
Abstract
Objectives
Chronic subdural hematoma (CSDH) generally has favorable outcomes; however, some patients develop balance and gait impairments, leading to prolonged hospitalization. This study examined the association between Mini-Balance Evaluation Systems Test (Mini-BESTest) scores, and length of hospital stay (LOS) after CSDH surgery.
Methods
This prospective cohort study was conducted at a single acute care hospital in Japan. Patients aged ≥ 65 years who underwent burr-hole drainage for CSDH were included. Exclusion criteria were orthopedic disease, psychiatric disease, inability to complete the Mini-BESTest, and premorbid modified Rankin Scale ≥ 4. Variables included age, sex, initial National Institutes of Health Stroke Scale, Glasgow Coma Scale, Mini-Mental State Examination–Japanese, residual hematoma thickness, premorbid modified Rankin Scale (mRS), Mini-BESTest score, and LOS. Spearman correlation and multivariable linear regression analyses were performed.
Results
Of 49 patients, 32 were analyzed after exclusions due to comorbidities, inability to complete the assessment, or premorbid disability. Twenty-five patients were men and the mean age was 81.8 ± 5.0 years. The median LOS was 8.5 (interquartile range [IQR] 8–11) days, and the Mini-BESTest was 18.5 (IQR 13.8–23.3). LOS was negatively correlated with Mini-BESTest (r = −0.499) and positively with initial NIHSS (r = 0.376). In multivariable regression, Mini-BESTest (β = −0.488) and initial NIHSS (β = 0.377) scores were associated with LOS.
Conclusions
Early postoperative balance function may be associated with LOS in patients with CSDH. Early Mini-BESTest assessment may help identify patients at risk for prolonged hospitalization and guide rehabilitation and discharge planning.
Keywords
Introduction
Global population aging is rapidly progressing, and the management of diseases prevalent among older adults has become an important healthcare issue. Japan is one of the most rapidly aging countries in the world and is often regarded as a model case of a super-aging society. The annual incidence of chronic subdural hematoma (CSDH) in Japan was 13.1 per 100,000 people in 1992 and increased to 20.6 per 100,000 in 2011, reflecting a rapid increase in incidence with population aging (Karibe et al., 2011; Kudo et al., 1992). CSDH often develops after a minor head trauma, with risk factors including cerebral atrophy-related bridging vein vulnerability and the use of antithrombotic agents (Rauhala et al., 2020). Hematoma expansion elevates intracranial pressure and compresses the brain parenchyma, leading to various clinical symptoms, such as headache, cognitive decline, disturbance to consciousness, and gait abnormalities (Feghali et al., 2020; Rauhala et al., 2020). Compression of the frontal lobes and dysfunction of subcortical networks caused by hematomas may also affect postural control (Noda et al., 2017). Postural control is established by integrating multisensory information, including visual, somatosensory, and vestibular inputs, and transforming these inputs into context-appropriate motor outputs. This process is regulated by neural networks involving the cerebral cortex, basal ganglia, brainstem, and cerebellum (Horak, 2006; Takakusaki, 2017). The frontal lobe contributes to anticipatory postural control, while the cerebral cortex is involved in the integration of multisensory information (Takakusaki, 2017). Therefore, dysfunction in these regions can affect multiple components which can be assessed using the Mini-Balance Evaluation Systems Test (Mini-BESTest), including anticipatory postural control and sensory orientation. Furthermore, chronic subdural hematomas can cause brain atrophy even after hematoma evacuation (Bin Zahid et al., 2018), while neurological recovery of the brain may require time, as processes such as cell death and inflammatory responses occur during recovery (Rauchman et al., 2023). Therefore, in patients with chronic subdural hematoma, the recovery of subcortical network function may remain incomplete even after hematoma removal, resulting in persistent impairment of balance function during the early postoperative period.
Surgical treatment of CSDH reportedly results in favorable functional recovery. Specifically, 84% of patients were reported to have a modified Rankin Scale (mRS) score of <4 at 6 months after surgery, where the mRS is used to evaluate functional outcomes after cerebrovascular disease (Feghali et al., 2020). In contrast, another study reported that 55.9% of patients with CSDH experienced a decline in gait ability compared with their pre-admission status, and 48.6% were discharged to destinations other than home (Carlisi et al., 2017). These findings were observed despite the patients receiving postoperative physical therapy. Although the mRS is widely applied to assess independence in activities of daily living, it may not adequately reflect aspects of dynamic balance and postural control during gait. In particular, actual home and community environments often require advanced attentional and adaptive abilities, such as turning while walking, obstacle avoidance, and mobility under dual-task conditions. These functions are considered to involve widespread neural networks, including the frontal and parietal lobes (Surgent et al., 2019; Takakusaki, 2017). Therefore, even when postoperative patients with chronic subdural hematoma demonstrate favorable functional outcomes on the mRS, gait instability and fall risk may persist, potentially prolonging discharge planning due to concerns about safety in the home environment.
Several factors have been reported to influence the length of hospital stay (LOS) after CSDH surgery, including age, sex, impaired consciousness, pre-admission functional independence, and medication status (Zolnourian et al., 2025). However, the relationship among dynamic balance function, gait, and LOS has not yet been clarified. Patients with CSDH have been reported to exhibit greater trunk sway during standing and walking tasks compared with healthy older adults (Sundström et al., 2016), suggesting that balance impairment may persist even after surgery. Previous studies have examined the relationship between CSDH and postoperative balance function (Sundström et al., 2016), as well as recurrence risk (Leroy et al., 2015; Zanaty et al., 2020) and surgical techniques (Amaral et al., 2025; Murai et al., 2025). However, no studies have investigated the association between postoperative dynamic balance function and LOS.
Prolonged hospital stay is a clinically important issue. Among patients with neurological disorders, early rehabilitation interventions have been reported to promote functional recovery, prevent complications (Lou et al., 2024), and reduce the length of hospital stay (Ding & Zhang, 2021). In addition, impaired balance has been associated with a decreased gait independence (Carlisi et al., 2017) and an increased risk of falls (Dominguez, 2020; Igarashi et al., 2025), which can contribute to prolonged hospitalization. Therefore, early postoperative assessment of dynamic balance function in patients with chronic subdural hematoma may be clinically important for optimizing rehabilitation strategies and discharge planning.
Traditionally, the Berg Balance Scale (BBS) has been widely used to assess balance. In contrast, the Mini-BESTest has been reported to demonstrate a lower ceiling effect and higher intra-rater reliability than the BBS (Godi et al., 2013). Furthermore, the Mini-BESTest enables the comprehensive assessment of multiple balance components, allowing for a more detailed evaluation of balance function. This study aimed to elucidate the extent to which dynamic balance function assessed using the Mini-BESTest is associated with LOS in patients after surgery for CSDH. In the present study, we hypothesized that the Mini-BESTest scores would be associated with the length of hospital stay in postoperative patients with chronic subdural hematoma. Specifically, we assumed that postoperative dynamic balance function may be a potential predictor of the length of hospital stay.
Materials and Methods
Study Design
This single-center prospective observational cohort study was designed to investigate whether postoperative balance function, assessed using the Mini-BESTest, predicts LOS in patients who underwent surgical treatment for CSDH. This study was conducted in accordance with the STROBE guidelines.
Participants
The participants were 49 Japanese patients aged ≥65 years who were admitted to a single acute care hospital in Japan between February and November 2024 and underwent burr-hole drainage for CSDH. Because CSDH predominantly occurs in older adults and age has been reported as a poor prognostic factor (Feghali et al., 2020), the study population was limited to patients aged ≥65 years. The exclusion criteria were as follows: (1) comorbid orthopedic conditions such as fractures or arthritis that restricted mobilization; (2) inability to complete the Mini-BESTest within 3 days after drain removal; (3) difficulty in independent indoor ambulation before onset (mRS ≥ 4); and (4) inability to complete assessments due to exacerbation of psychiatric conditions. The drains were removed within 24–48 h after surgery. Rehabilitation was initiated on the day after surgery, and mobilization was started after drain removal. Rehabilitation was provided 7 days per week, consisting of a total of 80 min per day of standard physical and occupational therapy. This program was based on the Japanese Stroke Guidelines 2021 (Japanese Stroke Society, 2021) and comprised muscle-strengthening exercises (primarily resistance training targeting the lower extremity muscles), balance training (including static and dynamic balance tasks), indoor and outdoor gait training, and cognitive rehabilitation exercises (attention and memory tasks). These interventions were continued until discharge. All rehabilitation was delivered by therapists with at least 2 years of clinical experience in stroke rehabilitation. This study was approved by the Ethics Committee of Saitama Sekishinkai Hospital (approval number: 2023-73). All participants provided written informed consent after receiving a full explanation of the study protocol.
Measurements
The variables assessed included age, sex, initial National Institutes of Health Stroke Scale (NIHSS) score, Glasgow Coma Scale (GCS) score at admission, Mini-Mental State Examination–Japanese (MMSE-J) score, residual hematoma thickness, premorbid mRS score, Mini-BESTest score, and LOS. The Mini-BESTest consists of 14 items grouped into four subscales—anticipatory postural adjustments, reactive postural control, sensory orientation, and dynamic gait. Each item was scored from 0 to 2, yielding a total score ranging from 0 to 28, with higher scores indicating better balance ability (Franchignoni et al., 2010). The Mini-BESTest is a clinical scale that comprehensively evaluates dynamic balance function and has demonstrated good inter-rater and intra-rater reliability as well as concurrent validity (Tsang et al., 2013). Based on a previous study in which postoperative physical function was assessed after drain removal (Carlisi et al., 2017), Mini-BESTest assessments in this study were conducted by physical therapists in a rehabilitation room within 3 days after drain removal. The Mini-BESTest was administered once to each patient by three physical therapists with more than 2 years of clinical experience in stroke rehabilitation. These physical therapists were not blinded to the patients’ clinical information, including NIHSS, GCS, and radiological findings. The LOS was defined as the number of days from admission to discharge. The NIHSS is a standardized scale widely used to assess neurological severity in patients with stroke. It consists of 11 items, including consciousness, motor function, sensory function, and language, with total scores ranging from 0 to 42; higher scores indicate greater neurological severity. High inter-rater reliability has been reported (Goldstein & Samsa, 1997). In this study, a physical therapist assessed NIHSS scores during the first postoperative rehabilitation session. GCS is widely used to assess the level of consciousness and reflects neurological severity (Teasdale & Jennett, 1974). GCS scores at admission were extracted from electronic medical records. The MMSE-J is the Japanese version of the MMSE, a widely used cognitive assessment scale. Total scores range from 0 to 30, with lower scores indicating greater cognitive impairment. High inter-rater and intra-rater reliability have been reported (Folstein et al., 1975). The MMSE-J was administered by occupational therapists. The median time from surgery to the MMSE-J assessment was 2 days, which was earlier than that for the Mini-BESTest assessment (median, 3 days). All the evaluators were adequately trained to administer the assessment scales. Residual hematoma thickness was included as an observational variable, as hematoma severity may be associated with postoperative outcomes (Leroy et al., 2015). Following previous methods (Senturk et al., 2010), the maximum thickness of the crescent-shaped hematoma was measured on axial computed tomography (CT) images obtained between surgery and drain removal. The slice with the greatest hematoma thickness was selected, and the maximum perpendicular distance from the inner skull table to the center of the hematoma was measured. Measurements were performed by a physical therapist experienced in CT image evaluation using an electronic medical record viewer. The mRS is used to evaluate functional outcomes in patients with cerebrovascular diseases. A score of 0 indicates no symptoms; scores of 1–2 indicate independence in activities of daily living; a score of 3 indicates that assistance is required for outdoor activities, although independent ambulation is possible; and a score of ≥4 indicates that assistance is required for walking. Premorbid mRS scores were determined based on interviews with patients and their families.
Sample Size
As no previous studies have directly examined the association between the Mini-BESTest and length of hospital stay among patients with chronic subdural hematoma, an effect size of 0.5 was assumed, and the required sample size was calculated at 29 participants.
Statistical Analysis
Baseline characteristics were presented as mean ± standard deviation and median [interquartile range] for continuous variables, and as counts and percentages for categorical variables. To examine associations with LOS, univariate analyses were performed using Spearman's rank correlation coefficient between LOS and Mini-BESTest scores as well as other variables. In addition, correlation analysis between the MMSE-J and Mini-BESTest was conducted to assess the relationship between cognitive and balance functions. Subgroup analyses were also performed to examine the associations between each Mini-BESTest subscale (anticipatory postural control, reactive postural control, sensory orientation, and dynamic gait) and LOS, using Spearman's rank correlation coefficient. Subsequently, variables that showed statistically significant correlations with the LOS were included as covariates, and a partial correlation analysis was conducted to evaluate the independent association between the LOS and Mini-BESTest scores. Furthermore, multivariable linear regression analysis was conducted using the same adjustment variables, with LOS as the dependent variable and Mini-BESTest scores and adjustment variables as independent variables. Given the limited sample size, the number of independent variables was minimized to avoid overfitting. The normality of the residuals was assessed using the Shapiro–Wilk test to verify the assumptions of the linear regression model. Multicollinearity among the independent variables was assessed using the variance inflation factor (VIF). As no missing data were observed for any of the analyzed variables, no imputation procedures were conducted. The interpretation of correlation coefficients was as follows: <0.10, negligible; 0.10–0.39, weak; 0.40–0.69, moderate; 0.70–0.89, strong; and ≥0.90, very strong (Schober et al., 2018). Statistical analyses were performed using R software (version 4.3.2; R Foundation for Statistical Computing, Vienna, Austria), and the significance level was set at p < 0.05.
Results
Between February and November 2024, 49 patients with CSDH who met the inclusion criteria were identified. Of these, 17 patients were excluded, and 32 patients were included in the final analysis. Details of the exclusion process are presented in Figure 1. The median time from surgery to the Mini-BESTest assessment was 3 (interquartile range [IQR], 2–3.25) days, and the median time from surgery to the MMSE-J assessment was 2 (IQR, 2–3) days. Baseline characteristics and descriptive statistics are presented in Table 1. The median LOS was 8.5 days (IQR, 8–11), the median Mini-BESTest score was 18.5 (IQR, 13.8–23.3), and the median NIHSS score was 0 (IQR, 0–1).
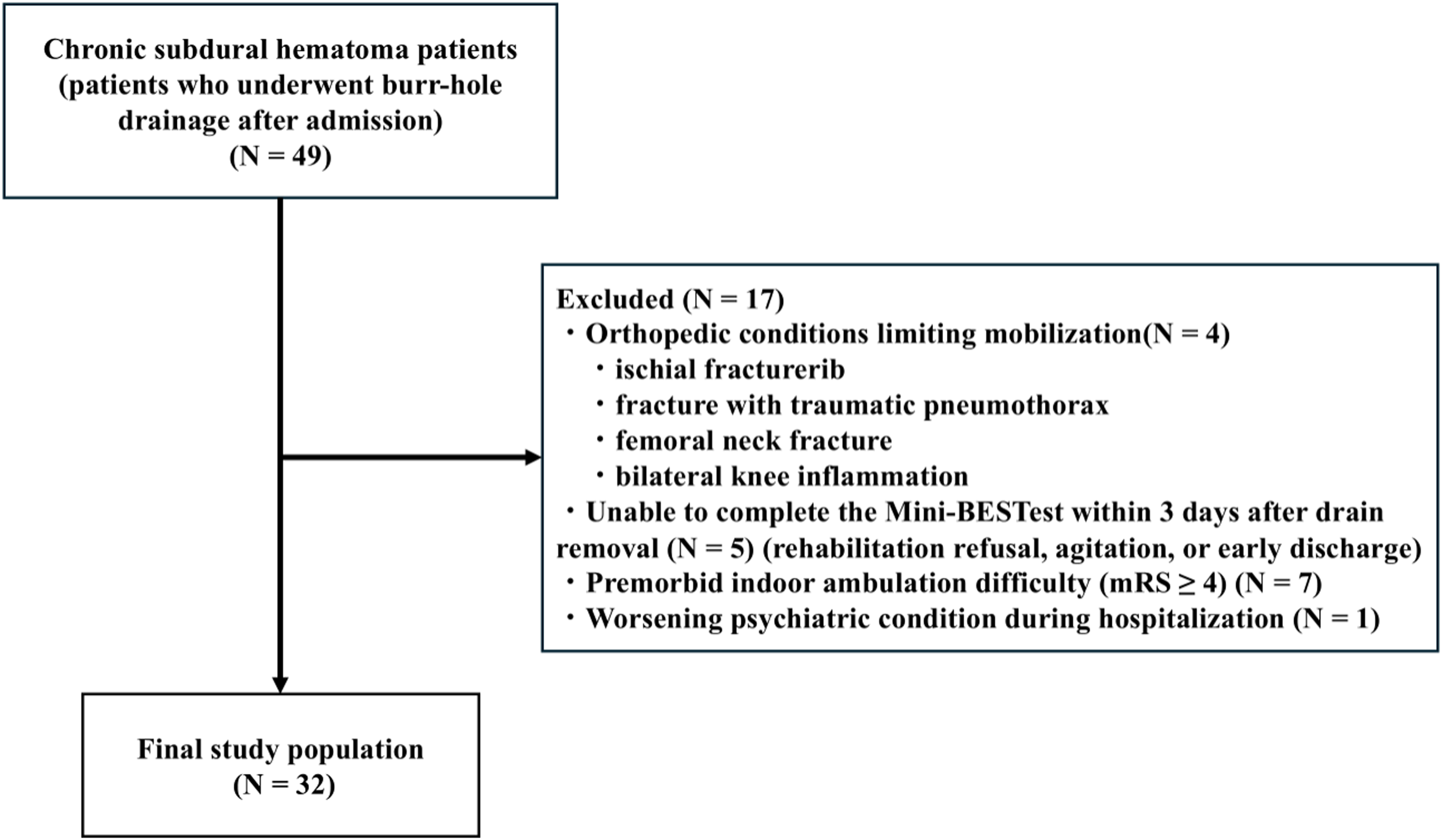
Flowchart of patient selection for analysis.
Descriptive Statistics of the Study Participants.
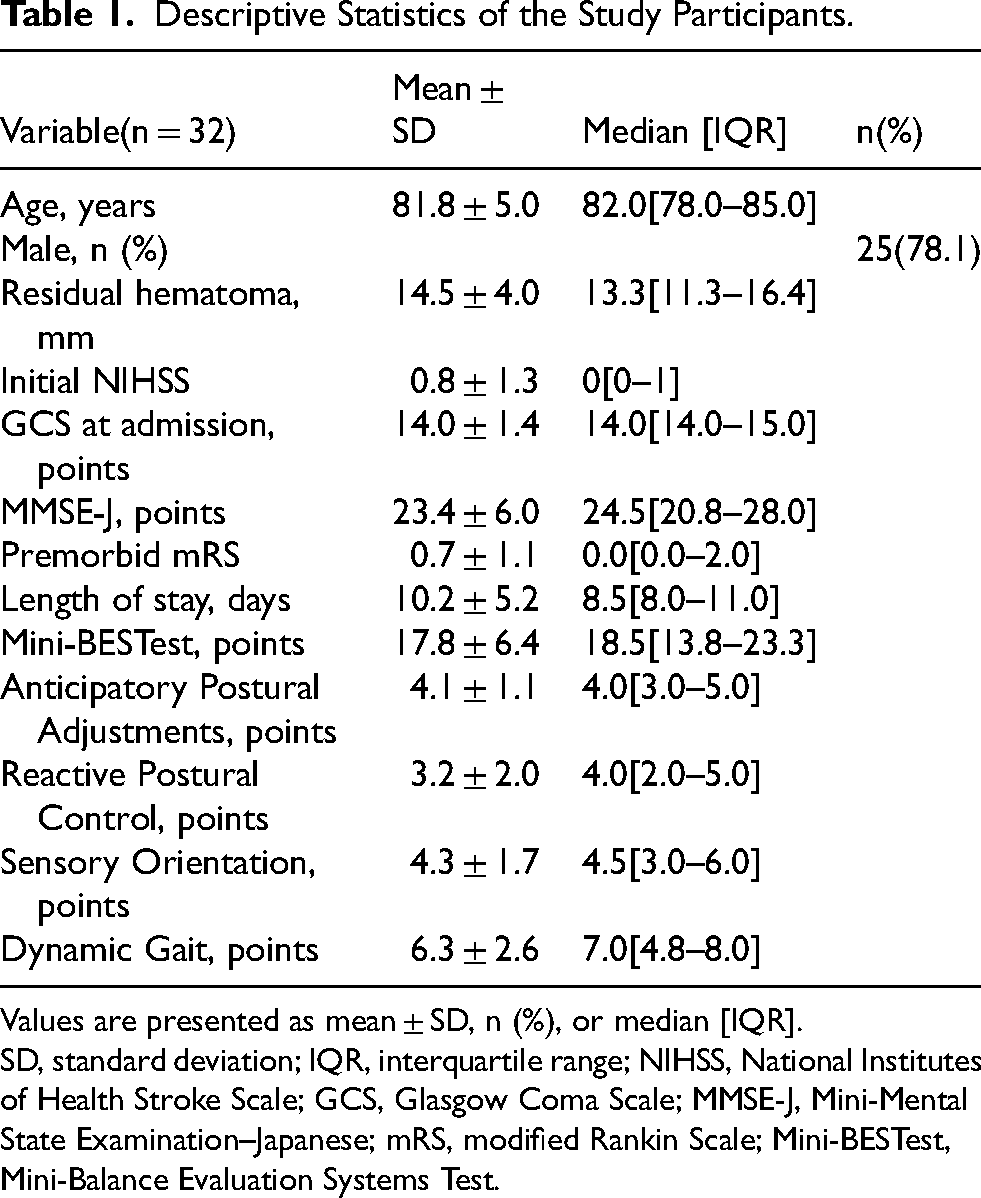
Values are presented as mean ± SD, n (%), or median [IQR].
SD, standard deviation; IQR, interquartile range; NIHSS, National Institutes of Health Stroke Scale; GCS, Glasgow Coma Scale; MMSE-J, Mini-Mental State Examination–Japanese; mRS, modified Rankin Scale; Mini-BESTest, Mini-Balance Evaluation Systems Test.
Table 2 shows the results of the correlation analyses between LOS and each variable. LOS was negatively correlated with the Mini-BESTest total score (r = −0.499, 95% confidence interval [CI]: −0.72 to −0.18, p = 0.003) and positively correlated with initial NIHSS (r = 0.376, 95% CI: 0.03 to 0.64, p = 0.034). In partial correlation analysis adjusted for initial NIHSS, a significant negative correlation between LOS and Mini-BESTest total score remained (r = −0.542, 95% CI: −0.75 to −0.24, p = 0.002). Figure 2 illustrates the scatterplot showing the correlation between LOS and NIHSS, indicating that patients with longer hospital stays tended to have higher NIHSS scores. In addition, a significant positive correlation was observed between Mini-BESTest and MMSE-J (r = 0.396, 95% CI: 0.05 to 0.65, p = 0.025).
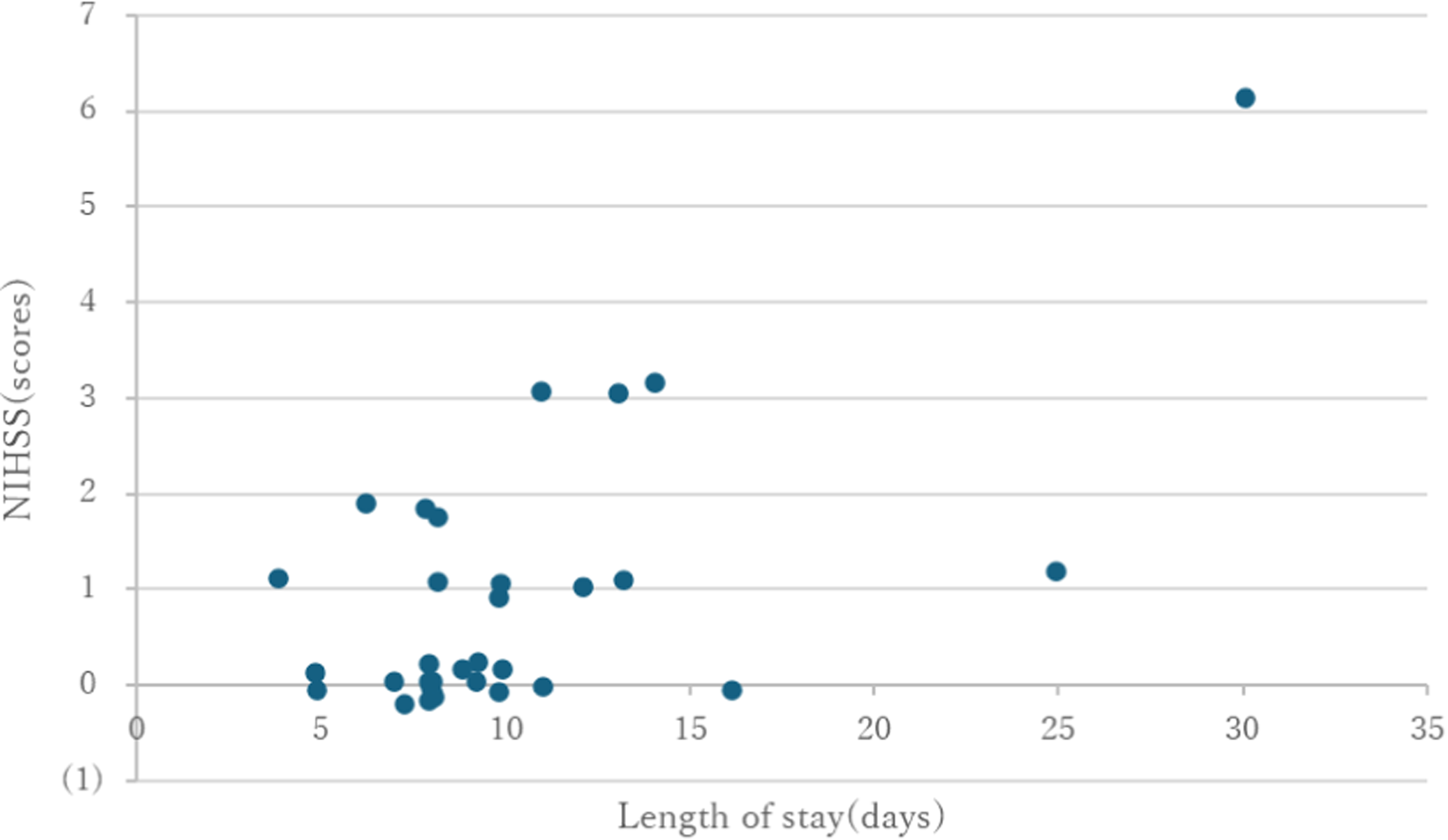
Scatterplot of length of hospital stay versus initial NIHSS score.
Spearman Correlations Between Length of Hospital Stay and Variables.
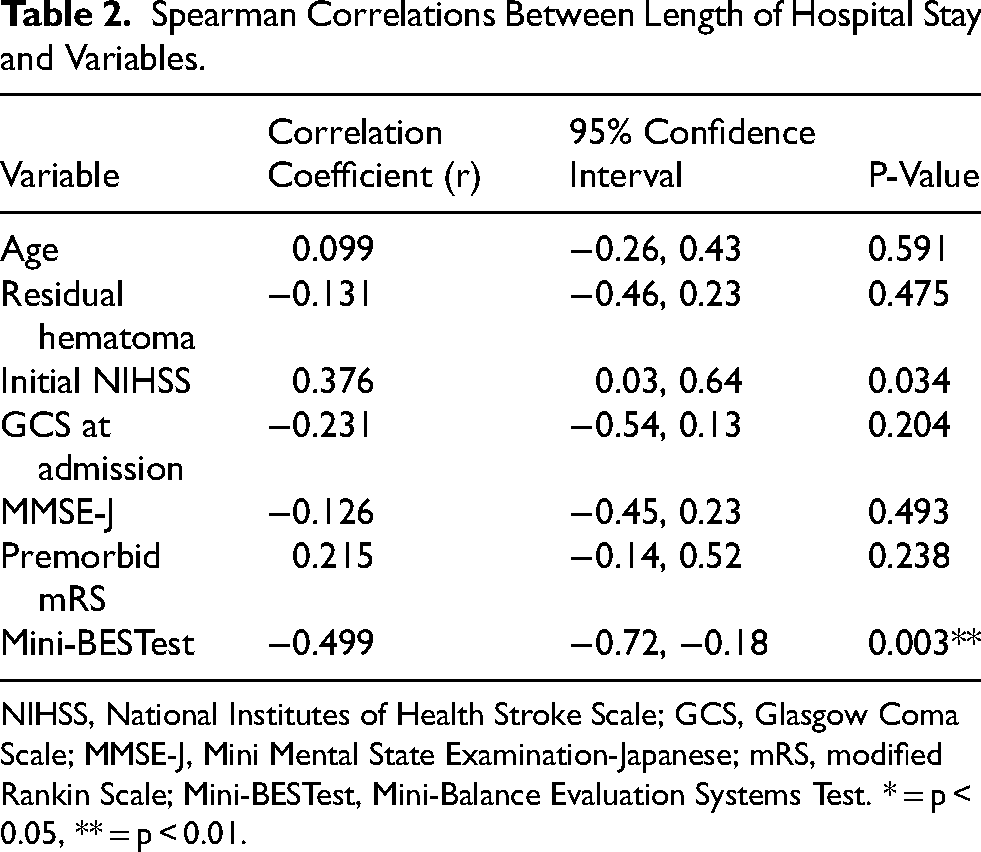
NIHSS, National Institutes of Health Stroke Scale; GCS, Glasgow Coma Scale; MMSE-J, Mini Mental State Examination-Japanese; mRS, modified Rankin Scale; Mini-BESTest, Mini-Balance Evaluation Systems Test. * = p < 0.05, ** = p < 0.01.
Table 3 presents the results of the multivariable linear regression analysis with LOS as the dependent variable and Mini-BESTest and initial NIHSS scores as independent variables. Both Mini-BESTest (β = −0.488, p = 0.002) and initial NIHSS (β = 0.377, p = 0.012) were significantly associated with LOS. The coefficient of determination for this model was R2 = 0.552, and the adjusted R2 was 0.521. The overall model was statistically significant (F = 17.89, p = 0.000009). The VIF were <2 for all variables, indicating no evidence of multicollinearity.
Multivariate Linear Regression Analysis with Length of Hospital Stay as the Dependent Variable.

R2 = 0.552, Adjusted R2 = 0.521, ANOVA F value = 17.89(degree of freedom = 2), NIHSS, National Institutes of Health Stroke Scale; Mini-BESTest, Mini-Balance Evaluation Systems Test. * = p < 0.05, ** = p < 0.01.
Subgroup analyses were conducted to examine the associations between Mini-BESTest subscales and LOS (Table 4). Significant negative correlations were observed for reactive postural control (r = −0.446, 95% CI: −0.69 to −0.12, p = 0.01), sensory orientation (r = −0.522, 95% CI: −0.74 to −0.21, p = 0.002), and dynamic gait (r = −0.488, 95% CI: −0.71 to −0.17, p = 0.004), with sensory orientation showing the strongest correlation.
Spearman Correlations Between Mini-BESTest Subcomponents and Length of Hospital Stay.
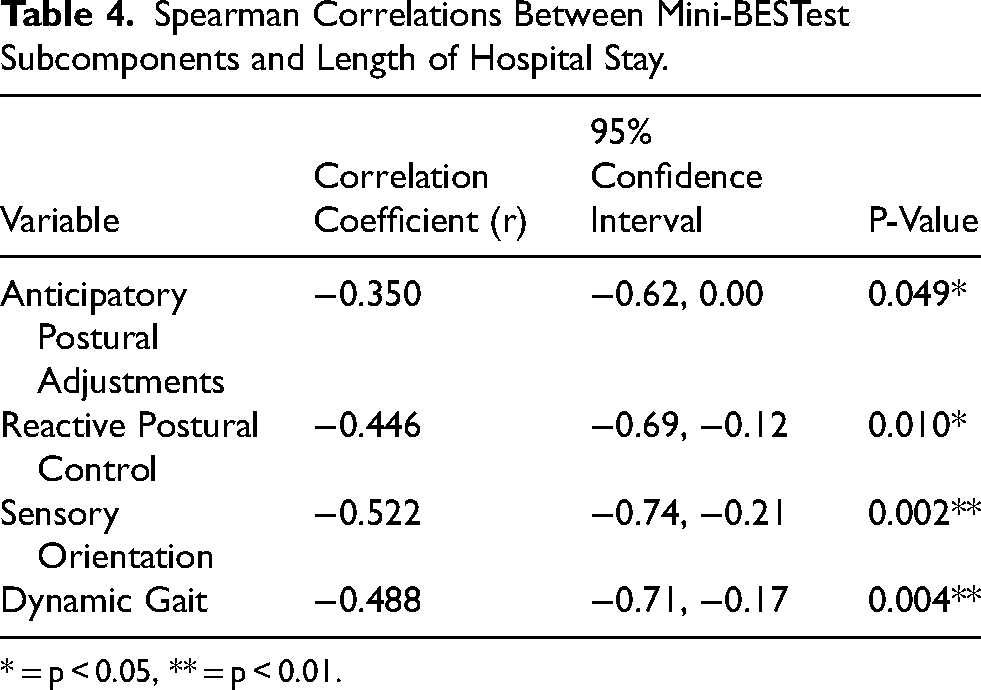
* = p < 0.05, ** = p < 0.01.
Residual diagnostics were conducted to assess the assumptions of the linear regression model. The Shapiro–Wilk test indicated that the residuals did not differ significantly from a normal distribution (p = 0.061), suggesting that the normality assumption was satisfied.
Discussion
This study demonstrated a significant negative correlation between the Mini-BESTest score and LOS in patients after CSDH surgery. Furthermore, both partial correlation analysis adjusted for initial NIHSS scores and multivariable linear regression analysis demonstrated an independent association between Mini-BESTest scores and LOS. These findings suggest that patients with poorer postoperative dynamic balance function tend to have longer hospital stays, supporting our study hypothesis.
To the best of our knowledge, no previous studies have examined the association between dynamic balance function and LOS in patients with CSDH. Therefore, this study is the first to investigate the relationship between postoperative balance function and LOS in this population. In contrast, in patients with stroke, several studies have reported an association between balance function and LOS. Previous studies (Hammad et al., 2024; Salter et al., 2010) have shown that balance function assessed using the Berg Balance Scale is associated with LOS. In general, impaired balance function is associated with an increased risk of falls and reduced gait independence. A previous study (Louie et al., 2022) reported that the ability to walk under supervision or better was an important predictor of discharge to home in patients with acute stroke. In other words, safe ambulation is required for home discharge, and adequate balance function is essential to achieve this. Similarly, in patients with CSDH, impaired balance may delay the recovery of safe walking ability. Taken together, these findings suggest that decreased dynamic balance function may delay the recovery of gait ability, resulting in prolonged discharge planning and extended hospital stays.
In this study, a positive correlation was observed between initial NIHSS and LOS in patients after surgery for CSDH. This finding is consistent with those of previous studies in patients with stroke (Chang et al., 2002; Kang et al., 2016) and suggests that neurological severity may influence LOS. However, in a study of patients with stroke (Chang et al., 2002), the median NIHSS score was 6, with 56% of patients classified as having mild neurological impairment (NIHSS score <7) and 44% as having moderate or greater impairment (NIHSS score ≥7). In contrast, in the present study, the median NIHSS score was 0, and all patients were classified as having mild neurological impairment (NIHSS score <7) (Figure 2). CSDH is a condition in which a hematoma forms between the brain surface and the dura mater, and neurological symptoms are often improved following surgical treatment (Shlobin et al., 2021). In the present cohort, many patients showed relatively mild neurological impairments, indicating that the NIHSS may have limited sensitivity at detecting subtle functional changes. In contrast, because the mini-BESTest comprehensively evaluates multiple components of dynamic balance function, it may have been able to detect functional impairments less readily identifiable by the NIHSS, thereby demonstrating a clearer association with the length of hospital stay. These findings indicate that in postoperative patients with chronic subdural hematoma, the assessment of neurological severity alone may be insufficient, and that evaluation of dynamic balance function may be more useful for predicting the length of hospital stay. In addition, a weak to moderate positive correlation was observed between MMSE-J and Mini-BESTest scores, suggesting that cognitive function may influence balance assessment. Because the Mini-BESTest requires task understanding and attention, cognitive function may affect balance evaluation performance.
In the Mini-BESTest subgroup analysis, the sensory orientation subscale showed the strongest association with LOS among the four subcomponents. Furthermore, the sensory orientation component of the Mini-BESTest includes tasks such as standing on foam or an inclined surface with eyes-closed and assesses postural control through the integration of visual, somatosensory, and vestibular inputs. Postural control is established by integrating multiple sensory inputs and their transformation into appropriate motor outputs (Horak, 2006). Prior studies have reported that this process is supported by widespread neural networks involving the frontal cognitive association areas, the parietal association cortex, and subcortical structures such as the basal ganglia (Sheridan & Hausdorff, 2007). In chronic subdural hematoma, compression of the frontal lobe and dysfunction of subcortical neural networks caused by the hematoma have been reported (Noda et al., 2017), which may impair the sensory integration involved in postural control. Furthermore, recovery of frontal–subcortical circuits and sensory integration function can require time, even after surgical evacuation of the hematoma. Consequently, under conditions in which visual input is restricted, such as standing on a foam pad or an inclined surface, impairments in postural control may become more apparent compared to tasks performed with the eyes open. Additionally, vestibular input plays a critical role in postural control, while vestibular dysfunction has been associated with increased fall rates, greater fear of falling, and reduced balance confidence (Wuehr et al., 2022). Taken together, these findings indicate that impairment of postural control related to sensory integration may contribute to prolonged hospitalization after surgery for chronic subdural hematoma.
The results of this study demonstrated an association between postoperative dynamic balance function and LOS in patients with CSDH. In this study, the Mini-BESTest was performed within 3 days after drain removal. The Mini-BESTest is a widely used clinical tool for assessing dynamic balance and is familiar to physical therapists. Assessments were conducted in a rehabilitation room after the patients’ general condition had stabilized. The equipment required for the Mini-BESTest, such as foam pads and inclined surfaces, are routinely available in our rehabilitation department. The assessment was performed by physical therapists with experience in neurological rehabilitation and required approximately 10–15 min. These findings suggest that the Mini-BESTest is a feasible assessment tool even in acute care settings, and can be applied for early postoperative functional evaluation. The findings of this study indicate that the early assessment of dynamic balance function may be useful for rehabilitation planning and discharge management in postoperative patients with chronic subdural hematoma. For example, balance training aimed at improving sensory integration may be important in patients with particularly low sensory orientation scores on the Mini-BESTest during the early postoperative period. Specifically, interventions designed to increase reliance on somatosensory and vestibular inputs, such as standing balance exercises under conditions of restricted visual input, balance tasks performed on unstable surfaces, and exercises incorporating head movements, may be effective. Physical therapy is commonly introduced in postoperative patients with chronic subdural hematoma to improve their gait ability and balance. Carlisi et al. reported that physical therapy, including muscle strengthening, balance training, and gait exercises, improved balance function at discharge (Carlisi et al., 2017). Based on both our findings and existing reports, rehabilitation programs may be individualized according to the Mini-BESTest scores. For example, patients with higher scores may progress to early gait and outdoor walking training, while those with lower scores may benefit from more fundamental interventions, such as muscle strengthening and balance training. Therefore, the Mini-BESTest may be useful for individualizing rehabilitation programs and developing treatment strategies. Furthermore, for patients with lower Mini-BESTest scores, initiating discharge planning at an early stage and considering the use of social support resources, such as enrollment in long-term care support programs and provision of assistive devices, may facilitate smoother discharge support. In Japan, acute rehabilitation often focuses on gait ability and activities of daily living. However, systematic evaluation of dynamic balance function in the early postoperative period has not been widely reported. The present findings suggest that early assessment of dynamic balance function may be useful for optimizing rehabilitation strategies and discharge planning in patients with CSDH.
This study has several limitations. First, this was a single-center prospective cohort study with a relatively small sample size. Therefore, we cannot completely exclude the possibility that the variables not identified as statistically significant in this study may be associated with LOS. Accordingly, the results of variables without significant associations should be interpreted with caution. Second, patients who were unable to complete the Mini-BESTest within 3 days after drain removal were excluded, which may have introduced selection bias. In particular, patients who did not complete the assessment may have had poorer physical function and longer hospital stays. Therefore, the findings of this study may be applicable primarily to patients with a relatively preserved functional status, and the association between balance function and LOS may have been underestimated. In addition, as the evaluators were not blinded to the clinical information, the possibility of assessment bias could not be excluded. Third, social factors such as living status and home environment were not evaluated, although these factors may influence LOS. Finally, the present study did not include an analysis adjusted for cognitive function as a covariate. Therefore, the potential influence of cognitive function on balance assessment could not be completely excluded. These limitations should be considered when interpreting the findings of this study, and causal inferences should accordingly be drawn with caution.
In conclusion, the present study found that postoperative dynamic balance assessed using the Mini-BESTest was significantly associated with the length of hospital stay in patients with chronic subdural hematoma. This association remained significant, even after adjusting for neurological severity (according to the NIHSS), indicating that dynamic balance is an independent factor associated with hospitalization duration. Notably, among the Mini-BESTest subscales, sensory orientation showed the strongest association with the length of hospital stay, indicating that postural control based on sensory integration may play an important role in postoperative recovery. These findings suggest that performing the Mini-BESTest within 3 days after drain removal may help to identify patients at risk of prolonged hospitalization and support individualized rehabilitation and discharge planning. Particularly, patients with lower sensory orientation scores may benefit from rehabilitation programs that focus on sensory integration, such as balance training, under reduced visual conditions and unstable surface tasks. Future studies incorporating larger sample sizes and social factors are required to further validate the external generalizability of these findings and to clarify the long-term clinical significance of balance dysfunction in patients with chronic subdural hematoma.
Footnotes
Acknowledgments
Ethical Considerations
This study was approved by the Ethics Committee of Saitama Sekishinkai Hospital (approval no. 2023-73).
Consent to Participate
Written informed consent was obtained from all participants after they were provided oral and written explanations of the study.
Consent for Publication
Not applicable.
Author Contributions
Mutsumi Shiraishi conceived and designed the study, collected the data, performed the statistical analyses, and drafted the manuscript. Shunsuke Ohji and Ryo Onuma contributed to the study design, interpretation of the data, and critically revised the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to ethical restrictions and the protection of patient privacy, but are available from the corresponding author on reasonable request.