
Abstract
Purpose
The longitudinal effects of combining intensive speech therapy (ST) with two separate courses of high-frequency repetitive transcranial magnetic stimulation (HF-rTMS) for aphasia remain unclear. This study retrospectively investigated longitudinal changes in language function in patients who underwent this combined protocol.
Methods
Sixteen patients with chronic aphasia underwent two courses of 2-week inpatient treatment combining fMRI-guided HF-rTMS and intensive ST between April 2018 and February 2025. The Standard Language Test of Aphasia (SLTA) total and modality-specific raw scores were assessed at four time points: at the 1st admission, 3 months after the 1st discharge, at the 2nd admission, and 3 months after the 2nd discharge.
Results
The mean SLTA total raw score significantly improved over time: 147 ± 51.6 at the 1st admission, 157 ± 49.9 at 3 months after the 1st discharge, 159 ± 48.8 at the 2nd admission, and 163 ± 50.2 at 3 months after the 2nd discharge. Significant improvements in speech function were observed in the Overall, Fluent Aphasia, and Non-fluent Aphasia groups. Notably, therapeutic effects were maintained without decline between the two admissions.
Conclusions
Two courses of HF-rTMS combined with intensive ST may be effective for the long-term improvement of language function, particularly speech function, in patients with chronic aphasia.
Introduction
Aphasia is one of the major sequelae following stroke, impairing all language modalities: listening, speaking, reading, and writing. Aphasia occurs in approximately 30% of stroke patients (Dickey et al., 2010). Aphasia causes depression, communication disorders, decreased activity, and a reduction in social networks, significantly negatively affecting health-related quality of life (HRQOL). Furthermore, these impairments are long-lasting and have a significant impact on family life and social participation (Ohata & Yoshino, 2015).
In recent years, repetitive transcranial magnetic stimulation (rTMS) has been applied as a non-invasive treatment for post-stroke aphasia, and its therapeutic effects are being examined both in Japan and internationally (Naeser et al., 2005; Kakuda et al., 2010; Abo et al., 2012; Zumbansen et al., 2022; Ohara et al., 2021). Systematic reviews have reported that rTMS is effective for treating post-stroke motor paralysis, depression, and aphasia (Lefaucheur et al., 2020). Clinically, rTMS is generally considered to have inhibitory effects on the cerebral cortex at low-frequency stimulation (1 Hz) and excitatory effects at high-frequency stimulation (e.g., 10 Hz) (Maeda et al., 2000; Klomjai et al., 2015).
Various validations of rTMS treatment for aphasia have been conducted from perspectives such as stimulation frequency and aphasia type. Previous studies combining low-frequency rTMS and ST based on brain activation findings during language tasks using functional MRI (fMRI) have reported significant improvements in auditory comprehension, reading comprehension, and repetition in patients with non-fluent aphasia, and in spontaneous speech in patients with fluent aphasia (Abo et al., 2012). Reports on low-frequency rTMS for patients with sensory aphasia have also observed improvements in speech function (Kakuda et al., 2010). Additionally, studies examining the effects of low-frequency rTMS on patients with subacute global aphasia reported significant improvements in Aphasia Quotient (AQ), spontaneous speech, auditory comprehension, and repetition scores on the Western Aphasia Battery (WAB) (Ren et al., 2019).
While many reports on rTMS treatment for aphasia involve low-frequency stimulation at 1 Hz, reports on treatment using high-frequency stimulation, such as 10 Hz, have been increasing in recent years. A report examining the combined effect of HF-rTMS and intensive ST stated that the Standard Language Test of Aphasia (SLTA) total raw score improved 3 months after admission compared to admission (Ohara et al., 2021).
Although previous studies suggest the efficacy of rTMS (Hara & Abo, 2021), most are examinations of a single course of inpatient treatment (1 session), and there are few reports on multiple interventions. In particular, it is not clear how language function changes over the long term when intensive ST is combined with two courses of HF-rTMS inpatient treatment. We believe that examining the effects of multiple courses of rTMS treatment and intensive rehabilitation can provide important findings for treatment planning and patient explanations. The purpose of this study was to retrospectively investigate cases that underwent two courses of HF-rTMS treatment and intensive ST and to examine changes in language function.
Materials and Methods
Study Design
This study is a retrospective observational study.
Subjects
Between April 2018 and February 2025, 111 patients visited the Department of Rehabilitation Medicine at our hospital, were judged to meet the indication criteria for aphasia rTMS treatment (Figure 1), and completed the inpatient treatment protocol combining HF-rTMS and ST. Of these, 16 patients (11 males, 5 females) who underwent two courses of inpatient treatment were included in the analysis, excluding those with a history of low-frequency rTMS treatment or missing data.
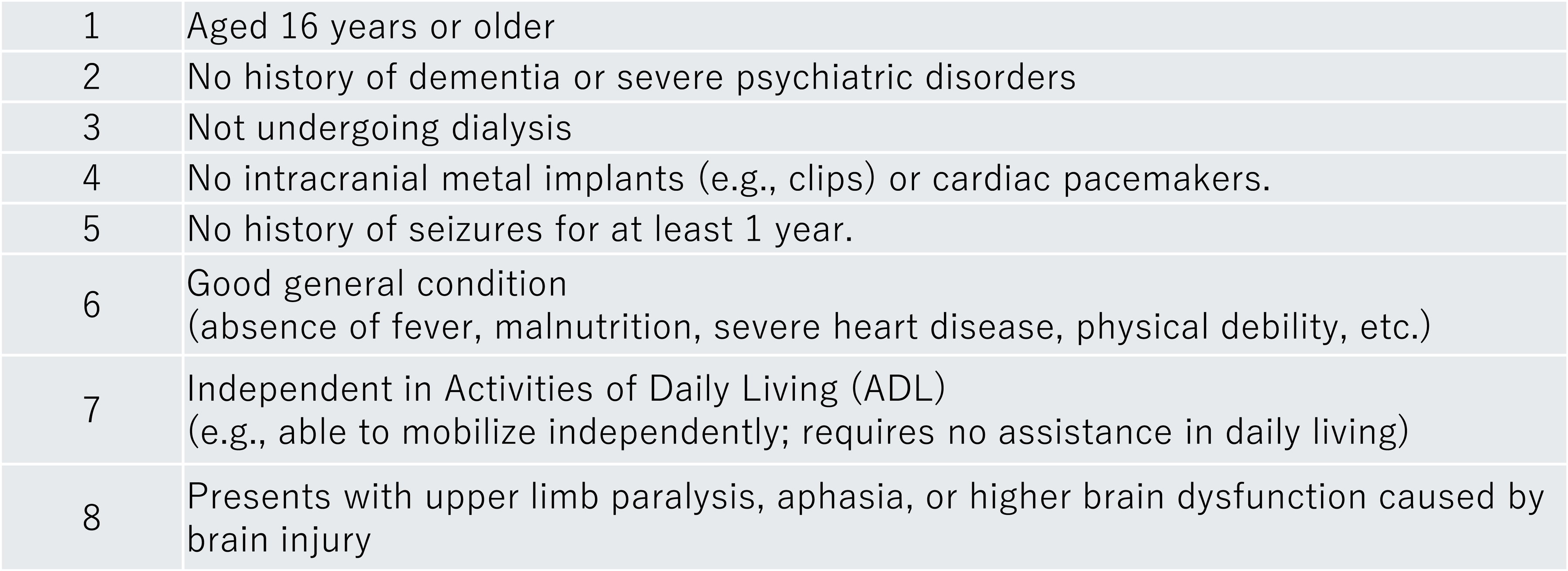
Indication criteria for rTMS Treatment of Aphasia.
Methods
rTMS Inpatient Protocol
The treatment flow at our hospital is as follows. After being diagnosed as indicated for treatment by a physician in our department, fMRI was performed before admission. A repetition task was used in fMRI to evaluate language function activation sites. Based on the evaluation results, the rTMS stimulation site was determined from either the left/right inferior frontal gyrus or the left/right angular gyrus (Ohara et al., 2021). Inpatient treatment was conducted for 2 weeks (every day except Sundays), combining HF-rTMS and intensive ST. The schedule is shown in Figure 2. HF-rTMS was performed in the morning, followed immediately by intensive ST, and additional ST was performed in the afternoon for a total of 120 min. For the delivery of HF-rTMS, a MagPro R30 stimulator (MagVenture Company, Denmark) equipped with a figure-of-eight 70 mm stimulating coil was used. One HF-rTMS session at 10 Hz included 2,400 pulses (total during admission: 28,800 pulses).
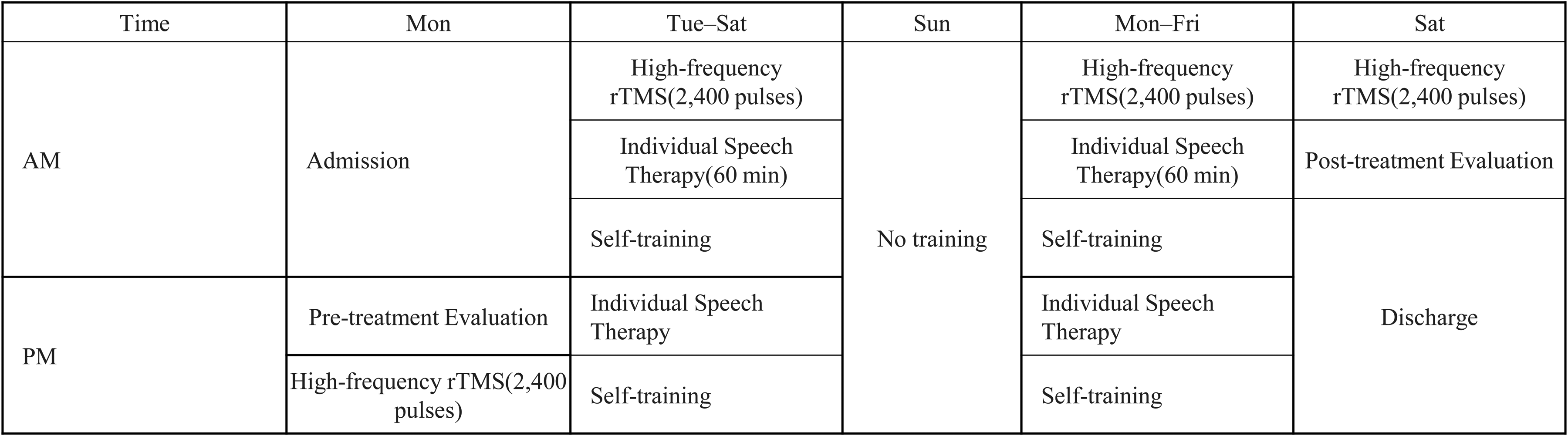
Inpatient Schedule for rTMS Treatment of Aphasia.
fMRI Data Acquisition and Analysis
MRI Data Acquisition
MRI data were acquired using a 3-Tesla MRI scanner (Signa Premier; GE Healthcare, Chicago, IL, USA) equipped with a 48-channel head coil. Functional MRI (fMRI) images were obtained using a gradient-echo echo-planar imaging (EPI) sequence combined with Hyperband (multiband) technology. The imaging parameters were as follows: repetition time (TR) = 1000 ms, echo time (TE) = 30 ms, flip angle = 60°, field of view (FOV) = 220 × 220 mm, matrix size = 64 × 64, and slice thickness = 3.0 mm (no gap). Fifty-one axial slices covering the whole brain were acquired, with 480 volumes per run. High-resolution 2D T1-weighted SPGR (Spoiled Gradient Recalled) images were acquired for anatomical reference with the following parameters: TR = 400 ms, TE = 4.25 ms, flip angle = 90°, FOV = 220 mm, slice thickness = 1.0 mm (no gap), and 152 slices.
ffMRI Task
Participants performed a language repetition task inside the scanner using a block design alternating between task blocks and rest blocks. Each trial within a task block consisted of a “listening” phase (4 s) and a “repetition” phase (5 s). Participants were instructed to listen to short sentences or word sequences presented through headphones during the listening phase and then vocalize (repeat) them during the subsequent repetition phase. The difficulty of the stimuli (e.g., 2-word or 3-word sentences) was individually adjusted to a performable level according to each participant's language function and severity. The stimuli were recorded by a professional announcer with clear articulation, and several patterns were created and used for randomization. The same task protocol was used for both fMRI sessions for each subject.
fMRI Data Analysis
Image preprocessing and statistical analysis were performed using SPM12 (Wellcome Trust Centre for Neuroimaging, London, UK) running on MATLAB. For preprocessing, realignment and unwarp procedures were performed to correct for head motion and susceptibility distortions. The T1-weighted images were co-registered to the mean functional image after correction. Subsequently, spatial smoothing was applied using a Gaussian kernel with a full-width at half-maximum (FWHM) of 8 mm. Statistical analysis was conducted in each participant's native space without normalization to a standard brain to preserve individual anatomical details. A general linear model was used to estimate brain activity related to the “listening” and “repetition” conditions. To remove the effects of head motion, six rigid-body transformation parameters were included in the model as covariates. A high-pass filter with a cutoff period of 240 s was applied to remove low-frequency noise. As the primary objective of this study was to evaluate brain activity during speech production, the analysis focused mainly on the “repetition” condition. Statistical significance was assessed using Family-Wise Error (FWE) correction for multiple comparisons, with a significance level set at p < 0.05.
Intensive Speech Therapy
ST was conducted in a one-on-one format by a speech-language-hearing therapist for a total of 120 min: 60 min in the morning and 60 min in the afternoon. The training content included oral expression exercises such as naming, repetition of words to short sentences, and reading aloud, as well as practical communication exercises including news summaries and PACE (Promoting Aphasics’ Communicative Effectiveness). Each task was adjusted for difficulty to ensure sufficient speech volume regardless of the severity of aphasia.
Outcome Measures
Age, sex, diagnosis, and time from onset to admission (in months) were investigated as basic attributes. Speech fluency and SLTA were used to evaluate language function. For SLTA, the total raw score of all items and raw scores by modality (Listening, Speaking, Reading, Writing) were calculated. The survey time points were: at the 1st admission, 3 months after the 1st discharge, at the 2nd admission, and 3 months after the 2nd discharge. Additionally, the rTMS stimulation sites at the 1st and 2nd admissions were investigated.
Statistical Analysis
Analysis was performed by classifying subjects into an Overall Group, a Fluent Aphasia Group, and a Non-fluent Aphasia Group. The Linear Mixed-Effects Model (LMM) analysis for the Overall Group was used to compare SLTA total raw scores and modality-specific raw scores at the four time points in each group. The estimated mean differences (Estimate) and Bonferroni-corrected p-values are reported for comparisons against the baseline (1st admission: T1) and the significance level was set at less than 5%. This study was conducted with the approval of the Ethics Committee of The Jikei University School of Medicine (Approval No. 32-338: 10423). Oral and written consent was obtained from all cases.
Results
Patient Characteristics
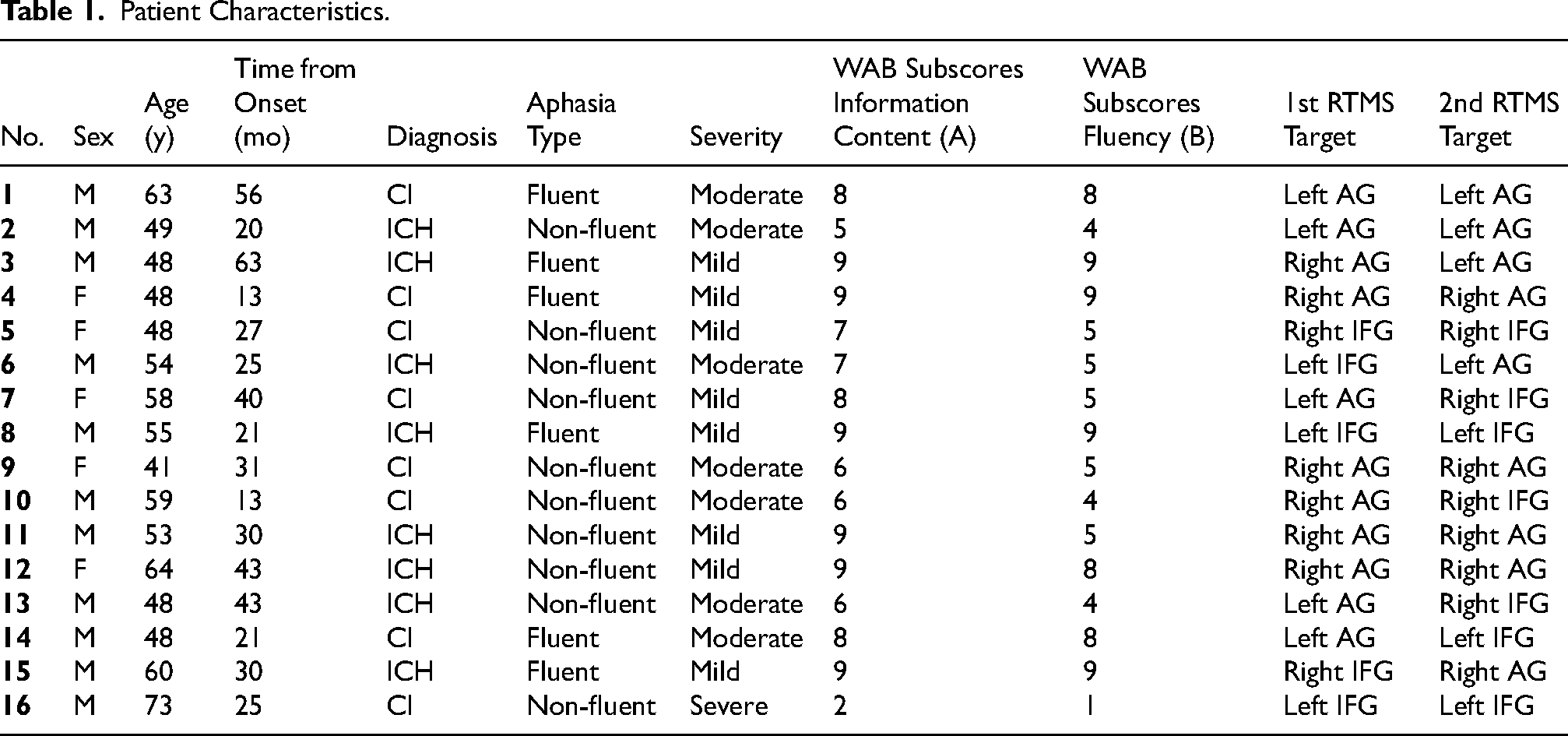
Table 1 shows the demographic and clinical characteristics of the 16 patients included in the analysis. The mean age at the first admission was 54.3 ± 7.9 years. The diagnoses included cerebral infarction in 8 patients and cerebral hemorrhage in 8 patients. The mean interval from the first admission to the second admission was 13.9 ± 17.6 months. Regarding aphasia severity, 8 patients were mild, 7 were moderate, and 1 was severe based on the SLTA. In terms of WAB subscores at baseline, the median score for Information Content (A) was 8 (range: 2–9), and for Fluency (B) was 8 (range: 1–9), reflecting the diversity of aphasia types in our cohort.
Patient Characteristics.
Longitudinal Changes in Language Function (LMM Analysis)
Table 2 shows the longitudinal changes in SLTA scores and the results of the LMM analysis for the Overall Group (n = 16). The estimated mean differences (Estimate) and Bonferroni-corrected p-values are reported for comparisons against the baseline (1st admission: T1).
Longitudinal Changes in Language Function.
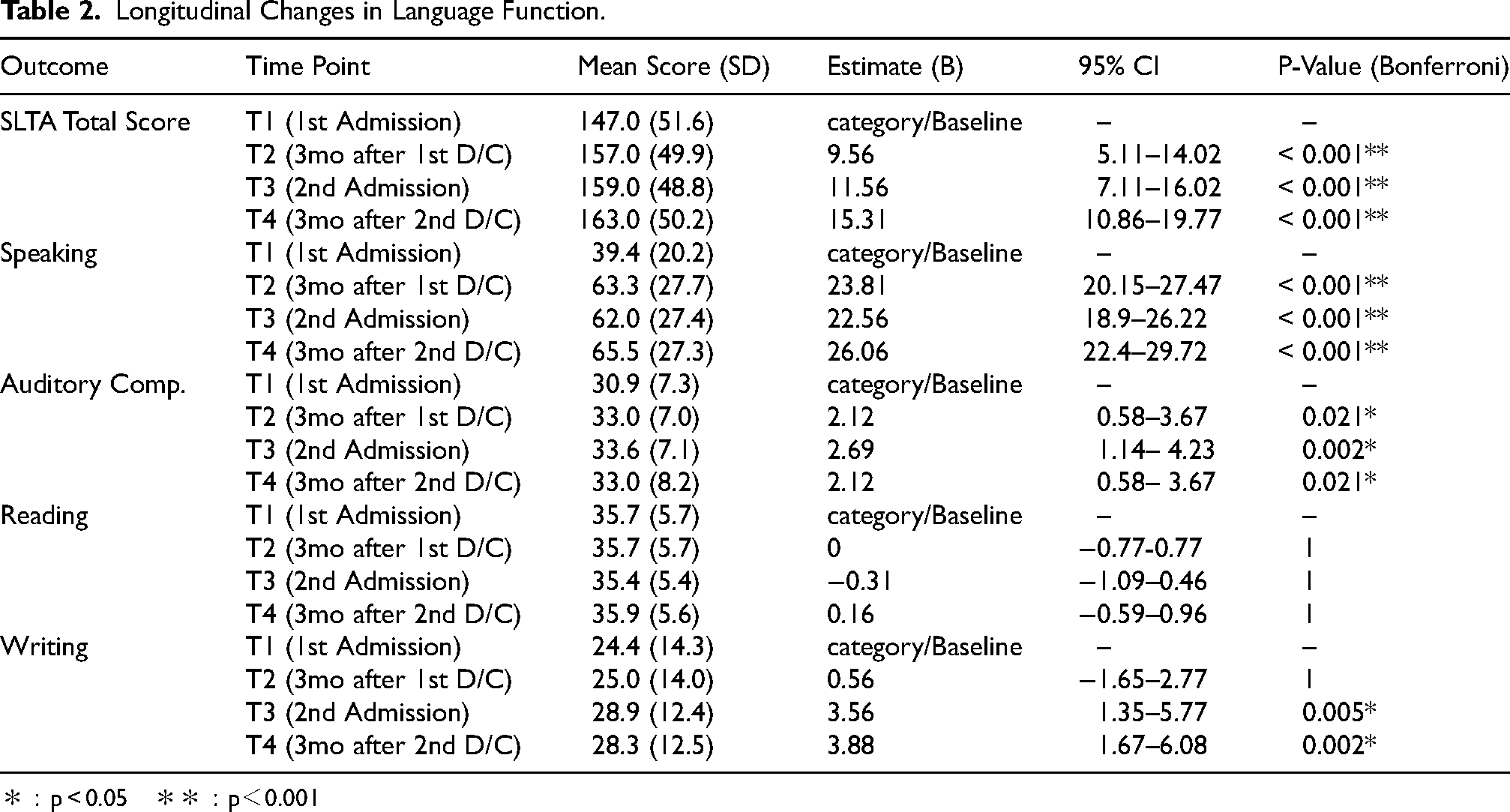
*:p < 0.05 **:p<0.001
SLTA Total Score: The total score showed significant improvement at all subsequent time points compared to T1. Specifically, significant increases were observed at 3 months after the 1st discharge (T2: Estimate = 9.56, p < 0.001), at the 2nd admission (T3: Estimate = 11.56, p < 0.001), and at 3 months after the 2nd discharge (T4: Estimate = 15.31, p < 0.001).
Speaking (Speech Function): Consistent with our hypothesis, the “Speaking” modality demonstrated the most robust and highly significant improvements at all time points. Large estimated gains were observed at T2 (Estimate = 23.81, p < 0.001), T3 (Estimate = 22.56, p < 0.001), and T4 (Estimate = 26.06, p < 0.001).
Auditory Comprehension: Significant improvements were observed at T2 (p = 0.021), T3 (p = 0.002), and T4 (p = 0.021) compared to T1.
Writing: Notably, the “Writing” score showed significant improvements at the 2nd admission (T3: Estimate = 3.56, p = 0.005) and at the final evaluation (T4: Estimate = 3.88, p = 0.002) compared to T1.
Subgroup Analysis
The results for the Fluent and Non-fluent subgroups are summarized in Table 3 and Table 4, respectively.
Fluent Subgroup.
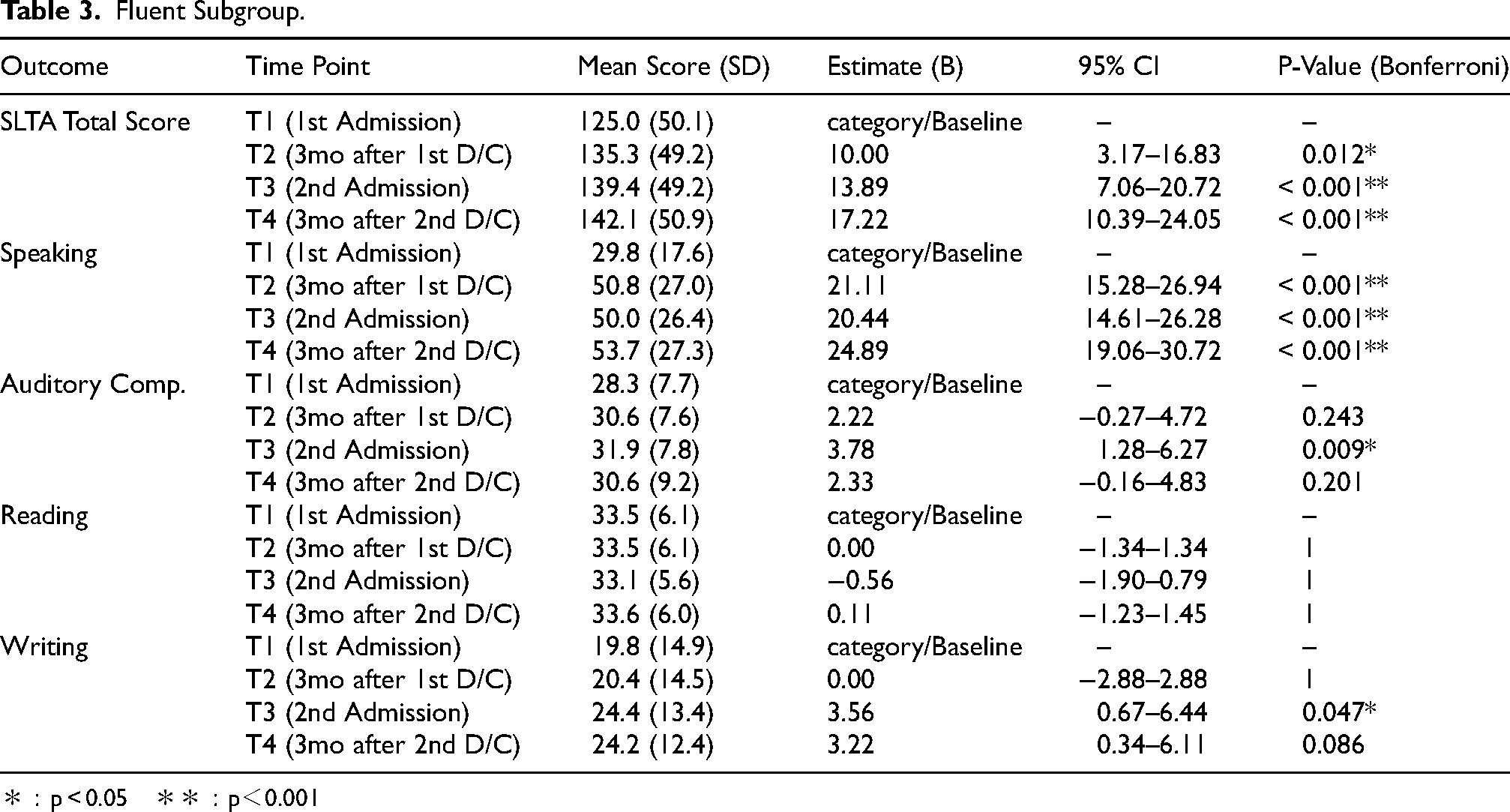
*:p < 0.05 **:p<0.001
Non-fluent Subgroup.
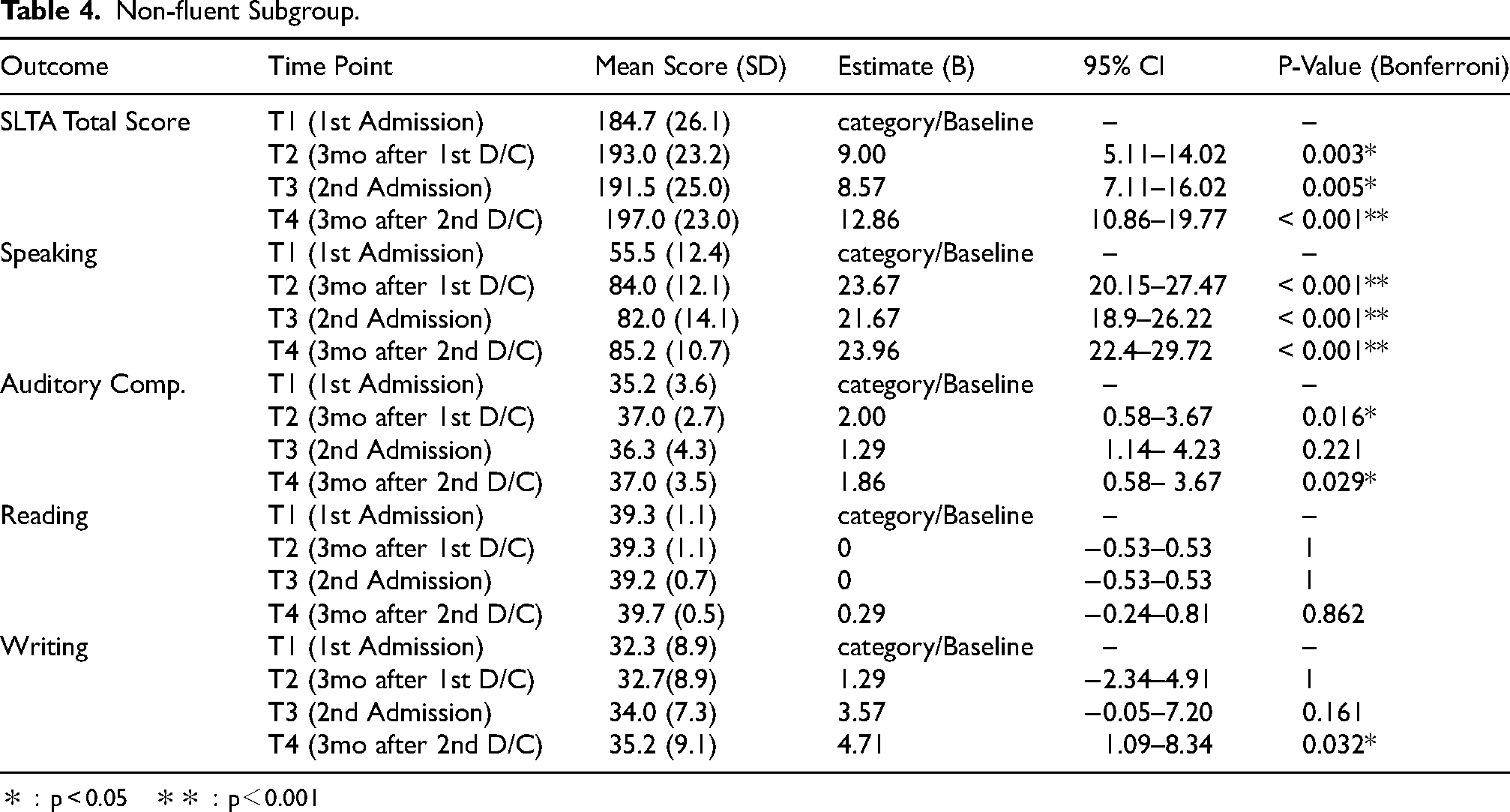
*:p < 0.05 **:p<0.001
Fluent Aphasia Group (n = 6)
Significant improvements were observed in the SLTA Total Score at T2 (p = 0.012), T3 (p < 0.001), and T4 (p < 0.001).
Non-fluent Aphasia Group (n = 10)
Significant improvements were observed in the SLTA Total Score at T2 (p = 0.003), T3 (p = 0.005), and T4 (p < 0.001).
Discussion
This study investigated the effects of combining two courses of HF-rTMS treatment and intensive ST for patients with chronic aphasia. The results showed significant improvement, particularly in speech function. This suggests that the combination of multiple courses of HF-rTMS treatment and intensive ST may contribute specifically to the improvement of speech function among language functions. Our previous study using a similar treatment protocol also reported significant improvement in speech items compared to reading comprehension and writing (Ohara et al., 2025). Other reports have also observed improvements in spontaneous speech and repetition following HF-rTMS (Fahmy & Elshebawy, 2021). The results of this study support these findings and reaffirm the efficacy of HF-rTMS treatment for speech function. The preferential improvement in the “Speaking” modality is likely attributable to our fMRI-guided targeting method. We utilized a repetition task during fMRI to identify the functional language area. This task primarily engages the dorsal language stream, which is essential for auditory-motor integration and speech production. By applying excitatory HF-rTMS to the specific network responsible for repetition, we directly modulated the neural circuits for “Speaking.” This suggests a task-specific effect of our rTMS protocol, consistent with the clinical observation that oral output often improves prior to literacy skills (reading/writing) in aphasia recovery.
Notably, there were cases where no decline in evaluation scores was observed during the period between the first discharge and the second admission (average of approximately 1 year). This suggests a maintenance of the therapeutic effect (carry-over effect). Previous studies have reported that improvement in language function was maintained for 1 to 2 months after HF-rTMS treatment (Fahmy & Elshebawy, 2021; Hu et al., 2018). In this study, function was maintained and improved at 3 months after the 1st discharge and even at the 2nd admission (average 13.9 months after the 1st admission), indicating a longer duration of effect than in previous studies. A factor in this may be the combination of rTMS with 120 min of daily intensive ST. It has been stated that the combination of rTMS and Multimodality Aphasia Therapy (M-MAT) resulted in greater improvement effects and sustainability than speech therapy alone (Low et al., 2025). The intensive rehabilitation in our hospital's protocol may have contributed to the long-term maintenance of effects.
Furthermore, it is important that the target was determined by individually evaluating language function activation sites using fMRI. Since rTMS affects brain function differently depending on the stimulation site, stimulation of the appropriate site is essential. In this study, there were cases where the rTMS stimulation site changed between the 1st and 2nd courses. This suggests the possibility that the networks responsible for language function and activity sites changed over time due to plastic changes in the brain. Regarding the role of the right hemisphere, previous studies have discussed both a “compensatory role” that supplements language function and an “interference role” that hinders recovery (Turkeltaub et al., 2012; Turkeltaub, 2015). There are also reports that residual areas around the left inferior frontal gyrus contribute to recovery (van Oers et al., 2010). Since the mechanism of language recovery differs depending on the individual case and timing, it is considered that identifying the active site using fMRI each time and applying high-frequency stimulation to the optimal site efficiently promoted the activation of the intracerebral network. It is suggested that the synergistic effect of this “setting of individualized stimulation sites” and “intensive speech training” led to long-term improvement and maintenance.
While this study is limited by the absence of a control group (ST alone), this design was chosen based on ethical and clinical considerations. The Japanese Guidelines for the Management of Stroke 2021 recommend rTMS as a treatment option, supported by evidence that combined therapy (rTMS + ST) is superior to ST alone (Rubi-Fessen et al., 2015; Lefaucheur et al., 2020). Consequently, withholding rTMS to create a control group was deemed ethically inappropriate in our clinical setting, where patients seek the maximal therapeutic benefit. Therefore, this study focused on evaluating the longitudinal maintenance of effects in a real-world clinical cohort.
Limitations
The limitations of this study include the small number of subjects (16 cases) and the lack of a unified interval between the 1st and 2nd admissions. Detailed comparative examination by aphasia type and severity is also a future task. Future verification of more effective intervention methods and indications by accumulating more cases is necessary.
Conclusions
Intensive speech therapy combined with HF-rTMS contributes to the improvement of language function in patients with chronic aphasia and may be particularly effective for improving speech function. Future detailed examination by severity and type through the accumulation of further cases is desired.
Footnotes
Acknowledgements
During the preparation of this work, the authors used Google Gemini (Alphabet Inc., Mountain View, CA, USA) in order to improve the clarity and readability of the manuscript. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Ethical Considerations
The study protocol was approved by the Ethics Committee of The Jikei University School of Medicine (Approval No. 32-338: 10423).
Consent for Publication
Written informed consent was obtained from all participants involved in the study.
Funding
This work was supported by JSPS KAKENHI Grant Number JP 23K10567.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.