
Abstract
Purpose
Individuals with stroke have difficulty rotating their trunk and adjusting their supporting foot when negotiating spatial constraints. This study aimed to classify movement patterns used when passing through narrow openings and to identify factors associated with stroke-specific patterns.
Methods
Twenty-three individuals with stroke (age: 60.7 ± 10.1 years, time after stroke: 15.2 ± 21.1 months, subacute and chronic, independently ambulatory), 23 age-matched community-dwelling adults (61.0 ± 9.7 years), and 12 young adults (25.4 ± 2.5 years) were recruited. Participants walked through openings of various widths. Movement patterns were independently classified by three trained physical therapists, and inter-rater agreement was assessed. Generalized linear mixed models with participants as a random effect were used to examine associations between pattern selection and clinical/environmental factors.
Results
Five passing patterns were identified: (A) pivot, (B-1) early pivot, (B-2) early pivot with reverse trunk rotation, (C) multiple steps, and (D) no-rotation. Inter-rater agreement was substantial (Cohen's κ = .76). Stroke-specific patterns were patterns B-2 and C. The mixed-model analysis showed that B-2 and C were more likely with narrower openings (odds ratio [OR]: .52, 95% confidence interval [CI]: .39–.70; and OR: .18, 95% CI: .11–.32, respectively; both p < .001). TUG performance was not significantly associated with pattern C (OR: 1.22, 95% CI: .99–1.49, p = .056).
Conclusion
Opening width was associated with stroke-specific pattern selection. Multi-step strategies may reflect increased stability demands, whereas pivot-like strategies may be associated with better mobility. These findings may help clinicians assess movement behaviors in constrained environments.
Keywords
Introduction
Stroke symptoms include unilateral motor paralysis and an asymmetric gait, complicating forward movement and balance (Jørgensen et al., 2000; Patterson et al., 2008). Patients with asymmetric gait have impaired coordination of mediolateral stability during straight walking (Beyaert et al., 2015; Pai et al., 1994; Turnbull et al., 1996). Balance difficulties are emphasized by gait patterns that must be modified in response to environmental constraints, including situations that necessitate turning, which increases the risk of falling sideways (Chan & Tsang, 2017; Zou et al., 2021). For individuals with stroke, rotating the trunk to pass through a narrow opening while walking forward may cause lateral loss of balance and collision with the frame (Muroi et al., 2017, 2022). To walk safely through a narrow opening, individuals must shift toward the center of the opening and adjust their posture to avoid collision with the frame (Bilhaut et al., 2023; Hackney et al., 2013, 2020; Higuchi et al., 2009, 2012; Lucaites et al., 2020; Warren & Whang, 1987). Assessing the ability to safely pass through an opening may clarify why controlling adaptive movements is difficult in individuals with stroke.
Previous studies examining turning behavior in individuals with stroke and older adults have commonly categorized movement patterns using three key components: (1) supporting foot, (2) trunk rotation direction, and (3) number of steps (Barrois et al., 2017; Dite & Temple, 2002; Sakazaki et al., 2026; Thigpen et al., 2000). These components represent fundamental biomechanical determinants of rotational movement and are frequently used to describe pivot-like turning and multistep turning, both in stroke populations and in older adults. Individuals with stroke exhibit different movement strategies depending on the supporting limb and rotation direction (Chen et al., 2014; Duval et al., 2011). When rotation is performed around the non-paretic limb, pivot-like movements are feasible; however, when the paretic limb serves as the supporting foot, reduced motor function may limit such strategies. As a result, individuals with stroke may adopt alternative strategies, such as multi-step rotations, to maintain stability. Understanding these movement patterns during passage through a narrow-opening is clinically important because the ability to realign the body in constrained spaces is essential for everyday mobility (e.g., doorways, furniture gaps), and difficulty with such adaptive movements contributes to mobility limitations in individuals with stroke.
A previous report (Muroi et al., 2017) targeting individuals with stroke in the acute or chronic phases revealed that the paretic and non-paretic sides entered at almost the same rate, possibly influenced by the frequent use of multiple steps. However, there was individual variation in the number of steps taken and the direction of rotation; thus, if the number of steps, entry direction, and supporting foot are not confirmed, the characteristics of the movement patterns of individuals with stroke may not be captured. These diverse behaviors suggest that distinct movement patterns may exist. However, previous studies (Muroi et al., 2017, 2022) have primarily focused on collision frequency or entry direction, and a comprehensive classification of movement patterns during narrow-opening passage is lacking. Therefore, the present study classified movement patterns during passage through a narrow-opening based on supporting foot, trunk rotation direction, and number of steps, which are key components of turning behavior (Barrois et al., 2017; Dite & Temple, 2002; Sakazaki et al., 2026; Thigpen et al., 2000). The authors hypothesized that individuals with stroke would exhibit distinct movement patterns when passing through narrow openings compared with healthy individuals. The authors further hypothesized that the selection of these movement patterns would be associated with opening width and individual mobility limitations. These findings may help clarify adaptive movement patterns under spatial constraints and inform rehabilitation approaches for safe mobility.
Methods
Participants
This cross-sectional study was approved by the ethics committee of Kameda Medical Center, Chiba, Japan (approval number: 12-089-150501) and was conducted in accordance with the Declaration of Helsinki. Participant recruitment and data collection were conducted between June 2013 and March 2015. All participants provided written informed consent.
Participants were divided into three groups: individuals with stroke, age-matched healthy older adults, and healthy young adults (detailed participant flow is shown in Supplementary Figure 1). Participants in the stroke group were recruited using a convenience sampling approach from current or discharged patients of a subacute hospital, all of whom were able to walk independently. Recruitment was conducted through therapist referral and hospital bulletin board advertisements, and participation was voluntary. Age-matched healthy older adults were recruited from community-dwelling individuals, whereas healthy young adults were recruited on a voluntary basis from hospital staff. All participants with stroke had residual hemiparesis of the lower limb with Brunnstrom recovery stage (BRS) 3–5 (Brunnstrom, 1966). The inclusion criteria were as follows: (a) at least 1 month after a first-time stroke, and (b) able to walk independently for more than 100 m with or without an assistive device. The exclusion criteria were as follows: (a) neurological, orthopedic, or other disorders that could affect walking; (b) history of visual deficits; (c) visual field deficits and visual spatial neglect (score of <3 on the visuospatial perception item of Stroke Impairment Assessment Set) (Liu et al., 2002; Tsuji et al., 2000); and (d) a score of <24 on the Mini-Mental State Examination (Holsinger et al., 2007). Age-matched and young control participants were recruited through hospital bulletin boards and the institutional intranet system. Individuals who expressed interest underwent eligibility screening. They were required to meet the same inclusion and exclusion criteria as the stroke group, except for a history of stroke. Young adults were included to examine whether age-related factors influence passing strategies independently of stroke. No priori sample size calculation was performed, as this study was exploratory in nature. The primary regression analyses were conducted within the stroke group. Moreover, to evaluate the adequacy of the current sample, post-hoc power analyses were conducted for the main group comparison and the primary generalized linear mixed models (GLMMs).
Clinical Measurements
Participant characteristics (sex, age, and height) and clinical documentation of stroke (stroke type, side of lesion, and date of stroke) were obtained from medical records. The mean body width at the shoulders was defined as the distance between the heads of the right and left humeri and was measured using a rigid measuring tape while participants stood in an upright position. This measure was adopted instead of the standard biacromial width because the aim was to capture the maximal frontal body width relevant to collision risk during passage through a narrow-opening, including soft tissue contributions. To minimize the influence of clothing, participants were asked to wear light or close-fitting garments during the measurement. This static measurement was used to determine the relative opening width for each participant. Moreover, the minimum passable width during dynamic walking was evaluated separately. Functional mobility was assessed with the Timed Up and Go (TUG) test (Ng & Hui-Chan, 2005). Participants were permitted to use their usual assistive devices during the TUG test. The proportion and type of assistive devices used by participants are presented in Table 1. The potential effect of assistive device use on TUG performance was not analyzed separately, as the primary aim was to evaluate overall functional mobility under usual walking conditions. Two trials were performed for each turning direction (toward the paretic and non-paretic sides). The order of turning direction was counterbalanced across participants to minimize potential order effects. The mean value of the four trials was used for analysis. Consistent with the standard TUG protocol, no practice trial was provided. Fall history during the past year was assessed using a questionnaire. Falls were defined according to Gibson's criteria (Gibson et al., 1987): an unexpected event in which a person comes to rest on the same level or a lower level, not as a result of a major intrinsic event (e.g., stroke onset), loss of consciousness, seizure, or external force, and excluding events such as bicycle accidents or incidental contact with environmental structures.
Participant Characteristics.
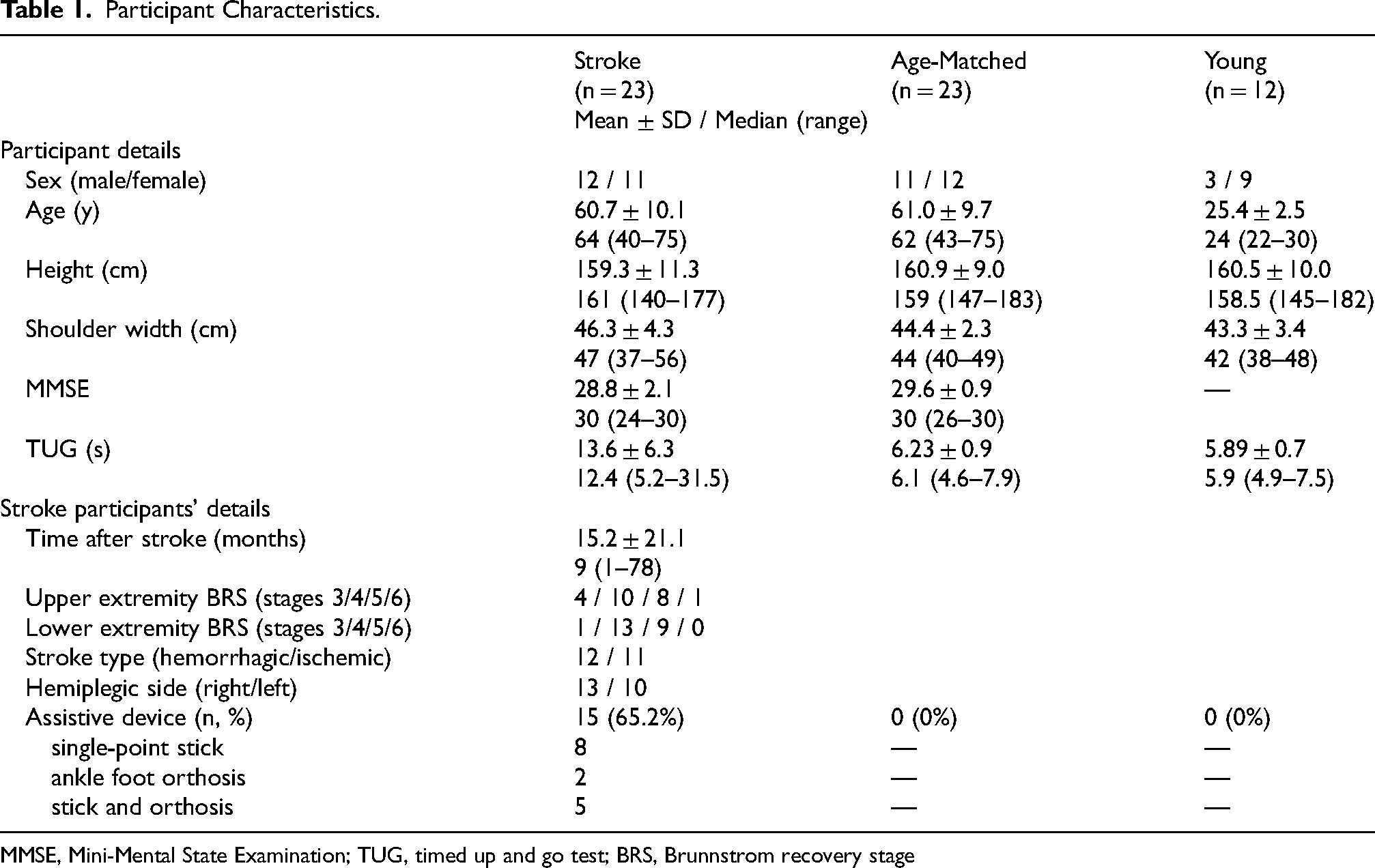
MMSE, Mini-Mental State Examination; TUG, timed up and go test; BRS, Brunnstrom recovery stage
Apparatus
The experiment was performed along a 6.0 m straight path. A door opening was located 4.0 m in front of the starting location. An opening was created as a space between two projector screens (Fig. 1). Each screen was attached to an aluminum frame (2.2 m wide × 2.0 m high), and the screens were perpendicular to the floor. The width of the opening was adjusted by changing the location of the edge of each screen. Although the frames were made of metal, they were not fixed to the floor, which reduced the impact of collision and ensured participant safety. This setup minimized the risk of injury while maintaining a realistic perception of an obstacle.

Experimental setup for the narrow-opening passing task.
Tasks and Procedures
Participants were instructed to walk at a normal speed and pass through the opening. Importantly, no instructions were given regarding the direction of body rotation. Participants were asked to use the movement strategy they naturally felt was easiest for passing through the opening. The opening widths were set at 0.9, 1.0, 1.1, 1.2, and 1.3 times the shoulder width of the participants. To ensure participants’ safety while attempting to pass through the opening, two physical therapists stood beside the door apparatus. The therapists were positioned behind the projection screens and were not visible to the participants until after passing through the opening, thereby minimizing potential visual influence on movement patterns. Participants who routinely used assistive devices (e.g., single-point cane and/or ankle–foot orthosis) were allowed to use them during the experiment for safety reasons. During the trials, collisions between the assistive device and the door frame were also monitored.
For each trial, the participants stood at the starting position with both feet aligned on the starting line in a quiet static stance while the opening was occluded by a large plate placed 20 cm in front of them. After adjusting the width of the opening, visual occlusion was removed. Participants were instructed to begin walking upon a verbal command from the examiner. Then the participants began walking. The order of opening widths was counterbalanced across participants using a computer-generated randomized sequence of three predefined assessment orders. After the pre-trial practice, the participants performed 15 trials (three trials for each opening width), and the task was recorded from the frontal and sagittal planes using two digital video recorders. Video data were analyzed to confirm the supporting foot and number of steps taken by the participants. After the task, the participants’ minimum passable widths were measured. The minimum passable width was defined as the minimum width that a participant could walk through the opening two consecutive times without body rotation. Participants were instructed to walk straight through the opening without rotating their trunk, even if collision occurred, and were encouraged to walk as naturally as possible. A trial was considered unsuccessful if any part of the body collided with the opening frame. The initial opening width was determined based on the participant's shoulder width or on the width at which collision had occurred during the main trials. If a collision occurred, the opening width was increased by 1 cm, whereas if the participant passed successfully, the width was decreased by 1 cm, and this procedure was repeated until the minimum width through which the participant could pass without collision in two consecutive trials was identified. Consequently, most participants completed the procedure within five trials. Body rotation was operationally defined as an observable rotation of the trunk relative to the walking direction. The relative minimum passable width was calculated as the ratio of the minimum passable width to the participant's shoulder width.
Video-Based Gait Analysis
Video-based gait analysis was performed without any dedicated motion-analysis software. Standard digital video cameras (HDR-CX430V; Sony, Japan) were used to record the frontal and sagittal views. Passing was defined using two temporal landmarks during the opening-crossing movement. First, the moment when the leading shoulder first crossed the plane of the opening was identified. At this moment, the supporting foot (pivoting foot) and the direction of trunk rotation were evaluated. Second, the movement was considered complete when the trailing shoulder fully passed through the opening. The number of steps was defined and counted starting from the leading shoulder crossing event and ending at the trailing shoulder clearance event. The number of steps taken between these two events was counted for each trial. All trials were recorded using a digital video camera at 60 frames per second. Prior to the formal analysis, the raters jointly reviewed sample videos to standardize the operational definitions of the passing events. The camera position was fixed to ensure a consistent viewing angle across all trials. For each trial, three physical therapists (clinical experience: 5, 7, and 12 years) independently identified (1) the supporting foot at the passing moment, (2) the direction of trunk rotation, and (3) the number of steps taken. The supporting (pivot) foot was defined as the limb in stance during the initial crossing of the leading shoulder. Accordingly, patterns were further interpreted based on whether the paretic or non-paretic limb served as the pivoting limb during trunk rotation. The raters were blinded to participants’ clinical data, including TUG performance and BRS scores, during the classification process. Inter-rater reliability for the initial independent classifications was assessed using Cohen's kappa coefficients calculated for each pair of raters, and the mean kappa value was .76, indicating substantial agreement. After an independent assessment, a consensus meeting was held among the three raters to resolve discrepancies and establish the final classification. The five passing patterns were operationally defined prior to analysis based on preliminary video observations and were treated as categorical variables for subsequent statistical analyses. The operational definitions of each pattern are provided in the Results section and Figure 2.
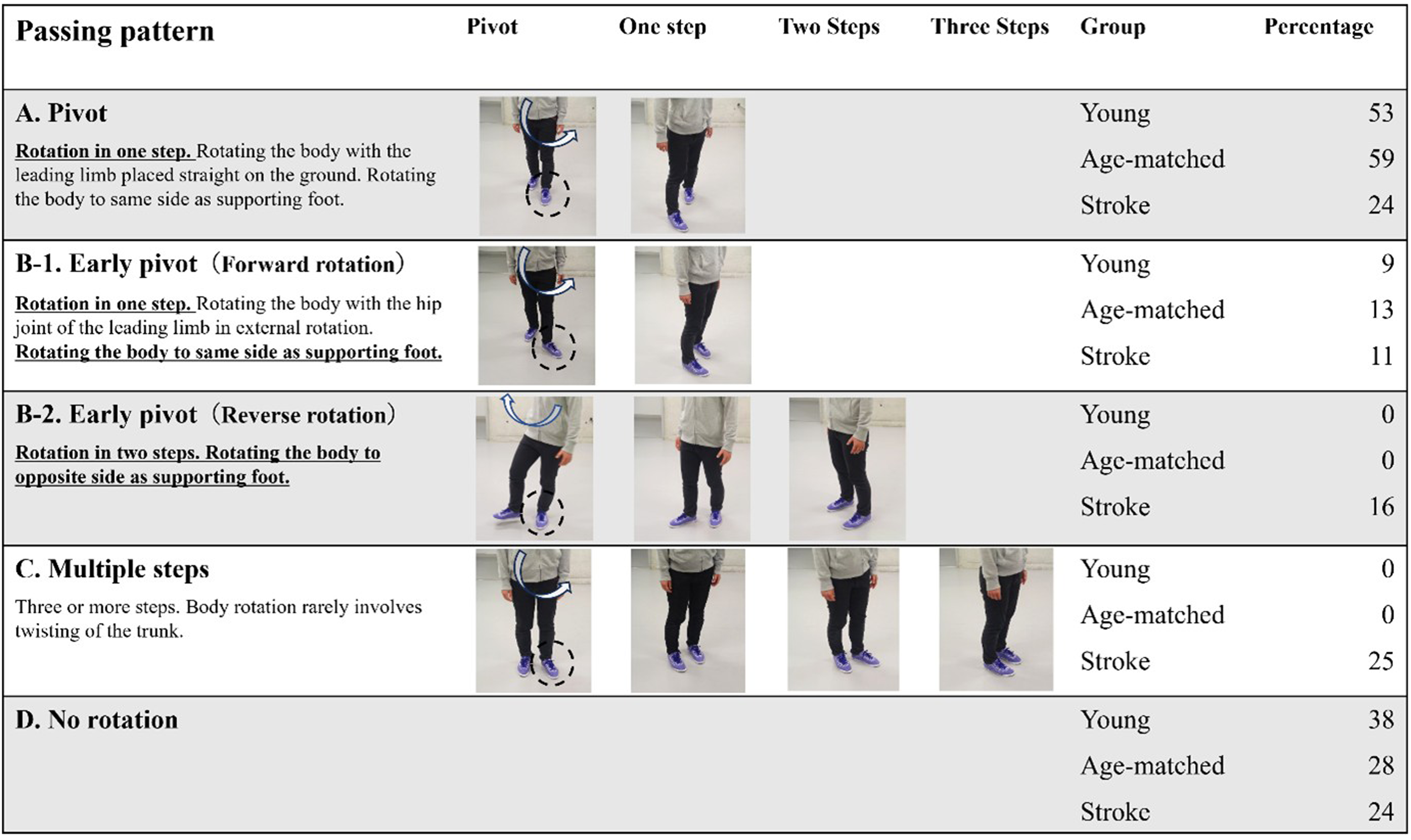
Passing patterns and selection ratio for each group.
Statistical Analyses
Pattern frequency for each opening width and rotation directions were compared using χ2 tests. The consistency of passing patterns across the three repeated trials within each opening-width condition was evaluated using repeated-measures analysis of variance. The primary analyses focused on the stroke-specific patterns (Patterns B-2 and C). Associations between pattern occurrence and clinical or environmental factors were examined using binomial GLMMs with a logit link. The unit of analysis was each trial, and participant-specific random intercepts were included to account for repeated observations within participants. Fixed effects included opening width, lower-limb BRS, TUG performance, fall history, and minimum passable width. Multicollinearity among the fixed-effect predictors was assessed using variance inflation factors (VIFs) before model fitting. Based on these assessments, all predefined predictors were retained in the GLMMs. The TUG test was entered into the models in seconds; therefore, odds ratios (ORs) represent the change in odds associated with each 1-s increase in TUG time. Opening width and minimum passable width were coded in 0.1 shoulder-width increments; therefore, ORs represent the change in odds associated with each 0.1 increase in relative width. Two of 345 stroke-group trials were excluded because incomplete video recordings prevented reliable classification. No imputation was performed. The marginal and conditional R2 values for the GLMMs were calculated as previously described (Nakagawa & Schielzeth, 2013). Statistical significance was set at p < .05. All analyses were performed using SPSS version 28.0 (Armonk, NY: IBM Corp) and R.
Results
Twenty-three patients with stroke, 23 healthy, age-matched participants, and 12 healthy, young participants participated. The stroke and age-matched groups partially overlapped with those reported in the previous study (Muroi et al., 2017); however, the present study addressed a different research question by conducting a novel video-based classification analysis focusing on the relationship between supporting foot selection and trunk rotation direction during passage through a narrow-opening. Moreover, data from 12 healthy young participants, which were not included in the previous report, were analyzed to further clarify stroke-specific and age-related behavioral characteristics (Table 1). Collisions between assistive devices and the opening frame were rare, occurring in only 2 out of 30 trials resulting in a collision.
The three physical therapists classified the opening passing patterns into five types (Fig. 2). Before introducing the abbreviated labels (A, B-1, B-2, C, and D), the movement characteristics of each passing pattern were defined based on the supporting foot, direction of trunk rotation, and number of steps required to complete the turn. Pattern A (“pivot”) involved a single-step rotation toward the same side as the supporting foot. Pattern B-1 (“early pivot–forward rotation”) described a one-step rotation performed with the leading limb placed in external rotation to facilitate trunk rotation toward the supporting foot side. Pattern B-2 (“early pivot–reverse rotation”) involved a two-step sequence in which the trunk rotated toward the opposite side of the supporting foot. Pattern C (“multiple steps”) consisted of three or more steps with minimal twisting of the trunk. Pattern D (“no-rotation”) represented a strategy in which participants passed through the opening without rotating their trunk. The concept of “early pivot” used in Patterns B-1 and B-2 was adapted from the turning-strategy classification described by Thigpen et al. (2000) and operationally applied to narrow-opening passage tasks in the present study. The agreement rate was high (inter-rater reliability = .76). The young and age-matched participants only had patterns where they either pivoted to the same side as their supporting foot or did not rotate at all. Patterns B-2 and C were exclusively observed in the stroke group (Fisher's exact test, both p < .001).
Among participants with stroke, body rotation was observed in 215 trials, of which 172 (80.0%) involved rotation around the lower limb on the non-paretic side. The proportions of rotation using the non-paretic side as the axis in each pattern were as follows: A (35 of 62 trials, 56.5%), B-1 (46 of 52 trials, 88.5%), B-2 (43 of 44 trials, 97.7%), and C (48 of 57 trials, 84.2%).
Passing patterns were generally consistent across the three repeated trials within each opening-width condition. Overall, the same passing pattern was observed in all three trials in 79.42% of the opening-width conditions. The consistency ratio was lowest at a width of 1.0 times shoulder width; however, differences across opening widths did not reach statistical significance (F(4, 88) = 2.35, p = .06). The descriptive statistics (mean [standard deviation]) for the consistency ratio across widths were as follows: 0.9 (.86 [.24]), 1.0 (.71 [.18]), 1.1 (.74 [.25]), 1.2 (.80 [.24]), and 1.3 (.87 [.17]).
In contrast, movement patterns varied across opening-width conditions. Each participant exhibited at least three different passing patterns across the five opening widths, demonstrating that pattern selection was not fixed across conditions. Only four of the 23 participants with stroke demonstrated patterns similar to those observed in the healthy controls (A, B-1, and D). For the other participants with stroke, patterns B-2 and C were observed; hence, although the patterns were consistent within individuals, they varied significantly among individuals. The post-hoc exact power for detecting this group-level difference was greater than 99.9%.
Figure 3 shows the frequencies of the passing patterns for each opening condition. The results confirmed that the frequency of passing patterns differed depending on the opening width (χ2(16): 175.27; p < .001).
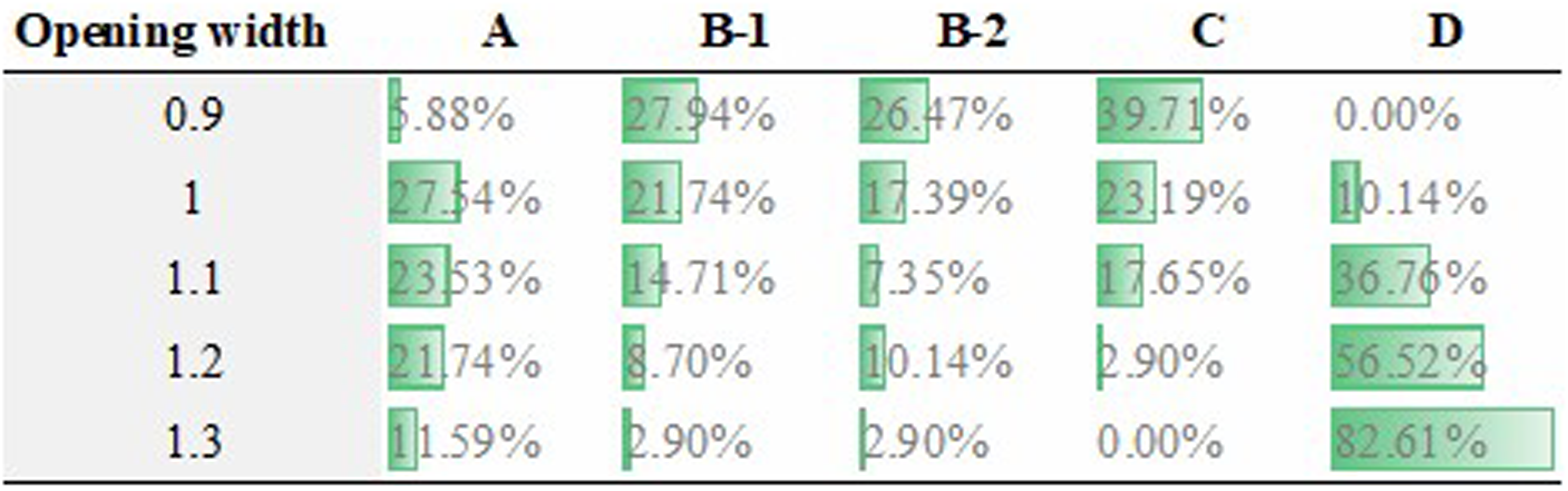
Passing pattern for each opening width in individuals with stroke.
Figure 4 shows the frequencies of rotation patterns for each participant. Preferred rotation patterns differed significantly among participants (χ2(110): 336.96, p < .001).
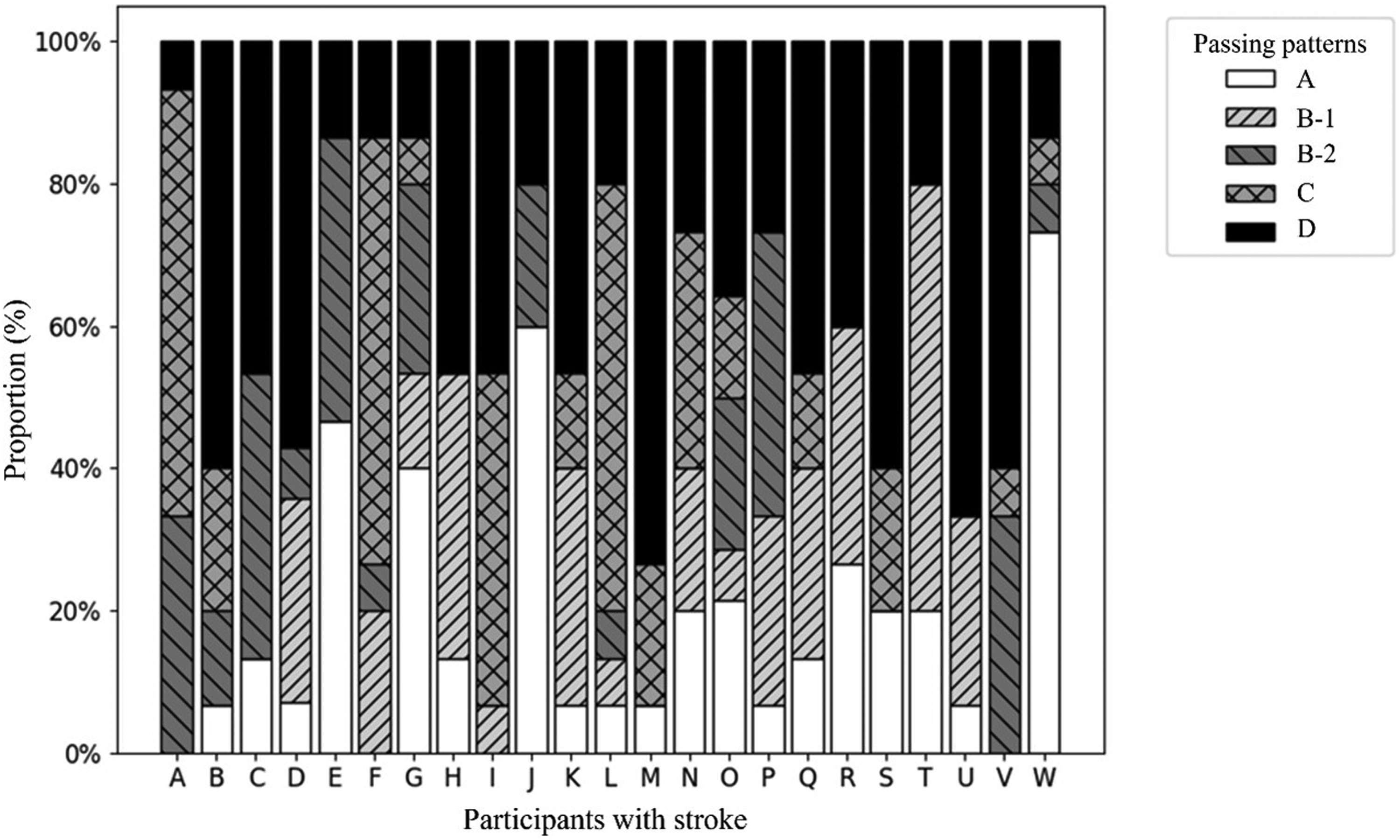
Passing pattern of each participant with stroke.
All VIF values were below 1.89, indicating no substantial multicollinearity among the predictors. Table 2 presents the results of the GLMM analysis for passing pattern B-2. Opening width was the only significant predictor (OR: .52, 95% confidence interval [CI]: .39–.70, p < .001). Table 3 presents the GLMM results for pattern C. Opening width was a significant predictor (OR: .18, 95% CI: .11–.32, p < .001), whereas the TUG performance did not reach statistical significance (OR: 1.22, 95% CI: .99–1.49, p = .056). The simulation-based post-hoc power analysis for the primary GLMMs showed that the estimated power was 99.1% for the opening-width effect on Pattern B-2 and 100.0% for the opening-width effect on Pattern C. In contrast, the estimated power for the observed TUG effect on Pattern C was 52.7%. Hence, post-hoc power was high for the opening-width effects but lower for the observed TUG effect.
Binomial GLMM for Pattern B-2.
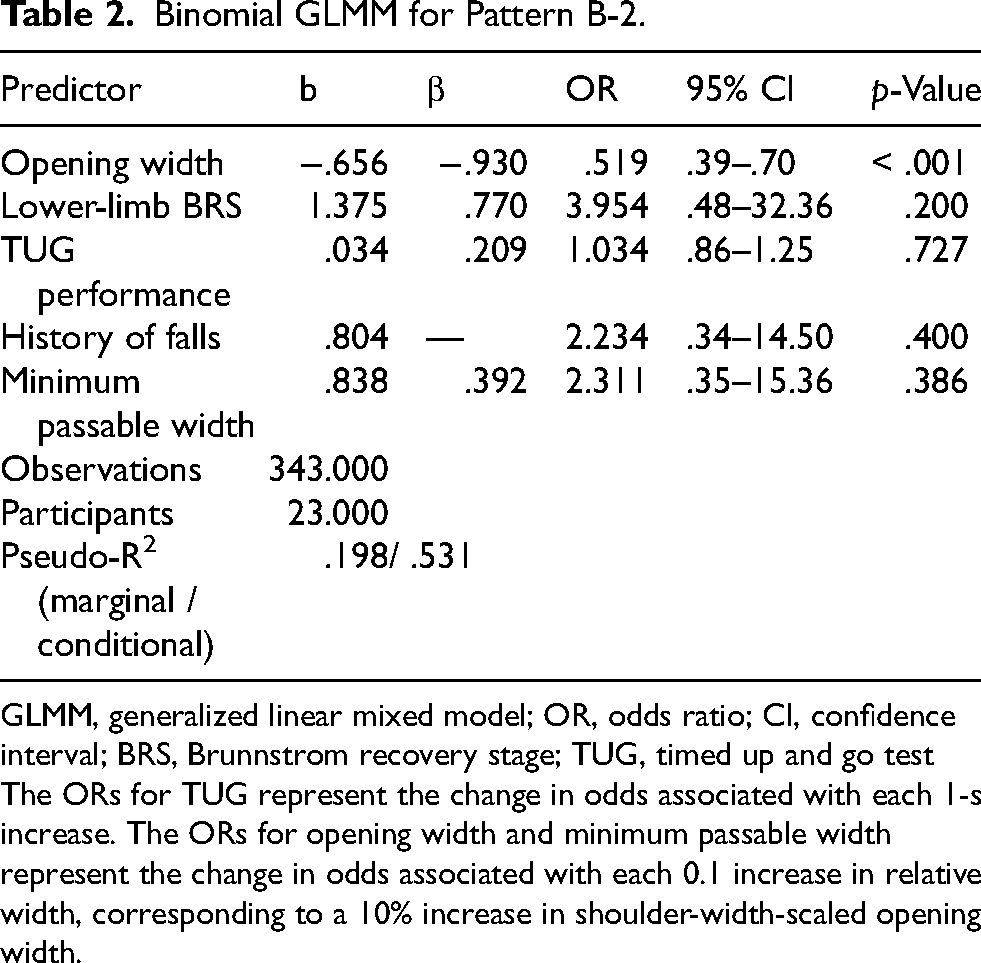
GLMM, generalized linear mixed model; OR, odds ratio; CI, confidence interval; BRS, Brunnstrom recovery stage; TUG, timed up and go test
The ORs for TUG represent the change in odds associated with each 1-s increase. The ORs for opening width and minimum passable width represent the change in odds associated with each 0.1 increase in relative width, corresponding to a 10% increase in shoulder-width-scaled opening width.
Binomial GLMM for Pattern C.
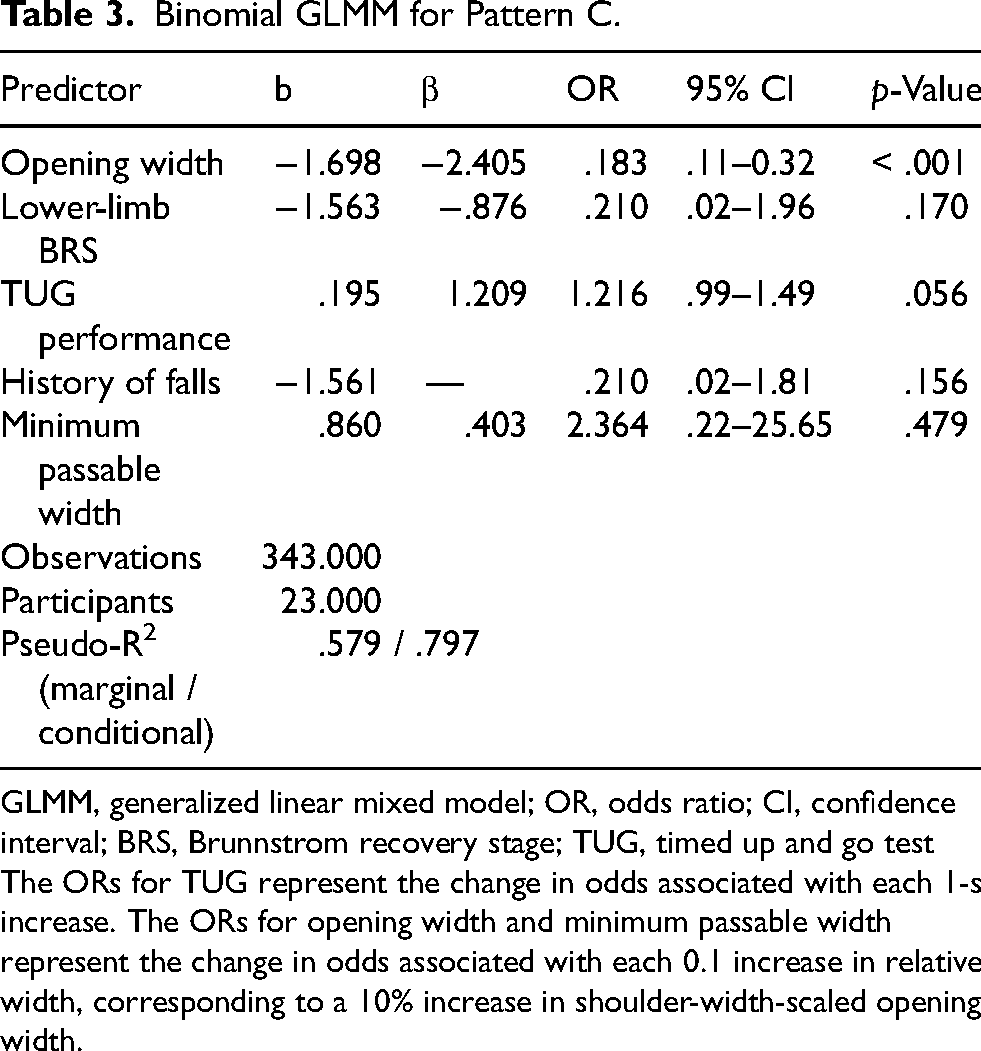
GLMM, generalized linear mixed model; OR, odds ratio; CI, confidence interval; BRS, Brunnstrom recovery stage; TUG, timed up and go test
The ORs for TUG represent the change in odds associated with each 1-s increase. The ORs for opening width and minimum passable width represent the change in odds associated with each 0.1 increase in relative width, corresponding to a 10% increase in shoulder-width-scaled opening width.
Discussion
Distinct movement patterns were observed during passage through a narrow-opening in individuals with stroke. Five movement patterns were identified based on the supporting foot, rotation direction, and number of steps taken. The pivot pattern (A), characterized by trunk rotation toward the same side as the leading foot, was most frequently observed in healthy young participants and age-matched controls. In contrast, when the opening width exceeded shoulder width, healthy participants predominantly selected pattern D (no-rotation). This finding is consistent with previous evidence that efficient gait and more normal trunk rotation are associated with smoother locomotor performance (Van Criekinge et al., 2017). Age-matched controls showed a lower occurrence rate of pattern D than younger participants, possibly because older adults initiate body rotation at wider openings (Hackney & Cinelli, 2011). Stroke-specific movement patterns were also identified. Pattern B-2, wherein the trunk was rotated to the opposite side of the supporting foot, was only observed in participants with stroke. Moreover, multiple-step pattern C was frequently observed under narrower opening conditions, particularly at the 0.9 times shoulder-width condition. Unlike findings from previous studies of older adult participants that reported multiple-step strategies for 180° turns (Thigpen et al., 2000), the age-matched controls in this study rarely demonstrated such behavior, likely because the required trunk rotation was smaller in this task. Participants with stroke appeared to have difficulty performing pivot-like movements that require ipsilateral rotation around the supporting foot, even under relatively mild spatial constraints. Rotation was predominantly performed around the non-paretic limb (80% of trials), suggesting that participants preferentially selected the more functional limb as a pivot to enhance stability. This tendency may reflect an adaptive choice to avoid loading the paretic limb during rotational control. Although the relationship between pivot limb selection and fall history was not directly examined, individuals with stroke may avoid using the paretic limb as a pivot due to perceived instability. Future studies should investigate whether pivot limb selection is associated with fall risk and balance confidence in individuals with stroke.
Patterns B-2 and C appeared to reflect compensatory strategies adopted under spatial constraints. Although impaired perceptual judgment can contribute to abnormal movement behaviors (Martens & Almeida, 2012), participants in this study showed passability judgments comparable to those of age-matched controls in previous work (Muroi et al., 2017). Therefore, the stroke-specific movement patterns observed here are more likely related to physical constraints, such as impaired motor control and reduced stability, rather than distorted perception of body size or space. Pattern B-2 was characterized by trunk rotation toward the side opposite the supporting foot and was observed almost exclusively when the non-paretic limb served as the pivot. This may reflect a strategy to minimize demands on the paretic limb while maintaining stability, partly through a wider base of support created by bilateral hip external rotation. Given that individuals with stroke tend to overuse the non-paretic side because of reduced motor function on the paretic side (Taub et al., 2006), this pattern can be interpreted as an adaptive use of the more functional limb. The association with opening width further suggests that pattern B-2 is strongly shaped by environmental constraints during passage. Pattern C, characterized by multiple steps, may represent a more stable strategy for controlling the center of mass during movement. Multiple step turns can facilitate moving the center of mass by re-orienting the foot (Fuller et al., 2007); and may reduce sudden loading or rotational demands on the paretic limb when it is used as the supporting foot. In the present study, narrower openings were associated with greater use of pattern C. Although TUG performance was included in the model, its association with pattern C did not reach statistical significance. Therefore, the present findings primarily support the influence of environmental constraints on the selection of this strategy. From a clinical perspective, patterns B-2 and C may reflect different levels of compensatory adaptations. Pattern B-2 may indicate relatively preserved mobility with strategic use of the non-paretic limb, whereas pattern C may reflect greater reliance on cautious balance-control strategies. These findings suggest that narrow-opening passage tasks may be useful for identifying how mobility limitations and stability demands shape movement adaptations in individuals with stroke.
From a clinical perspective, patterns B-2 and C may reflect different functional adaptations in individuals with stroke. Pattern B-2 can be interpreted as an active compensatory strategy that preferentially uses the non-paretic limb as the axis of rotation to maintain stability while preserving movement efficiency. In contrast, pattern C appears to represent a more conservative strategy characterized by multiple steps and reduced dynamic demands, likely adopted when balance or motor control is limited. These differences may help clinicians interpret how patients adapt to spatial constraints during walking. Predominant use of pattern B-2 may indicate difficulty with paretic-side stance control, whereas reliance on pattern C may reflect dependence on cautious balance-control strategies. Moreover, although the association between pattern C selection and TUG performance did not reach statistical significance, the observed effect may warrant further investigation in a larger sample. These findings also suggest that narrow-opening passage tasks may be useful for assessing adaptive locomotor behavior in environments that resemble everyday situations. Because opening width strongly influenced movement pattern selection, environmental constraints may play an important role in shaping compensatory behaviors after stroke. Therefore, in addition to addressing patient-specific impairments, modifying environmental conditions and practicing movement in constrained spaces may be relevant components of rehabilitation. Further studies are needed to determine whether changes in these movement patterns are associated with improved functional mobility and reduced fall risk.
This study has a few limitations. First, this exploratory single-center study included a relatively small and clinically heterogeneous sample recruited using convenience sampling, which may limit generalizability to other stroke populations or rehabilitation settings. Although post-hoc analyses suggested sufficient power to detect the observed effects of opening width, power was more limited for participant-level clinical predictors, such as TUG performance, lower-limb motor impairment, and fall history. Therefore, nonsignificant findings for these variables should be interpreted with caution. Second, movement patterns were classified using standard video recordings rather than 3D motion analysis. Although inter-rater reliability was substantial, some degree of subjective judgment and classification bias cannot be excluded. Future studies using quantitative biomechanical analyses are warranted to further validate these findings. Third, participants were allowed to use their usual assistive devices during testing for safety reasons, and the potential influence of assistive devices on movement pattern selection remains unclear. Fourth, individuals with unilateral spatial neglect were excluded; therefore, the findings may not be generalizable to stroke populations with significant perceptual or attentional impairments. Fifth, the instruction to avoid trunk rotation during the minimum passable width assessment may have influenced natural gait behavior and movement pattern selection. Finally, several experimental procedures, including the absence of TUG familiarization trials and the use of static shoulder-width measurements, may have introduced additional variability into the assessments.
Conclusions
This study classified the movement patterns used to pass through narrow openings by considering the supporting foot, trunk rotation direction, and number of steps. Individuals with stroke demonstrated two characteristic patterns not commonly observed in controls: (1) a pattern involving rotation of the trunk toward the paretic side while supporting the body with the non-paretic foot, and (2) a multi-step strategy requiring additional steps after the first shoulder had passed through the opening. Narrower opening widths increased the likelihood of adopting the multi-step strategy, indicating that environmental constraints play an important role in movement pattern selection. Although the association between TUG performance and the multi-step strategy did not reach statistical significance, mobility level may still be relevant to movement adaptation under spatial constraints. Given that the TUG test is widely used in clinical practice, future studies should further examine its relationship with movement strategy selection in constrained environments. Clinically, these movement patterns may help identify whether patients rely on relatively efficient or conservative compensatory strategies and may support rehabilitation planning aimed at improving safe mobility in narrow spaces.
Supplemental Material
sj-docx-1-nre-10.1177_10538135261464177 - Supplemental material for Stroke-specific Movement Patterns During Passage Through a Narrow-Opening: A Cross-Sectional Study
Supplemental material, sj-docx-1-nre-10.1177_10538135261464177 for Stroke-specific Movement Patterns During Passage Through a Narrow-Opening: A Cross-Sectional Study by Daisuke Muroi, Hiroshi Matsui, Takayuki Tomono, Juntaro Sakazaki, Yutaro Saito, Aki Nakazawa, Kentaro Kodama and Takahiro Higuchi in NeuroRehabilitation
Supplemental Material
sj-docx-2-nre-10.1177_10538135261464177 - Supplemental material for Stroke-specific Movement Patterns During Passage Through a Narrow-Opening: A Cross-Sectional Study
Supplemental material, sj-docx-2-nre-10.1177_10538135261464177 for Stroke-specific Movement Patterns During Passage Through a Narrow-Opening: A Cross-Sectional Study by Daisuke Muroi, Hiroshi Matsui, Takayuki Tomono, Juntaro Sakazaki, Yutaro Saito, Aki Nakazawa, Kentaro Kodama and Takahiro Higuchi in NeuroRehabilitation
Footnotes
Acknowledgments
Ethical Considerations
Approval was obtained from the ethics committee of Kameda Medical Center, Chiba, Japan (approval number: 12-089-150501). The procedures used in this study adhere to the tenets of the Declaration of Helsinki.
Consent to Participate
All participants who agreed to take part in the study received both oral and written information about its purpose and procedures. They provided written informed consent prior to participation. Consent to publish anonymized data was obtained from all participants.
Author Contributions
Conceptualization: DM, TH; Data curation: DM, YS, AK; Formal analysis: DM, HM, TT, JS, YS, AK, KK; Funding acquisition: DM; Investigation: DM, YS, AK; Methodology: DM, HM, TH; Project administration: DM; Resources: DM, TH; Software: DM, HM, TH; Visualization: DM, HM, TT, JS, KK; Writing – original draft: DM, HM; Writing – review & editing: DM, HM, TT, JS, KK, TH.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Society for the Promotion of Science (KAKENHI) (Grant numbers [23K16546 and 26K14074]). The funders had no role in the design, conduct, or reporting of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Study Registration
R000064253 UMIN000056244
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.