
Abstract
This study explored how early childhood intervention (ECI) professionals could support the development of secure attachment in children with developmental delay or disability (DD) within the context of ECI in Australia. Secure parent–child attachment is conducive to the aims of ECI to enhance the development, well-being, and participation of children with DD. Constructivist grounded theory methodology was applied to collect and analyze data from in-depth, semi-structured interviews with three parents and 18 professionals. Seven conceptual categories were selected: (a) Importance; (b) Challenges; (c) The System; (d) The Key Worker; (e) Assessment; (f) Strategies; and (g) Outcomes. Two dominant themes were identified: the quality of the relationship between the ECI professional and the family and self-regulation. An attachment-focused ECI framework is proposed, aligned with the ecological system model.
Background
Development of secure attachment between a child and their parent, within which a child has confidence that their parent will be available, protective, and comforting, is positively associated with communication (Belsky & Fearon, 2002), pro-social behavior (Mikulincer et al., 2005), self-regulation (Pallini et al., 2018), social skills (Groh et al., 2014), and resilience (Tharner et al., 2012). Insecure attachment is associated with intrusive, low-level, or inconsistent parental responsiveness, while insecure-disorganized attachment is associated with frightening or frightened parenting behavior (Fearon & Belsky, 2016). Insecure, and more so, disorganized attachment is associated with an increased likelihood of behavioral problems (Fearon et al., 2010), obesity (Maras et al., 2016), and diminished mental and physical health (Rapoza et al., 2016). A recent meta-analysis found that 42% of children with a developmental delay or disability (DD; n = 215) had a secure attachment compared with 62% in population samples (Alexander et al., 2021). Furthermore, 29% of children with DD were found to have disorganized attachment compared with 15% of children without DD (Alexander et al., 2021).
Early childhood intervention (ECI) professionals in Australia work with the families of infants and children under 7 years of age with DD to optimize their development, well-being, and participation (Early Childhood Intervention Australia, 2016). The Australian national guidelines for best practice in ECI (Early Childhood Intervention Australia, 2016) recommend a Key Worker or Primary Service Provider approach, with one ECI professional working holistically in the child’s natural environment, supporting parents in optimizing everyday activities and interactions. Each Key Worker is a qualified early childhood specialist educator, occupational therapist, physiotherapist, psychologist, social worker, or speech pathologist. Working closely with families in the critical early years when parent–child relationships are being established, ECI professionals are well-positioned to improve the attachment security of infants and children with DD. There is emerging evidence that many ECI professionals have not learned about attachment in their academic training and thus may not know how to effectively support secure parent–child attachment in their work with families (Alexander et al., 2018).
ECI professionals have used mainstream attachment intervention programs. Examples include Make the Connection (O’Neill et al., 2018), on which there is no published research including children with DD; Parent–Child Mother Goose (Koohi et al., 2016), which has one publication including children with hearing impairment; and Circle of Security (Powell et al., 2014), which has two publications including children with DD (Fardoulys & Coyne, 2016; Muddle et al., 2021). There does not appear to be literature regarding how ECI professionals can improve the attachment security of children with DD within the context of best practice ECI. This dearth of literature was an invitation for a constructivist grounded theory (CGT) to explore the possibilities (Charmaz, 2014).
Method
Aim
The current study aimed to investigate how attachment security could be improved within the context of ECI in Australia; however, the results have relevance for ECI practitioners, managers, researchers, and academic educators internationally. The research question was:
Research Question 1 (RQ1): How can ECI professionals improve the attachment security of children with a disability or developmental delay?
Method
CGT methods were utilized for this study as they are appropriate when little is known of the research area, the study is explorative; and the researcher does not assume one truth (Birks & Mills, 2015; Charmaz, 2014). As for other forms of grounded theory, the aim of CGT is to develop a theory that is “grounded in real world data” (Newby, 2014, p. 491). CGT stands out from classical grounded theory (Glaser & Strauss, 1967) in that the theory arising from the research process is viewed as a co-construction of the researcher and the participants (Charmaz, 2014).
The approach in the present research respected the existing knowledge, skills, and practices of ECI professionals and involved them in the process to achieve results that were meaningful and translatable to their practice because the data are grounded in their experience (Newby, 2014). CGT influenced decisions regarding how and from whom data were gathered and how data were analyzed, with these activities occurring concurrently (Charmaz, 2014) (see Figure 1). This ongoing analysis led to theoretical sampling; the emerging themes informed decision-making regarding ongoing participant recruitment (Birks & Mills, 2015; Charmaz, 2014). Focused-coding was undertaken to develop categories representing the major themes (Charmaz, 2014). Diagramming was then employed to facilitate the process of developing the proposed framework (Charmaz, 2014). Throughout every phase of this iterative process, memoing was employed, that is, written reflections regarding emerging ideas, insights, and feelings regarding the research and analysis, enhancing the ability of the researcher to identify theoretically relevant data, known as theoretical sensitivity (Birks & Mills, 2015). Memoing also facilitated theoretical analysis, informed theoretical sampling, and provided an audit trail of the process (Birks & Mills, 2015). Theoretical saturation was reached when no new codes emerged from the data (Birks & Mills, 2015).
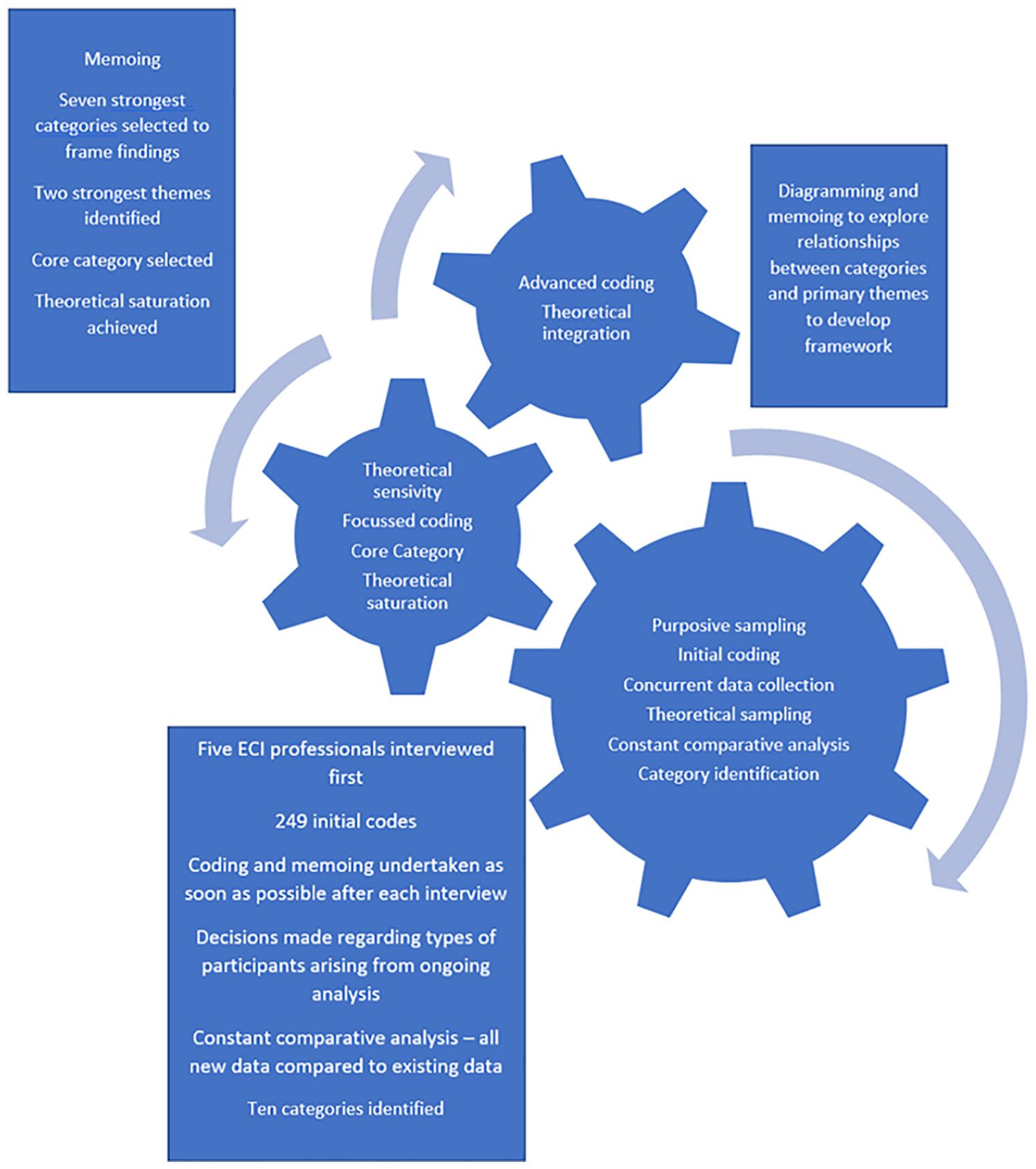
CGT Methods Used in Study.
Initially, the founders of grounded theory, Glaser and Strauss (1967), urged undertaking a literature review be deferred until after a theory was developed to minimize the risk of the emerging theory not being grounded in the data. Other grounded theorists, and Strauss himself, later acknowledged that this delay could be impracticable and that there were benefits to conducting a purposive preliminary review, like ensuring the research was required and theoretically sensitizing the researcher (Birks & Mills, 2015; Charmaz, 2014). As advised by Birks and Mills (2015), the preliminary literature review for the present study was contained to the minimum necessary, and a formal review was conducted following the development of a theory or, in this case, a framework. In keeping with the chronology of the study, new literature is introduced after the findings with the proposed framework and in the discussion (Dunne & Üstűndağ, 2020).
Participant Recruitment
Ethics approval was obtained from La trobe University Human Research Ethics (HEC1805).
In line with a CGT approach, the types of participants recruited evolved through the process of ongoing analysis of the data (Charmaz, 2014). The initial purposive sample (Sample type A, Table 1) consisted of five ECI professionals recruited voluntarily from one ECI provider organization offering a Key Worker approach. The provider organization had previously trained ECI professionals to enhance their knowledge of attachment and was selected for participant recruitment to enhance the likelihood of capturing effective practices.
Participant Details.
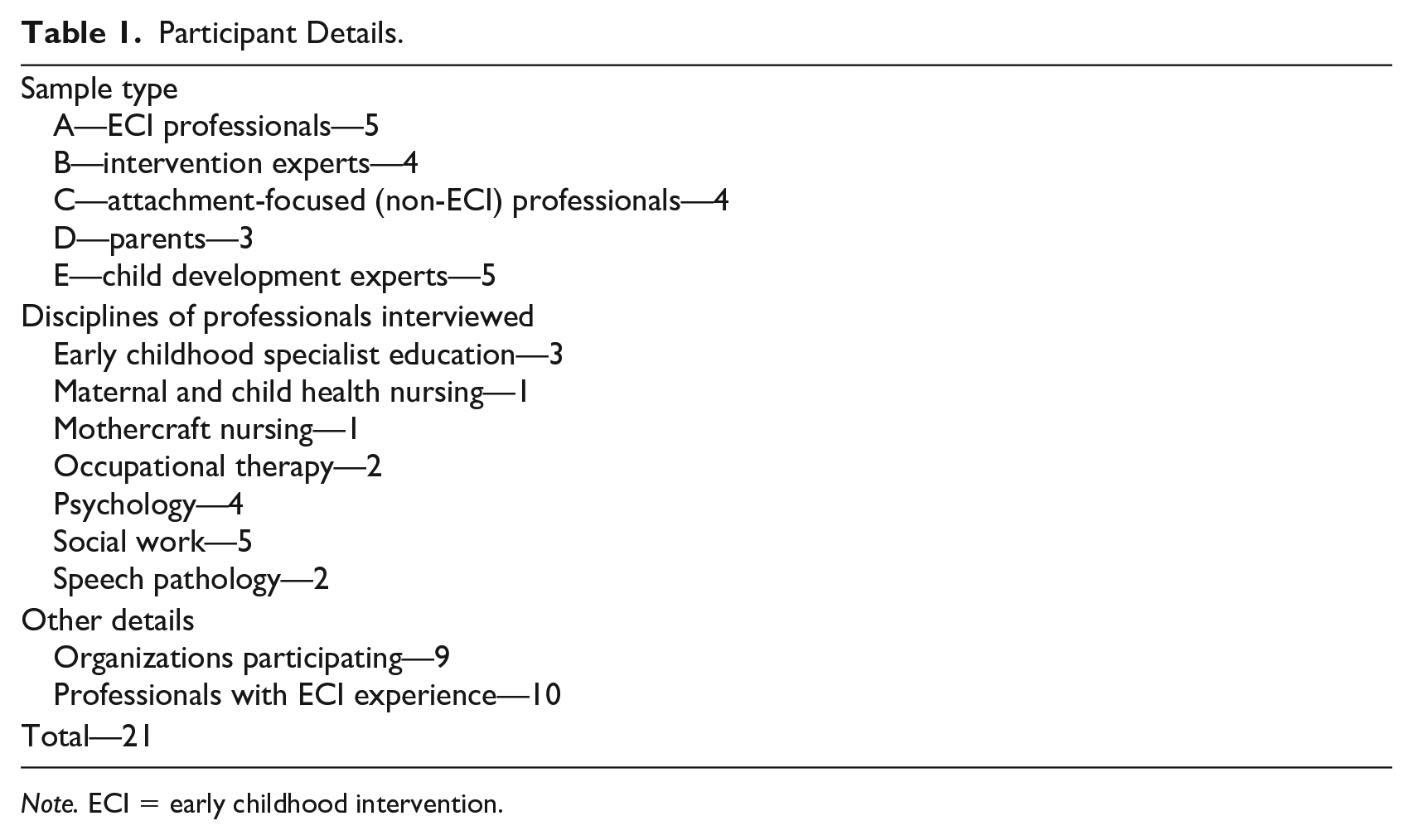
Note. ECI = early childhood intervention.
Next, four professionals with expertise in interventions or tools which target parent–child relationships (Sample type B, Table 1) were approached directly to participate in interviews with the consent of their organizations. The interventions or tools participants utilized included Parenting Interactions with Children—Checklist of Observations (PICCOLO) (Innocenti et al., 2013), Make the Connection (O’Neill et al., 2018), Parent–Child Mother–Goose (Scharfe, 2011), and Tuning in to Kids (Havighurst et al., 2009). PICCOLO is a tool designed to measure parent–child interactions in the domains of affection, responsiveness, encouragement, and teaching (Innocenti et al., 2013). Make the Connection is an attachment-focused parenting program that can be used in group or individual work with children and parents (O’Neill et al., 2018). Parent–Child Mother–Goose is a group program for parents and children using songs, rhymes, and stories to enhance child language and social skills and the parent–child bond (Scharfe, 2011). Tuning in to Kids is a group parenting program focusing on the emotional connection between children and their parents (Havighurst et al., 2009). The first three of these interventions or tools, while not designed especially for children with DD, nor all purported to address attachment, were selected as they were known by the authors to be used to varying degrees in ECI in Australia to positively influence the parent–child relationship and, fortuitously, experts in these tools and methods were in Victoria, enabling face-to-face interviews. The Tuning in to Kids interview was pursued as self-regulation was raised by five of the first eight interviewees, and another raised the Tuning in to Kids intervention.
Four organizations providing a range of community-based child and family services with an attachment focus were approached to participate in the study. Four staff with various roles, disciplines, and experience volunteered from one of the organizations (Sample type C, Table 1). Two experts (Sample type E, Table 1) came from another two of these organizations, while the fourth organization did not participate.
It became evident to the researchers from the ongoing data analysis that a parent perspective may bring greater depth to the data. Following an amendment to the ethics approval, parent participants (Sample type D, Table 1) were recruited via two organizations that had contact with over 7,000 families. Advertisements seeking parent volunteers were placed on the organization’s website, providing the initial sample of ECI professionals, and in the newsletter of a sixth organization.
Finally, five professionals were approached directly to explore emerging themes as they were known to have expertise in various areas of child development (Sample type E, Table 1), including infants’ experience of family violence, Australian First Nation’s People’s view of parenting, autism spectrum disorder (ASD) and attachment, child welfare and attachment, and ECI and child development. All agreed to participate.
Participants
Participants from Sample A had more than 20 years of experience working with children and families, primarily in ECI. Some also had experience in other related roles—early childhood education and family work with older children with disabilities. Participants from Sample B had experience training others in the program or tool about which they were interviewed. All professionals interviewed were qualified allied health or early childhood education professionals.
Three parents (Sample C) of children with DD volunteered and were interviewed—two biological mothers and an adoptive father. The disabilities or delays of their children included cerebral palsy, Down syndrome, global developmental delay, and intellectual disability. Two of the four children had some ASD symptomology but not a diagnosis of ASD.
The 18 professionals interviewed came from various disciplines (see Table 1 for details). The five expert informants (Sample E) and one of the intervention/tool experts had PhDs related to the topic for which they were interviewed. The parents (Sample C) also came from professional backgrounds. Participants were Caucasian (19), Australian First Nation (1), South Asian (1), female (19), and male (2). For anonymity, the quotes from interviews will be cited as “parent” or “professional.”
Data Collection
Interviews were conducted with parents and professionals to explore how ECI professionals could improve the attachment security of children with DD. Charmaz (2014) asserted that in-depth, semi-structured interviews are highly suitable in CGT methods as they enable expansive exploration of a topic and permit the interviewer and the interviewee to contribute more freely than a structured interview would allow. The interviews for the present study were all conducted by the first author, a PhD candidate who is a registered psychologist, between July 2017 and June 2020. The interviewer was an employee at the organization from which the first purposive sample was drawn and knew nine of the interviewees professionally. The other 12 interviewees were unknown to the interviewer prior to the interview. Interviews were audio-recorded, ranging from 28 to 96 min, with an average of 61 min. Interview schedules were developed by the first author as a guide for the interviews of each sample type of participant and individually for each expert. The second and third authors reviewed the schedules to promote content validity. Questions varied according to how each conversation evolved (Charmaz, 2014) but, in general, covered professionals’ experiences of working with families on attachment, families’ experiences of building a bond with their child and of ECI services, and strategies to improve attachment security experienced by parents or professionals. The interviews with the purposive sample all began with an invitation to talk about a time when they had worked with a family having had concerns about attachment. The intervention experts were asked to explain the intervention in detail, exploring the elements within the intervention and discussing how the interviewee perceived the effectiveness of the intervention with program participants. Interviews with parents began by asking them to talk about their child and family, what it was like developing a relationship with their child with a disability or developmental delay, and what professionals may have done, which was helpful or unhelpful to the parent–child relationship. The interviews with attachment-focused (non-ECI) professionals were similar to the purposive sample exploring the strategies they used to support the development of secure attachment. Finally, interviews with experts involved more detailed discussion on aspects of attachment that arose from the first 16 interviews and required more in-depth investigation of theoretical and empirical underpinnings. The first 13 interviews were conducted face-to-face, but then, due to the COVID-19 pandemic, the final eight interviews were conducted via Zoom (6) and via telephone (2). Despite designing the study to enable face-to-face interviewing, the researchers found, as did Sturges and Hanrahan (2004), that the modality of the interview did not negatively impact the quality of the data collected.
Data Analysis
Following CGT methods, theoretical analysis was conducted concurrently with data collection via coding and memoing (Charmaz, 2014). Transcripts were created following each interview, then coded, memoing undertaken and adjustments made to questions asked in subsequent interviews, together with decisions regarding further types of participants to recruit. The first five interviews were transcribed by a professional transcriber and checked by the first author. The first author transcribed the following 16 interviews with the assistance of Trint, a software program that transcribes audio into text. Transcriptions of the interviews were uploaded as they became available into NVivo 12, a software system used to assist with the management of qualitative data. The first author undertook initial coding with peer validation from the second and third authors.
The first author was the primary analyst for this study, with peer review conducted by the second and third authors at each stage of the process to enhance reliability. Reflexivity, facilitated by memoing and peer debriefing, were used to manage the influence of bias (Charmaz, 2014).
The first author leaned more toward coding as a “lumper,” coding larger tracts of data together rather than a “splitter” breaking down data into much smaller pieces (Saldana, 2016, p. 24). CGT maintains a focus on “actions and processes rather than themes and structures” (Charmaz, 2014, p. 15). Thus, initial coding was inductive and carried out using mainly Process Coding, otherwise known as action coding, which employs gerunds (“ing words”) because they focused on what people were doing (Saldana, 2016).
Once a transcript was coded, the first author hand-wrote memos detailing each code used in a transcript. As memoing is intended to be an “uninhibited activity” (Birks & Mills, 2015, p. 40) with “an emphasis on spontaneity and natural flow” (Birks & Mills, 2015, p. 43), handwriting was used. Memos facilitated constant comparative analysis (Birks & Mills, 2015), including discussion of the relationship between excerpts included under one code, example excerpts, relationships with other codes, and thoughts the author had regarding the data, the codes, and the process. The data coming from all 21 interviews were initially coded with 287 codes. The first author then reviewed every code, rereading all the excerpts in each code and ensuring appropriate placement. A codebook was then created by the first author listing every code with a definition, how many interviews it came from and how many excerpts were coded this way, example citations, and links to other codes. These further stages of analysis brought about some amalgamations of similar codes, reducing them to 249; for example, “Struggling to accept diagnosis” merged with “Not wanting child to have disability” as there was no clear distinction between excerpts under these codes. The second and third authors reviewed the codebook to enhance consistency.
Most codes were generated in the analysis of the first five interviews. Only two new codes were created by the 12th interview, and none from the 13th interview. The interviewer had anticipated a series of new codes to emerge from the parent interviews, but no new codes were developed. Rather, parents provided a first-person perspective of the issues raised by the professionals indicating data saturation. In CGT, theoretical saturation is sought, meaning that data gathering has reached a point where no new theoretical understandings are emerging to contribute to the developing theory or framework (Charmaz & Thornberg, 2021). The emerging themes were explored through individualized interviews with a range of experts. The interviewer again anticipated new codes would arise from the expert interviews, but instead, these interviews generated low numbers of existing codes as the discussion was more focused on themes raised in earlier interviews. The concepts in the proposed framework have been well explored in the interviews and can be supported by the data gathered.
The first author conducted focused coding. The process of constant comparison between the incident-by-incident codes from the initial coding phase facilitated the identification of ten conceptual categories. For example, a category named “The System” was generated from the grouping of conceptually linked codes, including “Helping parents understand what ECI is,” ‘Increasing skilled workforce,’ and “Waiting for help.” Further analysis of these 10 categories resulted in the selection of 7 primary categories, which have been used to structure the findings. The first author then undertook diagramming and memoing to analyze the relationships between the categories, identify the primary themes, select the core category, and create the proposed framework, which follows the “Findings” section. The proposed framework brings together the seven key conceptual categories and the two primary themes, which are further explored in the discussion.
Findings
The seven primary conceptual categories identified through focused coding were: (a) Importance; (b) Challenges; (c) The System; (d) The Key Worker; (e) Assessment; (f) Strategies; and (g) Outcomes. The research question was primarily answered in the category labeled “Strategies,” but the data also provided contextual information concerning how the ECI system and ECI professionals could deliver services conducive to positive outcomes and why this is important. The primary categories have been ordered to make the best narrative sense. Two codes gained primary thematic strength in the analysis. The first—“Key Worker connecting to family”—denoted excerpts regarding professionals forming relationships with families, and these gained dominance due to frequency, appearing 56 times across 15 interviews. The importance of the quality of the relationship between the professional and the family was evident in the stories told by both professionals and parents and was emphasized by several experts. “Key Worker” became the core category. The second—“Self-regulating”—denoted excerpts about a child’s ability to control their own emotions or behaviors and to self-manage their impulses and had strong interconnections with numerous other codes, which placed it in a somewhat central position. The theme of self-regulation was of such strength that it flowed through to several categories and the resulting framework. Due to the strength of the connection between attachment and self-regulation, this second primary code appears in the final framework as a sub-concept of attachment. The seven categories are used to structure the findings and are described and illustrated with quotes from the interviews as follows:
Importance
Evidence emerged from the interviews emphasizing the importance for children with DD to receive the kind of sensitive and responsive parenting that supports the development of secure attachment. Data indicated that (a) children with DD required considerable assistance, encouragement, and repetition to learn; (b) substantial assistance to build skills in self-regulation; and (c) had a sizable likelihood of experiencing abuse and neglect:
Learning
The following citation illustrates, for example, how parental patience, persistence, and sensitivity may be required to compensate for limitations in incidental learning: . . .the typical baby learns because they are absorbing, they are looking and absorbing everything from their social world, and they do what you do. If they’re not looking at you and engaging with you in that way, they’re not learning those things. (Professional)
Self-Regulation
Interviewees discussed children’s self-regulation skills as developing within a relationship through co-regulation as described by one parent who said, “. . .with that stressful tone in my voice and things like that, there were times where probably [my child] was looking to me to help her regulate herself, but I was unable to help her because I wasn’t regulated.”
Interviewees’ discussion of the effects of dysregulation encompassed babies with sleeping problems, toddlers having extended tantrums, and pre-schoolers running away, throwing objects, and physically assaulting their parents. Interviewees discussed the impact of these dysregulation effects in heightening parental stress, marital conflict, affecting the well-being of siblings, and impeding the capacity of both the child and the family to socialize.
Child Abuse and Neglect
A negative cycle was evident in the stories told by professionals, wherein family crises and distress escalated over time. Some of the families discussed by the professionals had some involvement with Child Protection Services. The complex links between attachment and abuse and neglect were discussed by several of the professional participants suggesting bi-directional effects, for example: . . . that dance of attachment, it’s a bilateral . . . it’s a mutually influential sort of impact, which I think if the parent isn’t getting as much back from the child and the child is flat, not engaging or frequently distressed, low frustration threshold, acting out, not smiling, just those basic sort of attachment-seeking behaviors. If they’re not there, the parent is not getting as much back, so they’re more irritable. They’re frustrated, and if there’s a growing sort of grief and loss or experience that “my child isn’t developing properly,” The parent can become depressed. The parent can feel “not as good as,” and depression, anxiety, we know, contributes to higher rates of abuse and neglect. (Professional)
Challenges
The data indicated that attachment security might be harder for children with DD to attain due to the emotional impact of parents realizing their child is developing atypically. This was evidenced through interviews with professionals and parents, referring to strong emotions such as guilt, grief, and devastation. The search for a diagnosis, the pressure felt by some parents to “fix” the child, and the stress inherent in gaining access to a multitude of services in pursuit of this aim was again evidenced by both professionals and parents. The child’s limitations in communication also arose from both parent and professional interviews as a clear factor in increasing frustration and impeding synchrony between the parent and the child: . . .if you think about how language works or about how conversations work, they always work within certain parameters, within certain timings. If somebody speaks too fast or too slow, then that makes the connection break down. . . (Professional) So, I don’t have any other children, so I don’t know what it should be like, but I guess with his speech delay, I have felt like there is a limit to how we connect. There’s just not really much back and forth, so there is only so deep you can go. (Parent)
Other interviewees indicated that difficulty in coming to terms with a diagnosis might impact a parent’s ability to emotionally connect and be attuned to the child’s needs and abilities, for example: . . .she was not being able to, or struggling to accept this diagnosis and that he did have an intellectual disability. She wasn’t really in tune with his skills or his abilities, and so she would often engage with him way above his ability. (Professional)
Having made a clear and free choice to adopt severely disabled children, the absence of emotional turmoil regarding the disability stood out with the adoptive parent. A mission to bond had been their clear and successful priority when each child came into their care. All three parents spoke of the emotional impact of professional insensitivity, for example: The pediatrician sent us to a physiotherapist who, at the end of the first session, when I was walking into the waiting room, said, “You should probably get him on NDIS [National Disability Insurance Scheme].” I left there crying. I mean, you want your child to be normal. I felt bad enough that I had to take him to a physiotherapist, and now she is telling me he has a disability as just an offhand remark while I am leaving. After the end of the second session, she said, “I think he has autism.” Once again, I left crying. I had to get my husband to come to the physio sessions with me because they upset me so much. (Parent)
The parent compared this negative experience to her experience with the next physiotherapist, who “is very positive,” making her feel better about herself as a parent and “feel better about my child. As a parent, you notice all the things your child can’t do, and having her notice what he can do makes me feel better about him.”
ASD was the most commonly discussed diagnosis, and interviewees suggested ASD may pose additional challenges to the attainment of attachment. Reasons provided by interviewees included that it can be harder for parents to synchronize with their child and tune into their interests. Also, it may be harder for parents to detect the more subtle or idiosyncratic signs that their child is attached to them, which can impact the parent’s feelings toward the child. In addition, sensory overload may distress the child and thus over-activate the child’s attachment system.
The System
Data emerged from the interviews about how aspects of the overarching system providing ECI funding and policy could be most conducive to improving attachment security for children with DD. First, interviewees indicated that the ECI system should enable early, easy access to high-quality services. The effectiveness of the intervention would thus be enhanced due to greater neural plasticity during early infancy. In addition, for families to access high-quality attachment-focused services, the overarching system providing ECI would need to foster the ongoing professional development of ECI professionals, as many of the professionals interviewed indicated that they did not learn about attachment in their undergraduate training. Some interviewees indicated that they had learned about attachment in subsequent professional development training, while others learned from their colleagues through transdisciplinary teaming and supervision, which also supported them emotionally to persevere in what was sometimes emotionally challenging work with families: Also, just being able to draw on the resources within the team, with my Team Leader and also with other team members. I did a lot of coming back and debriefing about what I was seeing and am I on the right track kind of thing. (Professional)
Finally, but importantly, data indicated that the system providing ECI should either only fund high-quality holistic ECI services or provide adequate support to families to understand best practices in ECI. The data indicated that parents were not being adequately supported to make informed choices about ECI approaches: I have heard about the Key Worker model, but I don’t really know much about it. The pediatrician told us we need physio, so we did that and then she sent us to the speechie, and she sent us to the OT, so we have gone full medical model without even necessarily choosing that. It seems like an important decision to make but I just don’t know. (Parent)
The Key Worker
The data analysis strongly indicated that the relationship between the parent and the ECI professional is critically important in effecting change. The importance of the professional-family relationship was discussed as not just a matter of role modeling positive interactions but, rather, as a deep, non-judgemental engagement with a professional who genuinely cared for the family and was sensitive to their individual and cultural needs because, for example: . . .it’s hard for someone to open up and talk about how they’re feeling as a parent and how they feel about their child if it’s not all glowing and how it should sound. So, to sit with that and be okay with that, I think is important (Professional)
A coaching approach, defined by Rush and Sheldon (2005) as a strategy to facilitate adult learning by supporting the ability of the learner to reflect, plan and develop the effectiveness of their actions, was supported by the data. In addition, examples provided by interviewees of interventions that did not have positive outcomes were contrary to a coaching approach. Effective coaching elements discussed by multiple interviewees included following the parent’s lead, partnering with parents so that they are co-designing strategies, modeling strategies, and asking parents questions to learn more about what they already know, do, and prefer. One professional described the effect of applying a coaching approach with a mother, saying: . . . I think if I hadn’t helped her develop that ability to reflect, she may never have gotten to that point of even looking inward and talking about how her relationship had changed with him in those early times, and then what she wanted to have happen.
Working with an attachment focus altered many aspects of what an ECI professional might do, say, think or even how they physically position themselves when working with a family. One interviewee described her attachment-focused approach in ECI as follows: . . .we’re entering the space of a family and so, our focus needs to be on them and their relationship and growing the skills between them. It’s not just building capacity of the parent. It’s actually that you can’t build capacity of the parent without the parent actually having a good relationship with their child. It has to start with a good relationship before we build the capacity for it to be effective. (Professional)
Assessment
Participants identified various ways of formally or informally assessing parent–child interactions. First, there was a range of risk factors for insecure and disorganized attachment, which, if present, could prompt ECI professionals to prioritize attending to the parent–child relationship. These risk factors, similarly identified by Rees (2005), included family violence, drug or alcohol abuse, mental illness, young families, poverty, social isolation, parents who have been in care themselves, parental disability, rural/remote, and families who have experienced intergenerational trauma such as First Nations or refugee families. One of the interviewees summed up the impact of these risk factors for insecure or disorganized attachment in addition to the risk arising from a child having DD as follows: In a sib[ling] group of three or four, this is just one child and then the parent might have the financial stress, the family violence, the partner distress, whatever’s going on, their own unresolved trauma from childhood, you know, their own limited capacity through their own disability like you know, you just get it stacked up against you in terms of setting the right conditions for a secure attachment to be formed. (Professional)
Participants discussed a range of tools that assisted professionals in understanding more about the parent–child relationship whether these risk factors were present or not. One interviewee described how the PICCOLO (Innocenti et al., 2013) assisted parents and professionals to reflect on parent–child interactions when used formally and how familiarity with the tool shaped the observations subsequently made by an ECI professional ensuring a focus on, and support of, the parent–child relationship. Interviewees discussed how tools that are commonly used in ECI, such as routines-based interviews and ecomaps (McWilliam, 2010) or, alternatively relational maps for First Nations children (Stewart & Allan, 2013), could provide information about how the child relates to others as follows: So, you know how we might sit with people and do like an ecomap or genogram to look at the humans in their world. You know, who’s their doctor? Or who’s their support people? . . . Who are their primary attachments? If this type of assessment included a relational understanding and professionals actually ask, “Hey, you know, is there any landscape that is really important to you? Are there any animals who are part of who you are? Are there particular ancestors that you think about?” Then that just allows the professionals to know some of the support network around the child a lot more but also, it makes the child feel a lot more seen. (Professional)
Participants from Sample group C (see Table 1) talked about what they looked for in more natural observations of parent–child interactions to guide their intervention, such as (a) ease with one another; (b) parental responsiveness to child cues; (c) reactions to tantrums or ruptures in the relationship; (d) following the child’s lead in play; (e) child response to separation from the parent; (f) alignment of parents; or (g) child’s comfort seeking. One expert recommended that when observing what happens when a parent and their autistic child separate, the focus should be more on proximity than on social behaviors such as eye contact. An Australian First Nations parenting expert stressed that care must be taken when observing First Nations’ children to ensure Western assumptions do not lead to misunderstandings, saying, “. . .it’s also dangerous because it’s so opposite to First Nations’ understanding of attachment. It can create the most terrible misunderstandings. Misunderstandings that have terrible outcomes.” For example, a First Nations child may not display distress when left alone because they may feel an ancestor is with them, or they may not be upset at being taken from their parent and placed with another relative as that relative may hold a parent status for them.
Strategies
The strategies emerging from the data were grouped into cognitive—those related to ways of helping parents shift their thoughts and/or feelings toward the child; and behavioral—those strategies focused on getting the parent to do something differently. Examples of cognitive strategies and illustrative quotes included:
i. Talking about attachment—helping parents understand what attachment is and why it is important, and how to identify their own child’s attachment behaviors, as described by one professional, “I think it’s very much about helping parents identify and interact, identify behaviors and also showing the parents “Yes, your child is attached to you. Look at these behaviors.”
ii. Supporting parent–child communication—helping parents read the child’s cues—are they engaged or disengaged? Do they need comfort? Space? Helping parents tune into the child’s attention and follow their lead, imagine what the child is thinking, and go at the child’s pace:
. . . that’s very much about trying to become synchronous with your child and building on key behaviours like joint attention and communication bids that the child emits and then responding in a contingent way to those bids. . . try and build up that synchrony so that the child can communicate effectively. . . (Professional)
iii. Helping the parent co-regulate—building the ability of the parent to notice, name, and regulate their emotions may enhance their capacity to co-regulate their child and build the child’s capacity for self-regulation. This was the foundation of Tuning in to Kids which teaches parents to emotion-coach their children: notice emotion, connect with the child, name and/or reflect the emotion, empathize, and if necessary, solve problems (Havighurst et al., 2009). Mindfulness techniques were used in both individual and group work by the attachment-focused professionals employed outside of ECI to help parents self-regulate, thus placing them in a calmer state to co-regulate with their children:
. . .we know that children are so good at picking up on physiological responses of their parents and caregiver as well and rely on that as their way of assessing safety. So, if a parent is presenting as highly anxious, they’re going to have an increased heart rate, be feeling quite tense and having all of those things going on internally which a child can subsequently pick up on and lead to them being unsettled. So, we do a breathing exercise of mindfulness of the breath. (Professional)
iv. Using video to reflect—showing the parent short snippets of video of the parent positively interacting with their child to reflect upon was a feature of several of the formal programs and tools discussed, as well as an informal strategy used by some ECI professionals. The aim of videoing was to find positive parent–child interactions that could be highlighted and encouraged to increase the likelihood of them happening more often. One interviewee stressed the importance of doing no harm, and also suggested training was required to enhance the professional’s ability to notice the positives. Examples provided erred more toward parents noticing things they would like to change. The experience of seeing themselves on video appeared to give parents new insights. For example, one professional describing the impact of a mother watching a video of her interacting with her child said, “I didn’t have to actually say anything. She looked at it and was just like “Oh my goodness I can’t stop talking to him. Just like I didn’t actually realize that I was so. . . I was just so directive.”
Other strategies emerged from the data that worked on more of a behavioral level. These focused on getting the parents to initially do something different, but ultimately might shift thoughts and feelings over time. Examples of behavioral strategies and illustrative quotes included:
v. Focusing on positives—Professional focusing on positives and helping parents identify and focus on positive aspects of their child’s behavior and traits. This is a key element of strength-based practice (SBP) (McCashen, 2010) in ECI, was exhorted by a parent as a key message for ECI professionals, “Be positive and encouraging,” and was further illustrated by this professional:
And so, the conversation was about, you know, “Okay, these are all the bad things that your daughter is doing, when do you have fun together? What are the good things?.” . . And so, I said, “It could even be that she sat down, you know, really simple. That she walked to the kitchen—if it needs to be that basic, rather than yelling and screaming and running all the time.” . . so they ended up being really, I think, the start of a shift in the mindset, to say that “Actually, my daughter is not all that bad. There are good things that she has, and we’ve just got to find them.” (Professional)
vi. Creating enjoyable parent–child engagement—playing games and having fun, using rhymes and songs, telling stories, and doing things together. This strategy was used in formal programs such as Make the Connection (O’Neill et al., 2018) and Parent–Child Mother–Goose (Terrett et al., 2013) as well as in individual work with families as depicted in the following quote:
So, we really want to foster that relationship and, yes, so the way to start that for me, was really “How can we have fun together?” And it was when we started talking about that, that I think Mum was then reflecting on “Actually yeah, I don’t have fun with her at all.” (Professional)
vii. Using touch—parents soothing a child physically, such as through cuddling or rocking, massage, and gentle touch in rhymes and songs, with one professional explaining, “Well, I would say that gentle touching rhymes are really important in establishing that gentle pleasure between parent and child. It helps to settle and soothe them and to build trust and to help also to regulate.”
viii. Sensory or self-regulation strategies—tactics used to help children manage sensory dysregulation. A parent of a child experiencing sensory overload as part of her disability talked about the positive flow-on effects of self-regulation strategies as they improved the child’s behavior, reduced the parent’s stress and increased their confidence, helping to tip the parent–child relationship in a more positive direction.
Finally, there were strategies discussed that may involve external supports or referrals:
ix. Counseling—Parental mental health was raised frequently by interviewees as an impediment to secure attachment. One parent encouraged ECI professionals to explore parental feelings further, “Ask parents how they are feeling about the diagnosis. Like really ask them about their emotions.” While another parent spoke of the role ECI professionals can play in connecting parents into counseling services:
. . .if you’re an OT or a speechie or a psychologist, it may not be your role to actually provide that mental health support to a parent or caregiver, [but] you are an important link in the chain and some of these families feel really isolated and they also may not realise that they need it. (Parent)
Formal programs—looking at the evidence and adopting or referring out to formal programs with a focus on parent–child interactions were discussed as being helpful. However, as stressed by one professional, only in addition to the individualized family work of an ECI professional, “We infuse our family services with these other programs that really do target the relationship base, but you can’t just do that.”
Some programs discussed required facilitators to run them to fidelity while others provided principles or a framework to guide practice. Formal programs discussed in the interviews included some with a clear focus on improving attachment security—Circle of Security (Powell et al., 2014), Make the Connection (O’Neill et al., 2018)—and those with a focus on improving parent–child interactions or communication: Cradle to Kinder (Fewster, 2016), Denver Model (Rogers, 2010), Hanen, Parent–Child Mother–Goose (Terrett et al., 2013), Peek-a-Boo (Bunston, 2006), PICCOLO (Innocenti et al., 2013), and Tuning in to Kids (Havighurst et al., 2009).
Outcomes
Finally, data arose from the interviews, which may help inform ECI professionals as to when their attempts to improve the attachment security of the children with whom they work are succeeding. Changes were observed in child development, such as improvements in communication, self-regulation, social skills, and behavior. Some children became more discriminating about who they approached for help. Changes were also observed in parental responsivity, affection, and encouragement, together with an enhanced understanding of their child’s perspective. Parents could see the positives and enjoy their child, their confidence increased, and they expressed more hope for the future. Parents gained skills in regulating their own and their child’s emotions. They reported less stress and were more visibly relaxed. Some parents followed the child’s lead more, were less emotionally dismissive, and more in tune with their child’s overall needs. The parent and child appeared more connected, enjoying each other’s company, and families were enjoying activities together: And she was saying, “We’re now playing Snakes and Ladders, the three of us. We can sit there, and we can play a whole game of Snakes and Ladders and it ends okay, you know? It doesn’t end badly.” And just those moments like that, that you’re just going, “Yeah, it’s been worth it.” (Professional)
The bi-directional nature of these changes was illustrated by some interviewees such as: And yeah, there was a noticeable change. She was conscious of not being too involved. She was able to step back, actually followed his lead, and allowed him to direct the play. So, when he changed play ideas, she went along with him and he opened up, like he responded to that. He actually got excited about what he was trying to show her or to play with and so immediately from the first visit video to the next you could see that he opened up. She naturally then became more positive because he was opening up to her and so, there was just a more of a team and more of a united relationship between the two of them. (Professional)
Proposed Framework
An attachment-focused framework of ECI was developed at the final stage of advanced coding and theoretical integration (Birks & Mills, 2015). The framework is visually represented in Figure 2. This nesting of child development outcomes within broader contexts is aligned with Bronfenbrenner’s Ecological Systems Model (Bronfenbrenner, 1979). The proposed framework has the developmental outcomes for children, which is the goal of ECI, at the center. The key categories of Importance, Challenges, and Outcomes sit at this innermost level of the framework, highlighting why attachment should be a central focus of ECI. The environment most conducive to positive developmental outcomes, secure attachment, is at the microsystem level. Self-regulation appears here as a sub-concept of attachment due to the pervasive connections found between self-regulation and attachment throughout the data. The key categories of Assessment and Strategies sit at the microsystem level, informing how ECI professionals can identify and support attachment security. The environment most conducive to secure attachment sits at the mesosystem level—the deep, engaged relationship between a knowledgeable, attachment-focused ECI professional and the family. The category named The Key Worker, sits at the mesosystem level as core elements of the Key Worker role, such as coaching and SBP, support the development of positive family-professional relationships. The exosystem level is synonymous with the key category, The System. The elements within the system identified as being conducive to security included the provision of early, easy access to best practice services and enabling the ongoing development and emotional support of the professionals within the system., The macrosystem level, which refers to social and cultural values, is not dealt with in the proposed framework, nor is the chronosystem level, which refers to changes over time. The macrosystem was raised to a limited extent in the interviews regarding limitations to the knowledge and focus of society on attachment and thus the paucity of attachment-focused service options available to families. There was also some limited discussion of changes over time, mainly concerning transition to educational settings being times when problems with attachment are likely to become apparent.
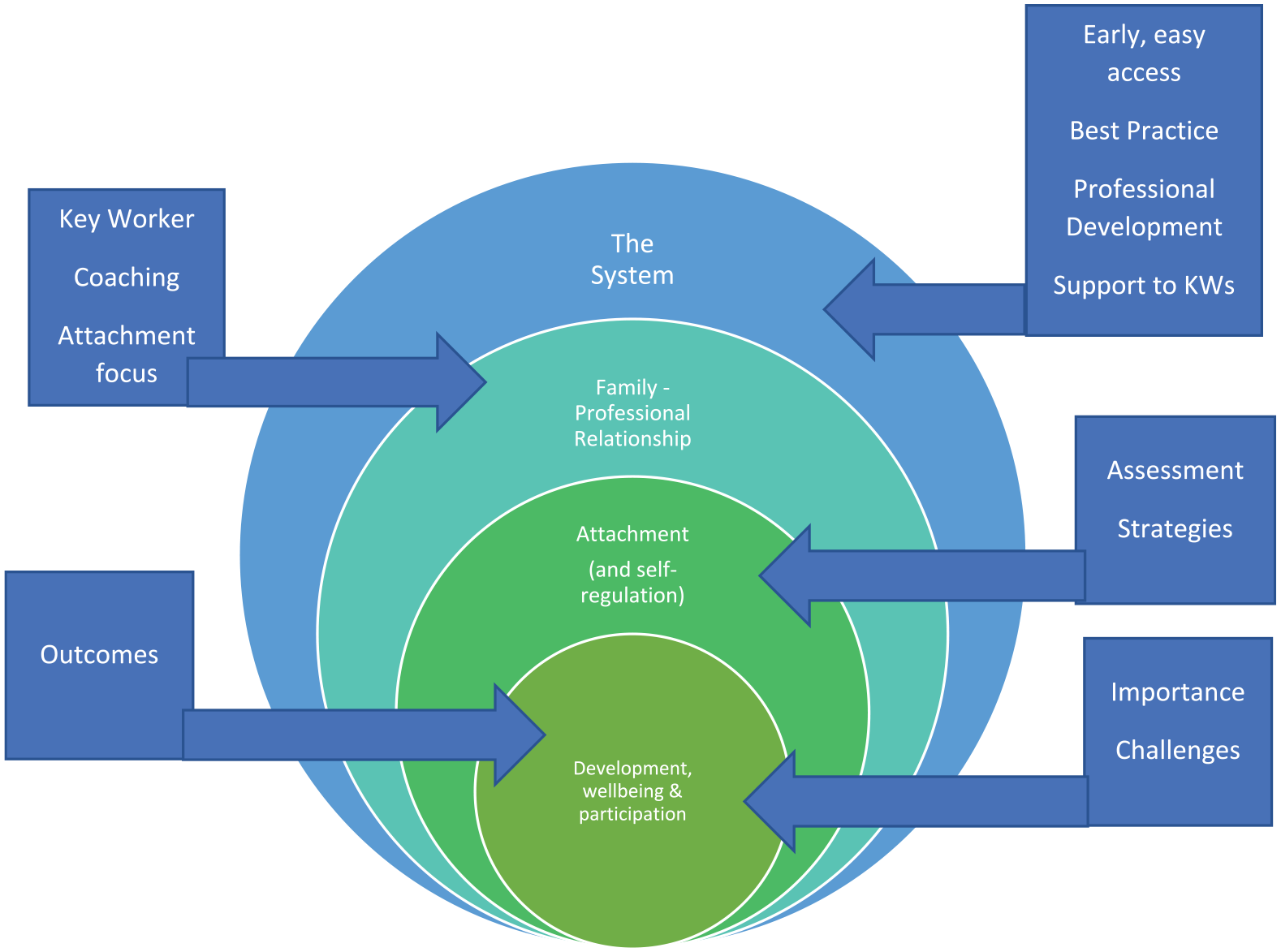
Attachment-Focused ECI Framework.
In accordance with CGT methodology (Charmaz, 2014), following the development of the proposed framework, a literature review was conducted on frameworks, theories, and models of ECI to compare prominent examples with the model proposed in the present research. For example, Guralnick’s developmental system approach (DSA) posits that child development is an outcome of the quality of parent–child interactions, the experiences provided by the family, and the health and safety families provide (Guralnick, 2005). These so-called family interaction patterns are influenced by stressors coming about from the child’s characteristics, such as DD. These stressors include the need to get information—for example, about services and prognosis; the distress parents may experience regarding the disability or delay; the need for resources; and the impact all of these might have on their confidence as parents (Guralnick, 2005). The DSA also looks at family characteristics or stressors that can impact these parent–child interactions, such as poverty, mental health, and social supports (Guralnick, 2005). The current proposed framework concurs with the DSA, and the authors see the DSA as the foundation of the Key Worker approach (Alexander & Forster, 2012). The proposed framework overlays an attachment lens to the DSA, so that in addition to the Key Worker addressing any stressors that may impact on parent–child interactions, they also directly attend to the parent–child relationship. The proposed framework also emphasizes the relationship between the ECI professional and the family and the care the system takes of these professionals. This required emphasis on attending to the positively cascading parallel processes that may result in improved parent–child interactions—from governments to services, services to communities, managers to staff, staff to parents and parents to children—that has been highlighted for several years in the ECI sector (Moore, 2007).
The integrated framework for practicing evidence-based ECI and family support posited by Dunst (2007) also underlays the Key Worker approach and is supported by the current study. Dunst’s framework stresses that as children learn through the interactions and experiences afforded them by their parents and other primary caregivers, ECI needs to focus on strengthening the skills and confidence of and the social supports available to parents and caregivers for the optimization of these interactions and learning opportunities (Dunst, 2007). The proposed framework endorses this and emphasizes the need to prioritize attending to the quality of the parent–child attachment.
The Routines-Based Early Intervention (RBEI) model also emphasizes that children learn best through their everyday activities, routines, and relationships (McWilliam, 2010). Key tools of the RBEI model, ecomaps and routines-based interviews, were discussed by some of the interviewees. These tools and the other key elements of the model—such as having one main professional working with the family in their home and supporting the other significant environments and relationships for children like early childhood education settings—are all elements supported by this research. The proposed framework would advocate an RBEI approach by an attachment-focused Key Worker. The same tools would be overlaid with an attachment focus.
Finally, the primary service provider coaching approach to ECI (Rush & Shelden, 2011) is supported by the current study’s findings, again with the addition of an attachment focus. The ECI professional would still be working with parents on parent-identified goals, letting the parent lead, asking questions, and supporting the parent to generate strategies that suit their family circumstances, but all through an attachment lens. In summary, the proposed attachment-focused framework that has emerged from this study contends the following:
The aim of ECI to optimize the development, well-being, and participation of children with DD is best supported within the context of the child having a secure attachment relationship with their primary caregivers.
Secure attachment for children with DD can best be supported by a Key Worker sensitive and responsive to individual needs, preferences and circumstances, connecting deeply with each family, taking a coaching approach with an attachment focus, and drawing on a range of tools and strategies as appropriate.
The system providing ECI services can be most conducive to this aim when it enables early, easy access to services for families, fosters the provision of a best practice Key Worker approach, and supports the ongoing professional development and emotional well-being of ECI professionals.
In brief, secure attachment is conducive to optimizing the development, well-being, and participation of children with a disability or developmental delay. It can be supported by an attachment-focused ECI professional deeply engaged with their family and supported by a system committed to this aim.
The current research affirms the contemporary best practice approach to ECI and adds the focus of attachment security. If adopted, the proposed attachment-focused ECI framework has the potential to improve attachment security and thus outcomes for children with DD and their families. The scope of factors that may be influenced by improved attachment security includes, but are not limited to, learning, communication, behavior, socialization, self-regulation, and the emotional well-being of children and families (Cassidy & Shaver, 2016). Secure attachment does not guarantee developmental outcomes but is critically involved in the initiation of complex developmental pathways and has lasting effects (Sroufe, 2005).
Discussion
The current study employed CGT methods (Birks & Mills, 2015; Charmaz, 2014) to explore how ECI professionals could improve the attachment security of children with DD. Seven key categories were identified: (a) Importance, (b) Challenges, (c) The System, (d) The Key Worker, (e) Assessment, (f) Strategies, and (g) Outcomes, as were two primary themes—the quality of the relationship between the ECI professional and the family, and self-regulation. An attachment-focused ECI framework was developed from the analysis of the relationship between these categories and primary themes. Clear strategies arose from the data which could be used within the context of ECI including education and awareness, support for parent–child communication and co-regulation, creating and focusing on enjoyable parent–child interactions, using video to reflect, and referrals for counseling and formal programs as required. The quality of the relationship between the ECI professional was found to the key element in effectively supporting the development of secure parent–child attachment. The other main theme identified, self-regulation, underpinned the importance and challenges of attachment for children with DD, and how to improve their attachment security.
The role co-regulation plays in the development of secure attachment has been explored in the literature with Schore and Schore (2008) going so far as to suggest that advances in neurobiology had shifted attachment theory to regulation theory. Despite awareness of this association, the predominance of the self-regulation theme in the present study’s data was an important finding. Self-regulation skills appeared to be impaired by attachment insecurity and disorganization. However, problems with self-regulation were also demonstrated to have an impact on nascent parent–child relationships—there was an inherent link between attachment and self-regulation in which each affects the other. Later problems in childhood regarding behavior, mental health, as well as family crises, appeared to be associated with ongoing difficulties in self-regulation.
These interconnections identified in the present study were supported in the literature. For example, some children with DD need additional support with self-regulation, sometimes due to challenges with hypo or hyper-sensory processing, with self-regulating capacity developing within the context of a relationship (Laurent & Gorman, 2017; Pallini et al., 2018). Secure attachment may enhance self-regulation skills, but it is also possible that challenges with the development of self-regulation skills could negatively influence the quality of attachment by placing additional strain on the parent–child relationship (Pallini et al., 2018). Parenting behaviors required for the development of secure attachment and those required for the development of self-regulation are similar to each other, namely regularly responding sensitively to their child’s distress and making the child feel safe when they explore (Pallini et al., 2018). The high rates of insecure and disorganized attachment for children with DD (Alexander et al., 2021) and the corresponding high rates of problems with self-regulation (Laurent & Gorman, 2017; Memisevic, 2015) are concerning. Having problems with self-regulation can lead to difficulties in cognitive and social development, behavior, emotional well-being, and academic success (Memisevic, 2015; Pallini et al., 2018). Problems in any of these areas can be stressful for parents and increased parental stress increases the likelihood of negative parenting behaviors which increases the likelihood of negative child behaviors (Hastings, 2002; Mitchell et al., 2015). Stress impacts parental sensitivity (Booth et al., 2018) and makes co-regulation more challenging (Murray et al., 2014). A negative cycle may develop in which an initial issue, such as difficulty settling a child to sleep, can compound over the years with bi-directional negative effects between parental stress, child behavior, and parental behavior (Hastings, 2002). Children with DD are three to four times more likely to experience abuse and neglect (Sullivan & Knutson, 2000), are overrepresented in out of home care (CREATE Foundation, 2012), have vastly higher rates of mental health problems (Emerson, 2003), and are overrepresented in the justice system (Holland et al., 2002). These are all extreme issues that are very expensive to address (McCarthy et al., 2016), and intervening later is more costly and less successful than intervening earlier (Perry, 2004). If parents had early, easy access to high-quality attachment-focused ECI in infancy and early childhood, some of these negative outcomes may be moderated (Alexander et al., 2019). Early support for the parent–child relationship and the fostering of secure attachment, might mitigate the risk of abuse and neglect, and maximize developmental outcomes, thus avoiding the ramifications of deficits in self-regulation.
Strengths, Limitations, and Recommendations
A strength of this study was the presentation of the breadth and depth of parents’ lived experience, and professionals’ practice, in combination with academic knowledge. The wide mix of disciplines represented across participants and by the authors provided a broad perspective reflective of the multi-disciplinary ECI sector. The authors are unaware of any other study exploring how ECI professionals can improve the attachment of children with DD. The proposed framework, while supporting contemporary best practice frameworks for ECI, adds a new lens.
A limitation of this study was that all participants were from the State of Victoria so may not be nationally representative. Despite participants being sought through two organizations involved with thousands of families with a child with DD, a limitation of this study was the low number of parents interviewed. All parent participants were middle-class professionals and none of them had experienced a Key Worker approach to ECI. Given that a global pandemic was underway and many families were experiencing high levels of stress, the authors deemed it inappropriate to recruit more participants, especially the marginalized or vulnerable families required to balance the sample. As always in CGT, the proposed framework or substantive theory, “is considered to be fallible, dependent on context and never completely final” (Sbaraini et al., 2011, p. 3). Further research is required to validate the framework.
Recommendations include that future research could explore outcomes from educating ECI professionals regarding the importance of attachment and how it can be addressed within a best-practice approach to ECI. Replication of this study might include a wider range of parents to consolidate findings.
Conclusion
Children with DD are less likely to develop a secure attachment and almost twice as likely to develop a disorganized attachment than children without DD and this has implications for their development, well-being, and participation in family and community life. The self-regulation skills of children with DD appeared in this study to play a central role in the importance, challenges and compounding implications of insecure and disorganized attachment for children with DD. This study proposes an attachment-focused framework for ECI to address this developmental disadvantage and optimize outcomes for children with DD and their families. Adoption of this proposed framework would involve systemic changes to support early, easy access to ECI professionals who not only operate from a best practice Key Worker coaching approach but are knowledgeable and focused regarding attachment. The quality of the relationship between the ECI professional and the family facilitates the effective use of strategies identified in this study to support the development of secure parent–child relationships which can be drawn on according to families’ individualized needs and preferences. An attachment-focused approach to ECI has the potential to guide the bi-directional effects of parent–child relationships on a positive developmental pathway.
Footnotes
Acknowledgements
The authors are deeply grateful to the parents and professionals who participated in this study, giving their time and sharing their wisdom and experience.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.