
Abstract
Background
Dual-task and augmented reality (AR)–based interventions have been used to improve balance and gait in patients with stroke; however, evidence for AR programs developed using accessible approaches such as ChatGPT-assisted programming remains limited.
Objective
This study aimed to investigate the effects of ChatGPT-assisted AR dual-task training on muscle strength, balance, gait parameters, and fall-related self-efficacy in patients with chronic stroke.
Methods
Twenty-eight patients with chronic stroke were randomly assigned to an experimental group receiving ChatGPT-assisted AR dual-task training or a control group receiving lunge training combined with a throwing task. Both groups trained for 10 min per session, five times per week for four weeks. Primary outcomes were lower-limb strength and balance (static and dynamic). Secondary outcomes included gait parameters and fall-related self-efficacy. Gait speed and step length were measured using the GAITRite system, and step-length symmetry was calculated using a symmetry index derived from paretic and nonparetic step lengths. Group × time interactions were analyzed using mixed-design ANOVA.
Results
Significant group × time interactions were observed for most primary and secondary outcomes (p < 0.05), in favor of the experimental group; however, the interaction for paretic step length was not statistically significant. Notably, improvement in dynamic balance, as assessed by the timed up and go test, exceeded the minimal clinically important difference in the experimental group.
Conclusions
ChatGPT-assisted AR dual-task training improved muscle strength, balance, gait performance, and fall-related self-efficacy more than conventional dual-task training, providing preliminary evidence of short-term benefits for ambulatory patients with chronic stroke.
Introduction
Stroke is a leading cause of long-term disability worldwide and frequently results in persistent muscle weakness, impaired postural control, gait asymmetry, and reduced fall-related self-efficacy, all of which substantially restrict functional independence and community participation (GBD 2021 Stroke Risk Factor Collaborators, 2024; Veerbeek et al., 2014). Hemiparetic gait is characterized by reduced paretic limb weight bearing, diminished forward propulsion, and step-length asymmetry, reflecting deficits in both neuromuscular force generation and motor control integration (Brunner & Rutz, 2013; Hayashi et al., 2024). In particular, weakness of the quadriceps and ankle plantarflexors is strongly associated with impaired stance-phase stability and decreased propulsive impulse, thereby limiting gait speed and efficiency in patients with chronic stroke (Asouzu et al., 2024; Ng et al., 2017). Consequently, targeted strengthening of these muscle groups remains a central therapeutic objective in contemporary stroke rehabilitation (Aguirre-Villanueva et al., 2025).
To address these functional limitations, task-oriented exercise has been widely adopted in stroke rehabilitation to improve lower-limb strength, balance, and gait performance (Lee & Lee, 2025). The lunge posture, as a weight-bearing task that challenges paretic limb loading and postural control, provides a biomechanically relevant framework for task-oriented stroke rehabilitation (Kwag & Park, 2025). Dual-task training, which simultaneously combines motor and cognitive demands, has been increasingly recognized as an effective rehabilitation strategy for stroke survivors (Mou & Jiang, 2025). Recent systematic reviews and meta-analyses have demonstrated that motor- cognitive dual-task training significantly improves gait speed, step length, and balance compared with conventional single-task training, and has been shown to promote motor control, motor learning, and reduce fall risk in daily life activities (Chiaramonte et al., 2022; Mou & Jiang, 2025). In recent years, augmented reality (AR) has emerged as a promising platform for delivering task-oriented motor–cognitive dual-task training by superimposing interactive virtual stimuli onto real-world movements in real time (Alberts et al., 2022; Khokale et al., 2023). Through external focus cues, adaptive task progression, and gamified feedback, AR-based interventions have demonstrated improvements in balance and mobility in patients with stroke and other neurological populations, including those with Parkinson's disease (Phan et al., 2022; Rosenfeldt et al., 2025). However, the integration of AR-based rehabilitation into routine clinical practice remains limited, as conventional systems often involve technical and implementation challenges (Gorman & Gustafsson, 2022).
Recent advances in generative artificial intelligence, particularly large language models such as ChatGPT, have enabled the generation and refinement of computer programs through natural language–based interactions (Schopow et al., 2023). Integration with open-source image-processing and interface platforms may support the development of adaptable AR environments incorporating real-time feedback and interactive task elements (Fuchter et al., 2025; Maggio et al., 2024). However, the clinical efficacy of AR-based dual-task training developed through such accessible approaches has yet to be validated in patients with stroke.
Therefore, the primary aim of this randomized controlled trial was to evaluate the clinical efficacy of a ChatGPT-assisted, coding-based AR dual-task program combined with lunge exercise on lower-limb strength (quadriceps and ankle plantarflexors), balance, spatiotemporal gait parameters, and fall-related self-efficacy in patients with chronic stroke, while also demonstrating the feasibility of ChatGPT-assisted program development as a secondary contribution. The comparator involved conventional lunge training combined with a throwing task. We hypothesized that AR dual-task lunge training implemented using a ChatGPT-assisted development approach would be associated with greater improvements in lower-limb strength, balance, gait performance, and fall-related self-efficacy compared with conventional lunge training combined with a throwing task.
Methods
Study Design and Participants
Participants were recruited via an open announcement targeting patients admitted to Happy-Hospital during a one-week public recruitment period. The required sample size was determined using G*Power software (version 3.1.2) based on data from a previous study (Lee et al., 2014), using F tests with ANOVA: Repeated measures, within-between interaction (effect size f = 0.332, α = 0.05, power = 0.85, number of groups = 2, number of measurements = 2). The analysis indicated that at least 22 participants were needed. Accounting for an anticipated 20% dropout rate, the minimum sample size was set at 28 participants. The inclusion criteria were as follows: (1) diagnosis of stroke more than 6 months prior to enrollment, (2) stable vital signs, (3) ability to independently walk at least 10 meters without assistive devices, (4) a score of 24 or higher on the Korean version of the Mini-Mental State Examination (K-MMSE). The exclusion criteria were as follows: (1) manual muscle test (MMT) grade < 3 in the quadriceps and ankle plantarflexors on the paretic side, (2) modified Ashworth Scale score of 3 or higher in the ankle plantarflexors, (3) current use of medications known to affect balance, gait, or alertness (e.g., sedatives, hypnotics, antipsychotics, and anxiolytics). A total of 28 patients who met the inclusion and exclusion criteria participated in the study and were included in the final analysis. All participants provided written informed consent and were informed of their right to withdraw at any time in the event of discomfort. This study was approved by the Institutional Review Board of Kyungnam University (IRB No. 1040460-A-2025-044; approval date: October 14, 2025) and was registered with the Clinical Research Information Service (CRIS No. KCT0011287). All procedures were carried out in accordance with the ethical principles outlined in the Declaration of Helsinki. No missing data were observed, as all participants completed the intervention and post-intervention assessments. The study adhered to the CONSORT 2010 guidelines (Figure 1).
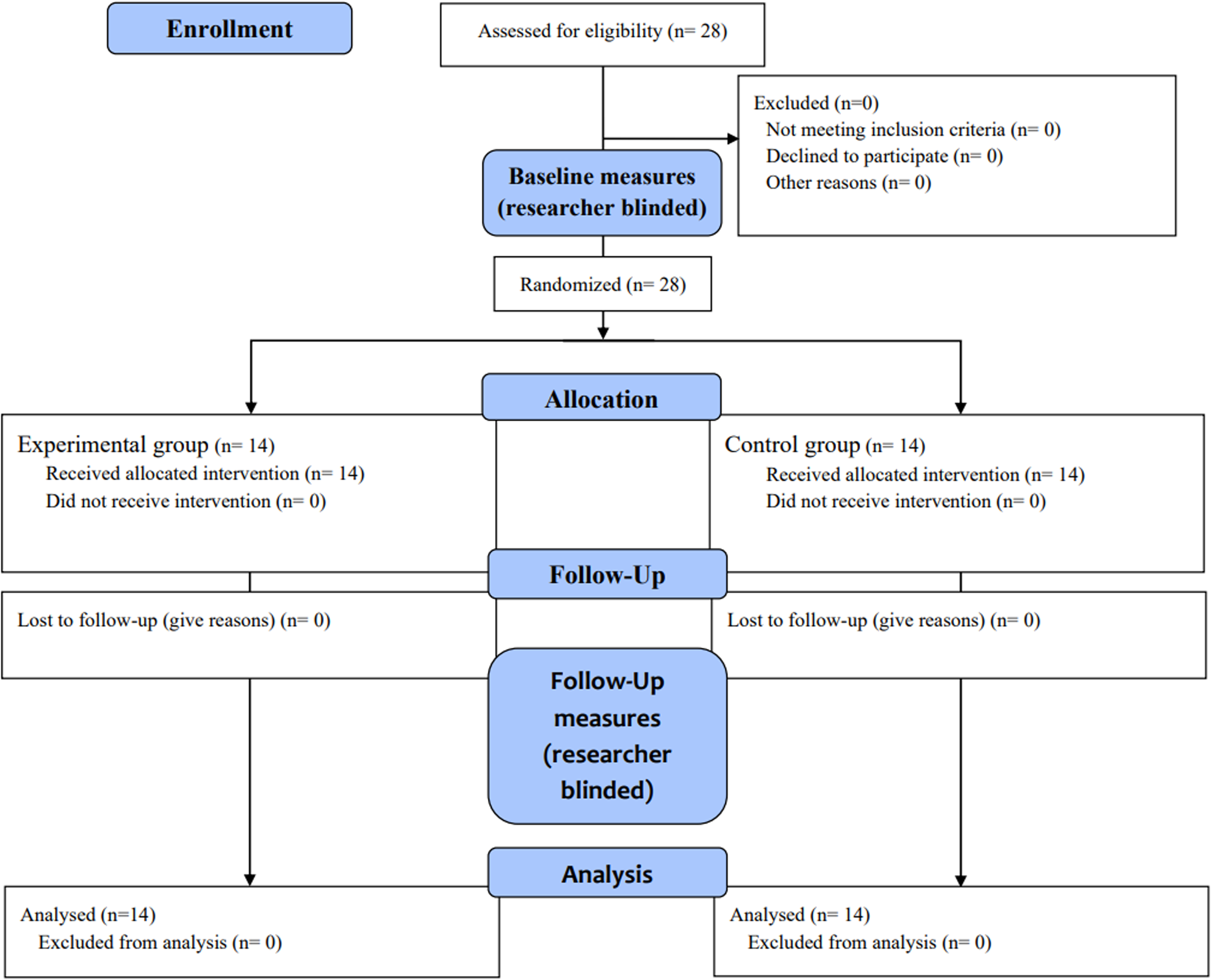
CONSORT flow diagram of participant recruitment, allocation, follow-up, and analysis.
Interventions and Procedures
This study employed a randomized controlled trial design. The principal investigator conducted randomization using an online tool (http://www.randomizer.org), assigning participants numbers from 1 to 28, which were then automatically allocated to the experimental or control group. To ensure allocation concealment, group assignments were generated by an independent researcher and placed in sealed opaque envelopes, which were opened after baseline assessments were completed. The experimental group (n = 14) performed AR dual-task lunge training developed with ChatGPT assistance (AR-DT lunge training), whereas the control group (n = 14) performed conventional lunge training combined with a throwing task. Each intervention session lasted 10 min and was conducted five times per week for 4 weeks, for a total of 20 sessions. A single-blind design was implemented to reduce bias, with only the assessors blinded to group assignments. In addition, all participants received standardized rehabilitation exercises for 30 min per session, and the type and duration of these exercises were uniformly controlled to ensure consistency across groups. All standardized rehabilitation exercises and study interventions were administered by licensed physiotherapists with more than five years of clinical experience, following a predefined and standardized protocol. Exercises that required functional levels beyond participant capacity, or that could directly influence the primary outcome measures, were excluded from the protocol. Baseline demographic and clinical characteristics were collected for all participants. Pre-intervention assessments were conducted one day before the start of the program, and post-intervention assessments were performed the day after the final session.
The primary outcomes were lower-limb strength and static and dynamic balance. Lower-limb strength was assessed using a PowerTrack II Commander hand-held dynamometer (J-Tech Medical, Salt Lake City, UT, USA). Static balance was evaluated using an AMTI force plate (AMTI, Newton, MA, USA) to quantify the total center of pressure (COP) sway distance, and dynamic balance was assessed using the timed up and go (TUG) test. The secondary outcomes included spatiotemporal gait parameters (gait speed and step length) and fall-related self-efficacy. Gait speed and step length were measured using the GAITRite system (GAITRite® Electronic Walkway, CIR Systems Inc., NY, USA). Fall-related self-efficacy was evaluated using the falls efficacy scale-international (FES-I).
Development of an AR Dual-Task Training Program with ChatGPT Assistance
The role of ChatGPT in the development process was limited to software implementation and debugging. The clinical design of the intervention—including task goals, therapeutic logic, and the lunge-based dual-task structure—was determined by the investigators based on established rehabilitation principles. ChatGPT-5 was used solely for iterative code generation and error correction through natural language prompts. The final functionality and safety of the program were verified by the investigators prior to clinical application. The system was implemented in Python 3.10 and integrated MediaPipe (v0.10) for real-time hand tracking, OpenCV (v4.8) for video capture and processing, and Pygame for interface and game logic (Bradski, 2000). Hand landmarks were mapped to virtual falling objects using a Euclidean-distance threshold, and performance-based visual feedback was provided through a scoring system. The detailed development procedures, representative prompts, and the complete source code are available in the supplementary material.
AR Dual-Task Lunge Training Developed with ChatGPT Assistance
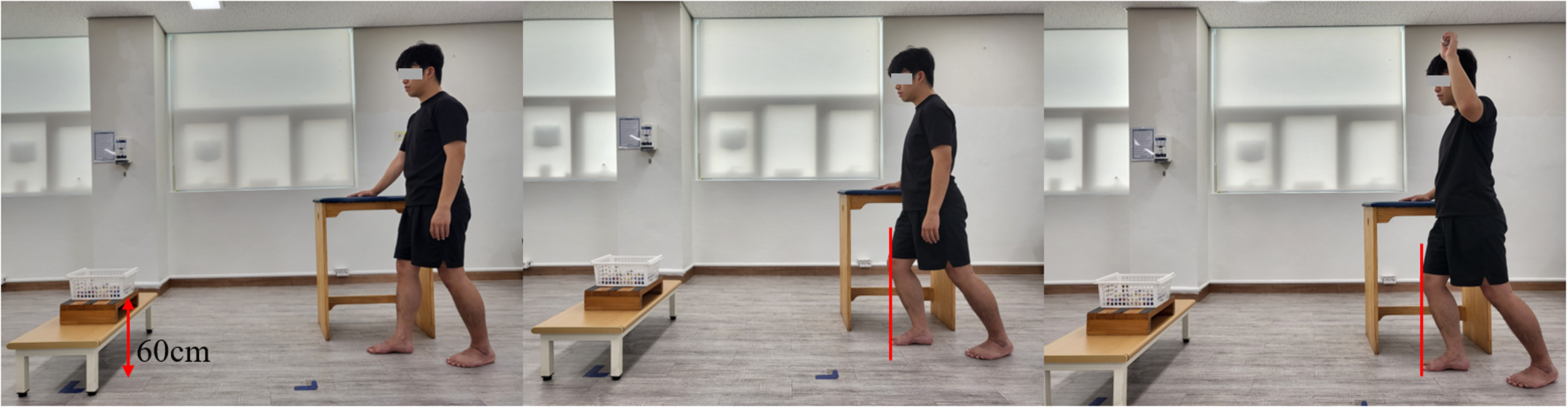
The experimental group performed AR-DT lunge training as follows (Figure 2): (1) Participants stood 2 m from a 34-inch monitor with the paretic leg forward and the paretic arm supported on a side table. (2) They performed a forward lunge by flexing the paretic knee in line with the second toe while keeping the non-paretic knee extended and the trunk upright. (3) The AR dual-task program was initiated (settings: 10 falling objects, speed 5; 5 trap objects, speed 5). (4) Participants earned points by matching falling objects with the non-paretic hand, and points were deducted when touching trap objects. (5) Task difficulty increased progressively by adjusting the number, speed, and frequency of trap objects. (6) If discomfort occurred, the session was stopped and resumed after rest as appropriate. (7) Total score across all sets was recorded and provided as feedback. (8) The intervention consisted of 10 sets of 30 s each, with 30-s rests, totaling 10 min.

Performance of AR dual-task lunge training developed with ChatGPT assistance. Written informed consent was obtained from the participant for publication of these images.
Conventional Lunge Training Combined with a Throwing Task
The control group performed conventional lunge training combined with a throwing task, which was implemented as follows (Figure 3): (1) Participants stood 2 m away from a target box (10 cm × 15 cm) placed 60 cm above the base, with the paretic lower limb positioned forward; the paretic upper limb was supported on a side table for safety. (2) Participants performed a forward lunge by flexing the paretic knee until it aligned vertically with the tip of the second toe, while keeping the non-paretic knee extended and the trunk upright. (3) Using the non-paretic hand, participants threw a 40 g ball into the target box. (4) If any discomfort occurred during the intervention, the exercise was stopped immediately; after a rest period, resumption was determined based on participant condition. (5) The intervention consisted of 10 sets, each comprising 30 s of exercise followed by 30 s of rest, totaling 10 min.
Performance of the conventional lunge training combined with a throwing task. Written informed consent was obtained from the participant for publication of these images.
Standard Rehabilitation Exercises
The standard rehabilitation exercises applied in this study were modified based on previous studies, as follows (Hosseini et al., 2019; Lee, 2023): (1) Passive and active range of motion exercises for the trunk, shoulder girdle, pelvic girdle, and upper and lower extremities were performed for 10 min. (2) To facilitate weight transfer, participants performed a 10-min training session consisting of seated side-to-side weight-shifting, standing side-to-side weight-shifting, and single-leg standing exercises. (3) Gait training was conducted on a treadmill, with each session lasting 10 min.
Outcome Measures
Muscle Strength
Lower limb muscle strength, specifically that of the quadriceps and ankle plantarflexors, was measured using a hand-held dynamometer (Yen et al., 2017). For quadriceps assessment, participants were seated on a mat with the hip and knee flexed at 90°, and the dynamometer was positioned at the distal one-third of the tibia on the paretic side. Participants were instructed to perform maximal isometric knee extension for 3 s, during which peak force was recorded. For ankle plantarflexors assessment, participants lay supine on a mat with the dynamometer placed against the plantar surface of the foot. They were asked to perform maximal isometric plantarflexion for 3 s. During all strength assessments, a standardized verbal cue, “Push as hard as you can,” was provided to ensure consistent effort across participants. Each measurement was expressed in newtons (N), repeated three times, and the mean value was used for analysis.
Static Balance
Static balance was assessed using an AMTI force plate with a load capacity of 130 kg and dimensions of 45.5 × 502 × 502 mm, recording data at 100 Hz (Meier et al., 2025). Participants stood barefoot in a standardized posture, focusing on a 15-cm target placed 3 m ahead, while total COP sway distance in the mediolateral and anteroposterior directions was measured for 30 s. Each trial was repeated three times, and the mean value was used for analysis.
Dynamic Balance
The TUG test was used to assess dynamic balance (Shumway-Cook et al., 2000). The procedure included: (1) standing up from a seated position in a chair, (2) walking 3 meters, (3) turning around and returning to the chair, and (4) sitting down again. The test was performed three times, and the mean value was used for analysis to enhance reliability. The Minimal Clinically Important Difference (MCID) for the TUG test was estimated at 3.51 s (Komiya et al., 2021).
Spatiotemporal Gait Parameters
Spatiotemporal gait parameters, including gait speed and step length, were measured using the GAITRite system (Sacco et al., 2023). The GAITRite walkway (461 cm × 88 cm) consists of 13,824 sensors, each 1 cm in diameter and spaced 1.27 cm apart, which capture spatial and temporal gait data. Participants began walking 2 m before the walkway and continued for 2 m beyond it to minimize acceleration and deceleration effects. Each assessment was performed three times, and the mean value was used for analysis to enhance measurement reliability. Step length symmetry was evaluated using the symmetry index (SI), which quantifies the relative difference between the paretic and non-paretic limbs, with 0% indicating perfect symmetry and higher values reflecting greater asymmetry (Patterson et al., 2010).
Fall-Related Self-Efficacy
The FES-I is an expanded version of the original falls efficacy scale, increasing the number of items from 10 to 16 to encompass tasks requiring greater physical demands as well as activities involving social participation (Yardley et al., 2005). Each item asks individuals to rate their level of concern about falling using a four-point scale ranging from no concern to a high degree of concern. Total scores range from 16 to 64, with higher scores indicating lower confidence in avoiding falls and greater fear of falling.
Statistical Analysis
Statistical analyses were conducted using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA). The Shapiro–Wilk test was applied to assess data normality. Baseline characteristics were compared with independent t-tests for continuous variables and chi-square tests for categorical variables. All variables satisfied the assumption of normality (p > 0.05). Step-length SI was calculated for each participant at baseline and post-intervention and entered as a dependent variable in the analysis. A mixed-design ANOVA was performed to evaluate group (experimental vs. control) × time (pre- vs. post-test) interactions. Within-group changes were assessed using paired t-tests. Effect sizes were calculated using Cohen's d for within-group comparisons based on paired t-tests, and partial eta squared (η2p) for group × time interaction effects derived from the mixed-design ANOVA. Cohen's d values were interpreted as small (0.20–0.49), moderate (0.50–0.79), and large (≥0.80) (Cohen, 1988). Partial eta squared values were interpreted based on conventional benchmarks (small = 0.01, medium = 0.06, large = 0.14) (Lakens, 2013).
Results
This study was completed over a four-week period with full participant retention. Baseline demographic and clinical characteristics are summarized in Table 1, and no significant group differences were identified at the start of the study.
Baseline Demographic and Clinical Characteristics of Participants.
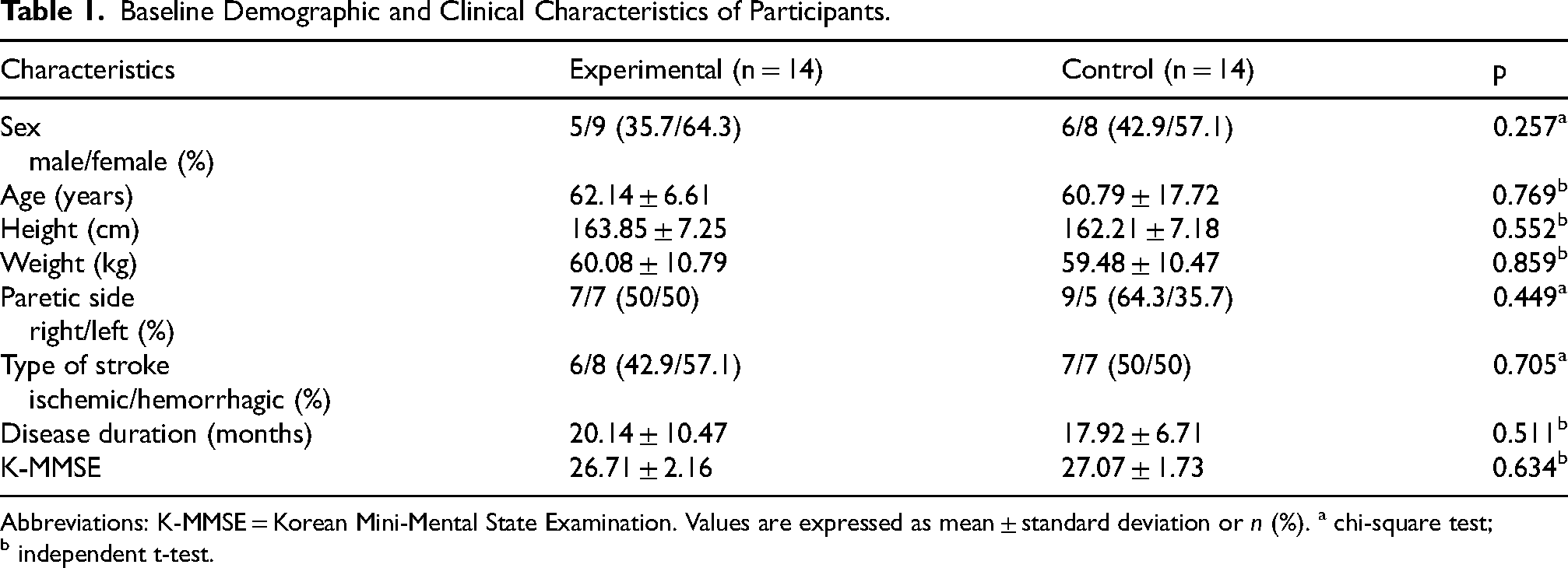
Abbreviations: K-MMSE = Korean Mini-Mental State Examination. Values are expressed as mean ± standard deviation or n (%). a chi-square test; b independent t-test.
Table 2 presents the outcome measures. Significant group × time interaction effects were observed for quadriceps strength (F(1, 26) = 6.44, p = 0.018, η2p = 0.198), ankle plantarflexor strength (F(1, 26) = 24.01, p < 0.001, η2p = 0.479), total COP sway distance (F(1, 26) = 36.19, p < 0.001, η2p = 0.582), TUG (F(1, 26) = 21.29, p < 0.001, η2p = 0.450), gait speed (F(1, 26) = 27.38, p < 0.001, η2p = 0.513), non-paretic step length (F(1, 26) = 20.82, p < 0.001, η2p = 0.445), step length SI (F(1, 26) = 8.72, p = 0.007, η2p = 0.251), and FES-I scores (F(1, 26) = 12.39, p = 0.002, η2p = 0.323). No significant interaction effect was found for paretic step length (F(1, 26) = 3.64, p = 0.068, η2p = 0.123). Significant main effects of time were observed for all variables, indicating improvements in both groups following the intervention (p < 0.05).
Results of Statistical Analysis for Variables.
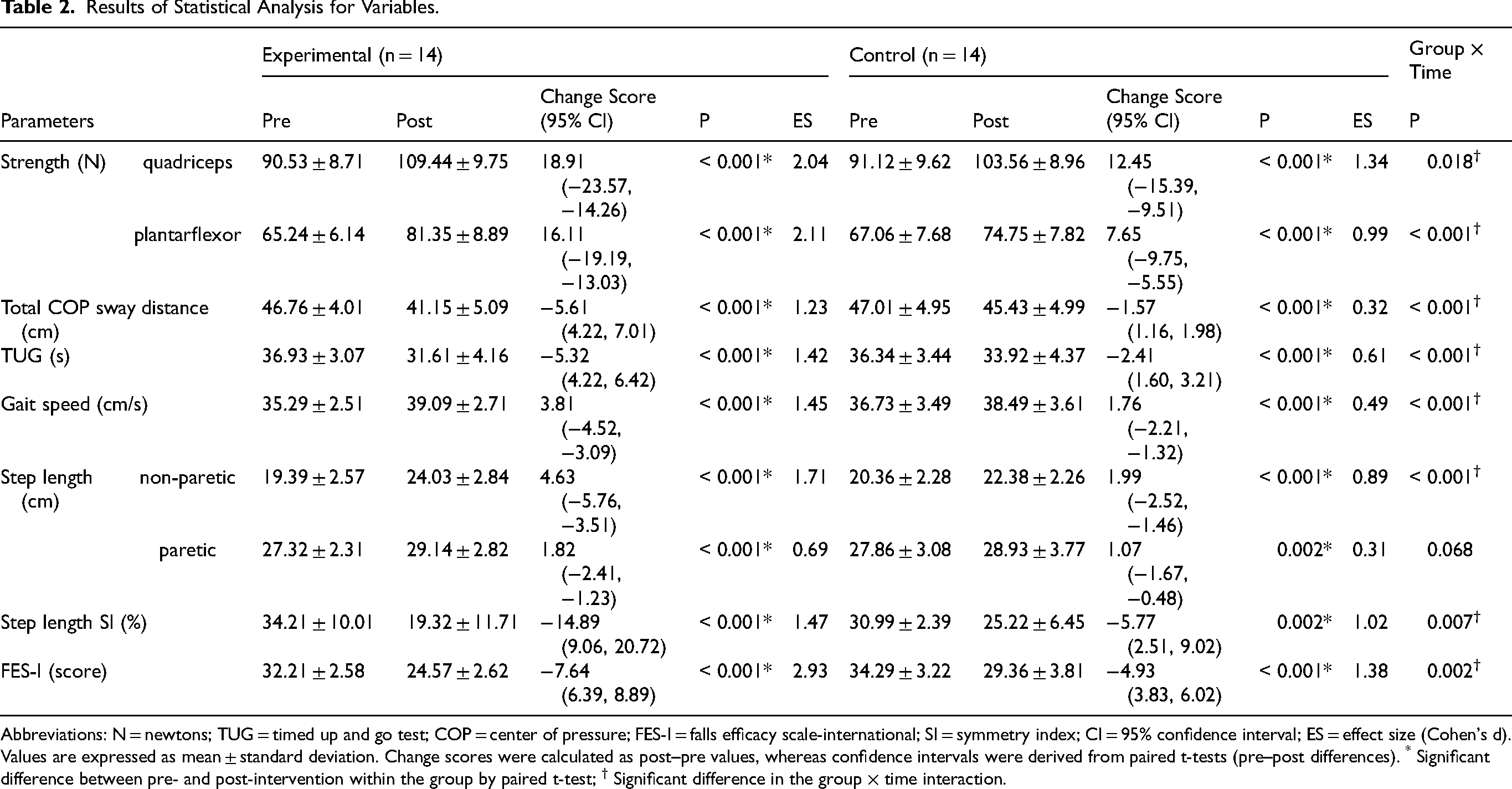
Abbreviations: N = newtons; TUG = timed up and go test; COP = center of pressure; FES-I = falls efficacy scale-international; SI = symmetry index; CI = 95% confidence interval; ES = effect size (Cohen's d). Values are expressed as mean ± standard deviation. Change scores were calculated as post–pre values, whereas confidence intervals were derived from paired t-tests (pre–post differences). * Significant difference between pre- and post-intervention within the group by paired t-test; † Significant difference in the group × time interaction.
Discussion
In this study, we examined the effects of dual-task training that combined an AR program developed with ChatGPT assistance with a lunge task in patients with chronic stroke. The experimental group demonstrated greater improvements than the control group across several outcomes, with the exception of paretic step length. To our knowledge, this study represents one of the first clinical attempts to implement an AR-based dual-task training program developed with ChatGPT assistance in stroke rehabilitation. The intervention was developed with ChatGPT assistance, which facilitated the iterative creation of a customized AR environment through natural language interactions. However, the clinical relevance of the present findings is primarily attributed to the therapeutic characteristics of the AR-based dual-task training, including task-oriented, weight-bearing, and cognitively engaging components, rather than the use of ChatGPT itself.
In the comparison of lower-limb strength, the experimental group demonstrated post-intervention increases of 20.9% and 24.7% in quadriceps and ankle plantarflexor strength, respectively, whereas the control group showed increases of 13.7% and 11.5%. The greater strength gains observed in the experimental group may be related to the multidirectional weight-shifting demands imposed by the AR-based dual-task lunge training. Ryan et al. (2021) reported that multidirectional loading applied to the gastrocnemius is more effective in attenuating strength loss than unidirectional loading, potentially due to the distribution of mechanical stress across muscle architecture. In this study, matching falling objects from multiple directions may have required repeated multidirectional weight shifts, which could have led to increased activation demands in both the medial and lateral quadriceps and the gastrocnemius–soleus complex, compared with the fixed-direction throwing task. The pronounced improvement in ankle plantarflexor strength may reflect a greater reliance on the ankle strategy during conditions that increase postural demands, such as multidirectional balance challenges (Pollock et al., 2019; Tan et al., 2024). Additionally, the strength gains observed over the four-week intervention may be further explained by the sustained isometric contraction required to maintain the lunge posture, which may have promoted neural adaptations including improved motor unit recruitment and reduced cortical inhibition, rather than structural hypertrophy, which typically requires longer training durations (Škarabot et al., 2021). Collectively, these findings suggest that the multidirectional demands and sustained postural loading of AR-based dual-task lunge training may have synergistically contributed to the superior neuromuscular gains observed in the experimental group. It should be noted, however, that despite these improvements, the post-intervention quadriceps strength of the paretic limb (mean: 109.44 N, approximately 18.6% of body weight) remained substantially below the normative range reported for healthy older adults (35.6–48.8% of body weight) (Bohannon, 2017), suggesting that longer-term interventions may be required to achieve more complete functional recovery.
In the comparison of balance performance, the experimental group demonstrated greater post-intervention improvements in both static (12.0%) and dynamic balance (14.4%) than the control group (3.36% and 6.66%, respectively). Immediate multimodal feedback may have enhanced postural control by increasing presence and sensorimotor engagement, consistent with prior findings that AR interventions have been shown to yield greater improvements in balance and mobility through real-time sensory feedback (Kim & Lee, 2012). Lamichhane et al. (2023) similarly reported that AR-based interventions produced superior improvements in balance and mobility through continuous real-time sensory feedback. Previous studies suggest that AR-based training may impose greater cognitive demands than simple motor tasks due to increased task complexity and multisensory integration (Buchner et al., 2022). AR environments incorporating gamified elements can further enhance engagement, motivation, and attentional focus (Levin et al., 2015; Phan et al., 2022). In this study, participants were required to continuously monitor multiple moving objects, make rapid visuomotor decisions, and adapt to progressively increasing task demands, which may have enhanced attentional engagement and cognitive processing. Furthermore, the multidirectional stimuli incorporated in the protocol may have increased demands on lumbopelvic stabilizers, thereby reinforcing trunk stability (El-Nashar et al., 2019). The dual-task condition may also have facilitated anticipatory postural adjustments via enhanced sensorimotor integration and preparatory activation of trunk and ankle musculature (Aruin et al., 1998; Sousa et al., 2015). Similar effects have been reported in healthy adults, in whom concurrent visual–cognitive tasks during quiet stance reduce postural sway (Polskaia & Lajoie, 2016). Taken together, these findings suggest that AR-based dual-task training may improve balance, potentially through enhanced cognitive engagement and sensorimotor integration. Clinically, the experimental group exceeded the MCID for the TUG (mean change: 5.32 s), whereas the control group did not (2.41 s) (Komiya et al., 2021). Effect sizes further supported greater clinical relevance in the experimental group (d = 1.42 vs. 0.61), indicating that the experimental intervention produced substantially greater clinical benefits. Nevertheless, the moderate within-group effect size observed in the control group (d = 0.61) suggests that the control intervention may also have produced a clinically relevant improvement in dynamic balance, despite not exceeding the MCID threshold.
Regarding gait performance, the experimental group demonstrated greater post-intervention increases in gait speed (10.78%) and non-paretic step length (23.94%) than the control group (4.79% and 9.93%, respectively). Although the experimental group also showed a larger within-group increase in paretic step length (6.66%) than the control group (3.84%), the group × time interaction for paretic step length did not reach statistical significance (p = 0.068). These improvements may be partly explained by strength gains in key lower-limb muscle groups. Quadriceps strength contributes to knee stability during loading response and supports weight bearing on the paretic limb, thereby facilitating longer and more symmetric contralateral step lengths (Li et al., 2018; Hyun et al., 2015). In addition, the ankle plantarflexors play a critical role in postural support and forward propulsion by controlling tibial progression in mid-stance and generating propulsive force during push-off, directly influencing gait speed and step length (Hsiao et al., 2015; Neptune et al., 2001). Consistent with this mechanism, prior studies have reported moderate-to-strong associations between lower-limb muscle strength and gait performance in patients with stroke (Kim & Eng, 2003). The experimental group also exhibited a greater reduction in the step-length SI (43.5%) compared with the control group (18.6%), indicating greater improvements in gait symmetry after the intervention (Patterson et al., 2010). Improved symmetry has been associated with more balanced inter-limb contributions during gait and may be clinically meaningful, given its relationship with impaired propulsion and inefficient gait biomechanics in chronic stroke (Allen et al., 2011; Awad et al., 2016). These findings suggest that improvements in spatiotemporal gait parameters may be related to increased paretic limb loading and enhanced propulsive capacity. However, it should be noted that improvements in SI do not necessarily reflect full clinical normalization of gait patterns. Given that gait asymmetry persisted in both groups post-intervention, further long-term studies are needed to confirm whether these changes translate into functionally meaningful gait recovery.
The FES-I score decreased by 23.7% in the experimental group and by 14.4% in the control group. Because fall risk is closely associated with balance impairment, balance training has consistently been shown to reduce fall risk in neurological and geriatric populations (Djurovic et al., 2021; Sherrington et al., 2019). Strength gains in the quadriceps are particularly relevant, as these muscles play a key role in upright posture and weight-bearing during stance, and greater quadriceps strength may contribute to improved postural stability by enhancing loading on the paretic limb (Scarborough et al., 1999; Yang et al., 2016). In addition, improvements in ankle plantarflexor strength may have reduced fall-related concerns by facilitating more effective use of the ankle strategy, which is essential for stabilizing the center of mass during both static and dynamic tasks (Mackey & Robinovitch, 2006; Sherrington et al., 2019). Consistent with this, plantarflexor weakness has been strongly associated with postural instability and increased fall risk (Yakut et al., 2024). Thus, enhanced lower-limb strength and postural control may have contributed to the greater improvement in fall-related self-efficacy observed in the experimental group.
Study Limitations
This study has several limitations. First, the findings may have limited generalizability because participants were restricted to ambulatory patients with chronic stroke. Second, the study did not include a direct comparison with conventional AR interventions, so the relative efficacy of the program developed with ChatGPT assistance remains unclear. Third, trunk muscle activation and core stability, previously reported to improve with AR-based dual-task training, were not assessed. Fourth, although the sample size was determined using G*Power, the relatively small cohort warrants caution when interpreting the findings. Fifth, the short intervention period precluded conclusions about long-term effects. Sixth, static balance was assessed using only total COP sway distance, which may not fully capture the complexity of postural control. Finally, the task demands were not perfectly matched between groups, which may have contributed to differences in cognitive and motor loading, thereby limiting the interpretability of direct between-group comparisons. Furthermore, given the multiple outcome measures assessed, the potential for Type I error due to multiplicity should be acknowledged, and the findings should be interpreted with caution.
Additionally, regarding the development process, the use of ChatGPT introduces several practical limitations. The generated code may vary depending on prompt design, making the output dependent on investigator proficiency. As a result, the same task may yield different implementations, and no standardized protocol currently exists for debugging AI-generated code. Furthermore, system performance may be influenced by hardware-related factors, such as computer specifications and webcam quality, which can affect input processing and error occurrence. These factors may influence the reproducibility of ChatGPT-assisted rehabilitation program development and highlight the need for careful validation and standardized implementation in future studies.
Future studies should include more diverse populations, larger samples, longer follow-up periods, and direct comparisons with conventional AR interventions to further establish the clinical utility of AR training developed with ChatGPT assistance.
Conclusion
This randomized controlled trial demonstrated that AR dual-task lunge training developed with ChatGPT assistance led to greater improvements in lower-limb strength, balance, spatiotemporal gait parameters, and fall-related self-efficacy compared with lunge training with a throwing task in ambulatory patients with chronic stroke. These findings provide preliminary evidence of the potential short-term benefits of AR-based dual-task training in this population. By demonstrating that clinicians without programming expertise can develop customized AR rehabilitation programs using ChatGPT, this study lays a foundation for broader application in clinical practice, while the role of ChatGPT is limited to facilitating intervention development rather than directly contributing to clinical outcomes.
Supplemental Material
sj-docx-1-nre-10.1177_10538135261449483 - Supplemental material for Effects of Augmented Reality Dual-Task Training with ChatGPT-Assisted Development on Strength, Balance, Spatiotemporal Gait Parameters, and Fall-Related Self-Efficacy in Patients with Chronic Stroke: A Randomized Controlled Trial
Supplemental material, sj-docx-1-nre-10.1177_10538135261449483 for Effects of Augmented Reality Dual-Task Training with ChatGPT-Assisted Development on Strength, Balance, Spatiotemporal Gait Parameters, and Fall-Related Self-Efficacy in Patients with Chronic Stroke: A Randomized Controlled Trial by Sangyong Han, Jeongeun Yoon and Donghwan Park in NeuroRehabilitation
Supplemental Material
sj-sav-2-nre-10.1177_10538135261449483 - Supplemental material for Effects of Augmented Reality Dual-Task Training with ChatGPT-Assisted Development on Strength, Balance, Spatiotemporal Gait Parameters, and Fall-Related Self-Efficacy in Patients with Chronic Stroke: A Randomized Controlled Trial
Supplemental material, sj-sav-2-nre-10.1177_10538135261449483 for Effects of Augmented Reality Dual-Task Training with ChatGPT-Assisted Development on Strength, Balance, Spatiotemporal Gait Parameters, and Fall-Related Self-Efficacy in Patients with Chronic Stroke: A Randomized Controlled Trial by Sangyong Han, Jeongeun Yoon and Donghwan Park in NeuroRehabilitation
Footnotes
Acknowledgements
We sincerely acknowledge the therapists, nurses, and administrative staff at Happy Hospital for their invaluable support in this study. We also extend our gratitude to all participants for their cooperation and commitment to this study.
Ethical Considerations
Approved by the Institutional Review Board of Kyungnam University (IRB No. 1040460-A-2025-044; approval date: October 14, 2025)
Informed Consent
Written informed consent for publication of identifiable images was obtained from the participant.
CRediT Authorship Contribution Statement
Sangyong Han: Conceptualization, Data curation, Methodology, Formal analysis, Investigation, Validation, Visualization, Writing – original draft.
Jeongeun Yoon: Conceptualization, Methodology, Software, Writing – original draft.
Donghwan Park: Conceptualization, Methodology, Supervision, Project administration, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are not publicly available due to privacy and ethical restrictions. Interested parties may contact the corresponding author for inquiries regarding data access.
Trial Registration
Clinical Research Information Service (CRIS), Republic of Korea (KCT0011287).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.