
Abstract
Objectives
Traumatic brain injury (TBI) is a leading cause of long-term disability. This study aimed to evaluate the effectiveness of a Post-Acute Care (PAC) program for patients with TBI in Taiwan and to identify the independent predictors associated with the magnitude of their functional recovery.
Methods
This retrospective cohort study included 168 patients with TBI admitted to a PAC program from a tertiary medical center. The primary outcome was the change score in the Barthel Index (BI)(ADL). The Wilcoxon Signed-Rank Test was used to assess changes in functional scores (BI(ADL), IADL, and EQ-5D) from admission to discharge.
Results
Patients demonstrated statistically significant improvements across all functional measures after the PAC intervention, including the BI(ADL), IADL, and EQ-5D (all p < .001). After adjusting for all covariates, length of stay was the sole significant independent predictor of the BI(ADL) change score (B = 0.309, p < .001), indicating that for each additional day of PAC, a patient's BI score was expected to improve by 0.309 points.
Conclusion
Post-Acute Care is a highly effective intervention for improving functional outcomes in patients with TBI. These findings provide a strong evidence base for clinicians to advocate for sufficient rehabilitation time and for policymakers.
Keywords
Introduction
Traumatic brain injury (TBI) represents a significant global public health challenge (James et al., 2021). The 2021 Global Burden of Disease Study reported approximately 20.84 million new cases of TBI worldwide, placing substantial economic and long-term care demands on societies globally (Hyder et al., 2007). The situation in Taiwan reflects this trend, with an estimated 333 TBI diagnoses per 100,000 emergency room visits annually (Wang et al., 2012).
The Taiwanese healthcare system, under the Taiwan Diagnosis-Related Groups (Tw-DRGs) payment system, often results in short acute hospital stays. This policy of early discharge frequently creates a critical care gap, leaving patients and their families unprepared to manage the complex transition from hospital to home (Luo et al., 2012; Wu, 2008), often leading to an increased need for long-term care services(Ding et al., 2016). This highlights the necessity of a structured transitional care program, as early discharge without adequate follow-up may merely shift healthcare costs rather than reducing the overall economic burden (Figueroa et al., 2021).
The key distinction between traditional inpatient rehabilitation and PAC rehabilitation lies in the latter's structured, multidisciplinary team approach, which includes physicians, physical therapists, occupational therapists, nurses, social workers, as well as medical and nutritional consultants. In addition, PAC patients benefit from comprehensive and highly individualized rehabilitation programs (Yang et al., 2021).
During the initial hospitalization, patients typically receive approximately 20 min of rehabilitation per day for a duration of 5 to 7 days. In contrast, PAC rehabilitation can provide 3 to 4 therapy sessions per day, each lasting up to one hour, thereby substantially enhancing rehabilitation potential.
The purpose of post-acute care (PAC) is to facilitate the recovery of functional independence among older adults or patients with disabilities, reduce the risk of hospital readmission, and prevent premature institutionalization. Domestic studies have shown that patients receiving PAC demonstrate greater functional improvement, lower 14-day and 30-day readmission rates, and reduced mortality compared with those not enrolled in PAC programs (Han, 2015; Yang et al., 2021).
To address this gap, Taiwan's National Health Insurance (NHI) has progressively implemented a post-acute care (PAC) model to bridge the transition from acute hospitalization to the community (Wang et al., 2017). Initially piloted for stroke patients, the PAC program aims to provide intensive, individualized rehabilitation during the critical recovery period, with the goal of restoring function and reducing hospital readmissions(Ministry of Health and Welfare, National Health Insurance Administration, 2017). While the effectiveness of PAC has been established for conditions like stroke in Taiwan, there remains a significant lack of research specifically evaluating the functional recovery outcomes for patients with TBI within this framework(Ouslander & Mandi, 2019.
Furthermore, identifying the key drivers of successful rehabilitation is crucial for optimizing care. International studies have indicated that the duration and efficiency of rehabilitation are critical variables. A large-scale study of top-tier TBI rehabilitation centers in the United States found that even after adjusting for patient severity, significant variations in outcomes remained, with the duration of inpatient rehabilitation being a key explanatory factor (Dahdah et al., 2014). This suggests a potential dose-response relationship in TBI rehabilitation that warrants further investigation within Taiwan's PAC system. At present, Taiwan's national policy stipulates that post-acute care for traumatic brain injury (TBI) is provided for an initial period of 3 to 6 weeks. For patients who are assessed by the post-acute care team as having ongoing care needs, the care period may be extended once, with a maximum total duration of up to 12 weeks.
Therefore, this study aimed to evaluate the effectiveness of a PAC program for patients with TBI in Taiwan and to explore the length of hospital stay associated with the greatest functional improvement, thereby informing potential adjustments to national policy programs. The primary objectives were: (1) to quantify the changes in functional status following PAC intervention; and (2) to identify the independent predictors, with a particular focus on the role of length of stay, that are associated with the degree of functional improvement.
Methods
Study Design and Setting
This study employed a retrospective cohort design to evaluate functional outcomes in patients with TBI following PAC. The study aimed to quantify the degree of improvement and identify independent predictors associated with functional recovery. Data were sourced from a tertiary medical center in central Taiwan with an established and integrated PAC network.
Study Population and Sample
We retrospectively reviewed the electronic medical records and PAC program database for all patients admitted between May 12, 2022 and May 11, 2023. Patients were included if they met the following criteria: (1) aged 18 years or older with a primary diagnosis of TBI; (2) presented with moderate functional disability at admission, defined by a Barthel Index (BI) (ADL) score between 40 and 70; (3) were medically stable and deemed to have rehabilitative potential by the clinical team; and (4) had sufficient family or caregiver support. Patients were excluded if they had a concurrent unstable spinal cord injury, a severe psychiatric disorder, long-term ventilator dependency, or a terminal illness. After applying these criteria, a total of 168 patients with complete data were included in the final analysis.
Data Collection and Variables
Data were retrospectively collected through a structured review of patient medical charts. The following variables were extracted:
Demographics: Age, gender, education level, marital status, employment status, current smoking status, and alcohol consumption habits. Clinical Characteristics: Length of stay in the PAC program, and comorbidities such as hypertension, diabetes, and kidney disease. Functional Outcome Measures: Scores from the BI(ADL), the Lawton-Brody Instrumental Activities of Daily Living (IADL) Scale, and the EuroQoL-5D (EQ-5D) were recorded at both admission to and discharge from the PAC program.
Outcome Measures
The primary outcome of this study was the change score in the BI(ADL), calculated as the BI(ADL) score at discharge minus the BI(ADL) score at admission. Secondary outcomes included the change scores for the IADL and EQ-5D, calculated in the same manner.
Statistical Analysis
All statistical analyses were performed using SPSS software (Version 29.0, IBM Corp., Armonk, NY). A two-sided p-value of < .05 was considered statistically significant. The analytical process was structured as follows:
Descriptive Statistics: Continuous variables were presented as median and interquartile range (IQR), while categorical variables were presented as frequencies and percentages (n (%)). Overall Efficacy Analysis: The Wilcoxon Signed-Rank Test was used to compare the median scores of the three functional scales (BI(ADL), IADL, EQ-5D) between admission and discharge to evaluate the overall effectiveness of the PAC program. Univariate Analysis: To screen for factors associated with the primary outcome, Spearman's rank correlation was used for continuous predictors (e.g., age, length of stay), and the Mann-Whitney U test was used for binary categorical predictors (e.g., gender, presence of comorbidities). Multivariate Analysis: Variables with a p-value < .20 in the univariate analysis, along with the baseline BI(ADL) score, were entered into a multiple linear regression model to identify the independent predictors of the BI(ADL) change score. Receiver operating characteristic (ROC) analysis was used to identify key predictor variables and to determine optimal cutoff points by correlating them with subsequent BI (ADL), IADL, and EQ-5D outcomes. These cutoffs were used to predict the optimal length of stay in post-acute care (PAC). Model performance showed accuracies ranging from 0.75 to 0.76. The BI (ADL), IADL, and EQ-5D scores were most strongly associated with hospital length of stay, with cutoff values of 28.3, 34.3, and 34.8 days and corresponding AUCs of 0.783, 0.837, and 0.816, respectively. The results are shown in Figure 1.
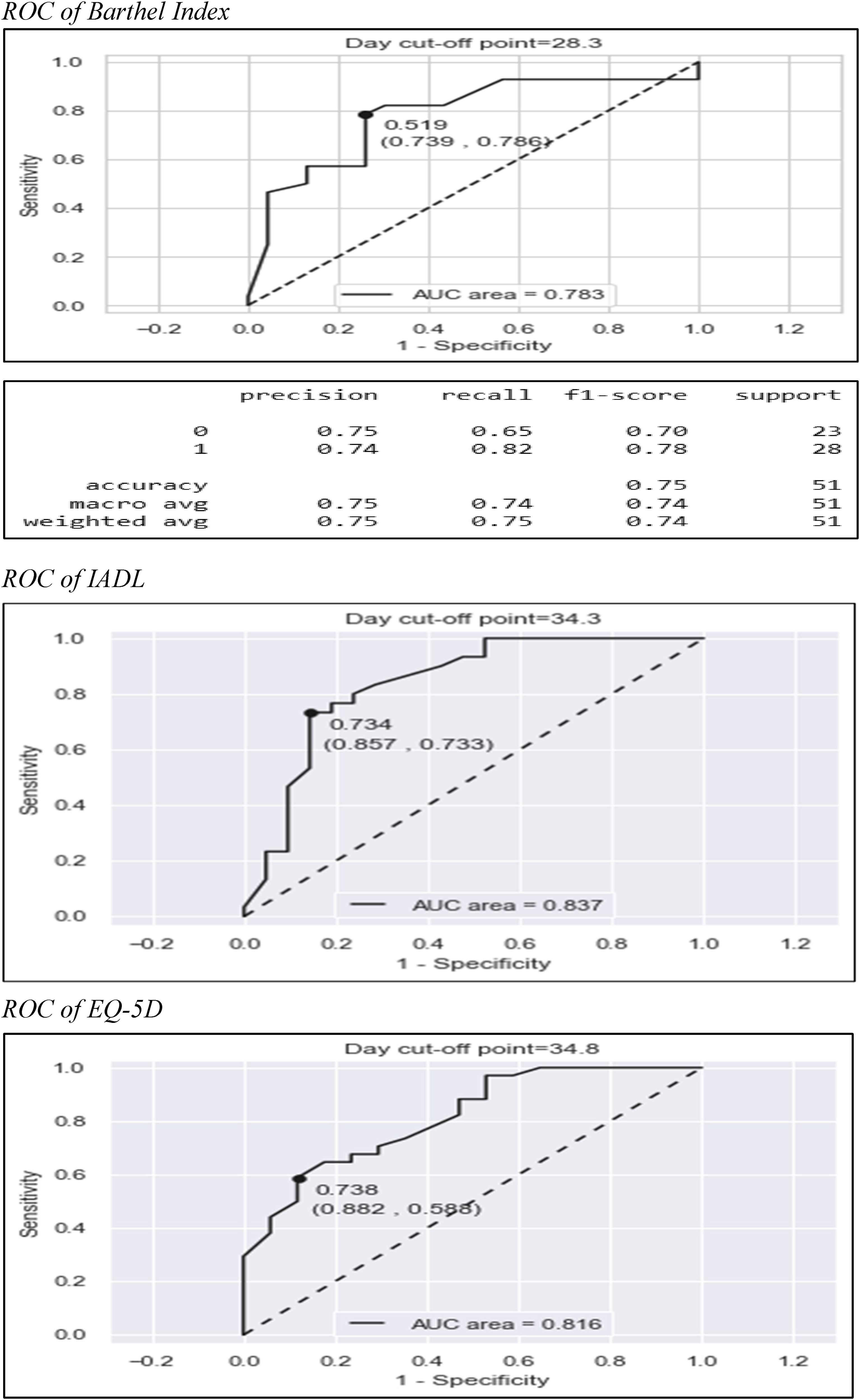
ROC of Barthel Index. Based on confusion matrix analysis, the optimal PAC length of stay was 28.3 days according to the Barthel Index (accuracy = 0.75), 34.3 days according to IADL (accuracy = 0.76), and 34.8 days according to EQ-5D (accuracy = 0.76), indicating moderate classification performance across outcome measures.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (IRB No: 220323). Due to the retrospective nature of the study and the use of de-identified data, the IRB granted a waiver of informed consent. All patient data were anonymized prior to analysis to ensure confidentiality.
Results
Patient Characteristics
A total of 168 patients with TBI undergoing PAC were included in this study. The median age of the cohort was 65 years, with 55.4% being male. On admission, patients generally presented with poor functional status, as indicated by a median BI(ADL) score of 40, signifying a state of severe dependence. The median length of stay in the PAC program was 31 days. Detailed demographic and clinical characteristics, along with descriptive statistics for all functional scales, are presented in Table 1.
Overview of Patient Characteristics (N = 168).
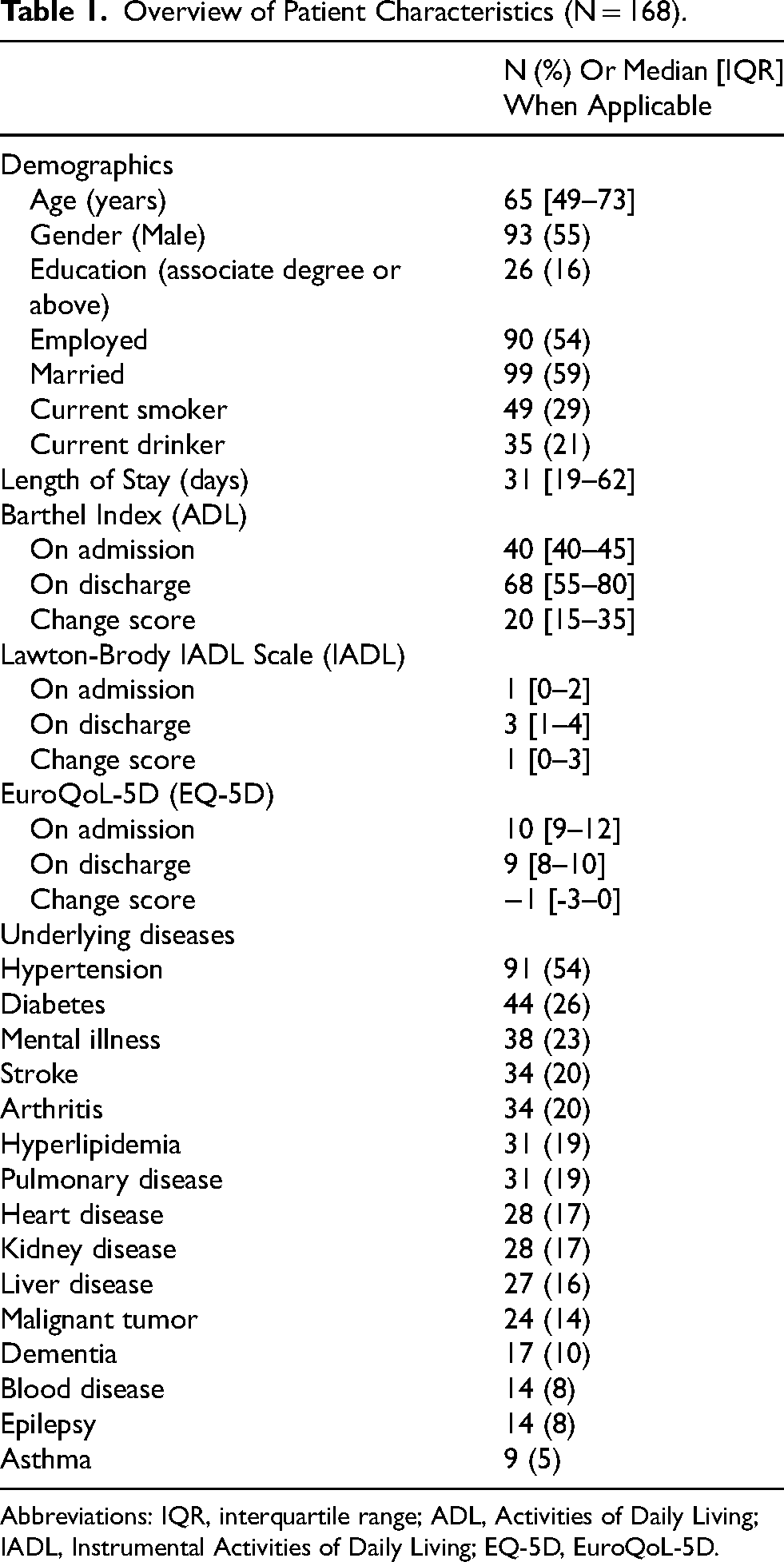
Abbreviations: IQR, interquartile range; ADL, Activities of Daily Living; IADL, Instrumental Activities of Daily Living; EQ-5D, EuroQoL-5D.
Overall Efficacy of Post-Acute Care
To evaluate the overall efficacy of the PAC program, the Wilcoxon Signed-Rank Test was used to compare patients’ functional scale scores at admission and discharge. The results revealed statistically significant improvements across all functional indicators following the PAC intervention. Specifically, the median BI(ADL) score significantly increased from 40 at admission to 68 at discharge (Z = 10.577, p < .001). Similarly, the median IADL score significantly improved from 1 to 3 (Z = 8.981, p < .001). Regarding quality of life, the EQ-5D score significantly decreased—indicating an improvement—with the median score dropping from 10 to 9 (Z = -9.312, p < .001).
Univariate Analysis of Functional Improvement
The study further explored potential factors associated with the BI(ADL) change score (Table 2). Spearman's rank correlation analysis revealed that age was significantly negatively correlated with the change score (ρ = -0.263, p < .001), whereas length of stay was significantly positively correlated (ρ = 0.551, p < .001). Furthermore, improvements in the BI(ADL) were highly correlated with improvements in the IADL (ρ = 0.535, p < .001) and EQ-5D (ρ = -0.474, p < .001). For categorical variables, the Mann-Whitney U test indicated that a higher level of education (p = .035) and the absence of kidney disease (p = .044) were associated with significantly greater BI(ADL) change scores.
Univariate Analysis of Change Score in Barthel Index(ADL) (N = 168).
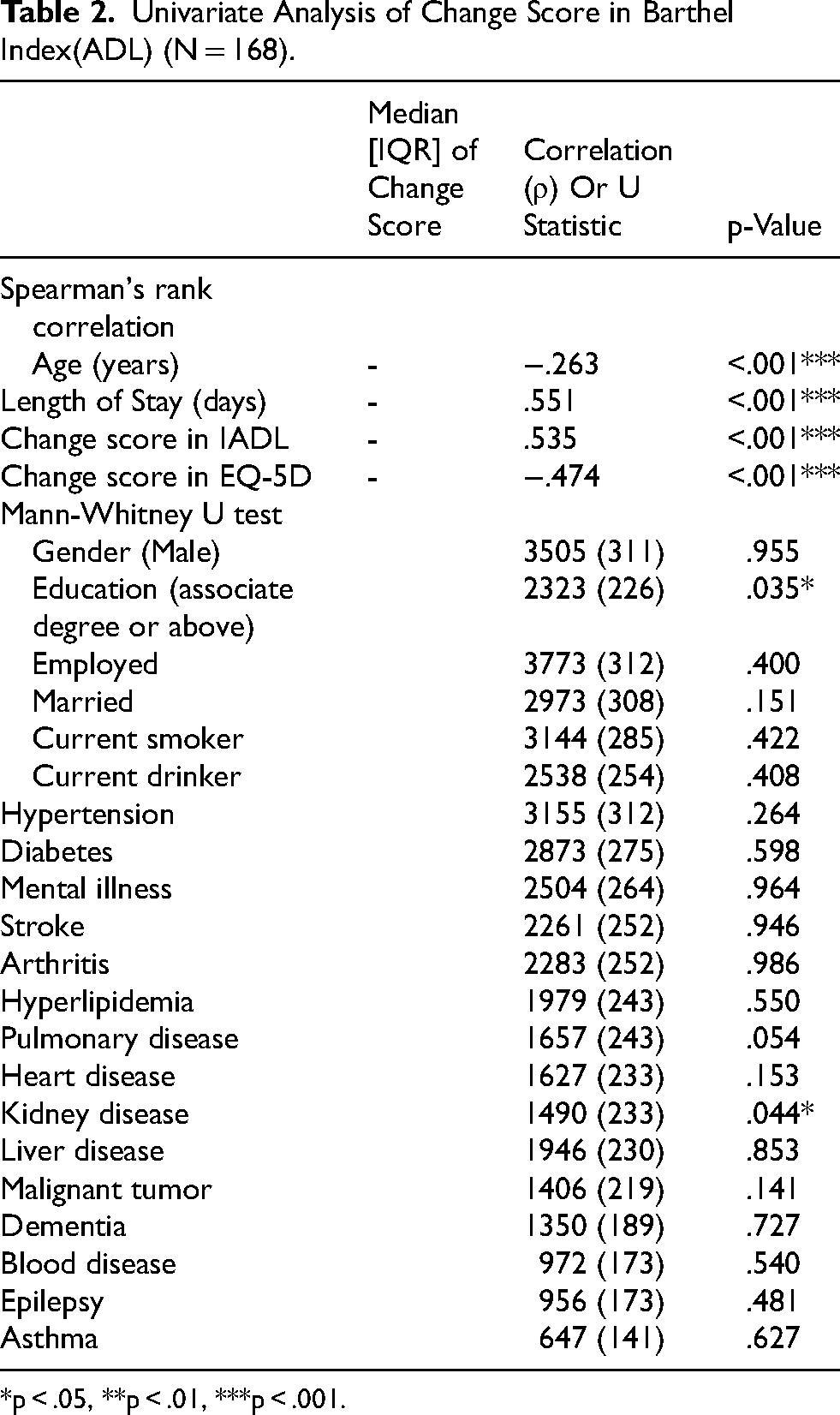
*p < .05, **p < .01, ***p < .001.
Independent Predictors of Functional Improvement
To identify independent predictors of the BI(ADL) change score, a multiple linear regression analysis was conducted (Table 3). The overall regression model was statistically significant (F (9, 158) = 9.627, p < .001) and explained 34.1% of the total variance in the BI(ADL) change score (Adjusted R2 = .341).
Multiple Linear Regression Predicting Change Score in Barthel Index (N = 168).
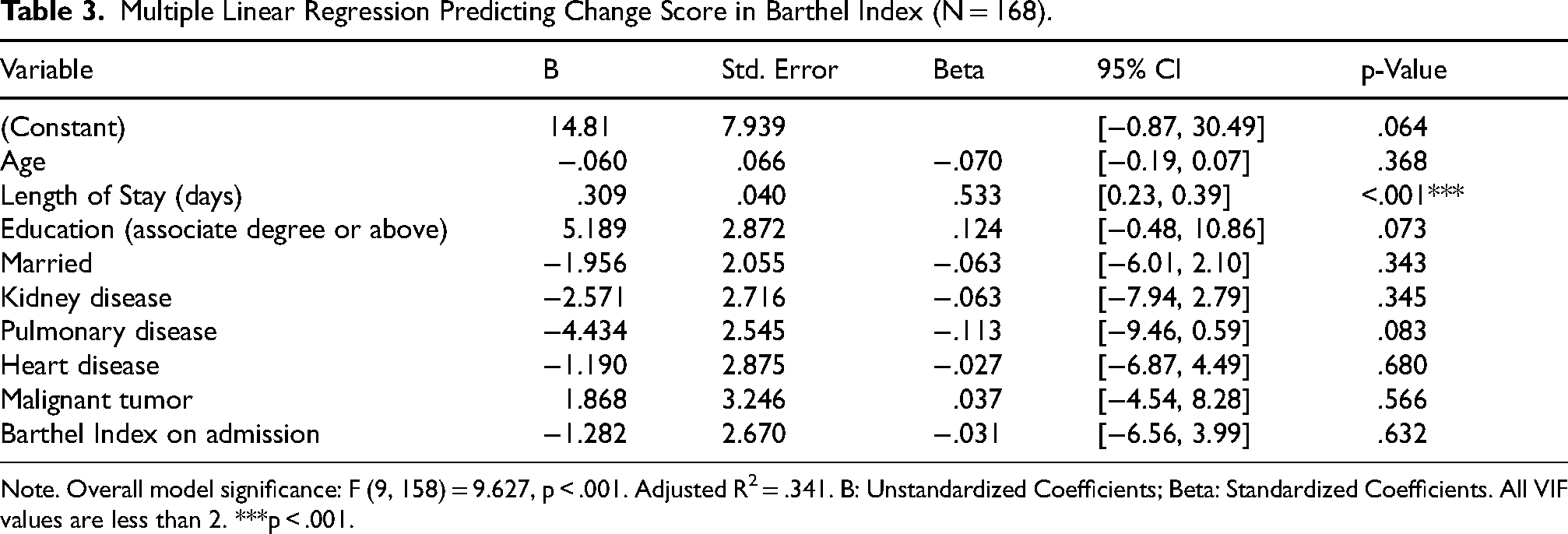
Note. Overall model significance: F (9, 158) = 9.627, p < .001. Adjusted R2 = .341. B: Unstandardized Coefficients; Beta: Standardized Coefficients. All VIF values are less than 2. ***p < .001.
After controlling for all variables in the model, length of stay emerged as the sole independent predictor to reach statistical significance (B = 0.309, p < .001). This result indicates that for each additional day in the PAC program, a patient's BI(ADL) score was expected to improve by 0.309 points, holding other factors constant. Notably, the significance of age and kidney disease, which was observed in the univariate analysis, disappeared in the multivariate model (p > .05), suggesting their initial associations were likely mediated or confounded by other factors included in the model, such as length of stay.
Discussion
Most existing studies have focused on patients with major conditions, such as traumatic brain injury (TBI), stroke, and hip fracture, who transition to post-acute, subacute, or mid-term care. These studies primarily examine functional recovery, long-term outcomes, care pathway selection, and cost-effectiveness, with further extensions to payment systems and national policy design. Evidence indicates that the absence of effective post-acute care (PAC) is associated with functional decline, disability, and an increased long-term care burden, whereas PAC has been shown to improve functional outcomes and prognosis. Moreover, payment mechanisms and policy design directly influence the accessibility, quality, and cost-effectiveness of PAC services. However, the optimal length of hospitalization during PAC remains insufficiently investigated.
In contrast to prior research, the present study focuses on examining the association between the length of stay in PAC and functional outcomes. In general, prolonged hospitalization may increase the risk of complications, such as infections, whereas excessively short hospital stays may be insufficient to achieve meaningful functional improvement.
This study aimed to evaluate the effectiveness of PAC for patients with TBI and to identify the key independent predictors of their functional recovery. Our findings demonstrate that PAC is a highly effective intervention, resulting in statistically significant improvements in patients’ activities of daily living (ADL), IADL, and quality of life. The most critical finding from our multivariate analysis is that length of stay was the sole, powerful independent predictor of the magnitude of functional improvement.
The central role of length of stay (B = 0.309, p < .001) provides strong quantitative evidence for a dose-response relationship in TBI rehabilitation; a longer duration of intensive therapy directly correlates with better functional outcomes. This finding carries significant clinical and policy implications, particularly within the context of Taiwan's DRGs payment system, which incentivizes shorter acute hospitalizations. This result is consistent with a large-scale study by Dahdah et al. (2014), which examined top-tier TBI rehabilitation centers in the U.S. and found that the duration of inpatient rehabilitation was a key variable explaining outcome differences, even after adjusting for patient severity (Dahdah et al., 2014; Wu et al., 2014). Furthermore, research on Taiwan's PAC program for stroke by Wang et al. (2017) noted that earlier transfer to PAC was associated with lower total costs, underscoring the importance of a well-structured care continuum where an adequate duration of PAC is essential to effectively manage patients discharged from the acute care system (Wang et al., 2017).
An insightful finding of this study was the role of confounding variables. While factors such as age and the presence of kidney disease were significantly associated with recovery in the univariate analysis, their predictive power disappeared in the multiple linear regression model. This suggests their initial association with poorer outcomes was likely mediated or confounded by other factors, such as a shorter length of stay. This phenomenon is not uncommon in prognostic research; for instance, a meta-analysis by Watson et al. (2020) on non-traumatic brain injury also found that certain cognitive predictors lost their independent predictive power in multivariate models (Watson et al., 2020). This highlights the importance of multivariate analysis in isolating the true drivers of recovery.
To our knowledge, this is one of the few studies in Taiwan to specifically quantify the effectiveness of PAC for a TBI cohort (Chien et al., 2020). Our results, which show significant and continuous functional gains, align with the natural recovery trajectory observed in prospective TBI studies, such as the one by de Oliveira et al. (2022), which noted the most pronounced recovery occurs in the first three months post-injury (de Oliveira et al., 2022). This reinforces that the post-acute phase is a critical window for recovery and that structured interventions like PAC are designed to maximize this potential.
The strengths of this study include a well-defined cohort and the use of a robust statistical plan, including a multiple linear regression model that controlled for multiple potential confounders. However, several limitations must be acknowledged. First, the retrospective design allows us to identify associations but not to establish causality. Second, being a single-center study, the findings may not be fully generalizable to other healthcare settings. Finally, despite controlling for numerous variables, there may be unmeasured confounders (e.g., cognitive status, social support intensity) that could also influence recovery outcomes.
Conclusion
In conclusion, this study provides strong evidence that Post-Acute Care is a highly effective intervention for promoting functional recovery in patients with traumatic brain injury. Our analysis demonstrated significant improvements across all functional domains, and crucially, identified that the length of stay in the PAC program was the sole independent predictor of the magnitude of this recovery. This highlights a clear dose-response relationship where a longer duration of care corresponds to greater functional gains.
These findings underscore the importance of providing an adequate period of intensive rehabilitation tailored to the needs of patients with TBI. This evidence serves as a critical reference for clinicians in discharge planning and for policymakers to consider when structuring healthcare policies, advocating for a focus on individualized rehabilitation needs rather than rigid, predetermined care durations. By quantifying the benefits of PAC for this specific population, our study reinforces the vital role of integrated transitional care in bridging the gap between acute hospitalization and a successful return to the community.
Footnotes
Abbreviations
Acknowledgments
Our team would like to thank Hao-Zhi Yin provided statistical analysis and support.
Ethics Approval and Consent to Participate
The Institutional Review Board (IRB) of Changhua Christian Hospital approved this retrospective cohort study, which was performed in the Changhua Christian Hospital affiliated PAC facility. The study was retrospective in nature and the personal information of each patient has been decoded from the raw datasets upon data analysis and discussion. This part has been approved by the IRB of Changhua Christian Hospital and waived the informed consent.
Consent for Publication
Consent was obtained from all authors to publish this retrospective queue study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Ju-Lan Yang, MS: Study design, bio-statistical analysis, manuscript writing, validation, data proofing, IRB preparation.
Ying-Lin Hsu, PHD: Data collection, validation, manuscript writing, bio-statistical analysis.
Chih Ming Lin, MD, MPH, PHD: Bio-statistical analysis, data collection, manuscript writing.
Ruoh-Lih Lei, PHD: data proofing, manuscript writing.
Chih Hao Lin, PhD: Bio-statistical analysis, manuscript writing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.