
Abstract
Background
Spastic cerebral palsy (CP) commonly impairs cervico-mandibular mobility and motor coordination due to increased muscle tone and altered postural control, potentially affecting head stability and orofacial function.
Objective
To compare the immediate effects of exercise- and manual therapy–based interventions on temporomandibular and cervical mobility in children with spastic CP, contrasting active versus passive rehabilitation strategies.
Methods
This single-blind, randomized crossover trial included 52 children with spastic CP (mean age 10.8 ± 2.4 years; GMFCS levels I–IV). Each received one exercise and one manual therapy session in randomized order with a one-week interval. Owing to missed second-week appointments, 44 children completed the exercise session and 48 completed the manual therapy session, resulting in partial crossover completion. Mandibular range of motion (maximal opening, lateral deviation, protrusion), cervical range of motion (flexion, extension, rotation), and craniovertebral angle were assessed immediately before and after each intervention.
Results
Both interventions produced significant immediate improvements in mandibular and cervical mobility (p < 0.001). Exercise resulted in greater gains in selected active mandibular movements, whereas manual therapy elicited larger improvements in cervical mobility. Craniovertebral angle increased following both interventions, with no significant between-intervention difference, indicating comparable effects on head posture. Effect sizes were moderate to large, and no carryover effects were detected.
Conclusion
Exercise and manual therapy induce modality-specific immediate neuromechanical responses in the cervico-mandibular system in children with spastic CP. These findings reflect short-term rather than long-term effects and suggest both approaches may be considered in individualized pediatric neurorehabilitation planning.
Clinical Messages
Both exercise and manual therapy produced statistically significant short-term improvements in temporomandibular and cervical range of motion in children with spastic cerebral palsy.
Exercise primarily enhanced selected active mandibular movements, likely reflecting improvements in task-specific motor control and coordination.
Manual therapy was associated with greater improvements in cervical mobility, although no significant between-intervention difference was observed for head posture (craniovertebral angle).
No adverse events occurred, and all participants tolerated both interventions well.
The findings suggest that these modalities may offer complementary short-term effects; however, the potential benefit of combining them requires further investigation, as combined interventions were not directly evaluated in this study.
Introduction
Cerebral palsy (CP) is the most common cause of childhood physical disability and is characterized by permanent, non-progressive disturbances in movement and posture arising from early brain injury (Blair & Cans, 2025). In addition to gross motor impairments, spastic CP frequently affects orofacial and cervical motor function, compromising chewing, swallowing, speech, and overall oral-motor efficiency (Liu et al., 2024; Serel Arslan et al., 2022). Persistent spasticity and altered postural control disturb the biomechanics of the temporomandibular joint (TMJ) and cervical spine, leading to restricted mobility and aberrant mandibular patterns that negatively influence functional performance and oral health–related quality of life (Almotareb & Al-Shamahy, 2024; De Castelo Branco Araújo et al., 2022; Joy et al., 2021).
The TMJ and cervical spine form an integrated functional complex connected through shared muscular, fascial, and neural pathways that coordinate mandibular and head–neck function (Fassicollo et al., 2021). Dysfunction in one region often affects the other; cervical impairments alter mandibular kinematics, whereas malocclusion or mandibular deviation may elicit compensatory cervical muscle activation (Peng et al., 2021). In children with spastic CP, asymmetrical muscle tone, impaired postural control, and altered movement patterns may further influence this functional interrelationship and contribute to limitations in jaw and cervical mobility (Bensi et al., 2020). Given that spastic CP represents the predominant motor subtype in pediatric populations, these alterations are most commonly observed within a hypertonic neuromuscular profile characterized by increased muscle stiffness and reduced selective motor control. Despite the clinical relevance of this interdependence, TMJ-focused rehabilitation remains limited within CP management, which traditionally emphasizes gross motor outcomes over integrated orofacial and cervical motor performance (Ibrahim et al., 2025; Serel Arslan et al., 2022).
Current rehabilitation perspectives underscore the necessity of combining active neuromuscular training with passive mechanical facilitation to restore mobility in complex multi-joint systems (Shaffer & Naze, 2023a, 2023b). Exercise-based interventions enhance voluntary motor activation, coordination, and movement control, whereas manual therapy produces rapid biomechanical and neurophysiological effects through mechanoreceptor stimulation and modulation of segmental motor excitability (Lu & Du, 2024). In adults with temporomandibular disorders (TMD), both modalities yield immediate improvements in mandibular and cervical kinematics (Fassicollo et al., 2021; Greco & Michelotti, 2025). However, the neurophysiological profile of spastic CP—including heightened reflex activity, increased muscle spindle sensitivity, and altered afferent processing—differs substantially from that of neurologically typical adults, creating uncertainty regarding the transferability of these findings to pediatric spasticity and pediatric neurorehabilitation contexts.
The spastic CP phenotype provides a unique model for investigating cervico-mandibular mobility-related interactions. Hypertonicity in the jaw and neck musculature disrupts afferent feedback, limits joint excursion, and contributes to functional chewing deficits (Serel Arslan et al., 2022). Interventions capable of transiently modulating tone or enhancing joint mobility may therefore elicit immediate neuromechanical responses that can inform subsequent rehabilitation planning (Lu & Du, 2024). Establishing these short-term responses is essential for understanding the responsiveness of the pediatric CP neuromuscular system and for informing clinical neurorehabilitation decision-making, including intervention sequencing and modality selection.
Although previous studies in healthy adults have examined either TMJ-focused or cervical-focused therapeutic approaches, no investigation has directly contrasted active versus passive interventions within the same pediatric CP cohort. To date, no randomized crossover trial has evaluated the immediate effects of exercise and manual therapy on both TMJ and cervical mobility in children with spastic CP, representing a notable gap in the pediatric neurorehabilitation literature.
The present investigation was designed to address this gap by comparing the immediate effects of exercise-based and manual therapy–based interventions on temporomandibular and cervical range of motion in children with spastic CP. It was hypothesized that both interventions would produce significant short-term improvements, with exercise expected to enhance mandibular mobility through active neuromuscular engagement and manual therapy anticipated to promote cervical flexibility via passive mechanical facilitation within a neurorehabilitative framework. Accordingly, the primary objective of the study was to determine the immediate effects of these two intervention approaches on mandibular mobility, whereas the secondary objective was to examine their effects on cervical mobility and craniovertebral angle.
Materials and Methods
Study Design
This investigation was structured as a single-blind, randomized crossover clinical trial designed to assess the immediate effects of exercise therapy and manual therapy on temporomandibular and cervical mobility in children with spastic CP. The assessor was blinded to the intervention order. The crossover framework enabled each participant to receive both interventions, thereby minimizing inter-individual variability and enhancing statistical precision—an important consideration given the heterogeneity in tone distribution and postural asymmetry typical of spastic CP. A one-week inter-intervention washout period was applied between the two sessions to minimize potential residual effects and reduce the likelihood of short-term carryover responses. This interval was selected based on previous rehabilitation studies reporting that immediate biomechanical effects of single-session interventions are transient and unlikely to persist beyond several days in pediatric populations. The crossover design was selected to enhance within-subject neurorehabilitation responsiveness while controlling for individual differences in spasticity severity. The study was conducted at a pediatric special education center between August 2023 and August 2024. All procedures adhered to the principles of the Declaration of Helsinki and were approved by the XXX University Ethics Committee (Approval No: 98, 24.07.2023). Written informed consent was obtained from parents or legal guardians, and verbal assent was provided by all participating children.
Participants
Participants were recruited from two branches of a pediatric rehabilitation center in Türkiye between August 2023 and April 2024. Inclusion criteria encompassed a confirmed diagnosis of spastic CP, age between 7 and 14 years, Gross Motor Function Classification System (GMFCS) Levels I–IV, and sufficient cognitive and postural capacity to maintain an upright sitting position and follow simple verbal instructions. Cognitive capacity was evaluated clinically based on the child's ability to understand and follow simple verbal commands during initial assessment, while postural capacity was determined by the ability to maintain a supported sitting position without external assistance. To control for the potential influence of excessive muscle tone on movement performance, only children with mild-to-moderate spasticity (Modified Ashworth Scale ≤2 for cervical muscle groups) were included. Exclusion criteria were established to avoid confounding influences and included fixed jaw or cervical deformities, orthopedic or neurosurgical procedures within the previous six months, botulinum toxin or antispastic drug administration within the past three months, acute orofacial pain or temporomandibular joint pathology, and uncontrolled epilepsy or significant cognitive impairment limiting cooperation.
A total of fifty-two children fulfilled these criteria and were enrolled through convenience sampling. Diagnoses and GMFCS classifications were independently confirmed by a pediatric neurorehabilitation physiotherapist and a dentist with expertise in orofacial assessment to enhance diagnostic accuracy. Although detailed cerebral palsy motor subtype classification (e.g., hemiplegic, diplegic, quadriplegic) was not systematically recorded within the present experimental protocol, spastic CP constitutes the predominant clinical presentation in pediatric populations, and the applied inclusion criteria (MAS ≤2) ensured a relatively homogeneous sample in terms of tone severity. The study did not further stratify participants according to CP subtype or degree of spasticity; therefore, potential variability related to these factors was controlled indirectly through within-subject comparison inherent to the crossover design. Randomization to either the Exercise–Manual Therapy (intervention order A) or Manual Therapy–Exercise (intervention order B) pathway was implemented using sequentially numbered, opaque, sealed envelopes prepared by an investigator not involved in data collection, ensuring allocation concealment (Figure 1).
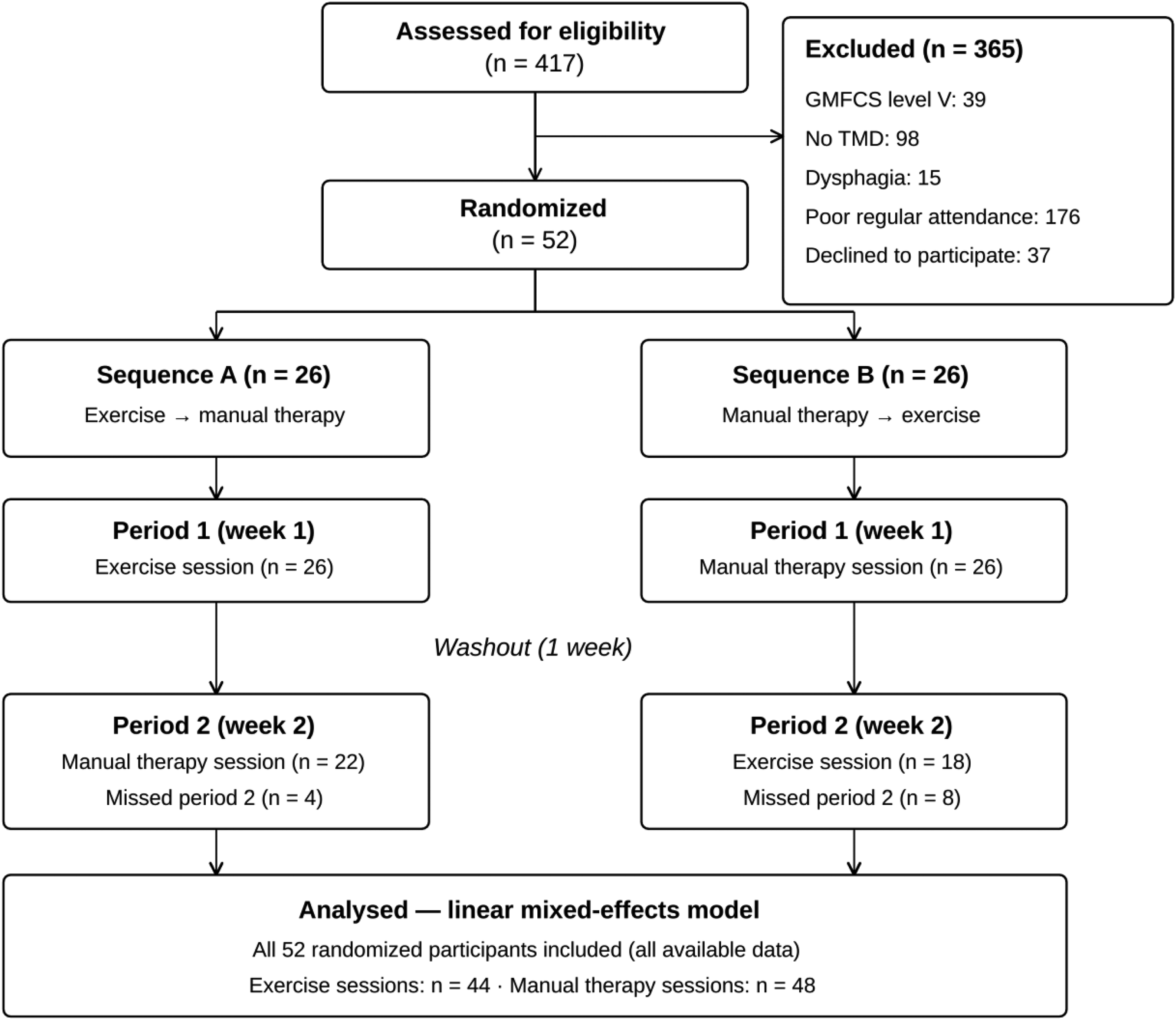
Flow diagram of participant recruitment and allocation.
Interventions
The exercise intervention, lasting approximately 20 min, targeted active neuromuscular control of the temporomandibular and cervical regions. Sessions began with a brief warm-up involving gentle cervical rotations and diaphragmatic breathing to facilitate relaxation and reduce spasticity. This was followed by active mandibular exercises—maximal opening, lateral deviation, and protrusion—performed in three sets of ten repetitions with 30-s rest intervals between sets. Mirror feedback was employed to improve midline alignment and motor accuracy. Cervical exercises included active flexion, extension, rotation, and lateral flexion executed in a supported seated posture within pain-free limits to avoid involuntary co-contraction and abnormal synergy. The final component of the intervention protocol involved combined mandibular–cervical coordination tasks designed to reinforce functional coordination between jaw and cervical movements (Figure 2). All exercises were performed under verbal supervision to ensure correct execution without manual assistance.
Protocol for active mandibular coordination and cervical mobility exercises.
Manual therapy sessions were delivered by a physiotherapist experienced in pediatric neurorehabilitation with more than five years of clinical experience and formal training in Maitland-based manual therapy techniques. Each session lasted approximately 20 min and followed a standardized protocol involving low-grade Maitland mobilizations of the temporomandibular joint (anterior and inferior glides, Grades I–II), passive segmental cervical mobilizations including traction, oscillatory flexion–extension glides, and graded lateral glides, as well as soft tissue release of the suboccipital, upper trapezius, and sternocleidomastoid muscles. These techniques were applied within comfortable limits without provoking pain or joint clicking. The final component of the session involved gentle axial traction to promote neutral craniovertebral alignment and short-term neuromuscular relaxation (Figure 3).

Application of passive temporomandibular joint and cervical mobilization techniques.
Outcome Measures
All outcomes were assessed immediately before and after each intervention to capture short-term therapeutic responses. Evaluations were performed by the same physiotherapist and dentist to minimize inter-rater variability. A standardized sitting posture—with feet flat, trunk supported, and head in a neutral position—was maintained throughout assessments, and environmental conditions such as lighting, seat height, and camera angle were kept consistent to reduce measurement error.
Mandibular range of motion was designated as the primary outcome measure and was measured using a digital goniometer with ±1° precision. Measurements included maximal mouth opening, right and left lateral deviation, and mandibular protrusion. Three repetitions were recorded for each movement, and mean values were used for analysis.
Cervical mobility—including flexion, extension, right and left lateral flexion, and rotation—served as a secondary outcome and was assessed using a universal goniometer according to the protocol described by Youdas et al. (Youdas et al., 1991). Forward head posture was quantified using the craniovertebral angle (CVA), calculated from standardized lateral photographs acquired with a tripod-mounted camera positioned 1.5 meters from the participant. Anatomical landmarks were marked to enhance measurement consistency, and images were analyzed using Kinovea software (version 0.9.5, Kinovea Open-Source Project, France). Smaller CVA values indicated a more pronounced forward posture.
Two measurements were taken for each CVA assessment, and mean values were analyzed. This approach was adopted to minimize fatigue and postural variability in children with spastic CP during repeated photographic acquisition. Calibration of all measurement devices was performed before data collection, and intra-rater reliability had been confirmed in a pilot phase, demonstrating excellent consistency (ICC > 0.90).
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics (version 25.0, Armonk, NY, USA). Normality of data distribution was assessed using the Shapiro–Wilk test. Continuous variables were summarized as mean ± standard deviation. Within-session changes were examined using paired-sample t-tests or Wilcoxon signed-rank tests depending on distributional properties. To evaluate the effects of intervention type and intervention order while accommodating the unbalanced data arising from partial crossover completion, a linear mixed-effects model was fitted with intervention type, time, sequence, and the intervention × time interaction specified as fixed effects, and participant entered as a random effect (random intercept). Because this model estimates parameters by restricted maximum likelihood under a missing-at-random assumption, it incorporates all available observations—including those from participants who attended only one of the two sessions—without listwise deletion or imputation; accordingly, all 52 enrolled participants contributed to the model. Potential order and carryover effects were assessed through the sequence and sequence × intervention terms. Given the crossover design, inter-individual variability related to clinical heterogeneity (including differences in motor presentation and spasticity levels) was further controlled through within-subject comparisons. Effect sizes were calculated using Cohen's d, classified as small (<0.2), moderate (≈0.5), or large (≥0.8). Statistical significance was set at p < 0.05, and all analyses included 95% confidence intervals.
Results
Fifty-two children with spastic cerebral palsy were initially enrolled and completed baseline assessments. Missed second-week appointments resulted in forty-four participants completing the exercise session and forty-eight completing the manual therapy session, yielding partial crossover completion. Analyses were therefore conducted using a linear mixed-effects model that incorporated all available pre- and post-intervention data; a sensitivity analysis restricted to participants who completed both intervention sessions yielded comparable outcomes, supporting the stability of the findings.
The study cohort (n = 52) consisted of 28 boys and 24 girls, with a mean age of 10.8 ± 2.4 years. Functional distribution across Gross Motor Function Classification System levels was homogeneous (Level I = 14; Level II = 28; Level III = 7; Level IV = 3). Baseline comparisons between intervention sequences (Exercise → Manual Therapy vs Manual Therapy → Exercise) revealed no significant differences in demographic or clinical variables (p > 0.05 for all), confirming successful randomization (Table 1).
Changes in Temporomandibular Joint Range of Motion (ROM).

E: Exercise; MT: Manual Therapy; mm: millimeter ; Δ = post–pre difference.
Both exercise and manual therapy resulted in significant pre–post improvements across all temporomandibular joint range of motion parameters. Exercise demonstrated significantly greater improvements in maximal mouth opening and mandibular protrusion compared with manual therapy, whereas no significant between-intervention difference was observed for lateral deviation (p = 0.12). Effect size analysis indicated large effects for exercise in mouth opening (d = 0.91) and protrusion (d = 0.85), while manual therapy demonstrated moderate-to-large effects across the same parameters. These findings suggest a differential responsiveness favoring exercise primarily for active mandibular movements rather than a uniform superiority across all temporomandibular outcomes (Table 1).
Cervical mobility increased significantly following both interventions. Manual therapy demonstrated significantly greater improvements in cervical flexion, extension, and rotation compared with exercise (p < 0.05 for all between-intervention comparisons). However, for craniovertebral angle (CVA), both interventions resulted in significant within-session improvements, and no significant between-intervention difference was observed (p = 0.28). Accordingly, neither intervention demonstrated superiority in immediate postural alignment outcomes. Effect size analysis indicated moderate-to-large effects for cervical mobility parameters, with manual therapy showing relatively larger effects for flexion and extension. CVA improvements demonstrated moderate effect sizes in both groups. No significant treatment-by-sequence interaction was detected (p = 0.41), indicating the absence of a measurable carryover effect within the crossover design (Table 2).
Changes in Cervical Range of Motion and CVA.

E: Exercise; MT: Manual Therapy; CVA: Craniovertebral Angle; Δ = post–pre difference.
Overall, the results indicate a modality-specific pattern of response, with exercise demonstrating greater effects on active mandibular mobility, whereas manual therapy produced larger improvements in cervical mobility parameters. Importantly, these effects were parameter-specific and should not be generalized across all outcomes. Improvements in craniovertebral angle were observed following both interventions without a statistically significant difference between modalities, indicating comparable short-term effects on head posture (Table 3).
Effect Sizes and 95% Confidence Intervals for Within-Session Intervention Effects.
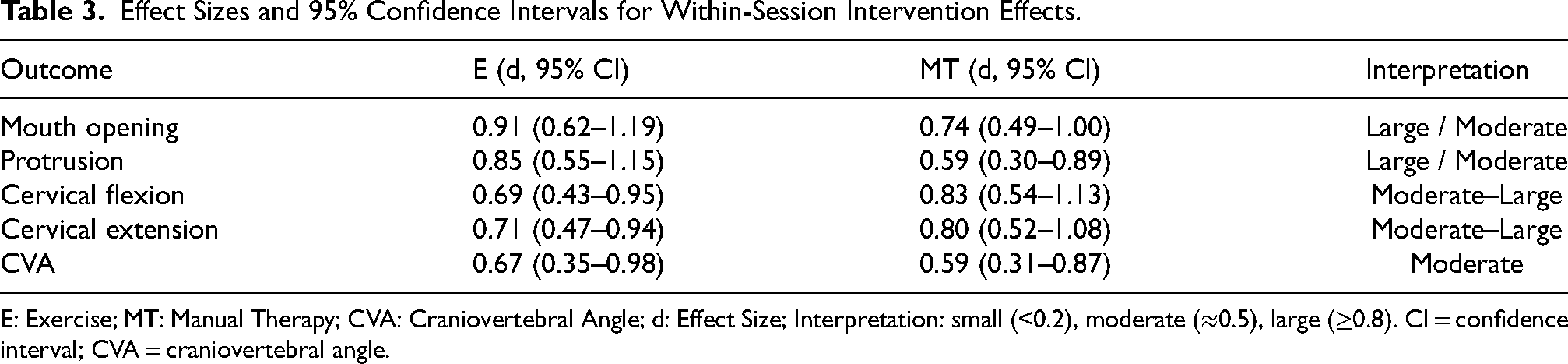
E: Exercise; MT: Manual Therapy; CVA: Craniovertebral Angle; d: Effect Size; Interpretation: small (<0.2), moderate (≈0.5), large (≥0.8). CI = confidence interval; CVA = craniovertebral angle.
Discussion
This randomized crossover trial examined the immediate effects of exercise-based and manual therapy–based interventions on temporomandibular and cervical mobility in children with spastic CP. Both interventions produced statistically significant short-term improvements in mandibular and cervical ROM, as well as improvements in head posture. However, the distribution of these improvements differed by intervention type: exercise yielded larger increases in active mandibular mobility, whereas manual therapy produced superior enhancements in cervical motion. Importantly, no significant between-intervention difference was observed for craniovertebral angle, indicating comparable effects of both modalities on immediate postural alignment. These findings demonstrate the capacity of both active and passive therapeutic approaches to induce short-term neuromechanical responses rather than long-term adaptations within the cervico-mandibular system of children with spastic CP.
The present results reinforce the concept that the TMJ and cervical spine operate as an interdependent functional unit, as described in previous biomechanical and neurophysiological studies (Fassicollo et al., 2021; Peng et al., 2021). Adult studies have demonstrated that cervical interventions can influence mandibular kinematics and that TMJ-focused interventions may affect cervical muscle activity, particularly in individuals with TMD (Minervini et al., 2023; Petronis et al., 2023; Shaffer & Naze, 2023a, 2023b). However, such findings have largely been reported in neurologically typical adults and in the context of chronic pain or mechanical dysfunction. To current knowledge, this investigation is the first to evaluate immediate cervico-mandibular responses to active and passive interventions in a pediatric neurological population, thereby extending current understanding of functional interaction between mandibular and cervical mobility to the context of childhood spasticity and pediatric neurorehabilitation practice.
The magnitude of change observed in mandibular mobility following exercise is consistent with short-term improvements reported in healthy adults undergoing proprioceptive neuromuscular facilitation or coordination-based training (Shimada et al., 2023). Likewise, the substantial increases in cervical flexion and extension following manual therapy parallel previously documented effects of low-grade mobilization techniques in individuals with cervical dysfunction (Sampsonis et al., 2025). The absence of a treatment-by-sequence interaction further suggests that the inter-intervention washout period was sufficient to prevent carryover effects, supporting the internal validity of the crossover design and the robustness of within-session intervention effects.
Differences in intervention responsiveness likely reflect distinct underlying mechanisms. Exercise-based interventions may enhance voluntary motor control and coordination through increased task-specific activation and practice-dependent motor engagement, which may preferentially support improvements in active mandibular movements. In contrast, manual therapy is associated with mechanical and reflex-mediated responses, including modulation of muscle tone, stimulation of peripheral mechanoreceptors, and temporary reductions in muscle stiffness (Clark, 2024; Raciti et al., 2025; Shaffer & Naze, 2023a, 2023b). These mechanisms should be interpreted as plausible physiological explanations rather than directly measured outcomes within the present study. Such effects may contribute to transient reductions in muscle stiffness and facilitate joint excursion, which may partly explain the greater improvements observed in cervical range of motion. However, given that neurophysiological variables were not directly assessed, these interpretations should be considered hypothetical (Marin et al., 2024; Tangüner & Doymaz, 2025).
The improvements observed in this study carry potential clinical implications for pediatric rehabilitation. Enhanced mandibular ROM may contribute to improved oral motor function, while improved cervical alignment may support head control and postural stability. However, it is important to emphasize that functional outcomes such as mastication, swallowing, or speech were not directly measured in the present study, and therefore these implications should be interpreted with caution (Happee et al., 2023; Joy et al., 2021; Kimura et al., 2025; Liu et al., 2024). The complementary profiles of the two interventions—exercise enhancing active neuromuscular recruitment and manual therapy improving passive tissue extensibility—suggest that a multimodal approach may be beneficial; however, this hypothesis requires direct investigation, as a combined intervention protocol was not evaluated in the current study.
Several methodological strengths support the credibility of these findings, including the randomized crossover design, use of an inter-intervention washout period to control for order effects, inclusion of children across GMFCS Levels I–IV, and use of standardized and reliable measurement tools with demonstrated intrarater consistency. Nonetheless, several limitations should be acknowledged. Although partial crossover completion occurred because some participants missed their second-week session, this unbalanced data structure was accommodated using a linear mixed-effects model that incorporated all available observations, thereby reducing the risk of bias associated with analysing only complete cases. The study assessed only immediate outcomes; therefore, conclusions regarding the persistence, retention, or functional integration of these improvements cannot be drawn. Longitudinal studies examining medium- and long-term effects, as well as functional outcomes related to feeding, communication, or daily activity performance, are needed. Additionally, incorporating objective neuromuscular assessments such as surface electromyography or three-dimensional motion analysis could provide deeper insight into the motor control changes underlying these short-term responses. A combined intervention arm (exercise plus manual therapy) may also help determine whether synergistic effects exceed those of isolated treatment modalities within structured neurorehabilitation programs.
This study focused on children with mild-to-moderate functional impairment (GMFCS I–IV); thus, the findings may not be generalizable to individuals with severe spasticity or dystonia. Furthermore, although spasticity level was controlled through inclusion criteria (MAS ≤2), the absence of detailed motor subtype classification limits interpretation across different CP phenotypes. However, the consistent within-session gains in both TMJ and cervical outcomes underscore the responsiveness of the pediatric CP neuromotor system to well-targeted interventions and support early-stage neurorehabilitation responsiveness.
Overall, both exercise and manual therapy techniques produced immediate neuromechanical responses in temporomandibular and cervical mobility in children with spastic CP. Exercise demonstrated greater influence on active mandibular movements, while manual therapy more effectively improved cervical ROM. No superiority was observed between interventions for postural alignment (CVA). These complementary effects suggest—but do not confirm—the potential value of integrating both modalities, and future longitudinal studies should investigate whether these acute responses translate into sustained functional gains in feeding, speech, and global motor performance within real-world neurorehabilitation settings.
Conclusion
Both exercise-based and manual therapy–based interventions produced immediate statistically significant short-term improvements in temporomandibular and cervical mobility in children with spastic cerebral palsy. Exercise generated greater enhancement in selected active mandibular movements, whereas manual therapy elicited greater gains in cervical mobility. However, no significant between-intervention difference was observed for craniovertebral alignment, indicating comparable effects of both modalities on immediate head posture.
These findings reflect transient neuromechanical responses rather than long-term adaptations and should be interpreted within the context of immediate post-intervention outcomes. The observed modality-specific effects suggest differential responsiveness depending on movement type (active vs passive), rather than a uniform superiority of one intervention over the other.
Although the results suggest that combining these modalities may be beneficial, this assumption remains speculative, as a combined intervention approach was not directly tested in the present study. Furthermore, functional outcomes such as feeding, speech, and sensorimotor performance were not directly assessed; therefore, their potential improvement cannot be inferred from the present findings.
Longitudinal studies are needed to determine the durability of these immediate neuromechanical changes and to establish their impact on functional independence and quality of life in children with spastic cerebral palsy.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to all children and their families who participated in this study. We also thank the clinicians and administrative staff at the XXX for their support during data collection.
Ethical Considerations and Consent to Participate
This study was approved by XXX Ethics Committee (Protocol No: XX, Decision No: XX, Date:24.07.2023). All procedures were conducted in accordance with the ethical standards of the institutional and national research committees and with the 1964 Helsinki Declaration and its later amendments. Written informed consent was obtained from all participants and their legal guardians prior to inclusion in the study.
Consent for Publication
Not applicable.
Authors’ Contributions
ÖBC and MFV were responsible for participant evaluation, data collection, and manuscript drafting. BUT contributed to the study design, supervised the assessments, and provided critical revisions. All authors participated in data analysis, interpretation of results, and manuscript preparation. All authors have read and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Thesis Statement
This article is derived from the doctoral thesis of Özge BAYKAN ÇOPUROĞLU, completed at Muğla Sıtkı Koçman University, Institute of Health Sciences, Department of Physiotherapy and Rehabilitation, under the supervision of Baki Umut TUĞAY. Portions of this research were presented as part of the doctoral dissertation and have not been published previously in any peer-reviewed journal.