
Abstract
Background
Hydrocephalus is a potentially serious complication of stroke that can lead to long-term neurological impairment. However, population-based evidence on its incidence and time-varying risk remains limited.
Methods
A retrospective cohort study was conducted using data from the Korean National Health Insurance Service–National Sample Cohort (2002–2013), including 16,514 patients newly diagnosed with hemorrhagic and ischemic stroke and 82,570 propensity score-matched controls. Stroke and hydrocephalus were defined based on codes set forth by the International Classification of Diseases, 10th Edition. Time-stratified Cox regression was applied owing to the violation of the assumption for proportional hazards.
Results
During a mean follow-up of 4.3 years, the incidence rate of hydrocephalus was 1.82 per 1,000 person-years in the stroke cohort, versus 0.11 in the controls (IRR, 17.11; 95% CI, 11.89–24.62). The adjusted hazard ratio (aHR) was highest within three years post-stroke (aHR, 29.53), declining over time but remaining elevated up to nine years. Patients with hemorrhagic stroke had a markedly higher early risk (aHR, 54.93), whereas those with ischemic stroke showed a delayed, biphasic risk pattern. Female and younger patients had higher relative risks despite lower absolute incidence. Risk was also elevated in association with smoking, alcohol use, high cholesterol, abnormal BMI, and higher income levels.
Conclusion
Stroke significantly increases the long-term risk of hydrocephalus, with distinct temporal patterns by stroke subtype. These findings emphasize the need for prolonged monitoring and individualized preventive strategies, especially for high-risk subgroups. Further research is warranted to refine risk prediction and guide post-stroke management.
Introduction
Stroke is a clinical syndrome characterized by sudden damage to brain tissue owing to either vascular occlusion (ischemic stroke) or rupture (hemorrhagic stroke), with symptoms persisting for more than 24 h or resulting in early death (Sacco et al., 2013). Both ischemic and hemorrhagic strokes can lead to acute brain injury, often causing severe neurological deficits or death. Long-term rehabilitation and ongoing medical care are required, significantly impairing quality of life and imposing substantial social and economic burdens (Lung & Institute; Naghavi et al., 2017). Among the various complications of stroke, hydrocephalus is relatively common and represents a significant clinical issue that can profoundly affect patient outcomes (Chen et al., 2017b; Graff-Radford et al., 1989).
Hydrocephalus is a condition characterized by the pathological accumulation of cerebrospinal fluid (CSF) in the ventricles and cranial cavity owing to an imbalance between CSF production and absorption or an obstruction in CSF circulation, leading to increased intracranial pressure and subsequent neurological dysfunction (Rekate, 2009). Starting with neurological impairment, hydrocephalus can lead to long-term functional decline (Koleva & De Jesus, 2022), frequent hospital readmissions (LeHanka & Piatt), and ongoing neurosurgical interventions (Dasher et al., 2024), collectively imposing a substantial burden on patients, their families, and the broader health care system (Koschnitzky et al., 2022).
In patients with stroke, the development of hydrocephalus may lead to secondary brain injury and neurological deterioration owing to elevated intracranial pressure, potentially delaying recovery and worsening long-term outcomes (Graff-Radford et al., 1989; Rekate, 2009). Early diagnosis and appropriate management to restore normal CSF circulation can mitigate these adverse effects and improve both survival and functional prognosis (Hamilton, 2009). However, large-scale studies investigating the incidence and risk factors of post-stroke hydrocephalus remain limited, posing challenges in the accurate identification of high-risk populations and implementation of timely interventions in clinical practice.
Previous studies on hydrocephalus following stroke have often focused on specific subpopulations, such as patients with aneurysmal subarachnoid hemorrhage (aSAH) or those undergoing decompressive craniectomy for malignant ischemic stroke. Most of these studies have been conducted in single centers with small sample sizes, limiting the generalizability of their findings to the broader population of patients who experienced stroke (Ovenden et al., 2023). For instance, hydrocephalus has been reported in approximately 10–20% of patients with intracerebral hemorrhage (Cai et al., 2022), whereas its incidence in aSAH varies widely, ranging from 6% to as high as 67% (Chen et al., 2024). These discrepancies are likely attributable to differences in study populations, follow-up durations, and diagnostic criteria. Furthermore, the lack of large-scale cohort studies that comprehensively include all stroke types hinders the accurate estimation of hydrocephalus incidence and its clinical implications in the overall population of patients with stroke.
Therefore, the present study aimed to analyze the incidence and time-specific risk of hydrocephalus over a period of up to 10 years in patients newly diagnosed with stroke, using a nationwide cohort dataset from the Korean National Health Insurance Service. By providing large-scale epidemiological evidence across a broad patient population, this study seeks to support early prediction and management of hydrocephalus following stroke.
Method
Data Sources and Study Population
This study utilized data from the National Sample Cohort 2002–2013, derived from the National Health Information Database established by the Korean National Health Insurance Service. The cohort comprises a representative sample of approximately one million individuals, accounting for about 2.2% of the Korean population as of 2002 (Lee et al., 2017). The dataset includes all medical utilization records, diagnostic codes, and health screening information collected from January 2002 to December 2013. South Korea operates a mandatory national health insurance system that covers approximately 98% of the population (Shin et al., 2016). Health care providers are required to submit diagnostic codes based on the International Classification of Diseases, 10th Edition (ICD-10), for reimbursement. In addition, enrollees are eligible for periodic health examinations every one to two years, depending on age, sex, and health risk factors.
The study was exempted from ethical review by the institutional review board of [blinded for review]. As the data provided by the National Health Insurance Service had been anonymized to prevent identification of individual participants, the requirement for informed consent was waived.
Case and Control Group Selection
The stroke cohort was defined as individuals who received at least one primary or secondary diagnosis of stroke during the observation period, based on ICD-10 codes I60, I61, I62, and I63. Hemorrhagic stroke was identified using codes I60, I61, and I62, whereas ischemic stroke was classified under code I63 (Table 1). The date of the first stroke diagnosis was set as the index date. To exclude individuals with preexisting stroke or conditions potentially associated with hydrocephalus—such as neurodevelopmental disorders, traumatic brain injury, prior stroke, encephalitis, autoimmune diseases, infections, dementia-related conditions, cancer, or metastatic brain tumors—we applied a three-year washout period from 2002 to 2004. The study excluded individuals diagnosed with stroke during this period. Additional exclusion criteria included the following: (1) absence of health screening records within three years prior to the index date, (2) age of under 20 or over 80 years at the index date, and (3) a diagnosis of hydrocephalus within three years prior to the index date.
Codes for Diseases in the International Classification of Diseases, 10th Revision (ICD-10).
The control group was selected from individuals who were not diagnosed with stroke during the observation period, after applying the same exclusion criteria used for the stroke cohort. Controls were matched to stroke cases using 1:5 propensity score matching based on sex, age, and year of health examination. The propensity score model included the following variables: smoking status, alcohol consumption, body mass index (BMI), total cholesterol, systolic and diastolic blood pressure, fasting blood sugar, and income level. For individuals with missing values in any of these variables, single imputation was performed using predictive mean matching. The index date for controls was assigned to match that of the corresponding stroke cases. The selection process for both stroke cases and matched controls is illustrated in Figure 1.
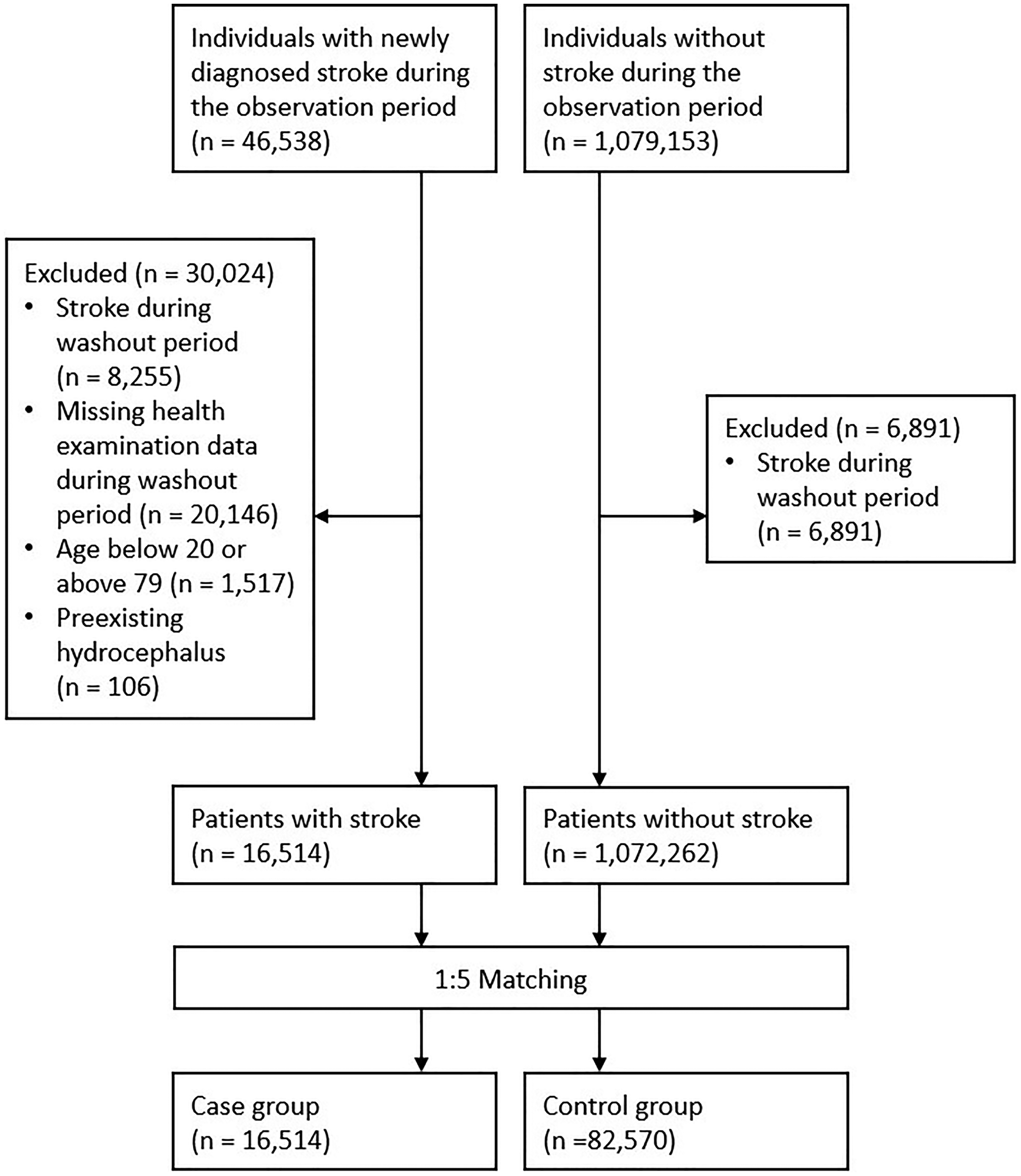
Flowchart for Stroke Case and Control Group Selection.
In total, the study included 16,514 individuals in the stroke cohort and 82,570 propensity score-matched controls. The total person-years of follow-up were 67,002.74 for the stroke cohort and 357,005.96 for the control group. The mean follow-up duration was 4.33 years (SD, 2.55) for the stroke group and 4.06 years (SD, 2.61) for the control group.
Primary Outcome
The primary outcome of this study was the development of new-onset hydrocephalus. To ensure diagnostic accuracy, we defined hydrocephalus as having received an ICD-10 code of G91 as either a primary or secondary diagnosis on at least two separate occasions (Table 1). The date of the second recorded diagnosis was set as the date of hydrocephalus diagnosis.
Variables
The variables included in the analysis were sex, age, smoking status, alcohol consumption, height, weight, BMI, total cholesterol, systolic blood pressure, diastolic blood pressure, fasting blood glucose, and income level. Information recorded closest to the date of the health examination was used. Height and weight were treated as continuous variables; all other variables were considered categorical.
Statistical Analysis
To compare the baseline characteristics between the stroke and control groups, we used student's t-test for continuous variables and Fisher's exact test or Pearson's chi-squared (χ²) test for categorical variables. Standardized differences were also calculated, with values less than 0.1 interpreted as negligible. To compare the incidence of hydrocephalus between the stroke and control groups, we calculated crude incidence rates (IRs) per 1,000 person-years and incidence rate ratios (IRRs). We used the Kaplan–Meier survival analysis and log-rank test to assess the cumulative incidence of hydrocephalus over time. Follow-up ended upon the diagnosis of hydrocephalus, death, or end of the study period (December 31, 2013), whichever occurred first. To evaluate the association between stroke and the risk of hydrocephalus, we used a multivariable Cox proportional hazards regression model. Because the proportional hazards assumption was violated based on Schoenfeld residuals, we applied an extended time-stratified Cox regression model by dividing the nine-year follow-up period into three-year intervals. Covariates included in the model were sex, age, smoking status, alcohol consumption, BMI, total cholesterol, and income level. Additionally, subgroup analyses were conducted based on the type of stroke. All analyses were conducted using R version 4.4.1. Two-sided tests were used, and statistical significance was set at p < 0.05.
Results
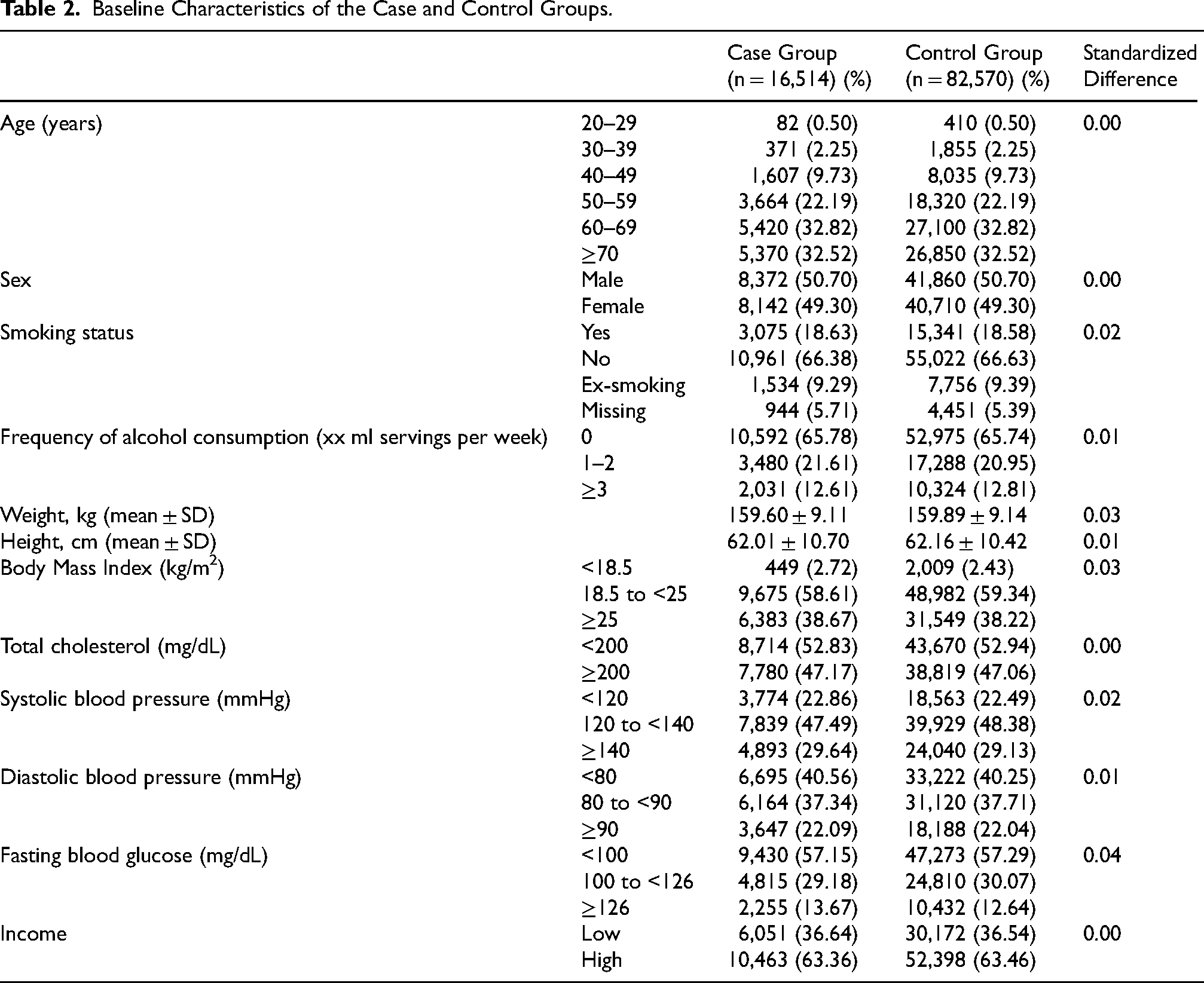
As shown in Table 2, all standardized differences in the baseline characteristics between the cohort and control groups were below 0.1, indicating negligible imbalance between the groups. Table 3 presents the crude IRs and IRRs of hydrocephalus in the stroke and control groups. During the follow-up period, hydrocephalus was diagnosed in 122 individuals (0.74%) in the stroke cohort and 38 individuals (0.05%) in the control group. The IR per 1,000 person-years was 1.82 (95% CI, 1.51–2.15) in the stroke cohort and 0.11 (95% CI, 0.07–0.14) in the control group. The IRR comparing the stroke cohort to the control group was 17.11 (95% CI, 11.89–24.62).
Baseline Characteristics of the Case and Control Groups.
Crude Incidence Rates and Risk Ratios for Hydrocephalus among Patients Diagnosed with Stroke and Matched Controls.
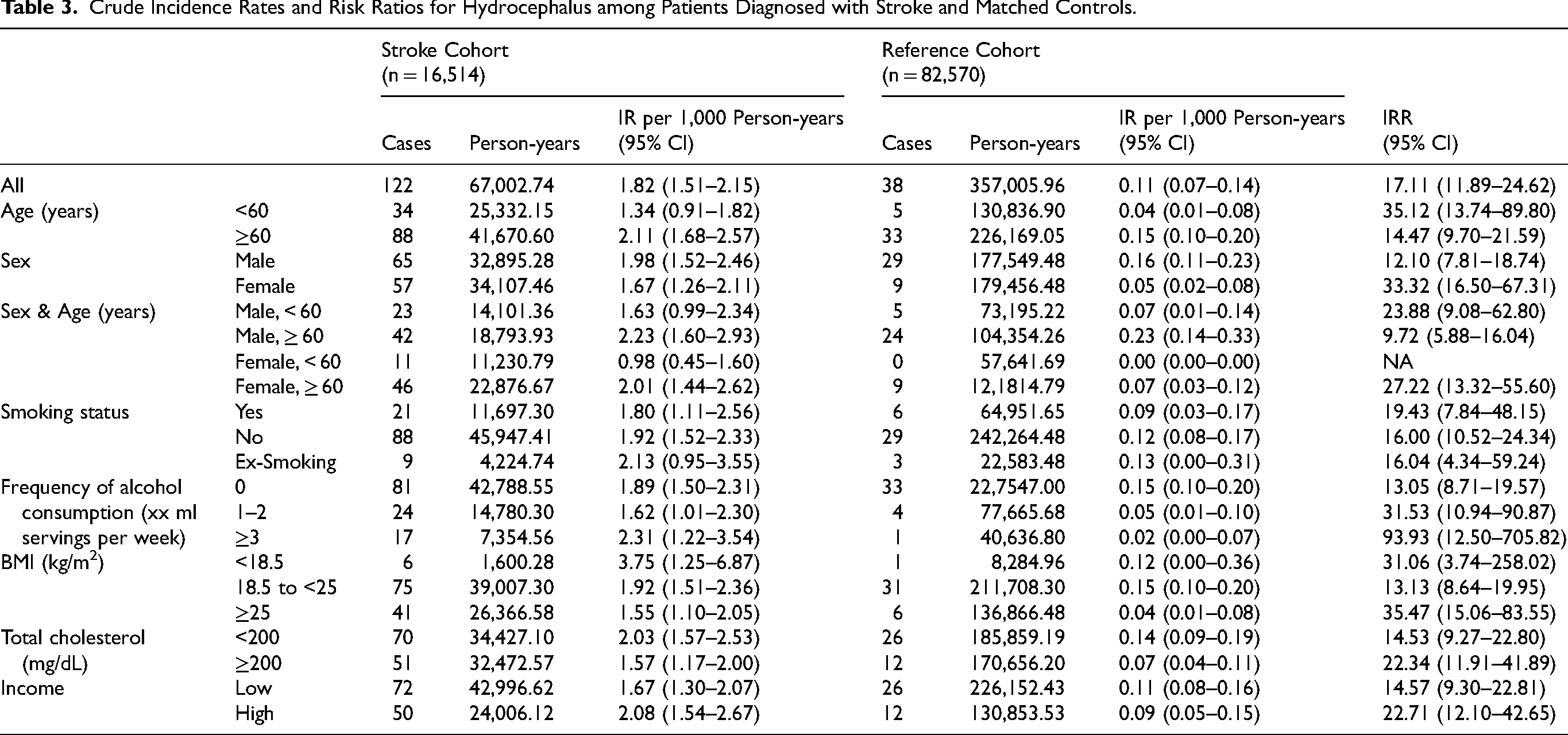
In the age-stratified analysis, patients diagnosed with stroke under the age of 60 years showed a lower IR of hydrocephalus compared with those aged 60 years and above (1.34 [95% CI, 0.91–1.82] vs. 2.11 [95% CI, 1.68–2.57] per 1,000 person-years), but a higher IRR when compared with their respective control groups (35.12 [95% CI, 13.74–89.80] vs. 14.47 [95% CI, 9.70–21.59]). We observed a similar pattern in the sex-stratified analysis. Male stroke patients had a higher IR of hydrocephalus compared with female patients (1.98 [95% CI, 1.52–2.46] vs. 1.67 [95% CI, 1.26–2.11] per 1,000 person-years), whereas men had a lower IRR compared with women (12.10 [95% CI, 7.81–18.74] vs. 33.32 [95% CI, 16.50–67.31]).
Additional analyses were conducted based on smoking status, alcohol consumption, BMI, total cholesterol levels, and income level. Current smokers showed a higher IRR for hydrocephalus (19.43 [95% CI, 7.84–48.15]) compared with non-smokers (16.00 [95% CI, 10.52–24.34]) and former smokers (16.04 [95% CI, 4.34–59.24]); however, these differences were not statistically significant. Regarding alcohol consumption, the IRR increased with the frequency of weekly alcohol intake: 13.05 (95% CI, 8.71–19.57) for zero times/week, 31.53 (95% CI, 10.94–90.87) for one–two times/week, and 93.93 (95% CI, 12.50–705.82) for ≥3 times/week, suggesting a dose-response trend. For BMI, both underweight (31.06 [95% CI, 3.74–258.02]) and overweight individuals (35.47 [95% CI, 15.06–83.55]) had a higher IRR of hydrocephalus compared with those with normal BMI (13.13 [95% CI, 8.64–19.95]). Individuals with high total cholesterol levels had a higher IRR (22.34 [95% CI, 11.91–41.89]) than those with lower levels (14.53 [95% CI, 9.27–22.80]). In terms of income, participants with income above the median showed a greater increase in hydrocephalus risk (22.71 [95% CI, 12.10–42.65]) compared with those with income below the median (14.57 [95% CI, 9.30–22.81]). The IRs and IRRs of hydrocephalus among patients with hemorrhagic and ischemic stroke are presented in Tables 4 and 5, respectively.
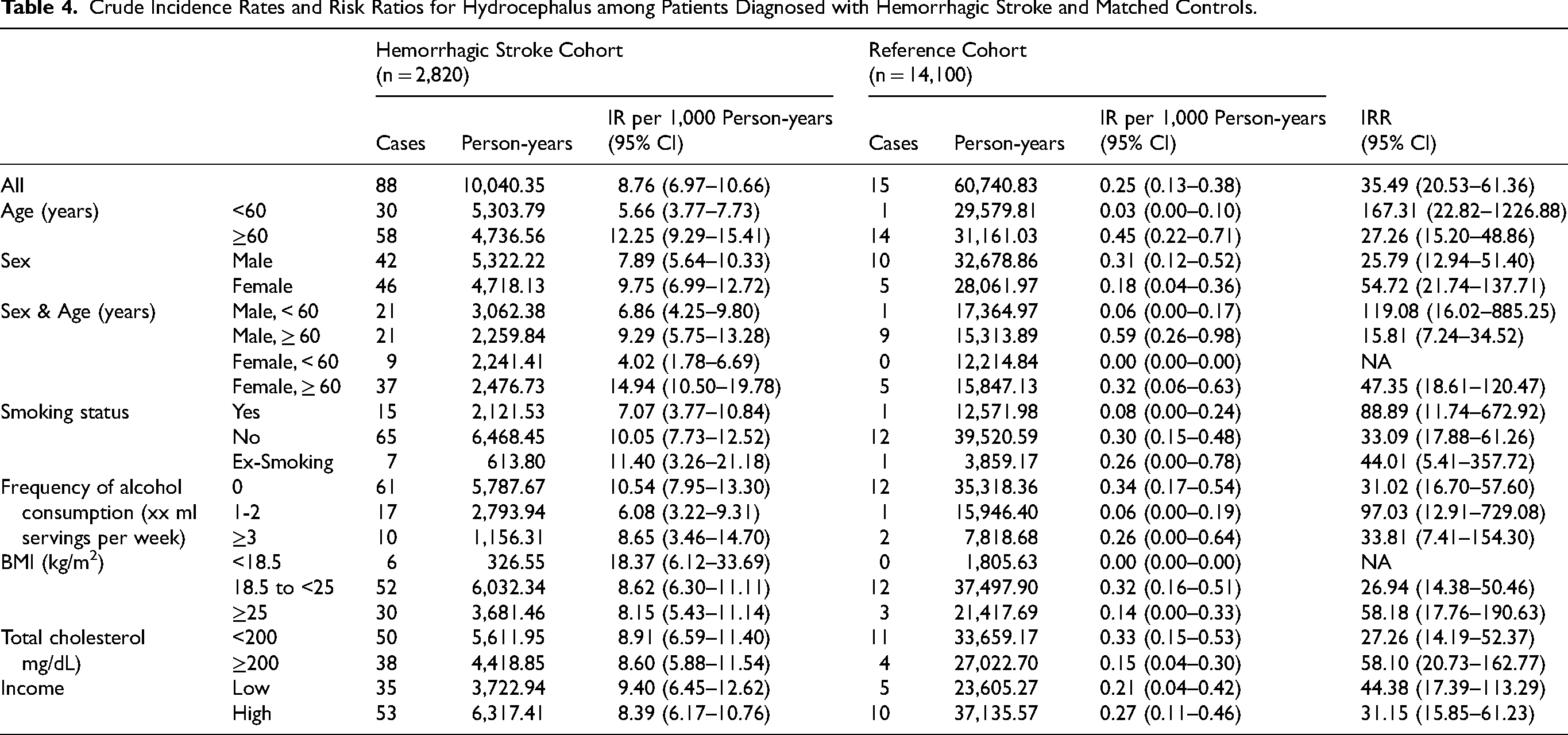
Crude Incidence Rates and Risk Ratios for Hydrocephalus among Patients Diagnosed with Hemorrhagic Stroke and Matched Controls.
Crude Incidence Rates and Risk Ratios for Hydrocephalus among Patients Diagnosed with Ischemic Stroke and Matched Controls.
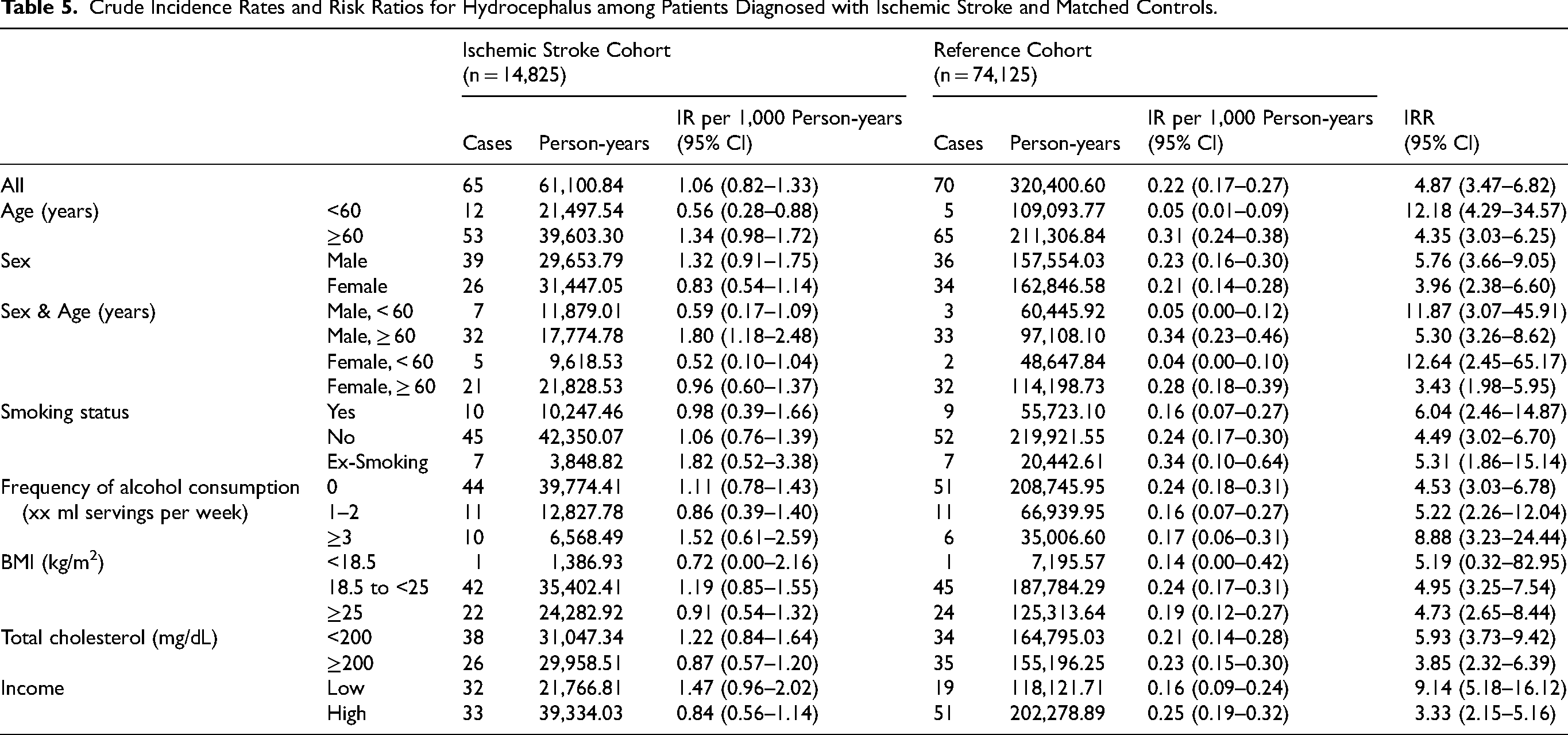
Figure 2 presents the Kaplan–Meier survival curves showing hydrocephalus-free survival over the nine-year follow-up period in the stroke and control groups. The overall stroke cohort showed a marked decline in survival probability early in the follow-up compared with the control group (Figure 2A), and this pattern was consistent with a violation of the proportional hazards assumption, as indicated by the Schoenfeld residual test. In the subgroup analysis by stroke type, the early and steep decline in hydrocephalus-free survival was most pronounced in patients with hemorrhagic stroke (Figure 2B). In contrast, patients with ischemic stroke demonstrated a more gradual decline that continued throughout the later follow-up period, particularly during years 6–9 (Figure 2C).
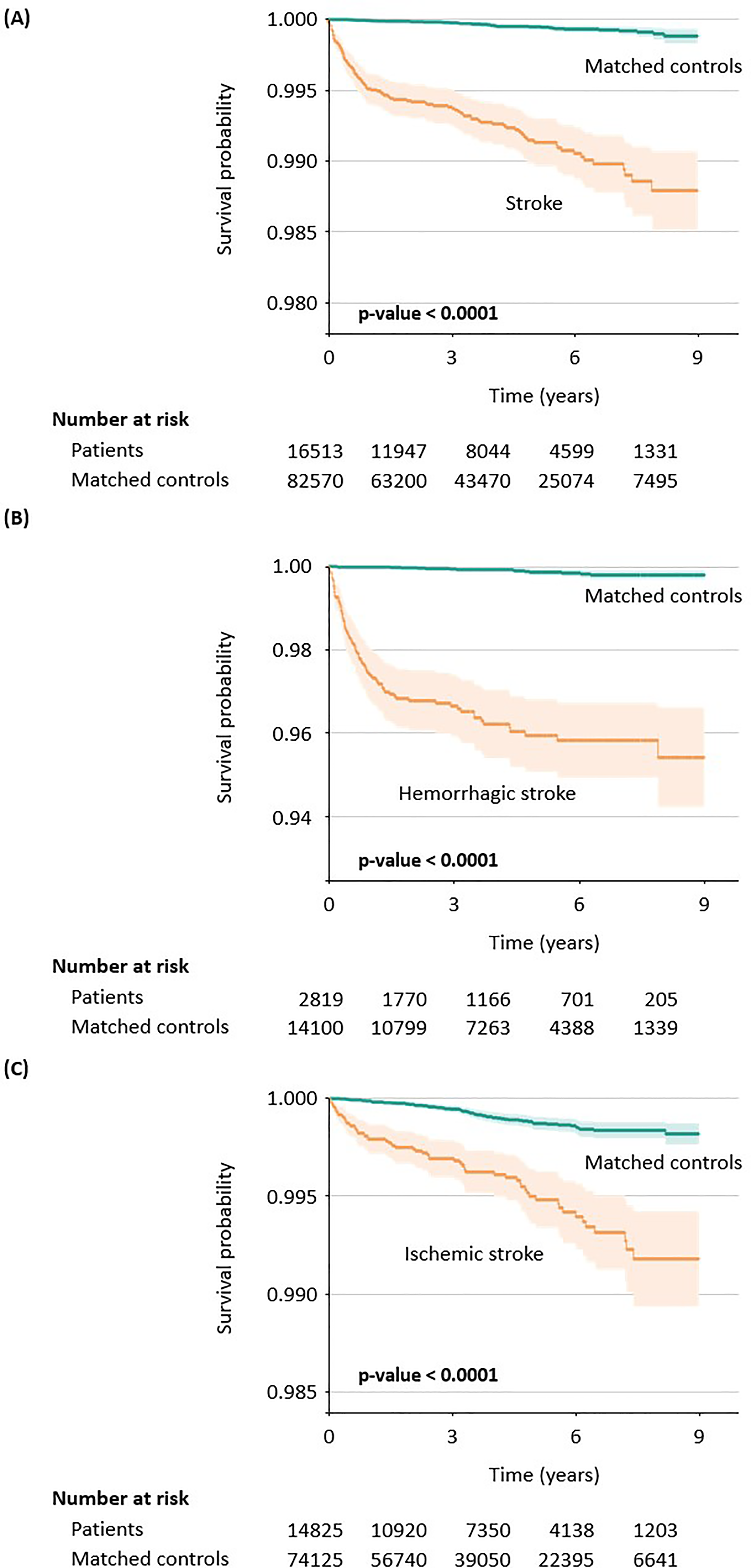
Kaplan–Meier Curves of Hydrocephalus-Free Survival among Patients Diagnosed with Stroke and Matched Controls: (A) Overall, (B) Hemorrhagic Stroke, and (C) Ischemic Stroke.
Figure 3 illustrates the results of the extended time-stratified multivariable Cox proportional hazards model, in which the follow-up period was divided into three-year intervals. The covariates were age, sex, smoking status, alcohol consumption, BMI, total cholesterol, and income level. During the first three years after stroke, the adjusted hazard ratio (aHR) for hydrocephalus was 29.53 (95% CI, 17.09–51.02). Although the risk decreased substantially in the mid-term follow-up period (years 3–6), it remained elevated at 6.18 (95% CI, 3.27–11.70) and persisted through years 6–9 (aHR, 8.32; 95% CI, 2.63–26.31) (Figure 3A). Subgroup analysis revealed different temporal patterns between hemorrhagic and ischemic stroke. In patients with hemorrhagic stroke, the risk of hydrocephalus was highest during the initial three years (aHR, 54.93; 95% CI, 25.32–119.17), declining in years 3–6 (aHR, 13.14; 95% CI, 4.47–38.65), and becoming statistically non-significant in years 6–9 (aHR, 4.19; 95% CI, 0.34–51.18) (Figure 3B). In contrast, patients with ischemic stroke had a lower early risk (aHR, 6.71; 95% CI, 4.16–10.82) but showed a relatively higher risk in the later follow-up period (years 6–9) compared with those with hemorrhagic stroke (aHR, 5.51 [95% CI, 1.77–17.12] vs. 4.19 [95% CI, 0.34–51.18]) (Figure 3C).
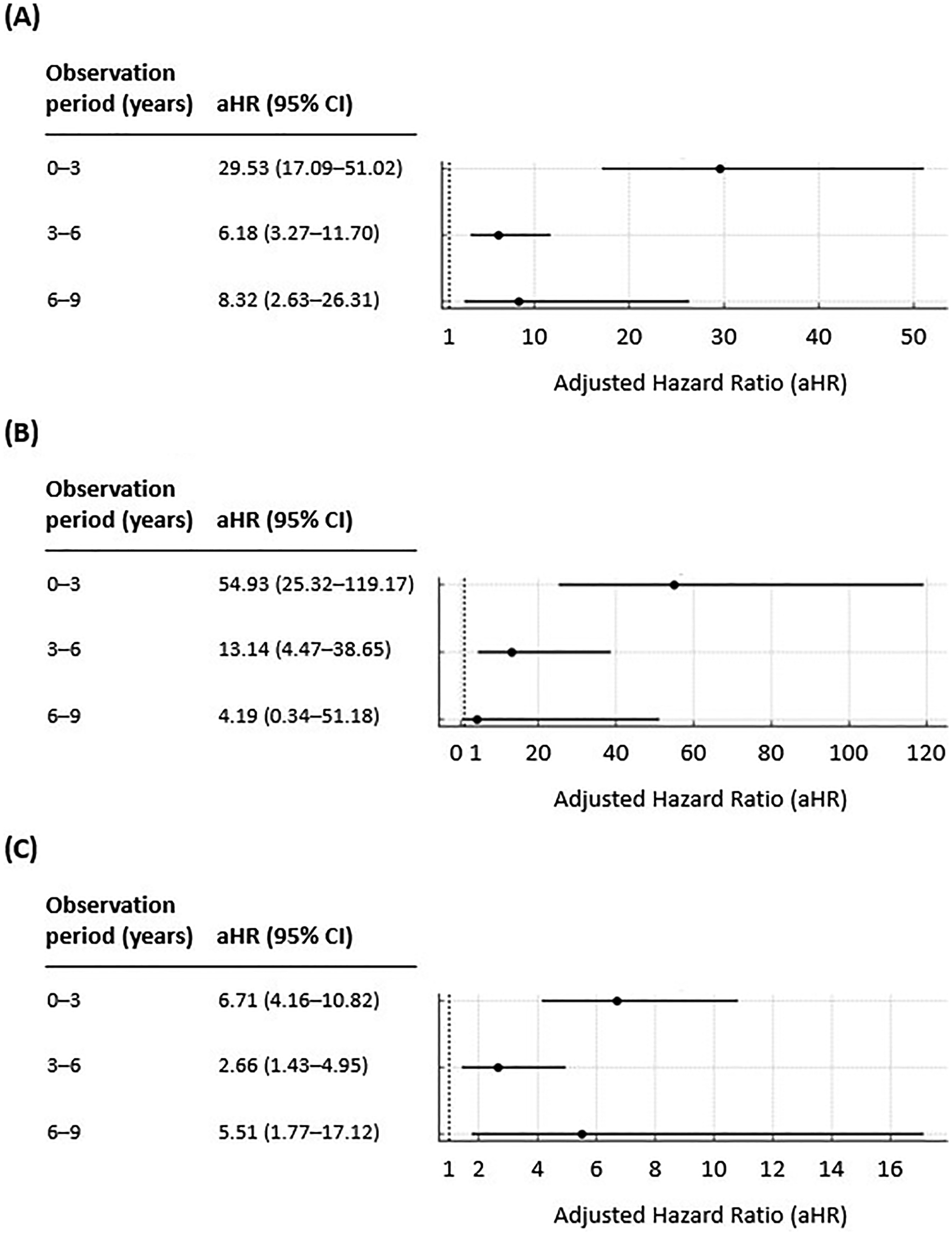
Forest Plots of the Risk of Hydrocephalus in the (A) Overall Stroke Group and (B) Hemorrhagic and (C) Ischemic Stroke Subgroups.
Discussion
In this nationwide retrospective cohort study, the incidence of hydrocephalus following stroke was found to be 17.11 times higher in the stroke cohort compared with the control group. The IRRs for hemorrhagic and ischemic stroke were significantly elevated at 35.49 (95% CI, 20.53–61.36) and 4.87 (95% CI, 3.47–6.82), respectively. Notably, the risk increase was more pronounced in women and younger individuals, with IRRs of 33.32 (95% CI, 16.50–67.31) and 35.12 (95% CI, 13.74–89.80), respectively. Both the overall stroke cohort and hemorrhagic stroke subgroup exhibited the highest risk of hydrocephalus during the first three years, followed by a decline. In contrast, the ischemic stroke group showed a biphasic pattern, with an initial increase in risk, a temporary decline, and a secondary rise during the period from years 6 to 9.
The IRR of hydrocephalus was significantly elevated in the stroke cohort overall, with increased risk observed in both hemorrhagic and ischemic stroke subgroups. These findings are generally consistent with previous literature reports (Cai et al., 2025; Chen et al., 2024; Ovenden et al., 2023). Hemorrhagic stroke frequently leads to hydrocephalus owing to bleeding into the ventricles or subarachnoid space, where iron and hemoglobin breakdown products trigger inflammation and fibrosis. These processes contribute to impaired CSF absorption and flow (Koduri et al., 2020; Wahjoepramono et al., 2023). Iron deposition, in particular, may exacerbate ependymal damage and further disrupt CSF circulation (Kuo & Huang, 2021). As for ischemic stroke, although the incidence of hydrocephalus is relatively lower, extensive infarction or severe cerebral edema may compress or obstruct the ventricles, resulting in acute hydrocephalus (Jeon et al., 2014). In cases of hemorrhagic transformation during reperfusion therapy, intraventricular hemorrhage may occur, leading to CSF flow obstruction through mechanisms similar to those seen in hemorrhagic stroke, thereby worsening clinical outcomes.
Older patients aged 60 years and above are at a significantly higher risk of developing hydrocephalus compared with younger individuals (Degos et al., 2013; Wang et al., 2022). In a cohort of patients with aSAH with a mean age of 52 years, the incidence of shunt-dependent hydrocephalus was 14.3%, and age over 60 years was identified as an independent risk factor (Hao & Wei, 2019). A meta-analysis citing this study reported that 19.5% of patients aged 60–69 years and 30.5% of those aged 70 years or older required shunt placement (Wilson et al., 2017).
In contrast, individuals under the age of 60 years generally exhibit lower IRs of hydrocephalus and are not typically considered at high risk, except in specific clinical contexts (Gluski et al., 2021). This difference may be attributed to age-related declines in CSF absorption capacity, heightened inflammatory responses, and delayed clearance of blood breakdown products in older adults (Rao et al., 2024). Consistent with previous findings, our study showed that participants under the age of 60 years recorded a lower absolute IR but a higher IRR. This may reflect the fact that older adults may have a higher baseline risk of hydrocephalus independent of stroke, whereas younger individuals rarely develop hydrocephalus prior to stroke, resulting in a greater relative increase in risk following a stroke event (Isaacs et al., 2018).
Meanwhile, although the crude IR of hydrocephalus was lower in women than in men, the IRR was higher in women. Studies have suggested a slightly increased risk of hydrocephalus in women following hemorrhagic stroke, but the findings remain inconsistent across the literature (Bhattacharjee et al., 2021; Rehman et al., 2023). Sex hormones are known to influence cerebral vasculature and CSF dynamics. In animal models, estrogen has been reported to exacerbate ventricular enlargement (Peng et al., 2021), whereas clinical studies have shown neuroprotective effects of estrogen in premenopausal women (Gu et al., 2010). After menopause, decreased estrogen levels may contribute to reduced vascular elasticity and alterations in CSF metabolism, potentially increasing the risk of complications (Rehman et al., 2023). As such, women may have a modestly elevated risk of hydrocephalus, but current evidence is inconclusive. Further research is needed to clarify the complex role of sex hormones in hydrocephalus development.
Smokers showed a slightly higher IRR of hydrocephalus compared with non-smokers and former smokers. This finding is consistent with a proposed mechanism in which chronic inflammation and vascular injury caused by smoking may exacerbate stroke severity and consequently increase the risk of hydrocephalus. Smoking has been associated with elevated oxidative stress and neuroinflammation in the CSF, as well as altered choroid plexus function, which may contribute to impaired CSF dynamics (Lallai et al., 2019; Liu et al., 2020a).
Clinical studies have reported higher rates of hydrocephalus and shunt placement in smokers compared with non-smokers, possibly owing to the toxic effects of cigarette smoke on the ependymal lining and arachnoid granulations, which are essential for CSF absorption (Wu et al., 2022). In addition, smoking is known to disrupt the blood–brain barrier and induce oxidative stress, both of which may increase the risk of hydrocephalus following traumatic brain injury (Sivandzade et al., 2020a; Sivandzade et al., 2020b). Notably, the crude IR was higher among former smokers than current smokers, which may suggest that former smokers represent a group with poorer baseline health status. Future studies should incorporate more refined analyses controlling for potential confounding factors.
We also found an association between an increase in alcohol consumption and a corresponding rise in the IRR for hydrocephalus. This relation may be explained by the effect of alcohol on coagulation pathways, which can lead to hematoma expansion and rebleeding, thereby increasing the risk of hydrocephalus. Studies have shown that while light to moderate alcohol intake may reduce the risk of ischemic stroke, heavy alcohol consumption significantly increases the risk of hemorrhagic stroke, in particular (Larsson et al., 2016). Animal studies have demonstrated that alcohol impairs glymphatic function and ciliary motility in the ventricular system (Liu et al., 2020b; Omran et al., 2017), and may adversely affect the ependyma and choroid plexus, thereby disturbing CSF circulation (Wu et al., 2022). These physiological mechanisms may help explain the dose-dependent increase in hydrocephalus risk observed in our study.
Among patients with hemorrhagic stroke, those with high cholesterol levels exhibited a higher IRR for hydrocephalus, whereas patients with ischemic stroke showed the opposite trend. In hemorrhagic stroke, elevated cholesterol may exacerbate atherosclerosis, reducing vascular compliance and worsening vascular injury. Studies on moyamoya disease have linked hyperlipidemia to poorer outcomes, suggesting increased vulnerability to secondary damage (Lee et al., 2023). In contrast, a phenomenon known as the “cholesterol paradox” has been proposed in ischemic stroke, where higher cholesterol levels may be associated with less severe infarctions and better survival outcomes (Patel et al., 2019). Additionally, patients with low cholesterol levels are often more critically ill, potentially leading to early mortality before hydrocephalus can be observed, thereby lowering the apparent incidence. This raises the possibility of immortal time bias (Chen et al., 2017a). Such biases should be carefully considered in the interpretation of our findings.
BMI exhibited a U-shaped association with the risk of hydrocephalus. Underweight individuals may be more vulnerable to worsening injury owing to impaired immune function and reduced tissue repair capacity (Stechmiller, 2010). In contrast, obesity is associated with chronic inflammation and metabolic disorders, which may contribute to impaired CSF circulation and increased intracranial pressure. Moreover, obesity is a well-established risk factor for idiopathic intracranial hypertension, suggesting that similar pathophysiological mechanisms may contribute to the development of hydrocephalus following stroke (Subramaniam & Fletcher, 2017; Westgate et al., 2022).
The higher IRR of hydrocephalus observed in higher-income individuals compared with lower income counterparts may suggest the presence of survivor bias. Individuals in lower-income groups may experience limited access to acute stroke care or die earlier before hydrocephalus can be diagnosed (Cox et al., 2006), whereas those in higher-income groups are more likely to receive timely treatment and follow-up, leading to a greater observed incidence. In addition, certain lifestyle factors more commonly observed in higher-income groups, including alcohol consumption, smoking, and obesity, may indirectly contribute to an increased risk of hydrocephalus. Another possibility is that a greater proportion of older adults are included in the higher-income group, which could have contributed to the difference in risk (Khang et al., 2010).
In both the overall stroke cohort and hemorrhagic stroke subgroup, the highest risk of hydrocephalus was observed within the first three years following stroke onset, followed by a sharp decline. In contrast, the ischemic stroke subgroup exhibited a biphasic pattern in which the risk initially increased, then temporarily declined during the mid-term period, and rose again at years 6–9 after stroke onset. Studies have primarily focused on the early risk of hydrocephalus during short-term follow-up (Hu et al., 2021; Walcott et al., 2015). Our study highlighted the dynamic changes in hydrocephalus risk over the long term.
The early surge in risk among patients with hemorrhagic stroke is likely attributable to structural obstruction and inflammatory and fibrotic responses triggered by residual blood products (Hu et al., 2021). In contrast, the delayed increase in hydrocephalus risk among ischemic stroke patients may result from progressive degenerative changes, such as white matter damage and the accumulation of cerebral small vessel disease, leading to chronic CSF circulation impairment (Cai et al., 2025). Therefore, patients with hemorrhagic stroke require careful monitoring for early complications, whereas those with ischemic stroke should be observed for delayed risk over time. Our findings emphasize the importance of developing long-term follow-up strategies tailored to each type of stroke.
Our findings should be interpreted with caution, considering several limitations. First, owing to the constraints of the dataset, the analysis could not include various clinical factors known to influence the risk of hydrocephalus after stroke. These include stroke severity, anatomical location of the lesion, and the distribution of affected vessels, which have been reported to be closely associated with hydrocephalus development (Bhattacharjee et al., 2021; Erixon et al., 2014; Hughes et al., 2015; Naidech et al., 2012; Wilson et al., 2017). In particular, the posterior communicating artery is anatomically adjacent to the fourth ventricle and has been linked to a higher risk of hydrocephalus (Cano et al., 2012; Yamada et al., 2015). These important anatomical and clinical factors could not be accounted for in this study. Second, treatment-related factors were not included in the analysis. Decompressive craniectomy, a common surgical procedure to reduce elevated intracranial pressure, has been reported to increase the risk of hydrocephalus following stroke (Waziri et al., 2007). Although findings on this association remain inconclusive (Kim et al., 2009; Rahme et al., 2010), information regarding the use of this procedure was not available in the dataset, which limits interpretation. Third, both stroke and hydrocephalus were identified using diagnostic codes from insurance claims data, which may differ from clinical diagnoses in practice and could lead to misclassification. These limitations highlight the need for future studies using clinically detailed datasets to better elucidate the development of hydrocephalus after stroke. A more precise evaluation of risk by stroke subtype will be essential to improve prediction and management strategies.
Conclusion
Our findings showed that patients with stroke had a significantly higher risk of developing hydrocephalus compared with the control group, with the risk being especially pronounced in the early post-diagnosis period and among women and younger individuals. These results highlight the need for targeted monitoring and early intervention strategies, especially in female and younger stroke patients, to prevent and manage hydrocephalus as a critical complication. Future large-scale prospective studies are warranted to refine the understanding of risk factors and to develop personalized approaches for the prevention and management of hydrocephalus in stroke survivors.
Footnotes
Ethical Considerations
This study was approved by Sungshin Women's University (SSWUIRB-2025-009).
Funding
This research was supported by SungKyunKwan University and the BK21 FOUR (Graduate School Innovation) funded by the Ministry of Education (MOE, Korea) and the National Research Foundation of Korea (NRF). Additionally, it was supported by the NRF funded by the Korean government (MSIT and MOE): NRF [grant number 2021-R1-I1A2(059735)]; RS [grant number 2024-0040(5650)]; RS [grant number 2024-0044(0881)]; and RS [grant number 2019-II19(0421)]. Hohyun Jung was partly supported by an NRF grant funded by the Korean government: RS [grant number 2024-0045(5553)].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets analyzed in this study can be obtained from the corresponding authors upon reasonable request.