
Abstract
One of the earliest indicators of autism spectrum disorder (ASD) is delay in language and social communication. Despite consensus on the benefits of earlier diagnosis and intervention, our understanding of the language growth of children with ASD during the first years of life remains limited. Therefore, this study compared communication growth patterns of infants and toddlers with ASD to growth benchmarks of a standardized language assessment. We conducted a retrospective analysis of growth on the Early Communication Indicator (ECI) of 23 infants and toddlers who received an ASD diagnosis in the future. At 42 months of age, children with ASD had significantly lower rates of gestures, single words, and multiple words, but significantly higher rates of nonword vocalizations. Children with ASD had significantly slower growth of single and multiple words, but their rate of vocalization growth was significantly greater than benchmark. Although more research is needed with larger samples, because the ECI was designed for practitioners to monitor children’s response to intervention over time, these findings show promise for the ECI’s use as a progress monitoring measure for young children with ASD. Limitations and the need for future research are discussed.
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by the early onset of behavioral deficits in the domains of social interaction and communication, and conversely, behavioral excesses in children’s display of restricted, repetitive behaviors and interests. Delay in expressive language is one of the earliest warning signs for infants who go on to develop ASD, including lack of babbling with their parents (Bryson et al., 2007), and challenges directing their vocalizations during interactions with others (Garrido et al., 2017). We know that these early, foundational language skills affect the development of later skills. For instance, the production of meaningful first words by 24 months of age is a predictor of functional outcomes, including better cognitive and adaptive skills, over 2 years later (Mayo et al., 2013). Importantly, the number of words produced by 2.5 years of age also has been found to be an important predictor of the expressive language, cognitive ability, and adaptive behavior of children with ASD (Kover et al., 2016). Thus, there is a general consensus that language skills are important intervention targets for children with ASD, and that intervention should target these skills early because they represent a pivotal domain that affects children’s long-term developmental potential.
Although not specific to ASD, delayed expressive communication is commonly reported and observed for many children later diagnosed with the disorder. Indeed, most clinicians can recall profound encounters with parents asking them to “help their children talk.” The onset of functional spoken words by the age of 5 years is one of the more robust predictors of positive outcomes for individuals with ASD. In fact, lack of expressive language by this age is such a strong predictor of poor adaptive outcomes into adulthood that we now have identified these children as being “minimally verbal” (Tager-Flusberg & Kasari, 2013), and developed interventions to target this at-risk subgroup of children with ASD (Goods et al., 2013; Kasari et al., 2014). It is well established that the earlier a delay in expressive communication can be identified, the more likely intervention will improve future outcomes (Hampton & Kaiser, 2016; Lane et al., 2016). However, intervention effects vary based on intervention and severity of autism symptoms (Rose et al., 2016). Furthermore, prevalence rates of ASD in males far exceeds females (Fombonne, 2005; Kreiser & White, 2014), but it is less clear whether or not there are gender differences in early communication for young children with ASD (Harrop et al., 2016). Van Wijngaarden-Cremers and colleagues’ (2014) meta-analysis revealed no significant gender differences in early communication across six studies of toddlers and preschoolers with ASD. However, due to the limited number of studies and small sample sizes, more research is needed to inform these findings (Halladay et al., 2015).
Limited Standardized Communication Measures Sensitive to Growth
The field has made progress in developing measures that help characterize the language of children with ASD. However, to date, there remains a dearth of standardized early language measures that are sensitive to change over time (Anagnostou et al., 2015; Bacon et al., 2014; Bolte & Diehl, 2013) and can be used by early childhood practitioners to inform intervention decision-making. Undeniably, the complex and often context-bound nature of language use—together with the unique communication deficits observed in young children with ASD (e.g., difficulty integrating gestures with words)—make it difficult to develop comprehensive outcome measures. Still, the lack of validated communication outcome measures has stifled intervention research efforts because it is difficult to (a) determine if some interventions are truly ineffective, (b) detect incremental changes that may occur for children with ASD, and (c) isolate communication growth that occurs as a result of intervention from growth that would have occurred without intervention.
Current outcome measures often require such extensive examiner training and administration time that it is difficult to integrate them into publicly funded early childhood services (e.g., Early Head Start [EHS] and Part C). This is a critical barrier because these services are the context through which many of the youngest children are first identified for diagnostic evaluation and ultimately receive ASD intervention. Practitioners in these programs need measures that allow them to monitor children’s response to intervention and better individualize their services for children and families (Akers et al., 2015; Moreno & Klute, 2011). To address this concern, Autism Speaks initiated a series of expert consensus workgroups to guide the evaluation and development of research on treatment outcome measures in autism and related disorders (Anagnostou et al., 2015). For the social-communication domain, the working group evaluated 38 measures that had relevant subscales. Table 1 lists six measures that were judged to be “appropriate” for outcome measurement purposes. As described by Anagnostou and colleagues (2015), each of these measures has value to the field, particularly for large-scale clinical trials. However, these measures are not typically used by interventionists to inform intervention decisions or monitor the progress of a child with ASD over time. Table 1 summarizes the characteristics of each measure identified by the working group that limit their use by interventionists. More information about the working group and their recommendations are available elsewhere (e.g., Anagnostou et al., 2015; Scahill et al., 2015). Finally, it is worth noting that the Preschool Language Scale, a common language outcome measure used in research (Buzhardt et al., 2020) but not included in the Autism Speaks workgroup, involves a lengthy administration, and its standard scores are prone to floor effects in this population.
Measures Identified by Autism Speaks to Assess Autism Treatment Outcomes.
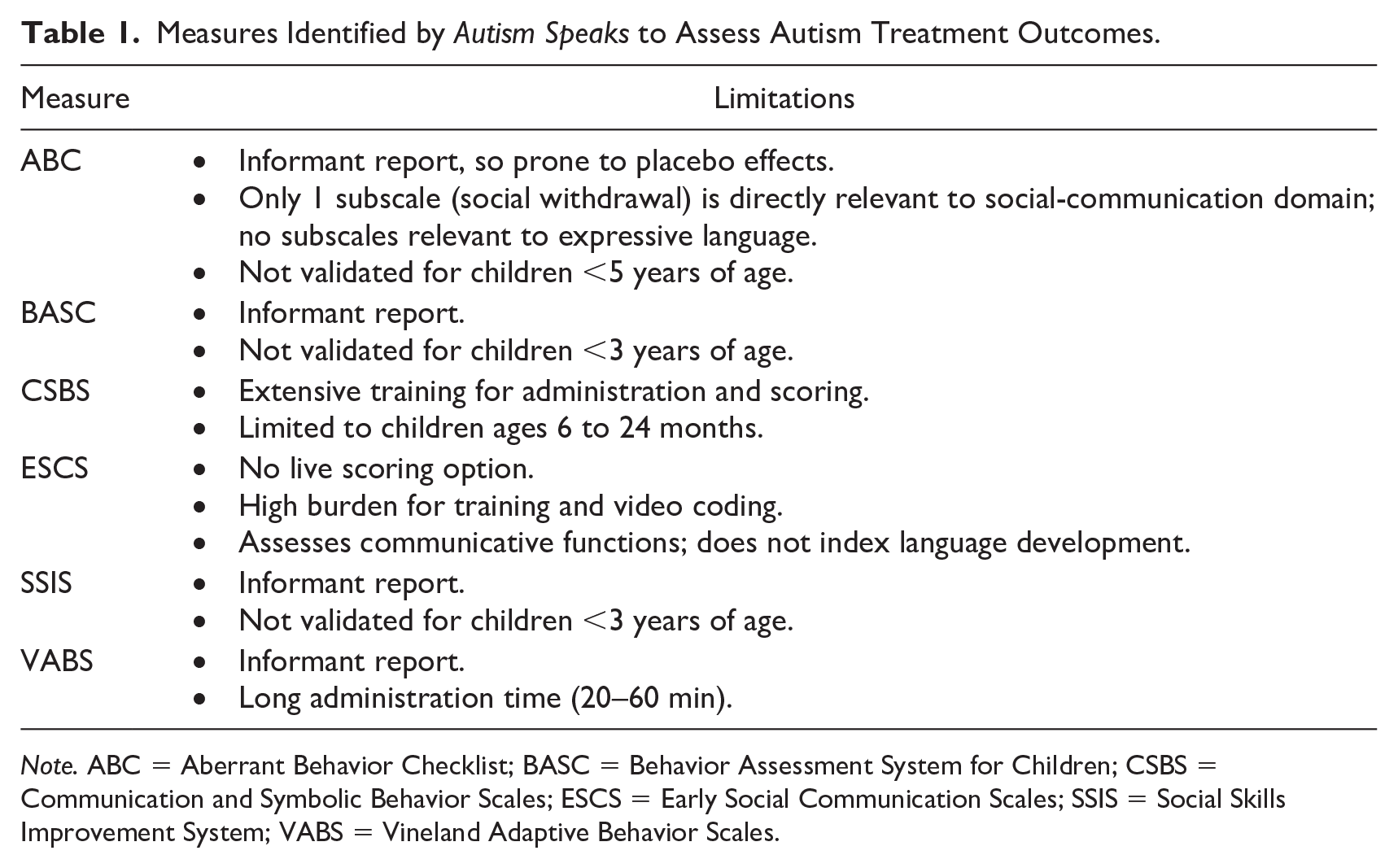
Note. ABC = Aberrant Behavior Checklist; BASC = Behavior Assessment System for Children; CSBS = Communication and Symbolic Behavior Scales; ESCS = Early Social Communication Scales; SSIS = Social Skills Improvement System; VABS = Vineland Adaptive Behavior Scales.
Recent trends in ASD treatment research, in particular, suggest a need for a different approach to language outcome measurement. This includes advancements in clinical trial designs with the application of adaptive trials, such as Sequential Multiple Assignment Randomized Trial (SMART) designs, to behavioral treatment research. Notably, Kasari and colleagues (2014) used adaptive trials to manipulate treatment dosage for minimally verbal children with ASD who are intervention nonresponders. To titrate dosage, these designs require assessment tools that can be quickly administered and scored to derive a “cut point” (i.e., identifying those children who do or don’t respond to the initial treatment regimen) based on a continuous score. At issue is that most current observational measures of language or social-communication are not brief enough to be easily administered to large samples to derive such cut points.
The Early Communication Indicator for Infants and Toddlers
The Early Communication Indicator (ECI) is one of the Individual Growth and Development Indicators (IGDIs) for infants and toddlers (Carta et al., 2004). The IGDIs were developed to address the need for brief measures of children’s growth in key domains that can be used to inform intervention decisions. The ECI, normed for children 6 to 42 months of age, measures children’s expressive communication through their use of four key skill elements: gestures, nonword vocalizations, single words, and multiple words (Greenwood, Carta et al., 2006). These key skills represent children’s progression from using prelinguistic means of communication through gestures and canonical babbling to express their needs, to more advanced linguistic means that include words and phrases. Prior studies have found that the observed dynamic relationship between these key skills is consistent with language development theory (Greenwood et al., 2013). For example, analyses of key skill growth trajectories consistently show accelerated rates of vocalizations until about 14 to 20 months of age, followed by a rapid decrease as single words develop; a similar rise and fall is observed for single words at about 30 to 36 months of age as children begin to use more multiple words (Greenwood et al., 2010, 2018).
Frequency counts of the child’s use of these key skills are coded by a trained observer while the child interacts with an adult play partner around a standardized toy set. The counts are entered into a web application, which generates progress monitoring graphs showing the child’s score relative to their age-based benchmark. As more assessments are administered over time, the child’s growth trajectory is calculated and graphed by the web application, displaying the child’s growth relative to expected growth at that age. Also, by indicating when an intervention or change in services began, the child’s current progress can be compared with growth prior to the change.
Figure 1 illustrates how a child’s ECI progress monitoring graphs (generated by the IGDI web application) support early identification of children at risk for language delay, as well as examination of a child’s response to intervention on this general outcome. The ECI’s Weighted Total Communication displayed in Figure 1 is the sum of the four key skill elements with additional weight given to the single-word and multiple-word key skills (Greenwood et al., 2010). Similar progress monitoring graphs are also generated for each of the ECI’s key skills, providing information that can be used by practitioners and interventionists to identify specific intervention strategies that target areas of need.
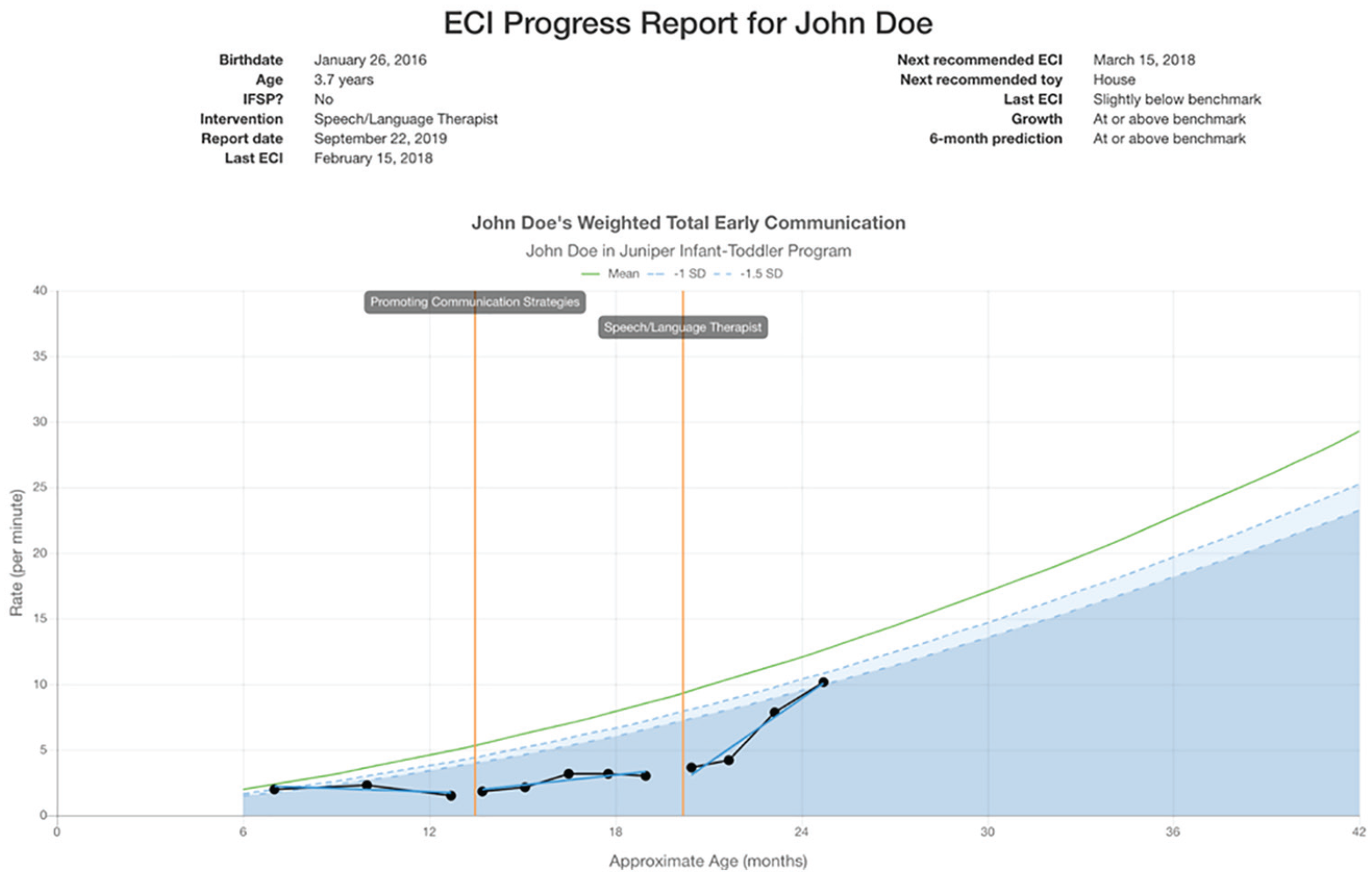
Sample progress monitoring graph from the IGDI web application displaying a child’s growth on the ECI’s Total Weighted Communication from 7 to 25 months of age, with a change in intervention services at 13 months and another at about 20 months of age.
The ECI has also shown sensitivity to individual differences among children, particularly those with disabilities. Comparisons of ECI growth patterns between children with and without an Individualized Family Service Plan (IFSP; i.e., an identified disability) demonstrate clear differences in the trajectories between these groups of children. For example, Greenwood and colleagues (2010) examined the ECI scores of children (n = 5,883) served by EHS and found that peak onset of nonword vocalizations occurred later and decreased slower for children with an IFSP, relative to children without an IFSP. In addition, for children with an IFSP, growth in single word use grew at a slower rate up to 24 months of age and use of multiple words was lower at 36 months of age.
Using the ECI to Support Intervention
The ECI has demonstrated promise in clinical trials investigating intervention effects on growth in expressive communication among infants and toddlers. In two separate cluster randomized controlled trials, EHS home visitors used the ECI to monitor language growth of children on their caseloads. Under investigation was the effect of home visitors’ use of an application to guide their data-driven decision-making practices. Because the ECI is designed for frequent administration, variation in children’s growth (i.e., slope) in expressive communication was used as an outcome measure rather than pre- and posttest performance based on a single assessment. In both studies, home visitors administered the ECI quarterly for all children to identify those who may be at risk for language delay. In the first study, (Buzhardt et al., 2011), children with home visitors in the experimental group demonstrated significantly stronger growth on the ECI relative to comparison children at a 6-month follow-up, p < .05, d = 0.41. Similarly, in the second, larger study (Buzhardt et al., 2018; 2020), children with home visitors in the experimental group grew at a significantly faster rate on the ECI than children served by comparison home visitors at a 6-month follow-up (p < .01, d = 0.56). Follow-up ECI data in both studies showed increased effect sizes at 9 months for the first study (d = 0.71) and at 12 months in the second study (d = 1.12), further demonstrating the ECI’s sensitivity to detect change over sustained periods of time.
Despite evidence that the ECI is sensitive to a child’s general disability status, to date, there have been no formal investigations of the measure’s sensitivity to specific diagnoses, such as ASD. Although the ECI has been used with thousands of children, and those assessments are stored in a central database, there are barriers to evaluating how it performs for children with diagnosed disabilities. Namely, although infants and toddlers may be identified as “at risk” for a disability or have a documented delay in a general domain (e.g., communication, motor skills, and adaptive skills), specific developmental disabilities, such as ASD, are often diagnosed at later ages. Because of this, information about specific disabilities is rarely entered into the ECI’s web application. Therefore, an exploratory analysis of children in the data system who received ECI assessments and who would go on to receive an ASD diagnosis in the future was warranted. For this purpose, we were able to identify a sample of children from an ASD diagnostic registry in a Midwestern city who had also received at least one ECI from a local EHS program.
Purpose of This Study
In this study, we sought to conduct exploratory analyses of ECI scores of children known to either have an ASD diagnosis at the time of administration (i.e., with ASD) or would receive a diagnosis in the future (i.e., at-risk for ASD) based on data from a local diagnostic registry. The registry also contained children’s scores from other assessments, allowing us to explore the degree to which other child-level variables are related to ECI performance of children with ASD. Comparing their ECI scores to the measure’s normative benchmarks provides preliminary, but meaningful, evidence of the measure’s psychometric properties for this subpopulation, as well as an initial ECI profile for children with or at-risk for ASD. Research questions and hypothesis are as follows:
Method
Participants
Benchmark sample
ECI scores of children with ASD were compared with the scores of the sample of children used to establish the ECI’s current benchmark scores (Table 2). These children (n = 5,883) were enrolled in EHS across 27 Midwestern programs, and thus, were not a nationally representative sample. EHS provides home visiting and/or center-based services for low-income families (i.e., at or below the federal poverty level) with children up to 36 months of age. Overall, 62% of the children received EHS services in parents’ homes, 36% received center-based services, and the remaining 2% received services in some other home-based setting (e.g., grandparent or foster parent). The programs serving these children adopted the ECI as part of their standard services to monitor their children’s language growth and to inform screening decisions related to potential language delay. They also reported aggregated ECI data as part of their state and federal reporting requirements of child outcomes. In this sample, 471 children (8%) received Part C services at some point during their enrollment in EHS, and thus had an IFSP designed to provide early intervention services and additional parent resources to address identified delays. Additional details about the sample and the ECI’s psychometric properties are available in Greenwood and colleagues (2010).
Benchmark Sample Characteristics.
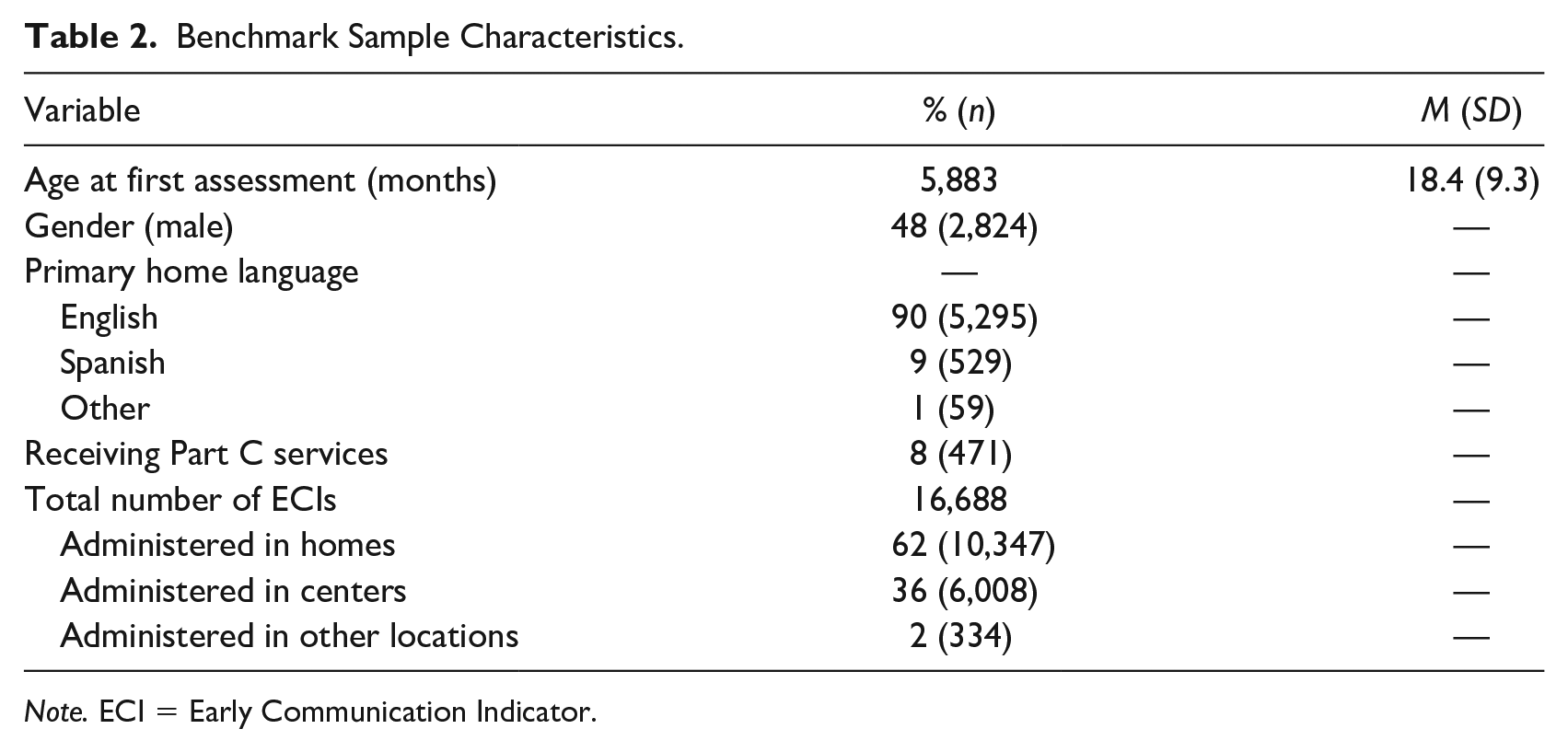
Note. ECI = Early Communication Indicator.
ASD sample
Data were drawn from an ASD diagnostic clinic in an academic medical center in a large metropolitan area. The sample (Table 3) included 23 children who met the following criteria: (a) received an autism (n = 21) or Pervasive Developmental Disorder–Not Otherwise Specified (n = 2) diagnosis either before or after their ECI assessment(s) and (b) had at least two ECI assessments in the IGDI web application.
ASD Sample Characteristics.
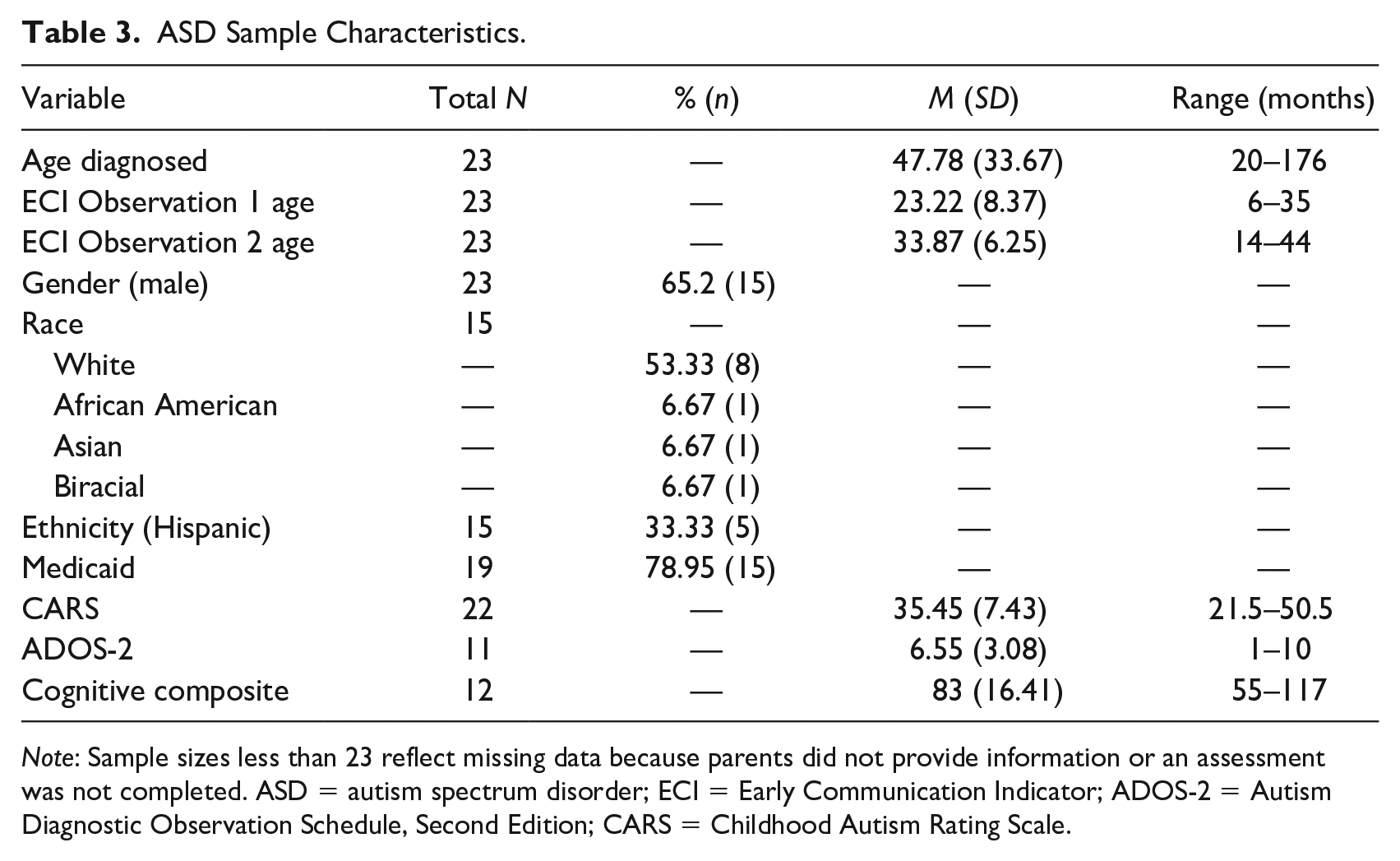
Note: Sample sizes less than 23 reflect missing data because parents did not provide information or an assessment was not completed. ASD = autism spectrum disorder; ECI = Early Communication Indicator; ADOS-2 = Autism Diagnostic Observation Schedule, Second Edition; CARS = Childhood Autism Rating Scale.
Procedures
Diagnostic registry
The ASD diagnostic center maintained records of children who completed intake paperwork or received a diagnostic evaluation for a range of neurodevelopmental disabilities. For this study, records from 2000 to 2018 were included, which means that children were diagnosed with autism using either the fourth edition of Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994) or the fifth edition of Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013) criteria. The registry contains detailed information collected as part of a multidisciplinary diagnostic evaluation, including medical history, clinical diagnostic interview, and standardized assessment measures, including developmental/cognitive, adaptive, and behavioral checklists. For each child, a multidisciplinary team made a final diagnostic determination of ASD based on available standardized measures, clinical observations, diagnostic interview, and medical interview/case history. No researchers involved in this study have ever been a part of the center’s multidisciplinary team.
The availability of data from other assessments allowed us to explore relationships between the language growth of infants/toddlers with ASD and other theoretically relevant variables, including cognitive functioning and autism severity. So, although these assessments vary in their administration and how they characterize constructs such as “cognition,” they were the standardized measures chosen by the diagnostic center’s multidisciplinary team to inform clinical decisions. Researchers for this study did not conduct assessments on children identified in the registry. Concurrent intervention services for children were not documented in the registry.
IGDI Web Application
Infant–toddler service providers who use the ECI enter child scores into a web application called the IGDI web application (Buzhardt et al., 2010) located at https://igdi.ku.edu. In addition to the ECI, the web application also accepts data from the other three IGDIs (Early Problem-Solving Indicator [EPSI], Early Movement Indicator [EMI], and Early Social Indicator [ESI]). As mentioned earlier, the primary purpose of the web application is to help service providers who often have limited experience in progress monitoring and data-driven decision-making to interpret individual children’s IGDI scores and progress over time. After initial staff training and certification, a secure account is created in the web application’s data system for the agency in which each staff member has unique login credentials. In addition to monitoring individual child progress to inform intervention decision-making, agency directors use the data system to generate group reports of all children or targeted subsets of children (e.g., only children with IFSP’s, individual classrooms, home visiting caseloads) to inform administrative decisions or report progress to funders and other stakeholders. Research groups that use IGDIs as outcome measures for clinical trials or other evaluation purposes also enter their scores into the data system. To date, the data system contains more than 98,000 assessments for more than 27,000 children in 30 states.
Matching procedures
Access to these databases is managed by the authors’ respective institutional review boards, and participants authorize use of data to report aggregated, de-identified outcomes for scientific purposes such as this article. After combining data from the two systems into a single spreadsheet, we used the Fuzzy Lookup add-in for Excel to identify matches between the diagnostic registry and the IGDI data system. The Fuzzy Lookup procedure is used to find approximate, or “fuzzy,” matches among selected variables. An advantage of using this procedure is that it provides perfect matches as well as a range of possible matches and a percentage based on the number of properties the variables share across registries. For the purposes of this study, we expected there may be slight deviations in name spelling across registries (e.g., Clare Doe born on 10/8/15 in one registry vs. Claire Doe born on 10/08/2015 in another registry), thus we wanted to examine approximate matches. To match children, we used the child’s first name, last name, and date of birth (DOB) between the two registries. We initially set the match threshold to 70% and then analyzed each match by hand for accuracy. A 70% match threshold means that across the three matching variables (i.e., first name, last name, DOB) approximately 70% of the variable properties matched between the two registries. This allowed us to exclude all highly unlikely matches. When analyzing by hand, we ensured the DOB matched and allowed for small deviations in last name or first name spelling. All matches had an accuracy of 91.85% and above for names and exact matches for DOB. Because the diagnostic registry primarily includes children and families from the state in which the diagnostic center resides and a neighboring state, we only examined ECI data from agencies in these states.
Measures
ECI
Administration
The ECI is a semi-structured, play-based, observational assessment of children’s expressive communication. During the 6-min assessment, an adult play partner engages with the target child around one of two commercially available toy sets (Fischer-Price® Barn or House). A 16-item administration checklist guides the play partner’s setup and ending of the session, as well as general guidelines for supporting and sustaining the child’s play and engagement with the play partner during the session. For example, the checklist directs the play partner to comment about what the child is doing, follow the child’s lead rather than directing play, and to respond to all verbal and nonverbal communication during the 6 min. Because the ECI is designed to be administered by practitioners more frequently than most standardized assessments (e.g., quarterly for children performing at/above benchmark, and more frequently for children at least 1 SD below benchmark), it is recommended to alternate between toy sets for consecutive assessments to help maintain the play sessions’ novelty for the child.
Scoring
The ECI is scored by a certified ECI assessor, either live or from a video recording of the session. Typically, particularly in home-visiting contexts, assessors score from video, allowing them to serve as the play partner during ECI administration and then score later. All ECI assessments for this sample were administered and scored by assessors trained and certified as described in the subsequent Training/Certification section. Using an ECI observation sheet or the IGDI Mobile app, the assessor counts the child’s use of gestures, vocalizations, single words, and multiple words.
As described by Greenwood and colleagues (2010), gestures are nonverbal physical movements by the child to communicate, which includes waving, shrugging shoulders, nodding head, and pointing, as well as giving and taking toys from the play partner. Only the total number of gestures is coded; there is no coding of the types or variety of gestures used by the child. Vocalizations are any verbal utterances by the child that are not understood as words by the coder. These include sounds such as babbling, cooing, and attempts to make animal or machine sounds (e.g., cars, tractors, kitchen sounds). These nonword vocalizations do not include involuntary sounds such as hiccups, burps, and sneezes. Single words are scored when the child says a word that can be understood by the coder and there is at least a 2-s pause between other words. No distinction is made between echoed/imitated words and spontaneous words. Multiple words are two or more words together understood by the assessor with less than a 2-s pause between them. They do not have to be grammatically correct or have a clear meaning. ECI key skills do not have to be directed to the play partner to be scored.
Entering ECI scores into the IGDI web application generates a Weighted Total ECI, and key skill scores for each child are expressed as a rate per minute, each plotted as line graphs against benchmark performance (see Figure 1). The Weighted Total ECI score is calculated by assigning a 1 to each gesture and vocalization, a 2 for each single word, and a 3 for each multiple word, and summing these values. This creates a growth-based total communication metric that factors in the reduction of gestures and vocalizations that occurs as children’s vocalizations are replaced by more advanced spoken communication.
Psychometric properties
ECI benchmarks were established based on scores from the 5,883 children (aged 6–42 months) described in the subsection “Participants.” The growth pattern in weighted total communication for all children increased monthly with a mean slope of 0.98 (SE = 0.022) responses per minute per month. Indicating sensitivity to children with disabilities, there were differences in the growth of children with versus without an IFSP (i.e., receiving disability services). Children with an IFSP grew at a rate of 0.79 communications per month versus 1.01 for children without an IFSP.
The reliability of the ECI has been demonstrated in applied settings by practitioners using it as part of their standard services and by researchers under controlled conditions. EHS service providers administering the ECI quarterly with their infants/toddlers in two states conducted annual reliability observations. For the 390 paired observations, Pearson’s r ranged from .91 to .97 between primary and reliability observations for total weighted communication and all key skills (Greenwood et al., 2013). Furthermore, Greenwood and colleagues (2006) assessed reliability of the ECI for three independent samples in which a reliability observer scored random samples of videotaped ECIs. Interrater agreement between reliability and primary observers was .90 in a sample of 90 observations, .88 (n = 31), and .85 (n = 20). Finally, Pearson’s r correlations of .62 with the Preschool Language Scale –3 and 0.51 with the Caregiver Communication Measure provide evidence of the ECI’s criterion validity against other validated measures of early language (Greenwood et al., 2006).
ECI training/certification
To receive an account to use the IGDI web application, assessors must be trained and certified by a certified IGDI trainer. Certification involves a three quarter day onsite training that includes a didactic lecture over the purpose, administration guidelines, and scoring definitions of the ECI (Walker & Buzhardt, 2010). Following lecture, trainees practice scoring samples of videotaped assessments as a group with the trainer. Finally, each trainee scores two full video ECI sessions focused on children’s communication skills and fidelity of administration. Each trainee must achieve at least 85% agreement with master scorings across all key skill elements on each video. Their attempts are checked by the trainer who provides individualized feedback until the mastery criterion is achieved.
Autism severity
Autism severity for this sample was based on scores on the Childhood Autism Rating Scale (CARS). Either the High Functioning (HF) or Standard (ST) form of the CARS-2 was used depending on the child (Schopler et al., 2010). The CARS-2 (Schopler et al., 1980) is a behavioral rating scale designed to identify ASD symptoms and their severity. It covers 14 domains related to severe ASD problems and ratings of overall severity. Summing the total points for each item provides a total CARS-2 score. Raw total scores ranging from 15 to 29.5 are non-autistic, 30 to 36.5 is mild to moderate autism, and 37 to 60 is moderate to severe autism. The internal consistency reliability alpha coefficient is .94, the interrater reliability correlation coefficient is .71, and the test–retest correlation coefficient is .88.
Cognitive measures
Measures of cognitive functioning were selected by the diagnostic center’s multidisciplinary team as appropriate for the child’s age and referral question. For children up to 3 years of age, the Bayley Scales of Infant and Toddler Development–third edition (BSID-III) is a standardized developmental assessment, with strong psychometric properties, for children up to 42 months of age (Bayley, 2005). The BSID-III yields a Cognitive Composite Score that was used for analyses. For children aged 3 years and older, the Kaufman Assessment Battery for Children–second edition (KABC-II; Kaufman & Kaufman, 2004a) was administered, and for children aged 4 years and older the Kaufman Brief Intelligence Test–second edition (KBIT-2; Kaufman & Kaufman, 2004b) was administered. Both the KABC-II and KBIT-2 are widely used standardized cognitive assessment measures with strong psychometric properties (Kaufman & Kaufman, 2004a, 2004b). The KABC-II Fluid Crystallized Intelligence Index and the KBIT-2 IQ Composite Standard Score were used for analyses. Of this study’s sample, 10 children received the BSID-III, one child received the KABC-II, and one child received the KBIT-2. Children who were administered a cognitive assessment and were below the age of 40 months received the BSID-III, whereas children 48 months and older received either the KABC-II or KBIT-2. Across each of these measures, cognitive scores were standardized with a mean of 100 and a standard deviation of 15 for use in analyses. Therefore, general cognitive ability across measures was comparable given the similar metric used for each standard score.
Analytic Methods
To address the first research question on examining differences in ECI slope and intercept between the benchmark and ASD samples, we began with the estimation of the trajectories of the communication outcomes (i.e., ECI weighted total and four key skills) based on only the ASD sample, using Multilevel Growth Modeling (Peugh, 2010; Raudenbush & Bryk, 2002). For each outcome, we determined the shape of its trajectory by comparing between linear and quadratic models using a chi-square test. Multilevel Growth Modeling allows us to appropriately deal with the clustered data in this study, that is, observations clustered within children. There were two levels in each growth model, observation-level and child-level. The observation-level estimated means of growth parameters, such as intercept, linear slope, and quadratic slope; and the child-level captured the variation of the growth parameters between children. Child age was treated as a continuous observation-level predictor, so that the trajectories of the communication outcomes can be estimated even with the unequal spacing of age (Raudenbush & Bryk, 2002). We centered children’s age at 42 months because this is the oldest age in which the ECI can be administered and the age at which children are most likely to use all four key skill elements, as evidenced by prior studies of the ECI’s psychometric properties (Greenwood et al., 2006, 2010, 2019), in clinical trials (redacted to maintain blind review), and investigations with non-U.S. population (redacted to maintain blind review). This allowed the estimated mean intercept of the growth trajectory to be interpreted as the mean of the outcome scores at 42 months of age.
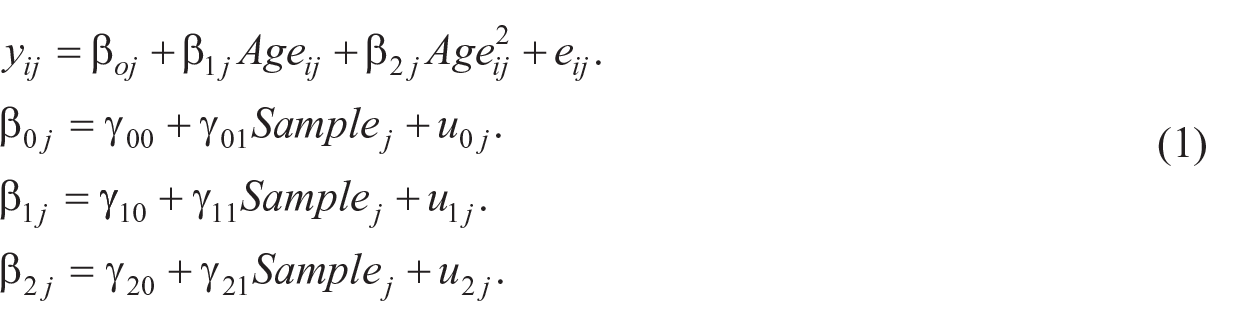
Next, to examine the differences in trajectories between the benchmark and ASD samples, we combined the two samples, and added a binary (0 = benchmark, 1 = ASD) child-level predictor to the growth models. Equation 1 shows such a model given the outcome followed a quadratic trajectory. The key parameters of interest in this model were those associated with this child-level predictor, that is, γ01, γ11, and γ21, which were referred to as cross-level interaction effects. These parameters represent the differences in intercepts, linear slopes, and quadratic slopes between children in the benchmark and ASD samples, respectively. This model was used fit to the two-sample combined data for each communication outcomes. The parameter β2j would equal zero for a linear outcome. This analysis was conducted through the software package R.
To address RQ2, we fit the growth models to the ASD data to examine the effects of child level predictors: gender, cognitive functioning based on a composite standard score of measures (BSID, KABC, and/or KBIT), and ASD severity based on the CARS. The variable Time Difference (months since first observation) was included as covariates to adjust for potential confounding effects. Full Information Maximum Likelihood (FIML) was used to address missing data in the predictors. This analysis was conducted with Mplus (version 7, Muthén & Muthén, 2019).
Results
Differences in Slope and Intercept Centered at 42 Months
Table 4 provides the results of the Multilevel Growth Modeling for weighted total communication and the four key skill elements, and Figures 2 and 3 provide estimated growth trajectories for both groups. Significant differences were found between the two samples on the intercept centered at 42 months for the ECI weighted total score and all key skills. Differences between groups on linear slope were found for vocalizations, single words, and multiple words. No between-group differences were found for quadratic slope. Thus, our hypothesis that children with ASD will have lower ECI slopes and intercepts was accepted, except in the case of gestures.
ASD Sample Versus Benchmark Sample.
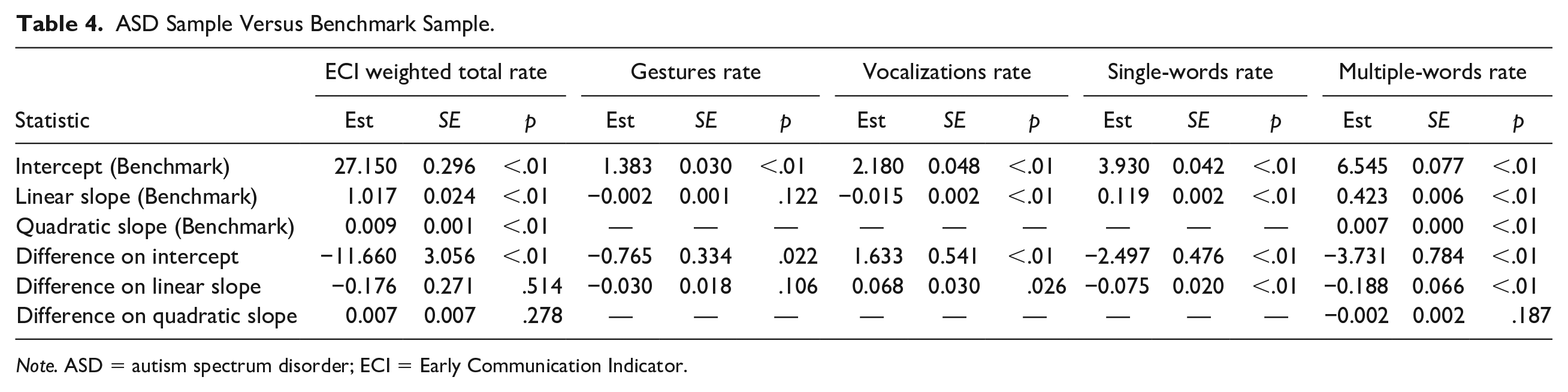
Note. ASD = autism spectrum disorder; ECI = Early Communication Indicator.
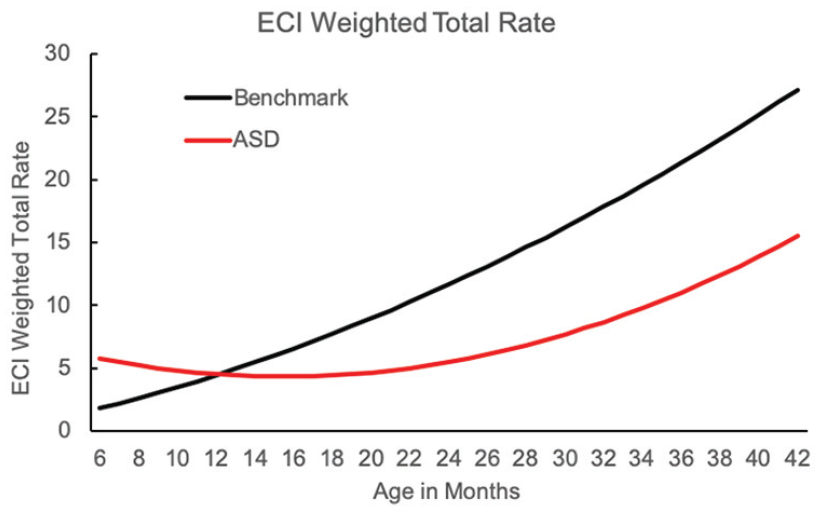
Growth trajectories of children with ASD compared with ECI benchmark sample on the ECI weighted total score.
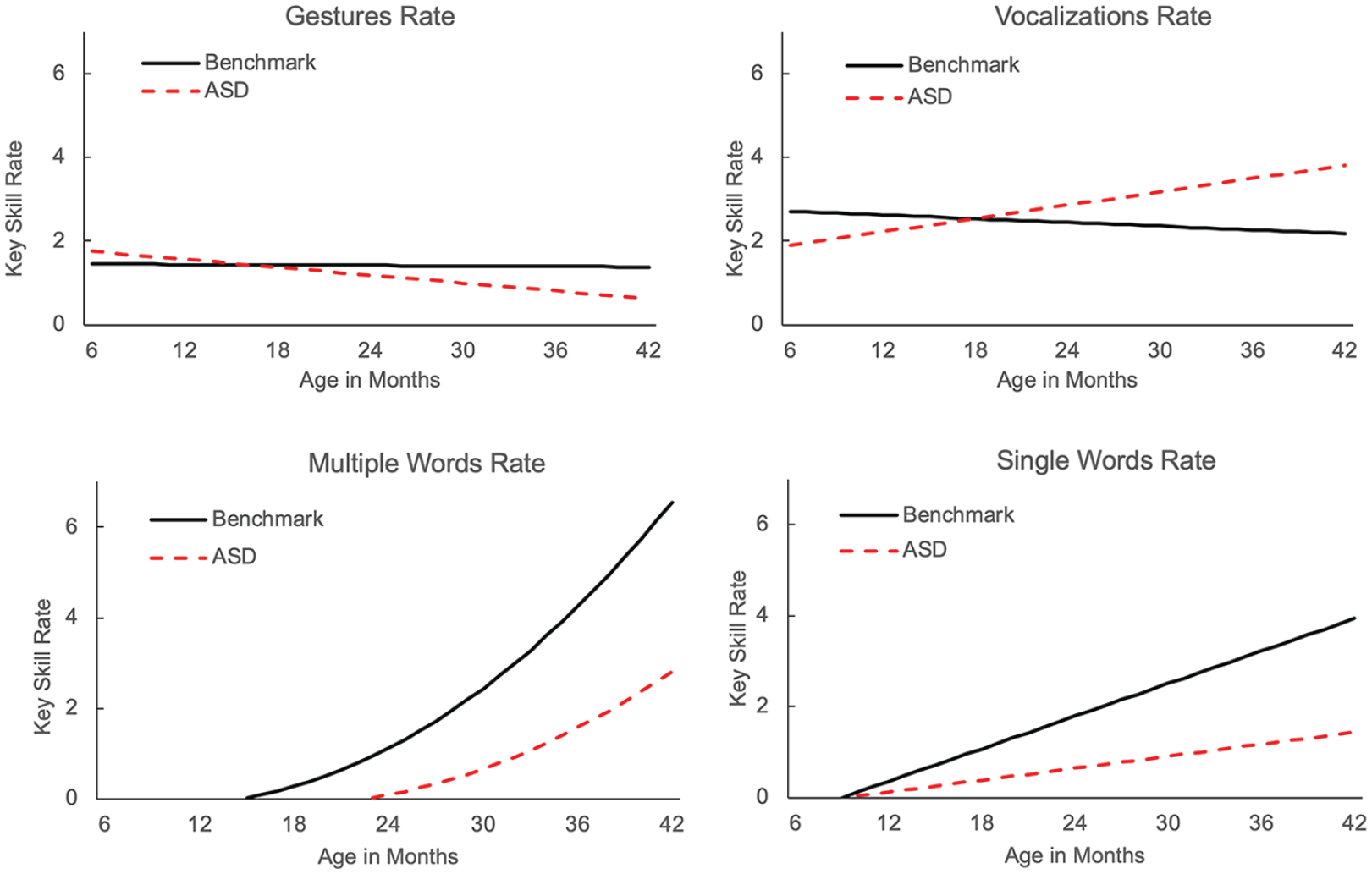
Growth trajectories of children with ASD compared with ECI benchmark sample on each ECI key skill element.
Children with ASD had significantly lower ECI total weighted scores than the benchmark sample (–11.66, SE = 3.06, p < .01) at 42 months of age, but there was no significant difference in the linear or quadratic slopes between the two samples. For gestures, the benchmark group had a significantly higher intercept at 42 months of age than the ASD sample, but no significant difference in slope. The ASD sample demonstrated significantly higher rates of nonword vocalizations than the benchmark sample at 42 months of age (1.63, SE = 0.54, p < .01), as well as a faster growth rate (0.07, SE = 0.03, p = .03). Conversely, for single words, the ASD sample used fewer single words at 42 months of age (–2.50, SE = 0.48, p < .01), and they had a lower linear growth rate than the benchmark sample. For multiple words, a similar pattern was observed whereby children with ASD demonstrated fewer multiple words at 42 months of age (–3.73,SE = 0.78, p < .01) and had a slower rate of linear growth (–0.19, SE = 0.06, p < .01).
Child Characteristics Associated With ECI Growth Trajectories
Our hypothesis that ECI growth would be related to autism severity was accepted, but we rejected the hypothesis that gender and cognitive ability would be related to ECI growth. Table 5 provides the findings of the effect of child-level characteristics on the ECI performance of children with ASD. Characteristics examined were gender, cognitive functioning, and autism severity as measured by the CARS. Autism severity demonstrated a significant effect on ECI performance. As autism severity increased, children’s use of gestures (–0.09, SE = 0.04, p = .04), vocalizations (–0.15, SE = 0.06, p = .02), and the weighted total ECI score (–0.39, SE = 0.21, p = .05) decreased. Gender and level of cognitive functioning were not related to ECI performance. This suggests that the ECI measures the communication skills of children with ASD largely independent of gender and level of cognitive functioning. Importantly, however, the ECI was sensitive to autism severity.
Effects of the Three Between-Level Predictors.
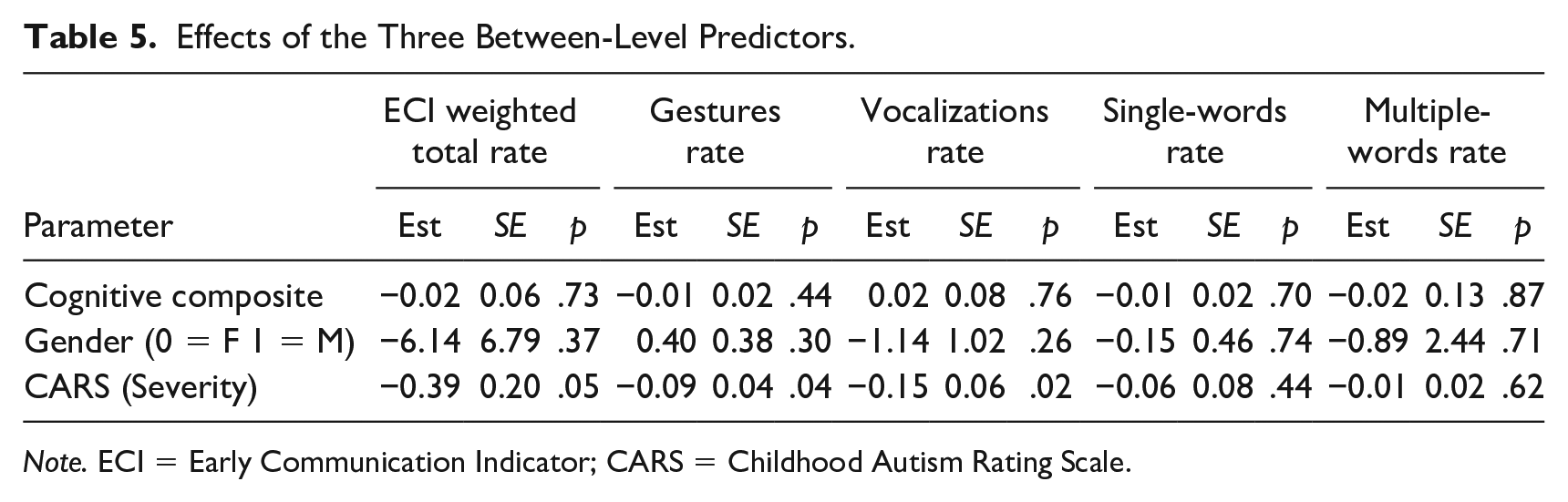
Note. ECI = Early Communication Indicator; CARS = Childhood Autism Rating Scale.
Discussion
There is a need for more psychometrically sound tools that identify ASD before preschool and improve the stability and confidence in early diagnoses (Ozonoff et al., 2018). Although further prospective studies are needed, these exploratory findings suggest that the ECI has promise for use in characterizing the communication profiles and trajectories of young children with ASD. We found that the magnitude of both prelinguistic (i.e., vocalizations, gestures) and linguistic (i.e., single and multiple words) communication skills differed between children with ASD when compared with a benchmark sample. In addition, we found that the key skill growth rates, with the exception of gestures, also differed from benchmark trajectories. Importantly, these differences often emerged prior to when the child likely would have received a formal ASD diagnosis. For example, for the single-word key skill, differences appear to emerge as early as 14 months of age. This suggests that the ECI may be sensitive to pre-diagnostic communication differences that emerge early in development for infants who eventually receive an ASD diagnosis.
When examining each key skill in more detail, we found trends that align with current research and knowledge about the communication development of children with ASD (Anderson et al., 2007; Mitchell et al., 2006). Specifically, for prelinguistic skills, although children in both groups began using gestures at similar rates, the decline in gestures over time for the ASD group resulted in significantly lower rate of gestures for this group at 42 months of age than the benchmark group. This finding is in line with research demonstrating that children with ASD, in general, use fewer gestures (Colgan et al., 2006; Watson et al., 2013; Wetherby et al., 2007) and struggle to integrate gestures with speech (Bryson et al., 2007; Stone et al., 1997). Specifically, these findings support prior research suggesting that deficits in gesture use by children with ASD are not present during infancy but begin to emerge during toddler years. For example, Colgan and colleagues (2006) found no differences in the total number of gestures used by infants with ASD from 9 to 12 months of age despite a well-established deficit in gesture use by children with ASD by 2 to 3 years of age (LeBarton & Iverson, 2016; Manwaring et al., 2018; Mitchell et al., 2006; Stone et al., 1997). Vocalizations, on the other hand, showed the opposite trend: Children with ASD demonstrated continued increases in nonword vocalizations over time, whereas the benchmark sample decreased their use of vocalizations as their use of words replaced vocalizations.
Prior research has found that both children at-risk for and with ASD show vocalization patterns characterized by more nonspeech-like and fewer directed vocalizations (Garrido et al., 2017; Patten et al., 2014), and younger siblings of children with ASD (i.e., those at increased genetic risk for ASD) appear to show a “hyper-vocalization” pattern as early as 9 months of age, with these infants producing more vocalizations than age-matched children without an older sibling with ASD (Swanson et al., 2018). Importantly, this hyper-vocalization pattern was associated with worse outcomes, including less social babbling and fewer conversational turns with adults. For this study, we lack qualitative information on whether the vocalizations of these children were directed (or not) to caregivers in their immediate environment; however, based on typical language development, the rate of nonword vocalizations should decline over time as children learn to articulate words (Greenwood et al., 2010). We do not see the expected decline in vocalizations occur in this sample of children with ASD.
Analyses of the linguistic skills (i.e., word use) of children with ASD revealed fewer single-word and multi-word combinations. There also appeared to be a delayed onset in these children’s transition from using single-word utterances to multiple-word phrases. This is relevant because longitudinal studies of ASD have found that the development of expressive language by 5 years of age is one of the most robust predictors of social, academic, and mental health outcomes into adulthood (Anderson et al., 2009; Beitchman et al., 2001; Rutter et al., 1967).
Although these findings align with prior research related to the language development of children with ASD (Trembath et al., 2019), it is important to note that correlations were only observed between gestures and total communication score and children’s severity of autism symptoms. No significant correlations were found for the other key skills or between the ECI and children’s cognitive ability or gender. This is essential for measurement purposes because it suggests that the ECI measures communication of children with ASD independent of their cognitive ability and gender. This could mean that the ECI is appropriate for the spectrum of children with ASD in this age range who demonstrate varying levels of intellectual ability. Although this study was not designed to detect gender differences in the communication patterns of young children with ASD, the finding that gender was not associated with ECI growth was consistent with prior studies reporting no gender differences in the language development of children with ASD (Van Wijngaarden-Cremers et al., 2014; Halladay et al., 2015).
Limitations
Small sample size, use of retrospective data, and lack of reliability estimates are key limitations of this exploratory study. We used matching criteria between two existing data sets to identify children who had received ECIs as an infant/toddler and later went on to be diagnosed with ASD. This analysis of retrospective data sets was needed as a first step in determining whether or not a larger, more robust longitudinal study is warranted. Conducting a longitudinal study with a prospective sample of infants/toddlers with, or at high risk for, ASD would allow us to determine the temporal stability or instability of these growth patterns for young children with ASD, as well as the ECI’s diagnostic predictive validity. Although training requirements are rigorous for the ECI and reliability estimates are strong for ECIs administered by community early childhood programs (i.e., not in research contexts; Greenwood et al., 2013), we do not have reliability estimates specific to this sample of ECI data from community programs. Future prospective studies are needed to estimate the ECI’s reliability and administration fidelity when used with young children with ASD.
The small sample size prevented us from conducting psychometric analyses to validate the ECI’s use with children with ASD. However, the data from this study are consistent with other findings in the field, such as delayed use of verbal communication and hyper-vocalizations, suggesting that the ECI is a promising instrument for measuring the communication profile of children with ASD. The sample size also was too small to examine subgroups of children with ASD that have been associated with different communication trajectories. For example, Ozonoff and colleagues (2011) found different social-communication trajectories for children with an early onset of ASD symptoms (i.e., those who showed symptoms in the first year of life) versus children who displayed some form of developmental regression (i.e., no obvious early delays prior to a loss of skills). Similarly, Landa et al. (2007) found that children with ASD diagnosed earlier in development had lower communication skills over time, between the ages of 14 to 24 months, when compared with children who were diagnosed at later ages. This further reinforces the need for tools that improve our ability to diagnose children and begin intervention at the earliest possible age.
Finally, our analysis of the influence of child-level predictors on ECI scores was limited to the demographic and assessment data available through the IGDI data system and ASD diagnostic registry. Specifically, we relied on the diagnostic team’s cognitive assessment decisions, which resulted in using cognitive scores across three measures (i.e., BSID-III, KABC-II, KBIT-2). Because nearly half of the sample did not receive a cognitive assessment, and those that did were assessed with one of three different measures, our finding of no relationship between the ECI and cognitive ability should be considered in light of these limitations. A prospective sample of children would allow us to assess other potential predictors of interest (e.g., language development on other assessments such as the Preschool Language Scale, presence of other disabilities, social-emotional development, and family characteristics) and use consistent measures for all children. Finally, a larger sample size would provide more power, allowing us to identify other weaker, yet significant, predictors.
Implications for Interventionists and Practitioners
These exploratory findings suggest that children with ASD may present a unique profile on the ECI that differentiates them from children without a language delay, but more research with a larger, prospective sample is needed to confirm this finding. This would be useful to early childhood practitioners and service providers in designing intervention plans for children on their caseload. For example, a child with delayed language growth who presents high rates of vocalizations or “hyper-vocalizations” after 20 months of age may benefit more from an intervention that addresses both ASD symptoms and language delay, and/or administering additional assessments to consider a potential ASD diagnosis. Also, because the ECI is designed to be administered more frequently than most standardized assessments, “rate of growth” on each key skill becomes a key outcome to inform intervention programming, rather than simply age of onset or performance at a specific age. More research is needed to determine whether or not the ECI growth patterns of children with ASD differ from children with a language delay who do not have ASD.
Although a strength of the ECI is the ability to monitor children’s progress over time, particularly those whose growth is below benchmark, and to inform data-driven decision-making for children receiving early intervention (Buzhardt et al., 2018; 2020; Walker et al., 2008), to date there is limited guidance for decision-making related to a specific delay or disability. While most interventionists working with children with ASD (e.g., Board Certified Behavior Analysts) will monitor children’s progress using outcome measures that are individualized to specific skills under specific conditions (e.g., responds to name, points to preferred items), the ECI can be administered frequently to monitor progress on a general outcome with standardized administration protocols. Given validation with a larger, more diverse sample of children, ECI benchmark growth trajectories for children with ASD will provide data on the impact of intervention on language as a general outcome.
Given the unique ECI growth patterns presented by children with ASD as well as alignment with theory and research, the ECI shows promise as a tool to help identify infants/toddlers with ASD and monitor progress following intervention. Additional research is needed to (a) replicate these findings with a larger, prospective sample to improve the generalizability of these findings, (b) investigate the feasibility of adding key skills to the ECI that are typically targeted by autism interventionists (e.g., joint attention), and (c) explore the impact of moderating variables on individual key skills.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, Office of Special Education Programs, or the Institute of Education Sciences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by federal Grants through the Institute of Education Sciences (R324A120365), Office of Special Education Programs (H327S140024), the Kansas Intellectual and Developmental Disabilities Research Center at the Life Span Institute of the University of Kansas (NIH Number HD002528), and by the Eunice Kennedy Shriver National Institute Of Child Health & Human Development of the National Institutes of Health under award number R01HD100364.