
Abstract
Objective
To investigate the effects of a two-week robot-assisted gait training (RAGT) program on walking performance and brain activation in children with spastic hemiplegic cerebral palsy (CP).
Design
Single-group, pre–post pilot study.
Methods
Eight children with CP were enrolled; six completed the protocol and provided usable gait and functional MRI (fMRI) data. Participants received 10 RAGT sessions over two weeks. Walking performance (6-min walk test [6MWT], 10-meter walk test [10MWT], GAITRite gait speed and cadence) was assessed at baseline, immediately after the intervention, and at one-month follow-up. Pre- and post-intervention fMRI during a lower-limb motor task quantified activated voxels in motor and cerebellar regions.
Results
6MWT distance, 10MWT speed, and GAITRite gait speed and cadence improved significantly (all p ≤ 0.009) at post-intervention and follow-up versus baseline. In children with isolated subcortical lesions (n = 4), activated voxels during the lower-limb task increased in the lesioned motor cortex (from 363 to 1,075; p = 0.02), with similar increases in ipsilesional cerebellar hemispheres (p = 0.02), whereas no significant changes were seen in children with additional hydrocephalus (n = 2). Change in cadence correlated positively with change in lesioned motor cortex activation (Spearman's ρ = 0.83, p = 0.03).
Conclusions
In this small cohort, a two-week RAGT program was associated with short-term improvements in walking performance and increased fMRI activation in motor-related regions, particularly in children with subcortical lesions. These preliminary, lesion-type–specific findings suggest neuroplastic responses to RAGT that warrant confirmation in larger controlled studies.
Keywords
Introduction
Cerebral palsy (CP) is the most common cause of motor disability in childhood, with a global prevalence ranging from 1.6 to 3.0 cases per 1,000 live births, depending on socioeconomic and healthcare factors (Oskoui et al., 2013). Among its various forms, spastic hemiplegic CP is characterized by unilateral motor impairment that significantly affects gait, balance, and functional independence. These motor deficits are often accompanied by altered neuromuscular control and reduced selective motor activation, which limit the child's ability to participate in daily activities and social environments (Rosenbaum et al., 2007). Early and intensive rehabilitation is therefore essential to promote motor development and functional autonomy (Novak et al., 2020).
In recent years, robotic-assisted rehabilitation has emerged as a promising approach to enhance gait training in children with CP. Robot-Assisted Gait Therapy (RAGT) provides repetitive, task-specific, and intensive training that can be tailored to the individual's motor abilities. Devices such as the Lokomat® and Gait Trainer GT-I® allow for partial body weight support and controlled movement patterns, facilitating motor learning and potentially inducing neuroplastic changes (Castelli et al., 2022; Kleim & Jones, 2008). A recent systematic review and meta-analysis by Cortés-Pérez et al. (2022) demonstrated that RAGT is more effective than conventional therapy in improving walking speed, walking distance, and gross motor function related to walking, running, and jumping. However, no significant differences were found when RAGT was compared to treadmill training, and the combination of RAGT with conventional therapy did not yield additional benefits.
Alongside these objective, performance-based measures of gait, standardized clinical scales and patient- or caregiver-reported outcome measures, such as the Gross Motor Function Classification System (GMFCS), the Pediatric Evaluation of Disability Inventory (PEDI), and parent/caregiver questionnaires, are widely used to quantify functional status, everyday motor performance, and participation in children with CP. These tools capture perceived changes that are meaningful for children and their families and are therefore essential to interpret the clinical relevance of treatment-induced improvements, complementing instrumented gait analysis and other objective assessments (Novak et al., 2020).
Despite encouraging functional outcomes reported for RAGT, the underlying neural mechanisms supporting its efficacy remain poorly understood. Most studies to date have focused on clinical and biomechanical measures, while the contribution of central nervous system reorganization has received limited attention. Functional magnetic resonance imaging (fMRI) offers a non-invasive method to investigate brain activation patterns associated with motor tasks and has been used to explore cortical plasticity in children with CP. For instance, Phillips et al. (2007) reported increased activation in motor-related brain areas following treadmill-based interventions. However, evidence on the impact of RAGT on brain function, particularly in children with spastic hemiplegia, is still scarce (Julien et al., 2024), and very few studies have attempted to relate neuroimaging changes to subjective or patient-reported motor improvements, leaving the link between neural reorganization and clinically meaningful functional gains largely unexplored.
The present study aims to address part of this gap by investigating the effects of a two-week intensive RAGT program using the Gait Trainer GT-I® on both functional gait parameters and brain activation patterns in children with spastic hemiplegic CP. In addition to standard walking assessments (see below), we employed fMRI to measure changes in brain activation within key motor regions. We also examined the relationship between functional improvements and neuroimaging outcomes, with particular attention to lesion type (subcortical vs. subcortical + hydrocephalus) and hemispheric differences. Within the constraints of this exploratory pilot study, we focused on a core set of objective gait and neuroimaging measures as an initial step toward integrating behavioral, neurophysiological, and patient- or caregiver-reported outcomes in future, larger-scale trials. By combining behavioral and neurophysiological data, this study seeks to provide a more comprehensive understanding of the mechanisms underlying motor recovery in CP and to support the rationale for incorporating RAGT into individualized rehabilitation programs.
Methods
Participants
Eight children diagnosed with spastic hemiplegic CP were consecutively recruited from our center. Inclusion criteria were: (a) diagnosis of spastic hemiplegic CP; (b) age between 6 and 18 years; (c) GMFCS level I, indicating the ability to walk independently without limitations (Palisano et al., 1997); (d) ability to actively dorsiflex the ankle on the affected side by at least 10°; (e) ability to maintain a sitting position; and (f) ability to follow verbal instructions during clinical and neuroimaging assessments (Phillips et al., 2007). Exclusion criteria included: (a) lower limb spasticity ≥ 2 on the Modified Ashworth Scale (Picelli et al., 2014); (b) botulinum toxin treatment within the previous six months; (c) recent changes in oral antispastic medications; (d) orthopedic or neurosurgical interventions within the past year; (e) comorbid orthopedic or neurological conditions affecting the lower limbs; and (f) cardiovascular disease.
All participants and their legal guardians provided written informed consent. The study was approved by the Review Board of our Department and conducted in accordance with the Declaration of Helsinki. Given the exploratory, pilot nature of this study and the logistical and ethical constraints associated with intensive RAGT combined with repeated MRI acquisitions in children, the planned sample size was limited to eight consecutively recruited participants. This number was considered sufficient to assess feasibility and to obtain preliminary estimates of treatment effects to inform the design of future, adequately powered trials.
Study Design and Timeline
Given the pilot nature of this study, a control group was not included. This design choice limits the ability to attribute observed changes exclusively to the intervention, restricts causal inference, and warrants cautious interpretation of the findings (see also the Discussion section). Participants underwent three assessments: baseline (T0), immediately after the intervention (T1, within 6 h of the final session), and one-month post-intervention (T2). Walking performance was evaluated at all three time points, while fMRI was conducted at T0 and T1. During the two-week intervention period, RAGT temporarily replaced participants’ usual physiotherapy and/or occupational therapy. No additional therapist-delivered rehabilitation sessions were scheduled alongside RAGT, so that any observed pre–post changes would reflect the effect of the robotic program rather than the addition of concurrent rehabilitation modalities.
Robotic Rehabilitation Protocol
The intervention consisted of 10 sessions of RAGT using the Gait Trainer GT-I® (Reha-Stim, Berlin, Germany), administered over two consecutive weeks (five sessions per week). Each session lasted 30 min. The Gait Trainer is a programmable footplate-based system that simulates the stance and swing phases of gait using a double crank and rocker gear mechanism (Schmidt et al., 2007). The system includes servo-controlled motors that adjust gait velocity and body weight support based on real-time feedback. Participants were secured in a harness suspended from a body-weight support system. Initially, 30% of body weight was supported, with progressive reduction to 0% by the end of the training period, contingent on the participant's ability to maintain knee extension during stance and a stable foot placement pattern. At the first session, an initial treadmill speed between 1.0 and 2.0 km/h was selected individually for each child, based on comfortable walking speed and safety. Thereafter, speed was progressively increased within and/or across sessions in small steps (0.2–0.5 km/h), provided that the participant maintained an adequate gait pattern (no excessive knee flexion or toe drag), did not report pain, and showed no signs of excessive fatigue (e.g., shortness of breath, inability to sustain the task). When these criteria were not met, treadmill speed was reduced and/or temporarily kept constant. The maximum training speed allowed by the protocol was 5 km/h. In addition to speed and body-weight support, other device parameters (step length, stance/swing ratio, and footplate trajectory) were adjusted at the beginning of the program according to each child's lower limb length, baseline gait pattern, and level of impairment, and could be further fine-tuned during the sessions to improve symmetry and avoid exacerbation of spasticity. A licensed physical therapist supervised all sessions, providing manual assistance at the pelvis or lower limbs when needed to facilitate proper alignment and weight transfer and to prevent compensatory movements.
Adherence to the intervention was monitored using a standardized treatment log, in which the therapist recorded, for each session, the actual duration of active walking, the percentage of body-weight support, the range of treadmill speeds used, any adjustments to device settings, and any adverse events or reasons for early termination. For the purposes of the present analysis, participants were considered to have completed the protocol if they attended all scheduled sessions and were able to perform the full 30 min of training, or if any missed time was due solely to technical issues rather than lack of cooperation or intolerance to the intervention (see Results for details on completion and attrition).
Walking Assessments
Walking performance was assessed using three validated tools: the 6-Minute Walk Test (6MWT), the 10-Meter Walk Test (10MWT), and the GAITRite® system (Gold, version 3.2b; CIR Systems, Sparta, NJ, USA). The 6MWT measured the distance walked at a self-selected pace over six minutes on a 20-meter oval track and is a reliable indicator of walking endurance in pediatric populations (Li et al., 2005). The 10MWT assessed walking speed by recording the time required to walk 10 meters, averaged over three trials. The GAITRite system, a 7.66-meter electronic walkway, captured spatiotemporal gait parameters including speed, cadence, stride length, and single/double support durations. In this pilot study, we intentionally focused on objective, performance-based walking measures to limit testing burden in a small pediatric neuroimaging sample. Standardized clinical scales and patient- or caregiver-reported outcome measures were not collected, which should be considered when interpreting the functional relevance of the observed changes.
fMRI Acquisition and Motor Tasks
MRI scans were performed using a 1.5 Tesla Symphony scanner (Siemens AG, Erlangen, Germany). Participants lay supine with their lower limbs relaxed and were instructed to remain as still as possible throughout the examination. Structural imaging included T2-weighted axial (TR = 4670 ms, TE = 24 ms, FOV = 256 × 256, matrix = 512 × 512, slice thickness = 3 mm) and high-resolution T1-weighted axial sequences (TR = 9 ms, TE = 3.33 ms, FOV = 256 × 256, matrix = 512 × 512, slice thickness = 1 mm).
Functional images were acquired using a T2*-weighted echo planar imaging (EPI) sequence (TR = 3500 ms, TE = 50 ms, voxel size = 5 × 5 × 5 mm, matrix = 64 × 64, 36 axial slices, slice thickness = 3.75 mm). Each fMRI run lasted approximately six minutes and included 100 volumes, arranged in a block design with five activation and five rest blocks. The first volumes of each run were discarded to allow for T1 equilibration.
Two motor tasks were performed with the affected limbs: (1) active ankle dorsiflexion and (2) finger tapping. Movements were paced at 1 Hz using a metronome, with a high-pitched tone signaling the start of each activation block. Participants were trained prior to scanning to ensure task compliance, and task execution was monitored visually through the scanner window and video camera to detect gross compensatory movements. However, range of motion, force production, and muscle activity were not recorded instrumentally during scanning. Finger tapping served as an internal control, as it was expected to produce consistent activation across sessions (Phillips et al., 2007).
fMRI Data Processing and Analysis
Functional data were analyzed using the fMRI Expert Analysis Tool (FEAT) version 5.98 within the FMRIB Software Library (FSL; www.fmrib.ox.ac.uk/fsl). Preprocessing steps included motion correction (MCFLIRT; Jenkinson et al., 2002), brain extraction (BET; Smith, 2002), slice-timing correction, spatial smoothing with a 7-mm FWHM Gaussian kernel, and high-pass temporal filtering (cutoff = 100 s).
Head motion and data quality were systematically assessed. For each run, the realignment parameters output by MCFLIRT were inspected, and framewise displacements were quantified. Datasets were excluded from further analysis if absolute head motion exceeded 3 mm of translation or 3° of rotation in any direction, or if more than 20% of volumes showed marked motion spikes or artefacts (e.g., signal dropout, ghosting) on visual inspection. In the remaining datasets, the six motion parameters were included as nuisance regressors in the first-level general linear model (GLM). All activation maps were visually inspected to verify adequate brain coverage, absence of major artefacts, and satisfactory registration to the anatomical images. As reported in the Results section, two participants were excluded from the fMRI analysis due to poor compliance and excessive motion.
Statistical analysis was conducted using FMRIB's Improved Linear Model (FILM) to generate activation maps of blood oxygenation level–dependent (BOLD) signal changes between active and rest conditions for each task (ankle dorsiflexion, finger tapping). Cluster-based thresholding was applied at p < 0.05, corrected for multiple comparisons, using the method described by Worsley et al. (2001). Functional images were co-registered to high-resolution anatomical scans and normalized to the Montreal Neurological Institute (MNI) 152 template using FLIRT (Jenkinson & Smith, 2001, 2002).
Regions of interest (ROIs) included the primary motor cortex (M1), premotor cortex (PMC), supplementary motor area (SMA), primary sensory cortex (S1), cerebellar hemispheres (CH), and cerebellar vermis (CV). ROIs were defined anatomically based on established criteria (Phillips et al., 2007) on the MNI template and then applied to each subject's normalized activation maps. For each child, lesions were identified on structural MRI and classified as (i) subcortical or (ii) subcortical with associated hydrocephalus. Based on lesion location, the hemisphere containing the lesion was labeled as “ipsilesional” and the contralateral hemisphere as “contralesional.” For cortical ROIs (M1, PMC, SMA, S1) and cerebellar hemispheres, the number of suprathreshold voxels was extracted separately for ipsilesional and contralesional ROIs, for each task and time point (T0 and T1). This allowed hemisphere-specific analyses and comparisons between lesion-type groups (subcortical vs. subcortical + hydrocephalus). Activation maps were overlaid on anatomical templates and inspected using MRIcro (www.mccauslandcenter.sc.edu/mricro).
Statistical Analysis
Statistical analyses were performed on a per-protocol dataset including the six children who completed the full RAGT program and had usable gait and fMRI data at the relevant time points. Data from the two enrolled participants who did not complete the intervention and/or provided unusable MRI data because of poor compliance and excessive motion artefacts were excluded from all analyses. No data imputation procedures were applied, and missing values were not replaced; for the six completers, complete datasets were available for the primary gait and fMRI outcomes at the analyzed time points.
All analyses were conducted using IBM SPSS Statistics version 27.0. Normality was assessed using skewness and kurtosis indices and visual inspection of histograms and Q–Q plots. When the assumptions of normality or homogeneity of variance (Levene's test) were violated, logarithmic transformation was applied and the transformed data were used for inference.
Non-normally distributed walking data were analysed using the Friedman test, followed by Bonferroni-corrected Wilcoxon signed-rank tests for pairwise comparisons (T1–T0, T2–T0), with the significance level adjusted according to the number of comparisons. For these analyses, effect sizes were reported as Kendall's W for the Friedman test and as r (Z/√N) for the Wilcoxon tests. fMRI data were analysed using repeated-measures ANOVA with TIME (T0, T1) as a within-subject factor and SIDE (lesioned, intact), LIMB (upper, lower), and LESION TYPE (subcortical, subcortical + hydrocephalus) as between-subject factors; when appropriate, Bonferroni-adjusted post hoc tests were used to explore significant main effects or interactions. For ANOVA models, effect sizes were quantified using partial eta squared (η2p).
Spearman's rank correlation coefficient (ρ) was used to assess associations between changes in walking performance and changes in fMRI activation. Given the small sample size and the exploratory nature of these correlations, ρ values were interpreted as effect size indices, and results were reported with exact p-values. Where multiple correlations were performed, findings were interpreted cautiously, and uncorrected p-values were explicitly reported as exploratory.
Results
Participant Characteristics
Of the eight children initially enrolled in the study, six completed the full protocol and were included in the final analysis. The remaining two participants discontinued the intervention and did not contribute any usable fMRI runs because of poor compliance and excessive head motion; in accordance with the predefined quality-control criteria, their data were excluded from all subsequent analyses. All completers attended 10/10 sessions and achieved a mean active walking time of approximately 30 min per session; no serious adverse events were reported. The mean age of the participants was 10.6 years (range: 8.7–12.1), and all were male. Five children presented with left-sided hemiplegia. Baseline MRI revealed subcortical lesions in the fronto-parietal white matter in all participants (right hemisphere: n = 5; left hemisphere: n = 1), with two children also exhibiting coexisting hydrocephalus.
Walking Performance
Significant improvements in walking performance were observed across the three time points (see Table 1). The Friedman test revealed significant changes in both the 6MWT and the 10MWT (p = 0.006). Post-hoc Wilcoxon signed-rank tests showed significant improvements from T0 to T1 and from T0 to T2 for both measures. Among the GAITRite-derived spatiotemporal parameters, gait speed (p = 0.006) and cadence (p = 0.009) also showed significant changes over time. Post-hoc analysis confirmed significant increases in both parameters between T0 and T1, as well as between T0 and T2. However, the temporal symmetry ratio did not show significant variation across the three time points.
Walking Measures at Baseline (T0), Post-Treatment (T1), and Follow-up (T2).
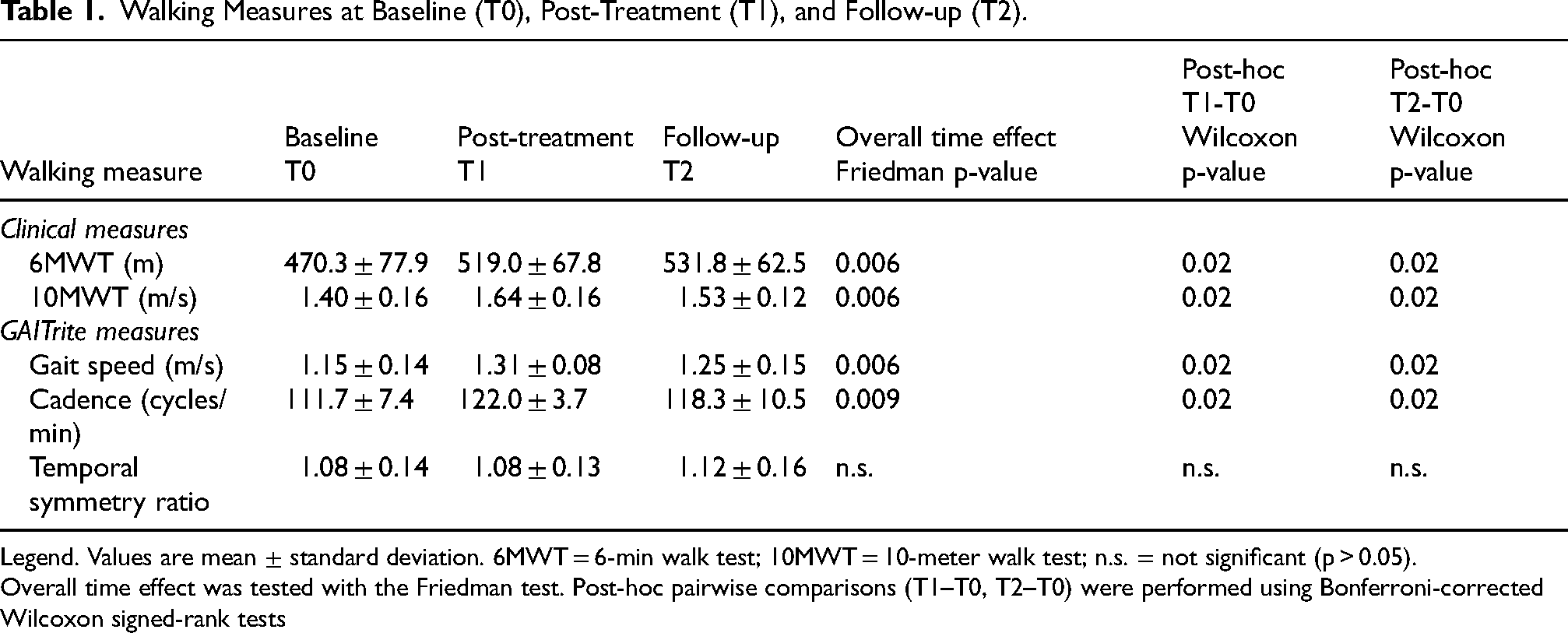
Legend. Values are mean ± standard deviation. 6MWT = 6-min walk test; 10MWT = 10-meter walk test; n.s. = not significant (p > 0.05).
Overall time effect was tested with the Friedman test. Post-hoc pairwise comparisons (T1–T0, T2–T0) were performed using Bonferroni-corrected Wilcoxon signed-rank tests
fMRI Activation Patterns
fMRI analyses are based on the six participants who completed the intervention and provided datasets that met all predefined motion and quality-control criteria. No fMRI acquisitions were performed at T2; therefore, neuroimaging results are restricted to the short-term comparison between T0 and T1. ROI analysis successfully identified the M1, PMC, SMA, CH and CV in all participants. The number of activated voxels during the lower limb motor task was quantified in both the lesioned and intact hemispheres at T0 and T1 (see Table 2).
Number of Voxels Activated During Lower Limb Motor Task.
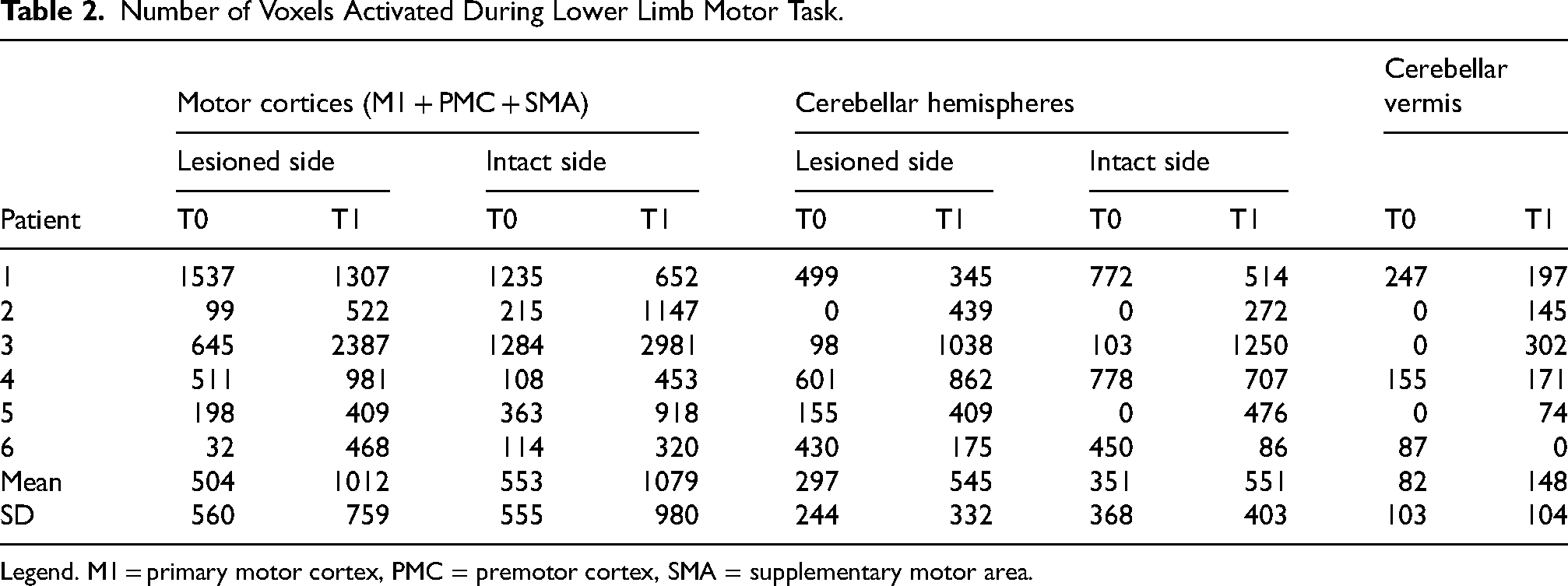
Legend. M1 = primary motor cortex, PMC = premotor cortex, SMA = supplementary motor area.
A repeated-measures ANOVA on the number of activated voxels in the motor cortices (M1 + PMC + SMA) revealed a significant main effect of TIME (F [1,16] = 11.3, p = 0.004) and a significant TIME × LIMB × LESION TYPE interaction (F [1,16] = 8.8, p = 0.009). No other main effects or interactions reached statistical significance. In participants with subcortical lesions only (n = 4), the number of activated voxels during the lower limb task significantly increased from T0 to T1 in both the lesioned hemisphere (T0: 363.3 ± 257.1; T1: 1074.8 ± 909.1; p = 0.02) and the intact hemisphere (T0: 492.5 ± 538.0; T1: 1374.8 ± 1109.1; p = 0.009). In contrast, the number of activated voxels during the upper limb task showed a non-significant decrease from T0 to T1 in both hemispheres (lesioned: T0 = 1111.0 ± 410.8, T1 = 886.0 ± 551.3; intact: T0 = 1212.0 ± 1168.5, T1 = 907.3 ± 810.5). In participants with subcortical lesions and hydrocephalus (n = 2), no significant changes in voxel activation were observed for either the upper or lower limb tasks between T0 and T1.
Cerebellar Activation
Analysis of cerebellar hemispheres revealed a significant TIME × LIMB × LESION TYPE interaction (F [1,16] = 11.5, p = 0.004). In the subcortical lesion group, the number of activated voxels during the lower limb task increased significantly from T0 to T1 in both the lesioned (T0: 213.5 ± 266.4; T1: 687.0 ± 312.3; p = 0.02) and intact hemispheres (T0: 220.3 ± 375.0; T1: 676.3 ± 421.8; p = 0.02). No significant changes were observed during the upper limb task.
In the subcortical + hydrocephalus group, cerebellar activation did not significantly change from T0 to T1 for either task.
Cerebellar Vermis Activation
For the cerebellar vermis, a significant TIME × LESION TYPE interaction was observed (F [1,8] = 7.5, p = 0.026). However, post-hoc analysis did not reveal any statistically significant changes in voxel activation between T0 and T1.
Correlation Between fMRI and Walking Measures
To explore the relationship between functional improvements and neural activation, we computed the difference in walking parameters (10MWT, GAITRite gait speed and cadence) between T1 and T0 and correlated these with changes in voxel activation in the lesioned and intact motor cortices, cerebellar hemispheres, and vermis.
A significant positive correlation was found between the change in cadence and the change in the number of activated voxels in the lesioned motor cortices (Spearman's ρ = 0.83, p = 0.03). This suggests that increased cortical activation in the lesioned hemisphere was associated with improved gait rhythm.
Although preliminary analyses indicated a strong inverse correlation between changes in 6MWT and voxel activation, these findings were excluded from the final analysis due to concerns about interpretability and potential data inconsistencies. Moreover, because fMRI data were collected only at T0 and T1, it was not possible to assess whether the T2 behavioral changes were accompanied by longer-term modifications in brain activation
Discussion
This pilot study explored the effects of a two-week RAGT program on both functional walking performance and brain activation patterns in children with spastic hemiplegic CP. In this small sample, we observed significant improvements in walking speed and cadence, as well as increased activation in motor-related cortical and cerebellar regions, particularly in children with subcortical lesions. These preliminary findings are consistent with the growing body of evidence suggesting that RAGT may be beneficial in pediatric neurorehabilitation and provide initial, lesion-type–specific insights into the neural mechanisms potentially underlying functional recovery.
The observed improvements in walking performance, as measured by the 6MWT, 10MWT, and GAITRite parameters, are consistent with previous literature. Cortés-Pérez et al. (2022) conducted a comprehensive meta-analysis of 15 controlled clinical trials and found that RAGT significantly outperformed conventional therapy in enhancing gait speed, walking distance, and gross motor function related to walking, running, and jumping. Our findings align with these results, particularly in terms of increased gait speed and cadence, and extend them by suggesting that such functional gains may be accompanied by measurable changes in brain activation.
The use of fMRI in this study allowed for the exploration of neuroplastic changes associated with RAGT. We observed a significant increase in the number of activated voxels in the M1, PMC, and SMA during lower limb motor tasks following the intervention. These changes were more pronounced in the lesioned hemisphere of children with subcortical lesions, a pattern that is compatible with the hypothesis that RAGT may facilitate reorganization of motor networks in response to intensive, task-specific training. This is in line with the findings of Phillips et al. (2007), who reported increased cortical activation during ankle dorsiflexion tasks in children with CP following body-weight-supported treadmill training. However, increased BOLD signal does not provide a unique marker of adaptive reorganization. Greater activation after training may also reflect reduced neural efficiency (i.e., recruitment of additional neural resources to support the same task), compensatory processing, or an increase in the magnitude or effort of the executed movement. In the absence of quantitative monitoring of motor output during scanning, the present results are best interpreted as showing training-related changes in motor system engagement rather than definitive proof of cortical reorganization.
Interestingly, the increase in cortical activation was not observed in children with coexisting hydrocephalus, indicating that lesion type may influence the capacity for neuroplastic adaptation. This observation underscores the importance of considering individual neuroanatomical profiles when designing and evaluating rehabilitation interventions. It also highlights the potential utility of fMRI as a biomarker for predicting treatment responsiveness and tailoring therapy to individual needs (Phillips et al., 2007).
The cerebellum, particularly the cerebellar hemispheres, also showed increased activation following RAGT in children with subcortical lesions. This finding supports the hypothesis that the cerebellum plays a compensatory role in motor learning and recovery, especially when cortical motor areas are compromised. The cerebellar vermis, however, did not exhibit significant changes, suggesting a more specific involvement of the lateral cerebellar regions in gait-related tasks. These results are consistent with previous studies indicating cerebellar contributions to motor coordination and adaptation during locomotor training (Schmidt et al., 2007).
A notable strength of this study is the integration of behavioral and neuroimaging data. The significant correlation between improvements in gait cadence and increased activation in the lesioned motor cortex in this small cohort suggests a close association between functional gains and underlying neural changes. This supports the concept of experience-dependent plasticity, whereby repetitive, goal-directed movement practice induces reorganization within motor networks (Kleim & Jones, 2008). Such findings reinforce the rationale for incorporating intensive, task-specific gait training, including RAGT, into early rehabilitation programs for children with CP, while recognizing that larger confirmatory studies are required.
Despite these promising preliminary results, several limitations must be acknowledged. First, the sample size was very small: eight children were enrolled, and only six completed the full protocol and provided usable pre- and post-intervention gait and fMRI data. While such numbers are typical of proof-of-concept neuroimaging studies in pediatric CP, they substantially limit the generalizability of the findings, reduce statistical power, and increase the risk of both type I and type II errors. The exclusion of two participants due to poor compliance with the RAGT and/or fMRI procedures further reduced an already limited sample and may have introduced selection bias. Moreover, the absence of a control group (e.g., receiving conventional therapy or no intervention) represents a major limitation, as it prevents definitive attribution of the observed improvements to the intervention itself. In addition, during the two-week intervention period RAGT temporarily replaced, rather than supplemented, participants’ usual physiotherapy and/or occupational therapy, so the present findings reflect the short-term effects of using RAGT as a stand-alone modality. We therefore cannot determine whether similar or greater improvements would have occurred if standard care had been continued or if RAGT had been added on top of usual therapy. These factors significantly restrict the internal validity of the study, and consequently we cannot conclusively attribute the observed changes to RAGT alone. Future studies should aim to recruit larger and more heterogeneous cohorts, implement strategies to improve compliance (e.g., mock scanner training, child-friendly scanning environments, motion-reduction techniques), and consider analytic approaches capable of dealing with partial or missing data.
Second, although we used well-established, objective walking assessments (6MWT, 10MWT, GAITRite) that are standard and reproducible, we did not include standardized clinical scales or patient- and caregiver-reported outcome measures such as the GMFCS, the PEDI, or parent questionnaires. As a result, the functional relevance of the observed gait improvements cannot be directly quantified in terms of overall gross motor function, everyday activities, participation, or quality of life. This limitation also prevented us from examining how changes in objective gait parameters and fMRI activation patterns relate to perceived functional gains. Future trials should adopt a more comprehensive outcome framework that combines performance-based measures, clinical scales, and patient- or caregiver-reported outcomes to better capture the clinical significance of RAGT-induced changes and to strengthen the link between neural reorganization and real-world functional improvements.
Third, several methodological aspects of the neuroimaging component warrant consideration. While fMRI provides valuable insights into brain activation patterns, it does not capture other aspects of neural function such as connectivity or structural integrity. In addition, the fMRI analyses were performed using repeated-measures ANOVA models that included LESION TYPE as a between-subject factor. Given the very small overall sample (N = 6) and the unequal subgroup sizes (n = 4 with subcortical lesions and n = 2 with subcortical lesions plus hydrocephalus), the statistical power to detect and reliably estimate higher-order interactions (e.g., TIME × LIMB × LESION TYPE) is extremely limited. Consequently, even when interaction terms reached conventional significance thresholds, these effects should be interpreted as preliminary, hypothesis-generating trends that require replication in larger and more balanced cohorts. Moreover, ankle dorsiflexion during fMRI was standardized by pacing at 1 Hz and by prior training, but range of motion, force production, and muscle activity were not measured instrumentally inside the scanner. It is therefore possible that participants generated larger or more effortful movements at T1 than at T0, and part of the observed increase in BOLD activation might reflect increased motor output rather than, or in addition to, training-induced changes in neural efficiency or network organization. Combining fMRI with other modalities, such as diffusion tensor imaging (DTI) or electroencephalography (EEG), could offer a more comprehensive understanding of the neural mechanisms underlying motor recovery. Furthermore, longitudinal follow-up assessments would help determine the durability of the observed changes and their relevance to long-term functional outcomes. Finally, the specificity of the motor tasks used during fMRI acquisition warrants consideration. In this study, ankle dorsiflexion was selected as the lower limb task, while finger tapping served as a control for upper limb activation. Although this approach is supported by prior research (Phillips et al., 2007), it may not fully capture the complexity of gait-related motor control. Future studies could incorporate more ecologically valid tasks or use virtual reality paradigms to simulate walking within the scanner environment.
From a clinical perspective, the findings of this pilot study support the potential use of RAGT as a valuable tool in the rehabilitation of children with spastic hemiplegic CP. The observed improvements in gait performance and the associated neuroplastic changes suggest that RAGT may enhance motor function and may promote reorganization within the central nervous system. This dual pattern is particularly relevant in pediatric populations, where early intervention can have lasting effects on developmental trajectories (Novak et al., 2020).
Moreover, the differential response observed between children with subcortical lesions and those with hydrocephalus highlights the need for personalized rehabilitation strategies. Neuroimaging may play a key role in identifying candidates most likely to benefit from RAGT and in monitoring treatment progress. As the field moves toward precision rehabilitation, integrating clinical, functional, and neuroimaging data will be essential for optimizing outcomes.
In conclusion, this study provides preliminary evidence that RAGT can be associated with both functional and neurophysiological improvements in children with spastic hemiplegic CP. The combination of enhanced gait performance and increased activation in motor-related brain regions is consistent with a role of RAGT in promoting neuroplasticity. While further research is needed to confirm and extend these findings, the results underscore the potential of robotic technologies to contribute to pediatric neurorehabilitation and, ultimately, to improve the lives of children with CP.
Footnotes
Acknowledgments section
None
Ethical Approval and Informed Consent Statements
The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Review Board of the Department of Neurosciences, Biomedicine, and Movement Sciences at the University of Verona (protocol code 206/10). Written informed consent was obtained from all participants prior to enrollment.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available on request from the corresponding author.