
Abstract
A survey of 955 early childhood practitioners in one Midwestern state was conducted to assess judgments of their desired use versus their current use or implementation of 10 sets of recommended practices from the Division for Early Childhood of the Council of Exceptional Children. Practitioners from early intervention, preschool, preschool special education, Early Head Start, Head Start, and other early childhood programs participated in the study. Results indicated large effect size differences in practitioners’ judgments of their desired versus current use of the practices, differences in terms in which practices were considered most valued and most frequently used by the practitioners, and a continued gap in the use of practices compared with results reported in similar studies conducted 15 and 22 years ago, respectively. The findings are discussed in terms of the need to adopt and use effective professional development practices to ensure practitioner use of valued practices and the need to develop a comprehensive system of personnel development to provide an infrastructure to support practitioners’ knowledge and skills of recommended practices.
Keywords
Building the capacity of early childhood (EC) practitioners in early intervention and early childhood special education (ECSE) to adopt and use effective intervention practices has been a focus of preservice and in-service training for more than three decades (e.g., Bailey, Palsha, & Huntington, 1990; Bruder, 2016; Bruder, Lippman, & Bologna, 1994; Bruder, Mogro-Wilson, Stayton, Smith, & Dietrich, 2009; Burke, McLaughlin, & Valdivieso, 1988). Interest in EC practitioner capacity building was promoted, to a large degree, initially by the Part H Infant and Toddler Program of the Education of the Handicapped Act (1986) and later the Part C Infant and Toddler Program in the Individuals with Disabilities Education Act (IDEA, 1990). As stated in Section 623 of the 1986 Part H legislation, for example, one goal of activities funded by the act is to “offer training about exemplary models and practices to State and local personnel who provide services to handicapped children from birth through eight” (Education of the Handicapped Act, 1986).
The Division for Early Childhood (DEC) of the Council for Exceptional Children has been at the forefront of both EC practitioner professional development (PD; e.g., Cochran et al., 2012; McCollum, McLean, McCartan, & Kaiser, 1989; Stayton & Miller, 1993; Stayton, Miller, & Dinnebeil, 2003) and the development and use of early intervention and ECSE recommended intervention practices (e.g., DEC Task Force on Recommended Practices, 1993; Sandall, Hemmeter, Smith, & McLean, 2005; Sandall, McLean, & Smith, 2000). DEC branded the practices as recommended practices (RPs), and McLean (2015) recently described the history and methodology to develop the DEC RPs over the past 21 years. During this time, there have been three sets of RPs, each a revision of the previous set. As noted by McLean (2015), research findings and practice feedback on the implementation of the practices informed and improved them through each revision and update (e.g., Guralnick, 1997; Smith, McLean, Sandall, Snyder, & Ramsey, 2005; Smith et al., 2002).
The first set of DEC RPs were completed in 1993 through an iterative process that involved the DEC membership, who provided input and feedback. (DEC Task Force on Recommended Practices, 1993). This set was revised in 2000 (Sandall et al., 2000). As was done with the first set, this revision was subjected to extensive input from the field through review and validation surveys (McLean, Snyder, Smith, & Sandall, 2002; Odom, McLean, Johnson, & LaMontagne, 1995). In 1995 and 2002, early childhood intervention (ECI) practitioners, as well as other constituent groups (family members and higher education faculty), were asked to indicate both the extent to which they agreed that different practices should be considered RPs and that the practices were being used with young children and their families. The results of these validation surveys informed the final set of DEC RPs (DEC, 2014).
Over the years, similar types of judgments about the value and use of ECI practices have been studied (e.g., Bailey, Buysse, Edmondson, & Smith, 1992; Bruder, Dunst, Mogro-Wilson, & Stayton, 2013; Dunst & Bruder, 2014; Ingber & Dromi, 2010; McWilliam, Snyder, Harbin, Porter, & Munn, 2000; Murphy, Lee, Turnbull, & Turbiville, 1995). Bailey et al. (1992), for example, reported large differences in practitioners’ judgments of ideal family involvement in early intervention and practitioners’ actual use of family involvement practices. Similarly, Bruder, Dunst, and Mogro-Wilson (2011) assessed the judgments of more than 1,800 ECI practitioners on their knowledge and skills about six different practice areas (family-centered practices, teaming and collaboration, assessment and evaluation, Individualized Family Service Plans [IFSPs] and Individualized Education Programs [IEPs], instructional practices, and natural environments and inclusion). The respondents included regular and special education teachers; speech, occupation, and physical therapist; psychologists; and social workers, all serving infants and young children with disabilities The majority of analyses showed that the practitioners judged themselves as more confident than competent in using the practices with children and families, regardless of discipline.
In all of these studies, including the validation studies of the initial and first revision of the DEC RPs, the findings showed discrepancies in practitioners’ judgments of the importance or value attributed to intervention practices and the current or actual use of the practices. That is, in all studies to date, the average ratings of current or actual use of practices were smaller than the average ratings of the importance or value attributed to the practices. Comparisons of the discrepancies reported in earlier studies (Bailey et al., 1992; Murphy et al., 1995; Odom et al., 1995), and in later studies (Ingber & Dromi, 2010; McLean et al., 2002; McWilliam et al., 2000; Summers et al., 2015), found similar gaps in the desired versus current use of ECI practices. The fact that discrepancies have persisted for many years raises questions as to whether the gap in desired use, or value of a practice in comparison with the current use of a DEC RP has changed: narrowed, remained the same, or widened.
The purpose of the study described in this article was to assess the match or discrepancy between EC practitioners’ judgments of the value or desired use of the 2014 DEC RPs and their current implementation of the practices and determine the relationship between the two. To do this, data from a survey that was developed and distributed to EC practitioners as part of a statewide initiative to develop an EC comprehensive system of personnel development (CSPD) were used to address the following research questions:
Method
Context of the Study
The data that are presented in this study were collected through a survey administered in one Midwestern state to inform the development of a CSPD for EC/ECSE practitioners. The state where this survey occurred has a population of approximately three million and 90.7% of the population are White, followed by Hispanic or Latino (6.2%), Black or African American (4%), and Asian American (2.7%). An increasing number of students in the state’s public schools (24.3%) are English language learners (6.1%; https://www.census.gov/quickfacts/fact/table/IA/PST045218).
Following the passage of the federal PL 94-142 in 1975, the state enacted a law mandating free appropriate public education (FAPE) for eligible children from birth to 21 years. Originally, the state’s intermediate educational units (IEUs) provided or made provisions for appropriate special education and related services for children, age birth through 5 years, and their families. In 2003, the State Education Agency (SEA) established policies to define the operation of a statewide, comprehensive, interagency system of services for infants and toddlers with disabilities or developmental delays under the federal IDEA, Part C. While the SEA identified the IEUs as having regulatory responsibility for the provision of early intervention services to families and children, age birth to 3 years, the local educational agencies (LEAs) are responsible for the provision of special education and related services for children beginning at the age of 3 years. The lead agency responsible for the administration of IDEA, Part C as well as Part B has remained with the SEA since 1986.
In 2007, the state’s general assembly established a voluntary preschool program for 4-year-olds, administered by LEAs, in collaboration with community EC providers. During the 2017-2018 school year, approximately 99.1% of LEAs provided preschool programs that were assessed as meeting quality program standards, which included a requirement for teachers to be appropriately licensed in EC education (Pre-K and Pre-K-3). Other statewide EC programs include state-funded at-risk parent support and preschool programs: Head Start, Early Head Start, Maternal Infant and Early Childhood Home Visiting (MIECHV) program, and other community preschool programs.
This state was one of the first states to develop a blended or unified competency-based EC licensure in 1996. This state licensure informed the curricula offered at state Institutions of Higher Education (IHEs) that prepared EC/ECSE teachers. However, there were no data on the current content of IHE EC/ECSE curricula, and it was unclear if IHEs addressed the pedagogy represented in the DEC RPs.
Recruitment
Practitioners from a number of different EC disciplines and programs were recruited to complete the assessment to ensure a representative sample of the large number and type of personnel and programs serving infants and young children with disabilities, and their families in this state. However, the SEA did not have a comprehensive contact list for educators serving young children (age 0 to 5 years with disabilities), which affected the ability of the research staff to estimate the total population for this survey. Therefore, a modified snowball sampling (Morgan, 2008) technique was used. Electronic invitations to participate in the study were sent to all public and private programs and agencies serving preschool-age children in the state. The invitations explained the purpose of the self-assessment, which was to measure the actual use of the DEC RPs. The invitations were sent by email to school districts, agencies, and regional or intermediate education agencies’ program directors, who were asked to forward the survey to eligible staff. The invitation was also sent to a list of practitioners identified by the SEA who participated in in-service activities. Finally, the invitation was shared with the state professional organizations (Head Start or DEC).
Practitioners were given 4 weeks to complete the survey, with two reminders sent either directly to those with contact information or the school, agency, or intermediate education units. Practitioners were eligible to complete the survey if they worked directly with infants and young children (some of whom were having disabilities) and/or their families as a routine part of their everyday practices. The SEA did not require institutional review board (IRB) procedures as surveys to assist with the identification of PD needs were considered routine evaluation activities.
Sample
The sample of survey respondents consisted of 955 professionals who provided services to infants, toddlers, and preschoolers age 0 to 5 (birth through 5 years). Table 1 shows the background characteristics of the respondents. The majority of respondents identified their disciplines or professions as EC education or ECSE (70%). It should be noted that the state offers both an ECSE endorsement for age birth through 5 years and a blended or unified early childhood (UEC) endorsement age birth to 8 years. As this state has had a blended or UEC licensure program for more than 20 years, some teachers who hold the blended or unified endorsement may have identified as an EC professional. Other disciplines that responded to the survey included speech and language pathology, occupational therapy, and physical therapy (18%), and the remainder represented eight additional disciplines or professions (12%).
Background Characteristics of the Survey Respondents.
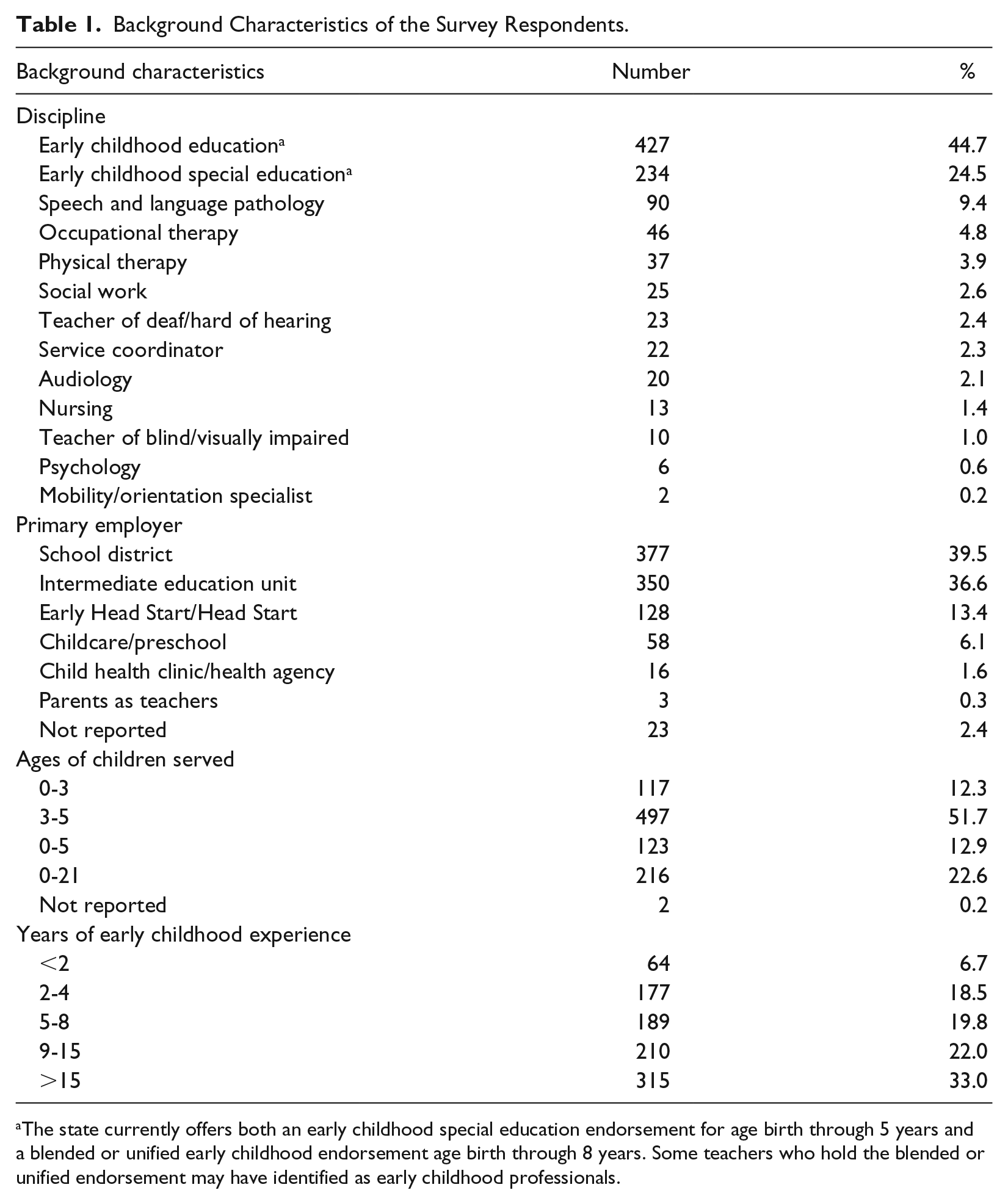
The state currently offers both an early childhood special education endorsement for age birth through 5 years and a blended or unified early childhood endorsement age birth through 8 years. Some teachers who hold the blended or unified endorsement may have identified as early childhood professionals.
The respondents were employed in EC programs in all of the nine IEUs in the state, across six different types of EC programs. The programs included school districts (40%), intermediate education agencies (37%), Early Head Start/Head Start programs (13%), childcare and preschool programs (6%), and other kinds of EC programs (4%). The respondents also reported working with birth to 3-year-old children (12%), 3- to 5-year-old children (52%), birth to 5-year-old children (13%), or children both younger and older than 5 years of age (23%). Three quarters of the practitioners had 5 or more years of experience working with young children, and 55% of the practitioners had 10 or more years of experience.
Survey
The respondents completed a survey that included information about their licensure, preservice and in-service experiences, and the extent to which they valued and were implementing the DEC RPs (DEC, 2014). The survey included practices in six of the DEC RPs’ strands: Assessment, Environment, Family, Instruction, Teaming and Collaboration, and Transitions. A seventh topic area, Interaction, was inadvertently omitted from the survey. Each strand included a number of practices that ranged from 2 (Transitions) to 13 (Instruction). Each respondent was asked to provide a judgment about their current use or implementation of each of the DEC RPs and their desired use of the DEC RPs. Both current and desired use was rated on a 5-point scale ranging from low to high. The respondents were instructed to score each DEC RP twice, first in terms of current implementation and, second, in terms of desired use of the practice. The respondents were also instructed not to complete any set of items or particular items if not applicable to their current position or role. As a result, the sample sizes for the topic area measures were not the same.
Data Preparation
To avoid Type I errors in the multiple statistical tests that were conducted on 47 individual practices, the responses to the current implementation ratings for each topic strand (except Transitions) were factor analyzed by principal components analysis with varimax rotation to identify subsets of practices measuring inherently similar types of practices. Each factor analysis, except one, resulted in two factor solutions. Teaming and Collaboration resulted in a one-factor solution. Table 2 shows the types of practices that loaded on each strand of assessment, instruction, environment, and family practices and an example of a practice for each set or subset of practices. The practice examples are based on the particular items that had the highest factor loadings in each set or subset of practices.
Types of Recommended Practices Constituting the Focus of Analysis.
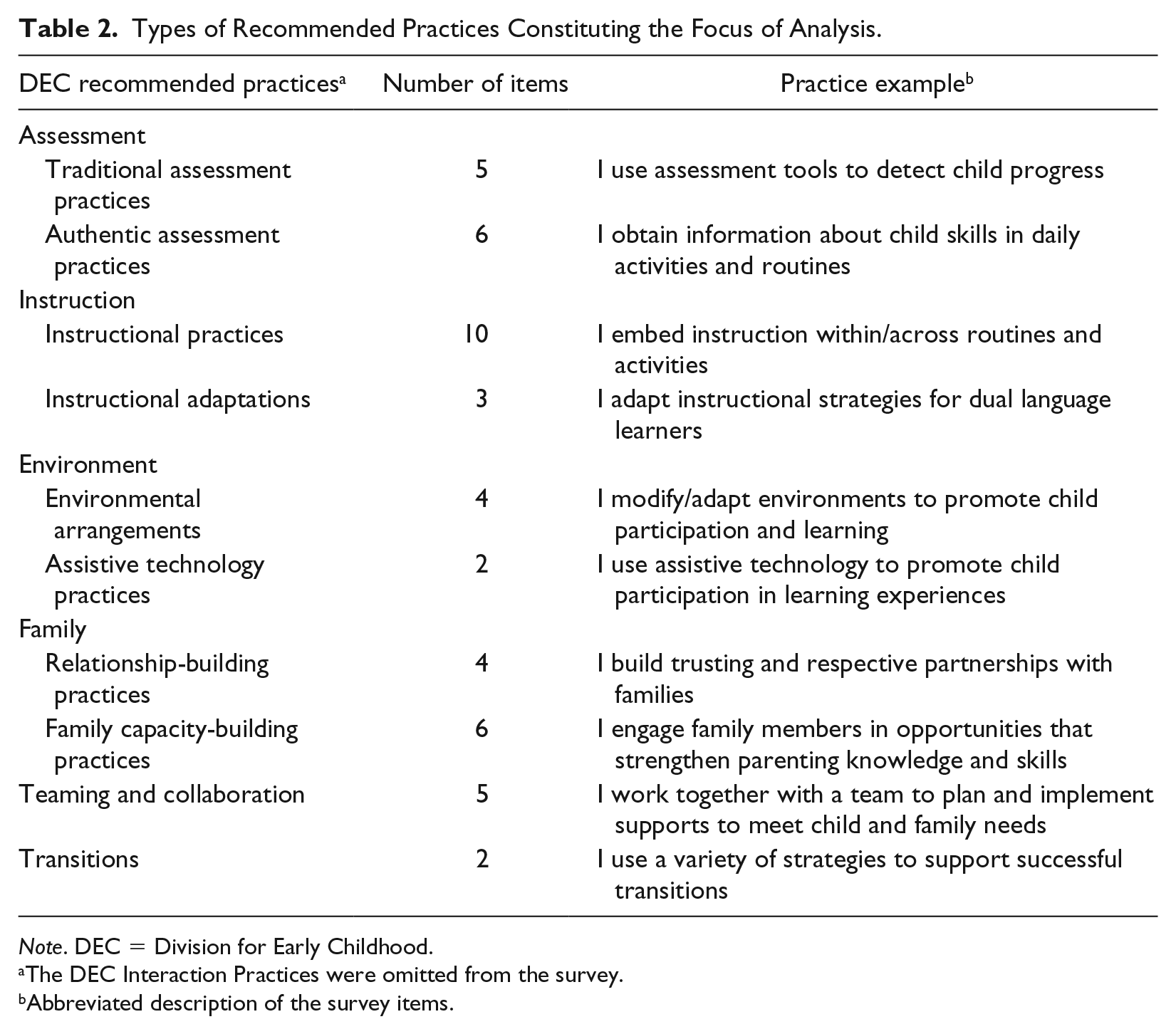
Note. DEC = Division for Early Childhood.
The DEC Interaction Practices were omitted from the survey.
Abbreviated description of the survey items.
Data Analysis
Paired t tests for the desired versus current implementation ratings were used to determine whether the differences between the two sets of ratings were zero. The dependent measures were the mean ratings for the items in each set or subset of practices (Table 2), so that each measure could range from 1 to 5. Statistical significance testing was supplemented with effect size estimates for the magnitude of differences for desired versus current implementation. Effect sizes, rather than statistical significance testing, were used for substantive interpretation of the survey results (Coe, 2002). The standardized mean difference effect sizes were computed as the average desired practices scores minus the average current practices scores, divided by the pooled standard deviation adjusted for the correlations between measures (Morris & DeShon, 2002). As noted by Morris and DeShon (2002), because the two sets of data were not independent, but rather correlated, the mean difference effect sizes needed to be adjusted with consideration to the degree of correlation between the desired and current practice measures. As a rule of thumb, Cohen’s d effect sizes between 0.20 and 0.49 are considered small, ds between 0.50 and 0.79 are considered medium, ds between 0.80 and 1.19 are considered large, and ds 1.20 or higher are considered very large (Ellis, 2010).
The extent to which valued or desired practices were related to current use of the practices was determined in two ways. First, we computed Spearman’s rank order correlations for the relationships between the average scores for the 10 sets of practices shown in Table 3, and for the percent of practice indicators rated the highest on a 5-point scale for desired and current implementation of practice. This was because the average scores for the three practice strands were the same, though this was not true for the percent of indicators (see Table 3). We also computed the pairwise Cohen’s d effect sizes for all between practice strand mean scores to determine whether respondents valued certain practices more than others (desired) and considered themselves more proficient in certain practices (current implementation). The mean difference effect sizes were computed using the same formula described above for both sets of data.
Paired t-Test Results and Effect Size Estimates for the Desired Use and Current Implementation of the Recommended Practices.
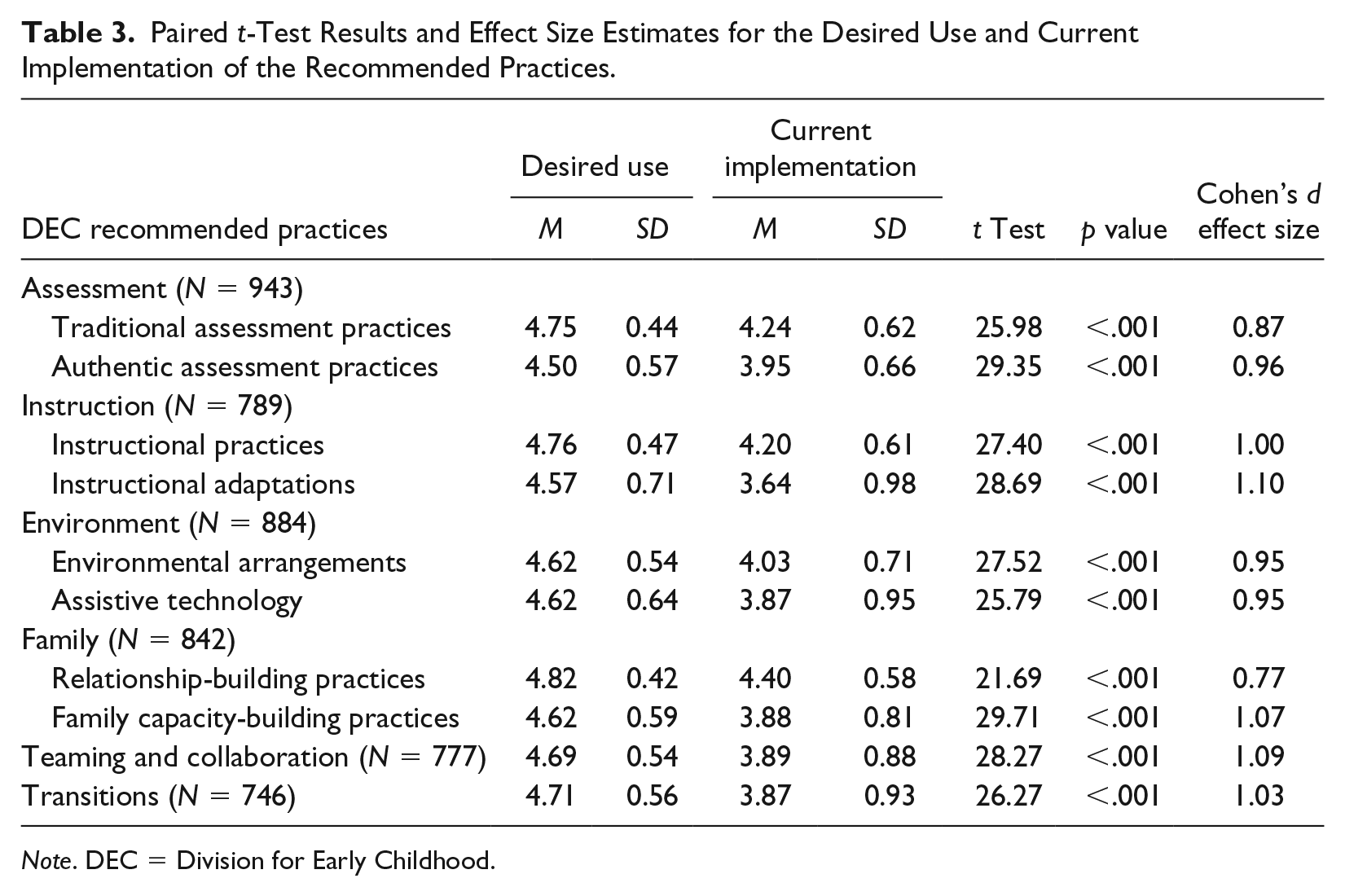
Note. DEC = Division for Early Childhood.
Whether the gap between valued or desired practices and the current use of the practices has narrowed, remained the same, or has widened was evaluated by comparing the sizes of effects and 95% confidence intervals (CIs) from the current study and those from earlier DEC RPs validation studies (McLean et al., 2002; Odom et al., 1995). A CI not including zero indicates that the average effect differs significantly from zero at a p < .05 level (Shadish & Haddock, 2009). The comparisons were limited to practice strands that overlapped with the assessment, instruction, assistive technology, family, and transition DEC RPs in the present study. These included the assessment, family participation, general curriculum, and transition practices in the Odom et al. (1995) validation study, and the assessment, child-focused intervention, family-based practices, and technology application practices in the McLean et al. (2002) validation study. A between-validation study independent samples Kruskal–Wallis test was used to determine whether the average effect sizes for desired versus current use of the DEC RPs were significantly different. These effect sizes were also regressed on the year of each study to ascertain whether there was a decrease in the gap between desired versus current use of the practices.
Results
Desired Versus Current Implementation
Table 3 shows the results from the 10 sets of desired versus current implementation analyses. All of the paired t tests were significant at the p = .001 level and all of the effect sizes for the between-contrast differences were large. The effect sizes ranged from 0.80 (relationship-building practices) to 1.06 (teaming/collaboration and transitions). In all 10 analyses, current implementation of a practice was rated lower than the value of the practice was rated (desire to use). The sizes of effects indicated large discrepancies in the practitioners’ ratings of desired or valued use and current implementation of the practices.
Relative Importance of the Recommended Practices
Table 4 shows the rank ordering of the participants’ judgments of desired use and current implementation of each practice area based on the mean scores in Table 3. The rank order correlation was rs = .63, p = .026. The average percent of the desired DEC RPs rated 5 was 75.93% (SD = 5.51, range = 66-85) and the average percent of the current use items rated 5 was 36.81% (SD = 8.07, range = 25-53). The rank order correlation of the percentages was rs = .72, p = .010. Both results indicated that the more the respondents valued certain practices (desired use), the more likely they indicated they used the practices (current implementation). As shown in Table 4, relationship-building, instructional, and traditional assessment practices were most valued (desired) and more often used (current implementation). In contrast, instructional adaptations and authentic assessment practices were less valued (desired), whereas instructional adaptations were the least used practices. There were, as described next, a number of differences between the practices that were valued and those that were used, as evidenced by mean effect size differences.
Rank Ordering of the Practitioners’ Average Ratings of the Desired Use and Current Implementation of the DEC Recommended Practices.
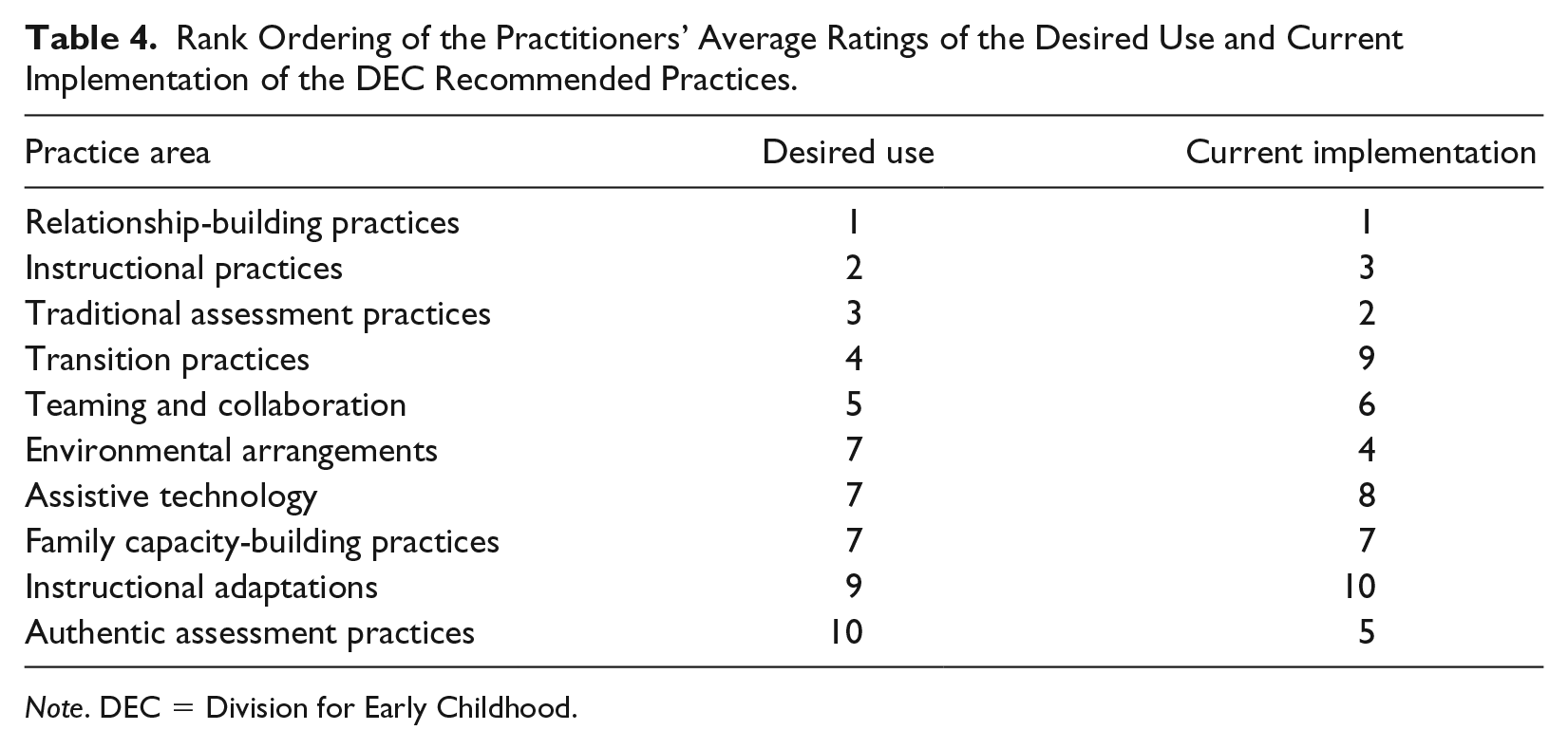
Note. DEC = Division for Early Childhood.
The effect sizes for all between practice area comparisons are shown in Table 5. There were large numbers of between practice area effect size differences for both the current and the desired use of the 10 sets of practices as demonstrated by the number of mean difference effect sizes for the between practice area comparisons beyond what would be expected by chance. Twenty-five of the 44 comparisons (56%) for desired use, and 31 of the 44 comparisons (69%) for current implementation, had small to large effect size differences. The sizes of effects for the between practice area comparisons were larger for current implementation compared with desired use, as shown by the average effect sizes for the two sets of results. The average effect size for desired use was d = .23, 95% CI = [.18, .27], whereas the average effect size for current use was d = .36, 95% CI = [.28, .43], t(88) = 78.66, p = .0040.
Cohen’s d Effect Sizes for All Between Recommended Practice Area Comparisons.
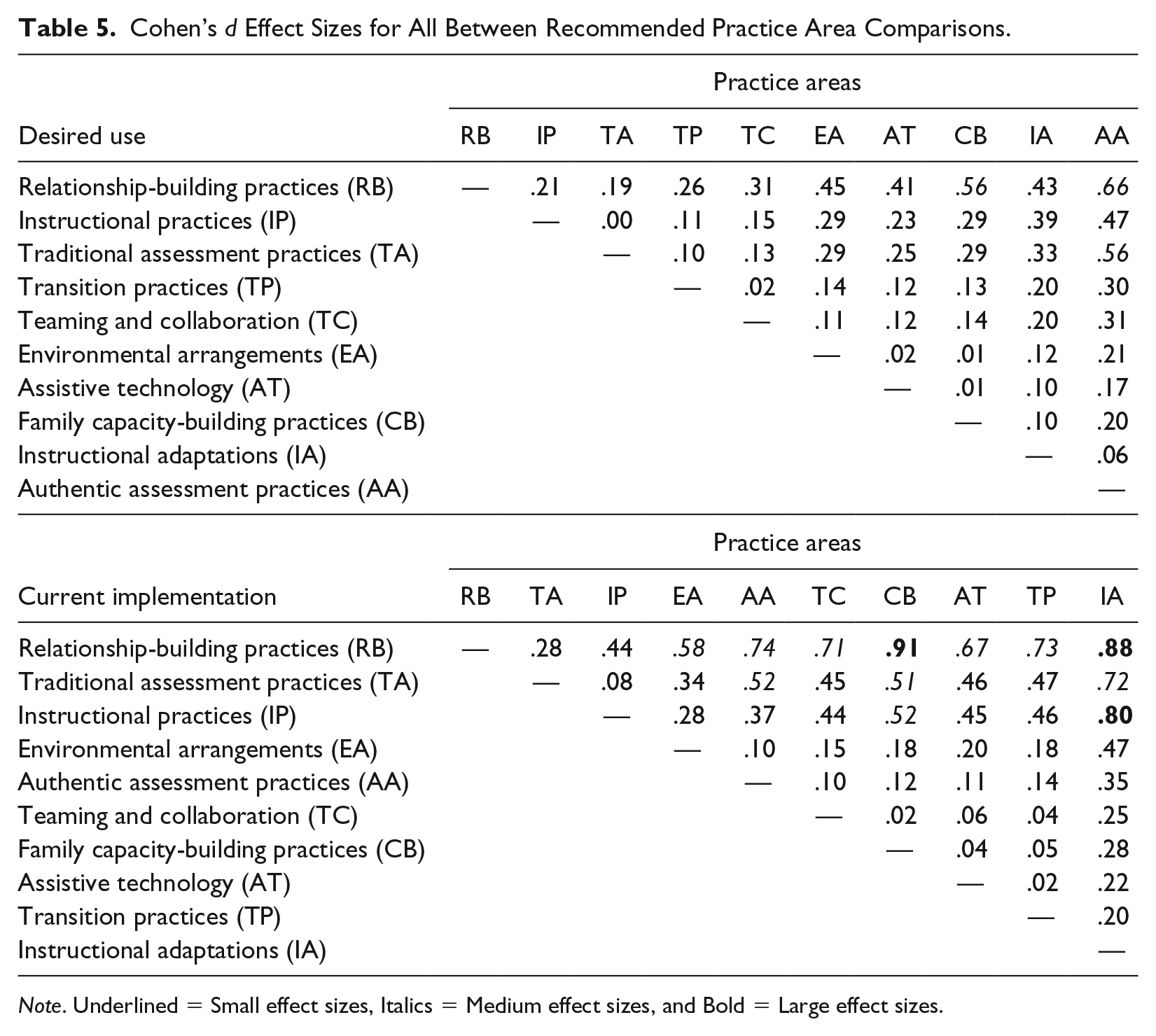
Note. Underlined = Small effect sizes, Italics = Medium effect sizes, and Bold = Large effect sizes.
Several discernible patterns of results are evident in Table 5. First, relationship-building practices were the most valued and most used practices, in comparison with every other practice area. Second, instructional and traditional assessment practices were judged as more valued than all other practices. These two practices were also used more often than all other practices. Third, authentic assessment practices were the least valued practices, as evidenced by the fact that the mean difference effect sizes for every other topic area were all small or medium (except assistive technology). In contrast, instructional adaptations were the least used practices for the same reason. Taken together, the results in Table 5 indicate considerable variability in the practitioners’ appraisals of desired and current use of the 10 different sets of DEC RPs. Both sets of between-practice comparisons indicate that certain practices were valued more than other practices, and that certain practices were used more frequently than other practices.
Validation Study Comparisons
The average effect sizes for practitioners’ judgments of desired versus current use of the DEC RPs for topic areas are shown in Figure 1 for the data reported in Odom et al. (1995), McLean et al. (2002), and the present study. These results need to be considered best estimates for three reasons. First, practitioners’ judgments in the Odom et al. (1995) and McLean et al. (2002) studies were made in response to the same two questions: “Is this a recommended practice?” (importance) and “To what extent is this practice followed by programs with which you are familiar?” (current use). The present study assessed importance and use in terms of each respondent’s judgments of his or her own beliefs about the value of importance of a practice and use of a practice. Second, the standard deviations in the Odom et al. (1995) study on the scores for mean importance and current use had to be estimated as they were not reported in any publication about the data source (McLean & Odom, 1996). These estimates were based on results in the McLean et al. (2002) study. Third, whereas the effect sizes in the current study were adjusted for the correlations between desired and current use (Morris & DeShon, 2002), this was not possible for data in the two previous validation studies because the correlations between RPs and use of the practices were not reported.
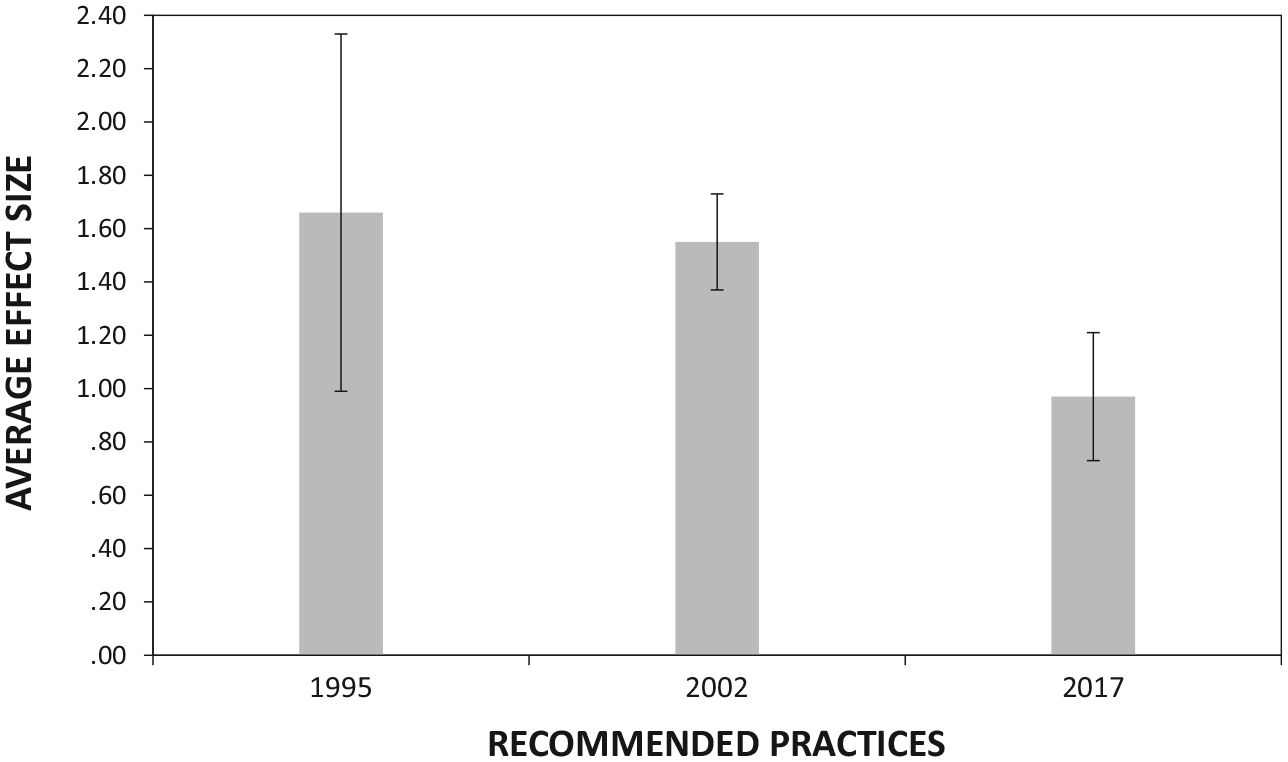
Average effect sizes and 95% confidence intervals for the mean differences in the importance and use ratings of the DEC recommended practices in the 1995 (Odom et al., 1995), 2002 (McLean et al., 2002), and in the 2017 (current study) validation studies.
Notwithstanding between-study methodological differences, the results in Figure 1 indicate that (a) the average effect size differences for valued and currently used practices were very large in both the 1995 and 2002 validation studies, and (b) the average effect size differences for valued and currently used practices in the present study were large. There was, however, a statistically significant between-validation study difference in the average sizes of effects, H = 7.72, df = 2, 10, p = .021, and a significant linear decrease in the size of effects across time, β = –.82, t(11) = 4.82, p = .001. The results indicate that there are still large differences between the practices which are valued and practitioners’ use of these practices, as evidenced by the absence of zero in the 95% CIs for all three average effect sizes.
Discussion
Findings from the survey described in this article indicated that there were large discrepancies in EC practitioners’ judgments of the value, and desired use of the DEC RPs, and their current implementation of the practices. These results are consistent with findings in earlier studies that examined the relationship between practitioner belief appraisals of different kinds of practices and their use of the practices (see, for example, Fang, 1996; Trivette, Dunst, Hamby, & Meter, 2012). This pattern of results is best understood by considering the practitioners’ judgments of desired practices as a proxy for social validity appraisals (Foster & Mash, 1999; Luiselli & Reed, 2011) and their judgments of current implementation as a proxy for self-competence appraisals (Bruder et al., 2011). Similar findings have been reported in previous studies where participants made judgments about practices using ideal ratings (Bailey et al., 1992), importance ratings (Murphy et al., 1995), agreement ratings (McLean et al., 2002; Odom et al., 1995) in comparison with their rating their typical use (Bailey et al., 1992), current performance (Murphy et al., 1995), and current use of practices (McLean et al., 2002; Odom et al., 1995).
Although the gap between the valuing of a practice and implementing the practice seems to have narrowed in comparison with findings in earlier studies (McLean & Odom, 1996; McLean et al., 2002; Odom et al., 1995), the effect sizes for desired versus current use of the DEC RPs reflect ongoing challenges to implementation as reported by the survey respondents.
This study also adds to our understanding of the relationship between socially valued practices and self-competence appraisals by showing that the 10 strands of DEC RPs were differentially valued by the practitioners, and that these values were related to differences in self-competence appraisals. Results indicated that the more a practice was valued, the more the practitioners reported using the practice. The relationship between valued and current use of the DEC RPs is important because it has been suggested that subjective judgments of the importance and acceptability of intervention practices influence the adoption and use of practices (e.g., Dunst, Raab, & Hamby, 2016; Strain, Barton, & Dunlap, 2012; Wainer & Ingersoll, 2013; Wehby, Maggin, Moore Partin, & Robertson, 2011). Strain et al. (2012), for example, noted that these relationships are important because they help explain the conditions under which any kind of intervention practice is likely to be used by practitioners. This type of relationship was found in a study of PD provided to a group of Head Start teachers. The social validity ratings given to an intervention practice taught during the PD influenced the teachers’ responsiveness to learning the intervention practices (Trivette, Raab, & Dunst, 2014).
Another explanation for the correlation found with the practitioners’ positive appraisal of a practice, and their implementation of the practice, could be related to the feelings of self-efficacy they experience when using a practice. That is, one could question whether valuing a practice would encourage a practitioner to consistently use the practice, or whether consistently using a practice resulted in positive child and family outcomes, and these results encouraged the practitioner to implement the practice with competence. As noted by both Desimone (2009) and Guskey (2002), most educators are interested in improving learner outcomes, and when explicit emphasis is placed on practice–outcome linkages, practitioners will more likely see benefits of investing time and energy in learning to use a practice.
The results reported in this article have a number of implications for advancing the adoption and use of intervention practices, several of which we highlight. One implication has to do with the continued gap in desired and current use of practices, in this case the DEC RPs. After nearly 25 years of existence, it is disconcerting to have such gaps between the perceived values of the DEC RPs versus their use by practitioners. An implication of this gap is to further examine how practitioners are taught to use the DEC RPs and other interventions, during both preservice preparation programs and in-service activities. That is, a distinction must be made between the implementation of recommended ECI practices and the adult learning methods and practices used by faculty and PD trainers to promote practitioners’ use of effective intervention practices.
It has long been suggested that adult learning practices be embedded in preservice preparation and ongoing in-service PD activities in ECSE (Bruder, 2010, 2016; Bruder & Nikitas, 1992; Dunst, 2015; Dunst, Trivette, & Hamby, 2010; Gomez, Kagan, & Fox, 2015). As noted by Dunst and Trivette (2009), “no intervention practice, no matter its evidence, is likely to be learned and adopted if the methods and strategies used to teach or train . . . practitioners . . . are not themselves effective” (p. 164). Fixsen, Naoom, Blase, Friedman, and Wallace (2005) made this distinction in terms of implementation practices (e.g., PD) and intervention (e.g., recommended) practices and the need to use both with fidelity to produce observed and enduring changes.
Effective adult practices have most recently been described through a metasynthesis of 15 research reviews of in-service PD that were found to be associated with changes and improvements in educator and student outcomes (Dunst, Bruder, & Hamby, 2015). All 15 research syntheses reported or described core features or conditions under which in-service PD was found to be most effective. These included (a) trainer introduction, demonstration, and explanation of the benefits of mastering content knowledge or practice; (b) active and authentic teacher learning experiences; (c) opportunities for teachers to reflect on their learning experiences; (d) coach or mentor supports and feedback during the in-service training; (e) extended follow-up supports to reinforce in-service learning; and (f) in-service training and follow-up supports of sufficient duration and intensity. The results of these syntheses provide guidance for any in-service PD activity that is focused on the improvement of practitioner knowledge and skills and child outcomes. To lessen the gap between valued and actual implementation of the DEC RPs as was found in this study, it could be recommended that both preservice preparation and in-service PD include the six core features of adult learning that are associated with positive outcomes to ensure practitioner competence using the DEC RPs.
Another implication is the need for a continuum of preservice teaching and in-service PD support available for practitioners (Bruder, 2010). The DEC RPs are of value only when practitioners are able to implement them with fidelity across all infants and young children and families. To ensure this happens, both EC faculty at IHEs and state ECI PD providers must align the pedagogy of the training and support they provide to those serving children age birth to 5 years. This alignment of knowledge and skills should be competency-based and represent a continuum of high leverage EC personnel standards (preservice) and intervention practices (in-service) that reflect the evidence we have to improve outcomes for children, family, and systems. Furthermore, this type of continuum could be personalized and driven by the practitioners’ self-assessment of their own ECI competency (Bruder, 2016).
Limitations
As was the case in previous studies of desired and current use of the DEC RPs (McLean et al., 2002; Odom et al., 1995), this study has certain limitations. A first limitation was in the sampling procedure and sample. As noted, the state did not have a list of those in the population to be sampled. The sample could have been limited and skewed by the snowball recruitment method, though the respondents were representative of the demographic of the target population. A second limitation was the fact that the study was conducted in only one state. Thus, we do not know whether similar results would have been found if practitioners were surveyed more broadly across other states. A third limitation, which was also the case in previous studies (McLean et al., 2002; Odom et al., 1995), was the rating scale used to measure the desired use and current implementation of PRs. The scales in all three studies included nonoperationally defined markers that may have skewed response patterns. Finally, the reliance on the practitioners’ personal judgments of desired use and current implementation of RPs could be a limitation. Respondents may have assigned judgments based on personnel experiences, education, values, familiarity with the terms that were used, as well as a host of other differing variables. Notwithstanding these limitations, the results of this study demonstrate the current status of practitioners’ judgments of valued practices, their use of the practices, and the extent to which they use the practices in their everyday interactions with young children and their families.
Conclusion
The results in this study are consistent with findings in other studies demonstrating a discrepancy between practitioners’ appraisals of the value of different practices and their ability to actually implement the practices (see, for example, Fang, 1996; Trivette et al., 2012). In addition, the findings on the differential values assigned to the DEC RPs by practitioners in this survey suggest a need to continually assess the abilities of practitioners to implement practices they value as being effective to facilitate child and family change. Finally, the results provide evidence that the practitioners who responded to the survey value the DEC RPs, which would suggest that they are ready to adopt and use them.
This survey was administered to assess the needs of EC practitioners and to examine preservice, practitioner licensure, and in-service reform as part of a statewide CSPD initiative. The results suggest a need to embed opportunities for practitioners to learn to implement the DEC RPs during both their initial preservice preparation and through ongoing in-service PD activities that jointly align to EC pedagogy and state licensure. These findings will be embedded into this state’s CSPD infrastructure to support and facilitate the EC workforce to implement the most effective interventions for each child and family.
Footnotes
Authors’ Note
Angela Van Polen is now affiliated with Positive Early Learning Experiences Center, University of Denver. Gloria Frolek Clark is now affiliated with Private Practice, Adel, IA, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.