
Abstract
Background
In post-acute stroke rehabilitation, cognitive assessment is clinically important but frequently incomplete. Complete-case analysis excludes much of the sample, reducing representativeness.
Objectives
To determine whether incomplete routine post-stroke cognitive assessments can still yield clinically interpretable relationships among cognitive, clinical, and contextual variables, and support group-level stratification using a reduced feasible cognitive set.
Methods
Retrospective cohort study of adults admitted to post-acute stroke neuro-rehabilitation between 2007 and 2026 with at least one neuropsychological assessment. The baseline cohort included 2654 patients, with 5417 assessments within 6 months available for confirmatory analysis. The 24-subtest baseline battery showed 37.5% to 88.4% missingness. Five representative cognitive measures were selected based on data availability, domain coverage, and within-domain Spearman correlations. Bayesian networks were fitted in the baseline cohort, their stability was assessed by bootstrapping, key dependencies were examined across all available assessments.
Results
Stable, bootstrap-supported dependency patterns were recovered and broadly replicated in the confirmatory analysis. Replicated associations linked age and time since injury to verbal learning and naming; stroke subtype to verbal learning, timed orientation/performance, and phonemic fluency. Verbal learning occupied a central position, with additional replicated links to naming, timed orientation/performance, and attentional span. Among the contextual variables, economic status was the only one showing a direct link to a cognitive measure (attentional span). Group-level stratification of verbal learning showed moderate performance (R2 = 0.42).
Conclusions
Incomplete routine cognitive assessments need not rely on complete-case restriction or score imputation; they can still support clinically meaningful interpretation and group-level stratification in post-acute stroke rehabilitation.
Keywords
Introduction
Post-stroke cognitive impairment (PSCI) is frequent, affecting approximately half of stroke survivors within the first six months after stroke, and recent evidence suggests that this prevalence may be underestimated (El Husseini et al., 2023; Godefroy et al., 2025). PSCI is clinically important because it is associated with greater disability, institutionalization, stroke recurrence, and mortality, and current guidelines emphasize early identification and appropriate neuropsychological evaluation (Godefroy et al., 2025).
In practice, however, cognitive assessment data after stroke are often incomplete. Patients may be unable to complete testing because of severe morbidity, aphasia, visual deficits, fatigue, difficulties attending assessments, loss to follow-up, or refusal, and these reasons are often heterogeneous and incompletely reported (Sujanthan et al., 2025a, 2025b). Because these factors are closely linked to stroke severity and patient characteristics, missing cognitive data are unlikely to be random. In addition, patients with communication deficits, particularly aphasia, are frequently excluded or underrepresented, further contributing to systematic gaps in post-stroke cognitive datasets (Shiggins et al., 2024).
These challenges have important methodological consequences. Restricting analyses to patients with complete cognitive batteries can substantially reduce the usable sample and may preferentially exclude more impaired patients, thereby introducing selection bias (Little & Rubin, 2019; Sterne et al., 2009). In addition, analyzing individual cognitive tests in isolation overlooks the fact that post-stroke cognitive impairment is multidomain, with overlapping deficits across cognitive functions rather than fully independent impairments (Demeyere et al., 2015; Kelleher et al., 2026; Phillips et al., 2024).
Because missing cognitive data can severely limit complete-case analyses, methods that make use of partially observed assessments may help recover clinically relevant relationships that would otherwise be missed (Ameur et al., 2023). Rather than treating each test in isolation, such approaches can characterize the pattern of relationships among cognitive measures and clinical variables, showing whether some tests capture broader aspects of post-stroke cognitive vulnerability while others reflect more specific or context-dependent influences (O'Donoghue et al., 2022). Such an approach may also support clinically meaningful stratification, by estimating expected cognitive performance across combinations of age, stroke subtype, and time since injury rather than considering these factors one at a time (Aam et al., 2020; Gallucci et al., 2024).
To address these issues, we applied a Bayesian network approach, a probabilistic graphical modelling framework that can represent conditional dependencies among variables and support inference under uncertainty, to a real-world cohort of post-acute stroke neuropsychological assessments collected in a neuro-rehabilitation setting (Scutari & Denis, 2021). Although Bayesian networks have previously been applied in stroke research, these studies have mainly focused on outcome prediction, complication or risk profiling, and forecasting cognitive decline. We first estimated the network using the baseline assessment of each patient and then evaluated the replication of key dependencies across all available assessments. Focusing on representative cognitive tests with broad domain coverage and higher data availability, our aim was to characterize the pattern of relationships among cognitive measures and clinical variables, and to derive clinically interpretable stratification of cognitive performance.
We hypothesized that the main dependency pattern identified in the network derived from each patient's baseline assessment would be replicated when the analysis was extended to all available assessments. In addition, we hypothesized that, among the selected cognitive measures, at least one test would occupy a central position within the network, showing direct relationships with both sociodemographic and clinical characteristics and with other cognitive domains. Identifying such a centrally connected measure could help distinguish tests with broader cross-domain relevance from those reflecting more specific deficits, and could provide clinically useful information for interpreting performance patterns within incomplete post-acute stroke assessment data.
Methods
Study Design
We conducted a retrospective observational cohort study using routinely collected clinical data from inpatients admitted for neuro-rehabilitation at Institut Guttmann hospital, Badalona, Spain. The study was reported in accordance with the STROBE statement for observational research (Vandenbroucke et al., 2007). Data were extracted from routine clinical assessments performed as part of standard care.
Participants and Setting
Eligible participants were adults (≥18 years) admitted to the post-acute neuro-rehabilitation program at Institut Guttmann hospital, Badalona, Spain, within 6 months of a first-ever ischemic or hemorrhagic stroke between 2007 and 2026, who underwent at least one neuropsychological assessment during admission. Individual assessments could be partially incomplete, but patients were required to have at least one recorded cognitive evaluation to enter the analytic sample. The facility comprises 152 inpatient beds across four specialized units staffed by multidisciplinary teams. Exclusion criteria were severe pre-stroke multi-impairment, stroke in the context of another neurological condition, and transfer to an acute care facility after admission to inpatient rehabilitation.
Clinical Included Variables
Demographic and clinical variables included sex, age, stroke subtype (ischemic or hemorrhagic), and time since injury (TSI), defined as the number of days between stroke onset and neuropsychological assessment.
The cognitive battery comprised 24 subtests covering orientation, attention, working memory, executive function, language, memory, and visuospatial abilities (Table 1). Measures were drawn from the Barcelona Test (Peña-Casanova et al., 1991), Wechsler Adult Intelligence Scale-III (Wechsler, 1997), Trail Making Test part A (Reitan & Wolfson, 1985) and part B (Periáñez et al., 2007), the Stroop test (Stroop, 1935), Rey Auditory Verbal Learning Test (Schmid, 1996), Wisconsin Card Sorting Test (Heaton & Staff, 1993), and PMR (Artiola i Fortuny et al., 1999). Table 1 summarizes each test, the cognitive domain assessed, the identifier used in the analyses, and baseline missing data.
Baseline Cognitive Assessments, Domains, and Missing Data in the Study Cohort (N = 2654).
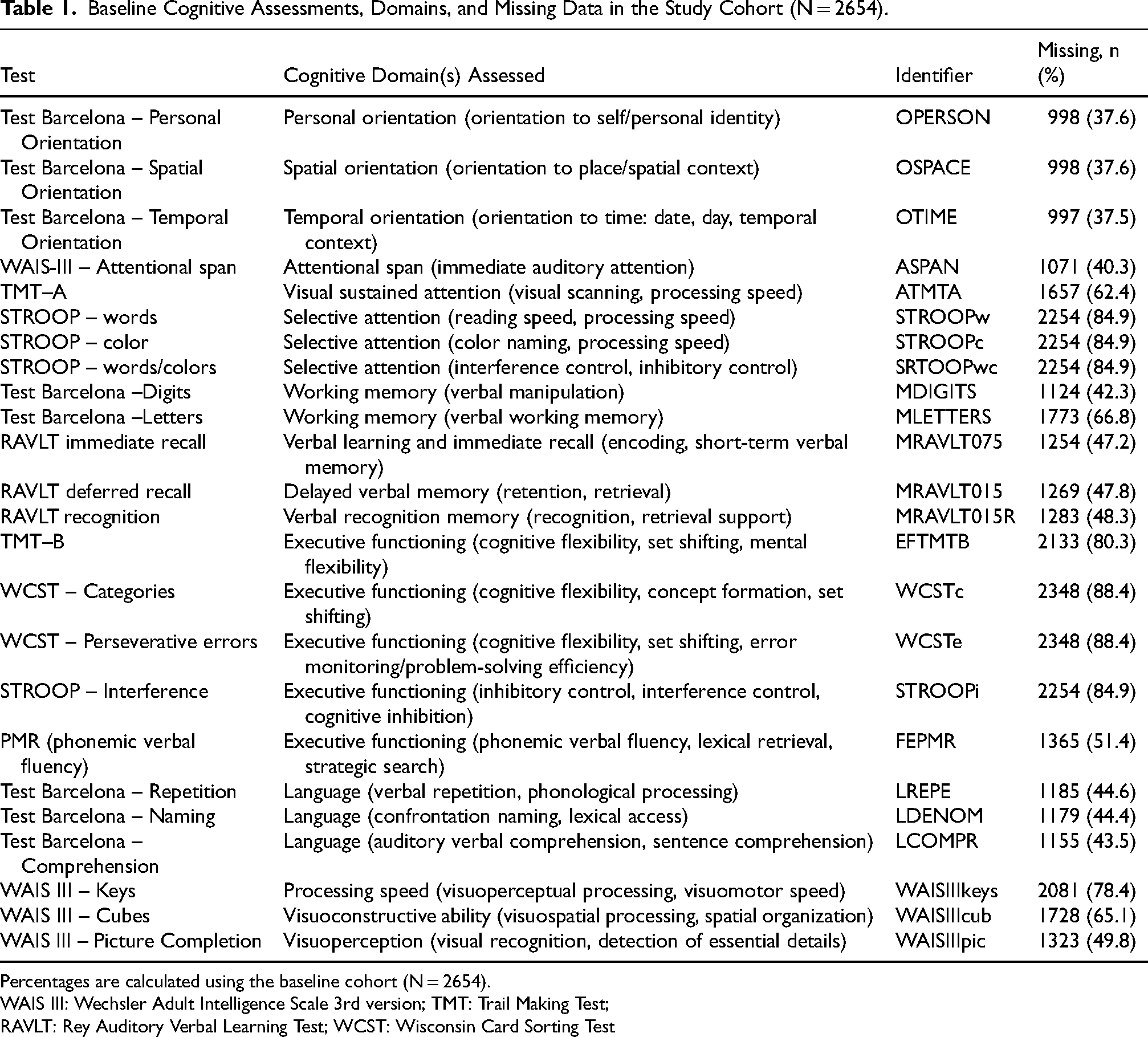
Percentages are calculated using the baseline cohort (N = 2654).
WAIS III: Wechsler Adult Intelligence Scale 3rd version; TMT: Trail Making Test;
RAVLT: Rey Auditory Verbal Learning Test; WCST: Wisconsin Card Sorting Test
Cognitive data completeness was considered at three levels. First, at the level of the full baseline battery, restricting the analysis to patients with complete data across all 24 cognitive subtests would have reduced the analytic sample from 2654 to 125 patients, excluding 95.3% of the baseline cohort.
Second, at the level of individual tests, missingness varied substantially across the baseline battery, ranging from 37.5% to 88.4% (Table 1). The lowest missingness was observed for the Barcelona temporal orientation subtest (OTIME; 37.5%), whereas the highest was observed for WCST-derived measures (88.4%). High missingness was also present in Stroop variables (84.9%) and Trail Making Test part B (80.3%).
Third, at the level of variable selection, five representative cognitive measures were retained for network analysis according to two criteria: comparatively higher data availability at baseline and coverage of distinct cognitive domains. The selected measures were OTIME, ASPAN, MRAVLT075, FEPMR, and LDENOM, which together provided a clinically heterogeneous but analytically feasible subset of the baseline battery (McMahon et al., 2022). Selection was additionally supported by within-domain correlations among conceptually similar tests, which suggested substantial overlap in some domains and more partial overlap in others (Supplementary Figures S1–S5).
Additional contextual variables related to living situation, economic status, and home environment were included in the network analysis. These variables were obtained at baseline through a structured social work interview conducted with the patient and core family, had no missing data, and are described in Supplementary Table S1.
Statistical Analyses
Bayesian networks were used to characterize relationships among demographic, clinical, contextual, and cognitive variables in post-acute stroke. Analyses were performed in R using the bnlearn package (Scutari, 2017). A reduced set of variables was selected a priori from the baseline battery based on clinical relevance, representation of distinct cognitive domains, and comparatively higher data availability, including age, sex, stroke subtype, time since injury (TSI), living situation, economic status, home environment, and five representative cognitive measures (OTIME, ASPAN, MRAVLT075, FEPMR, and LDENOM). Two datasets were analyzed: a baseline dataset including the first available assessment for each patient within 6 months after stroke, and a confirmatory dataset including all available assessments within the same time window. Network structures were learned using a score-based hill-climbing algorithm within a conditional Gaussian framework (Lauritzen & Jensen, 2001) allowing joint modelling of continuous and categorical variables (Scutari & Denis, 2021). To improve interpretability and impose clinically plausible directions, a blacklist of forbidden arcs was specified: arcs from continuous to categorical variables were disallowed, and no incoming arcs were permitted to age, sex, stroke subtype, or TSI. Model parameters were estimated by maximum likelihood. Network stability was assessed by non-parametric bootstrap resampling (200 iterations), (Friedman et al., 1999). from which arc strength and directional probability were derived. Arcs with strength ≥0.70 and direction ≥0.85 in the baseline network were considered stable (Scutari & Denis, 2021), and their replication was then evaluated in the confirmatory analysis. Only bootstrap-supported associations replicated across both datasets were examined in detail, and model-based predictions were generated from the fitted baseline network for representative clinical profiles. Continuous variables were treated as numeric and categorical variables as factors.
To further characterize the local dependency structure of the baseline network, Markov blankets were derived for the five selected cognitive measures. The Markov blanket of a node comprises its parents, its children, and the other parents of its children, and therefore represents the minimal set of variables that renders that node conditionally independent of the rest of the network. In the present study, Markov blankets were used to identify which cognitive measures showed broader cross-variable connectivity and which appeared to reflect more specific or context-dependent patterns within the selected network (Scutari & Denis, 2021).
Results
A total of 2654 patients met the study eligibility criteria and contributed baseline data to the analysis. Table 2 summarizes the baseline characteristics of the full cohort and of the subset complete on the five selected cognitive measures. Restricting the analysis to patients with complete data on these five tests would have reduced the analytic sample to 1149 patients (43.3% of the baseline cohort). Although these comparisons are descriptive only, because the complete subset was nested within the full cohort, the complete 5-test subset showed very similar age, sex, and stroke subtype distributions, a somewhat shorter mean time since injury to assessment, and consistently higher mean scores across all five selected cognitive measures, indicating a more favorable cognitive profile than that of the full baseline cohort.
Baseline Characteristics of the Full Cohort and the Complete Subset for the Five Selected Cognitive Measures.
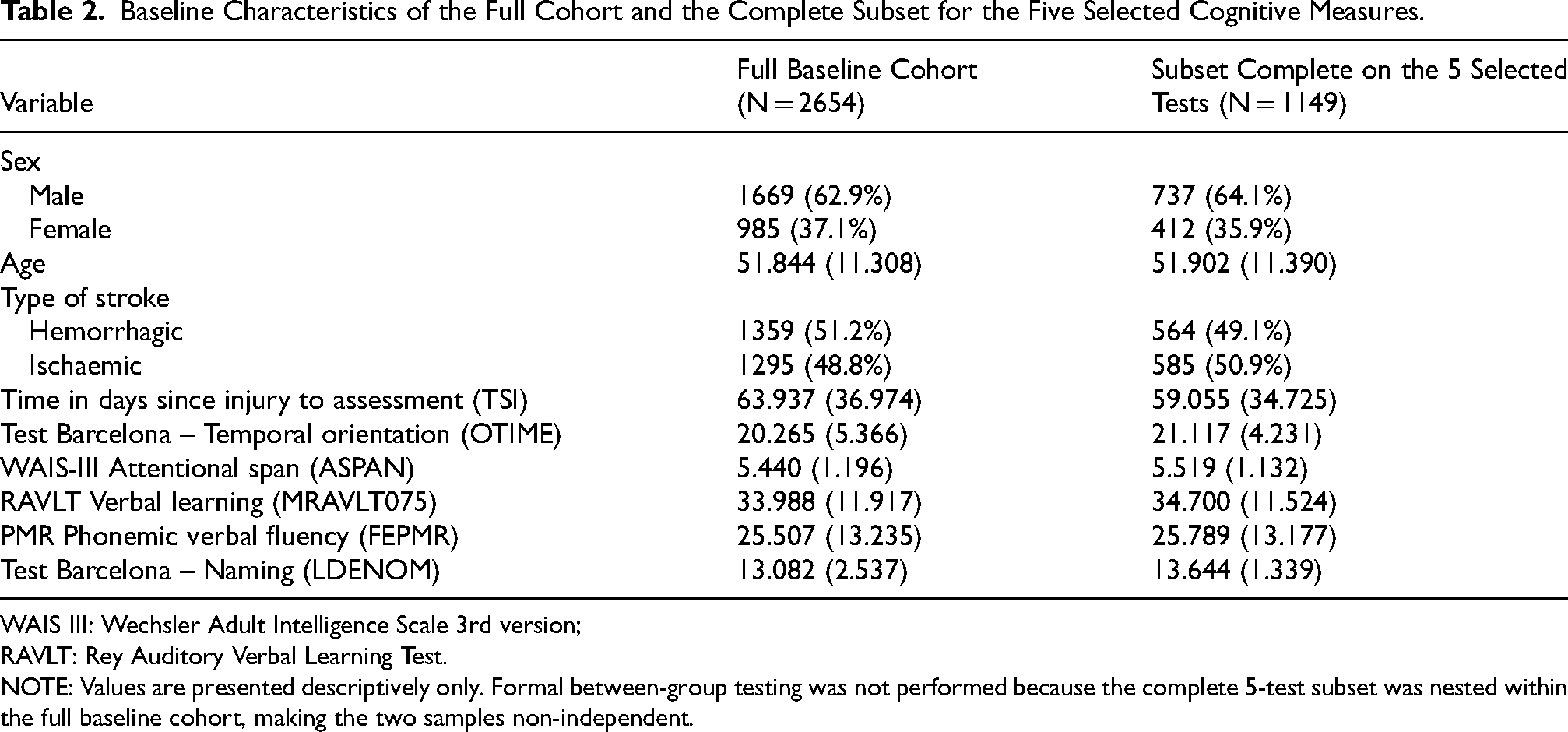
WAIS III: Wechsler Adult Intelligence Scale 3rd version;
RAVLT: Rey Auditory Verbal Learning Test.
NOTE: Values are presented descriptively only. Formal between-group testing was not performed because the complete 5-test subset was nested within the full baseline cohort, making the two samples non-independent.
Bayesian Network Structure at Baseline and Replication Across all Available Assessments
Figure 1 shows the bootstrap-supported Bayesian network identified in the baseline cohort. Among the cognitive measures, MRAVLT075 occupied the most connected position, showing direct relationships with age, stroke subtype, time since injury, and with three other cognitive measures (ASPAN, OTIME, and LDENOM). FEPMR showed a more restricted pattern, with a direct relationship to OTIME, whereas ASPAN and LDENOM appeared as more specific downstream cognitive nodes. Contextual variables were mainly linked to sex and stroke subtype, and economy showed an additional direct relationship with ASPAN. OTIME emerged as the main convergence point within the cognitive subnetwork, receiving direct links from stroke subtype, MRAVLT075, and FEPMR.
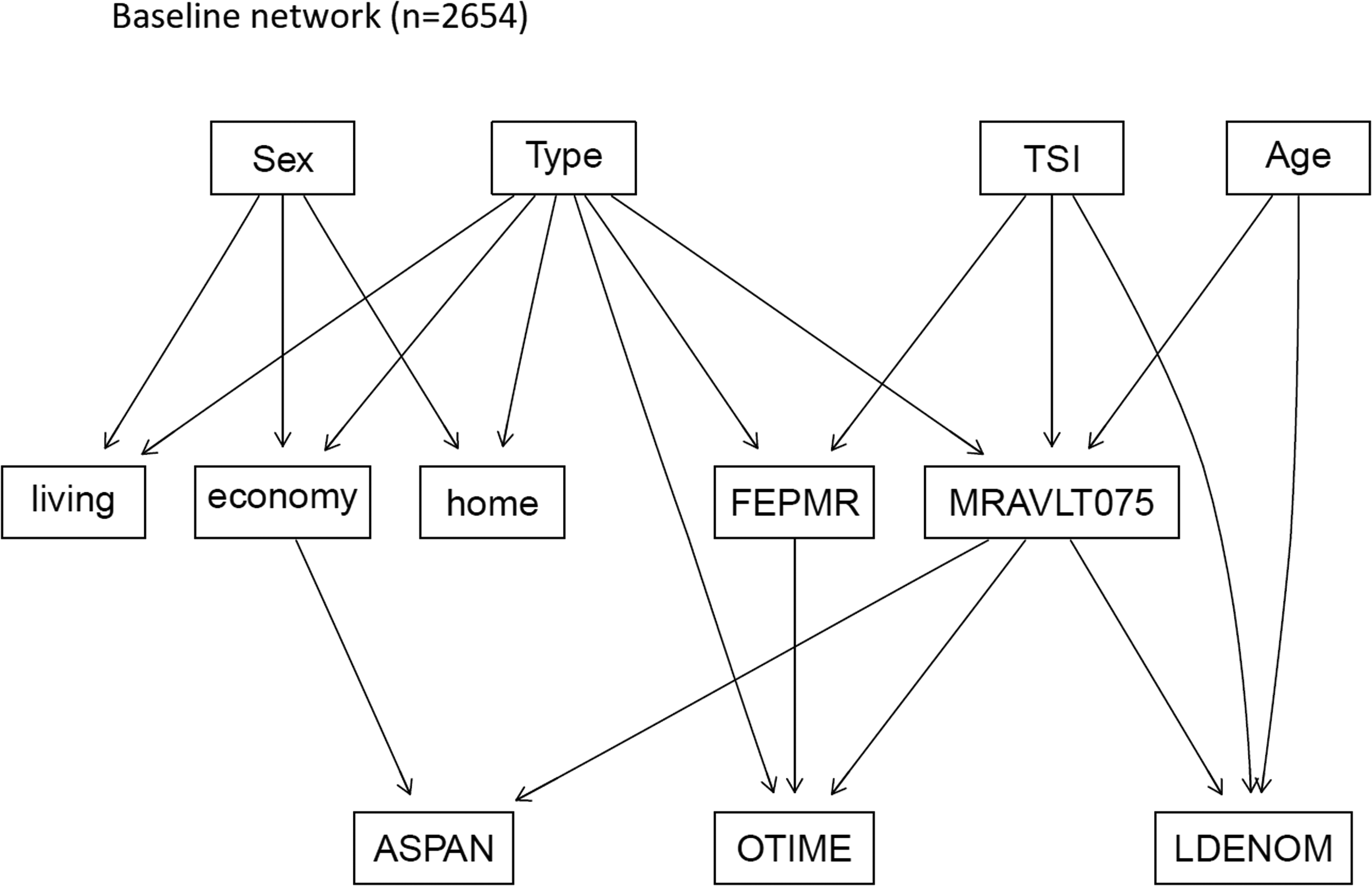
Baseline Bayesian network of selected cognitive, clinical, and contextual variables (N = 2654). Directed acyclic graph estimated from the first neuropsychological assessment of each patient within 6 months post-stroke.
Figure 2 shows the network estimated across all available assessments within 6 months post-stroke (n = 5417), which broadly replicated the baseline structure, confirming the central role of MRAVLT075 and the main cognitive and clinical dependencies identified in the primary analysis.
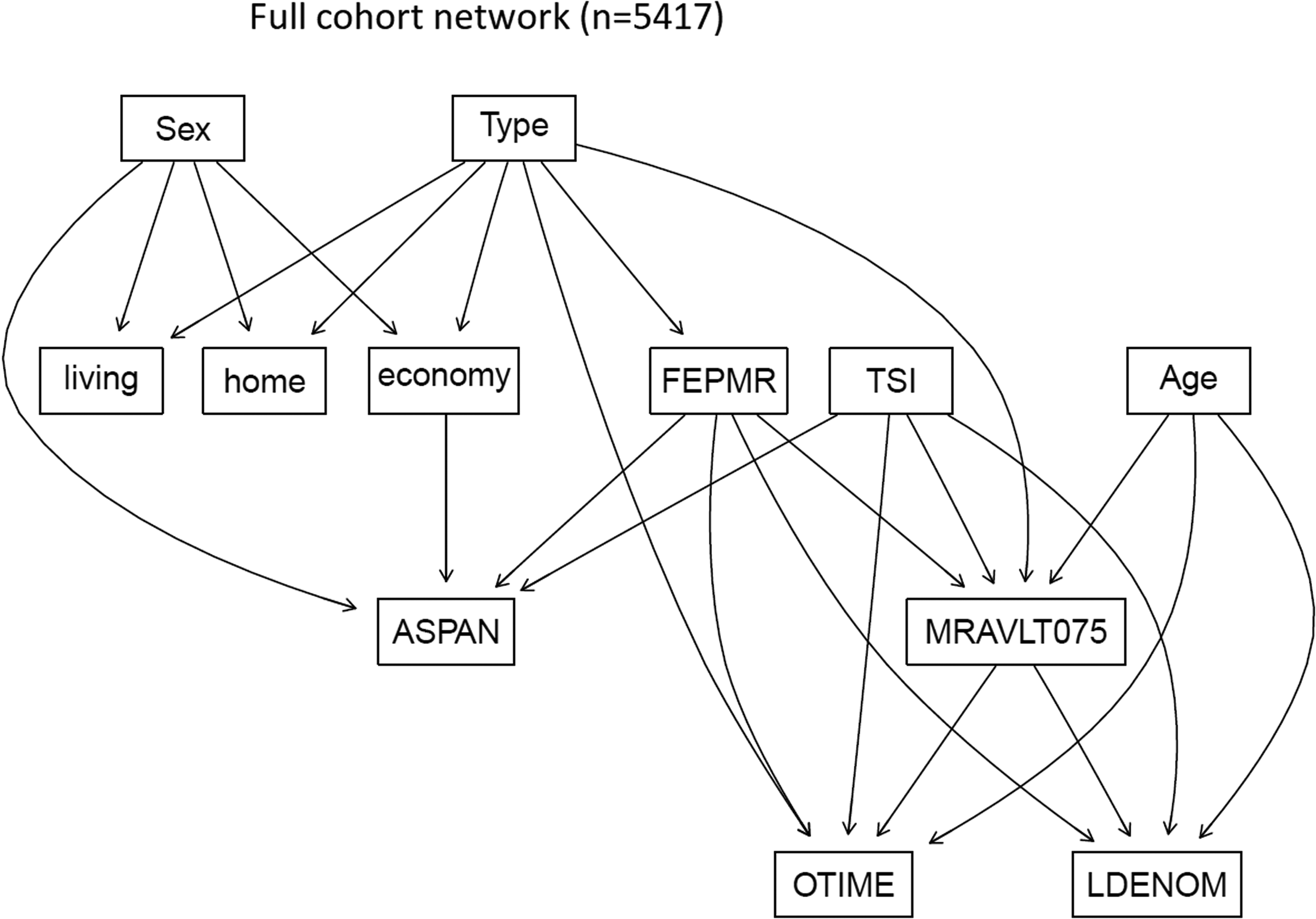
Confirmatory Bayesian network across all available assessments within 6 months post-stroke (N = 5417 assessments. The network was used to examine whether the main dependency pattern identified at baseline was reproduced when repeated assessments were included. Arcs shown correspond to bootstrap-supported dependencies meeting the predefined stability criteria (strength ≥ 0.70 and direction ≥ 0.85).
Replicated Bootstrap-Supported Dependencies and Model-Based Stratification
Table 3 summarizes the arcs that showed strong bootstrap support in the baseline network and were also recovered in the confirmatory network including all available assessments. Overall, the replicated structure showed a consistent pattern linking demographic, clinical, contextual, and cognitive variables. MRAVLT075 was the cognitive measure with the most prominent replicated links, receiving direct connections from age, stroke subtype, and time since injury, and showing additional replicated associations with OTIME and LDENOM. LDENOM also showed stable direct links with age and time since injury, whereas FEPMR and OTIME were each directly linked to stroke subtype. Among the contextual variables, economy showed a stable direct link with ASPAN. Replicated cognitive-to-cognitive arcs were observed between MRAVLT075 and LDENOM, MRAVLT075 and OTIME, and FEPMR and OTIME, supporting a non-random internal organization of the selected cognitive measures across both datasets.
Replicated Bootstrap-Supported Arcs in Baseline and Full-Cohort Bayesian Networks.
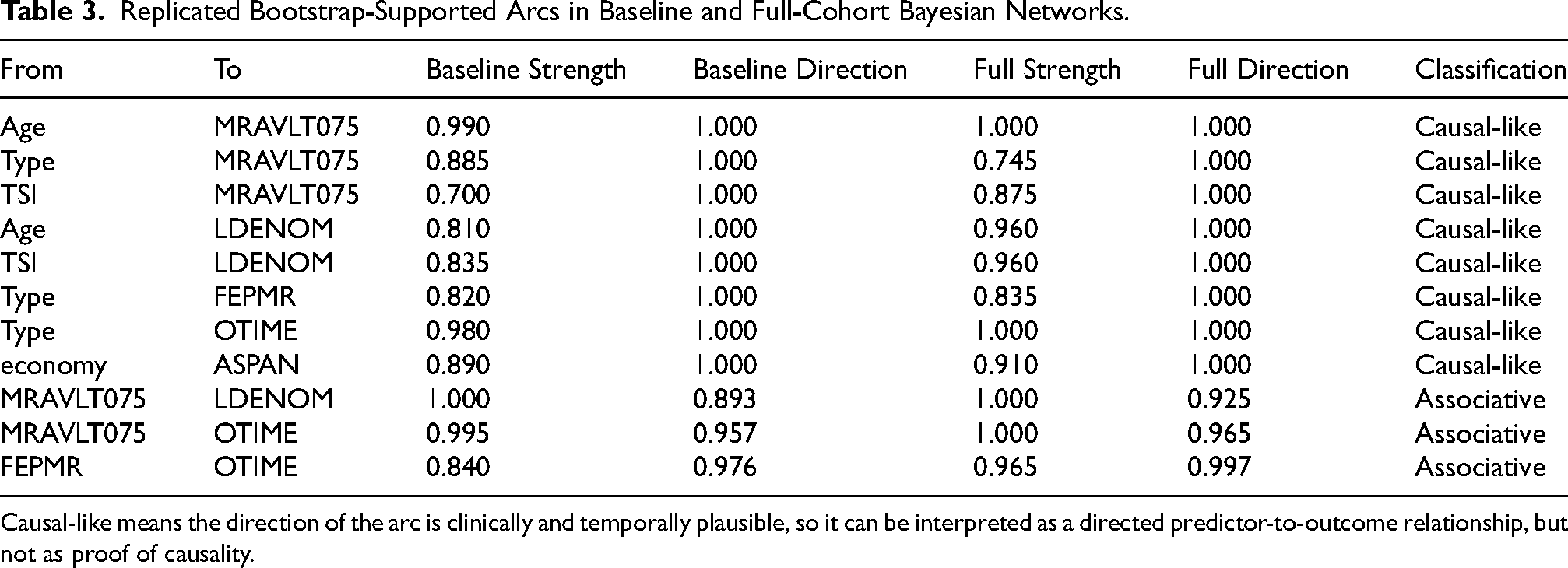
Causal-like means the direction of the arc is clinically and temporally plausible, so it can be interpreted as a directed predictor-to-outcome relationship, but not as proof of causality.
Because MRAVLT075 showed the largest number of replicated clinically interpretable links, it was selected for detailed model-based stratification across representative age, stroke subtype, and time-since-injury profiles. Table 4 presents predicted MRAVLT075 values derived from the fitted baseline Bayesian network across combinations of these variables, while holding the remaining parent variables constant at representative values. The predictions showed progressively lower expected verbal learning scores with older age and longer time since injury in both stroke subtypes, with higher predicted values in ischemic than in hemorrhagic stroke at comparable profiles. The local model for MRAVLT075 showed moderate explanatory performance, accounting for 42% of the observed variance (R2 = 0.42). The root mean squared error was 8.9 points and the mean absolute error was 7.1 points. Given the 0–75 scale range of MRAVLT075, this corresponds to an average prediction error of approximately 10–12% of the total scale range, indicating that the model is more suitable for group-level stratification than for precise individual-level prediction.
Model-Based Predicted MRAVLT075 Values Across Representative age, Stroke Subtype, and Time-Since-Injury Profiles.
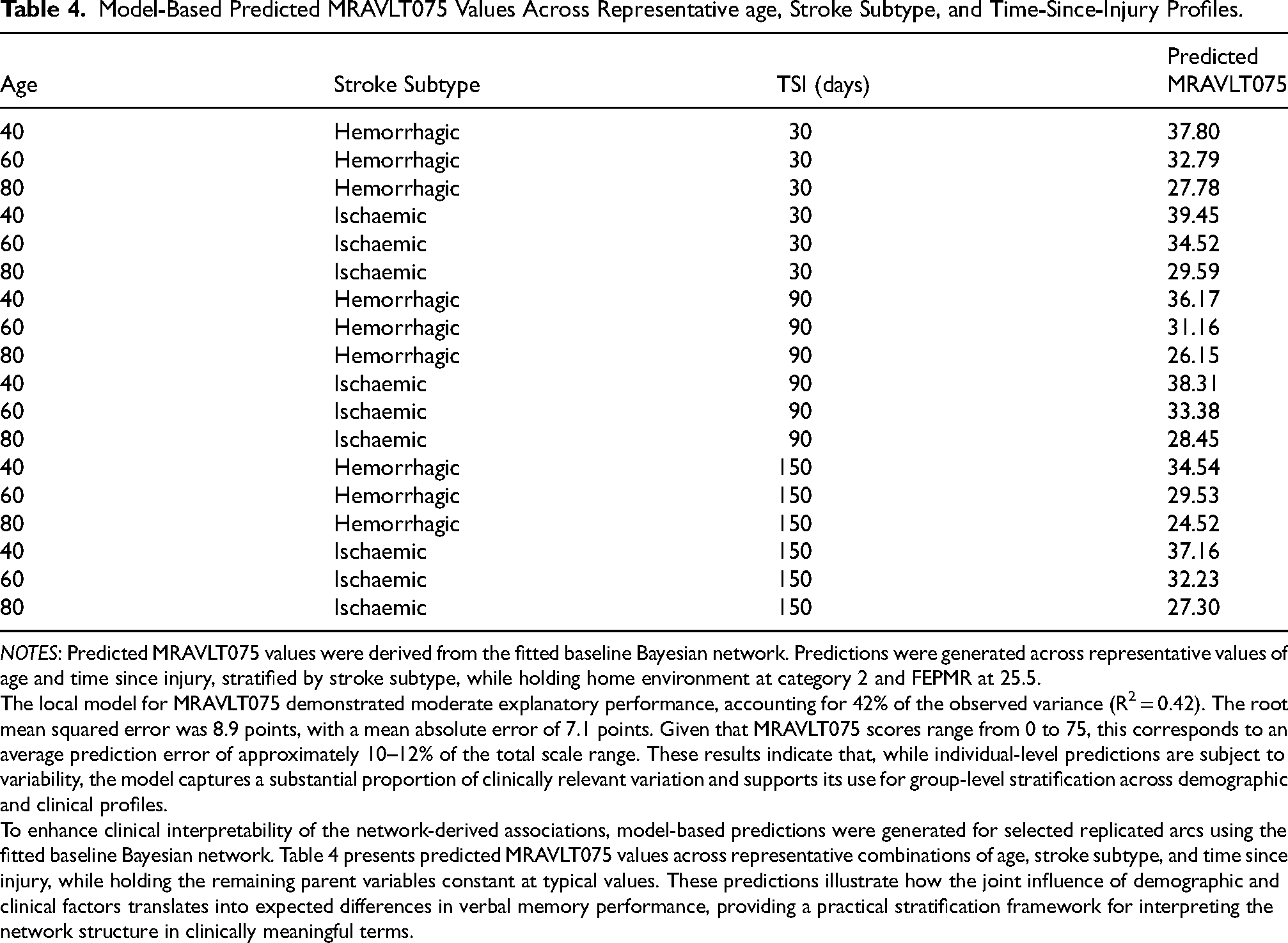
NOTES: Predicted MRAVLT075 values were derived from the fitted baseline Bayesian network. Predictions were generated across representative values of age and time since injury, stratified by stroke subtype, while holding home environment at category 2 and FEPMR at 25.5.
The local model for MRAVLT075 demonstrated moderate explanatory performance, accounting for 42% of the observed variance (R2 = 0.42). The root mean squared error was 8.9 points, with a mean absolute error of 7.1 points. Given that MRAVLT075 scores range from 0 to 75, this corresponds to an average prediction error of approximately 10–12% of the total scale range. These results indicate that, while individual-level predictions are subject to variability, the model captures a substantial proportion of clinically relevant variation and supports its use for group-level stratification across demographic and clinical profiles.
To enhance clinical interpretability of the network-derived associations, model-based predictions were generated for selected replicated arcs using the fitted baseline Bayesian network. Table 4 presents predicted MRAVLT075 values across representative combinations of age, stroke subtype, and time since injury, while holding the remaining parent variables constant at typical values. These predictions illustrate how the joint influence of demographic and clinical factors translates into expected differences in verbal memory performance, providing a practical stratification framework for interpreting the network structure in clinically meaningful terms.
Markov Blanket Analysis and Structural Roles of the Selected Cognitive Measures
Markov blanket analysis showed that the five selected cognitive measures occupied distinct roles within the baseline Bayesian network (Table 5). MRAVLT075 was the only cognitive variable present in the Markov blankets of all other cognitive tests, indicating that verbal learning was the most broadly connected measure within the selected cognitive subnetwork. In contrast, OTIME showed a convergent local dependency pattern composed of MRAVLT075, FEPMR, and stroke subtype, whereas ASPAN and LDENOM showed more selective dependency patterns, involving MRAVLT075 together with socioeconomic and age/time-since-injury factors, respectively. FEPMR showed a more restricted pattern, contributing mainly to OTIME. Overall, these findings suggest that the selected tests were not interchangeable, but reflected different roles within the post-stroke cognitive network.
Markov Blankets and Structural Roles of the Representative Cognitive Tests in the Baseline Bayesian Network.
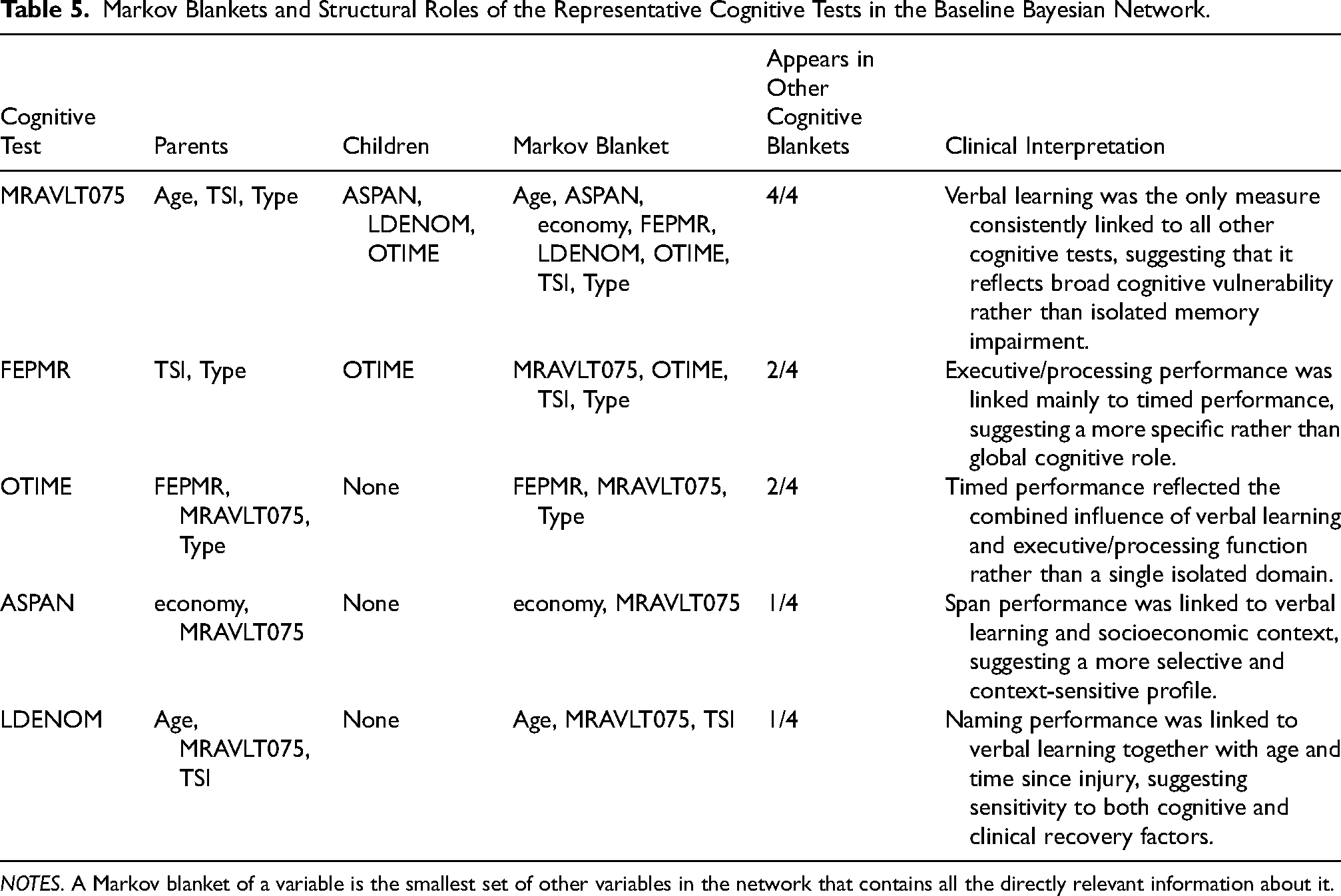
NOTES. A Markov blanket of a variable is the smallest set of other variables in the network that contains all the directly relevant information about it.
Discussion
In this large real-world cohort of post-acute stroke rehabilitation, complete-case analysis of the full baseline battery would have excluded 95.3% of patients. Even after reducing the battery to five representative tests, complete-case restriction would still have retained only 43.3% of the baseline cohort; nevertheless, stable and clinically interpretable relationships were recovered from incomplete cognitive assessments. This is the main practical contribution of the study: incomplete cognitive data, which affected the full battery rather than only language-dependent measures, should be understood as a routine feature of clinical practice rather than an exceptional limitation. A second contribution is that the main dependency pattern identified at baseline was reproduced when all available assessments within 6 months were analyzed, suggesting that meaningful relationships can be recovered from partially observed routine data and are not restricted to a single assessment snapshot. A third contribution is that the selected cognitive tests were not interchangeable. Verbal learning (MRAVLT075) showed the broadest set of relationships, timed orientation/performance (OTIME) reflected combined influences, and ASPAN, LDENOM, and FEPMR showed more specific patterns. Clinically, this suggests that low performance across these measures should not be interpreted in the same way, particularly when only a partial cognitive assessment is available.
Alternative strategies to address missing cognitive data after stroke include adapting assessment delivery (e.g., telephone or computerized testing), using non-verbal measures for patients with communication deficits, and applying analytic approaches such as multiple imputation (Sujanthan et al., 2025a, 2025b). However, remote assessment still leaves substantial incompleteness in stroke cohorts, and non-verbal approaches mainly address language-related exclusion rather than the broader, battery-wide missingness seen in routine neuro-rehabilitation data.
Multiple imputation is often recommended for incomplete clinical data, but it is not assumption-free and may be problematic when missingness is clinically informative rather than ignorable (Groenwold, 2020; Heymans & Twisk, 2022). In post-stroke cognitive assessment, non-completion is frequently linked to factors such as severe morbidity, communication deficits, visual difficulties, fatigue, or non-attendance, suggesting that missingness may reflect patient status rather than random loss of information (Sujanthan et al., 2025a, 2025b). In such settings, imputing plausible scores may preserve sample size, but it may also obscure information carried by the missingness pattern itself; more generally, when data are missing not at random, multiple imputation does not guarantee valid results, and the MAR versus MNAR distinction cannot be established from observed data alone (Heymans & Twisk, 2022)
Bayesian networks treatment of missing data is completely different. They factorize the joint distribution into a set of local conditional models, so an observation does not need to be complete across all variables to contribute information to the analysis. Instead, each patient contributes to the estimation of the specific node-parent relationships for which data are available, meaning that missingness reduces information locally rather than removing the entire case, as occurs in complete-case analysis. This local factorization is particularly advantageous in routine clinical datasets with uneven test completion. In our study, the conditional Gaussian framework further allowed continuous and categorical variables to be modeled jointly within the same network. As a result, partially observed assessments could still contribute to the estimation of clinically interpretable dependency patterns without requiring every missing score to be imputed.
Previous Bayesian-network studies in stroke have mainly focused on outcome prediction, complication risk, behavioral risk profiles, or cognitive-decline forecasting (Etholén et al., 2025; Liu et al., 2025; Park et al., 2018; Seixas et al., 2018). In contrast, the present study applies Bayesian-network modelling to incomplete routine cognitive assessments in post-acute stroke rehabilitation, with the aim of recovering clinically interpretable relationships among selected cognitive, clinical, and contextual variables, examining whether these relationships replicate across baseline and all available assessments, and exploring group-level stratification in a relatively young rehabilitation cohort.
Several limitations should be noted. This was a single-center study conducted in a specialized post-acute neuro-rehabilitation setting, which may limit generalizability; however, the cohort was large and the cognitive instruments and analytic approach are widely used. The cohort was also relatively young for a stroke population (mean age 51 years), which increases relevance to working-age stroke survivors but may limit extrapolation to older cohorts at higher cognitive risk. In addition, the network analysis was based on five selected cognitive measures rather than the full 24-test battery; this reduced the cognitive space studied, but it was necessary to preserve domain coverage while avoiding the extreme loss of sample size associated with complete-case analysis. The confirmatory analysis also included repeated assessments from the same patients, so it should be interpreted as replication of the main dependency pattern rather than as an independent validation sample. Finally, Bayesian networks identify conditional dependency patterns rather than causal effects, and the MRAVLT075 stratification is more appropriate for group-level interpretation than for individual-level prediction.
Conclusions
Incomplete cognitive assessment is a routine reality in post-acute stroke neuro-rehabilitation and should not automatically render a case unusable. In our cohort, complete-case analysis would have excluded most patients and retained a cognitively less impaired subgroup, whereas preserving partially observed assessments better reflected the population actually treated in routine rehabilitation. The present findings also suggest that partial cognitive assessments should not be read as collections of equivalent scores. Within a feasible reduced battery, some measures were linked to broader clinical-cognitive patterns, whereas others reflected more specific or context-dependent difficulties. Clinically, this supports a more selective interpretation of incomplete assessments and argues against treating all available scores as equally informative. The direct association between economic status and attentional span further suggests that contextual factors may shape cognitive performance even within routine rehabilitation datasets. Overall, incomplete routine cognitive data may still support meaningful interpretation and group-level stratification without relying solely on complete-case restriction or blanket score imputation.
Supplemental Material
sj-docx-1-nre-10.1177_10538135261464181 - Supplemental material for Incomplete Cognitive Assessment in Post-Acute Stroke Rehabilitation: Recovering Clinically Interpretable Relationships from Routine Neuropsychological Data
Supplemental material, sj-docx-1-nre-10.1177_10538135261464181 for Incomplete Cognitive Assessment in Post-Acute Stroke Rehabilitation: Recovering Clinically Interpretable Relationships from Routine Neuropsychological Data by Alejandro García-Rudolph, Rocío Sánchez-Carrión, Katryna Cisek, Thi Nguyet Que Nguyen, Claudia Teixido-Font, Eloy Opisso, Rory O'Connor, Gelu Onose and Gunnar Cedersund in NeuroRehabilitation
Supplemental Material
sj-docx-2-nre-10.1177_10538135261464181 - Supplemental material for Incomplete Cognitive Assessment in Post-Acute Stroke Rehabilitation: Recovering Clinically Interpretable Relationships from Routine Neuropsychological Data
Supplemental material, sj-docx-2-nre-10.1177_10538135261464181 for Incomplete Cognitive Assessment in Post-Acute Stroke Rehabilitation: Recovering Clinically Interpretable Relationships from Routine Neuropsychological Data by Alejandro García-Rudolph, Rocío Sánchez-Carrión, Katryna Cisek, Thi Nguyet Que Nguyen, Claudia Teixido-Font, Eloy Opisso, Rory O'Connor, Gelu Onose and Gunnar Cedersund in NeuroRehabilitation
Supplemental Material
sj-doc-3-nre-10.1177_10538135261464181 - Supplemental material for Incomplete Cognitive Assessment in Post-Acute Stroke Rehabilitation: Recovering Clinically Interpretable Relationships from Routine Neuropsychological Data
Supplemental material, sj-doc-3-nre-10.1177_10538135261464181 for Incomplete Cognitive Assessment in Post-Acute Stroke Rehabilitation: Recovering Clinically Interpretable Relationships from Routine Neuropsychological Data by Alejandro García-Rudolph, Rocío Sánchez-Carrión, Katryna Cisek, Thi Nguyet Que Nguyen, Claudia Teixido-Font, Eloy Opisso, Rory O'Connor, Gelu Onose and Gunnar Cedersund in NeuroRehabilitation
Footnotes
Acknowledgments
Special thanks to Olga Araujo from Institut Guttmann – Documentation department for her support and assistance with literature retrieval.
Ethical Approval and Informed Consent Statements
The study was approved by the Institut Guttmann Ethics Committee of Clinical Research. The participants were anonymized and non-identifiable. Participants provided informed written consent to be included in research studies addressed by the hospital.
Author Contributions
AG-R: Conceptualization, Methodology, Formal analysis, Data curation, Software, Investigation, Visualization, Writing – original draft, Writing – review & editing, Project administration.
RS-C: Conceptualization, Investigation, Validation, Data curation, Methodology, Resources, Writing – review & editing.
KS: Software, Formal analysis, Methodology, Data curation, Visualization, Writing – review & editing
TNQN: Software, Formal analysis, Methodology, Data curation, Visualization, Writing – review & editing
CT-F: Conceptualization, Investigation, Validation, Data curation, Methodology, Resources, Writing – review & editing.
EO: Conceptualization, Supervision, Project administration, Software, Funding acquisition, Writing – review & editing.
RO: Conceptualization, Supervision, Project administration, Writing – review & editing.
GO: Conceptualization, Methodology, Supervision, Project administration, Writing – review & editing.
GS: Conceptualization, Supervision, Project administration, Software, Funding acquisition, Writing – review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially funded by EU HORIZON EUROPE STRATIF-AI - Continuous stratification for improved prevention, treatment, and rehabilitation of stroke patients using digital twins and AI (Grant Agreement 101080875 – Research and Innovation Action).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Use of Generative AI Disclosure
GPT-5.2 (OpenAI) was used to assist with language editing, improving writing flow, and refining the clarity of the manuscript. The authors reviewed and edited all AI-assisted text and take full responsibility for the final content of the manuscript
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.