart for Risk of Bias Assessment. (A): Risk of bias summary. “+” means low-risk bias; “?” means unclear risk bias; “-” means high-risk bias; (B): Deviation chart for risk of bias.
Synthesis of Results
As shown in Figure 3, 14 studies reported PAS scores. Fixed-effect model analysis revealed that, at 1 week, three studies showed TMS significantly improved swallowing function in stroke patients (MD = −1.41, 95% CI: −2.17 to −0.65; I2 = 0.00%, P < 0.001). At 2 weeks, the improvement remained significant (MD = −1.06, 95% CI: −1.27 to −0.85; I2 = 56.77%, P < 0.001). At 4 weeks, the effects of TMS persisted, with further improvements in swallowing function (MD = −2.16, 95% CI: −2.54 to −1.77; I2 = 85.81%, P < 0.001). Overall, the meta-analysis confirmed that TMS treatment led to statistically significant improvements in swallowing dysfunction among stroke patients (MD = −1.32, 95% CI: −1.50 to −1.14; I2 = 76.92%, P < 0.001).
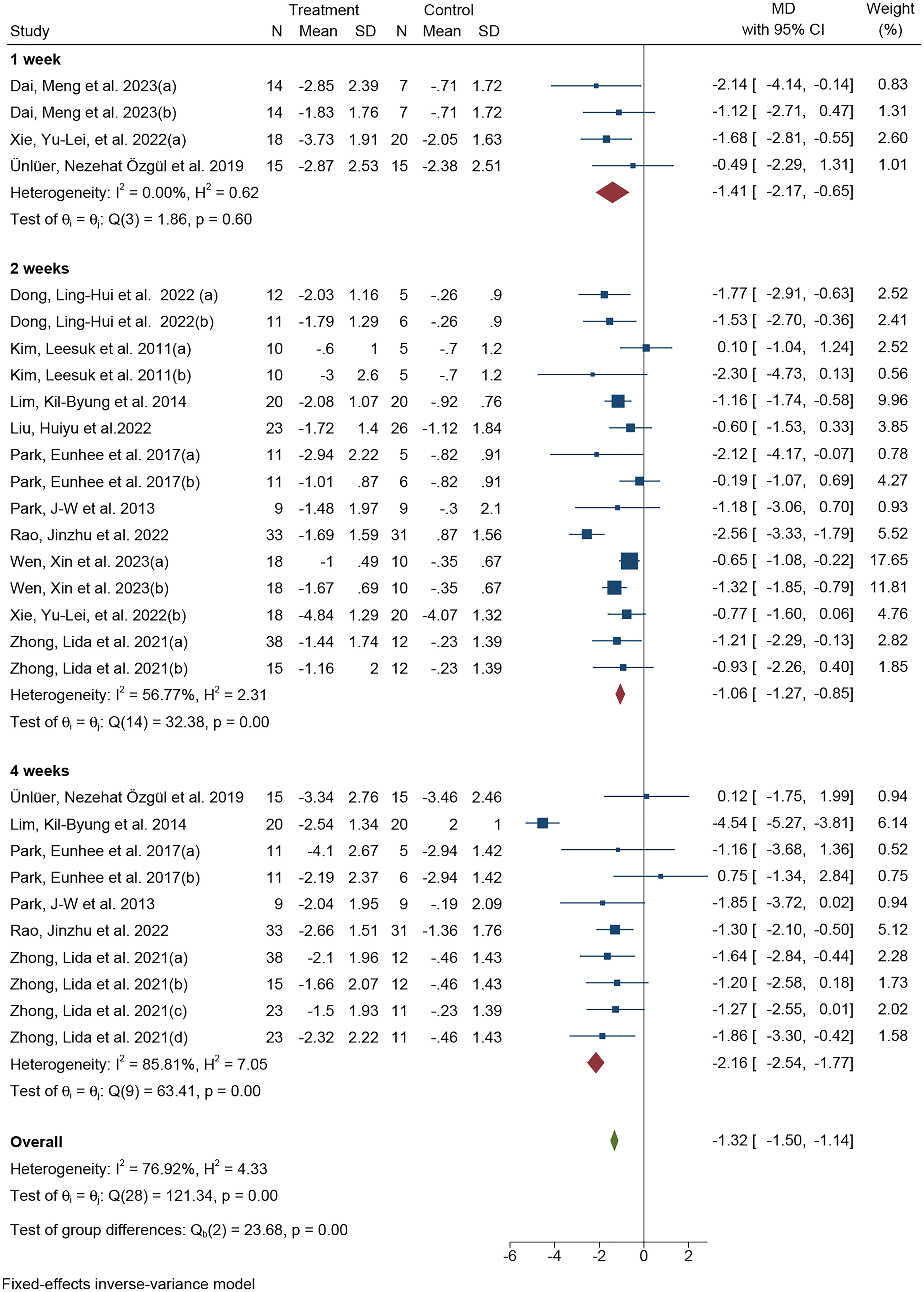
Forest Plot for PAS.
As shown in Figure 4, eight studies reported SSA scores. Fixed-effect model analysis indicated that five studies provided SSA scores at 2 weeks, showing significant improvement in swallowing function among stroke patients treated with TMS (MD = −1.74, 95% CI: −2.30 to −1.17; I2 = 0.00%, P < 0.001). At 4 weeks, the analysis demonstrated that TMS treatment continued to enhance swallowing function significantly (MD = −2.82, 95% CI: −3.71 to −1.94; I2 = 0.00%, P < 0.001). Overall, the meta-analysis confirmed that TMS resulted in statistically significant improvements in swallowing dysfunction among stroke patients (MD = −1.97, 95% CI: −2.43 to −1.50; I2 = 0.00%, P < 0.001).
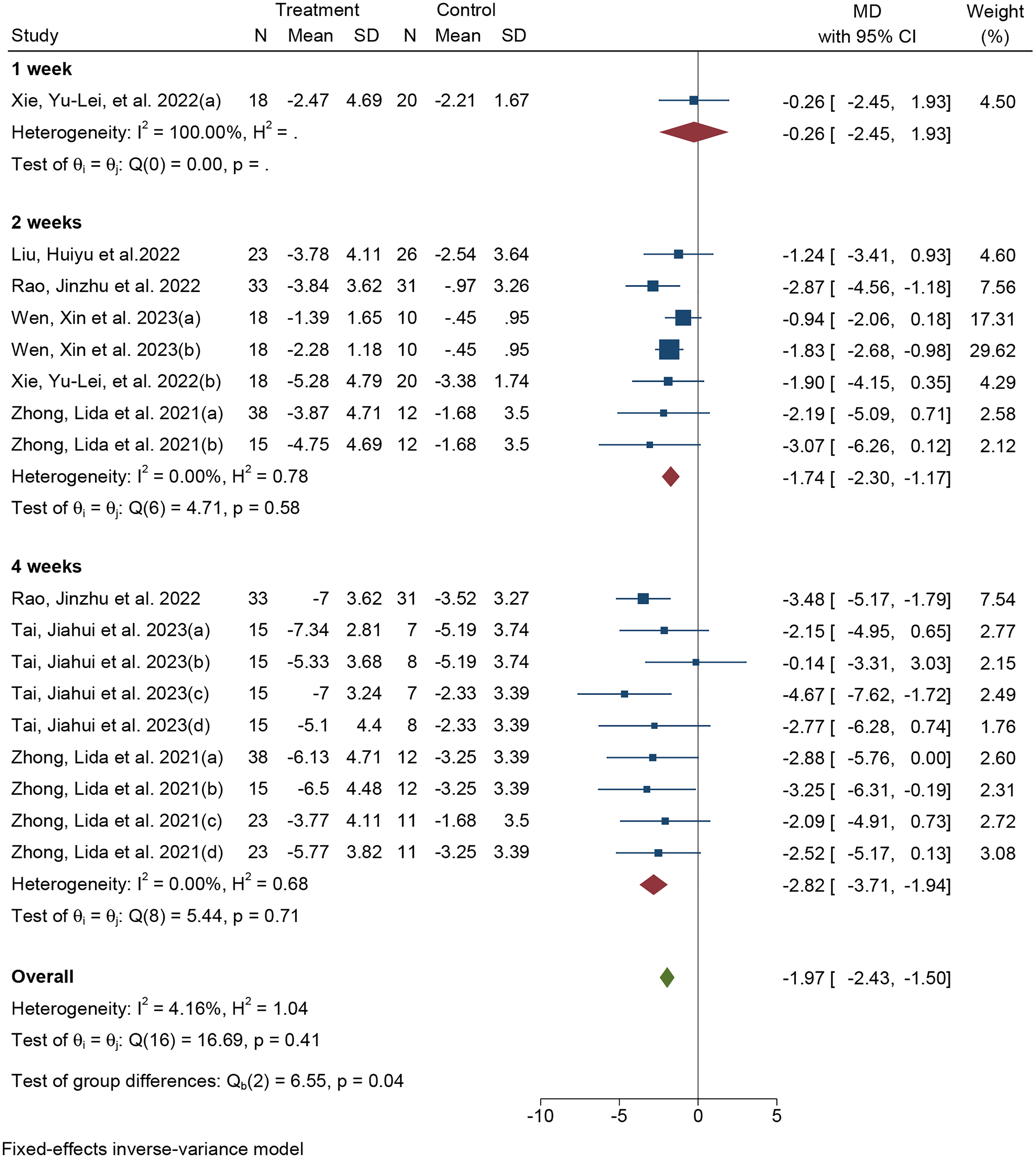
Forest Plot for SSA.
As shown in Figure 5, four studies reported FEDSS scores. Fixed-effect model analysis revealed that TMS significantly improved swallowing function in stroke patients at 2 weeks (MD = −0.64, 95% CI: −0.88 to −0.41; I2 = 4.93%, P < 0.001). At 4 weeks, the results indicated sustained improvement in swallowing function (MD = −0.67, 95% CI: −0.99 to −0.35; I2 = 0.00%, P < 0.001). The overall analysis further confirmed that TMS treatment led to statistically significant improvements in swallowing dysfunction in stroke patients (MD = −0.65, 95% CI: −0.84 to −0.46; I2 = 0.00%, P < 0.001).
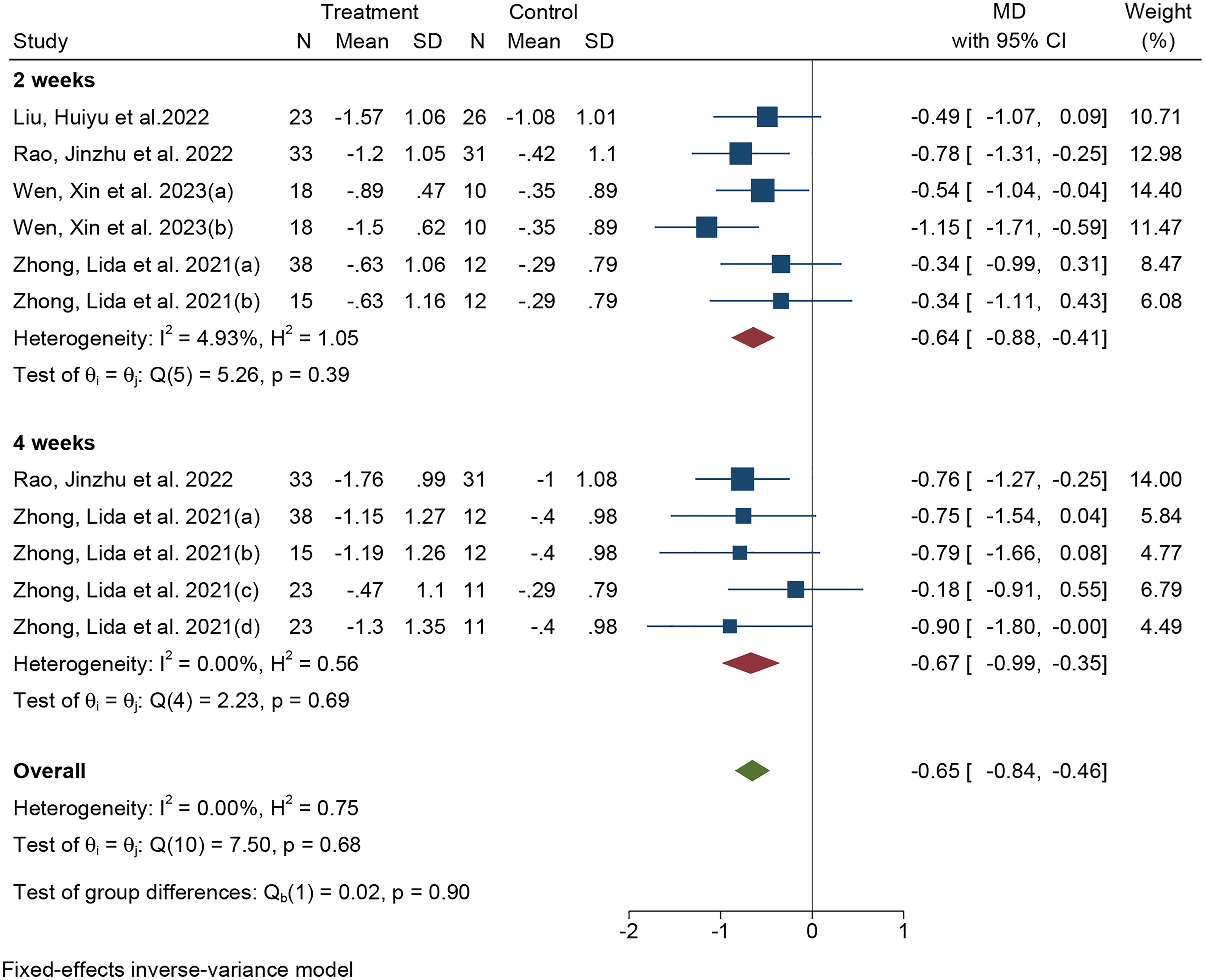
Forest Plot for FEDSS.
As shown in Figure 6, four studies reported results using the FOIS. A fixed-effect model analysis revealed that three studies provided FOIS scores at the 2-week mark, demonstrating significant improvement in swallowing function among stroke patients treated with TMS (MD = 0.96, 95% CI: 0.70 to 1.22; I2 = 24.52%, P < 0.001). Overall, the meta-analysis indicated that TMS treatment led to statistically significant improvements in swallowing function for stroke patients (MD = 0.92, 95% CI: 0.72 to 1.13; I2 = 25.88%, P < 0.001).
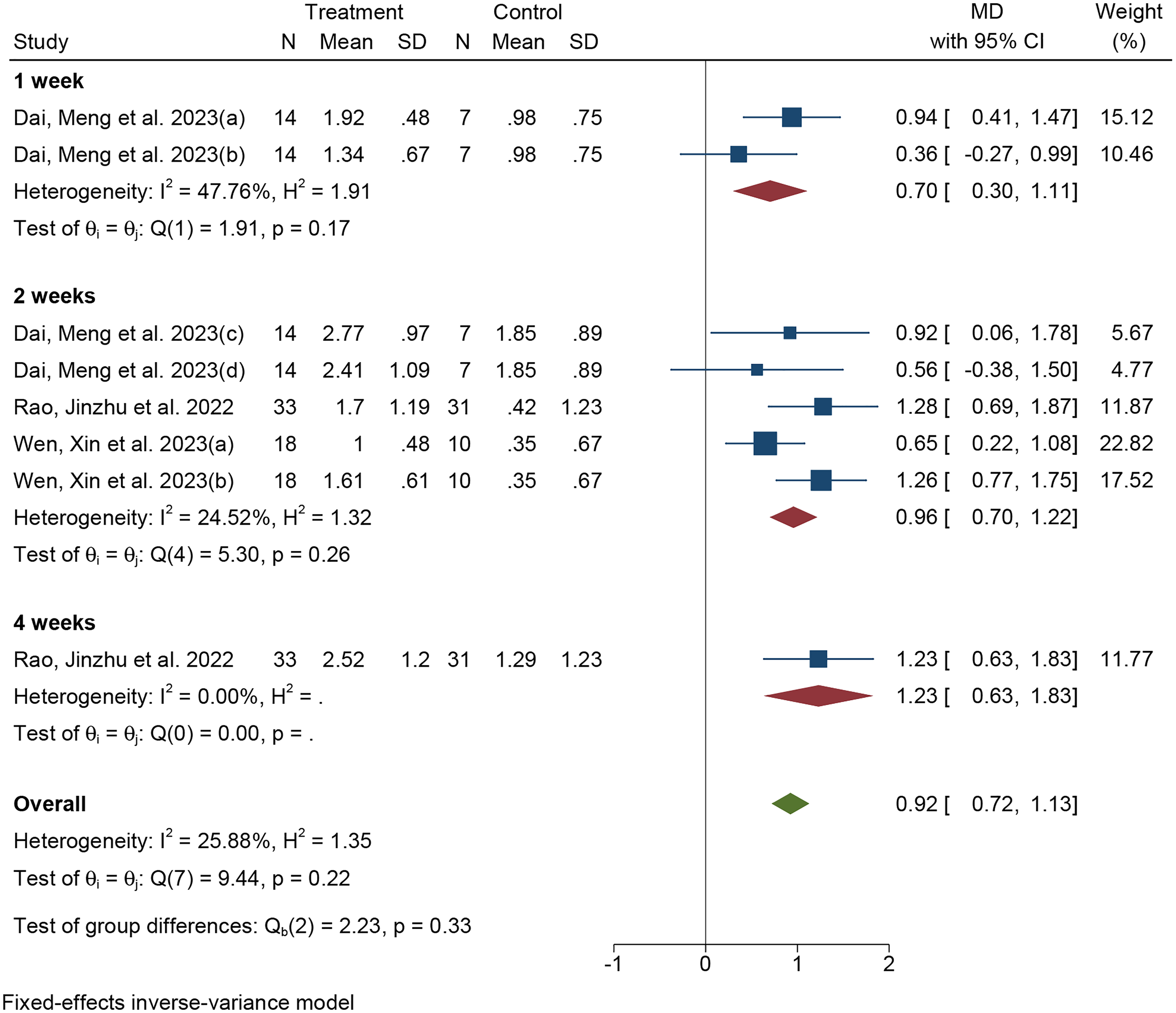
Forest Plot for FOIS.
As shown in Figure 7, four studies reported FDS scores. Fixed-effect model analysis revealed that three studies provided FDS data at 2 weeks after TMS treatment in stroke patients, showing significant improvement in swallowing function (MD = −5.65, 95% CI: −7.71 to −3.60; I2 = 56.39%, P < 0.001). Overall analysis further confirmed that TMS significantly improved swallowing dysfunction in stroke patients, with statistically significant results (MD = −5.54, 95% CI: −7.48 to −3.60; I2 = 46.14%, P < 0.001).
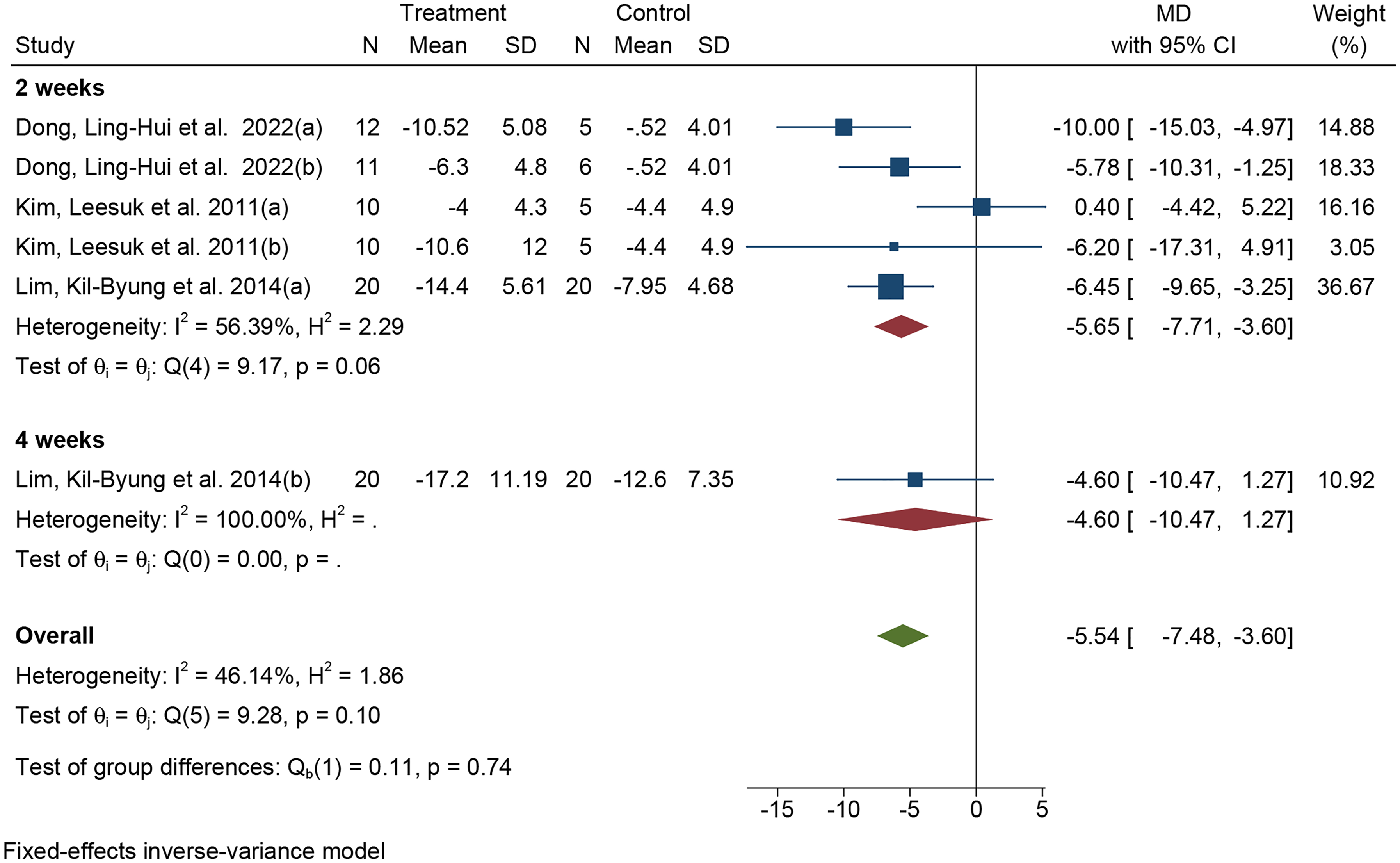
Forest Plot for FDS.
Subgroup Analysis
To explore the effects of different TMS stimulation modes, targets, frequencies, unilateral versus bilateral stimulation, and total treatment duration (≤2 weeks vs. > 2 weeks) on swallowing function in stroke patients, we conducted a subgroup analysis based on these parameters, integrating data from five assessment scales. The results showed that, compared to the control group, both unilateral stimulation (SMD = −0.75, 95% CI: −0.90 to −0.59; I2 = 50.52%, P < 0.001) and bilateral stimulation (SMD = −0.61, 95% CI: −1.19 to −0.04; I2 = 70.31%, P = 0.04) significantly improved swallowing function, with both showing superior outcomes over the control group. Subgroup analysis based on stimulation modes indicated that both rTMS (SMD = −0.70, 95% CI: −0.88 to −0.53; I2 = 56.75%, P < 0.001) and TBS (SMD = −0.81, 95% CI: −0.99 to −0.62; I2 = 30.65%, P < 0.001) led to significant improvements in swallowing function. Analysis by stimulation targets further demonstrated that both cerebellar stimulation (SMD = −0.67, 95% CI: −1.01 to −0.32; I2 = 62.17%, P < 0.001) and non-cerebellar stimulation (SMD = −0.73, 95% CI: −0.90 to −0.56; I2 = 54.50%, P < 0.001) significantly improved swallowing function. Analysis by treatment duration further demonstrated that both protocols ≤2 weeks (SMD = –0.76, 95% CI −0.91 to −0.60; I2 = 46.7%; P < 0.001) and protocols >2 weeks (SMD = –0.36, 95% CI −0.63 to −0.08; I2 = 32.3%; P = 0.01) significantly improved swallowing function. More detailed results are presented in Table 2.
Subgroup Meta-Analysis and Sensitivity Analysis of the Transcranial Magnetic Stimulation for Improving Post-Stroke Dysphagia.
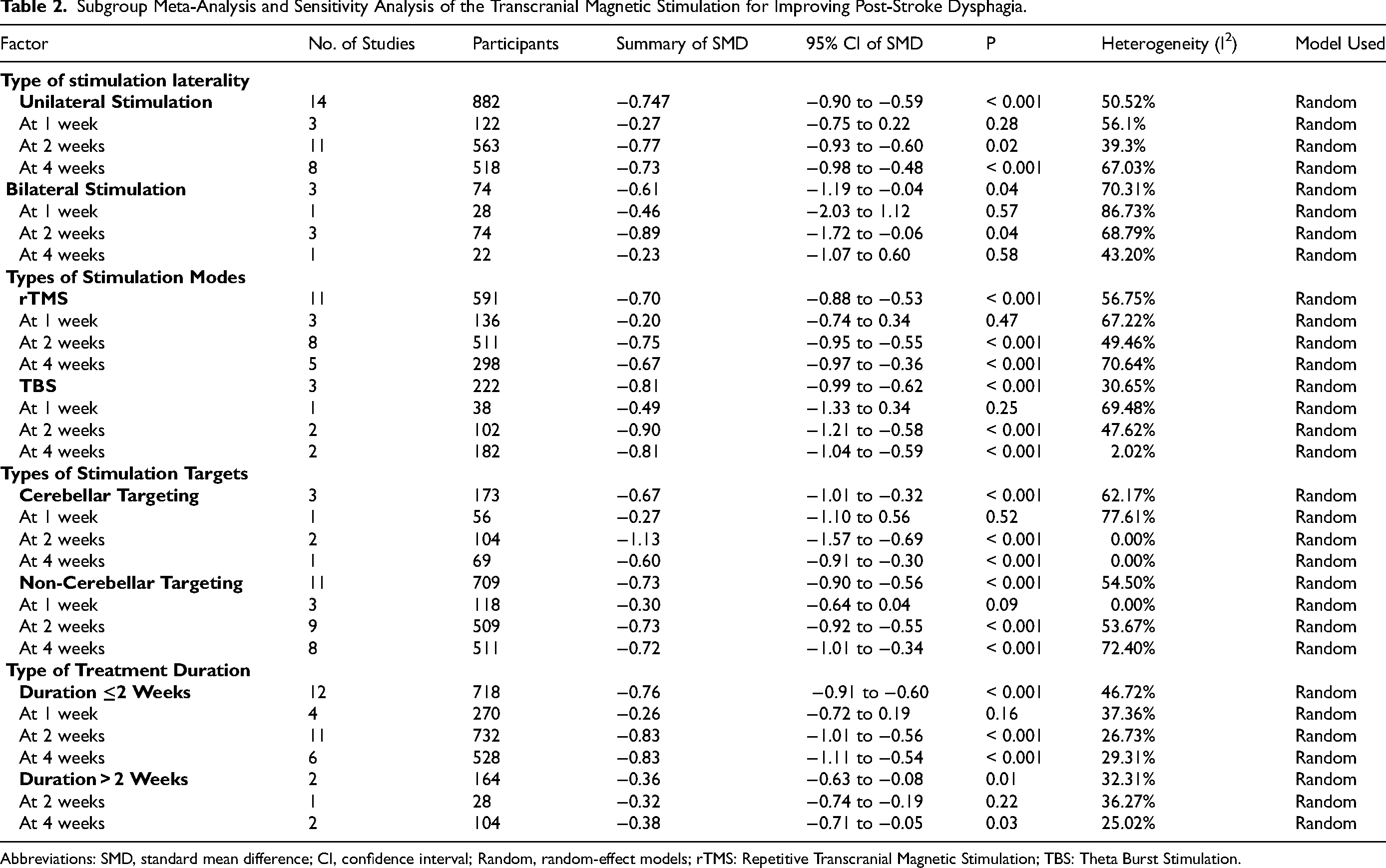
Abbreviations: SMD, standard mean difference; CI, confidence interval; Random, random-effect models; rTMS: Repetitive Transcranial Magnetic Stimulation; TBS: Theta Burst Stimulation.
Sensitivity Analysis and Publication Bias
In the enhanced funnel plot (Supplementary Figure 1), the two studies imputed by the trim-and-fill method both lie within the zone of statistical significance, indicating that no publication bias is present and that any apparent asymmetry is likely attributable to other factors. Neither Egger's regression (β₁ = –0.05, P = 0.913) nor Begg's test (Kendall's score = –38.00, P = 1.535) detected significant small-study effects.
GRADE Evaluation of Evidence
Table 3 presents the GRADE ratings and summary information; detailed data are available in the supplementary Raw data file. The overall certainty for the primary outcomes was moderate, downgraded primarily due to small sample sizes and inter-study heterogeneity.
Summary of Primary Outcomes with GRADE Evidence Assessment.
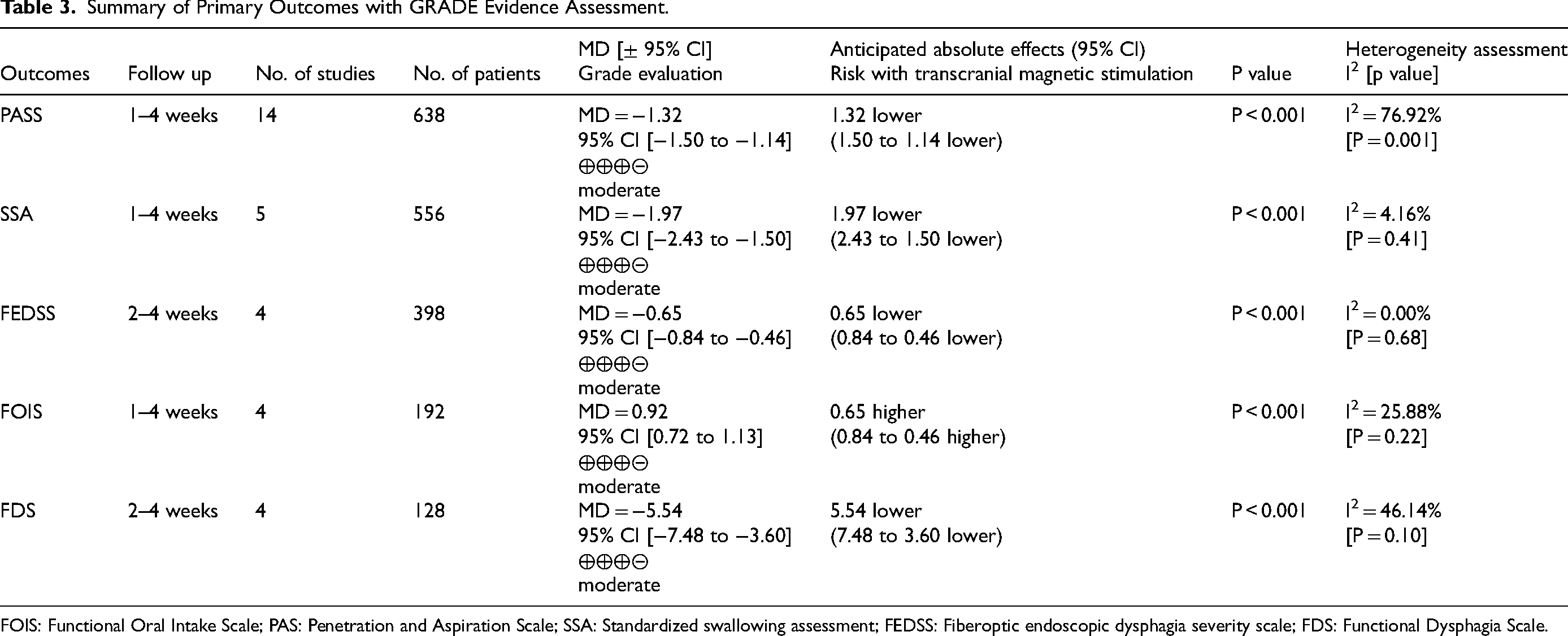
FOIS: Functional Oral Intake Scale; PAS: Penetration and Aspiration Scale; SSA: Standardized swallowing assessment; FEDSS: Fiberoptic endoscopic dysphagia severity scale; FDS: Functional Dysphagia Scale.
Discussion
This meta-analysis systematically evaluated the effectiveness of TMS in improving swallowing function in patients with stroke. The results showed significant improvements across multiple outcome measures, including PAS, SSA, FEDSS, FOIS, and FDS. Scores at different time points indicated a trend toward greater improvements by the fourth week, suggesting stable short-term treatment effects and notable relief of swallowing dysfunction. Subgroup analysis further explored the impact of different stimulation modes (repetitive TMS [rTMS] and theta burst stimulation [TBS]), targets (cerebellar and non-cerebellar), frequencies, and unilateral versus bilateral stimulation. Across all subgroup categories, TMS consistently demonstrated significant therapeutic benefits. Sensitivity analysis and publication bias assessments confirmed the stability and reliability of the findings, with no evidence of substantial publication bias. However, since most of the included studies were conducted in Asian patient populations, caution is warranted when generalizing these findings to non-Asian stroke patients. These results support TMS as an effective intervention for post-stroke dysphagia and provide valuable insights for optimizing stimulation parameters.
The recovery of swallowing function after a stroke is complex, involving various brain regions such as the primary sensorimotor cortex, insula, cingulate gyrus, prefrontal cortex, temporal lobe, and occipital area (Mihai et al., 2014). Damage to the corticobulbar tract, medullary reticular formation, or cranial nerve nuclei can impair the swallowing muscles, leading to dysfunction. The corticomedullary tract, a crucial connection between the brainstem and the swallowing cortex, has been linked to improved swallowing safety when its excitability increases (Wilmskoetter et al., 2020). The swallowing system is bilaterally innervated but asymmetrical, and reorganization of the contralateral pharyngeal cortex is essential for recovery.
Subgroup analysis based on different stimulation targets showed that both cerebellar and non-cerebellar stimulation significantly improved swallowing function compared to the control group, with no significant difference in efficacy between the two. The observed equivalence between cerebellar and non-cerebellar targets (p > 0.05) expands therapeutic options, suggesting flexibility in target selection (Qiao et al., 2022). The mylohyoid cortical region and cerebellum were the most frequently targeted areas, with the mylohyoid cortical area considered particularly effective due to its higher electromyographic response amplitude (Gallas et al., 2007). A meta-analysis and systematic review on cerebellar rTMS for post-stroke dysphagia found that combining cerebellar rTMS with traditional swallowing exercises offers greater improvement in swallowing function than using exercises alone (Liu et al., 2024). This highlights the importance of selecting the appropriate stimulation mode, with cerebellar TMS showing significant potential in post-stroke swallowing recovery. However, there is limited research directly comparing different targets, leaving the optimal stimulation site undetermined. Studies targeting the cerebellum and vagus nerve near the mastoid process have also shown potential, highlighting the flexibility of TMS in addressing multiple targets (Lin et al., 2018; Neren et al., 2016; Rao et al., 2022). Different stimulation strategies may improve swallowing through distinct mechanisms. Unilateral cortical stimulation is often based on the interhemispheric inhibition model, which suggests that after brain injury, the unaffected hemisphere overly inhibits the damaged hemisphere, causing dysfunction (Tarameshlu et al., 2019). Low-frequency rTMS can suppress the contralateral hemisphere, while high-frequency rTMS enhances excitability in the ipsilateral hemisphere, restoring balance and improving function (Liao et al., 2017; Lim et al., 2014). Notably, brief TMS courses (≤2 weeks) yielded larger, more consistent improvements in swallowing function, whereas extended regimens (>2 weeks), although still beneficial, produced smaller effects with greater variability. This likely reflects the rapid induction of neural plasticity by concentrated, high-frequency stimulation, while longer protocols, varying more in parameters and timing, lead to fluctuating outcomes. The unequal distribution of studies across duration groups may also influence these findings. Future trials should standardize stimulation parameters and systematically investigate the duration–response relationship to identify the optimal treatment length. Moreover, direct comparisons of different stimulation targets and personalized approaches are necessary to elucidate mechanisms and optimize TMS protocols for post-stroke dysphagia.
Subgroup analysis of unilateral and bilateral stimulation showed that, compared to the control group, TMS significantly improved swallowing function in stroke patients, regardless of whether unilateral or bilateral stimulation was used. However, the difference in efficacy between unilateral and bilateral stimulation was insignificant. Unilateral stimulation, targeting either the unaffected or affected hemisphere, showed similar improvements in swallowing function with 5Hz-rTMS, but no significant differences in outcomes (Michou et al., 2019; Zhang et al., 2020). While some studies suggest that bilateral stimulation may be more effective, this meta-analysis did not provide sufficient evidence to support this claim (Cai et al., 2019; Momosaki et al., 2014). Swallowing function is closely associated with the pharyngeal cortex in both hemispheres, which exhibits interhemispheric asymmetry. When the dominant hemisphere is damaged and the non-dominant hemisphere fails to compensate, swallowing dysfunction is more likely (Hamdy et al., 1996). Recovery may primarily depend on the unaffected hemisphere, while bilateral stimulation might enhance swallowing function by activating cortical networks on both sides (Wilmskoetter et al., 2018).
In the subgroup analysis of stimulation modes, we compared the effects of rTMS and TBS on swallowing function in stroke patients. The results showed that both rTMS and TBS significantly improved swallowing function, with no significant difference in their therapeutic effects. TBS, a newer treatment approach compared to rTMS, offers advantages such as shorter intervention time, lower stimulation intensity, and greater efficacy (Lin et al., 2017; Mistry et al., 2012). TBS includes two main protocols: intermittent TBS (iTBS) and continuous TBS (cTBS). Research indicates that iTBS enhances cortical excitability, while cTBS has an inhibitory effect on cortical excitability, giving iTBS a unique advantage in improving neurological function (Xie et al., 2022; Yu-Lei et al., 2022). Studies have shown that iTBS significantly improves swallowing function in both primary and secondary dysphagia, with effects still better than the sham stimulation group after 3 months (G. Cosentino et al., 2020; Jiang et al., 2015). This suggests that iTBS may provide long-lasting benefits, making it a promising treatment (Zhang et al., 2019). However, due to the limited number of studies in this research, we did not analyze its effects beyond 4 weeks. Research by Xie et al. also indicates that iTBS outperforms traditional 10 Hz rTMS in terms of efficacy, safety, and tolerance for improving swallowing in patients with upper brainstem stroke (Xie et al., 2022). Additionally, other studies suggest that iTBS may have advantages in treating cerebellar spasm-related dysphagia following a stroke (Bethoux & Sutliff, 2013; Rao et al., 2022). Cosentino et al. explored the impact of iTBS on dysphagia caused by conditions like stroke, Parkinson's disease, and aging, finding that it effectively improves swallowing function (Cosentino et al., 2022). Lin et al. found that iTBS enhances cortical excitability in the mylohyoid muscles of the ipsilateral hemisphere, activates the affected hemisphere, and helps restore balance between both hemispheres, leading to better swallowing function (Lin et al., 2017). From a clinical utility perspective, TBS requires only 3–10 min per session, substantially less than the 20–30 min needed for conventional rTMS, which can reduce staffing and facility costs and significantly increase patient throughput. According to the GRADE assessment, the certainty of evidence for the primary outcomes was moderate, indicating reasonable reliability but also highlighting the need for further confirmation due to limitations such as small sample sizes and heterogeneity. However, because conventional rTMS devices are more widely available in most healthcare settings, clinicians should balance time efficiency against equipment accessibility when selecting a protocol. Future studies should incorporate detailed cost and resource considerations to perform comprehensive economic evaluations and guide optimal treatment strategies across different contexts.
The strength of this study lies in the comprehensive literature search across multiple databases, ensuring a broad and diverse dataset. Additionally, standardized scales were used for evaluation, allowing for effective comparison and integration of results from different studies. This study also has some limitations. First, by pooling only studies that used the same assessment scales and applying a fixed-effect model, we may have underestimated between-study variability. Second, the relatively small sample sizes limit the robustness and generalizability of our findings. Third, most included trials were conducted in Asian patient populations, so the applicability of our results to non-Asian stroke patients remains uncertain. In addition, only a few crossover trials were included and analyzed with parallel-arm trials without adjustment for design differences, which may have introduced minor bias but is unlikely to have affected the overall conclusions. Future large-scale RCTs across diverse clinical settings, with standardized instruments and analyzed using random-effects models, are needed to confirm our findings, enhance external validity, and strengthen data reliability.
Conclusions
This meta-analysis confirms that both rTMS and TBS significantly improve swallowing in post-stroke dysphagia, unilaterally or bilaterally, and targeting cerebellar or cortical regions, with low heterogeneity across most outcome scales. However, the relatively short follow-up periods for functional assessments may limit insights into long-term efficacy, and heterogeneity observed in certain key subgroups (e.g., stimulation frequency and delivery mode) may affect generalizability; notably, improvements in swallowing safety were confirmed at 4-week follow-up, whereas oral function was only assessed up to 2 weeks post-treatment, limiting conclusions about its longer-term recovery. Large-scale, prospective trials with standardized protocols, extended follow-up durations, and more uniform subgroup criteria are needed to refine optimal clinical strategies.
Supplemental Material
sj-docx-1-nre-10.1177_10538135251382914 - Supplemental material for Comparative Effects of Repetitive Transcranial Magnetic Stimulation and Theta-Burst Stimulation on Post-Stroke Dysphagia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-nre-10.1177_10538135251382914 for Comparative Effects of Repetitive Transcranial Magnetic Stimulation and Theta-Burst Stimulation on Post-Stroke Dysphagia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials by Chunhua Liu, Jiayan Wang, Huajian Lin, Zegen Ye, Liqin Wang, Xilin Liu and Yongfei Zheng in NeuroRehabilitation
Supplemental Material
sj-xlsx-2-nre-10.1177_10538135251382914 - Supplemental material for Comparative Effects of Repetitive Transcranial Magnetic Stimulation and Theta-Burst Stimulation on Post-Stroke Dysphagia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Supplemental material, sj-xlsx-2-nre-10.1177_10538135251382914 for Comparative Effects of Repetitive Transcranial Magnetic Stimulation and Theta-Burst Stimulation on Post-Stroke Dysphagia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials by Chunhua Liu, Jiayan Wang, Huajian Lin, Zegen Ye, Liqin Wang, Xilin Liu and Yongfei Zheng in NeuroRehabilitation
Footnotes
Abbreviations
Acknowledgements
We thank Professor Zheng and Ye for their criticism and guidelines, and the participants in our study for their contributions.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Authors’ Contributions
C.L. and Y.Z. were responsible for the study design. The manuscript was drafted by C.L. The search strategies were developed by C.L. and J.W., while C.L., J.W., and Z.Y. collected the data. Data analysis was performed by C.L., L.W., J.W., and H.L. contributed to data interpretation. Y.Z. reviewed and revised the manuscript. All authors have read and approved the final version of the manuscript.
Funding
Zhejiang Provincial Traditional Chinese Medicine Science and Technology Program under the category of the Traditional Chinese Medicine Heritage and Innovation Talent Support Program, (grant number No. 2024ZR202).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The included studies and extracted data have been uploaded in the Raw Data file for review and verification. For additional information, please contact the authors.
Clinical Trial Number
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.