
Abstract
Objective
To perform the cross-cultural adaptation of the Patient-Reported Impact of Spasticity Measure (PRISM) into Mexican Spanish and to examine the internal consistency and preliminary convergent validity of the PRISM-MX in adults with post-stroke spasticity.
Methods
This cross-sectional pilot study included 30 adults with ischemic or hemorrhagic stroke and clinically confirmed spasticity attending an outpatient rehabilitation clinic in Merida, Mexico. Cross-cultural adaptation followed standard procedures, including forward translation, synthesis, back-translation, expert committee review, and cognitive debriefing. Preliminary psychometric evaluation included descriptive item-level analysis, internal consistency of the original 41-item PRISM-MX version, and exploratory correlations with disability, motor performance, and quality-of-life measures.
Results
The Mexican Spanish version was considered understandable, culturally relevant, and acceptable by participants during cognitive debriefing. The original 41-item PRISM-MX version was retained, and no item deletion was performed based on the present pilot sample. No missing PRISM-MX item responses were observed. Internal consistency was high for the total score (Cronbach's alpha = .956). Higher PRISM-MX scores were significantly associated with greater disability and poorer quality of life, with correlation coefficients ranging from ρ = −.46 to ρ = .61, supporting preliminary convergent validity.
Conclusions
PRISM-MX was successfully cross-culturally adapted and showed preliminary evidence of acceptability, high internal consistency, and clinically plausible associations with disability and quality-of-life indicators. Definitive psychometric validation, including structural validity, test-retest reliability, responsiveness, measurement error, and measurement invariance, remains pending.
Keywords
Introduction
Spasticity is one of the most frequent and disabling sequelae after stroke and represents a major challenge in neurorehabilitation. Its reported prevalence varies widely, ranging from approximately 30% to 80%, depending on lesion characteristics, time since stroke, study sample, and assessment methods (Glaess-Leistner et al., 2021; Lundström et al., 2008; Opheim et al., 2015; Parry-Jones et al., 2025; Watkins et al., 2002; Zeng et al., 2021). Clinically, spasticity may manifest as increased muscle tone, involuntary muscle activity, and resistance to passive stretch, which can contribute to pain, impaired motor control, reduced mobility, and loss of independence in activities of daily living (Doussoulin et al., 2019; Li et al., 2024; Morone et al., 2023; Suputtitada et al., 2024; Wissel et al., 2013; Zhu et al., 2024). Beyond its physical manifestations, spasticity may also affect emotional well-being, social participation, and overall quality of life, thereby influencing the broader rehabilitation process and the lived experience of stroke survivors (Esquenazi et al., 2023; Lumbantobing et al., 2025; Schinwelski et al., 2019).
Because the consequences of spasticity extend beyond muscle tone abnormalities, its assessment should not rely exclusively on clinician-rated measures. Although tools such as the Modified Ashworth Scale remain widely used in practice (Bohannon & Smith, 1987), they do not fully capture how spasticity is experienced by patients in daily life. Patient-reported outcome measures (PROMs) provide complementary information on symptom burden, activity limitations, emotional distress, and social consequences, and are increasingly recognized as essential in rehabilitation research and clinical decision-making (Cano & Hobart, 2011; De-la-Rosa-Molina et al., 2017). Incorporating the patient perspective may improve goal setting, monitoring of treatment response, and shared decision-making in neurorehabilitation settings.
Among the available PROMs for spasticity, the Patient-Reported Impact of Spasticity Measure (PRISM) is one of the most recognized multidimensional instruments. PRISM was selected for this study because it is a spasticity-specific patient-reported outcome measure that captures the perceived impact of spasticity across daily activities, psychosocial burden, need for assistance, and social participation. Unlike clinician-rated tone measures such as the Modified Ashworth Scale, PRISM reflects the patient's lived experience of spasticity in daily life. Compared with generic quality-of-life instruments, PRISM is more directly focused on spasticity-related consequences and may therefore provide clinically actionable information for rehabilitation goal setting, shared decision-making, and patient-centered outcome assessment. Developed originally in English for the spinal cord injury population, PRISM has shown acceptable validity and reliability in prior studies (Balioussis et al., 2014; Cook et al., 2007; Ertzgaard et al., 2020).
However, instruments developed in one language and cultural context cannot be assumed to be directly transferable to another. Cross-cultural adaptation is necessary to ensure semantic, idiomatic, experiential, and conceptual equivalence and to reduce the risk of measurement bias (Beaton et al., 2000; Wild et al., 2005). Inadequate translation or insufficient cultural adaptation may alter item meaning, modify the internal structure of the scale, and compromise psychometric performance. Previous PRISM adaptations have been conducted in other languages and clinical populations, including Arabic-speaking individuals with spinal cord injury and Serbian-speaking individuals with multiple sclerosis (Aldaihan et al., 2024; Knezevic et al., 2015). However, these adaptations were developed in linguistic and clinical contexts that differ from Mexican Spanish-speaking adults with post-stroke spasticity. Therefore, a specific cross-cultural adaptation was required to ensure that the PRISM-MX was semantically, idiomatically, experientially, and conceptually appropriate for the Mexican neurorehabilitation context.
In the Mexican context, cultural and linguistic adaptation is particularly relevant because patients may describe spasticity using everyday terms such as stiffness, tightness, pulling, heaviness, or difficulty moving rather than biomedical terminology. In addition, the perceived impact of spasticity may be shaped by family caregiving practices, expectations regarding independence, access to rehabilitation services, and social participation roles. Therefore, experiential and conceptual equivalence are essential to ensure that PRISM-MX captures not only literal item meaning but also the way Mexican patients understand and report the burden of spasticity.
In Mexico, despite the clinical relevance of post-stroke spasticity and the growing interest in PROMs within rehabilitation practice, no culturally adapted Mexican Spanish version of PRISM was available. This represents an important gap, since the absence of culturally appropriate instruments limits the ability to assess patient-perceived impact, compare outcomes across studies, and incorporate the patient voice into rehabilitation planning. A Mexican Spanish version of PRISM may therefore support both clinical assessment and research in stroke-related spasticity.
Accordingly, the aim of this study was to perform the cross-cultural adaptation of the Patient-Reported Impact of Spasticity Measure (PRISM) into Mexican Spanish and to examine the internal consistency and preliminary convergent validity of the PRISM-MX in adults with post-stroke spasticity. Specifically, we examined item-level performance and internal consistency and explored associations with disability, motor performance, and quality of life.
Methods
Study Design and Setting
This was a cross-sectional, single-center pilot study conducted to translate, culturally adapt, and preliminarily evaluate the Mexican Spanish version of the Patient-Reported Impact of Spasticity Measure (PRISM-MX) in adults with post-stroke spasticity.
Participants
A consecutive convenience sample of 30 adults aged 18 years or older with a documented diagnosis of ischemic or hemorrhagic stroke and clinically confirmed spasticity was recruited between December 2024 and March 2025. Eligible participants were required to be able to read, speak, and understand Spanish. Patients were excluded if they were pregnant or had diagnosed dementia, intellectual disability, major psychiatric disorders, communication impairments interfering with questionnaire completion, or other pre-existing neuromusculoskeletal conditions. Patients who declined participation were not enrolled. Consented participants who completed the questionnaire and study procedures were included in the final analysis. No consented participant had incomplete PRISM-MX responses. A formal sample size calculation was not performed because this was designed as a preliminary single-center pilot study. Therefore, a consecutive convenience sample was used, and all eligible patients attending the outpatient rehabilitation service during the recruitment period were invited to participate. The final sample size reflected the number of available patients who met the inclusion criteria within the study period.
Recruitment was limited by the single-center nature of the study, the defined recruitment period from December 2024 to March 2025, and the availability of eligible patients with documented stroke and clinically confirmed spasticity attending the outpatient rehabilitation service. Although stroke represents an important cause of mortality and disability in Mexico, national epidemiological data specifically focused on post-stroke spasticity remain scarce (Secretaría de Salud, 2022; Torres-Viloria et al., 2022). International evidence suggests that post-stroke spasticity affects only a subset of stroke survivors, with pooled prevalence estimates around 25%, although reported frequencies vary according to time since stroke, lesion characteristics, and assessment methods (Zeng et al., 2021). Locally, institutional data from the rehabilitation service of Hospital General Regional No. 1 in Mérida, Yucatán, indicate that stroke is the leading cause of spasticity among patients treated with botulinum toxin, representing 48% of cases in that clinical service (Brito Uribe, 2024). Therefore, all eligible patients during the recruitment period were invited, and the final sample reflected the number of participants who met the criteria and completed the study procedures.
Instrument
The Patient-Reported Impact of Spasticity Measure (PRISM) was originally developed in English for the spinal cord injury population and has shown acceptable validity and reliability in prior studies (Balioussis et al., 2014; Cook et al., 2007; Ertzgaard et al., 2020). The original PRISM is a 41-item self-report questionnaire designed to assess the impact of spasticity on daily life across multiple domains, including social avoidance/anxiety, psychological agitation, daily activities, need for assistance/repositioning, positive impact, need for intervention, and social embarrassment. Items are rated on a 5-point Likert scale ranging from 0 to 4, with higher scores indicating greater perceived negative impact of spasticity.
Cross-Cultural Adaptation
The translation and cross-cultural adaptation of PRISM into Mexican Spanish followed established recommendations for self-report measures and patient-reported outcomes (Beaton et al., 2000; Wild et al., 2005). Two independent forward translations were produced by bilingual native Spanish translators, one with clinical expertise and one without clinical involvement in the construct. These versions were synthesized into a single reconciled translation. Subsequently, two independent back-translations were completed by native English speakers who were blinded to the original instrument.
The expert committee included 2 rehabilitation physicians, 2 methodologists, 2 linguists, and 2 translators, who reviewed all versions to ensure semantic, idiomatic, experiential, and conceptual equivalence (Beaton et al., 2000; Wild et al., 2005). A pre-final Mexican Spanish version was then administered to 30 adults with post-stroke spasticity, who completed the questionnaire and participated in cognitive debriefing interviews to assess clarity, cultural relevance, and acceptability. No wording changes were required after pilot testing, and the pre-final version was retained as the PRISM-MX for preliminary psychometric evaluation.
Additional Clinical Measures
In addition to PRISM-MX, participants were evaluated with the Modified Ashworth Scale to assess muscle tone (Bohannon & Smith, 1987), the Demeurisse Motor Index to assess motor performance (Demeurisse et al., 1980), the modified Rankin Scale to determine global disability, and the World Health Organization Quality of Life Questionnaire (WHOQOL-BREF) to assess quality of life.
Statistical Analysis
Statistical analyses were performed using Jamovi (version 2.7.6). Initial data screening included verification of response ranges for PRISM items, inspection of missing values, and descriptive statistics for item-level performance. No missing PRISM-MX item responses were observed; therefore, no imputation was required.
Psychometric evaluation included descriptive item-level analysis, corrected item-total correlations, and Cronbach's alpha after item deletion to explore item performance, with low item-total correlations considered indicative of weak contribution to the scale (Streiner, 2003). Internal consistency was assessed using Cronbach's alpha for the total PRISM-MX score.
Given the preliminary nature of the study and the limited sample size, structural validity was not formally tested through exploratory or confirmatory factor analysis. Psychometric analyses were restricted to descriptive item-level performance, internal consistency, and exploratory correlations with clinical, functional, and quality-of-life measures. The original 41-item PRISM structure was retained, and no item deletion was performed based on the present pilot sample. Findings were interpreted as preliminary psychometric evidence rather than definitive psychometric validation.
Preliminary convergent validity was explored through Pearson or Spearman correlation analyses, as appropriate, between PRISM-MX scores and motor performance, disability, and quality-of-life measures. The WHOQOL-BREF global score was transformed to a 0–100 scale, with higher scores indicating better quality of life (Fayers & Machin, 2007). For exploratory correlation analyses, the social and psychological domain scores were analyzed as raw domain scores. Correlations were interpreted as preliminary evidence of convergent validity. Statistical significance was set at p < .05, and findings were interpreted cautiously given the sample size.
Ethical Considerations
The study was conducted in accordance with institutional and national regulations for research involving human participants and with the principles of the Declaration of Helsinki. The protocol was reviewed and approved by the Local Research and Ethics Committee No. 3201 (approval numbers R-2024-3201-080 and R-2025-3201-035). All participants provided written informed consent before enrollment, and all data were coded and anonymized to protect confidentiality.
Results
Participant Characteristics
Thirty adults with post-stroke spasticity were included in the study. The sample was predominantly male (27/30, 90.0%), with a mean age of 61.0 years (SD = 7.6; range, 46-77). Most participants were married (73.3%), had ischemic stroke (90.0%), and presented with left hemiparesis (63.3%). Mean disability was 2.63 (SD = 1.16) on the modified Rankin Scale (possible range, 0–6), mean motor performance was 87.3 (SD = 11.1) on the Demeurisse Motor Index (possible range, 0–100), and the mean WHOQOL-BREF global score was 72.1 (SD = 10.2) after transformation to a 0–100 scale (possible range, 0–100). Detailed participant characteristics are presented in Table 1.
Participant Characteristics (n = 30).
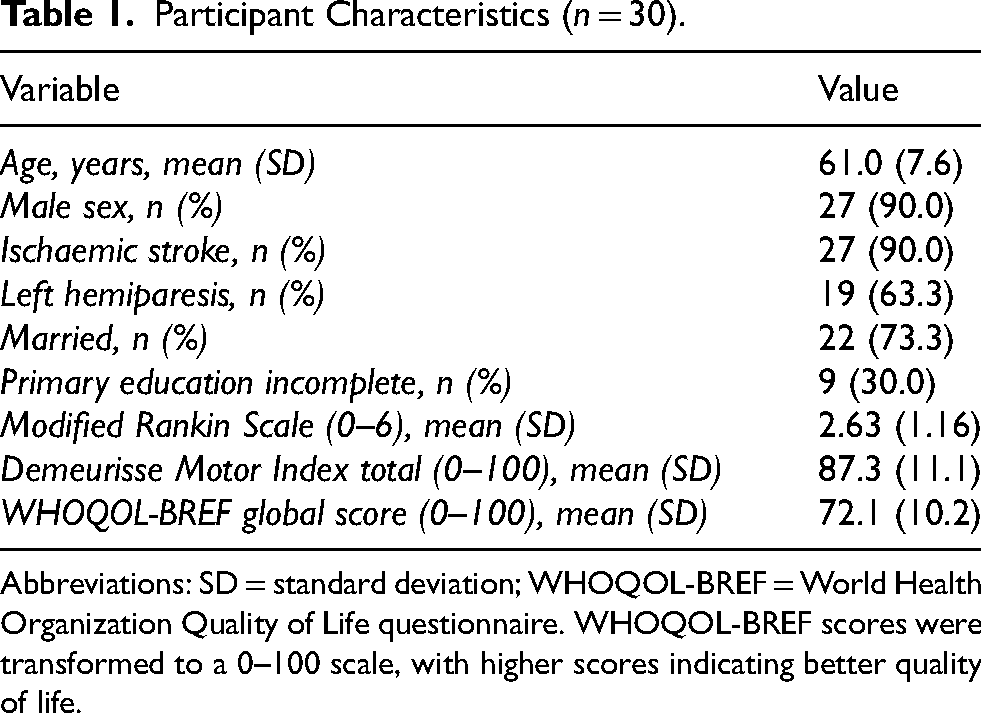
Abbreviations: SD = standard deviation; WHOQOL-BREF = World Health Organization Quality of Life questionnaire. WHOQOL-BREF scores were transformed to a 0–100 scale, with higher scores indicating better quality of life.
Clinical and Functional Profile
Spasticity assessed with the Modified Ashworth Scale was generally mild to moderate across muscle groups. Increased tone was most frequently observed in elbow flexors, particularly the biceps brachii, followed by forearm pronators, finger flexors, hip adductors, knee flexors, and tibialis posterior. MAS scores of 3 or higher were uncommon, and no MAS 4 scores were observed. The distribution of spasticity severity across muscle groups is presented in Supplementary Table S1.
Cross-Cultural Adaptation
Participants considered the Mexican Spanish version of the Patient-Reported Impact of Spasticity Measure to be understandable, culturally relevant, and acceptable. No relevant difficulties in comprehension or interpretation were identified during cognitive debriefing, and no wording modifications were required after pilot testing. Therefore, the pre-final translated version was retained as the final PRISM-MX for preliminary psychometric evaluation. The cross-cultural adaptation process is summarized in Figure 1.
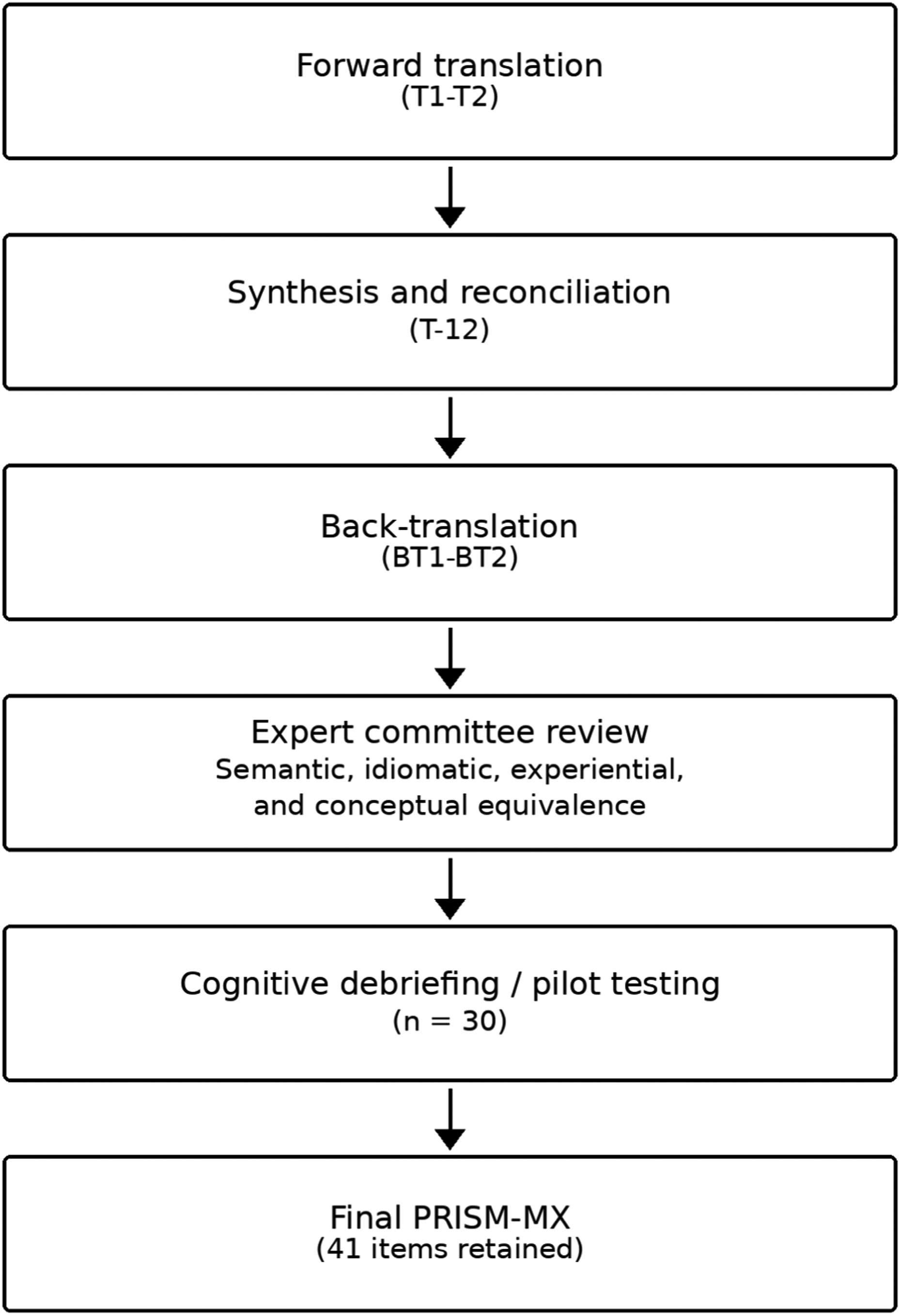
Cross-cultural adaptation process of the patient-reported impact of spasticity measure into Mexican spanish. Forward translation by 2 bilingual translators (T1-T2), synthesis (T-12), back translation (BT1-BT2), expert committee review, pre-final version, pilot testing with cognitive debriefing (n = 30), and final PRISM-MX (41 items retained).
Item Analysis and Internal Consistency
No missing PRISM-MX item responses were identified. The original 41-item PRISM-MX version was retained, and no item deletion was performed based on the present pilot sample. Item responses covered the full range of response options, and no evident floor or ceiling effects were observed. Internal consistency was high for the total PRISM-MX score (Cronbach's alpha = .956).
Preliminary Convergent Validity
Higher PRISM-MX scores were associated with greater disability and poorer quality of life. The strongest correlation was observed with the modified Rankin Scale (Spearman's rho = .61, p < .001). Moderate negative correlations were found with the WHOQOL-BREF global score (rho = −.39, p = .039) and the WHOQOL-BREF social domain (rho = −.46, p = .014). The association with the WHOQOL-BREF psychological domain was also negative (rho = −.33, p = .085), although it did not reach statistical significance. Correlations between PRISM-MX and motor performance were negative but weak and non-significant (Demeurisse Motor Index: rho = −.29, p = .139). Correlation coefficients are presented in Table 2, and scatterplots for the strongest and moderate associations are shown in Figure 2.
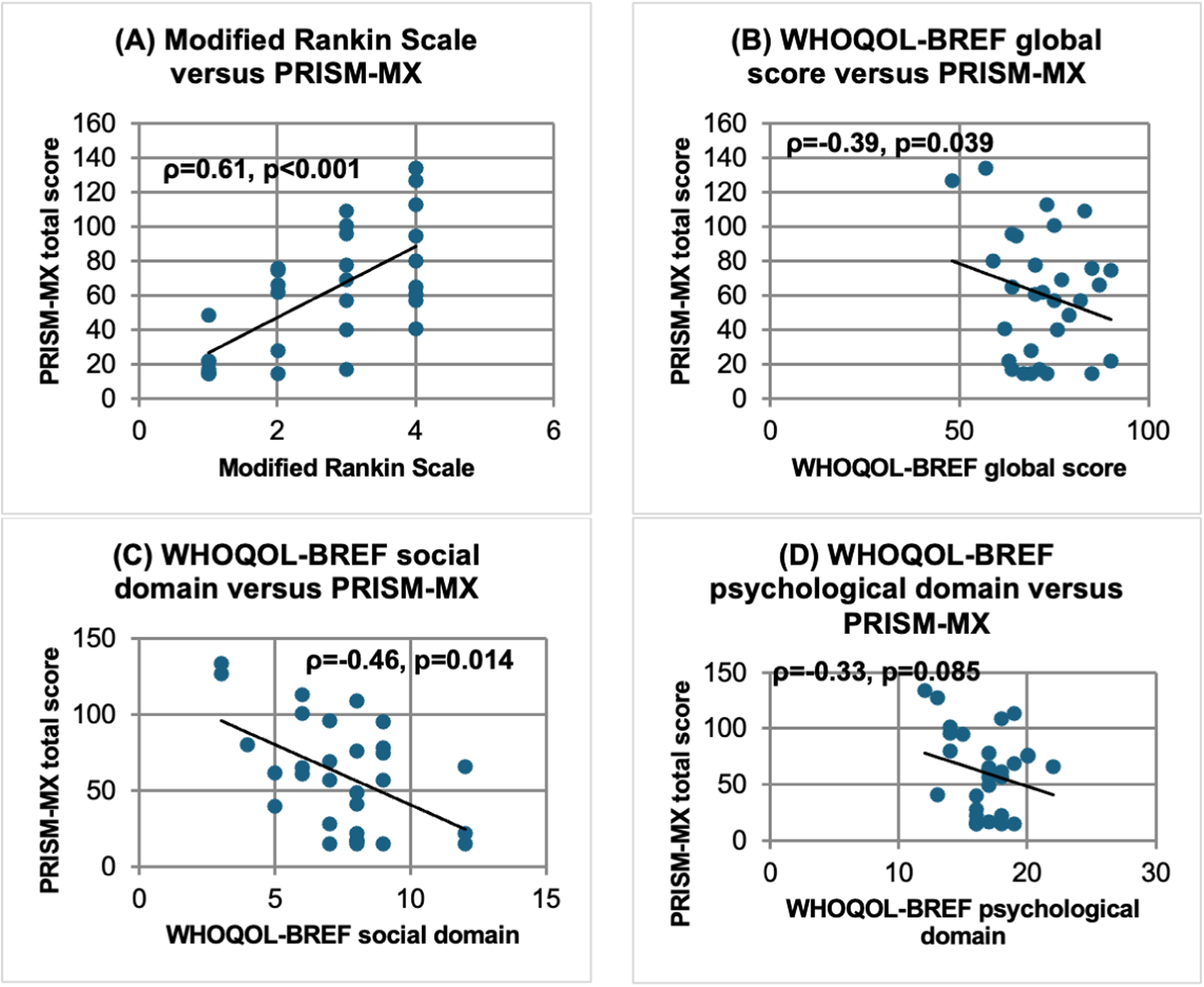
Scatterplots showing the associations between PRISM-mx total score and (A) modified rankin scale, (B) WHOQOL-BREF global score, (C) WHOQOL-BREF social domain, and (D) WHOQOL-BREF psychological domain. Higher PRISM-MX scores indicate greater perceived impact of spasticity. Higher WHOQOL-BREF scores indicate better quality of life. The WHOQOL-BREF global score was transformed to a 0–100 scale, whereas the social and psychological domain scores are presented as raw domain scores.
Correlations Between PRISM-MX and Clinical Scales.
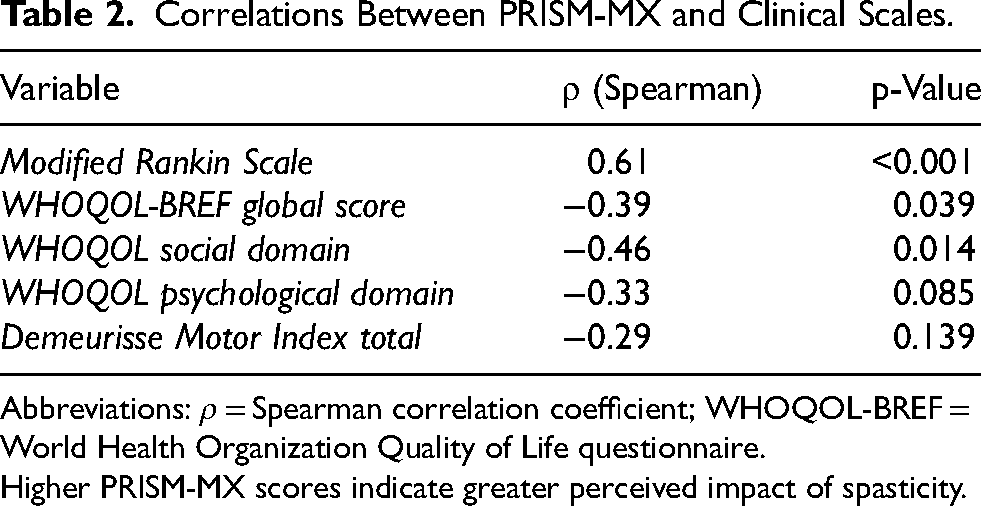
Abbreviations: ρ = Spearman correlation coefficient; WHOQOL-BREF = World Health Organization Quality of Life questionnaire.
Higher PRISM-MX scores indicate greater perceived impact of spasticity.
Discussion
This study provides the first Mexican Spanish cross-cultural adaptation and preliminary psychometric evaluation of PRISM-MX in adults with post-stroke spasticity. In this context, the availability of a culturally adapted patient-reported outcome measure is especially valuable, since patient experience cannot be fully captured by clinician-rated assessments of muscle tone alone (Bohannon & Smith, 1987; Cano & Hobart, 2011; De-la-Rosa-Molina et al., 2017).
The cross-cultural adaptation process followed established recommendations for self-report measures and patient-reported outcomes, including forward translation, synthesis, back-translation, expert committee review, and cognitive debriefing (Beaton et al., 2000; Wild et al., 2005). No wording modifications were required after pilot testing, suggesting that the Mexican Spanish version was understandable, culturally appropriate, and acceptable for the target clinical group. This is an important finding because previous work has shown that PROM adaptation involves more than literal translation and requires preservation of semantic, idiomatic, experiential, and conceptual equivalence across cultural contexts (Aldaihan et al., 2024; Beaton et al., 2000; Knezevic et al., 2015; Wild et al., 2005). The successful adaptation of PRISM-MX therefore supports the feasibility of using this instrument in Mexican neurorehabilitation settings and is consistent with prior international adaptation efforts.
For conceptual continuity with the source instrument, the original PRISM domain structure was retained. Given the limited sample size, the present study was not designed to formally test structural validity or to support item reduction. Therefore, no factor structure is proposed for PRISM-MX based on this pilot sample. In this study, the PRISM-MX total score was used as an overall indicator of patient-perceived spasticity impact, while future adequately powered studies should evaluate the dimensional structure of the instrument in Mexican patients with post-stroke spasticity.
Preliminary convergent validity findings also support the clinical relevance of PRISM-MX. Higher perceived impact of spasticity was associated with greater global disability and poorer quality of life, particularly in social and global quality-of-life indicators. These associations are clinically plausible and align with prior evidence showing that post-stroke spasticity may affect daily living, participation, emotional well-being, and broader life experience beyond motor impairment alone (De-la-Rosa-Molina et al., 2017; Doussoulin et al., 2019; Esquenazi et al., 2023; Lumbantobing et al., 2025; Morone et al., 2023; Schinwelski et al., 2019). The association with disability, as measured by the modified Rankin Scale, further supports the preliminary convergent validity of PRISM-MX and suggests that patient-reported spasticity burden is meaningfully related to overall functional status in adults with stroke-related spasticity.
By contrast, correlations between PRISM-MX and motor performance were weak and not statistically significant. This finding is also clinically meaningful. It suggests that patient-perceived spasticity impact is not simply a proxy for muscle strength or motor performance, but rather a broader construct that includes discomfort, daily restrictions, emotional burden, and social consequences. This interpretation is in line with conceptual critiques of health measurement that highlight the need to distinguish between impairment, activity limitation, participation, and subjective experience (Cano & Hobart, 2011; Fayers & Machin, 2007). It also reinforces the value of using PROMs alongside clinician-rated measures such as the Modified Ashworth Scale and motor performance indices, since these instruments capture different but complementary aspects of the rehabilitation process (Bohannon & Smith, 1987; Cook et al., 2007; Demeurisse et al., 1980).
From a neurorehabilitation perspective, PRISM-MX may provide a practical and structured way to incorporate the patient voice into the assessment of post-stroke spasticity. Current approaches to spasticity management increasingly emphasize individualized rehabilitation goals, multidisciplinary care, and attention to participation and quality-of-life outcomes, rather than focusing solely on tone reduction (Li et al., 2024; Morone et al., 2023; Suputtitada et al., 2024). In this context, a culturally adapted PROM may support clinical decision-making, help identify patient-perceived burden, and contribute to outcome assessment in both routine care and research. It may also facilitate comparison with other spasticity-related patient-reported tools described in the literature and strengthen future collaborative research in neurorehabilitation (Balioussis et al., 2014; Ertzgaard et al., 2020).
This study has several limitations. First, the sample was small, drawn from a single center, and predominantly male, which limits the external validity of the findings and prevents generalization to all Mexican patients with post-stroke spasticity. Second, because this was a preliminary psychometric evaluation, structural validity was not formally tested and item reduction was not performed. Third, test-retest reliability was not assessed; therefore, the temporal stability of PRISM-MX and its usefulness for monitoring longitudinal changes during rehabilitation remain to be established. Responsiveness to change and measurement error were also not evaluated. Nevertheless, the study has important strengths, including the use of a structured cross-cultural adaptation process, cognitive debriefing with patients, the integration of patient-reported and clinical measures, and the focus on a clinically relevant but previously unmet need in Mexican stroke rehabilitation.
Overall, the present findings suggest that PRISM-MX is a promising instrument for assessing the patient-perceived impact of post-stroke spasticity in Mexico. Future studies should include larger, multicenter, and more demographically balanced samples to evaluate structural validity, test-retest reliability using intraclass correlation coefficients in clinically stable patients, responsiveness to change, and measurement invariance across relevant clinical and sociodemographic groups.
Conclusion
In conclusion, the Mexican Spanish version of the Patient-Reported Impact of Spasticity Measure (PRISM-MX) was successfully cross-culturally adapted and was considered understandable, culturally relevant, and acceptable by adults with post-stroke spasticity. In this preliminary pilot study, the original 41-item structure was retained, and initial analyses suggested high internal consistency and clinically plausible associations with disability and quality-of-life indicators. These findings support the potential usefulness of PRISM-MX as a patient-reported outcome measure for assessing the perceived impact of spasticity in Mexican neurorehabilitation settings. However, definitive psychometric validation remains pending. Future studies with larger, multicenter, and more demographically balanced samples are needed to evaluate structural validity, test-retest reliability, responsiveness to change, measurement error, and measurement invariance.
Supplemental Material
sj-docx-1-nre-10.1177_10538135261462949 - Supplemental material for PRISM-MX for Post-Stroke Spasticity: Cross-Cultural Adaptation and Preliminary Psychometric Evaluation in a Mexican Sample
Supplemental material, sj-docx-1-nre-10.1177_10538135261462949 for PRISM-MX for Post-Stroke Spasticity: Cross-Cultural Adaptation and Preliminary Psychometric Evaluation in a Mexican Sample by Roberto C. Pech-Argüelles, Axel V. Ortiz-Chávez, Ana R. Abreo-Hernández, Shilia L. Vargas-Echeverría and Rajiv Reebye in NeuroRehabilitation
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to the patients and their families for their valuable participation in this study. We also acknowledge the healthcare professionals and rehabilitation staff of Hospital General Regional No. 1 “Lic. Ignacio García Téllez” of the Mexican Social Security Institute (IMSS), whose collaboration and support were essential for participant recruitment, data collection, and the overall development of this project.
Special thanks are extended to the members of the expert panel and the translators who contributed to the cross-cultural adaptation process. In particular, we gratefully acknowledge Olivia Stringel Montes de Oca and Emmanuel Duvignau-Dondé for their work as bilingual Spanish translators; Clayton Blunk and Omar Argüelles for their contributions as native English back-translators; and María José Góngora for her valuable support and guidance throughout the adaptation process.
The authors also wish to express their special appreciation to William Barry McKay for generously sharing the original version of the Patient-Reported Impact of Spasticity Measure (PRISM) and its measurement scales, which made this study possible.
Ethical Considerations
The study was conducted in accordance with institutional and national regulations for research involving human participants, including the Mexican General Health Law and the principles of the Declaration of Helsinki. The research protocols were reviewed and approved by the Local Research and Ethics Committee of the Instituto Mexicano del Seguro Social (IMSS). Approval was granted under protocol numbers R-2024-3201-080 and R-2025-3201-035.
Consent to Participate
Written informed consent to participate was obtained from all participants prior to enrollment in the study.
Consent for Publication
Not applicable.
Author Contributions
Roberto C. Pech-Argüelles contributed to study conceptualization, participant recruitment, data collection, and drafting of the manuscript. Axel V. Ortiz-Chávez contributed to participant assessment, data collection, and critical revision of the manuscript. Ana R. Abreo-Hernández contributed to participant assessment, data interpretation, and critical revision of the manuscript. Shilia L. Vargas-Echeverría contributed to methodological design, formal analysis, interpretation of results, and manuscript writing and editing. Rajiv Reebye contributed to study conceptualization, supervision, interpretation of findings, and critical revision of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. Data are not publicly available due to privacy and institutional restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.