
Abstract
Family outcomes of early intervention (EI) for autism spectrum disorder (ASD) have received limited research attention to date. This study explored potential predictors of family outcomes and EI perceived helpfulness on the Family Outcomes Survey–Revised, utilizing an adapted double ABCX framework. Participants were 97 mothers of children aged 4 to 5 years (M = 60.47 months; SD = 6.62; 87.6% male) participating in the Longitudinal Study of Australian Students with Autism (LASA). Parent and family factors were significant predictors, whereas child characteristics were largely nonsignificant beyond variance explained by parent and family factors. Findings highlight the importance of parent and family factors when considering family outcomes of EI and whether parents perceive benefits from their engagement with EI services. Overall, a shift in the focus of EI outcome evaluation is indicated, which views parents and families as meaningful to overall optimal EI outcomes.
Keywords
Autism spectrum disorder (henceforth autism) is a spectrum neurodevelopmental disorder characterized by pervasive differences or difficulties in reciprocal social communication and interaction, and repetitive and restrictive behavior/interests (American Psychiatric Association, 2013) that affects approximately 1 in 59 children (Baio et al., 2018). Autism characteristics manifest in childhood, with diagnosis possible from 2 years of age (Kleinman et al., 2008) and most common in the preschool years (Randall et al., 2016). Early intervention (EI) is often suggested to be critical for improving outcomes for children on the autism spectrum (National Research Council, 2001) and has been associated with improvements in child communication, social skills, and challenging behavior (for a review see Wong et al., 2015). Parental involvement in EI is recommended and encouraged within policy and practice; however, scarce research to date has focused on outcomes of EI for families, with child outcomes dominating the literature (Karst & Van Hecke, 2012).
Impact of Autism Diagnosis on Parents and Families
While parenting a child on the autism spectrum can be a rewarding experience, it also can present multifaceted challenges (Pottie & Ingram, 2008). Parents of children on the autism spectrum report greater levels of parenting stress compared with parents of typically developing children and children with a range of neurodevelopmental disabilities (Adams et al., 2018), intellectual disability, and cerebral palsy (for a review see Hayes & Watson, 2013). A higher prevalence of depression and anxiety (e.g., Eisenhower, Baker, & Blacher, 2005) and poorer overall well-being (Blacher & McIntyre, 2006) have been documented in parents of children on the autism spectrum compared with typically developing controls. High levels of parenting stress have been linked to a greater number of child autism characteristics (Zaidman-Zait et al., 2014), more frequent or severe challenging behaviors (Davis & Neece, 2017), and poorer communication skills (Harrop, McBee, & Boyd, 2016). Mutually influential relationships between these factors have been proposed (Zaidman-Zait et al., 2014), which reciprocally influence parent and family functioning (Jellett, Wood, Giallo, & Seymour, 2015).
The emotional impact of raising a child on the autism spectrum across the family system has also been investigated (for review see Karst & Van Hecke, 2012). Research suggests that families of a child on the autism spectrum report less satisfaction with their Family Quality of Life (FQoL) than families of a child with typical development or Down syndrome (Hsiao, 2018). Maternal reported FQoL has been linked to child externalizing behaviors, family sense of coherence (FSOC), coping strategies, and access to social support (McStay, Trembath, & Dissanayake, 2014; Pozo, Sarriá, & Brioso, 2014), with lower levels of child externalizing behavior and higher levels of FSOC and coping found to predict greater FQoL. In addition, Jellett et al. (2015) found that maternal depressive symptoms determined the relationship between child challenging behaviors and family functioning and suggest that this reflects the indirect negative impact of parental overburden upon the family due to the challenges arising from behaviors of their child on the autism spectrum.
Research has identified associations between raising a child on the autism spectrum and various additional family stresses (Randall & Parker, 1999). Additional practical demands that influence the family system include significant time pressures, potential financial strain, increased provision of supports (developmental and educational), and necessary child-advocacy (Woodgate, Ateah, & Secco, 2008). Research suggests that the financial burden of raising a child on the autism spectrum predicts child treatment outcomes (i.e., developmental outcomes), with low SES families, who have reduced available financial resources, reporting poorer outcomes for their child (Gabriels, Hill, Pierce, Rogers, & Wehner, 2001). The broader influence of SES has also been reported (Pickard & Ingersoll, 2016), including the negative impact of reduced access to social support on lower SES families (Boyd, 2002). Given the complex nature of the associations proposed between child, parent, and family factors, it stands to reason that researchers should consider EI outcomes at each of these levels.
EI for Children on the Autism Spectrum
Intervention within the early years of development targeting the specific characteristics of autism (e.g., language skills, reciprocal attention, and restrictive behavior patterns) is strongly emphasized in both policy and practice in Australia (Prior & Roberts, 2012) and internationally (e.g., National Autism Center [NAC], 2015; National Institute for Health and Care Excellence [NICE], 2013; U.S. Department of Education, 2018). This message places pressure upon parents to engage in various forms of EI for their young children, including developmental-, behavioral-, and learning-based approaches identified as effective in the short term for attaining improved child outcomes (NAC, 2015; Prior & Roberts, 2012; Wong et al., 2015). International guidelines provide key practices for providers, including a parent focus that recognizes the central role of families in children’s lives and measurement and evaluation by EI services from child, family, and community perspectives (e.g., Early Childhood Intervention Australia, 2016; NICE, 2013). However, despite these recommendations, evaluation of outcomes of EI generally center on the child (Karst & Van Hecke, 2012). The impact and perceived benefits of EI on parents and the whole family and the factors that can influence such perceptions therefore warrants further exploration in the research literature.
Family Outcomes of EI
According to Bailey et al. (2006), family outcomes represent “benefits experienced by families as a result of services received” (Bailey et al., 2006, p. 228). Bailey et al. suggest that families of children with disabilities should be viewed as recipients of EI services due to the critical roles they play in children’s development and the dynamic nature of the family context. The concept of family outcomes of EI was not specifically defined prior to Bailey et al.’s (2006) study conducted via the Early Childhood Outcomes Center (ECO) with the support of the U.S. Office for Special Education Programs. Lack of specification precipitated the development of the Family Outcomes Survey (FOS; Bailey et al., 2006), which was later amended to the Family Outcomes Survey–Revised (FOS-R; Bailey et al., 2011). Both measures were developed with extensive U.S. national stakeholder inputs. Five broad outcomes were identified: (a) families understand their child’s strengths, abilities, and needs; (b) families know their rights and advocate effectively for their child; (c) families help their child develop and learn; (d) families have support systems; and (e) families are able to gain access to desired services and activities in their community (Bailey et al., 2006). These outcomes serve as a framework by which U.S. government bodies can monitor whether EI provision is benefiting families of children with disabilities and the extent of the benefits received.
Due to the relative novelty of the measure, knowledge and understanding regarding family outcomes measured by the FOS-R are still in infancy. The importance and validity of the FOS-R in assessing outcomes of EI for families of children on the autism spectrum has also been supported with a U.S. sample (Wainer, Hepburn, & McMahon Griffith, 2017). Furthermore, emerging research has tested the psychometric features of the FOS-R and investigated attainment of FOS-R family outcomes for children with disabilities, and caregivers’ perceptions on the extent to which EI has served their needs, across Singapore (Poon, Ooi, Bull, & Bailey, 2014) and Japan (Ueda, Yonemoto, & Bailey, 2015). The FOS-R has been used previously as a measure of family outcomes for children with disabilities on the autism spectrum in the Australian context (Adams, Keen, Heussler, Wicks, & Roberts, 2019). However, this study simply described the FOS-R family outcomes and did not explore factors that may predict or influence whether families reach such outcomes following EI.
Double ABCX Model of Family Adaptation
Prior research centered on EI for those with a diagnosis on the autism spectrum has largely been atheoretical, with EI outcome variables for parents and families often excluded from investigations. Thus, models that assist in understanding factors affecting outcomes have been underutilized in the family outcomes and EI literature. The double ABCX model of family adaptation (McCubbin & Patterson, 1983) is an established framework for investigating the relationships between factors that influence various outcomes for parents and families of children. The model is underpinned by the proposition that family adaptation and outcomes, measured in terms of psychopathology (e.g., stress symptoms) and/or overall well-being (e.g., quality of life), are the product of a dynamic, ongoing process that is influenced by multiple factors, including individual experience of crisis and stress, characteristics of the child, and available family support resources (Paynter, Riley, Beamish, Davies, & Milford, 2013). This framework sits within broader ecological models (e.g., biopsychosocial, ecological systems) by including individual-level biological (e.g., child characteristics), psychological (e.g., coping styles), and social (e.g., external/social support) as important influences on family outcomes (Bronfenbrenner, 1979).
Previous research supports the utility of the double ABCX model for investigation centered on parents and families of children on the autism spectrum across racially diverse families, ages, and countries (e.g., Manning, Wainwright, & Bennett, 2011; McStay et al., 2014; Paynter et al., 2013; Stuart & McGrew, 2009). An interplay of factors that affect family adaptation and outcomes (X) under stressful circumstances is posited (McStay et al., 2014). These include the stressor (A) and pileup (i.e., accumulation) of additional demands or stressors (aA), internal (B) and external (bB) resources, responses to the stressor (C), and the availability of effective coping strategies (cC). The current study employed an adapted version of the framework to explore predictors of family outcomes of EI in children on the autism spectrum, utilizing variables of interest across components of the model (see Figure 1). Factors included in the adapted model were chosen in line with previous research (Boyd, 2002; Davis & Neece, 2017; Gabriels et al., 2001; Harrop et al., 2016; Hayes & Watson, 2013; Pickard & Ingersoll, 2016; Zaidman-Zait et al., 2014) as noted above. As the current study was a preliminary, exploratory investigation, direct effects between variables were of sole interest.
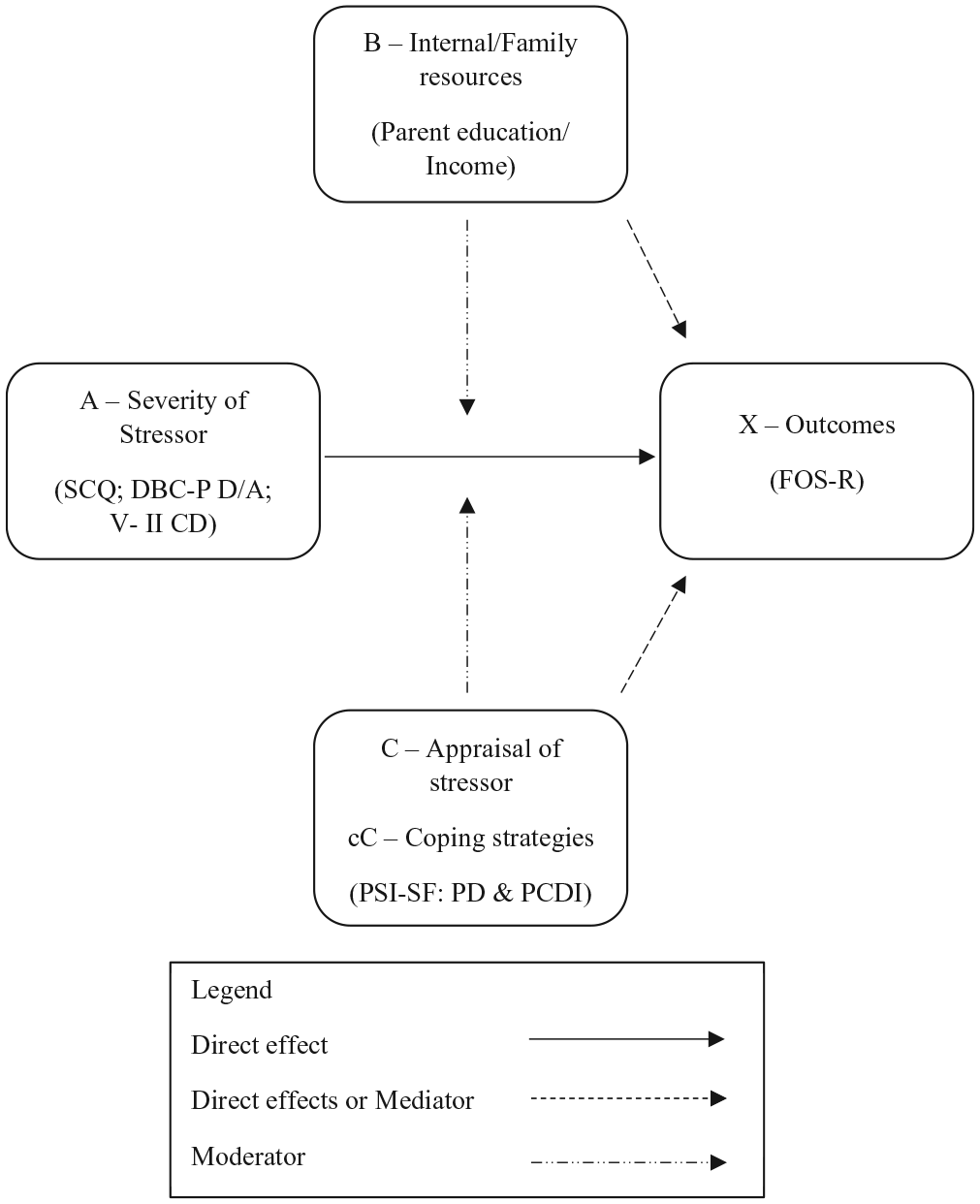
Modified double ABCX model (based on McCubbin & Patterson, 1983).
Summary and Research Questions
Knowledge regarding outcomes for families participating in EI programs for autism and the factors that may be influential to family outcome attainment is scant, as most studies maintain a narrow focus on child outcomes (Karst & Van Hecke, 2012; Zwaigenbaum et al., 2015). This may be due to family outcomes being regarded as secondary to child outcomes in the broader EI sphere. As posited by Wainer et al. (2017), shifting the focus to include and consider parent/family variables as meaningful outcomes of EI may benefit service provision to enhance outcomes for children, parents, and families holistically. The FOS-R has emerged as a potential measure of family outcomes for children with disabilities that may be utilized to address this lack in knowledge, with FOS-R outcomes for families of children on the autism spectrum and factors that potentially influence outcomes yet to be explored within a sound theoretical framework. Thus, this study utilized the FOS-R to explore the extent to which family outcomes of EI are being attained for Australian families of children on the autism spectrum, how helpful parents perceive EI has been to their family, and factors that potentially influence these aspects in line with an established theoretical framework. To do so, the modified double ABCX model was utilized to explore potential child, parent, and family correlates that may explain FOS-R family outcomes and the reported perceived helpfulness of EI for parents of children on the autism spectrum. Although an Australian sample was used, findings are relevant outside of the Australian context as the impact on families has been observed internationally (Manning et al., 2011; McStay et al., 2014; Paynter et al., 2013; Stuart & McGrew, 2009). The following research questions were asked:
Method
Participants
Data for this study were extracted from the first data collection point of the Longitudinal Study of Australian Students with Autism (LASA), an ongoing sequential study financially supported by The Cooperative Research Center for Living with Autism (Autism CRC; for a full protocol, see Roberts et al., 2017 for details). In brief, parents of two cohorts of children on the autism spectrum (age 4-5 years and 9-10 years) complete a range of questionnaires annually. Parents were requested to provide diagnostic reports to evidence their child’s autism status and complete the Social Communication Questionnaire (SCQ) as verification. SCQ score of 11 or above was used as support for autism diagnosis as recommended by Eaves, Wingert, Ho, and Mickelson (2006). The diagnostic reports of all children with an SCQ score of 11 to 15 were checked and diagnoses were confirmed using a formal assessment method. As the current study centered on recent family experiences of EI and parents’ perceived helpfulness of EI, only participants from the 4 to 5 years cohort (N = 132) were included in this study. Ten participants were excluded due to SCQ scores below the recommended cutoff; eight participants were excluded due to stating that they had not accessed EI services. In addition, 13 fathers were excluded due to a low number of male respondents. Participants with missing standardized measure scores were also excluded to maintain the integrity of analyses conducted (n = 4). Subsequently, 97 data sets were retained for analysis, see Table 1 for demographic and clinical characteristics.
Mother, Child, Family, and EI Demographic Characteristics for Included Participants (N = 97).
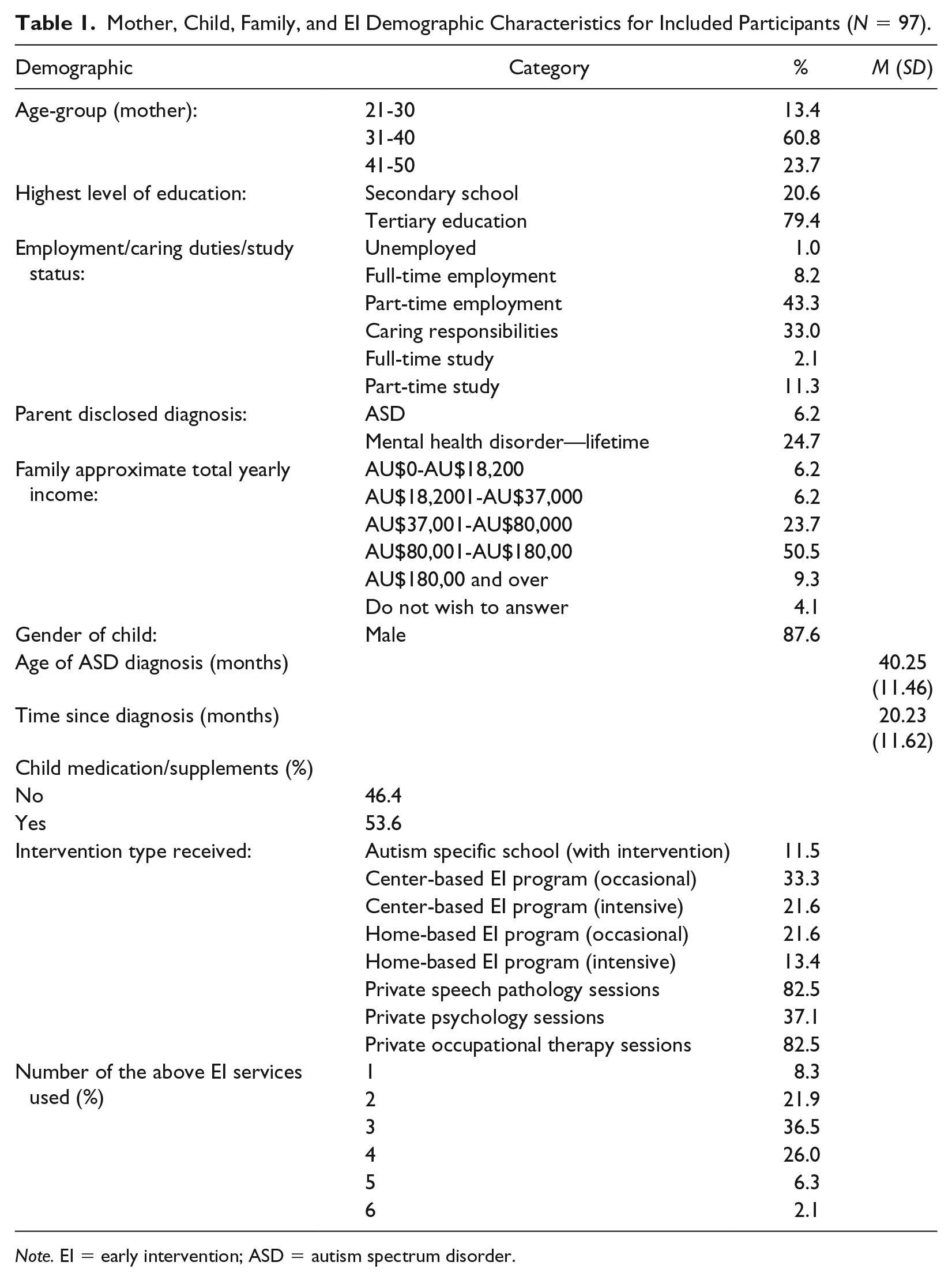
Note. EI = early intervention; ASD = autism spectrum disorder.
Data suggested that mothers were predominantly aged 31 to 40 years, had predominantly completed higher education (i.e., university level), varied in work status/caregiver/study responsibilities, and were a moderate to high family income group (59.8%; AU$80, 000 and above, equivalent to median income for an individual in Australia (Australian Bureau of Statistics, 2017). Mean child age was 60.47 months (SD = 6.62; 87.6% male), mean age of parent-reported autism diagnosis was 40.25 months (SD = 11.46), and mean time since diagnosis was 20.23 months (SD = 11.62). In addition to a diagnosis of autism, 42.7% of the children had a parent-reported additional diagnosis of another medical condition or disability. The most frequently listed comorbid diagnoses were Attention Deficit Hyperactivity Disorder (ADHD; n = 11, 11.5%), Global Developmental Delay or/and Intellectual Disability (GDD/ID; n = 5, 5.2%), Oppositional Defiant Disorder (ODD; n = 4, 4.2%), anxiety (n = 3, 3.1%), Sensory Processing Disorder (SPD, n = 3, 3.1%), hearing issues (n = 3, 3.1%), and epilepsy (n = 3, 3.1%). Most mothers reported utilizing two to four intervention services for their child (84.4%), with 8.3% utilizing one service, 6.3% utilizing five, and 2.1% utilizing six. The most common intervention services utilized were private speech pathology and occupational therapy sessions, private psychology sessions, and occasional center-based intervention program participation.
Measures
The current study utilized a subset of measures employed in the longitudinal study related to the variables of interest in line with the double ABCX model as outlined below.
Autism characteristics (A)
The SCQ (Rutter, Bailey, & Lord, 2003) was used to measure autism characteristics as in previous research (e.g., Schwenck & Freitag, 2014). Research has shown the SCQ to have good psychometric properties (Chandler et al., 2007; Eaves et al., 2006; Snow & Lecavalier, 2008). Full-scale Cronbach’s alpha for the present sample was .91.
Challenging behavior (A)
The Developmental Behavior Checklist–Parent Form (DBC-P; Einfeld & Tonge, 2002) Disruptive/Antisocial subscale was used to measure externalizing behavior as per previous research (e.g., Chandler et al., 2016). This subscale shows high internal consistency (Disruptive/Antisocial subscale α = .91, Einfeld & Tonge, 2002). Cronbach’s alpha for the current sample was .90 for this subscale.
Communication skills (A)
The Vineland Adaptive Behavior Scales, Second Edition: Parent/Caregiver Rating Form (Vineland-II; Sparrow, Cicchetti, & Balla, 2005) communication domain standard score was used to measure child communication skills as indicated by previous research in the autism field (e.g., Klin et al., 2007). A clinical cutoff of 70 or below was used (as recommended by Sparrow et al., 2005). This measure shows good reliability and validity (Sparrow et al., 2005).
Internal/family resources (B)
Information on the parent’s highest education level (B) and current employment/caregiver/study status; family income (B) were collected as part of the background demographics questionnaire.
Parental stress (C; cC)
The Parental Stress Index–Short Form (PSI-SF; Abidin, 2012) Parent Distress (PD) and Parent–Child Dysfunctional Interaction (PCDI) subscales were used due to previous research showing these measures being highly associated with parenting stress (Ornstein Davis & Carter, 2008). These subscales show high internal consistencies (PD = .88, PCDI = .88; Reitman, Currier, & Sickle, 2002). Cronbach’s alphas for the current sample were .87 and .83, respectively.
Family outcomes of EI (X)
The FOS-R (Bailey et al., 2011) assesses core family outcomes and the perceived helpfulness of EI for families of children with disabilities. This measure was selected as it has a section (section B) that specifically asks families about the helpfulness of EI in reaching specific outcomes. Section A comprises 24 items assessing five broad family outcomes related to (a) understanding your child’s strengths, needs, and abilities (four items); (b) knowing your rights and advocating for your child (five items); (c) helping your child develop and learn (four items); (d) having support systems (five items); and (e) accessing the community (six items). Section B comprises 17 items across three Helpfulness Indicators assessing the extent to which families perceive EI has helped them (a) know and understand their rights (five items), (b) communicate their children’s needs (six items), and (c) help their children develop and learn (six items). Respondents rate each item on a 5-point Likert-type scale. For Section A—how each item best describes their family right now (1 = not at all to 5 = completely). For section B—how helpful EI has been to them and their family over the past year (1 = not at all helpful to 5 = extremely helpful). Data can be analyzed at item, subscale, and overall total levels (Raspa, Hebbeler, & Bailey, 2009). All subscales showed adequate to good reliability in previous studies (Bailey et al., 2011; Ueda at al., 2015). Cronbach’s alphas for the current sample were in line with previous research (FOSA total = .89, O1 = .86, O2 = .87, O3 = .88, O4 = .81, O5 = .76; FOSB total = .97, HI1 = .93, HI2 = .92, HI3 = .97). For the purposes of the current study, individual subscales were analyzed separately. Mean and total outcome/helpfulness indicator-level scores were calculated, with lower scores indicating lesser achievement and higher scores indicating greater achievement of the outcome/indicator. Based on Ueda et al.’s (2015) recommendations, an outcome was deemed to have been “attained” if a participant’s outcome mean score was 4 or above for that outcome.
Data Analysis
Frequencies and descriptive analysis of mother and child clinical characteristics for predictor variables were calculated. As per data screening, FOS-R subscale sample size varied by analysis according to exclusions of multivariate outliers identified in regression diagnostics. Cases were excluded listwise by analysis to maximize the sample available for each. To evaluate FOS-R attainment, percentages, means, and standard deviations per FOS-R subscale were examined, with variability in reported attainment of interest.
Hierarchical Multiple Regression (HMR) analyses, with each FOS-R subscale as the outcome variable, were conducted to investigate the variance explained by the combination of factors and unique contributions of each. HMR analyses were chosen as added variance by each predictor group (i.e., child, parent, and family) were of interest. To ensure thorough exploration of the double ABCX model, all predictor variables were included per regression model regardless of bivariate associations found with individual FOS-R subscales. Inclusion of all predictors was also based on previous double ABCX research showing variance explained in family functioning and parenting stress by similar constructs (Manning et al., 2011). To capture components of the double ABCX model, child characteristics (A) were entered at Step 1, including autism characteristics (SCQ total), externalizing behaviors (DBC-P Disruptive/Antisocial subscale), and communication skills (Vineland-II Communication domain). Parent coping/appraisal (C, Cc) and internal resource (B) variables were entered at Step 2, including parent distress (PSI-PD subscale), parent/child dysfunctional interaction (PSI-PCDI subscale), and parent education level. Family income was entered at Step 3 as “family resources” (B) in each analysis. Family income was interpreted as a proxy for socioeconomic status (SES), which can be considered as an external resource within the double ABCX framework linked to greater social support, funding, and material supports, which lends to fewer buildup of stressors (Aa factors).
As the current study was a novel exploration of individual FOS-R subscales and associated predictors, aimed at highlighting areas for in-depth investigation in future research, increased risk of Type I errors was considered less of a concern than Type II errors. Although the design required multiple analyses that potentially raised the possibility of increased Familywise error, Bonferroni correction was considered too conservative (Perneger, 1998). Thus, the decision was made a priori to retain a p value of .05 across analyses. Effect sizes were interpreted according to Cohen’s (1998) recommendations for correlation analyses (small = .1, moderate= .3; and large = .5).
Results
Data Screening
Data were screened for outliers and meeting the assumptions of parametric analyses. No major violations of assumptions were found. Missing value analysis of each variable showed < 5% missing with analysis, suggesting that data were missing completely at random, Little’s MCAR test χ2(83) = 87.87, p = .336, ns. Thus, multivariate outliers identified as influential were deleted listwise by analysis as per recommendations under these conditions (Tabachnick & Fidell, 2007), with n subsequently varying by model tested in final analyses.
Inspection of residual plots for each analysis indicated no violations of normality, linearity, homoscedasticity, or independence. Bivariate correlation analysis revealed no collinearity of predictors (r > .80), thus all were retained; see Table 2. Initial bivariate correlations however included multivariate outliers identified through regression diagnostics to assess overall associations between pairs of predictors.
Pearson Correlations Between Child, Parent, and Family Predictor Variables (N = 97).
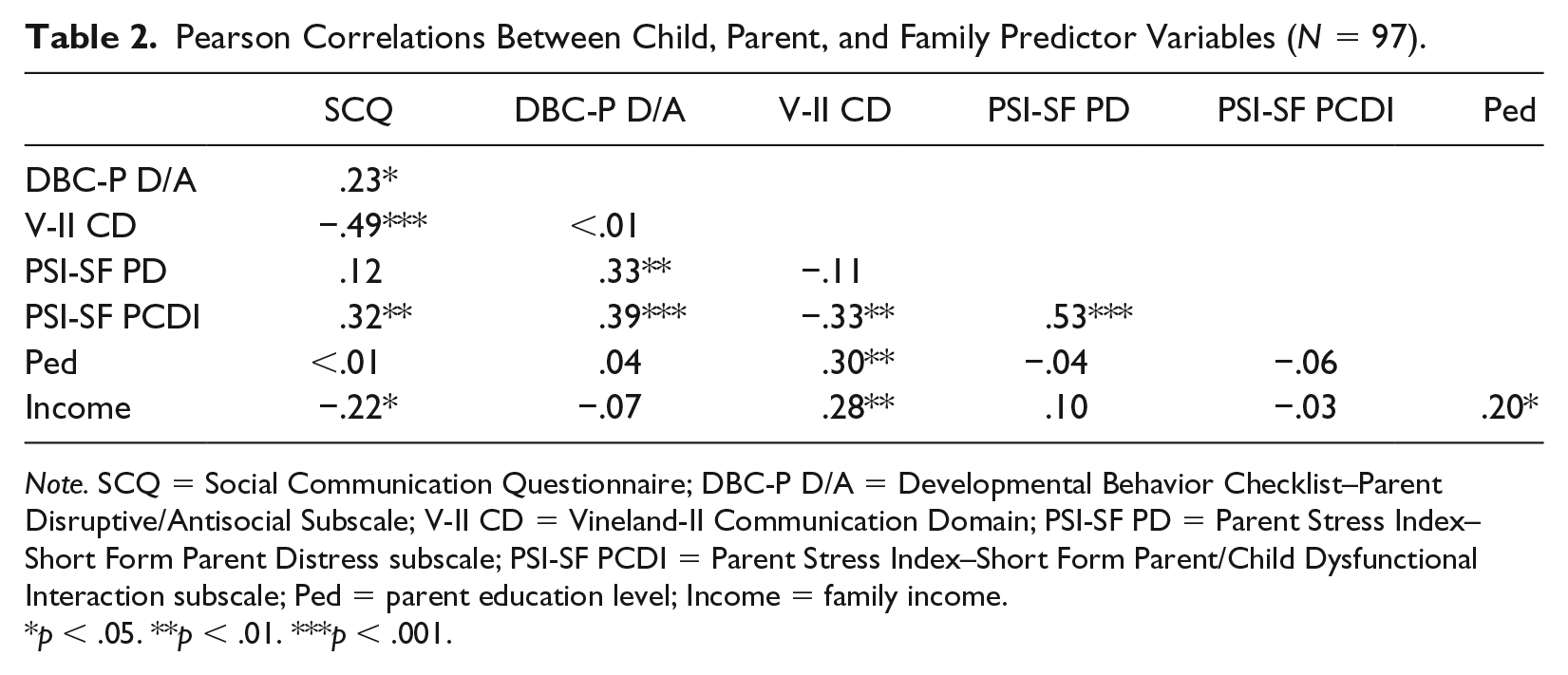
Note. SCQ = Social Communication Questionnaire; DBC-P D/A = Developmental Behavior Checklist–Parent Disruptive/Antisocial Subscale; V-II CD = Vineland-II Communication Domain; PSI-SF PD = Parent Stress Index–Short Form Parent Distress subscale; PSI-SF PCDI = Parent Stress Index–Short Form Parent/Child Dysfunctional Interaction subscale; Ped = parent education level; Income = family income.
p < .05. **p < .01. ***p < .001.
Descriptive Analyses
Clinical characteristics of participating mothers and their children are shown in Table 3. Of the mothers, 41.2% reported clinically significant levels of overall perceived parenting stress (90th percentile and above).
Mother-Reported Clinical Characteristics of Participants (N = 97).
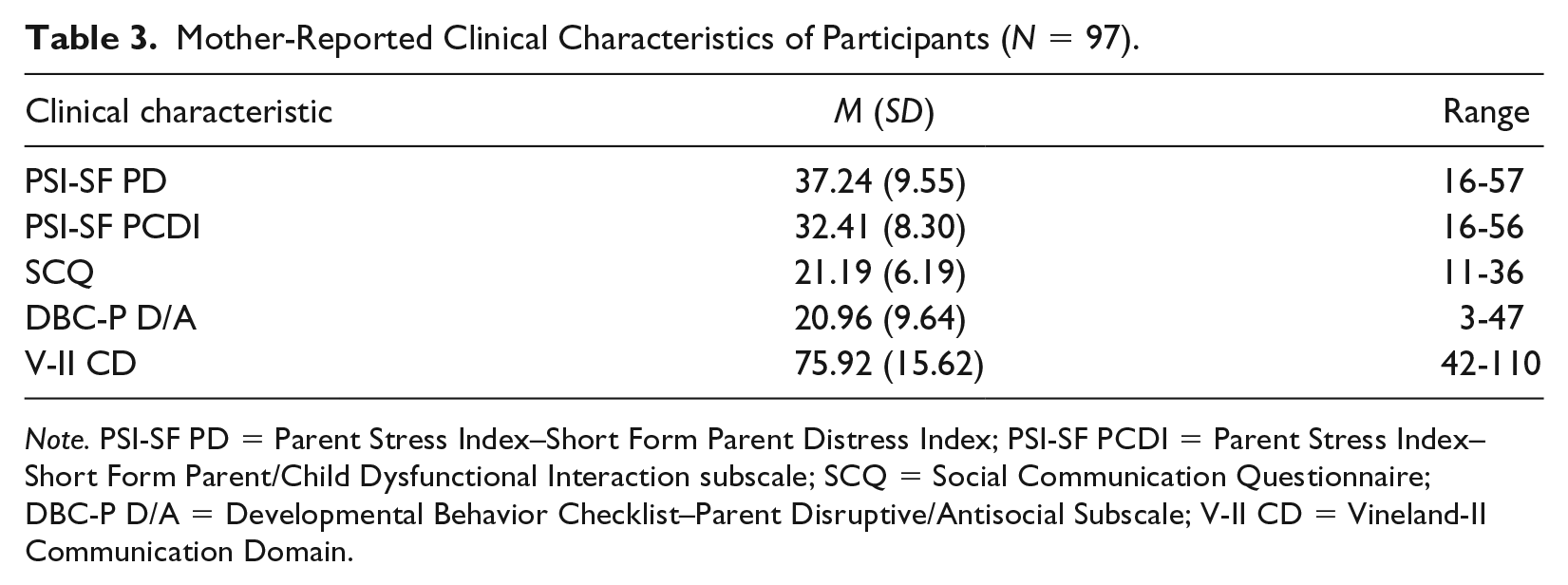
Note. PSI-SF PD = Parent Stress Index–Short Form Parent Distress Index; PSI-SF PCDI = Parent Stress Index–Short Form Parent/Child Dysfunctional Interaction subscale; SCQ = Social Communication Questionnaire; DBC-P D/A = Developmental Behavior Checklist–Parent Disruptive/Antisocial Subscale; V-II CD = Vineland-II Communication Domain.
FOS-R Subscale Attainment
Mother-reported FOS-R subscale attainment percentages, mean scores per item, standard deviations, and subscale score ranges are shown in Table 4. Due to variation in number of items across subscales, mean score per item was calculated for ease of comparison. Overall, attainment (a mean score of 4 or more for each outcome) was moderate (64.2% or fewer rating almost/completely), with the highest percentage of attainment for outcomes related to understanding child strengths, needs, and abilities (O1), and child development/learning (O3). Of the FOS-R family outcomes with a mother-reported attainment percentage below 50%, having support systems (O4) was the lowest, followed by knowledge of rights and advocacy (O2). Results also showed attainment for all three EI helpfulness indicators was less than 50%, with greater variability and range of scores noted for these subscales compared with the family outcome subscales.
Percentage of Families “Attaining” Each Outcome (i.e., a Mean FOS-R Subscale Score of 4 and Above), Subscale Item Means and Standard Deviations, and Subscale Ranges.
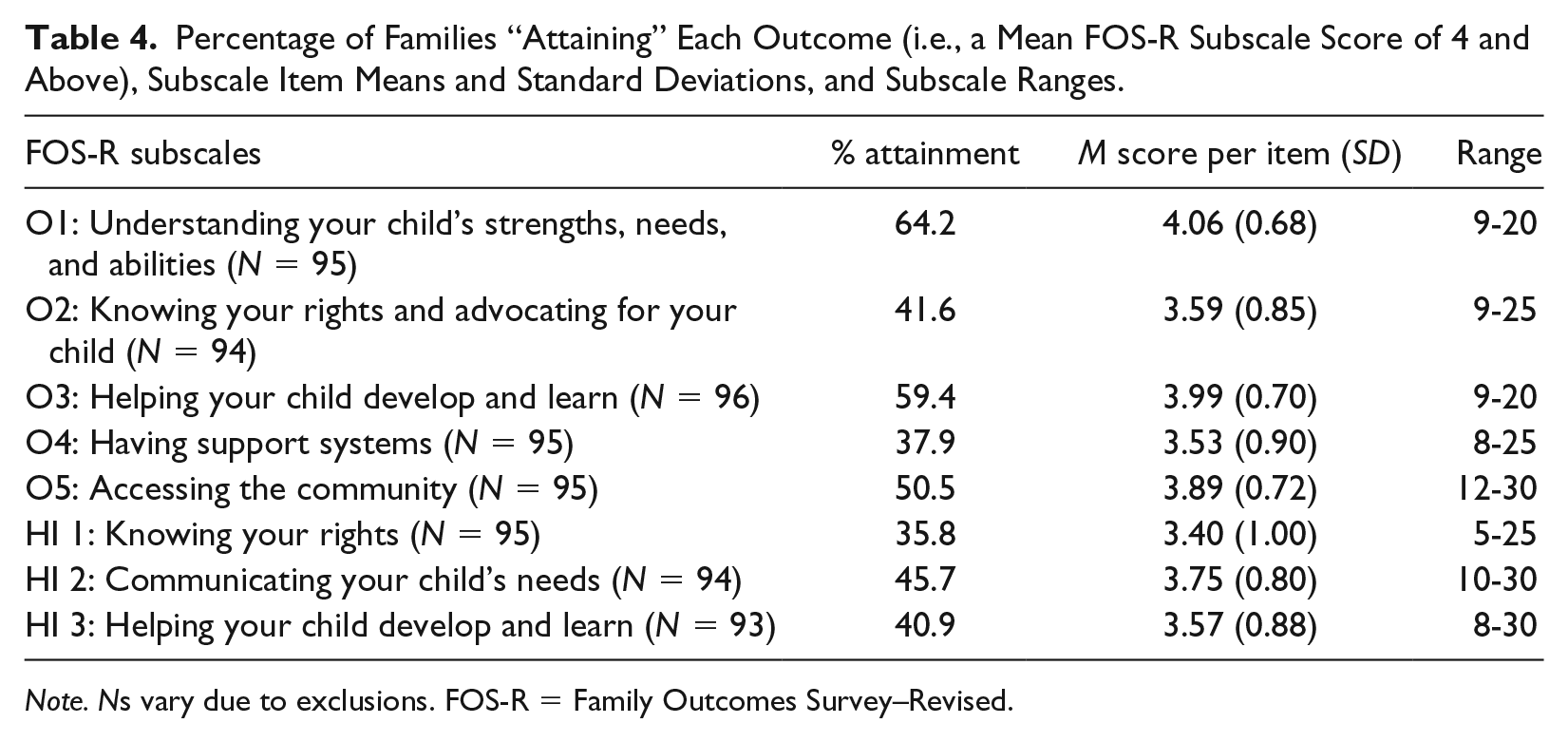
Note. Ns vary due to exclusions. FOS-R = Family Outcomes Survey–Revised.
Predictors of FOS-R Outcomes and Helpfulness Indicators
Results of HMR analyses are shown in Table 5 (FOS-R Section A) and Table 6 (FOS-R Section B). As outlined in the data analysis section above, child, parent, and family factors were entered into the model in consecutive steps to investigate the additional variance each accounted for.
HMR Analyses Regressing FOS-R Outcome Subscales, Child, Parent, and Family Predictor Measures.
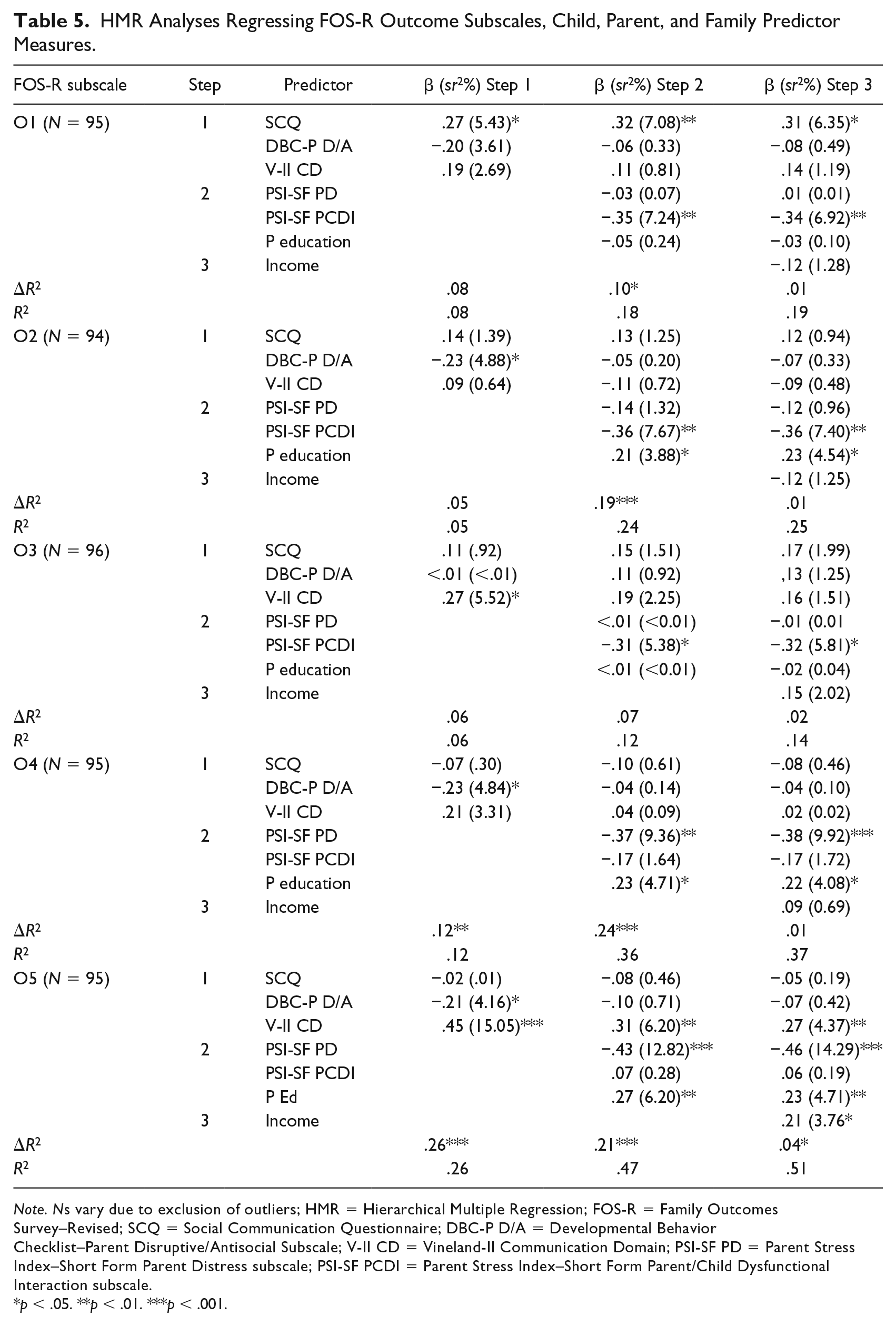
Note. Ns vary due to exclusion of outliers; HMR = Hierarchical Multiple Regression; FOS-R = Family Outcomes Survey–Revised; SCQ = Social Communication Questionnaire; DBC-P D/A = Developmental Behavior Checklist–Parent Disruptive/Antisocial Subscale; V-II CD = Vineland-II Communication Domain; PSI-SF PD = Parent Stress Index–Short Form Parent Distress subscale; PSI-SF PCDI = Parent Stress Index–Short Form Parent/Child Dysfunctional Interaction subscale.
p < .05. **p < .01. ***p < .001.
HMR Analyses Regressing FOS-R Helpfulness Indicator Subscales, Child, Parent, and Family Predictor Measures.
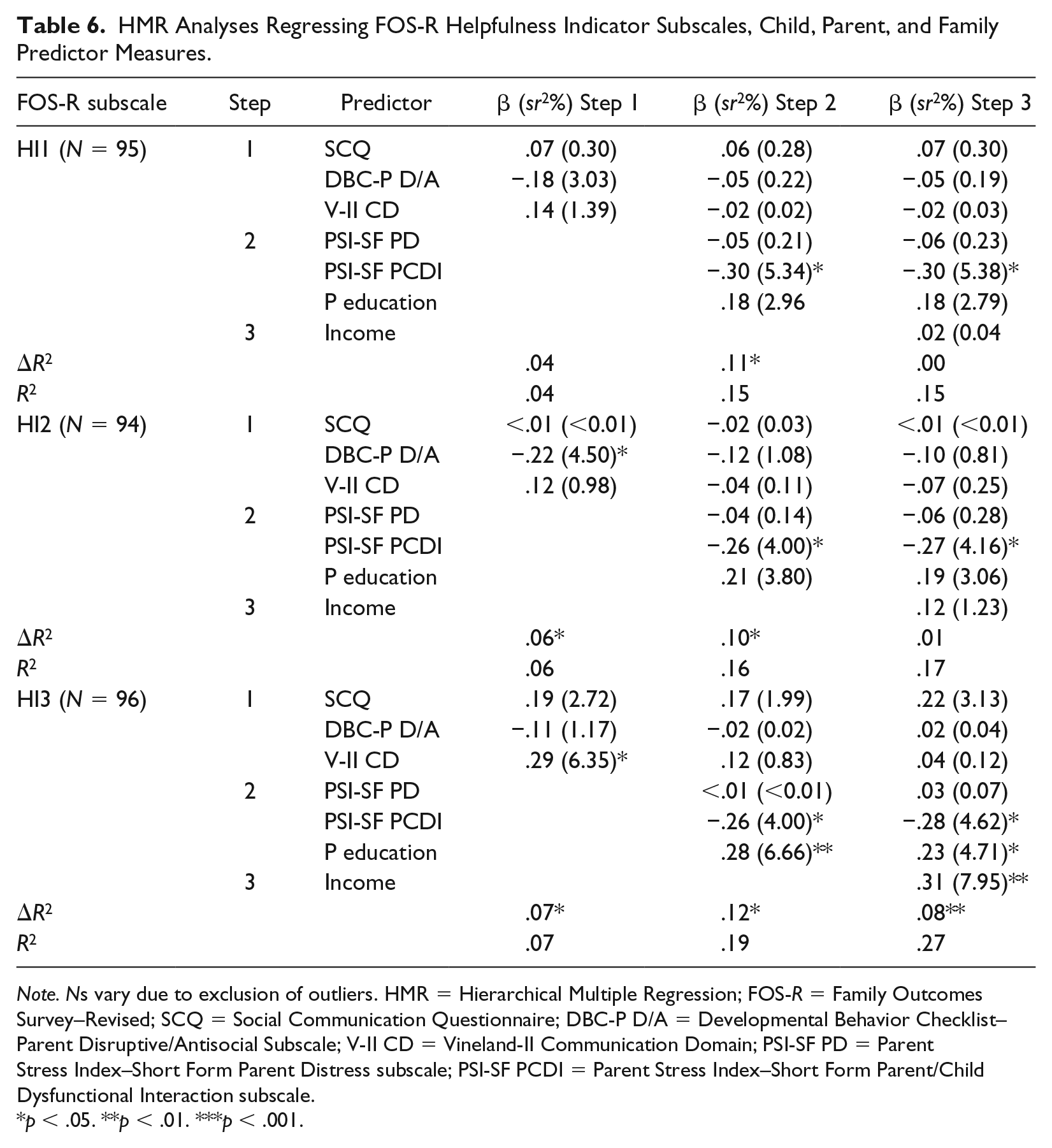
Note. Ns vary due to exclusion of outliers. HMR = Hierarchical Multiple Regression; FOS-R = Family Outcomes Survey–Revised; SCQ = Social Communication Questionnaire; DBC-P D/A = Developmental Behavior Checklist–Parent Disruptive/Antisocial Subscale; V-II CD = Vineland-II Communication Domain; PSI-SF PD = Parent Stress Index–Short Form Parent Distress subscale; PSI-SF PCDI = Parent Stress Index–Short Form Parent/Child Dysfunctional Interaction subscale.
p < .05. **p < .01. ***p < .001.
Section A
Understanding your child’s needs, strengths, and abilities (O1)
At Step 1, 8% of the variance in O1 was accounted for by the combination of child autism characteristics, externalizing behaviors, and communication skills, Fchange(3, 91) = 2.48, p = .066. At Step 2, the addition of PD, PCDI, and parent education level accounted for an additional and significant 10% of the variance, Fchange(3, 88) = 3.68, p = .015. At Step 3, a further and nonsignificant 1% of the variance was explained by family income, Fchange(1, 87) = 1.36, p = .246. Overall, the model tested indicated that 19% of the variance was explained by the combination of double ABCX factors. Child autism characteristics and PCDI were found to be unique predictors explaining 6.53% and 6.92% of the variance respectively. This indicated that greater autism characteristics and higher PCDI predicted lower attainment of O1.
Knowing your rights and advocating for your child (O2)
At Step 1, 5% of the variance in O2 was accounted for by the combination of child autism characteristics, externalizing behaviors, and communication skills, Fchange(3, 90) = 1.70, p = .173. At Step 2, the addition of PD, PCDI, and parent education level accounted for an additional and significant 19% of the variance, Fchange(3, 87) = .08, p < .001. At Step 3, a further and nonsignificant 1% of the variance was explained by family income, Fchange(1, 86) = 1.45, p = .232. Overall, the model tested indicted that 25% of the variance was explained by the combination of double ABCX factors. PCDI and parent education were found to be significant unique predictors explaining 7.40% and 4.54% of the variance, respectively. This indicated that higher PCDI and lower parent education level predicted lower attainment of O2.
Helping your child develop and learn (O3)
At Step 1, 6% of the variance in O3 was accounted for by the combination of child autism characteristics, externalizing behaviors, and communication skills, Fchange(3, 92) = 1.84, p = .145. At Step 2, the addition of PD, PCDI, and parent education level accounted for an additional nonsignificant 7% of the variance, Fchange(3, 89) = 2.29, p = .084. At Step 3, a further and nonsignificant 2% of the variance was explained by family income, Fchange(1, 88) = 2.08, p = .153. Overall, the model tested indicated that 14% of the variance was explained by the combination of double ABCX factors. PCDI was found to be the sole significant unique predictor explaining 5.81% of the variance, indicating that higher PCDI predicted lower attainment of O3.
Having support systems (O4)
At Step 1, 12% of the variance in O4 was accounted for by the combination of child autism characteristics, externalizing behaviors, and communication skills, Fchange(3, 91) = 4.31, p = .007. At Step 2, the addition of PD, PCDI, and parent education level accounted for an additional and significant 24% of the variance, Fchange(3, 88) = 11.05, p < .001. At Step 3, a further and nonsignificant 1% of the variance was explained by family income, Fchange(1, 87) = .95, p = .333. Overall, the model tested indicated that 37% of the variance was explained by the combination of double ABCX model factors. PD and parent education level were found to be significant unique predictors explaining 9.92% and 4.08% of the variance, respectively. This indicated that higher PD and lower parent education level predicted lower attainment of O4.
Accessing the communty (O5)
At Step 1, 26% of the variance in O5 was accounted for by the combination of child autism characteristics, externalizing behaviors, and communication skills, Fchange(3, 91) = 10.70, p < .001. At Step 2, the addition of PD, PCDI, and parent education level accounted for an additional and significant 21% of the variance, Fchange(3, 88) = 11.86, p < .001. At Step 3, a further and significant 4% of the variance was explained by family income, Fchange(1, 87) = 6.93, p = .011. Overall, the model tested indicated that 51% of the variance was explained by the combination of double ABCX factors. Child communication skills (4.37%), PD (14.29%), parent education level (4.71%), and family income (3.76%) were found to be significant unique predictors. This indicated that higher PD and lower child communication, parent education, and family income predicted lower attainment of O5.
Section B
Knowing your rights (HI 1)
At Step 1, 4% of the variance in HI 1 was accounted for by the combination of child autism characteristics, externalizing behaviors, and communication skills, Fchange(3, 91) = 1.28, p = .285. At Step 2, the addition of PD, PCDI, and parent education level accounted for an additional and significant 11% of the variance, Fchange(3, 88) = 3.82, p = .013. At Step 3, no additional variance was explained by family income, Fchange(1, 87) = .04, p = .849. Overall, the model tested indicated that 15% of the variance was explained by the combination of double ABCX factors. PCDI was the sole significant unique predictor found explaining 5.38% of the variance, indicating that higher PCDI predicted reduced perceived helpfulness of EI regarding knowledge of rights.
Communicating your child’s needs (HI 2)
At Step 1, 6% of the variance in HI 2 was accounted for by the combination of child autism characteristics, externalizing behaviors, and communication skills, Fchange(3, 90) = 1.94, p = .129. At Step 2, the addition of PD, PCDI, and parent education level acounted for an additional and significant 10% of the variance, Fchange(3, 87) = 3.49, p = .019. At Step 3, a further nonsignificant 1% of the variance was explained by family income, Fchange(1, 86) = 1.29, p = .260. Overall, the model tested indicated that 17% of the variance was explained by the combination of double ABCX factors. PCDI was the sole significant unique predictor found explaining 4.16% of the variance, indicating that higher PCDI predicted reduced perceived helpfulness of EI regarding communicating child needs.
Helping your child develop and learn (HI 3)
At Step 1, 7% of the variance in HI 3 was accounted for by the combination of child autism characteristics, externalizing behaviors, and communication skills, Fchange(3, 89) = 2.24, p = .089. At Step 2, the addition of PD, PCDI, and parent education level acounted for an additional and significant 12% of the variance, Fchange(3, 86) = 4.05, p = .010. At Step 3, a further and significant 8% of the variance was explained by family income, Fchange(1, 85) = 9.22, p = .003. Overall, the model tested indicated that 27% of the variance was explained by the combination of double ABCX factors. Family income (7.95%), PCDI (4.62%), and parent education level (4.71%) were found to be significant unique predictors. This indicated that higher PCDI and lower family income and parent education level predicted reduced perceived helpfulness of EI regarding helping children’s development and learning.
Discussion
The current study is the first to investigate family outcomes resultant of EI engagement as measured by the FOS-R utilizing the double ABCX model of family adaptation. As such, the study contributes to addressing the atheoretical nature of intervention research in the early childhood period and gaps within the literature. Elevated levels of stress were found in over a third of participants consistent with previous research (see review by Hayes & Watson, 2013). Child characteristics (autism characteristics, challenging behavior, and communicative skills) were largely nonsignificant in predicting family outcomes and perceived helpfulness once combined with parent and family factors. In accordance with the double ABCX model, parent and family factors emerged as significant predictors, highlighting their importance in explaining family outcomes and reported perceived helpfulness of EI related to aspects measured by the FOS-R. Notably, aspects of parent stress, particularly perceptions of stress related to interaction with their child (PCDI), were most consistently related and the strongest predictors of family outcomes and perceived EI helpfulness.
FOS-R Attainment
On average, ratings at group level for mothers of 4- to 5-year-old children on the autism spectrum who reported accessing EI suggested moderate family outcome attainment related to understanding and knowledge of their child, their rights and advocacy capability, and access to support systems and the community, relative to services received. Fewer mothers reported attainment and perceived helpfulness of EI related to knowing their rights, advocating for their child, and accessing support systems compared with other FOS-R outcomes. This suggests that, despite various benefits gained from EI engagement, some mothers may feel their families are less supported in these respects. Family outcome and helpfulness ratings were comparatively lower across all FOS-R indices than those described in Bailey et al.’s (2011) and Poon et al.’s (2014) samples of families of children with unspecified disabilities receiving EI services. However, this may reflect inherent differences in child groups between studies as research has shown poorer overall outcomes for parents of children on the autism spectrum compared with other disabilities (for review see Hayes & Watson, 2013), and this previous research does not outline children’s specific diagnoses.
Predictors of FOS-R Outcomes and Helpfulness Indicators
Child characteristics (autism characteristics, challenging behavior, and communicative skills) had less statistical influence (i.e., did not independently contribute) to explaining FOS-R outcomes or EI perceived helpfulness once parent and family characteristics were accounted for. Thus, the assumption that positive outcomes for the child automatically translate to positive outcomes for their parents and families is challenged (Karst & Van Hecke, 2012), while the need for greater focus on parent and family factors both in EI practice and evaluation is highlighted. This finding is important as it suggests that rather than positioning the child first when considering EI, primary consideration should be given to parents, followed by the child, within the family system. The limited influence of child factors (A) across various FOS-R outcomes is incongruent with the direct effects proposed by McCubbin and Patterson’s (1983) model. However, the direct influence of pileup demands (e.g., SES) found is consistent with model predictions. Conversely, our findings showed that characteristics of the child are important to consider as on their own they had varied influence; however, results suggest that parent and family factors take precedence in overall explanation. This aspect aligns with the moderating or mediating effects of these factors proposed by the double ABCX model.
Parent factors (i.e., PD, PCDI, and parent education) were consistently predictive of various family outcomes and the perceived helpfulness of EI, with PCDI and PD explaining lower outcome attainment across FOS-R indices. This finding is consistent with previous research investigating family outcomes utilizing the double ABCX model (e.g., Paynter et al., 2013) and highlights the particular importance of aspects of parent stress when considering family outcomes and the perceived helpfulness of EI for mothers of children on the autism spectrum. Moreover, the negative impact of differential aspects of parental stress on the perceived helpfulness of EI is in line with findings by Sarimski, Hintermair, and Markus Lang (2013), whereby parents with higher perceived child-related stress reported less satisfaction with the professional support they received.
Notably, PCDI was the strongest, most consistent predictor in the current study, contributing the largest percentage of variance in explaining family outcomes and parent perceived helpfulness of EI across most FOS-R outcomes. This finding is novel and may emphasize how meaningful the parent–child relationship is relative to the benefits and helpfulness of engagement with EI services perceived by parents. Alternatively, the finding may reflect the influence of mothers’ negative appraisal styles more broadly, which may be symptomatic of heightened psychological distress and/or depression prevalent in parents of children on the autism spectrum (Eisenhower et al., 2005). For example, greater indication of negative appraisals has been linked to elevated levels of psychological stress and negative family impact utilizing the double ABCX framework (Paynter et al., 2013). Hence, these negative perceptions may be moderating how mothers see their child and EI, which influences family outcome attainment; however, variability across FOS-R index scores indicates this may vary across outcome contexts. Measures such as the Family Implications of Childhood Disability (FICD; Trute & Hiebert-Murphy, 2002) could be used by service providers to screen for parent appraisals, both at intake and throughout time, to identify those parents who may benefit from receiving individualized personal support related to their relationship with their child. Such additional support may help them perceive their child and EI more positively, facilitate positive EI engagement, and enhance outcomes for their child and family. Moreover, inclusion of parent appraisal and parent–child interaction quality measures in future research would inform practice through better understanding of the role these play in determining family outcomes and the helpfulness of EI perceived by parents.
PD and education level were both significant independent predictors of mothers’ perceptions of their support systems and ability to access the community. This finding aligns with previous research acknowledging the relationships between parent stress, education level, reduced access to social support, and subsequent withdrawal from the larger community (Boyd, 2002). Moreover, parent education significantly predicted the perceived helpfulness of EI in facilitating parents to support their child’s learning and development. This may reflect an inherent ability of those with a higher education level (i.e., university level) to access, digest, and apply information concerning child development and learning regardless of their engagement with EI professionals.
As predicted by the double ABCX model, family income (which may be viewed as a pileup demand when in the lower range) significantly explained family outcomes related to facilitating families’ access to their communities and the perceived helpfulness of EI in facilitating parents to support their child’s learning and development. Family income was interpreted as a proxy for SES and can be considered as an external resource within the double ABCX framework linked to greater social support, funding, and material supports, which lends to fewer buildup of stressors (Aa factors). These findings may broadly reflect the link between SES and unmet service needs for families of children on the autism spectrum found by Pickard and Ingersoll (2016). Results may suggest services needed to better meet the needs of lower SES families through targeted provision of additional supports for those identified at risk, greater flexibility in service provision, clear dissemination of information tailored to parent level of understanding, and access to counseling and other community services.
HMR models
Overall, the combination of parent factors accounted for significant additional variance across the majority of HMR analyses once child factors were controlled. Although the models tested yielded significant results, wide variability in variance explained by the combination of factors was found, ranging from 15% (HI 1: knowing your rights) to 51% (O5: accessing the community). Overall, while the findings explain part of the picture, unexplained variance across indices suggests that other factors may be involved, such as additional life stressors and parent appraisals, self-esteem, and coping strategies as suggested by both the double ABCX model and previous research (Paynter et al., 2013; Stuart & McGrew, 2009). Subsequently, further research is required to elicit further factors that should be measured.
Implications
Results of this study point to potential parent and family risk factors for reduced family outcome attainment and perceived benefits from engagement with EI services for families of young children on the autism spectrum. This is particularly important as whether families feel they benefit from services they receive is critical for determining positive engagement with support services and long-term outcomes for children. The predictive value of heightened parental stress indicated suggests that screening for this at intake and across time using the Parent Stress Index–Short Form (Abidin, 2012) and providing targeted access to counseling and support services may enhance family outcome attainment across a range of aspects for those parents identified as at risk. Given our findings indicate that greater parental stress related to interactions with their child on the autism spectrum is the largest contributor to lower perceived benefit from EI for their family, we recommend the provision of targeted interventions aimed at enhancing parent–child interaction quality for those parents found to be at risk.
Furthermore, areas of EI service provision where the needs of families were not well met (i.e., advocacy, knowledge of rights, and access to support networks and the community) were identified. This is particularly important considering that, in both public-funded (e.g., National Disability Insurance Scheme [NDIS]; Department of Families, Housing, Community Services and Indigenous Affairs [DFHCSIA], 2012 in Australia) and privately funded services (e.g., in parental selection of interventions, they pay privately), there is increasing pressure on families to select and implement interventions and advocate on their child’s behalf. Under the NDIS and similar schemes internationally (e.g., “Autism Funding: Under Age 6 Program“ in Canada [Ministry of Children and Family Development, 2017]), responsibilities of planning and petitioning for funding are largely placed upon parents, rather than receiving a set amount, as was previously the case in Australia (for a summary of the changes to funding models for children on the autism spectrum in Australia see Adams et al., 2019 and for the historical and current provision of Early Childhood Intervention (ECI) in Australia see Sukkar, 2013). Although these schemes provide for greater choice and control over service selection by families, greater parental agency, knowledge, and the ability to advocate for their child are necessitated to ensure adequate funding allocation and subsequent EI engagement. We recommend that EI service providers utilize the FOS-R as a review and evaluation tool to monitor parent satisfaction with the services they receive and identify at-risk families to address their specific needs. This will aid to ensure that ongoing engagement with EI services is perceived as worthwhile to all families and facilitate best possible outcomes for children on the autism spectrum, their parents, and their family.
Limitations and Future Directions
While the study contributes to understanding of the factors related to family outcomes of EI for families of children on the autism spectrum, key limitations should be considered. First, we did not correct for the heightened risk of Type I error consequential of multiple analyses. However, given the exploratory nature of the study to identify areas for future research, minimizing Type II error to ensure thorough exploration of the model was deemed of greater importance. The strong effects found suggest the value in future research that could both confirm and extend upon the current findings (e.g., structural equation modeling or longitudinal designs to investigate the underlying causal nature of the relationships highlighted). Furthermore, the current sample was relatively homogeneous in terms of SES, with a high proportion of participants being university educated (79.2%), with moderate to high family income (75%; AU$80,000 and above). Consequently, these families may represent a unique subset of the population, such that they possess the resources and time to participate in large-scale sequential studies such as the LASA. Finally, information regarding participant demographics and family characteristics were limited to that collected as part of the larger study. As such, more detailed information regarding marital status and race/ethnicity were not available for analysis.
Conclusion
This study aimed to address a shortfall in research by focusing on EI outcomes for families of young children on the autism spectrum, which are fundamental to full understanding of treatment effectiveness (Karst & Van Hecke, 2012). Factors that contribute to, or diminish, FOS-R family outcome attainment and the perceived helpfulness of EI received by families of children on the autism spectrum were explored utilizing an adapted double ABCX model. Findings highlight the importance of parent and family characteristics, over and above child characteristics, when considering the perceived effectiveness of EI service provision in supporting families’ various needs. Moreover, the study provides valuable insight into areas where EI service provision may be falling short in supporting families’ needs, particularly regarding understanding their or their childs’ rights. This is especially pertinent, given the increased level of knowledge and advocacy capability necessitated to plan for their childs’ needs under funding models such as the NDIS (DFHCSIA, 2012). Supporting families through this process is imperative to ensuring positive engagement with EI services, which ultimately facilitates optimal short- and long-term outcomes for both children on the autism spectrum, their familities, and the larger community. Overall, the study indicates that altering the focus of EI evaluation to include parents and families as important to positive outcomes may enable professionals to enhance outcomes for children, parents, and families individually and holistically.
Footnotes
Acknowledgements
The authors wish to thank the parents who have contributed to this research and acknowledge the work of the LASA team members: Jacqueline Roberts (Project Leader), Susan Bruck, Trevor Clark, Sandra Devaraj, Robyn Garland, Antoinette Hodge, Patricia Howlin, Honey Heussler, Deb Keen, Kate Simpson, Natalie Silove, David Trembath, Madonna Tucker, Marleen Westerveld, and Katrina Williams.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the financial support of the Cooperative Research Center for Living with Autism (Autism CRC), established and supported under the Australian Government’s Cooperative Research Centers Program.