
Abstract
Sources of support and quality of life of 50 grandmother-headed families raising grandchildren with and without disabilities were examined. Comparative analyses revealed significant differences between grandmothers raising grandchildren with and without disabilities in regard to sources of support and family quality of life. Informal support was significantly higher for grandmothers raising grandchildren without disabilities. In addition, grandmothers raising grandchildren without disabilities rated satisfaction with all aspects of family quality of life except parenting as significantly higher than grandmothers raising grandchildren with disabilities. Correlational analyses showed a moderate correlation between sources of support and family quality of life for both groups of grandmothers. While total informal social support was significantly correlated with satisfaction ratings of family quality of life for both groups of grandmothers, total formal support was significantly correlated with satisfaction ratings of family quality of life only for grandmothers raising grandchildren with disabilities. Multiple regression analyses revealed a significant relationship between presence of child disability and satisfaction ratings of family quality of life.
Grandparents raising grandchildren is a growing phenomenon that affects 5.8 million children in the United States. The latest census data show that there are 1.6 million children living in grandparent-headed households with no biological parent present (U.S. Bureau of the Census, 2010). In addition, 1 in 10 grandparents will take on the role of primary caretaker to a grandchild for at least 6 months before the child is age 18 (Silverstein & Vehvilainen, 2000). Many children living with grandparents are at risk for or have developmental, cognitive, neurological, behavioral, and/or emotional problems (Kelley, Whitley, & Campos, 2011; Shakya, Usita, Eisenberg, Weston, & Liles, 2012; G. C. Smith & Palmieri, 2007; Whitley & Kelley, 2008) due to prenatal or early life experiences that may have involved drug/alcohol exposure, neglect/abuse, poor nutrition, lack of preventive medical/dental care, and inconsistent or dangerous living conditions (A. B. Smith & Dannison, 2008).
Empirical evidence suggests that regardless of their racial status, grandparents raising grandchildren are negatively affected by their caregiving responsibilities in many areas including social and economic well-being, psychological stress, and physical health (Kelley, Whitley, & Campos, 2013a; Minkler & Roe, 1993; Musil et al., 2011; Neely-Barnes, Graff, & Washington, 2010). Kelley, Whitley, Sipe, and Yorker (2000) and Kelley et al. (2013a) found that fewer family resources, less social support, and poorer physical health were related to greater levels of psychological distress among grandmothers raising grandchildren. Likewise, studies of the long-term effects of grandparent caregiving report high rates of depression, poor self-rated health, and/or frequent presence of chronic health problems, especially among grandmothers (Minkler, Fuller-Thomson, Miller, & Driver, 1997). Custodial grandparents’ experiences can influence parenting and child outcomes, often negatively (Campbell & Miles, 2008).
Grandparents raising grandchildren with developmental disabilities often face unique and ongoing challenges (Lecavalier, Leone, & Wiltz, 2006). The demands of assuming a parental role later in life are exacerbated by raising a grandchild who is experiencing physical, emotional, or behavioral difficulties (Conway, Jones, & Speakes-Lewis, 2011; Grant, 2000; Sands & Goldberg-Glen, 2000) as children with disabilities typically require more time and attention than children without disabilities. The persistence and strength of these negative effects can compromise positive coping and enjoyment of daily life (Bailey et al., 2006). Moreover, grandparents may under-report levels of emotional distress for fear of being viewed as incapable of raising grandchildren (Force, Botsford, Pisano, & Holbert, 2000).
Grandparent caregivers of children with disabilities often experience heightened needs. McCallion, Janicki, Grant-Griffin, and Kolomer (2000) reported that grandparents caring for a child with a disability received less social support than did other family caregivers. Grandparents also reported experiencing higher levels of role strain, financial strain, and life disruption than either custodial grandparents raising grandchildren without disabilities or traditional grandparents (Emick & Hayslip, 1999). Gallagher, Kresak, and Rhodes (2010) examined the perceived needs of grandmothers who were primary caregivers of grandchildren with disabilities. Findings confirmed that grandmothers had unique needs including informational and respite, as well as needs for strategies to deal with issues related to their grandchild’s disability.
Grandparents raising grandchildren, especially those with disabilities, often rely on social supports, spiritual support, and formal support (Seligman & Darling, 2007). Theoretically, social support is seen as the resource that buffers the relationship between caregiver stress and well-being (Crowther & Rodriguez, 2003). Gerard, Landry-Meyer, and Roe (2006) found that grandparents dealing with numerous child health problems and frequent stressors related to common parenting tasks benefitted from receiving formal support, which reduced role-related stress and enhanced quality of life. Also, grandparents responded positively to assistance in the form of support groups, health services, legal and social services, as well as to recreational programs for their grandchildren.
Sources of informal and formal support, however, are often limited or unavailable; thus, social isolation and inadequate social support networks are key problems for custodial grandparents (Hayslip & Kaminski, 2005a; Shakya et al., 2012). Because grandparent caregiving has been linked to negative outcomes such as decreased peer-network interaction and social isolation, depression, and lowered life satisfaction (Fuller-Thomson & Minkler, 2000; Kelley et al., 2000; Musil et al., 2011), it is important to identify social support resources that may facilitate positive development among grandparent caregivers (Landry-Meyer, Gerard, & Guzell, 2005). The extent to which the emotional and psychological support needs of grandparents are addressed will influence the overall functioning of the grandchild and the family (Schalock & Alonso, 2002). Likewise, by examining family quality of life, professionals may be better able to identify possible challenges and quality of life supports for families, especially grandparents raising grandchildren (Purcell, Turnbull, & Jackson, 2006).
Therefore, examining the mediating effects of social support on familial well-being or quality of life, the focus of this study, may help professionals identify and enhance sources of support for all grandparent caregivers. Furthermore, while researchers have looked at grandparents raising grandchildren, few have focused on grandparents raising grandchildren with disabilities (Kolomer, McCallion, & Janicki, 2002). The research questions were as follows:
Method
In this study, we investigated the sources of support and satisfaction ratings of family quality of life for 50 grandmothers. We also examined the potential impact of four family characteristics: (a) age of grandmother, (b) educational level of grandmother, (c) age of grandchild, and (d) presence of child disability on sources of support and family quality of life. For the purposes of this study, grandmother referred to a grandmother or great grandmother who was raising one or more grandchildren, while a child with a disability was defined as an individual who currently received services under PL 108-446, the Individuals With Disabilities Education Improvement Act of 2004 (IDEA; 2004), Americans With Disabilities Act (ADA; 1990), or Section 504 of the Rehabilitation Act (1973), and had an Individualized Education Plan (IEP) or 504 Plan. Grandmothers of children receiving only speech-language services through their IEP were excluded from the study.
Participants
The sample was comprised of 50 English-speaking grandmothers who considered themselves to be the primary caregiver for at least one grandchild. Twenty-six (52%) grandmothers were raising at least 1 grandchild with a disability while 24 (48%) grandmothers were raising grandchildren without disabilities. To be eligible, the grandchild’s biological parents had to be absent from the household and grandchildren needed to be between the ages of 3 and 12 years. If grandmothers were raising more than one child with a disability, the oldest child with a disability meeting the age requirement was chosen as the participant child.
Recruitment
Grandmothers were recruited from public agencies that focus on aging and other statewide agencies serving children with disabilities in a 35 county area in the northwest sector of a southern state. Agencies were given copies of the invitation letters and the criteria for inclusion in the study. Agency representatives delivered invitation letters to potential participants. The first author contacted grandmothers recruited by the agencies after permission was obtained. No other contact was made with the recruiting agencies or the grandmothers following the individual data collection session.
Measures
Family support was measured by the Family Support Scale (FSS; Dunst, Jenkins, & Trivette, 1986), a 19-item self-report measure that assesses the helpfulness of sources of support to families raising a young child with disabilities or at risk for poor developmental outcomes (Dunst, Trivette, & Deal, 1988). The FSS captures five major sources of support: (a) Kinship Support (2 items), (b) Spouse/Partner Support (3 items), (c) Informal Support (6 items), (d) Programs/Organizations (4 items), and (e) Professional Services (4 items). Respondents rate each item on a five-point Likert-type scale ranging from not at all helpful (1) to extremely helpful (5). Scores on the first four sources of support subcategories are combined to obtain the Informal Social Support Score; the sum of the Professional Services subcategory is the Formal Support Score. The Total Family Support Scale score is obtained by summing the Informal Social Support score and the Formal Support score. Higher scores on both the subscales and the total scale are reflective of increased social support. In the present study, per scoring guidelines, family support was also analyzed and reported using the mean of each of the five subscales of support. Because this instrument was designed for parents of children with developmental disabilities, two wording changes were made so that items addressed grandparent caregivers rather than parents. The researcher was given written permission to use the FSS with grandparents (C. Dunst, personal communication, October 26, 2011). Internal consistency reliability for the FSS was .77, split-half reliability was .77, and test–retest reliability was .75, while internal consistency reliability for the FSS subscales were Kinship (.56), Spouse/Partner Support (.67), Informal Support (.72), Programs/Organizations (.53), and Professional Services (.56; Dunst, Jenkins, & Trivette, 1984).
Family quality of life was measured with the Beach Center Family Quality of Life Scale (FQOL; Hoffman, Marquis, Poston, Summers, & Turnbull, 2006; Summers et al., 2005), which assesses families’ perceptions of their satisfaction with different domains of family quality of life. The FQOL Scale is a 25-item self-report questionnaire that can be used with families of children of varying ages, disability types, and severity. It is comprised of five subscales that include (a) Family Interaction (6 items), (b) Parenting (6 items), (c) Emotional Well-Being (4 items), (d) Physical/Material Well-Being (5 items), and (e) Disability-Related Support (4 items). Each item is rated on a five-point Likert-type scale ranging from (1) very dissatisfied to (5) very satisfied. For the present study, only families raising children with disabilities completed the Disability-Related Support subscale. For families raising children without disabilities, a slightly revised version of the FQOL Scale (previously used by Zuna, Selig, Summers, & Turnbull, 2009) was administered. This version omits the four items pertaining to family members with disabilities. FQOL total score is obtained by summing the subscale scores. Individual subscale scores are obtained by calculating the mean for each of the five subscales. Higher scores on both the subscales and the total scale are reflective of greater satisfaction ratings of family quality of life. Family quality of life was measured and reported using the summation of the satisfaction ratings for the overall FQOL Scale and the mean satisfaction ratings for each of the five subscales. High convergent validity, internal consistency, and test–retest reliability have been demonstrated with this scale among families of children with and without disabilities (Beach Center on Disability, 2006; Poston et al., 2003; Zuna, Turnbull, & Summers, 2009). Zuna, Selig, and colleagues (2009) found that Cronbach’s alpha for the overall FQOL Scale was excellent (.92), which is similar to Cronbach’s alpha for the disability-only sample (.88) that was previously reported by Hoffman and colleagues (2006). In addition, alphas for the four individual subscales were in the acceptable range (.75-.85) and were also similar to the range of consistency indices reported by Hoffman et al. (.74-.90), thus demonstrating that families of children without disabilities perceive the FQOL construct in a similar fashion as families of children with disabilities.
Procedures
Grandmothers were contacted by email or phone and asked if they had a grandchild between the ages of 3 and 12. Only two potential participants were excluded from participating in the study because none of their grandchildren were between the ages of 3 and 12. Grandmothers were also asked, “Does your grandchild have a disability,” and if they replied yes, they were asked who determined and/or diagnosed the disability and what services, if any, their grandchild received at school. Only those grandmothers who reported their grandchild had an IEP and/or was diagnosed with a disability by a medical doctor were placed in the grandmothers raising grandchildren with disabilities group.
The first author met individually with each participant to obtain written informed consent as well as to collect the participant’s responses to the two instruments. These data collection sessions were held in settings chosen by the participant, such as the participants’ homes, public libraries, restaurants, or senior centers. The informed consent and instruments were read aloud to account for any issues of low literacy. The definition of “family” was taken from the instructions of the FQOL Scale, typed on an 8.5 × 11 inch paper, and laminated (see appendix). The definition was then read to grandmothers in the study prior to the implementation of the FQOL Scale. When administering the standardized instruments, the order was alternated to prevent an order effect. Participants received a US$10 gift card for their time.
Results
Demographics
Participants ranged in age from 39 to 85 years of age, with a mean age of 60.16 years (see Table 1). Thirty-eight percent of participants reported a high school diploma, while 44% reported some college (see Table 1). The majority of participants (54%) reported annual household incomes of US$30,000 or less. The number of grandchildren in their care ranged from 1 to 5, but the majority (n = 43) were raising one or two grandchildren. Grandchildren in their care ranged from 2 to 21 years of age, with a mean age of 8.8 years. The mean length of time the grandchildren were in the care of participants was 7.24 years (range = 1-12 years). Of the index grandchildren, 64% were male and 36% were female.
Characteristics of Grandmothers Raising Grandchildren With and Without Disabilities
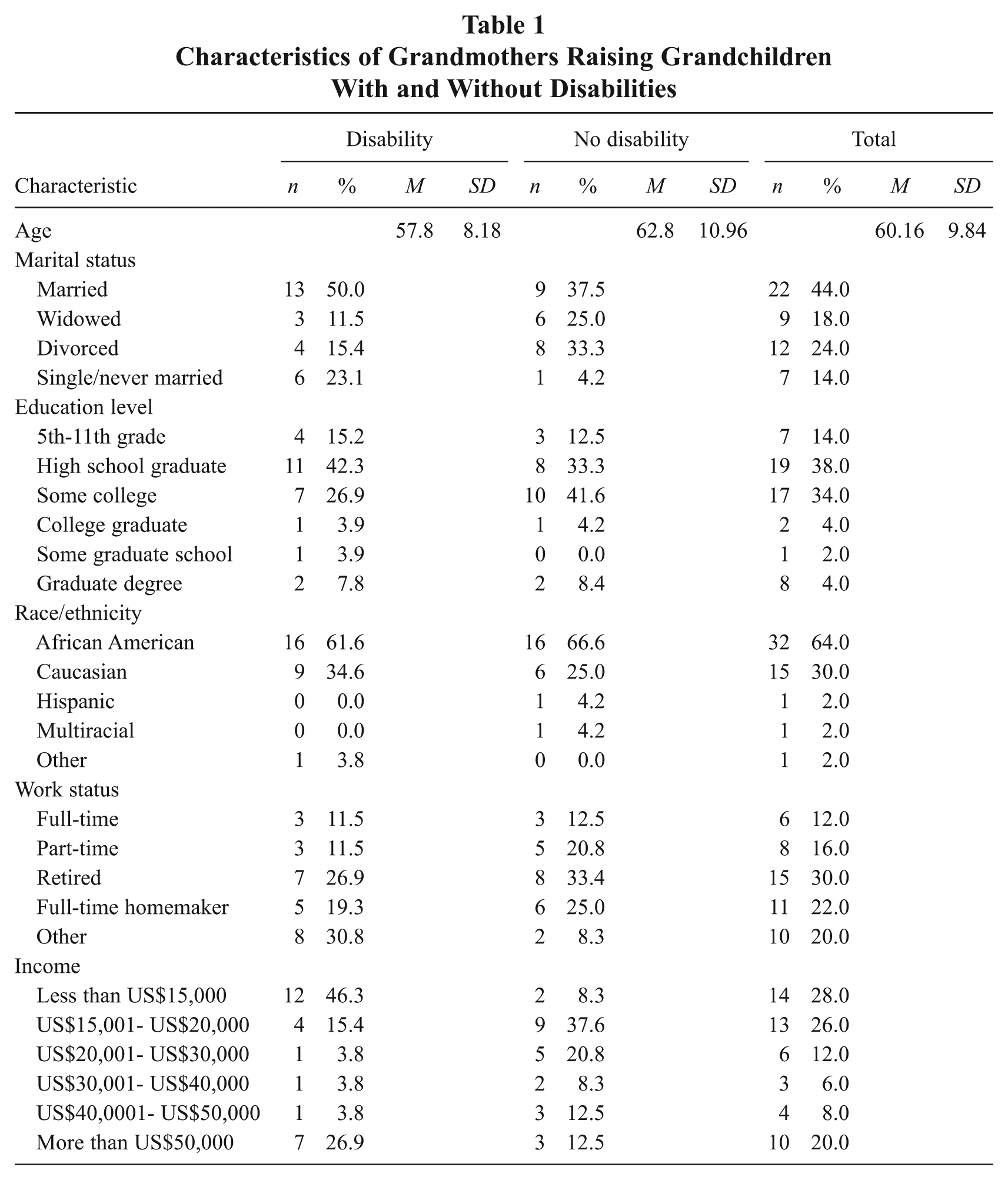
Between-group comparisons were made between participants raising grandchildren with and without known disabilities. T-tests revealed no statistically significant group differences in grandmother age, grandchild age, number of grandchildren living in the home, or length of time as caregiver. Chi-square analyses revealed no group differences in participant educational attainment, race/ethnicity, or marital status. Analysis by Chi Square Test of Association did, however, reveal differences, χ2 (5, N = 50) = 14.61, p = .012, between presence of child disability and income. Proportionately more participants in the disability group (61.7%) had incomes of US$20,000 or less compared with the non-disability group (45.9%). Chi Square Test of Association, χ2 (1, N = 50) = 6.61, p = .010, also showed a significant association between presence of child disability and gender of grandchild with proportionately more males (65.6%) than females (27.8%) in the disability group.
The majority of grandchildren with disabilities were reported by grandmothers to have multiple disabilities (50.0%). Other disability categories included attention deficit hyperactivity disorder/attention deficit disorder (ADHD/ADD; 27.0%), fetal alcohol syndrome (7.8%), behavior disorder (3.8%), cerebral palsy (3.8%), fragile X (3.8%), and learning disability (3.8%). With regard to a question asking, “What is the severity of your grandchild’s disability?” 42.3% of children were rated by grandmothers as having a mild level of severity, 35% as having a moderate level, 19% as having a severe level, and 4% were rated as having an unknown level of severity.
Sources of Support
Our first research question compared the sources of support reported by grandmothers raising grandchildren with and without disabilities. Results of findings on the Family Support Scale are displayed on Table 2. No significant difference was found between grandmothers raising grandchildren with and without disabilities on the Family Support Scale total score, F(1,48) = 2.089, p > .05. A significant difference was found between the mean ratings of the two groups on the Informal Support subscale, F(1,48) = 5.535, p < .05). Informal support was significantly higher for grandmothers raising grandchildren without disabilities (M = 2.35, SD = 0.96) compared with grandmothers raising grandchildren with disabilities (M = 1.67, SD = 1.06). There were no statistically significant differences on the remaining subscales.
Comparison of Means for Family Support Composite and Subscales by Presence of Disability
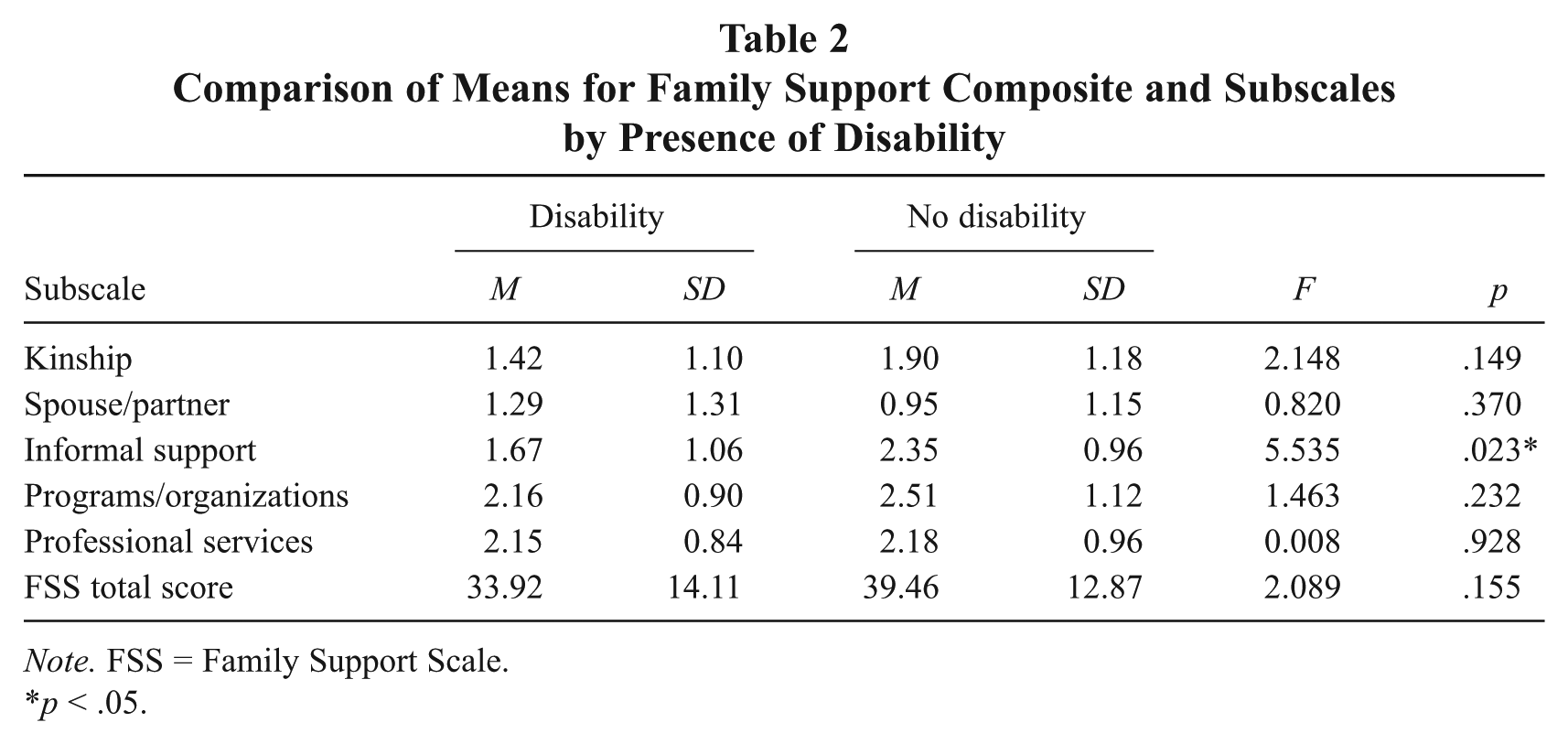
Note. FSS = Family Support Scale.
p < .05.
Family Quality of Life
Our second research question sought to compare the satisfaction ratings of family quality of life reported by grandmothers raising grandchildren with and without disabilities. A significant difference was found between the mean satisfaction ratings of grandmothers raising grandchildren with and without disabilities, F(1,48) = 8.019, p < .05, on the Family Quality of Life Scale (see Table 3). Grandmothers raising grandchildren without disabilities rated satisfaction with total family quality of life significantly higher (M = 87.08, SD = 10.40) than grandmothers raising grandchildren with disabilities (M = 75.58, SD = 17.21). Significant differences were found between groups on the Family Interaction subscale, F(1,48) = 6.239, p < .05, the Emotional Well-Being subscale, F(1,48) = 5.096, p < .05, and the Physical/Material Well-Being subscale, F(1,48) = 7.260, p < .05, with grandmothers raising grandchildren without disabilities rating satisfaction significantly higher than grandmothers raising grandchildren with disabilities. No significant difference was found between the mean satisfaction ratings on the Parenting subscale for the two groups, F(1,48) = 3.048, p > .05.
Comparison of Means for Family Quality of Life Composite and Subscales by Presence of Disability
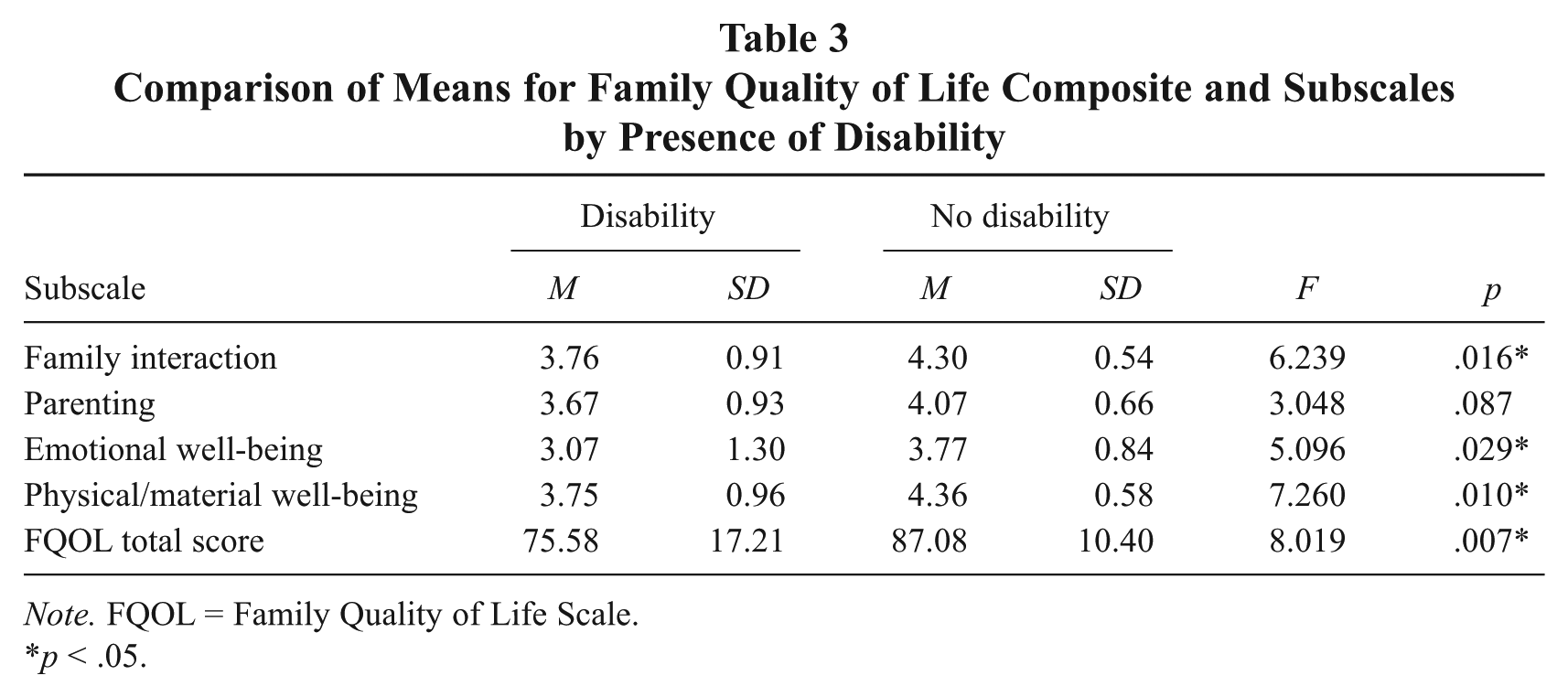
Note. FQOL = Family Quality of Life Scale.
p < .05.
Differences With Disabilities
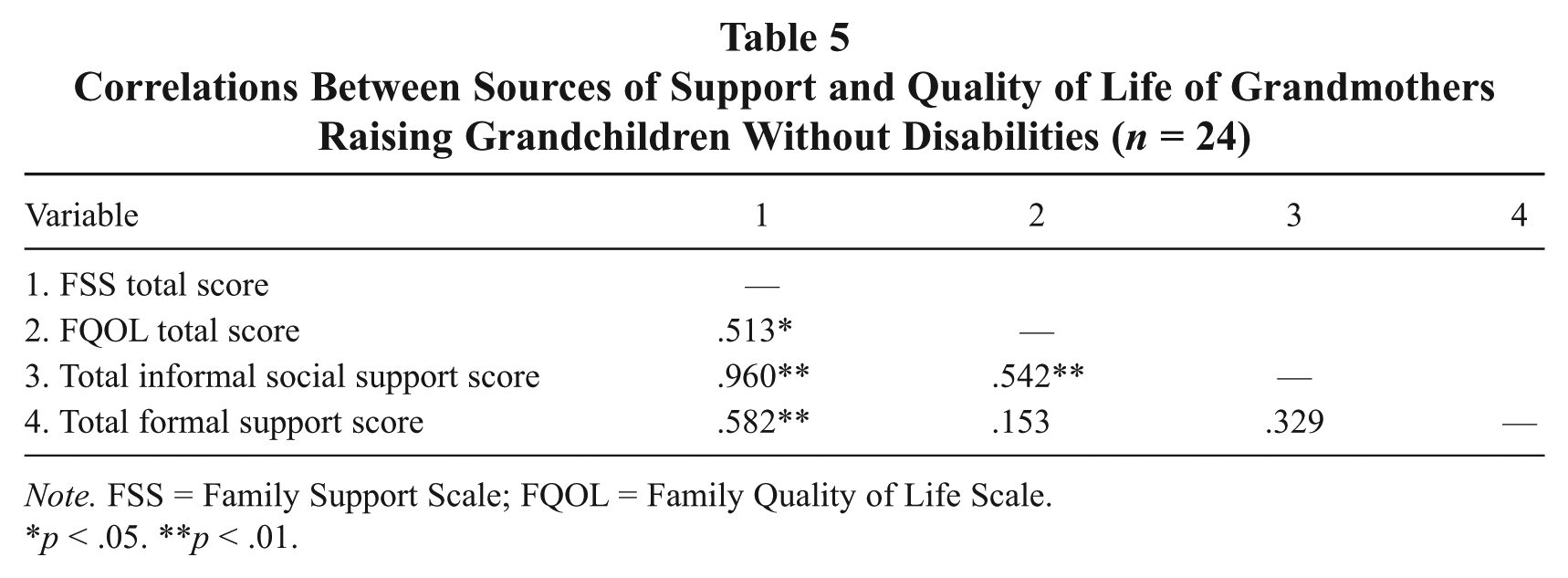
Our third research question sought to determine whether the relations among sources of support and family quality of life differed for grandmothers raising grandchildren with or without disabilities. Correlation analyses revealed a relationship among sources of support and family quality of life for both grandmothers raising grandchildren with and without disabilities. For grandmothers raising grandchildren with disabilities (see Table 4), sources of support were moderately correlated with satisfaction ratings of family quality of life, including the disability-related subscale (r = .624, p < .01). For grandmothers raising grandchildren without disabilities (see Table 5), sources of support were moderately correlated with satisfaction ratings of family quality of life (r = .513, p < .05). Degrees of correlation are described by Cohen (1977) as high (above .75), moderate (.50-.75), and low (.25-.50).
Correlations Between Sources of Support and Quality of Life of Grandmothers Raising Grandchildren With Disabilities (n = 26)
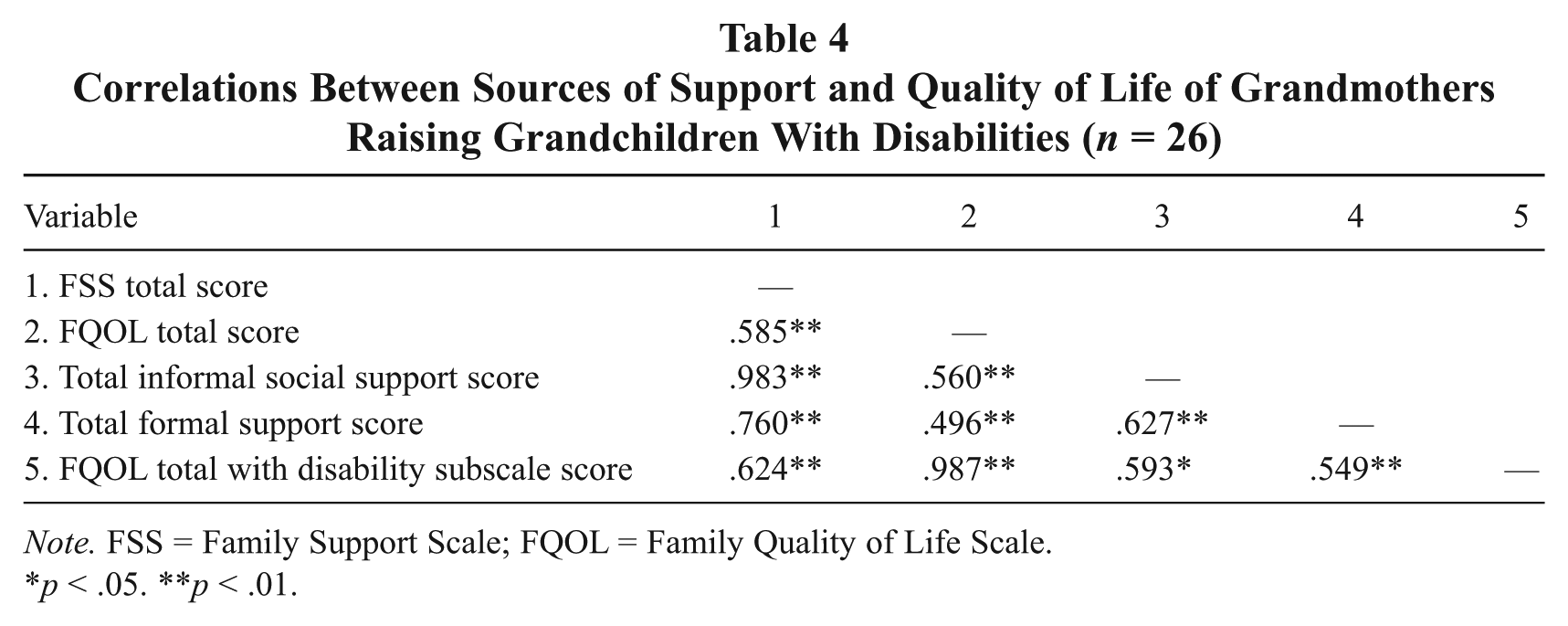
Note. FSS = Family Support Scale; FQOL = Family Quality of Life Scale.
p < .05. **p < .01.
Correlations Between Sources of Support and Quality of Life of Grandmothers Raising Grandchildren Without Disabilities (n = 24)
Note. FSS = Family Support Scale; FQOL = Family Quality of Life Scale.
p < .05. **p < .01.
Total informal social support was significantly correlated with satisfaction ratings of family quality of life for both grandmothers raising grandchildren with disabilities (r = .560, p < .01) and grandmothers raising grandchildren without disabilities (r = .542, p < .01). However, these two groups of grandmothers differed with regard to their ratings of the helpfulness of formal support. Total formal support was significantly correlated with satisfaction ratings of family quality of life for grandmothers raising grandchildren with disabilities (r = .549, p < .01), as seen in Table 4. No significant correlation was found between total formal support and satisfaction ratings of family quality of life for grandmothers raising grandchildren without disabilities (r = .153, p > .05), as seen in Table 5.
Predictor Factors
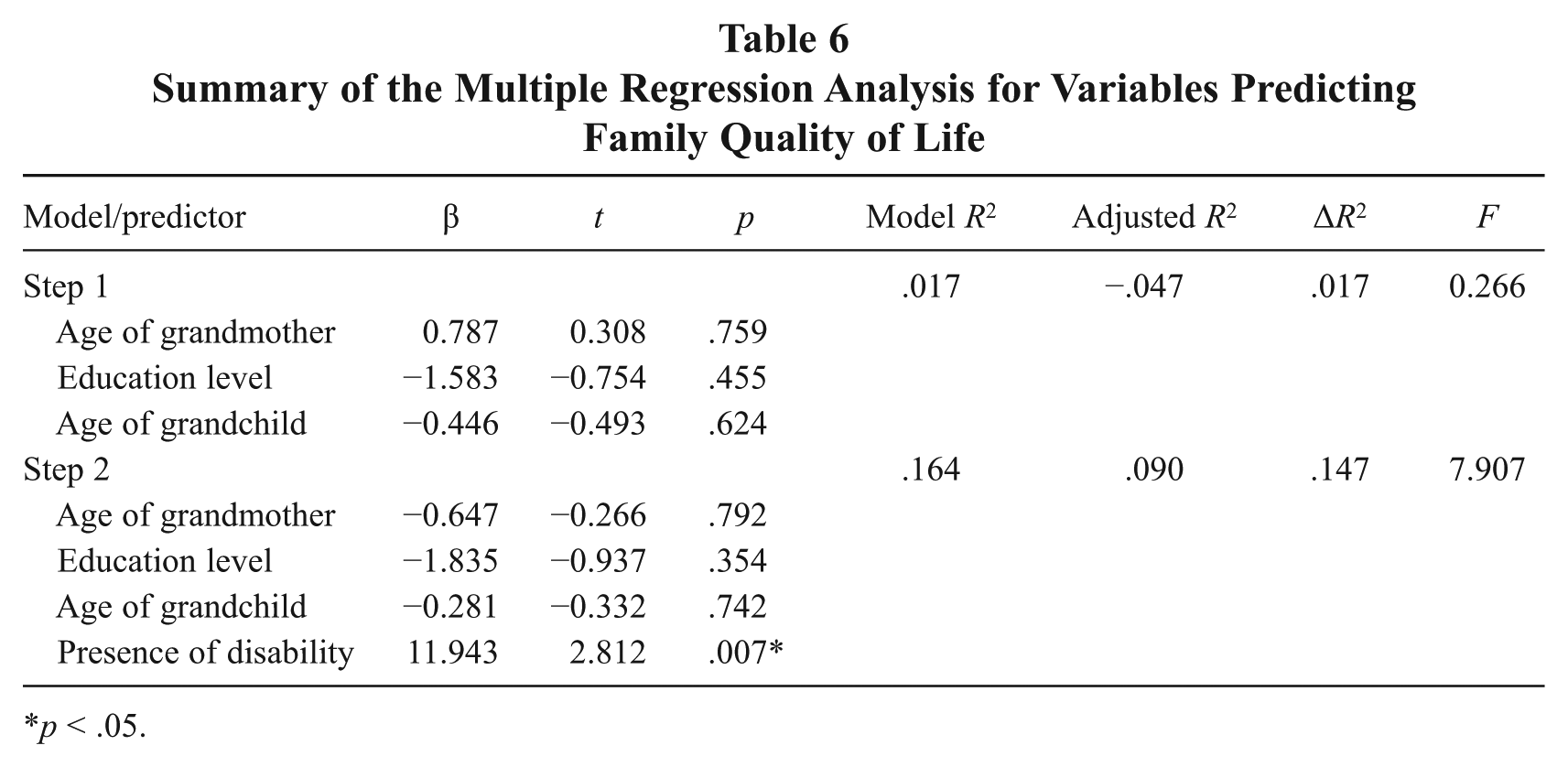
Our fourth research question sought to compare which factors predict family supports and quality of life for grandmothers raising grandchildren with and without disabilities. Multiple regression analyses were used to identify the strongest predictors of family quality of life (total satisfaction with FQOL), as presented on Table 6. As a control strategy, age of grandmother, education level of grandmother, and age of grandchild were entered in Step 1 of the regression. Presence of child disability was entered in Step 2. There was a significant relationship between presence of child disability and satisfaction ratings of family quality of life (t = 2.812, p < .05). Presence of child disability did contribute to the overall relationship with family quality of life, F(1,45) = 7.907, p < .05, increasing the R2 by .147. Presence of child disability accounted for 15% of the unique variance.
Summary of the Multiple Regression Analysis for Variables Predicting Family Quality of Life
p < .05.
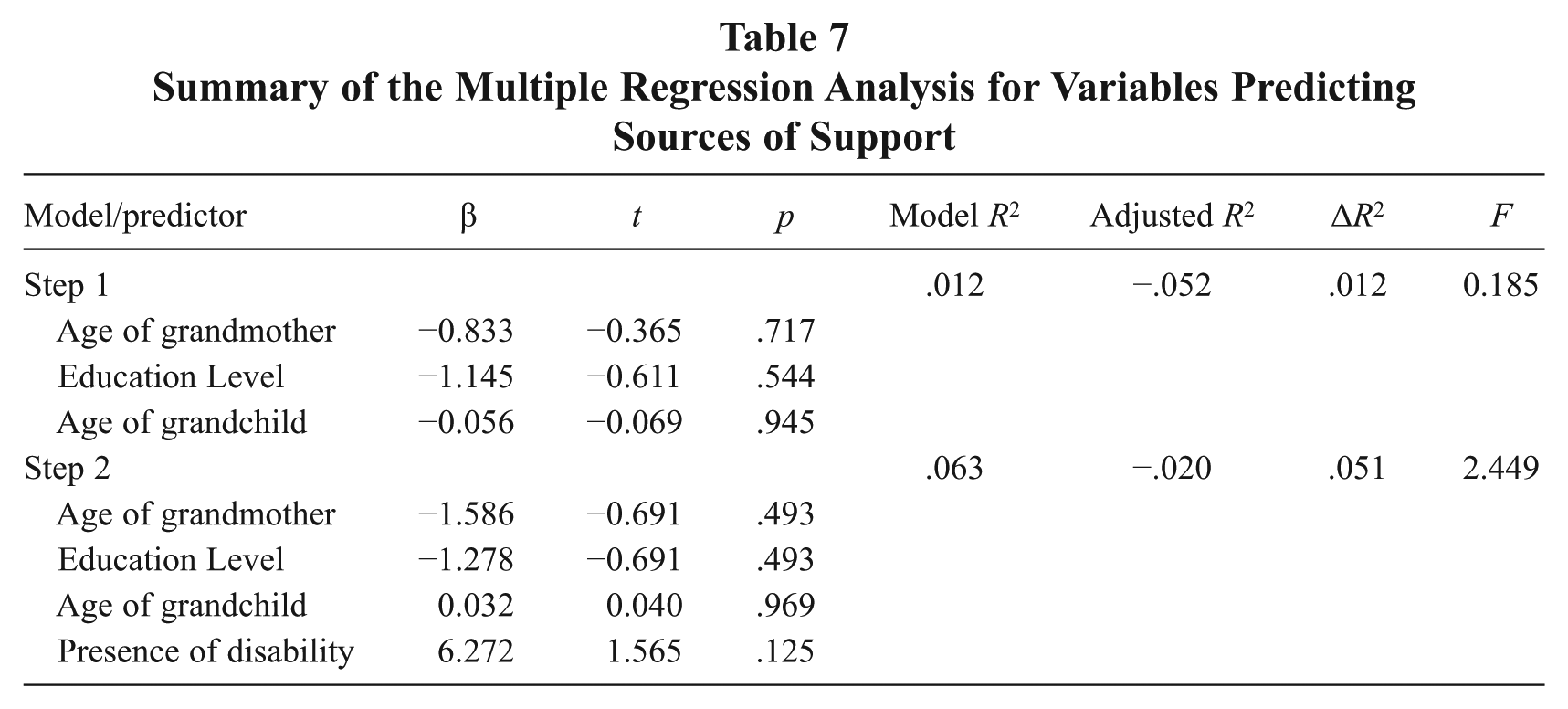
Multiple regression analyses were used also to identify the strongest predictors of sources of support (see Table 7). As a control strategy, age and education level of grandmother and age of grandchild were entered in Step 1 of the regression model. Presence of disability was entered in Step 2 of the regression. Presence of child disability did not contribute significantly to the overall relationship with sources of support, F(1,45) = 2.449, p > .05.
Summary of the Multiple Regression Analysis for Variables Predicting Sources of Support
Discussion
Grandmothers raising grandchildren without disabilities reported significantly more informal support than grandmothers raising grandchildren with disabilities. This result is consistent with that of previous researchers (Emick & Hayslip, 1999; McCallion et al., 2000) who found grandparents raising grandchildren with emotional, behavioral, and learning difficulties received less social support than those caring for grandchildren without disabilities. Caring for grandchildren with disabilities may be more demanding than caring for grandchildren without disabilities. Family and friends may not be able, or willing, to provide support for grandmothers raising grandchildren with disabilities, especially when the grandchildren exhibit challenging behaviors. Therefore, it is plausible that grandmothers raising grandchildren with disabilities view sources of informal support as less helpful than grandmothers raising grandchildren without disabilities.
Both groups of grandmothers reported professional services as only sometimes helpful. This finding supports previous researchers (Hayslip & Kaminski, 2005b; Janicki, McCallion, Grant-Griffin, & Kolomer, 2000; McCallion et al., 2000) who have shown that grandparents could not access, did not seek, or did not utilize formal sources of support. Researchers have found that accessing and navigating the formal service network presents a multitude of challenges for grandparents who are raising grandchildren (Grant, 2000; Janicki et al., 2000; McCallion et al., 2000). It may be that formal networks are not equipped to meet the unique needs of grandparent caregivers or that grandparents are not aware of available services. But some grandparents may not access services because they feel that they can take care of things themselves or do not want others to know about their grandchild’s disability. Still others may not have the motivation nor the time or energy to enlist the services they need. Janicki and colleagues (2000), for example, found that many grandparents experienced stress when attempting to secure help or specialty services related to their grandchild’s disabilities and, therefore, were low users of existing services even though they reported a high need. Such perspectives on generational differences and behavior patterns and attitudes need further investigation in future research.
When compared with grandmothers raising grandchildren with disabilities, those raising grandchildren without disabilities reported greater satisfaction with each aspect of family quality of life except parenting. Similarly, Zuna, Turnbull, et al. (2009) found that families of children who are typically developing tended to have higher family quality of life ratings than families of children with disabilities.
Hayslip and Kaminski (2005a) found that grandparents raising grandchildren are often socially isolated from their peers and friends, which can affect their emotional well-being. Grandmothers raising grandchildren with disabilities may be even more socially isolated, because either they do not have or do not access their own social network due to the special needs of their grandchildren. Therefore, it is not surprising that grandmothers raising grandchildren with disabilities in the present study would rate themselves less satisfied with that aspect of family quality of life. The grandchild’s disability might preclude these grandmothers from participating in family events or activities, resulting in decreased contact with the family. This could also explain why grandmothers raising grandchildren with disabilities rated satisfaction with family interaction significantly lower than grandmothers raising grandchildren without disabilities. Likewise, in the present study, grandmothers raising grandchildren with disabilities rated satisfaction with physical/material well-being significantly lower than grandmothers raising grandchildren without disabilities. It may be that the increased financial expenses of raising a grandchild with disabilities contributes to increased levels of personal distress, which could affect grandmothers’ physical health.
Another interesting finding was the significant positive correlation between sources of support and satisfaction ratings of family quality of life for both grandmothers raising grandchildren with and without disabilities. Researchers have found that support from family and friends (i.e., informal support) enhances emotional well-being (Davis & Gavidia-Payne, 2009), especially in families of children with disabilities (King, King, Rosenbaum, & Goffin, 1999). Our findings show that having more helpful sources of support, especially informal support, may increase satisfaction ratings of family quality of life.
Based on our findings, raising a grandchild with a disability is significantly related to caregiver satisfaction with family quality of life. Not surprisingly, those raising grandchildren with disabilities reported less satisfaction. Presence of disability, however, did not significantly affect the helpfulness of support grandmothers received from either formal or informal sources. These results provide support for Bronfenbrenner’s (1979) ecological theory, which emphasized the significance of the external environment on families’ and children’s well-being. Informal support has shown the strongest relationship to any number of child, parent, and family outcomes (Dunst, 2000). Therefore, the provision or mobilization of supports and resources could improve family quality of life (Dunst & Bruder, 2002), especially for families raising grandchildren with disabilities.
Implications
Results of this study underscore the critical need to provide support for grandmothers raising grandchildren, especially those raising grandchildren with disabilities. Program strategies that strengthen grandmothers’ social support and family resources are essential to increasing family quality of life, which can promote positive family and child outcomes (Bailey et al., 2006). The extent to which families have adequate formal and informal support systems is highly associated with successful adaptation (Crnic & Stormshak, 1997), and maintaining healthy social networks is an essential component for positive adaptation in the family system (Ylven, Bjorck-Akesson, & Granlund, 2006).
A major emphasis of increasing positive adaptation for grandmothers raising grandchildren should be strengthening and building natural support systems, as well as promoting the acquisition of knowledge and skills that make a family more competent. Researchers (Kelley, Whitley, & Campos, 2010, 2013b; Kelley, Whitley, & Sipe, 2007) have found that one way to accomplish this is to use strengths-based case management and group support services that build on strengths grandparents already possess. In addition, support groups for grandparents and/or grandchildren may also enhance the general well-being of grandparents while providing a nurturing environment for their grandchildren. Grandparents who have utilized support groups have reported that group meetings are helpful in obtaining information about available services, in providing a forum in which to share concerns about their current caregiving situation, and in reducing feelings of isolation (Cox, 2003; McCallion, Janicki, & Kolomer, 2004). However, attendance at support group meetings is difficult for grandparents raising grandchildren with disabilities, due to the special needs of the grandchildren. With a limited social support network, grandparents raising grandchildren have fewer resources available for child care. Efforts should be made to increase the amount of support provided to grandparents raising grandchildren with disabilities.
Appropriate policies, programs, and outreach efforts are needed to better address the needs of grandparents raising grandchildren. Involving faith-based organizations, senior centers, public health departments, community mental health centers, divisions of child and family services, and educational institutions in these interventions may help ensure that grandparents receive the support they require to increase their family quality of life. A positive family quality of life should be an outcome of policies and services for families (Bailey et al., 1998; Turnbull, Blue-Banning, Turbiville, & Park, 1999).
Limitations
There are several limitations to this study, including the representativeness of the sample and the reporting of specific disabilities and severity level. The participants in this study were from the northwest sector of a southern state and may not be representative of other sections of the state or country. That said, 50 grandparents is one of the larger studies completed and one of the only ones to compare grandparents raising grandchildren with and without disabilities. In addition, it is impossible to know whether grandmothers who did not participate differed in their perspectives on caregiving from those who did choose to enroll in the study. Because participants were recruited from settings where they were already receiving services, it is not known whether they differ from those who do not access available resources.
Another limitation to be noted is that while disability of the child and the rating of severity level were reported by the grandparent, including verification that the child had an IEP and/or had been diagnosed with a disability by a medical doctor, the actual IEP or medical evaluation was not reviewed by the researchers. Also a large majority (73%) of grandchildren with disabilities, as reported by the grandmothers, fell into one of two disability categories: ADHD/ADD or multiple disabilities. Thus, the results may not be generalizable to grandmothers raising grandchildren with different disabilities. Given that severity was based on the grandmothers’ perception, it is not known whether this perception contributed to their satisfaction ratings of family quality of life. Future studies could look at grandmothers raising grandchildren with a wide variety of disabilities to see whether there are impacts related to the disability. It would also be helpful to know what services grandparents or their grandchildren are receiving, including financial resources (e.g., from a child welfare agency or developmental disabilities agency), as well as any health and mobility needs of the grandparents.
Future Research
Responses for sources of support and satisfaction ratings of family quality of life were provided only by the grandmother caregivers in this study. Instead of basing inferences about the family on the report of only one person, it could be important to obtain responses from grandfathers as well as grandmothers to examine whether there are differences in their perceptions of family quality of life or the availability of sources of support. Different family members may utilize different sources of support, which could affect their emotional well-being.
Including the reason for the caregiving situation in the demographic data could provide invaluable information regarding family quality of life. Grandparents assume care of their grandchildren due to diverse and unpredictable circumstances such as substance abuse, violence and/or neglect, or death of a parent. These differing circumstances can put the grandparents at risk for psychological distress and most likely affect their well-being (Ross & Aday, 2006; Shakya et al., 2012). It would be beneficial to professionals to know the effect of the reason for the assumption of care on the sources of support and family quality of life to provide the appropriate support and services needed by the grandparents.
Research of this type that directly targets grandparents is challenging to accomplish, both in terms of finding and recruiting grandparents, and the logistics of meeting with them. In our present research, where we interviewed 50 grandmothers, the process itself of finding and meeting individually with the grandmothers targeted over six agencies in an 11-county area of one state. Data collection took over a year, including weekends and evenings, with travel of over 600 miles. The findings and results are certainly worth the effort, but future researchers need to be aware of the resources needed in terms of time and logistics to accomplish such grass-roots research.
Conclusion
As the definition of a family continues to expand beyond children and their biological parents, researchers and practitioners must likewise broaden their views of what constitutes a family. This expanded view must include grandparents as primary caregivers. Results of this study underscore the importance of grandmothers who are raising grandchildren having access to informal supports, especially when they are raising grandchildren with disabilities. Having more impactful sources of informal support may increase satisfaction with family quality of life for grandmothers raising grandchildren. Professionals can promote family access to resources through referrals to community-based services and by helping families strengthen their support networks. Strengthening grandparents’ support networks is likely to have a positive effect on family quality of life, including improved child and family outcomes.
Footnotes
Appendix
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.