
Abstract
Background
Evidence on the feasibility of integrating music therapy into routine post-stroke aphasia rehabilitation in real-world settings remains limited.
Objective
To examine the feasibility of integrating a structured music therapy protocol into conventional speech-language therapy for post-stroke aphasia and explore preliminary outcomes.
Methods
This quasi-experimental study was conducted in an outpatient speech-language clinic in Thailand. Participants received standard speech-language therapy or therapy combined with a manualised music therapy protocol. The intervention represents a dose-augmented feasibility design, as the experimental group received increased overall therapeutic contact time. Language performance was assessed using the Thai Adaptation of the Western Aphasia Battery, and anxiety using the State–Trait Anxiety Inventory, Form Y-2. Pre–post changes were examined using descriptive statistics and exploratory analyses, including paired tests for within-group comparisons and independent tests for between-group differences.
Results
The intervention was feasible, with complete delivery and assessment. Within-group improvements in language performance were observed in both groups, with greater gains in the music therapy–augmented group; however, between-group differences were not statistically significant. Anxiety scores decreased in both groups, with no significant differences. Interpretation of anxiety outcomes is limited by the use of a trait-based measure, which may reflect the limited sensitivity of trait-based measure to short-term changes.
Conclusions
Integrating music therapy into routine speech-language rehabilitation for post-stroke aphasia is feasible in a real-world outpatient setting. Findings should be interpreted as exploratory and reflective of increased therapeutic exposure rather than modality-specific effectiveness. These results inform the design of future dose-matched and methodologically rigorous trials.
Keywords
Introduction
Stroke frequently results in long-term disability, with aphasia being one of the most disabling sequelae, affecting approximately one-third of stroke survivors and often persisting into the chronic phase (Flowers et al., 2016; Grefkes & Fink, 2020). Aphasia-related language impairment can substantially disrupt social participation, independence, and psychosocial well-being (Code & Herrmann, 2003; Hilari et al., 2012).
Speech-language therapy is central to aphasia rehabilitation; however, treatment responses vary widely depending on aphasia subtype, severity, time since stroke, and individual cognitive and emotional factors, highlighting the need for complementary approaches to support engagement and communication practice (Brady et al., 2016; Kertesz & McCabe, 1977; Watila & Balarabe, 2015).
Music-based interventions have been increasingly incorporated into aphasia rehabilitation as adjunctive strategies, with emerging clinical evidence suggesting potential benefits in supporting language recovery and participation in real-world rehabilitation settings (Altenmüller & Schlaug, 2015; Gu et al., 2024; Liu et al., 2022; Schlaug et al., 2009).
In addition to language impairment, anxiety is common among individuals with post-stroke aphasia and may influence communication confidence and participation in rehabilitation (Morris et al., 2017; Rafsten et al., 2018). Music-based activities have been reported to support emotional regulation and relaxation in neurological populations (Harney et al., 2023; Särkämö et al., 2016); however, evidence describing anxiety-related outcomes specifically in aphasia remains limited, partly due to measurement challenges.
Most studies of music therapy for aphasia have been conducted in controlled research settings with small samples, which may limit applicability to routine clinical practice (Ree et al., 2026; Zumbansen et al., 2014). In real-world rehabilitation contexts—particularly where patient numbers are limited and clinical heterogeneity is high—randomized controlled trials are often difficult to implement. Consequently, feasibility-focused and exploratory studies embedded in routine care are needed to inform intervention development and future trial design (Eldridge et al., 2016; Shadish et al., 2002).
Accordingly, the present study aimed to examine the feasibility and explore outcome trends associated with integrating music therapy into conventional speech-language therapy for individuals with post-stroke aphasia receiving outpatient rehabilitation. Using a quasi-experimental controlled pre–post design, the study focused on feasibility and descriptive patterns of change in language performance and anxiety, rather than on causal inference.
Methods
Study Design and Setting
This study employed a quasi-experimental controlled pre–post design conducted under real-world clinical conditions to examine feasibility and exploratory outcome patterns of music therapy integrated with speech-language therapy in individuals with post-stroke aphasia.
Although a computer-generated allocation sequence was used to assign participants to groups, key features of a randomized controlled trial—such as allocation concealment, blinding, and prospective trial registration—were not implemented. Accordingly, the study is more appropriately classified as quasi-experimental, reflecting pragmatic and feasibility-focused objectives rather than a fully randomized controlled design (Eldridge et al., 2016; Shadish et al., 2002).
A fully randomized controlled trial and stratified randomization were not feasible due to the limited number of eligible participants and substantial clinical heterogeneity in aphasia subtype and severity, conditions under which strict randomization may increase the risk of group imbalance and reduce clinical feasibility (The RELEASE Collaborators, 2022; Shadish et al., 2002). Participants were recruited from the Speech Therapy Clinic at Khon Kaen Hospital, Thailand, between August and November 2024.
Participants and Sample Size
Participants were adults with ischemic stroke and aphasia with predominant expressive language impairment, receiving outpatient speech-language therapy at a hospital-based clinic in Thailand. Eligibility was based on predominant expressive language impairment rather than strict aphasia syndrome classification, acknowledging the overlap and fluidity of aphasia profiles in clinical practice. Consecutive sampling was used during the study period. The sample reflected the clinical heterogeneity typical of aphasia rehabilitation, including variability in aphasia subtype, severity, and time since stroke (Kertesz & McCabe, 1977; Watila & Balarabe, 2015).
Sample size determination was guided by feasibility considerations rather than formal hypothesis testing, consistent with the exploratory aims of the study. In line with recommendations for pilot and early-phase rehabilitation research, the primary objectives were to assess intervention feasibility, examine outcome variability, and identify preliminary patterns of change to inform future trials (Eldridge et al., 2016; Julious, 2005). The target sample size was informed by prior pilot and small-scale studies of music-based and melodic intonation–based interventions in post-stroke aphasia reporting large within-subject improvements, particularly among individuals with non-fluent aphasia (Conklyn & Meehan, 2018; Raglio et al., 2016), as well as by practical constraints related to patient availability and clinical heterogeneity. All enrolled participants completed the intervention and outcome assessments and were included in the analysis.
Eligibility criteria included age ≥18 years, at least one-month post-stroke, and evidence of predominant expressive language impairment based on a standardized speech–language screening assessment (Supawatrajarugon & Eua-siriratnaphaisan, 2016). Individuals with a documented diagnosis of depression were not eligible, given the potential influence of mood disorders on language and anxiety outcomes (Hilari et al., 2012). Participants were excluded if they demonstrated severe auditory comprehension impairment on the TWAB, which would limit meaningful participation in structured intervention activities (Dardaranda et al., 2017). Withdrawal criteria included medical instability, clinical deterioration during the intervention period, or attendance below 80% of scheduled sessions (Watila & Balarabe, 2015).
Group Allocation
Participants were allocated to either an experimental group (music therapy combined with speech-language therapy) or a comparison group (speech-language therapy alone). Allocation was generated using a computer-based random sequence to reduce allocation bias (Harris et al., 2006; Shadish et al., 2002). Formal allocation concealment procedures were not implemented; however, group allocation was determined prior to baseline outcome assessment to minimize selection bias. Stratified randomization was not employed due to the limited number of eligible participants and substantial heterogeneity in aphasia subtype and severity, as stratification under these conditions may compromise feasibility and group balance (Release Collaborators, 2022; Shadish et al., 2002). Consequently, baseline comparability between groups was assessed descriptively rather than assumed. Although computer-generated allocation was used, the study was not prospectively registered as a randomized controlled trial. Given these real-world clinical constraints and the feasibility-focused aims, the study was therefore labeled as quasi-experimental, consistent with methodological guidance for nonrandomized intervention research embedded in routine clinical care. While random sequence generation was applied to reduce allocation bias, the absence of allocation concealment and other methodological safeguards limits the classification of this study as a randomized controlled trial.
Intervention Procedures
Speech-Language Therapy
Standard speech-language therapy was delivered by two qualified speech-language therapists using a standardized protocol applied consistently across both groups. All participants received conventional speech-language therapy using a traditional approach commonly applied in aphasia rehabilitation. Therapy focused on non-meaningful sound articulation, vowel production, picture naming, and progression to phrase and sentence production, consistent with standard speech-language therapy practices for post-stroke aphasia (Brady et al., 2016; Rose et al., 2014). Sessions were delivered in a standardized format by qualified speech-language therapists.
Music Therapy
Participants in the experimental group received music therapy in addition to speech-language therapy over the intervention period. Music therapy sessions followed a structured protocol delivered by a trained music therapist and were informed by principles of neurologic music therapy and melodic intonation–based approaches (Thaut & Hoemberg, 2025; Thaut & McIntosh, 2014). The intervention consisted of the following components:
Single-syllable vocal exercises, emphasizing breathing control and phonation using vowels and consonants with a steady rhythmic pulse to support vocal initiation and timing (Thaut et al., 2015; Tomaino, 2015). Singing or humming familiar songs, selected based on patient preference, to enhance emotional engagement and facilitate language production through preserved musical and memory networks (Altenmüller & Schlaug, 2015; Särkämö et al., 2016). Rhythmic gap-filling vocalization, in which participants produced target words during intentional pauses in familiar song phrases to promote rhythmic anticipation and natural speech timing (Thaut & Abiru, 2010; Wan et al., 2010). Rhythmic speech production through song, incorporating hand tapping and rhythmic cues to support auditory–motor coordination and speech fluency (Thaut et al., 1999; Thaut & McIntosh, 2014). Word and phrase generation through song, using simple melodies paired with functional daily expressions and gradually increasing linguistic complexity to support lexical retrieval and functional communication (García-Casares et al., 2022; Lim et al., 2013).
While activities were flexibly adapted to individual language abilities, the core therapeutic structure was preserved across sessions to ensure consistency. The vocal training program was collaboratively developed by the first author, a trained music therapist, in consultation with the third author, a speech-language therapy specialist, to ensure alignment with established speech therapy principles. Participants’ hearing status was screened clinically as part of routine care; however, formal audiometric testing and systematic assessment of musical background were not conducted.
Intervention Dose and Contact Time
Participants in the control group received standard speech-language therapy once weekly (45 min per session), consistent with routine outpatient practice. Participants in the experimental group received music therapy twice weekly (30–45 min per session) over six weeks (12 sessions in total), in addition to standard speech-language therapy. One music therapy session per week was scheduled immediately following speech-language therapy within the same visit, while the second session was delivered on a separate day. This schedule reflects real-world clinical logistics and aims to optimize feasibility while minimizing participant burden.
Intervention adherence was monitored using session attendance records, categorized as full attendance, one missed session, or two missed sessions. This study was not designed as a dose-matched comparison of intervention modalities; rather, it represents a pragmatic, dose-augmented feasibility design in which music therapy was integrated alongside routine care to examine implementation, acceptability, and preliminary outcome patterns under increased therapeutic exposure.
Therapist Training and Intervention Fidelity
The interventionist was a trained music therapist with more than 700 h of supervised clinical training across neurological, medical, and psychosocial populations, supporting appropriate adaptation of the intervention for individuals with post-stroke aphasia while preserving core therapeutic intent.
The intervention followed a manualised five-activity protocol targeting vocal initiation, rhythmic speech timing, melodic facilitation, and functional word production. Although activities were tailored to individual language abilities, the core structure, sequencing, and therapeutic goals were applied consistently to support intervention fidelity. Formal fidelity checklists were not employed; however, adherence was supported through a predefined session structure and delivery by a single trained therapist. This represents a methodological limitation and will be addressed through structured fidelity monitoring in future studies. Although participants’ musical backgrounds were not systematically recorded, familiarity was incorporated during Activity 2 by allowing participants to select preferred songs from a predefined list of culturally appropriate Thai songs.
Outcome Measures
Language performance was assessed using the Thai Adaptation of the Western Aphasia Battery (TWAB), which evaluates multiple language domains and yields an Aphasia Quotient (AQ) to indicate aphasia severity (Dardaranda et al., 2017; Kertesz, 2006). Anxiety was assessed using the State–Trait Anxiety Inventory, Form Y-2 (STAI-Y2)
Instrument Quality Assurance
Content validity of the music therapy intervention protocol was established prior to study implementation. The proposed activities were reviewed by the research supervisor and subsequently evaluated by a panel of five experts (two speech-language pathologists, two certified music therapists, and one rehabilitation physician) for relevance and feasibility in post-stroke aphasia rehabilitation. The protocol was revised based on expert feedback, and all five activities achieved a content validity index (CVI) of 1.00, indicating excellent agreement among experts. All outcome assessments were conducted by a single qualified speech-language therapist; therefore, inter-rater reliability was not assessed, and the assessor was not blinded to group allocation due to clinical constraints. This limitation is acknowledged, and results should be interpreted with caution, although the use of standardized assessment instruments was intended to minimize measurement bias.
Statistical Analysis
Data analysis focused on descriptive and exploratory comparisons. Descriptive statistics were used to summarize participant characteristics and outcome measures. Within-group pre–post changes were examined using paired statistical tests, and between-group comparisons were conducted using independent tests applied to change scores, consistent with the exploratory aims and quasi-experimental design of the study and with analytic approaches commonly used in quasi-experimental rehabilitation studies (Harris et al., 2006; Shadish et al., 2002). Given the quasi-experimental design, limited sample availability, and clinical heterogeneity, analyses were conducted to identify patterns and signals of change rather than to establish causal effects. All statistical findings were interpreted with appropriate caution. Exploratory sensitivity analyses were conducted descriptively by aphasia subtype and baseline severity to examine the consistency of outcome patterns, without inferential testing.
Ethical Considerations
The study protocol was approved by the Human Research Ethics Committee of Khon Kaen University (HE662272) and the Human Research Ethics Committee of Khon Kaen Hospital (HE662202). Written informed consent was obtained from all participants or their legally authorized representatives prior to participation.
Methodological Considerations
This study was designed as an exploratory investigation reflecting real-world clinical constraints in aphasia rehabilitation. The absence of stratified randomization and assessor blinding represents acknowledged methodological limitations; however, the design allows for pragmatic evaluation of intervention feasibility and descriptive outcome trends in a heterogeneous clinical population. Reporting was informed by the principles of the TREND statement for nonrandomized evaluations, with transparent description of allocation procedures, intervention delivery, and analytic limitations (Des Jarlais et al., 2004).
Results
Participant Characteristics
A total of 18 participants with post-stroke aphasia were included in the analysis, with nine participants allocated to the control group and nine to the experimental group (Figure 1). Recruitment and retention were high, with no participants excluded or withdrawn during the study period. Session attendance was high in both groups, with all participants attending at least 80% of scheduled sessions (Table 3), and no adverse events related to either intervention were observed.
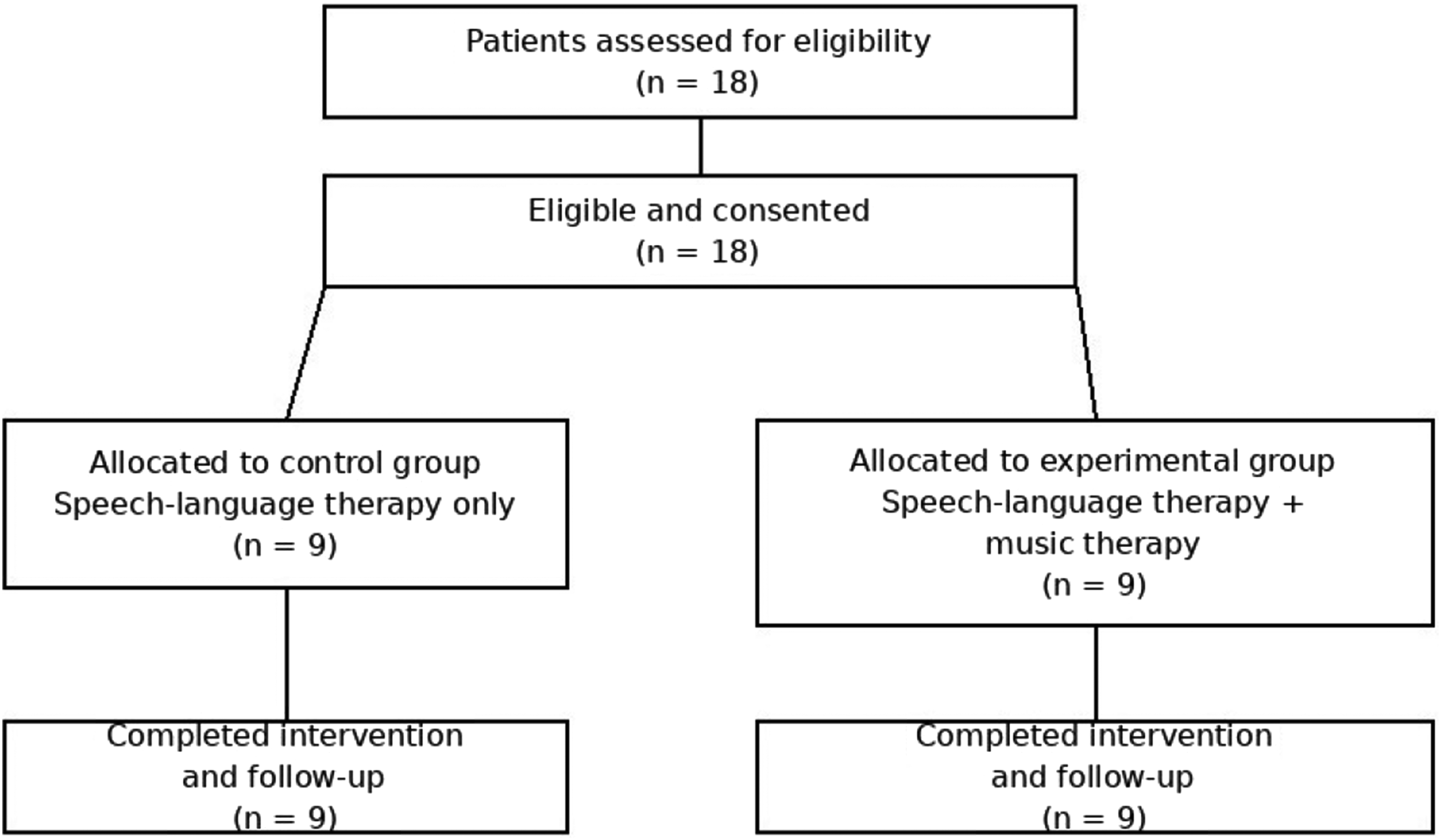
Participant flow diagram.
Baseline demographic and clinical characteristics are presented in Table 1. The mean age was 66.44 ± 10.56 years in the control group and 62.56 ± 13.57 years in the experimental group. Most participants were male, and education level and time since stroke were comparable between groups. No statistically significant between-group differences were observed in baseline demographics, aphasia severity (AQ), or anxiety levels (STAI-Y2).
Baseline Characteristics of Participants.
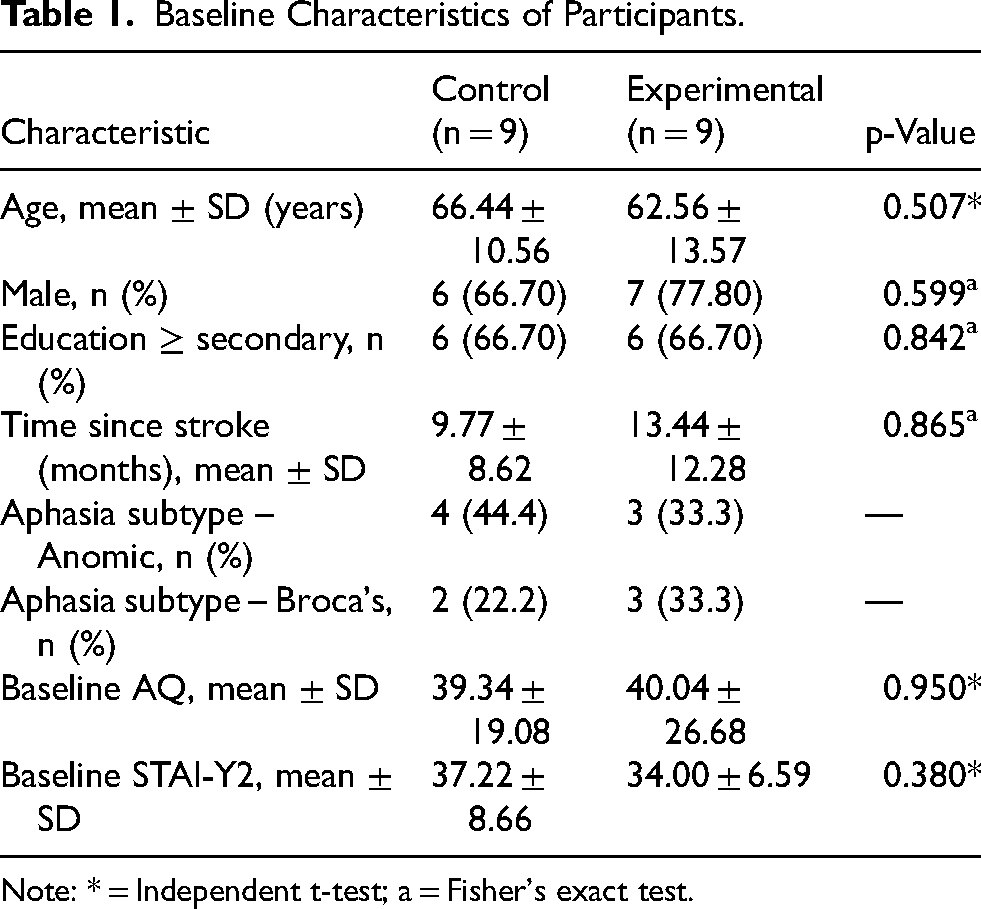
Note: * = Independent t-test; a = Fisher's exact test.
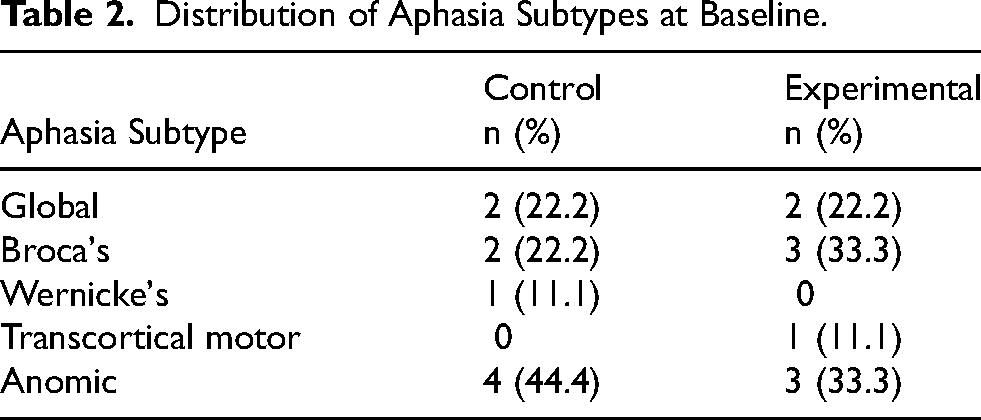
The distribution of aphasia subtypes at baseline (Table 2) demonstrated clinical heterogeneity across both groups, with anomic and Broca's aphasia being the most common subtypes. This heterogeneity reflects the clinical diversity of the sample and supports the ecological validity of the study in a real-world rehabilitation context.
Distribution of Aphasia Subtypes at Baseline.
Intervention Adherence and Attendance as Feasibility Indicators.
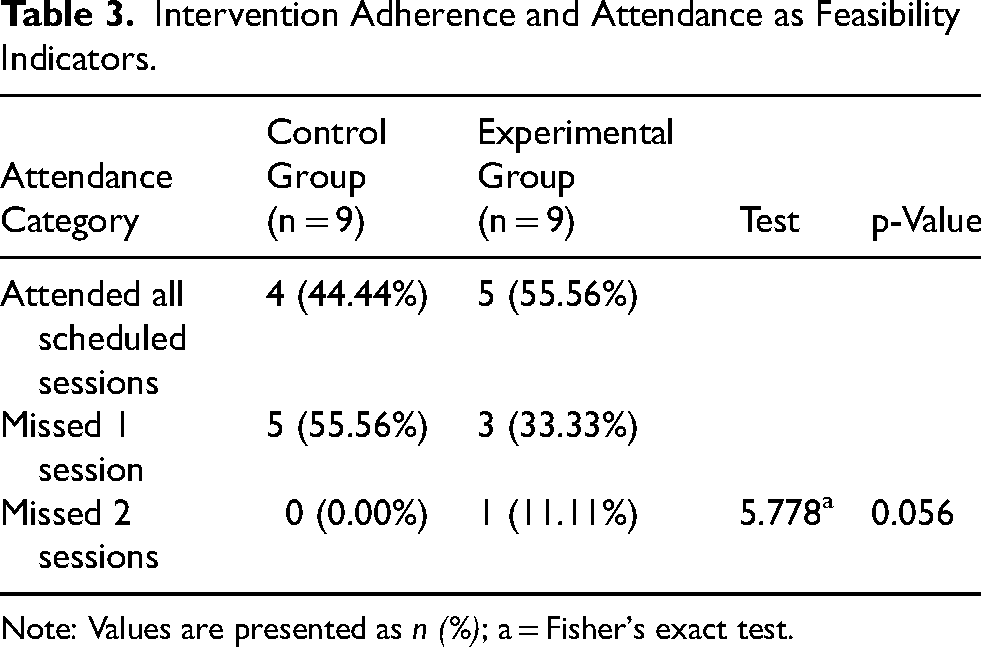
Note: Values are presented as n (%); a = Fisher's exact test.
Within-Group Changes in Language Outcomes
Exploratory within-group analyses revealed improvements in language performance following the intervention period in both groups (Table 4). In the control group, significant pre–post improvements were observed in spontaneous speech, auditory comprehension, naming, and total AQ score. The mean AQ score increased from 39.34 ± 19.08 at baseline to 47.09 ± 21.64 post-intervention (mean difference [MD] = 7.93, 95% CI 4.67–11.19, p < .001).
Within-Group Pre–Post Changes in Language Outcomes
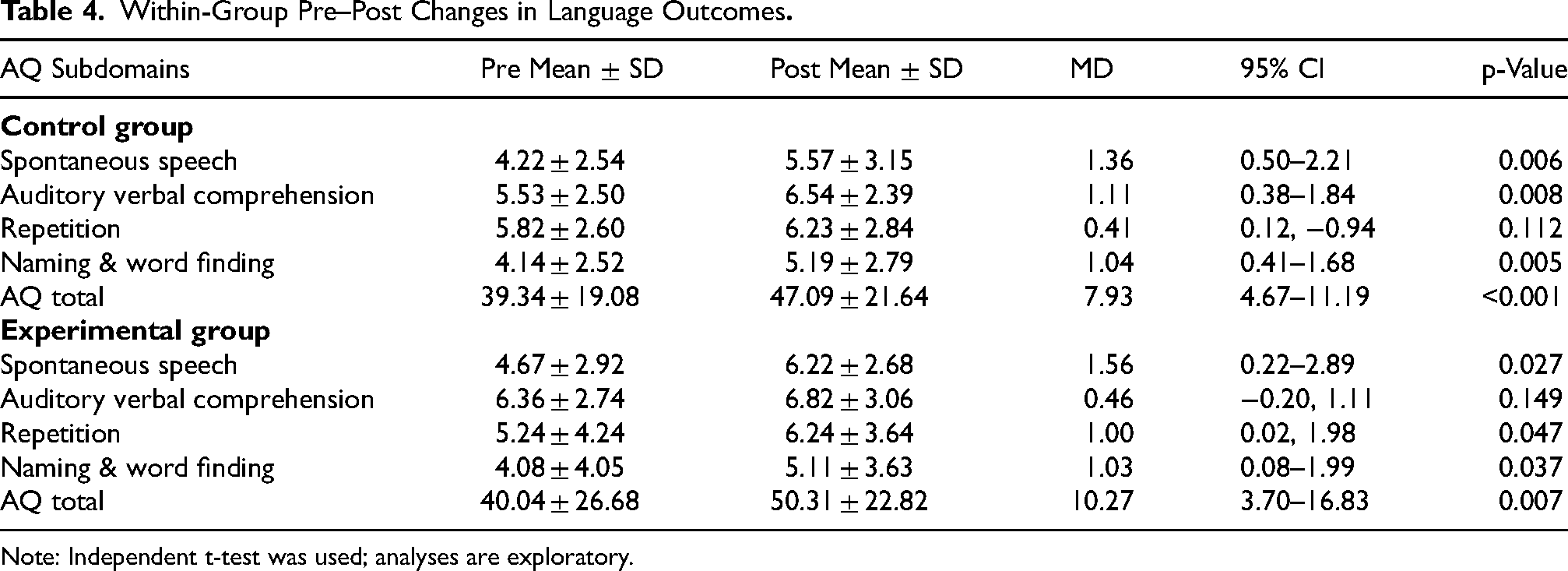
Note: Independent t-test was used; analyses are exploratory.
Similarly, participants in the experimental group demonstrated statistically significant improvements in spontaneous speech, naming, and total AQ score. The AQ score increased from 40.04 ± 26.68 at baseline to 50.31 ± 22.82 after the intervention (MD = 10.27, 95% CI 3.70–16.83, p = .007). Improvements in auditory comprehension were observed descriptively but did not reach statistical significance.
Between-Group Comparisons of Language Change Scores
Between-group comparisons of change scores are presented in Table 5. Although the experimental group demonstrated numerically greater improvements in total AQ scores compared with the control group (ΔAQ = 10.27 vs. 7.74), these differences did not reach statistical significance. No significant between-group differences were observed across AQ subdomains, including spontaneous speech, auditory comprehension, naming, and repetition. These between-group comparisons should be interpreted cautiously, as the study was not designed as a dose-matched comparison and observed differences may reflect increased therapeutic exposure rather than modality-specific effects.
Between-Group Comparison of Change Scores in Language Outcomes.
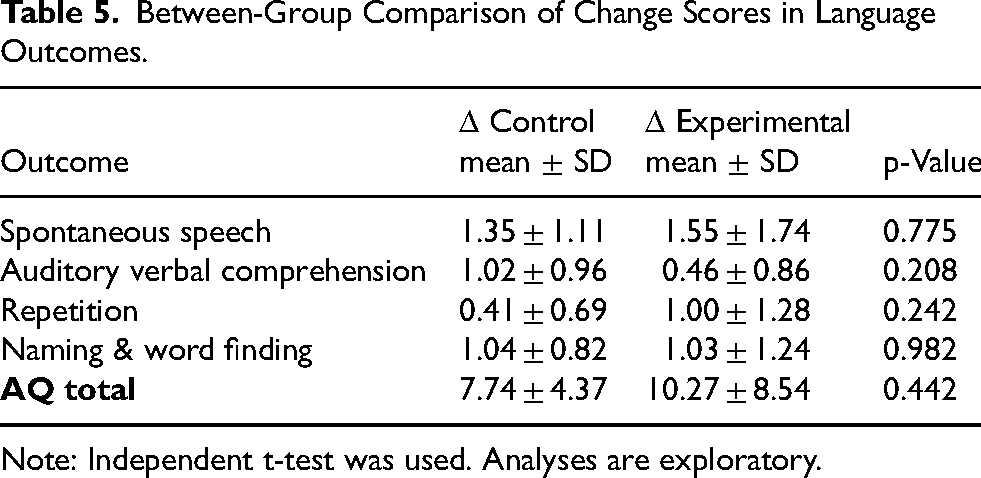
Note: Independent t-test was used. Analyses are exploratory.
Changes in Anxiety Outcomes
Changes in anxiety outcomes within and between groups are summarized in Table 6. Although both groups demonstrated reductions in STAI-Y2 scores over time, neither within-group changes nor between-group differences reached statistical significance. Confidence intervals for STAI-Y2 change scores reflect exploratory estimation and should be interpreted cautiously.
Changes in Anxiety Scores (STAI-Y2) Within and Between Groups.
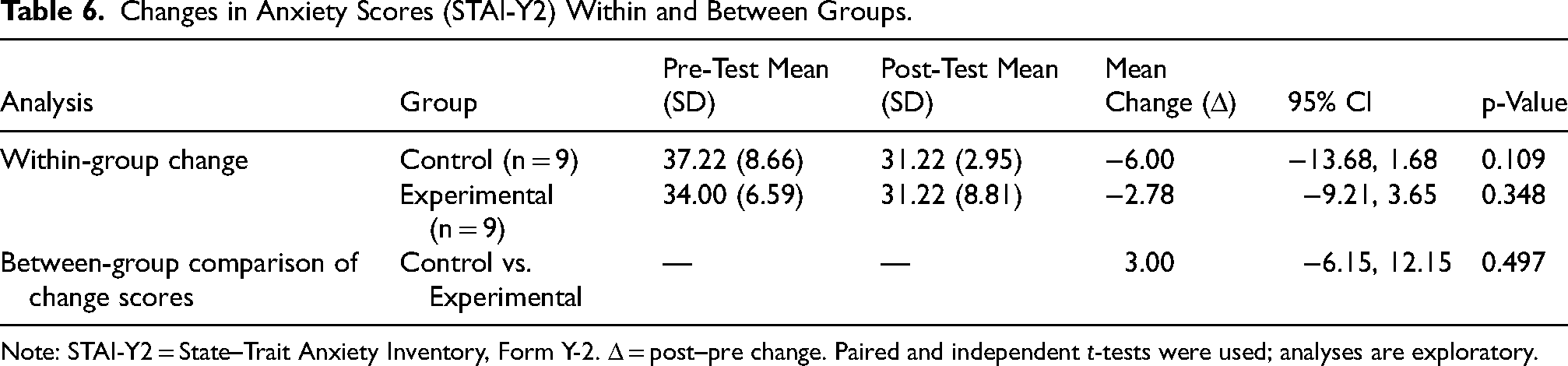
Note: STAI-Y2 = State–Trait Anxiety Inventory, Form Y-2. Δ = post–pre change. Paired and independent t-tests were used; analyses are exploratory.
Standardized Effect Sizes for Language and Anxiety Outcomes
Standardized effect sizes based on change scores are presented in Table 7. Large within-group effects were observed for AQ in both groups, whereas between-group standardized differences were small and not statistically meaningful. Anxiety outcomes showed small to moderate within-group reductions, with no clear between-group separation. All effect size estimates are exploratory and should be interpreted cautiously. An exploratory sensitivity analysis excluding the participant with receptive-dominant aphasia yielded descriptive outcome patterns consistent with the primary analysis (Supplementary Table S1).
Standardized Effect Sizes (Hedges g) for Language and Anxiety Outcomes.
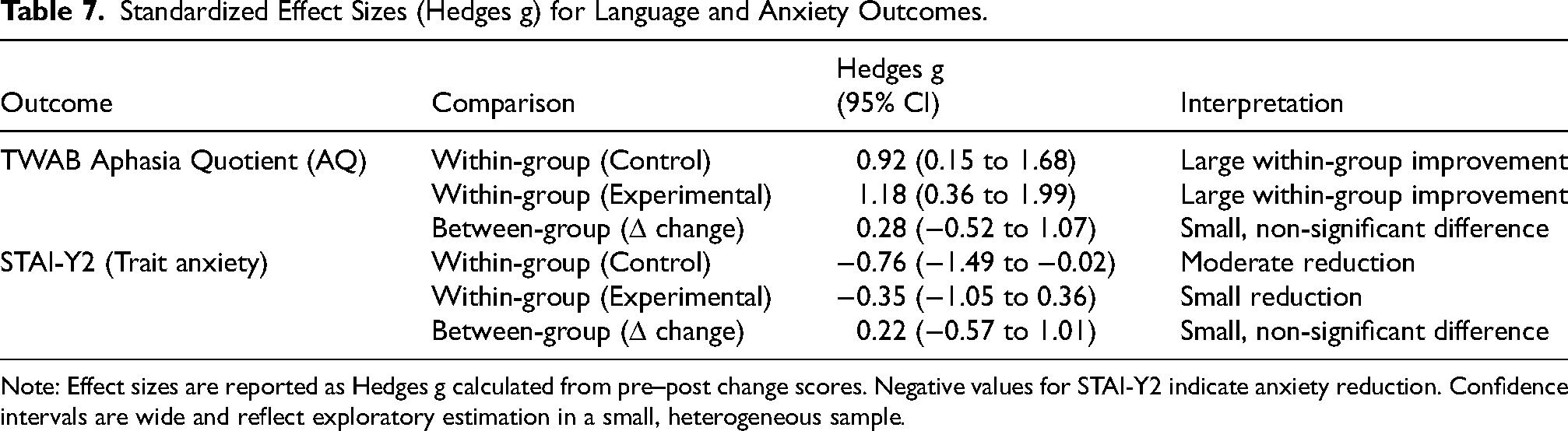
Note: Effect sizes are reported as Hedges g calculated from pre–post change scores. Negative values for STAI-Y2 indicate anxiety reduction. Confidence intervals are wide and reflect exploratory estimation in a small, heterogeneous sample.
Aphasia Subtype Transitions
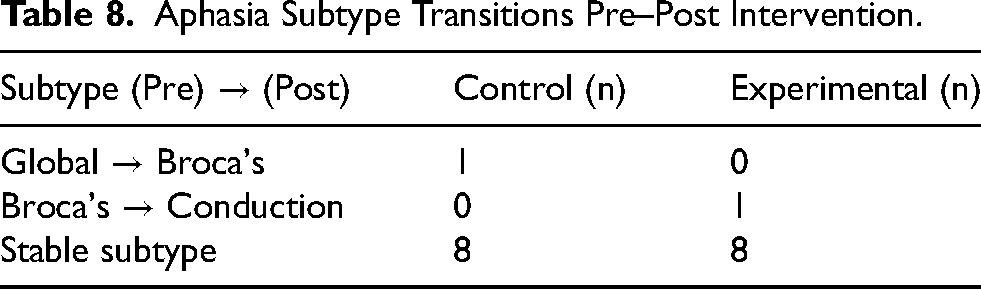
Changes in aphasia subtype classification from pre- to post-intervention are summarized in Table 8. Most participants in both groups retained the same aphasia subtype following the intervention period. Limited subtype transitions were observed, including a shift from global to Broca's aphasia in one control participant and from Broca's to conduction aphasia in one experimental participant. Descriptive sensitivity analyses suggested broadly consistent directions of language change across aphasia subtypes and baseline severity levels, with variability in magnitude (Supplementary Table S1). Illustrative case-level clinical observations contextualizing quantitative outcomes are presented in Supplementary Table S2. These observations are descriptive and intended to highlight individual variability rather than to represent formal qualitative analysis.
Aphasia Subtype Transitions Pre–Post Intervention.
Clinically Observed Communication Changes
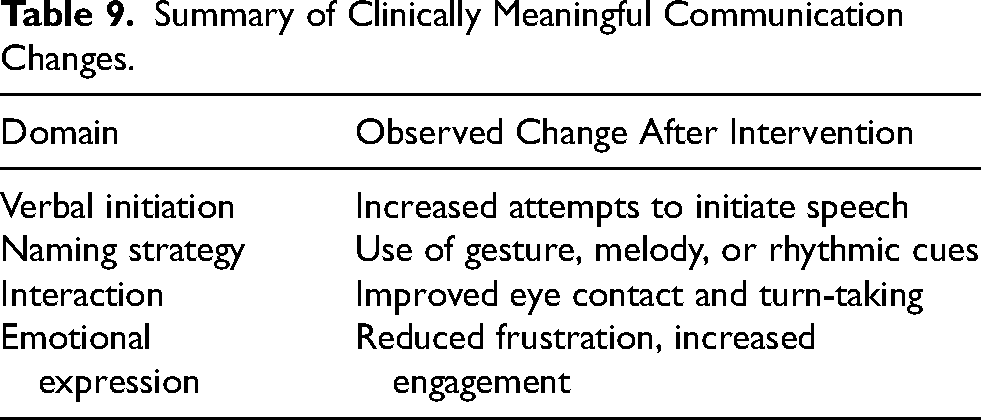
Qualitative synthesis of clinical observations is summarized in Table 9. Across both groups, participants demonstrated clinically meaningful changes in communicative behavior, including increased attempts to initiate verbal expression, greater use of compensatory strategies such as gestures and melodic or rhythmic cues, improved interactional engagement, and reduced frustration during communication tasks. These observations provide contextual support for the quantitative findings.
Summary of Clinically Meaningful Communication Changes.
Discussion
The primary aim of this study was to evaluate feasibility and implementation characteristics rather than to establish treatment efficacy. The present findings support the feasibility of integrating a structured, manualised music therapy protocol into routine speech-language rehabilitation in a real-world outpatient setting. Consistent with feasibility frameworks, the study demonstrates acceptability, implementability, and preliminary outcome variability as key objectives of early-phase intervention research embedded in clinical practice (Bowen et al., 2009; Eldridge et al., 2016; Skivington et al., 2021). The collaborative development of the vocal training program by music therapy and speech-language therapy specialists represents a methodological strength, enhancing content validity and clinical relevance. High session attendance across both groups further supports the practical feasibility and acceptability of integrating music therapy alongside standard care under routine clinical constraints. In the absence of established minimal clinically important difference thresholds for the TWAB Aphasia Quotient, observed changes are described as having potential clinical relevance rather than definitive clinical significance.
Participants in the experimental group received additional music therapy alongside standard speech-language therapy, resulting in increased overall therapeutic contact time. This study should therefore be interpreted as a dose-augmented feasibility design rather than a dose-matched comparison of intervention modalities. Observed outcome patterns likely reflect increased therapeutic exposure rather than modality-specific effects. Accordingly, findings should not be interpreted as evidence of superiority of music therapy, but rather as preliminary signals under conditions of increased therapeutic exposure. Transparent reporting of therapy dose supports appropriate interpretation and informs the design of future dose-matched trials. Potential order effects, including priming or fatigue associated with consecutive sessions, cannot be excluded and were not systematically examined; future research may address these issues through counterbalanced or separated session scheduling. Consistent with prior literature, observed improvements should be interpreted cautiously, as therapy dose is a key determinant of aphasia recovery across intervention types (Bhogal et al., 2003; Brady et al., 2016; Warren et al., 2007).
Exploratory analyses demonstrated within-group improvements in language performance in both groups, with numerically greater gains in the music therapy–augmented arm. However, between-group differences were not statistically significant, and the study was not powered to detect such differences. These findings should therefore be interpreted as descriptive and hypothesis-generating rather than evidence of treatment effectiveness. While the observed trends are broadly consistent with prior literature suggesting potential benefits of rhythmic and melodic cueing (Altenmüller & Schlaug, 2015; García-Casares et al., 2022; Schlaug et al., 2009), they should be interpreted with caution. Given the small sample size and heterogeneity of the sample, the study was not designed to test efficacy or detect statistically significant between-group differences. Although standardized effect sizes appeared large, confidence intervals were wide, reflecting substantial uncertainty in this small sample. Descriptive case-level observations further illustrate individual variability in response (Supplementary Table S2). In line with prior work, changes in aphasia measures are interpreted in relation to functional communication and participation rather than fixed cut-offs (Gilmore et al., 2019; Kertesz & McCabe, 1977).
Anxiety scores decreased over time in both groups, although no statistically significant differences were observed. Interpretation should consider the use of a trait-based measure (STAI-Y2), which, while feasible in individuals with aphasia, may be less sensitive to short-term or session-specific emotional changes (Spielberger, 1983; Thapinta, 1992). Given that music-based interventions may exert immediate or session-level effects, the use of a trait-based measure (STAI-Y2) may have limited sensitivity to transient emotional responses. Measurement of anxiety in post-stroke populations, particularly among individuals with communication impairments, remains methodologically challenging (Lincoln et al., 2013). The selection of STAI-Y2 reflects a pragmatic trade-off between feasibility and measurement sensitivity within the clinical context. Accordingly, the modest and non-significant changes in anxiety may partly reflect limitations of the trait-based measurement approach.
The findings suggest that structured music therapy can be integrated into routine outpatient speech-language rehabilitation workflows with minimal additional resource burden, particularly when aligned with existing therapy schedules. The intervention was delivered using a manualised protocol and required no specialized equipment beyond standard clinical resources, supporting its feasibility and scalability in outpatient settings. Importantly, this study provides practical insights into how music-based interventions may be incorporated into existing rehabilitation workflows in real-world and resource-constrained clinical environments, including a non-Western context. From a service development perspective, implementation may require consideration of therapist training, interdisciplinary coordination, and allocation of session time within existing rehabilitation programs. Such feasibility data may inform planning of scalable music therapy services and support integration into multidisciplinary neurorehabilitation models.
This study should be interpreted within the context of its feasibility-focused design. The findings primarily reflect implementation feasibility, acceptability, and exploratory outcome patterns rather than treatment efficacy. Several methodological limitations, including the quasi-experimental design, absence of allocation concealment and blinding, small sample size, and imbalance in therapy dose between groups, limit causal inference. Outcome variability may also reflect clinical heterogeneity and unmeasured individual factors.
From a clinical and implementation perspective, the findings suggest that structured music therapy can be feasibly integrated into routine speech-language rehabilitation in a real-world outpatient setting. These results provide practical insights into implementation under routine clinical constraints and inform the design of future, methodologically rigorous trials.
Limitations
This study has several limitations. The quasi-experimental design, absence of stratified randomization, and lack of pre-registration limit causal inference. Outcome assessments were conducted by a single, non-blinded assessor without evaluation of inter-rater reliability, introducing potential detection bias. Although random sequence allocation was used, the absence of allocation concealment and blinding may introduce both selection and detection bias. The inclusion of heterogeneous aphasia presentations may have introduced variability in treatment response.
Anxiety was measured using a trait-based instrument (STAI-Y2), which has acceptable reliability and feasibility in aphasia but may be insufficiently sensitive to transient or session-specific emotional responses. The lack of aphasia-adapted measures (e.g., visual scales, proxy ratings, or physiological indicators) further limits sensitivity to short-term emotional change.
Formal fidelity monitoring was not implemented. Although intervention delivery followed a manualised protocol by a trained music therapist, the absence of structured fidelity assessment limits reproducibility. Given the imbalance in therapy dose between groups, findings should be interpreted as reflecting a dose-augmented feasibility condition rather than modality-specific effects. This design inherently limits attribution of outcomes to the intervention modality, as increased therapy intensity may be a primary driver of observed changes. Individual variability may reflect unmeasured factors such as musical background or auditory processing abilities. While speech-language therapy was standardized, contamination through implicit rhythmic or prosodic cueing in the control condition cannot be entirely excluded.
Future Directions
Future studies should adopt dose-matched or factorial designs to isolate modality-specific effects from overall therapy intensity, with stratification or covariate adjustment by aphasia subtype and severity. Blinded outcome assessment and structured fidelity monitoring are recommended to enhance methodological rigor. In addition, structured fidelity monitoring using standardized checklists should be incorporated to enhance reproducibility. Future research should consider examining more clinically homogeneous aphasia subgroups to better understand differential responses to music-based interventions.
For affective outcomes, future research should incorporate state-based or aphasia-adapted measures (e.g., STAI-Y1, visual analogue scales, proxy ratings, or physiological indicators such as heart rate or heart rate variability) to better capture short-term emotional responses. Assessment of hearing status and musical background may help identify moderators of treatment response. Structured feasibility and acceptability metrics should be incorporated to support progression to larger-scale trials and inform implementation strategies, including therapist training, protocol standardization, and integration into multidisciplinary rehabilitation programs.
Conclusion
This study supports the feasibility of integrating a structured music therapy protocol into routine outpatient speech-language rehabilitation for individuals with post-stroke aphasia. Although causal inferences cannot be made, the findings highlight outcome variability and exploratory signals of change in language performance and anxiety that may inform intervention refinement and future research. Further studies employing dose-matched designs, blinded assessment, and sensitive outcome measures are needed to clarify the contribution of music therapy within aphasia rehabilitation.
Supplemental Material
sj-docx-1-nre-10.1177_10538135261465902 - Supplemental material for Feasibility of Integrating Music Therapy into Routine Speech-Language Rehabilitation for Post-Stroke Aphasia: A Real-World Outpatient Study
Supplemental material, sj-docx-1-nre-10.1177_10538135261465902 for Feasibility of Integrating Music Therapy into Routine Speech-Language Rehabilitation for Post-Stroke Aphasia: A Real-World Outpatient Study by Nattapat Taarmat, Benjamas Prathanee, Pornpan Kaenampornpan, Natthasart Unasri and Nichapatr Phutthikhamin in NeuroRehabilitation
Footnotes
Acknowledgements
The authors sincerely thank the individuals with aphasia for their willingness to participate in this research. Their involvement created meaningful value for the field of music therapy by informing the planning and adaptation of therapeutic approaches for diverse individuals living with aphasia.
Ethics Approval
This study was approved by the Human Research Ethics Committee of Khon Kaen University and the Human Research Ethics Committee of Khon Kaen Hospital. Written informed consent was obtained from all participants or their legally authorized representatives.
Author Contributions
NT: Conceptualization; Methodology; Investigation; Data Curation; Formal Analysis; Visualization; Writing – Review & Editing; Project Administration. NP: Supervision; Conceptualization; Methodology; Formal Analysis; Validation; Writing – Original Draft; Writing – Review & Editing. AK: Conceptualization; Methodology; Investigation; Validation; Writing – Review & Editing; BP: Conceptualization; Methodology; Investigation; Validation; Writing – Review & Editing. NU: Data Curation; Formal Analysis; Writing – Review & Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by the Integrated Epilepsy Research Center, Khon Kaen University. The authors gratefully acknowledge this support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Non-Financial Disclosures
The authors declare no conflicts of interest.
Trial Registration
Not applicable.
Supplemental Material
Supplemental material for this article is available online.