
Abstract
Background
Chronic stroke survivors often have persistent upper limb impairment. Two distinct therapeutic pathways have emerged: contralateral C7 (CC7) nerve transfer and technology-assisted/high-dose rehabilitation. Direct comparisons and detailed descriptions of rehabilitation protocols between these approaches are lacking.
Objective
To systematically compare upper limb rehabilitation strategies and outcomes in chronic stroke patients with versus without CC7 nerve transfer, and to identify key evidence gaps regarding rehabilitation dose, content, and delivery models.
Methods
A systematic search of multiple databases and trial registries was conducted. Studies on technology-assisted rehabilitation (2016–2025) and CC7 studies (no date restriction) were included. Eligible studies involved adults with stroke and reported upper-limb rehabilitation strategies/outcomes. Evidence was grouped into: (1) CC7 studies, (2) RCTs of technology-assisted rehabilitation, and (3) systematic reviews/meta-analyses.
Results
48 studies were included. Non-surgical interventions (e.g., high-dose training, virtual reality, robotics) yielded small-moderate improvements, especially with high intensity/adherence. CC7 studies reported greater motor function gains and spasticity reduction, but postoperative rehabilitation protocols were poorly described, heterogeneous, and rarely quantified. No trial directly compared CC7 plus structured rehabilitation with optimized non-surgical programs. Most reviews were low quality, and RCTs had short follow-up.
Conclusions
CC7 transfer should be framed as an adjunct to, not a substitute for, high-intensity rehabilitation. Future studies should validate integrated pathways pairing surgery with technology-assisted training, supported by standardized reporting of rehabilitation dose and durable outcomes.
Keywords
Introduction
Stroke remains a leading cause of long-term disability worldwide. Upper limb impairment, characterised by paresis, spasticity, and learned non-use, is particularly prevalent and persistent. Epidemiological data indicate that one-third to one-half of chronic stroke survivors experience significant upper limb deficits, which severely limit daily independence and increase caregiver burden. Even after standard rehabilitation (Allison et al., 2016; Dembele et al., 2024), developing effective strategies for the chronic phase remains a paramount challenge.
Over the past two decades, numerous rehabilitation strategies have emerged, including high-dose task-oriented training, constraint-induced movement therapy (CIMT), robotics, virtual reality, and non-invasive brain stimulation. Systematic reviews confirm that these approaches can yield small to moderate improvements in motor function and activities of daily living (Adams et al., 2023; Bai et al., 2020; Bertani et al., 2017; Hernandez et al., 2022). However, in real-world clinical practice, the benefits are often constrained by insufficient rehabilitation dose and poor patient adherence (Da-Silva et al., 2018; Duncan Millar et al., 2019). Recently, telerehabilitation and home-based technology-assisted interventions have shown promise in increasing training dose and accessibility, especially in resource-limited settings (Carbajal-Galarza et al., 2025; Gebreheat et al., 2024; Guo et al., 2023; Kuo et al., 2023). Nonetheless, considerable heterogeneity in intervention protocols and a lack of direct comparisons between these strategies complicate evidence synthesis and clinical application.
Beyond conventional and technology-enhanced rehabilitation, contralateral C7 (CC7) nerve transfer has emerged as an innovative surgical intervention for chronic spastic arm paralysis. Evidence since the seminal reports by Hua and Zheng demonstrates that CC7 transfer can shorten regeneration distance, reconstruct motor pathways, and induce cortical plasticity, leading to significant reductions in spasticity and functional gains that surpass conventional rehabilitation alone (Hua et al., 2015; Zheng et al. 2018). Subsequent studies and meta-analyses have further elucidated its anatomical rationale, surgical evolution, and central mechanisms, affirming its potential for substantial upper limb recovery with acceptable donor-site morbidity (Bai et al., 2022; Luo et al., 2023; Xu, 2025).
Critically, however, the long-term success of CC7 transfer is highly dependent on structured postoperative rehabilitation. Existing studies describe postoperative protocols that are typically based on conventional therapy but are highly heterogeneous in their timing, content, dose, and follow-up (Bai et al., 2022; Guan et al., 2020; Hua et al., 2015; Luo et al., 2023; Zheng et al., 2018). While a meta-analysis has quantified the added value of the surgery itself, it did not detail the structure of rehabilitation programs or relate them to the broader upper limb rehabilitation literature (Luo et al., 2023). This creates a stark contrast: the evidence base for non-surgical rehabilitation, though heterogeneous, extensively reports on intervention dose and content; whereas the CC7 literature, while robust on surgical efficacy and mechanisms, provides minimal and inconsistent detail on the crucial rehabilitation that follows.
From a mechanistic perspective, this disparity mirrors two different approaches to recovery: CC7 transfer surgically creates a new peripheral pathway and redistributes motor control, whereas most advanced non-surgical strategies aim to strengthen residual pathways and promote neuroplasticity. For CC7 recipients, recovery thus entails a dual challenge: overcoming the common barriers of dose and adherence faced by all chronic stroke patients (Carbajal-Galarza et al., 2025; Da-Silva et al., 2018; Guo et al., 2023), and meeting the unique requirement of optimally training newly established neural pathways. Currently, no review has systematically mapped and compared the rehabilitation protocols—their content, dose, and follow-up—used for patients with and without nerve transfer. This gap obscures our understanding of where the most pressing deficits in rehabilitation strategies and reporting truly lie.
Against this background, the systematic review, “Identifying Gaps in Rehabilitation Strategies for Chronic Stroke: A Systematic Review of Evidence in Patients With and Without Nerve Transfer,” aims to synthesize evidence from randomized trials, prospective cohorts, and high-quality reviews. Its objectives are threefold: First, to describe and compare rehabilitation models, doses, and outcome measures across both patient groups. Second, to contrast functional outcomes and identify deficiencies in the evidence base regarding dose, therapeutic windows, and scalability. Third, to summarize reporting limitations and provide guidance for future research. By examining rehabilitation through the dual lens of surgical and non-surgical pathways, this review seeks to clarify the most evidence gaps to inform clinical practice and future research.
Methods
Design and Reporting
This study was designed as a systematic review of rehabilitation strategies for chronic upper limb dysfunction after stroke in patients with and without nerve transfer. The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA 2020) recommendations for planning, conduct, and reporting of systematic reviews (Page et al., 2021). Any deviations from the initial plan are described in the Results and Discussion sections.
Eligibility Criteria
Eligibility criteria were defined a priori using the PICOS framework (Population, Intervention, Comparator, Outcomes, Study design).
Population
Adults (≥18 years) with upper limb motor impairment due to ischemic or hemorrhagic stroke beyond the acute phase.
Chronic stroke was defined as at least 3 months after stroke onset, or studies explicitly describing participants as “subacute/chronic” or “chronic”.
For the nerve transfer dataset, additionally included patients with central upper limb hemiplegia due to stroke, traumatic brain injury, or cerebral palsy who underwent contralateral C7 (CC7) or related nerve transfer procedures, given the limited evidence base.
Interventions
Non-surgical rehabilitation strategies for the paretic upper limb, including but not limited to:
Conventional high-intensity task-specific training and constraint-induced movement therapy Technology-assisted and home-based programs such as tele-rehabilitation, virtual reality, gaming-based therapy, wearable or robot-assisted training, brain-computer interfaces, and self-directed training programs. Neuromodulation assisted approaches (e.g., non-invasive brain stimulation, peripheral magnetic or electrical stimulation, vagus nerve stimulation) provided they were combined with structured rehabilitation.
Comparators
Any comparator was eligible, including conventional in-person rehabilitation, other active rehabilitation strategies, sham stimulation, or usual care. For case series and single-arm studies of nerve transfer, the absence of a comparator group was accepted.
Outcomes
Studies were eligible if they reported at least one of the following upper limb outcomes:
Motor impairment or motor function, for example, Fugl-Meyer Assessment of the Upper Extremity (FMA UE), Action Research Arm Test (ARAT), Wolf Motor Function Test, Jebsen Taylor Hand Function Test, Box and Block Test, or similar validated measures Muscle tone or spasticity (for example, Modified Ashworth Scale) Activity and participation measures, including activities of daily living, quality of life, patient-reported use of the paretic arm, or satisfaction with rehabilitation For nerve transfer studies, additional outcomes such as range of motion, strength, donor limb morbidity, and neurophysiological measures (electrophysiology) were extracted when available.
Study Design
For non-surgical rehabilitation strategies, included randomized controlled trials (parallel or crossover) and high quality prospective controlled studies.
For nerve transfer procedures, included randomized controlled trials, prospective or retrospective cohort studies, and case series with clearly described surgical techniques and follow-up.
In addition, included systematic reviews and meta-analyses of post-stroke upper limb rehabilitation when they reported quantitative synthesis of randomized or quasi-experimental studies. These reviews were used to map the broader evidence base and to contextualise the primary studies. Narrative reviews, editorials, conference abstracts without sufficient data, animal studies, and technical notes without clinical outcomes were excluded.
Information Sources
A comprehensive search of electronic databases was conducted from January 2016 to November 2025 for studies on high-dose upper-limb rehabilitation and technology-assisted interventions. In parallel, given the limited and historically concentrated evidence base for contralateral C7 (CC7) nerve transfer, the search for primary CC7 clinical studies was conducted without publication date restrictions. The following sources were searched:
PubMed and MEDLINE via the PubMed interface Web of Science Core Collection Scopus Cochrane Library, including the Cochrane Central Register of Controlled Trials (CENTRAL) and the Cochrane Database of Systematic Reviews World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) ClinicalTrials.gov.
In addition, reference lists of all included articles and relevant systematic reviews were manually screened to identify further eligible studies that might have been missed by the electronic search.
Search Strategy
Two main concept blocks were constructed:
Chronic stroke and upper limb impairment Rehabilitation strategies and nerve transfer procedures
For the stroke and upper limb concept, keywords and controlled vocabulary included “stroke”, “cerebrovascular accident”, “hemiplegia”, “hemiparesis”, “upper limb”, “upper extremity”, “arm”, and “hand”.
For the rehabilitation and nerve transfer concept, terms included “rehabilitation”, “telerehabilitation”, “virtual reality”, “robot assisted therapy”, “brain–computer interface”, “self directed”, “constraint induced movement therapy”, “non invasive brain stimulation”, “transcranial direct current stimulation”, “repetitive transcranial magnetic stimulation”, “vagus nerve stimulation”, “extracorporeal shock wave therapy”, “localized muscle vibration”, “transcutaneous electrical nerve stimulation”, “upper limb technology”, “contralateral C7”, “cervical 7 nerve transfer”, “nerve transfer”, and related synonyms.
The two blocks were combined with the Boolean operator AND. Search filters for adults and humans were applied when available, but no restrictions on publication type or study design were used at the electronic search stage, to maximize sensitivity. The full search strategies for all databases are provided in Supplementary Appendix A.
Study Selection
All search results were exported into EndNote 21 (Clarivate Analytics). Duplicates across databases were removed using the automatic de-duplication function followed by a manual check of author names, titles, and publication details.
Study selection was conducted in two stages:
PRISMA 2020 flow diagram depicting the study selection process.
Data Extraction
Pilot testing was conducted on qualified research samples from each thematic group. The extracted items included:
Study characteristics: first author, year of publication, country, setting, funding source Study design: randomized trial, crossover trial, cohort, case series, systematic review, or meta-analysis Participants: sample size, age, sex distribution, time since stroke, type of stroke, inclusion and exclusion criteria Surgical details for nerve transfer studies: type of procedure (for example, contralateral C7 to C7 cross transfer, Huashan prespinal route, posterior route), timing relative to stroke, follow-up duration, and reported complications Rehabilitation intervention characteristics: modality (for example, telerehabilitation, virtual reality glove, exoskeleton assisted training, robot assisted therapy, neuromodulation, self-directed programs), dose (session duration, weekly frequency, total number of sessions), setting (inpatient, outpatient, home-based, hybrid), technology platform, and involvement of therapists or tele supervision Comparator details: type and dose of conventional therapy or other interventions Outcomes: all predefined primary and secondary upper limb outcomes at baseline and at each reported follow-up time point, including adherence and dropout where reported Systematic reviews: search period, number and type of included primary studies, main findings, and conclusions regarding efficacy and safety.
Risk of Bias and Quality Assessment
Risk of bias was assessed separately according to study design. Randomized controlled trials were evaluated with the Cochrane Risk of Bias 2.0 tool for randomized trials (RoB 2) (Sterne et al., 2019). Non-randomized comparative and observational studies of nerve transfer were appraised using the ROBINS-I tool for non-randomized studies (Sterne et al., 2016). Case series were assessed with the Joanna Briggs Institute critical appraisal checklist for case series (Munn et al., 2015), and systematic reviews or meta-analyses with the AMSTAR 2 instrument (Shea et al., 2017). These judgments informed the interpretation of findings and, where meta-analysis was possible, sensitivity analyses excluding studies at high risk of bias.
Data Synthesis and Analysis
Because the primary aim of this review was to identify gaps in rehabilitation strategies rather than to derive a single pooled effect estimate, substantial clinical and methodological heterogeneity across interventions, populations, and outcome measures was anticipated. Accordingly, a two-level synthesis strategy was prespecified.
For randomized controlled trials, a meta-analysis was planned when at least three studies evaluated similar interventions in comparable populations and reported the same outcome at a similar time point. In such cases, random effects models were to be applied. Effect sizes for continuous outcomes (for example, FMA-UE, ARAT, and the Modified Ashworth Scale) were expressed as mean differences or standardized mean differences with 95% confidence intervals, and statistical heterogeneity was quantified using the I2 statistic. When meta-analysis was not judged appropriate, trial findings were synthesized narratively.
In addition, a structured narrative synthesis was conducted across major intervention families. For each category (such as tele-rehabilitation and virtual reality, robot-assisted and exoskeleton training, neuromodulation-assisted rehabilitation, self-directed programs, brain–computer interfaces, and nerve transfer surgery with postoperative rehabilitation), study characteristics, intervention dose, outcomes, and safety profiles were summarized. The narrative was organized to compare rehabilitation strategies in chronic stroke populations without nerve transfer, rehabilitation content, timing, and outcomes after CC7 or related nerve transfer procedures, and the overlaps and gaps between these two populations, particularly with respect to training dose, follow-up duration, adherence, and the use of hybrid or home-based models. Where possible, findings from included systematic reviews were mapped against the primary trials identified in this review to avoid double counting and to distinguish areas supported by high quality randomized evidence from those in which only lower level studies or case series are currently available.
Certainty of Evidence
For key intervention outcome pairs supported by more than one randomized controlled trial, the certainty of the evidence was considered narratively. In judging certainty, particular attention was paid to risk of bias, consistency of findings across studies, directness of the populations and outcomes, precision of effect estimates, and the possibility of publication bias. Formal summary of findings tables were not generated because of the limited number of sufficiently homogeneous trials for most comparisons.
Results
Study Selection Process
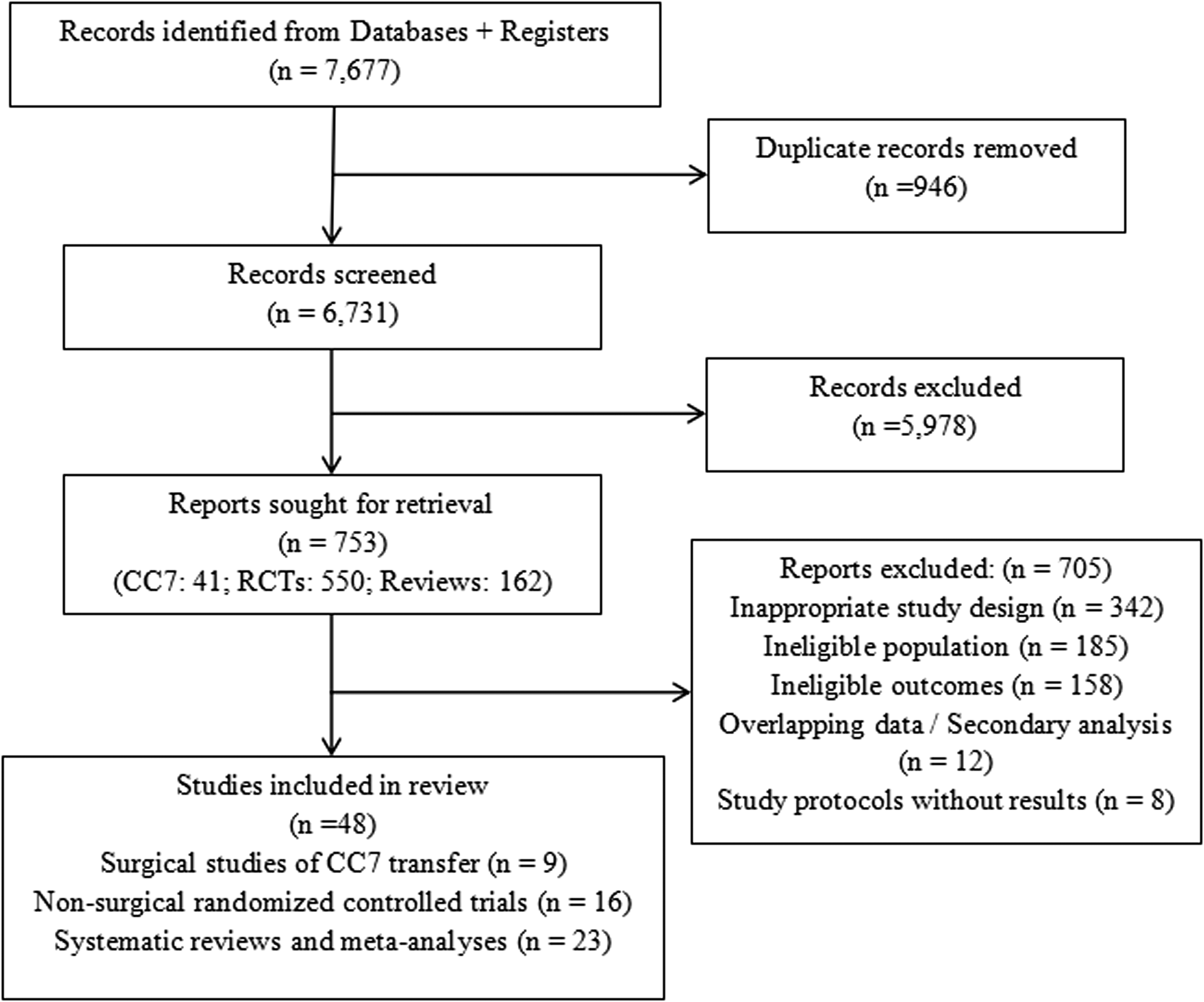
Based on the predefined search strategy, a total of 7,677 records were retrieved from PubMed, Scopus, Web of Science, the Cochrane Library, and the WHO ICTRP/ClinicalTrials registry. All records were imported into EndNote for automated duplicate removal, yielding 6,731 remaining records. Subsequently, studies were screened by title and abstract to exclude those clearly irrelevant.
Within the reference manager, upper limb-related records were further organised into three broad thematic groups based on keywords and subject headings: original upper limb rehabilitation studies, randomized controlled trials involving the upper limb, and systematic reviews or meta-analyses on upper limb rehabilitation. Focused screening within these groups yielded 41 potentially relevant reports related to contralateral C7 (CC7) or other nerve transfer procedures, 550 randomized trials of telerehabilitation or technology-assisted upper limb rehabilitation, and 162 systematic reviews or meta-analyses addressing upper limb rehabilitation. The marked reduction from the initial 6,731 records to this subset (753 reports in total) reflects the combination of a deliberately broad, sensitive search strategy and strict eligibility criteria focusing on chronic stroke upper limb rehabilitation with and without nerve transfer.
Full texts of these three sets of studies were then assessed against the prespecified inclusion and exclusion criteria. Studies were excluded if they did not involve a stroke population, did not include upper limb outcomes as a main endpoint, or were non-interventional in design (e.g., narrative reviews, case reports), were available only as study protocols without final results, or represented duplicate publications/overlapping data. In total, 48 studies met the inclusion criteria, comprising 9 clinical studies related to CC7 or related nerve transfer procedures, 23 systematic reviews or meta-analyses on upper limb rehabilitation, and 16 predominantly randomized trials of technology-assisted or remote upper limb rehabilitation.
The complete study selection process is summarized in the PRISMA flow diagram (Figure 1), which presents the number of records screened and the total of 705 reports excluded at the full-text assessment stage, together with the main reasons for exclusion, including inappropriate study design, ineligible population, ineligible outcomes, overlapping data, and study protocols without final results.
General Characteristics of Included Studies
Overall, the included studies were conducted predominantly in upper middle and high income settings. Most CC7-related reports originated from single-center or small multicenter cohorts in China, whereas non-surgical upper limb rehabilitation trials were mainly undertaken as single or multicenter randomized controlled trials in Europe, North America, East Asia, and the Middle East.
With regard to study design, the CC7 literature comprised one prospective randomized controlled trial (for example, the trial reported by Zheng and colleagues), several prospective or retrospective controlled cohorts, single-arm observational cohorts, and multiple case series, alongside a small number of narrative or overview papers. The systematic reviews generally followed PRISMA or comparable reporting frameworks, although a subset were narrative reviews without formal protocol registration. The original rehabilitation trials were predominantly two-arm parallel group RCTs, with a few studies adopting three-arm designs or randomized crossover designs.
Participant characteristics also differed across study groups. CC7 studies typically enrolled patients with chronic unilateral spastic hemiparesis of the upper limb, most often with a duration of at least one year after stroke and, in some cohorts, more than five years, representing patients with little or no further improvement under conventional rehabilitation. Non-surgical rehabilitation trials covered a wider range of time since stroke, from subacute to chronic phases. Some trials restricted inclusion to patients at least 3 or 6 months post stroke, whereas others combined acute, subacute, and chronic participants in the same analysis. In most studies, at least moderate impairment of upper limb function was required for inclusion, commonly defined or stratified using the Fugl-Meyer Assessment of the upper extremity, Brunnstrom staging, or manual muscle testing.
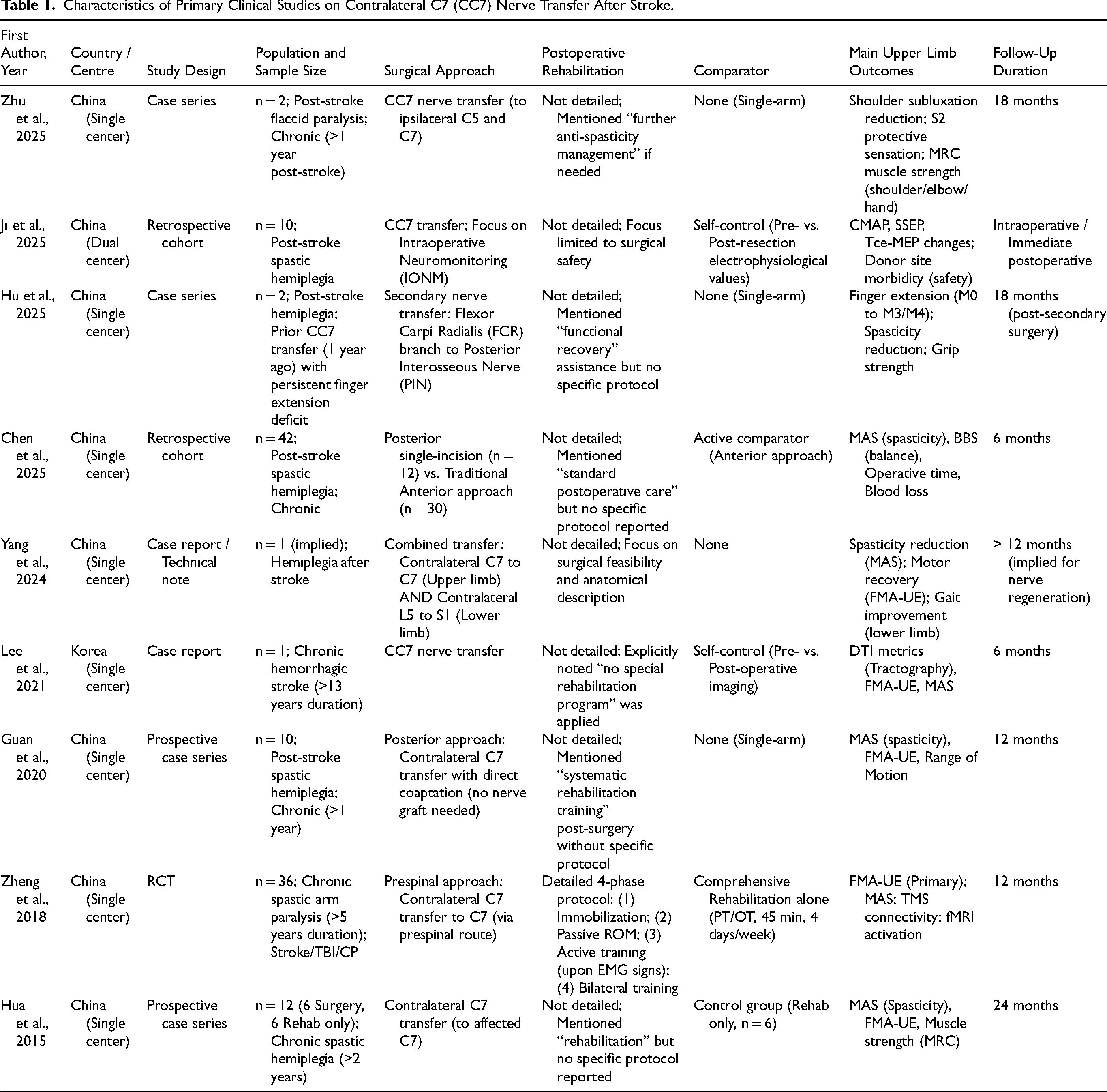
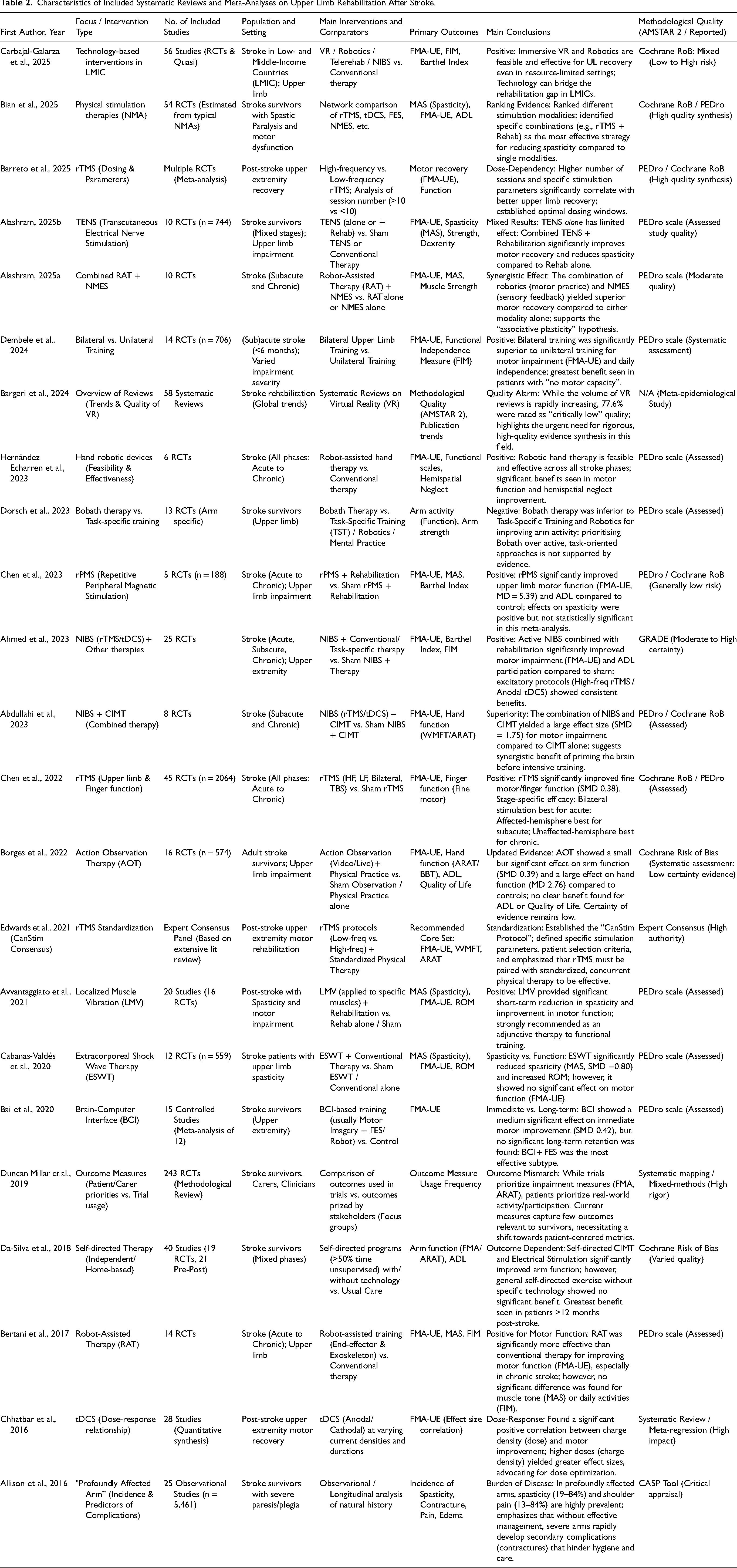
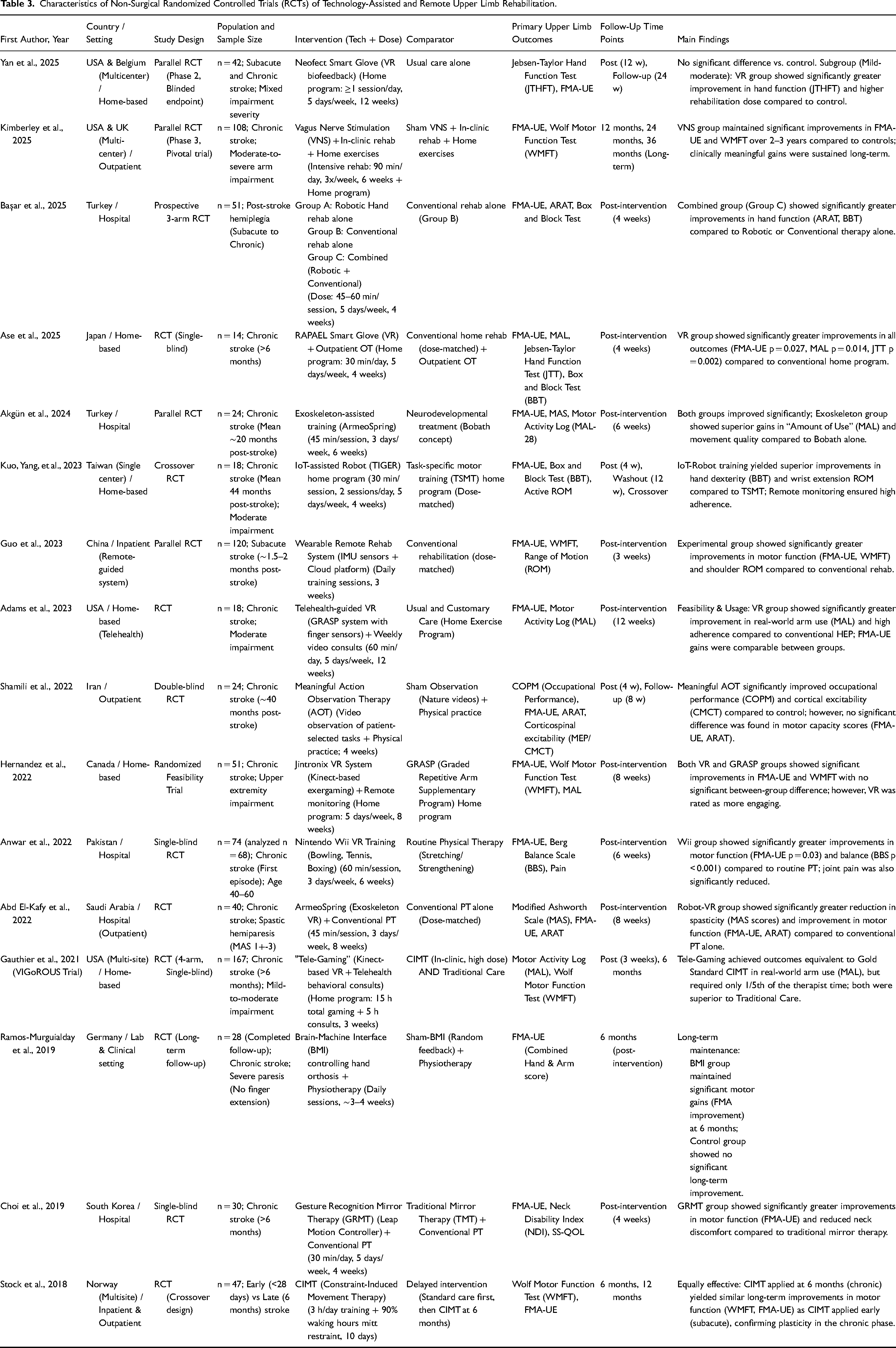
A relatively consistent set of outcome measures was used across the included studies. The most frequently used measures included the Fugl-Meyer Assessment-Upper Extremity (FMA-UE), the Modified Ashworth Scale (MAS), the Action Research Arm Test, the Wolf Motor Function Test, the Barthel Index, and the Motor Activity Log, thereby covering impairment, activity, and basic activities of daily living. Several studies additionally reported grip strength, hand dexterity tests, pain scales, and health-related quality of life measures. The general characteristics of the included studies are summarized separately in Table 1 (CC7 related studies), Table 2 (systematic reviews and meta-analyses), and Table 3 (original randomized controlled trials).
Characteristics of Primary Clinical Studies on Contralateral C7 (CC7) Nerve Transfer After Stroke.
Characteristics of Included Systematic Reviews and Meta-Analyses on Upper Limb Rehabilitation After Stroke.
Characteristics of Non-Surgical Randomized Controlled Trials (RCTs) of Technology-Assisted and Remote Upper Limb Rehabilitation.
Rehabilitation Strategies for Patients Without Nerve Transfer
In chronic stroke populations who have not undergone nerve transfer, the included literature demonstrates a wide range of upper limb rehabilitation approaches that can be broadly grouped into several categories.
High Dose Task-Oriented Training and CIMT
Multiple systematic reviews and randomized controlled trials have shown that constraint-induced movement therapy (CIMT) and other forms of high-dose task-oriented training can produce moderate improvements in FMA-UE scores and activities of daily living, particularly in chronic patients who retain some residual voluntary movement in the affected arm (Da-Silva et al., 2018; Dembele et al., 2024; Dorsch et al., 2023). Some studies have compared early versus delayed initiation of CIMT, reporting similar long-term outcomes at 12-month follow-up but a steeper early recovery trajectory in the early intervention group (Stock et al., 2018).
Virtual Reality and Game-Based Rehabilitation
Systematic reviews consistently indicate that training that uses virtual reality technology produces small to moderate positive effects on upper limb motor function, and at the same time allows higher training doses and greater patient engagement compared with conventional therapy (Bargeri et al., 2024; Carbajal-Galarza et al., 2025). Among the randomized controlled trials included in this review, programs delivered at home or under remote supervision and using virtual reality systems such as glove devices with motion sensors and serious game platforms have led to significant improvements in outcomes, including the Jebsen–Taylor Hand Function Test, the Fugl–Meyer Assessment of the Upper Extremity (FMA-UE) and the Motor Activity Log. In several trials, gains in FMA-UE and arm use reached or approached accepted minimal clinically important difference thresholds, suggesting that virtual reality and game-based rehabilitation can provide clinically meaningful benefits for everyday arm and hand use in chronic stroke survivors (Adams et al., 2023; Ase et al., 2025; Hernandez et al., 2022).
Robotics and Wearable Devices
Systematic reviews of robot-assisted upper limb training generally conclude that programs which combine robotic therapy with conventional rehabilitation produce greater gains in upper limb motor function than conventional therapy alone, with particularly clear benefits in chronic stroke populations (Alashram, 2025a; Hernández Echarren & Sánchez Cabeza, 2023). However, effects on muscle tone, spasticity, and independence in daily activities are less consistent across studies. More recent randomized trials indicate that adding robotic devices to standard physical or occupational therapy can yield larger improvements in Fugl–Meyer Assessment of the Upper Extremity scores, activities of daily living, and hand grip strength than traditional approaches delivered at a similar dose (Abd El-Kafy et al., 2022; Akgün et al., 2024; Ko et al., 2023). In these trials, upper limb exoskeletons or wearable sensor-driven training systems were used as part of high-frequency, highly repetitive practice blocks, and the findings suggest that such mechanically assisted training can safely increase the use of the paretic limb in everyday tasks and enhance patient engagement in longer-term rehabilitation programs.
Non-Invasive Brain Stimulation and Peripheral Stimulation
Meta-analysis of non-invasive brain stimulation indicates that repetitive transcranial magnetic stimulation and transcranial direct current stimulation, when combined with conventional rehabilitation, can provide small to moderate improvements in upper limb motor function in the acute and subacute phases and may also enhance activities of daily living as reflected by Barthel Index scores (Ahmed et al., 2023; Chen et al., 2022; Chhatbar et al., 2016). In the chronic phase, effects appear more modest and seem to depend on higher stimulation doses, careful optimisation of stimulation parameters, and close pairing with task-oriented training (Ahmed et al., 2023; Chhatbar et al., 2016). For peripheral modalities such as transcutaneous electrical nerve stimulation, repetitive peripheral magnetic stimulation, and localised muscle vibration, recent systematic reviews and meta-analyses suggest potential benefits in reducing spasticity, improving proximal strength, and alleviating some activity limitations, whereas effects on distal hand dexterity, global functional independence, and long-term quality of life remain uncertain (Alashram, 2025b; Avvantaggiato et al., 2021; Chen et al., 2023).
Brain–Computer Interfaces and Self-Directed Training
Brain-computer interface (BCI) based interventions that couple neural signals with functional electrical stimulation or robotic assistance have been associated with significant short-term improvements in FMA-UE scores at the end of treatment in people with chronic stroke (Bai et al., 2020; Ramos-Murguialday et al., 2019). However, it remains uncertain to what extent these gains are sustained over longer term follow-up, as most studies include relatively small samples and limited post-intervention assessments. Self-directed training programs, including home exercise plans, remotely supervised practice, and systems with wearable feedback devices, generally report substantial increases in daily practice time and higher use of the affected limb in chronic stroke, with improvements in independence for selected daily activities, particularly among patients with relatively higher baseline function (Adams et al., 2023; Da-Silva et al., 2018). Taken together, rehabilitation strategies for patients without nerve transfer span a continuum from traditional high-dose task-specific training to multiple technology-assisted modalities. However, there is marked heterogeneity in treatment dose, combinations of modalities, intervention duration, and follow-up length, which complicates direct comparisons between approaches and limits the robustness of evidence synthesis across this body of literature.
Rehabilitation Strategies and Outcomes After CC7 Nerve Transfer
The 12 included CC7 related studies collectively reflect the evolution of this procedure from early anatomical verification and feasibility work, through refinement of surgical approaches, to longer term clinical follow up in patients with central spastic arm paralysis.
Functional Outcomes
The pivotal randomized controlled trial demonstrated that patients receiving CC7 transfer in addition to standard rehabilitation achieved an increase of about 15 points in FMA-UE at 12 months, clearly exceeding the gains observed in the rehabilitation only group (Zheng et al., 2018). This improvement was accompanied by significant reductions in MAS scores, indicating concurrent relief of spasticity and enhancement of voluntary motor control. Subsequent pooled analyses and systematic reviews have confirmed that CC7 surgery yields medium to large effect sizes for FMA-UE, joint range of motion, and spasticity reduction, while having only limited impact on donor side upper limb function, most commonly transient sensory changes rather than persistent weakness or disability (Bai et al., 2022; Luo et al., 2023; Xu, 2025).
Surgical Approaches and Complications
Anatomical and technical studies have documented a progression from early subcutaneous tunnelling techniques to the Huashan prespinal route and, more recently, to posterior or intraspinal approaches for contralateral C7 transfer (Bai et al., 2022; Du et al., 2022; Guan et al., 2021; Xu, 2025; Zheng et al., 2018). The overall trend has been towards shortening the regeneration distance, reducing the need for interposed nerve grafts, and lowering the risk of vertebral artery injury. Findings from small cohort follow-up suggest that posterior or other short-distance approaches are associated with shorter operative times, reduced intraoperative blood loss, and lower rates of persistent postoperative numbness and pain compared with earlier techniques (Bai et al., 2022; Du et al., 2022; Guan et al., 2021). Across series, donor-side morbidity has generally been limited to transient reductions in sensation or mild weakness, with most patients recovering function over time (Luo et al., 2023; Zheng et al., 2018). However, individual reports have noted that a minority of patients develop clinically significant neuropathic pain after surgery, which may require combined pharmacological and physical therapy interventions and should be discussed with patients during preoperative counselling (Bai et al., 2022; Xu, 2025).
Postoperative Rehabilitation Protocols and Follow-up
Most CC7 studies state that a standardised rehabilitation program was provided after surgery, but the specific content and dose of these programs are reported with considerable variability (Bai et al., 2022; Du et al., 2022; Guan et al., 2021; Luo et al., 2023; Zheng et al., 2018). Common elements include passive range of motion, positioning strategies and protection of the donor limb during the early postoperative phase, followed by progressive introduction of bilateral coordinated movements, mirror therapy and task-oriented training in parallel with the expected course of nerve regeneration. In a few reports, additional modalities such as robotic training, non-invasive brain stimulation, or local neuromodulation were explored as adjunctive interventions, but these were applied in small, heterogeneous cohorts and without clear reporting of dose or timing (Bai et al., 2022; Xu, 2025).
Despite these descriptions, very few studies have systematically quantified the intensity of postoperative rehabilitation, the actual dose completed by patients, adherence over time, or long-term follow-up of functional trajectories (Luo et al., 2023; Xu, 2025). Direct comparative trials that contrast CC7 specific postoperative rehabilitation protocols with rehabilitation strategies used in non-surgical chronic stroke populations are essentially lacking. This gap constitutes a central issue highlighted by the present review, which seeks to highlight, particularly in relation to rehabilitation dose, adherence, and the potential role of hybrid or home-based models for patients after CC7 nerve transfer.
Quality of Evidence and Risk of Bias
Application of the AMSTAR 2 tool to the included systematic reviews showed that only a small number could be rated as of moderate or higher methodological quality. Most reviews were judged to be of low or critically low confidence because of incomplete or poorly reported search strategies, lack of protocol registration, limited or absent assessment of risk of bias in the primary studies, and insufficient exploration or explanation of statistical heterogeneity.
For the original randomized controlled trials, risk of bias was assessed using the RoB 2 tool. In general, reporting on random sequence generation and allocation concealment was acceptable in most studies. However, several recurrent limitations were identified. First, blinding of therapists and participants was rarely feasible, which means that performance bias cannot be ruled out, even though outcome assessors were often masked. Second, trials frequently used multiple outcome measures at different time points, and selective reporting of outcomes or time points cannot be excluded. Third, follow-up periods were usually short, with relatively few studies extending beyond six months, which limits inferences about long-term effectiveness and adherence.
For non-randomized comparative and observational studies of CC7, ROBINS-I ratings were mostly in the serious or critical risk of bias categories, mainly because of nonrandom allocation, baseline imbalances, and limited control for potential confounders. Case series appraised with the Joanna Briggs Institute checklist showed additional concerns related to small sample size, unclear recruitment methods, and incomplete follow-up.
Among the CC7-related studies, all designs other than the pivotal randomized trial were nonrandomized, including single-arm cohorts and uncontrolled case series. These studies showed serious risks of bias due to selection of participants and inadequate control for potential confounding, as well as variable completeness of follow-up. In addition, postoperative rehabilitation protocols were often insufficiently standardised or poorly described, making it difficult to disentangle the specific contribution of the surgical procedure itself from the effects of intensified or prolonged rehabilitation.
Discussion
Summary of Main Findings
This review identified 48 studies after screening 6,731 records. The evidence reveals three key observations. First, in chronic stroke without nerve transfer, diverse —from high-dose task training to technology-assisted interventions—yield small to moderate functional improvements, though marked heterogeneity in dose and follow-up limits cross-trial comparisons (Ahmed et al., 2023; Bai et al., 2020; Bertani et al., 2017; Carbajal-Galarza et al., 2025). Second, CC7 transfer achieves medium-to-large effect sizes in reducing spasticity and restoring motor control, with generally transient donor-side morbidity (Bai et al., 2022; Hua et al., 2015; Luo et al., 2023; Zheng et al., 2018). Third, and most critically, reporting of postoperative rehabilitation after CC7 is strikingly inconsistent and less detailed compared to non-surgical trials, creating a major gap that hinders comparison and clinical translation (Luo et al., 2023; Xu, 2025). Thus, while CC7 can reconstruct pathways, long-term recovery depends on postoperative rehabilitation—the very component that is least well documented and studied.
Comparison Between Postoperative Rehabilitation After CC7 and non-Surgical Rehabilitation
The evidence for non-surgical upper limb rehabilitation is mature and detailed. High-dose task-oriented training and CIMT consistently improve function, with some evidence favoring earlier initiation (Da-Silva et al., 2018; Dorsch et al., 2023; Stock et al., 2018). Virtual reality/gaming increasing engagement and dose (Bargeri et al., 2024; Carbajal-Galarza et al., 2025). Robotics enhance repetition and outcomes beyond conventional therapy (Akgün et al., 2024; Bertani et al., 2017; Hernández Echarren & Sánchez Cabeza, 2023). Non-invasive brain stimulation shows phase-dependent benefits (Barreto et al., 2025; Chen et al., 2022), while peripheral modalities help manage spasticity though effects on global function are mixed (Avvantaggiato et al., 2021; Cabanas-Valdés et al., 2020). Brain-computer interfaces yield notable short-term gains (Bai et al., 2020), and self-directed/tele-rehabilitation programs boost practice time and limb use (Adams et al., 2023; Da-Silva et al., 2018; Guo et al., 2023).
In stark contrast, the CC7 literature focuses on surgical technique and mechanisms, with rehabilitation often summarised vaguely as “a standardised rehabilitation program was provided.” Few reports detail frequency, duration, task content, or progression (Guan et al., 2020; Hua et al., 2015; Zheng et al., 2018). Telerehabilitation/hybrid models and adherence metrics are rarely reported. Consequently, while we have rich data on how to train on-surgical patients, and robust evidence on why CC7 works and how to perform it, a clear gap exists in how to train after surgery.
Implications for Designing Postoperative Rehabilitation After CC7
Synthesising the evidence suggests key principles for post-CC7 rehabilitation design:
Adopt a high-dose, task-oriented framework with long follow-up. Clinically important gains in non-surgical studies correlate with adequate dose and duration (Akgün et al., 2024; Da-Silva et al., 2018). Post-CC7 protocols must move beyond vague descriptions to specify weekly minutes, repetitions, and staged goals to exploit new neural pathways.
Embed bilateral, task-specific practice. Recovery after CC7 involves cortical reorganisation (Lee et al., 2021; Zheng et al., 2018). Early bilateral/mirror therapy may harness the contralateral cortex, transitioning later to unilateral fine-motor tasks, consistent with bilateral training evidence (Dembele et al., 2024).
Leverage tele-rehabilitation/technology to maintain dose and adherence. Home-based virtual reality/robotics increase practice time and adherence in chronic stroke (Adams et al., 2023; Guo et al., 2023). A hybrid model—intensive initial in-person training followed by home-based technology-assisted practice with remote supervision—is promising for CC7 patients who face travel burdens.
Standardise adherence and dose reporting. Technology trials explicitly report completed sessions and relate them to outcomes (Yan et al., 2025). Future CC7 studies must report prescribed vs. completed dose to distinguish surgical efficacy from rehabilitation adequacy.
Evidence Gaps and Directions for Future Research
The review highlights critical gaps:
Standardised deficit: Post-CC7 protocols lack standardisation, with scant detail on dose, phase-specific goals, or modality combinations. Future trials should make the rehabilitation protocol the primary variable (Hua et al., 2015; Luo et al., 2023).
Lack of direct comparison with intensive rehabilitation: CC7's incremental effect over equally intensive non-surgical rehabilitation is unknown, as most comparisons use modest-dose controls (Hua et al., 2015; Zheng et al., 2018). Dose-response relationships underscore the importance of this comparison (Chhatbar et al., 2016). Unexplored feasibility of telerehabilitation/hybrid models POST-CC7: While feasible in non-surgical populations (Adams et al., 2023; Guo et al., 2023), the safety and feasibility of home-based training for CC7 recipients during nerve regeneration are unstudied.
Limited long-term and economic data: Most trials have short follow-up; costs and caregiver burden are rarely analyzed, hindering scalability assessment, especially in resource-limited settings.
Outcome measures mismatch: Common scales (e.g., FMA-UE) fail to capture patient-prioritised outcomes like daily arm use and caregiver burden (Duncan Millar et al., 2019). Future research should include these patient-centred measures.
Priority should be given to multicenter PCTs testing hybrid telerehabilitation models post-CC7, comparing different doses and technology combinations for long-term outcomes, adherence, and cost-effectiveness.
Strengths and Limitations of This Review
Strengths include a comprehensive search strategy, structured screening yielding three coherent study groups, and a focused comparison that provides a direct reference for future trial design. Limitations involve the use of narrative synthesis over meta-analysis for some outcomes, potential selection bias from single-reviewer involvement in screening/quality assessment, restriction to English publications, and clinical/methodological heterogeneity among included studies. A small subset of CC7 studies included non-stroke populations, which may slightly limit generalisability. Overall, CC7 and non-surgical rehabilitation are complementary strategies. The central challenge is integrating them postoperatively and testing, via high-quality trials, whether combined surgical-hybrid rehabilitation delivers durable, cost-effective gains in real-world settings.
Conclusions
This review synthesizes evidence on rehabilitation for chronic upper limb impairment post-stroke. For non-surgical patients, high-dose task-oriented training is foundational, augmented by various technology-assisted strategies, albeit with persisting heterogeneity. CC7 transfer is a feasible, effective option for spastic paresis. However, its postoperative rehabilitation is poorly specified, and direct comparisons with intensive non-surgical rehabilitation are lacking.
Clinically, CC7 should be viewed as an adjunct within a broader rehabilitation intensification in carefully selected patients. Most chronic stroke survivors are likely to continue relying on high-dose, task-oriented training as a first-line rehabilitation intensification strategy, not a replacement. Hybrid/remote models are crucial for sustaining training. Outcome assessment must better incorporate patient-reported measures.
The most pressing research gaps concern post-CC7 rehabilitation. Priorities include trials with rehabilitation as the primary variable, head-to-head comparisons of CC7 plus intensive rehab versus intensive rehab alone, feasibility studies of hybrid models for CC7 recipients, and longer-term economic evaluations. In conclusion, CC7 nerve transfer and non-surgical rehabilitation are complementary: one surgically modifies pathways, the other provides high-dose, often remote tools for retraining. Integrating them into scientifically robust, scalable care pathways is essential for improving outcomes in chronic stroke.
Supplemental Material
sj-docx-1-nre-10.1177_10538135261454931 - Supplemental material for Identifying Gaps in Rehabilitation Strategies for Chronic Stroke: A Systematic Review of Evidence in Patients With and Without Nerve Transfer
Supplemental material, sj-docx-1-nre-10.1177_10538135261454931 for Identifying Gaps in Rehabilitation Strategies for Chronic Stroke: A Systematic Review of Evidence in Patients With and Without Nerve Transfer by Haoting Shi, Chao Ren and Siti Ruzita Mahmod in NeuroRehabilitation
Footnotes
Acknowledgments
We thank all researchers, clinicians, and patients who contributed to the included studies, as well as colleagues for their methodological support in conducting this systematic review.
Ethical Approval
This study is a systematic review of previously published literature and does not involve new data collection from human or animal subjects. Therefore, ethical approval from an institutional review board was not required.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Haoting Shi: Conceptualization, Methodology, Investigation (Literature search, study selection, and data extraction), Formal analysis, Writing – Original Draft, Writing – Review & Editing, Visualization.
Chao Ren: Investigation (Study selection and data extraction), Validation (Cross-checking of extracted data), Formal analysis, Writing – Review & Editing.
Siti Ruzita Mahmod: Conceptualization, Methodology, Validation, Resources (Supervision of the review process), Writing – Review & Editing, Project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
The datasets supporting the conclusions of this article (including the list of included studies and extracted data) are available from the corresponding author upon reasonable request.
Authors’ Agreement
We confirm that all authors have read and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.