
Abstract
Background
Gait variability is a sensitive marker of neuromotor function and a clinically relevant indicator of fall risk and mobility impairment in neurological and geriatric populations. The Enhanced Gait Variability Index (eGVI) has emerged as a promising composite measure that captures multidimensional gait irregularity in a single interpretable score, offering a practical advantage over single-parameter approaches. Despite growing clinical interest, the evidence base supporting its standardized implementation has not been mapped.
Objectives
To characterize populations and clinical contexts where the eGVI has been applied, map assessment protocol heterogeneity, and identify methodological gaps limiting precision medicine-aligned implementation in neurological and geriatric rehabilitation.
Methods
A scoping review following PRISMA-ScR guidelines was conducted using PubMed, CINAHL, Scopus, Emcare, and Web of Science. Peer-reviewed studies reporting eGVI outcomes were included. Data were extracted on participant characteristics, gait assessment protocols, and outcomes, with attention to factors influencing clinical interpretation.
Results
Eighteen studies involving 1,915 participants were included, predominantly examining Parkinson's disease (39%) and older adult populations (22%). The eGVI demonstrated preliminary sensitivity to neuromotor impairment, age-related gait changes, and increased task complexity during dual-task walking; findings were most consistent in Parkinson's disease, based on limited number of studies (n = 7). Substantial heterogeneity in walkway systems, walking conditions, assistive device use, and reference populations limited comparability.
Conclusion
While the eGVI shows promise as a clinical outcome measure, protocol variability and reliance on a single unvalidated normative reference limit its clinical use. Population-specific protocols and normative data consistent with a precision medicine approach, are essential for reliable adoption.
Keywords
Introduction
Gait variability, the natural stride-to-stride fluctuation present in every walking pattern (O'Sullivan et al., 2019), is a sensitive marker of neuromotor health. In healthy walking, optimal variability supports adaptability, allowing the neuromuscular system to use movement synergies to maintain and restore balance in response to environmental perturbations (Hausdorff, 2005; Ó'Reilly & Federolf, 2021). When this regulatory capacity is disrupted by aging or neurological diseases, gait variability becomes inconsistent, less automatic, and more vulnerable to external demands (Hausdorff, 2005; Leon & Woo, 2018; Mueller & Maluf, 2002). Clinically, altered gait variability is associated with increased risk of falls and reduced mobility (Hausdorff, 2005), while deviations from the optimal range in either direction may reflect underlying postural instability and motor impairment (Sidoroff et al., 2021), making precise quantification of gait variability a clinical and a research priority.
Beyond general aging-related decline, neurological conditions such as Parkinson's disease (PD), Multiple Sclerosis, and Huntington's disease precipitate a more fundamental breakdown in the natural rhythmic structure of locomotion, producing distinct gait signatures that set them apart from the healthy population (Moon et al., 2016). These signatures manifest as measurable, reproducible changes in stride-to-stride fluctuations that reflect the specific pattern of neuromotor dysregulation underlying each condition. In PD, gait variability markers can differentiate idiopathic disease from atypical Parkinsonian syndromes such as multiple system atrophy, and gait variability increases progressively with disease severity (Sidoroff et al., 2021). In Huntington's disease, stride-to-stride fluctuations correlate with disease progression and functional status (Gaßner et al., 2020). In Multiple Sclerosis, gait variability is sensitive to fatigue and cognitive load, revealing neuromotor deficits that standard walking speed measures alone fail to detect (Mofateh et al., 2017; Müller et al., 2021). These disease-specific signatures make gait variability a uniquely informative digital biomarker - a physiological signal that sensor-based systems can capture continuously, and that sensitively reflects the integrity of the underlying neurological control system (Baek et al., 2024; Coravos et al., 2019; Klucken et al., 2013; Moon et al., 2016; Pieruccini-Faria et al., 2021; Schaefer et al., 2015; Strongman et al., 2023). This sensitivity is further amplified during dual-task walking, where dividing cognitive resources leads to immediate deterioration that predicts falls more accurately than single-task performance in both older adults and in neurological populations (Mofateh et al., 2017; Yogev et al., 2005).
Accurate quantification of gait variability requires appropriate measurement tools, and the choice of system has direct implications for clinical applicability. Instrumented walkways such as Zeno and GAITRite systems detect discrete footfall events and capture spatiotemporal parameters with high validity in controlled clinical environments (Bilney et al., 2003; Vallabhajosula et al., 2019). Motion capture systems offer superior kinematic accuracy but are constrained by cost, setup complexity, and the need for specialist operators (Simon, 2004), limiting their use outside research settings. For more accessible assessment, wearable accelerometers enable continuous monitoring during natural walking conditions, capturing stride-to-stride fluctuations that laboratory snapshot assessments may miss (Del Din et al., 2016). Smartphone-based accelerometers offer a low-cost alternative (Baek et al., 2024), although they sacrifice some spatial precision (Strongman et al., 2023). The selection of an appropriate system should be guided by the clinical context, the population of interest, and the specific gait parameters under investigation. However, the clinical value of any measurement system depends on the validity and standardization of the analytical framework applied to its output.
Gait variability has traditionally relied on single-parameter metrics such as standard deviation and coefficient of variation of stride time and stride length, which provide an incomplete picture of the multidimensional nature of walking (Ellis et al., 2015; Gaßner et al., 2020; Karatsidis et al., 2025). To address this, Gouelle et al. (2013) introduced the Gait Variability Index (GVI), a composite measure derived from nine spatiotemporal parameters, including step length, stride length, step time, stride time, swing time, stance time, single support time, double support time, and walking velocity (Gouelle et al., 2013). However, redundancy within the parameter set limited its discriminative power (Gouelle et al., 2018). Gouelle et al. (2018) subsequently developed the Enhanced Gait Variability Index (eGVI), retaining only five non-redundant parameters (step length, step time, stance time, single support time, and stride velocity) and merging data from both limbs to improve clinical interpretability. Scores are normalized against a healthy normative group aged approximately 12–62 years (Gouelle et al., 2013), where 100 represents typical gait variability with a standard deviation of 10, and higher scores are associated with elevated falls risk (Gouelle et al., 2018). The eGVI offers rehabilitation clinicians a single interpretable composite score that reflects multidimensional gait irregularity, representing a meaningful advance over both single-parameter metrics and the redundancy-affected GVI. At the same time, composite indices carry inherent trade-offs. Collapsing several gait parameters into a single value may obscure which specific impairment is driving a given score, limiting interpretability at the individual-patient level. It also remains unclear whether this added complexity improves clinical decision-making relative to simpler, more transparent single-parameter metrics. These considerations make it important to examine how, and how consistently, the eGVI has actually been applied in practice.
Despite the methodological advance, the eGVI's translation into clinical rehabilitation practice remains limited, and three gaps are particularly consequential for clinical adoption. First, the clinical interpretation of eGVI scores remains uncertain, as score thresholds have not been established for specific clinical populations. Second, acquisition protocols vary widely across studies, with no standardized approach to walkway type, walking distance, or assistive-device use. Third, the eGVI relies on a single normative reference that has not been validated for the clinical populations to which it is applied. Since its introduction in 2018, the eGVI has been applied across a growing range of neurological and geriatric conditions, yet no synthesis of this literature has addressed these gaps.
This review aims to: (1) characterize the populations and clinical contexts in which the eGVI has been applied; (2) map the heterogeneity of current assessment protocols; and (3) identify methodological gaps that must be addressed to support precision medicine-aligned implementation of the gait assessment in neurological and geriatric rehabilitation.
Methods
This scoping review followed the methodological framework for scoping reviews and is reported in accordance with the Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist. The protocol was registered on Figshare (registration number:10.6084/m9.figshare.29537939).
Eligibility Criteria
Studies were eligible for inclusion if they (1) employed the eGVI as an outcome measure, predictor variable, or in psychometric evaluation; (2) included adult aged ≥ 18 years; (3) examined populations with neurological conditions or age-related changes; and (4) were peer-reviewed articles published in English. Hierarchical exclusion criteria were applied to ensure consistent screening. Studies were excluded if they (1) were not published in English, (2) were not full-text peer-reviewed publications (e.g., conference abstracts, editorials, commentaries, or dissertations), (3) involved pediatric populations, (4) did not include neurological or older adult populations, or (5) did not report the eGVI in one of the eligible outcomes.
Search Strategy
A comprehensive literature search was conducted on July 13, 2025, and repeated on February 1, 2026, across PubMed, CINAHL, Scopus, Emcare, and Web of Science (M.W.), complemented by grey literature searches in SPORTDiscus and Google Scholar. The same search string, comprising the terms “Enhanced Gait Variability Index” OR “eGVI”, was applied across all sources, combined with population terms: “neurological”, “aging”, “seniors”, “older adults”. No date restrictions were applied, but results were limited to English-language studies involving human participants. A pilot search was undertaken to refine the strategy before full implementation. Grey literature records were screened against the same inclusion and exclusion criteria as the database records, and the full selection flow is shown in Figure 1.
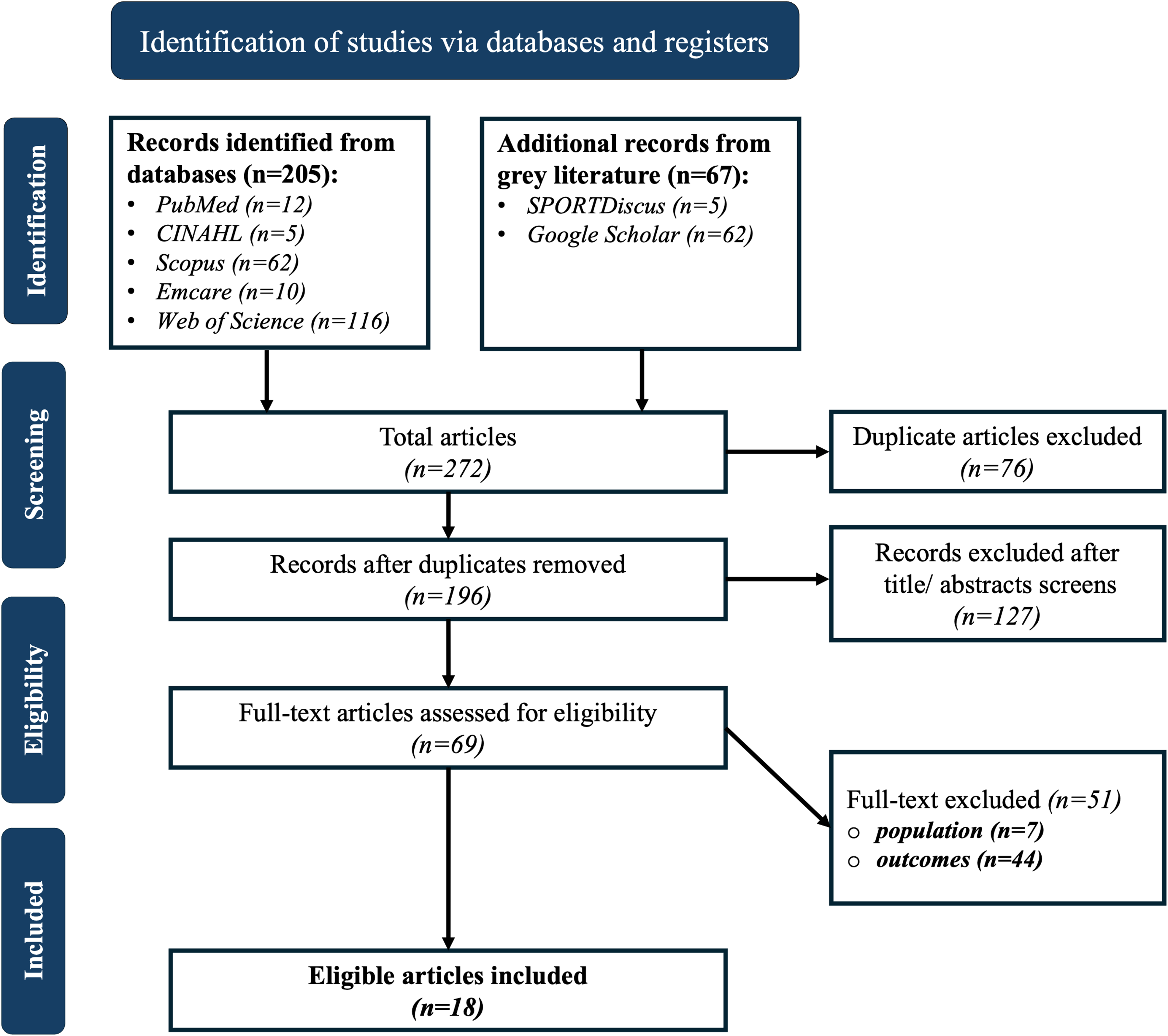
Flowchart illustrating the screening process for study selection (PRISMA-ScR).
Study Selection
Search results were imported into a systematic review management platform (Rayyan Systems Inc., Doha, Qatar) for deduplication and management. Two reviewers (M.W. and P.K.) independently screened titles and abstracts against inclusion criteria. Full-text assessments were conducted for potentially eligible studies with disagreements resolved through discussion and consensus. The study selection process is summarized in the PRISMA flow diagram (see Figure 1).
Data Analysis
Data from all eligible studies were manually extracted by one reviewer (M.W.) into a Microsoft Excel, capturing authors, publication year, study design and aims, participant and assessment characteristics, walking protocols, eGVI outcomes, and key findings, and were independently validated by a second reviewer (P.K.). Discrepancies were resolved through discussion and consensus. Owing to methodological heterogeneity, results were summarized descriptively in tables and complemented by a narrative synthesis.
Results
Eighteen studies published between 2019 and 2026 met the eligibility criteria, collectively encompassing 1,915 participants. The initial database search identified 272 records, which were reduced to 196 studies after removing duplicates in Rayyan. Title and abstract screening reduced the number of studies eligible for full-text review to 69, of which 18 met the inclusion criteria. The remaining 51 studies were excluded, including 7 studies with the wrong population, and 44 studies investigating unrelated outcomes of which 1 study focused on the development of the eGVI methodology.
Characteristics of Included Studies
All 18 eligible studies were published between 2019 and 2026, following the introduction of the eGVI in 2018. Included study characteristics are summarized in a chronological order (see Table 1). Blank cells in the table indicate information that was not reported in the original publications. Seventy-two percent of studies used an observational design, while the remaining implemented an interventional approach. Study locations were identified primarily from the methods sections or, when unspecified, inferred from author affiliations.
Characteristics of the Included Studies.
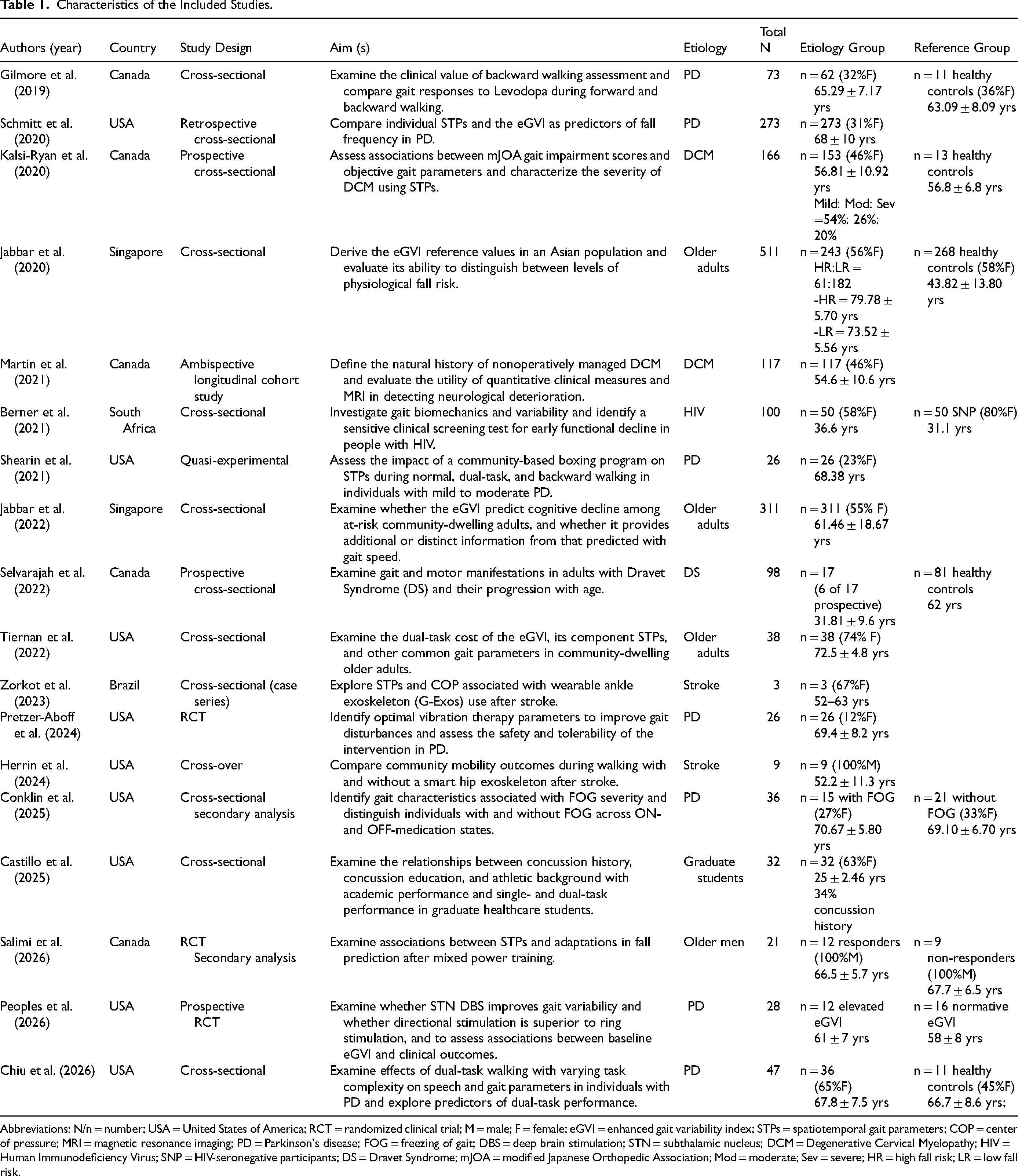
Abbreviations: N/n = number; USA = United States of America; RCT = randomized clinical trial; M = male; F = female; eGVI = enhanced gait variability index; STPs = spatiotemporal gait parameters; COP = center of pressure; MRI = magnetic resonance imaging; PD = Parkinson's disease; FOG = freezing of gait; DBS = deep brain stimulation; STN = subthalamic nucleus; DCM = Degenerative Cervical Myelopathy; HIV = Human Immunodeficiency Virus; SNP = HIV-seronegative participants; DS = Dravet Syndrome; mJOA = modified Japanese Orthopedic Association; Mod = moderate; Sev = severe; HR = high fall risk; LR = low fall risk.
Population
In total, 1,915 participants were analyzed in this review, aged 21 to 90 years. In studies with clinical conditions (n = 13), the mean age was 60.95 years. Among studies reporting gender (n = 15), 45% of participants in the clinical groups were female. Two studies did not report gender (Peoples et al., 2026; Selvarajah et al., 2022). A further study lacked subgroup data (Castillo et al., 2025) and was excluded from the pooled calculation of gender percentages. Diagnoses included PD (n = 7) (Chiu et al., 2026; Conklin et al., 2025; Gilmore et al., 2019; Schmitt et al., 2020; Shearin et al., 2021; Peoples et al., 2026; Pretzer-Aboff et al., 2024), degenerative cervical myelopathy (n = 2) (Kalsi-Ryan et al., 2020; Martin et al., 2021), adults with Dravet Syndrome (n = 1) (Selvarajah et al., 2022), stroke (n = 2) (Herrin et al., 2024; Zorkot et al., 2023), and Human Immunodeficiency Virus (n = 1) (Berner et al., 2021). Additionally, older adults (n = 4) (Jabbar et al., 2020, 2022; Salimi et al., 2026; Tiernan et al., 2022), and graduate healthcare students (n = 1) were also included in this review (Castillo et al., 2025). Fifty percent of 18 studies incorporated control groups with clinical populations.
Walking Protocols
Walking protocols varied considerably across the included studies (see Table 2). All studies assessed forward walking at a self-selected speed, while 7 studies included additional conditions to examine task-dependent variability, including backward walking (n = 3) (Castillo et al., 2025; Gilmore et al., 2019; Shearin et al., 2021), dual-task walking (n = 5) (Berner et al., 2021; Castillo et al., 2025; Chiu et al., 2026; Shearin et al., 2021; Tiernan et al., 2022), or fast-paced walking (n = 3) (Berner et al., 2021; Peoples et al., 2026; Shearin et al., 2021). Participants walked barefoot in 4 studies (Berner et al., 2021; Jabbar et al., 2020, 2022; Kalsi-Ryan et al., 2020), and the use of assistive devices was restricted in 2 studies (Kalsi-Ryan et al., 2020; Schmitt et al., 2020), whereas the remaining studies did not report these specific conditions. The number of walking trials also varied, as one study conducted two trials (Pretzer-Aboff et al., 2024), 5 studies conducted three trials (Berner et al., 2021; Castillo et al., 2025; Chiu et al., 2026; Jabbar et al., 2020; 2022), and 7 studies conducted four trials. Two studies reduced the number of trials as task complexity increased (Gilmore et al., 2019; Shearin et al., 2021), such as when changing walking direction or incorporating dual-task activities, whereas 1 study used a single trial per condition (Conklin et al., 2025), and 2 studies did not specify the number of trials (Martin et al., 2021; Salimi et al., 2026). Data were primarily collected using pressure-sensitive walkways, with Zeno used in 13 studies, GAITRite in 2 studies, and both systems used in combination in 2 studies. One study used a three-dimensional portable motion-capture system (Berner et al., 2021).
Gait Assessment Equipment & Walking Protocols.
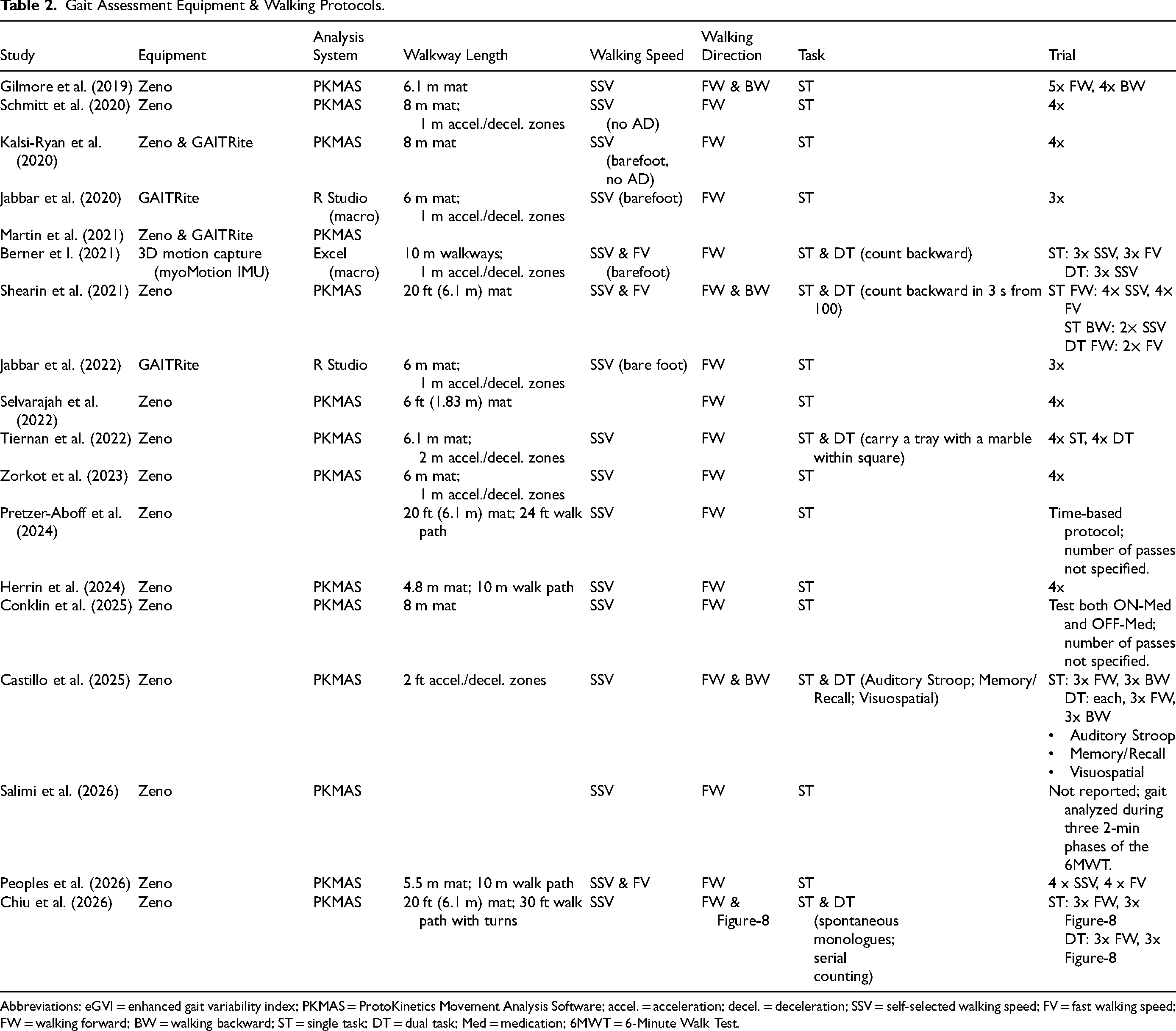
Abbreviations: eGVI = enhanced gait variability index; PKMAS = ProtoKinetics Movement Analysis Software; accel. = acceleration; decel. = deceleration; SSV = self-selected walking speed; FV = fast walking speed; FW = walking forward; BW = walking backward; ST = single task; DT = dual task; Med = medication; 6MWT = 6-Minute Walk Test.
Outcome Measures
The eGVI was applied for three primary analytical purposes across the 18 studies (see Table 3). Six studies utilized the eGVI as a predictor variable, examining its associations with cognitive function (Jabbar et al., 2022), falls (Jabbar et al., 2020; Schmitt et al., 2020), disease progression (Kalsi-Ryan et al., 2020; Martin et al., 2021), and concussion-related variables (Castillo et al., 2025). Five studies evaluated the psychometric or discriminative properties of the eGVI (Berner et al., 2021; Chiu et al., 2026; Gilmore et al., 2019; Shearin et al., 2021; Tiernan et al., 2022). The remaining studies measured the eGVI to evaluate responsiveness to interventions or experimental conditions, including exercises (Salimi et al., 2026; Shearin et al., 2021), medication effects (Conklin et al., 2025), exoskeleton-assisted walking (Herrin et al., 2024; Zorkot et al., 2023), vibration therapy (Pretzer-Aboff et al., 2024), and deep-brain stimulation effects (Peoples et al., 2026).
eGVI Score & Findings.
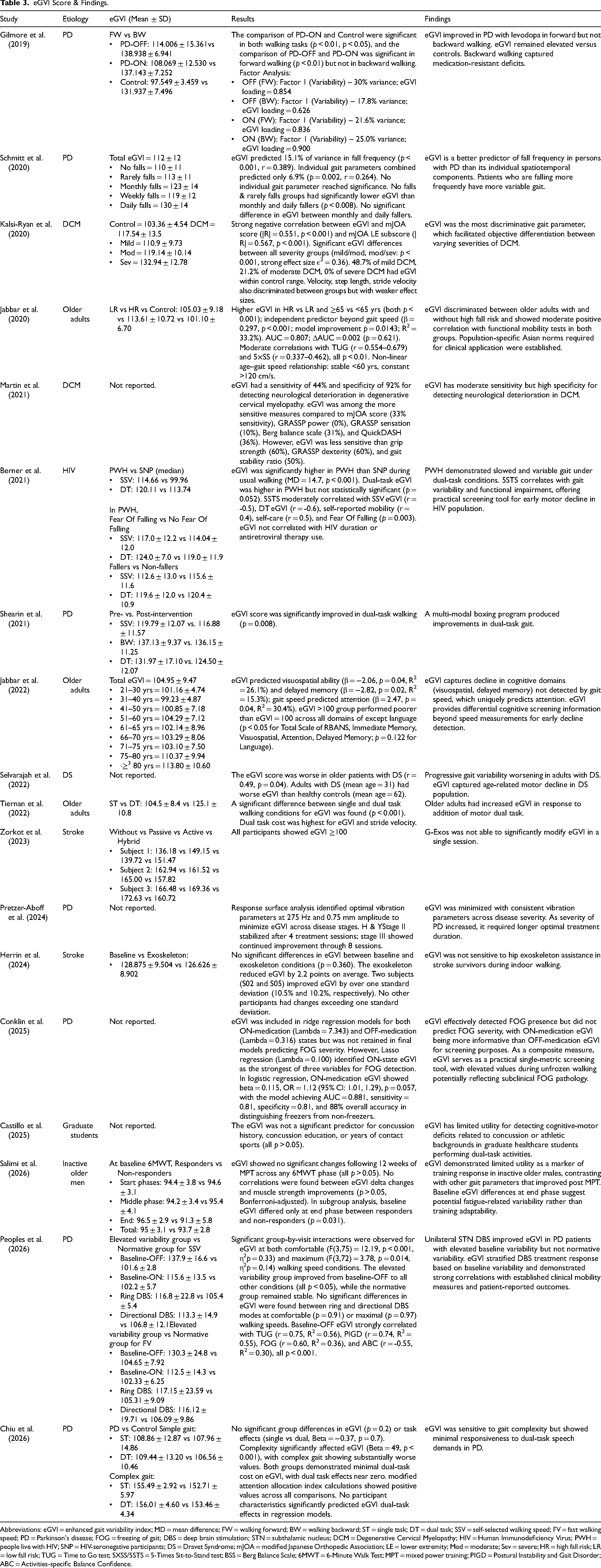
Abbreviations: eGVI = enhanced gait variability index; MD = mean difference; FW = walking forward; BW = walking backward; ST = single task; DT = dual task; SSV = self-selected walking speed; FV = fast walking speed; PD = Parkinson's disease; FOG = freezing of gait; DBS = deep brain stimulation; STN = subthalamic nucleus; DCM = Degenerative Cervical Myelopathy; HIV = Human Immunodeficiency Virus; PWH = people live with HIV; SNP = HIV-seronegative participants; DS = Dravet Syndrome; mJOA = modified Japanese Orthopedic Association; LE = lower extremity; Mod = moderate; Sev = severe; HR = high fall risk; LR = low fall risk; TUG = Time to Go test; 5XSS/5STS = 5-Times Sit-to-Stand test; BSS = Berg Balance Scale; 6MWT = 6-Minute Walk Test; MPT = mixed power training; PIGD = Postural Instability and Gait Disorder; ABC = Activities-specific Balance Confidence.
Discussion
This scoping review represents the first systematic synthesis of research exploring the eGVI as an outcome in neurological populations and older adults since its introduction in 2018.
Population
All 18 studies evaluated eGVI scores against the normative reference established by Gouelle et al., in which a score of 100 represents typical gait variability in a healthy population with a standard deviation of 10. The consistent use of this single reference across studies reflects a shared assumption providing a universal benchmark for gait variability. No study examined whether this reference is appropriate for the populations under investigation. Evidence from one study conducted in an Asian population (Jabbar et al., 2022) reported eGVI scores that differed from those observed in Western cohorts, raising questions about the assumption of generalizability across ethnicities, despite the single study findings requiring confirmation. Those populations differ substantially from the healthy reference group, in terms of age, ethnicity, diagnosis, and functional capacity. None of the reviewed studies established reference values for younger versus older adults, different gait speeds, walking directions, task challenges, or gender-specific thresholds. Among studies reporting gender, 45% of participants in clinical groups were female. No study conducted gender-stratified analyses, despite established gender differences in gait biomechanics and changes with aging (Johansson et al., 2016). Fall risk is disproportionately high in female rehabilitation populations (Johansson et al., 2016), and whether eGVI thresholds for elevated fall risk differ between genders remains an unanswered clinical question.
Study populations were substantially older than the healthy reference group used for eGVI calculation, with a mean age of 60.95 years in clinical studies and an age range spanning 21 to 90 years across all included studies. This age discrepancy aligns with observed eGVI elevations, as gait variability naturally increases with age-related declines in sensorimotor integration and executive control (Nóbrega-Sousa et al., 2020). This consistent pattern across the included studies suggests that eGVI detects age-related neuromotor decline. However, none of the reviewed studies established age-stratified reference values. The degree to which eGVI elevations reflect true pathology versus expected aging therefore remains unresolved. This gap is particularly consequential in older adult rehabilitation, where distinguishing pathological from age related physiological gait change directly informs intervention decisions. Only four studies incorporate younger participants, which further limits the generalizability of current eGVI evidence to younger populations.
Among the neurological conditions represented in this review, PD was the predominant focus. The eGVI in these studies consistently showed sensitivity to PD-related gait impairments, including reduced speed, asymmetry, and disrupted rhythm (Zhang et al., 2022). This supports its potential as a monitoring tool in Parkinsonian rehabilitation. While gait variability impairments are well-documented in conditions such as stroke (Balasubramanian et al., 2009), Multiple Sclerosis (Socie et al., 2013), Huntington's disease (Gaßner et al., 2020), cerebellar ataxia (Serrao et al., 2012), and peripheral neuropathy (Dingwell & Cavanagh, 2001), the eGVI has not been systematically applied across these populations. Each condition damages distinct features of gait rhythm, symmetry, and timing that differ from the Parkinsonian pattern. Whether the eGVI captures disease-specific gait signatures or reflects a more general measure of neuromotor dysregulation cannot be determined from the current literature. Rehabilitation units routinely manage patients with more complex and/or mixed neurological diagnoses, and this gap means that the eGVI cannot yet be applied with equal confidence across all clinical populations.
Standardized Protocol
Inconsistent acquisition protocols represent a fundamental barrier to the clinical implementation of the eGVI. All 18 studies assessed forward walking at self-selected speed in controlled laboratory environments, approximating overground walking while capturing natural gait variability. However, laboratory investigations do not fully reflect daily-life walking, with notable differences between these environments existing especially in the elderly and neurologic population (Hillel et al., 2019; Rojer et al., 2021).
Only 3 studies examined backward walking in this review, yet all reported substantially elevated eGVI relative to forward walking. This consistent finding suggests that backward walking may reveal neuromotor deficits not captured during forward walking alone, consistent with prior evidence that backward walking spatiotemporal measures decline more precipitously with age than forward walking measures (Fritz et al., 2013). Backward walking requires increased motor cortex activation and greater recruitment of sensorimotor pathways compared to forward walking (Kurz et al., 2012; Sasaki et al., 2024), which likely explains its greater sensitivity to neuromotor impairment. Despite this consistency, backward walking is absent from most eGVI protocols, representing a critical gap in current assessment practice that can lead to the systematic underestimation of the true level of gait variability. A similar gap exists for faster walking speeds. Fast walking challenges stability through rapid weight transfers and increased propulsive forces (Browne & Franz, 2017). Only 3 studies examined how gait speed variations affect eGVI scores (Berner et al., 2021; Peoples et al., 2026; Shearin et al., 2021), and their findings could not be directly compared due to differing speed increments and conditions.
Five studies in this review used dual-task paradigms that produced contrasting findings. The eGVI increased under motor dual-task conditions (Tiernan et al., 2022), consistent with the established principle that competing motor demands stress gait automaticity. Conversely, the eGVI showed near-zero responsiveness to cognitive-verbal dual-task demands (Chiu et al., 2026), suggesting that adding a verbal task does not reliably challenge the motor control processes the eGVI captures. However, gait complexity rather than cognitive load produced large and significant eGVI increases in both PD and control groups in the same study (Chiu et al., 2026). The eGVI may be more sensitive to the motor complexity of the walking task itself than to concurrent cognitive demands, a distinction with important implications for protocol design. Because these observations derive largely from a single study, they should be regarded as hypothesis-generating and in need of replication. This inconsistency, combined with limited overall application, represents a significant gap, as walking rarely occurs as an isolated motor activity in daily life. Cognitive load increases gait variability during indoor walking, whereas environmental load increases it during outdoor walking (Ho et al., 2019; Montero-Odasso et al., 2012), highlighting the distinct contributions of different task demands to gait control. Dual-task conditions are particularly valuable since they reveal gait deficits that remain concealed during single-task walking (Zukowski et al., 2021). Clinically, dual-task gait deterioration predicts falls more accurately than single-task performance in older adults (Beauchet et al., 2009; Muir-Hunter & Wittwer, 2016), and insufficient dual-task assessment risks underestimating real-world functional impairment in rehabilitation settings.
Only 4 studies standardized footwear and assistive device use. The remaining studies either did not standardize these conditions or did not report them. Barefoot walking increases joint motion, reduces ground reaction force, and lowers plantar pressure compared to shoe conditions (Franklin et al., 2015), whereas footwear or assistive devices can alter cadence and shorten stride length (Bryant et al., 2012; Franklin et al., 2015). Unstandardized footwear may introduce variability that confounds the eGVI score itself. Two studies on individuals with stroke incorporated exoskeleton-assisted walking (Herrin et al., 2024; Zorkot et al., 2023). The eGVI remained substantially elevated across all exoskeleton conditions in both studies, with minimal and non-significant reductions observed. This suggests that eGVI elevations during exoskeleton-assisted walking may reflect persistent neurological impairment rather than a failure of the device. Rehabilitation clinicians using assistive technology as an intervention should interpret elevated eGVI scores in this context with caution.
The number of walking passes used to calculate eGVI varied across studies, ranging from a single walk to multiple repeated passes. The original GVI protocol employed multiple passes (Gouelle et al., 2018), yet no consensus exists on the minimum number required for stable variability estimates. No minimum stride count was specified for clinical populations. Research in PD has established that a minimum of 40 consecutive steps is required to achieve a stable variability estimate (Rennie et al., 2017, 2018). No equivalent guideline exists for other neurological conditions. An eGVI derived from insufficient stride counts may reflect measurement noise rather than one's true gait variability. The absence of a universal minimum stride count standard is one of the most practically addressable barriers to reliable eGVI use in clinical and research practice.
Analytical Utility
The eGVI was applied as a predictor of clinical outcomes, a psychometric measure, and an intervention outcome measure across the included studies. These applications indicate that the eGVI can capture valuable variations in gait control among neurological and aging populations, consistent with evidence that variability-based gait indices are sensitive markers of neuromotor impairment (Zhang et al., 2022). However, this diversity of analytical purpose, combined with the protocol heterogeneity described above, limits synthesis. A measure used to predict falls in one study and evaluate medication effects in another will yield meaningful individual findings, but without standardized acquisition conditions, the cumulative evidence base remains fragmented.
Clinical Implications
Several practical considerations follow from this review, though all remain provisional given the limited and heterogeneous evidence. We recommend interpreting absolute eGVI scores cautiously and tracking within-patient change under a consistent protocol rather than relying on normative comparison. Acquisition conditions, including footwear and assistive-device use, walking direction and speed, and the number of walking passes, need to be ideally standardized before eGVI scores are compared. The eGVI appears to be most informative in PD, where the available evidence is concentrated, and may warrant more cautious interpretation in other neurological conditions where evidence remains sparse. Overall, the eGVI is a promising measure to inform clinical practice, but does not yet appear ready for use as a standalone, normatively referenced clinical outcome measure.
Limitations
The review has several limitations. First, the evidence base is small. Only 18 studies met the inclusion criteria, and they were unevenly distributed across populations, with PD overrepresented. This imbalance limits the generalizability of our findings to other neurological and geriatric groups. Second, substantial heterogeneity in study designs, gait assessment protocols, instrumentation, outcomes, and data processing restricted our ability to draw direct comparisons or perform quantitative synthesis. Third, most included studies were conducted in controlled laboratory settings, so the extent to which eGVI findings reflect functional mobility under daily-life conditions remains unclear. In addition, the search strategy targeted adults with neurological conditions and age-related gait changes, therefore results cannot be generalized to pediatric populations, and only peer-reviewed, English-language studies were included, which may have introduced language and publication bias. Consistent with scoping review methodology, a formal critical appraisal of the included studies was not conducted, as the aim of this review was to assess the breadth of eGVI applications. A transparent screening process following PRISMA-ScR guidelines was employed to enhance reproducibility.
Conclusions
The eGVI is a clinically relevant composite measure of gait variability that has shown preliminary sensitivity in detecting gait variability in neurological and geriatric rehabilitation populations, with the most consistent findings reported in PD. However, two critical gaps limit its clinical implementation. Protocol heterogeneity across studies undermines comparability, and the universal application of a single normative reference without validation for clinical populations raises concerns about score interpretability. Standardized acquisition protocols and population-specific normative databases are recommended before the eGVI can be adopted with confidence as a clinical outcome measure. Longitudinal evidence of responsiveness to rehabilitation-induced changes is also required to support its use as a monitoring tool. These findings underscore the need for a precision medicine approach to gait variability assessment, in which population-specific protocols and reference values replace uniform benchmarks to better reflect individualized rehabilitation.
Footnotes
Acknowledgments
Not applicable.
Ethical Considerations
This article is a review and does not involve any studies with human participants or animals performed by the authors.
Consent to Participate
Not applicable.
Consent to Publication
Not applicable.
Author Contributions
Conceptualization, P.K. and M.W.; methodology, P.K. and M.W; investigation, P.K. and M.W; validation, P.K. and M.W; data curation, P.K. and M.W; writing – original draft, M.W.; writing – review and editing, P.K. and M.W; visualization, M.W.; supervision, P.K.; project administration, M.W.
All authors have read and agreed to the published version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Not applicable.