
Abstract
Caregivers are critical partners in early intervention service delivery; therefore, it is essential to ensure that early intervention practitioners (EIPs) have sufficient training in family-centered strategies to assist families with reaching targeted family and child outcomes. The triadic strategies from the Parents Interacting With Infants (PIWI) framework comprise a set of six practitioner strategies that align with family-centered caregiver coaching practices. For this mixed methods study, we used single-case research design to investigate a virtual training and coaching program for EIPs to increase their use of triadic strategies with caregivers during teleintervention sessions. We also conducted interviews to understand the experiences of EIPs and families with triadic strategy use. Results suggest practitioners demonstrated modest increases in strategy implementation, with marked decreases in directive strategy use. Participants described experiences with strategy use as well as factors potentially influencing implementation. Implications for practice and research are discussed.
Keywords
Caregivers’ early interactions with their children influence children’s learning and development in multiple domains. The literature suggests that supports targeting children’s development are most effective when initiated early in life and when actively involving the child’s family members (Phillips & Shonkoff, 2000). Federal grant funding offered under Part C of IDEA assists states with the provision of early intervention (EI) services to support families and their young children under the age of 3 with disabilities (Bruder, 2010). One of EI’s primary goals is to strengthen families’ capacity to support children’s growth and development (Friedman et al., 2012) through the delivery of family-centered care. As one of the first service providers families encounter, EI practitioners (EIP), are in a unique position to help caregivers meet the needs of their child’s growth and development. However, most families of children in EI receive only 2 hr a week of service or less, with a small percentage receiving less than 30 min each week (McWilliam, 2012). Given their limited service hours, it is essential that EIPs use effective strategies to promote the greatest possible positive impact on child and family outcomes. Ensuring that EIPs have sufficient training to assist families with reaching targeted family and child outcomes is essential. In this study, we aimed to support EIPs in using triadic strategies and understand how these evidence-informed strategies enhance their skills and knowledge to support caregiver-child interaction.
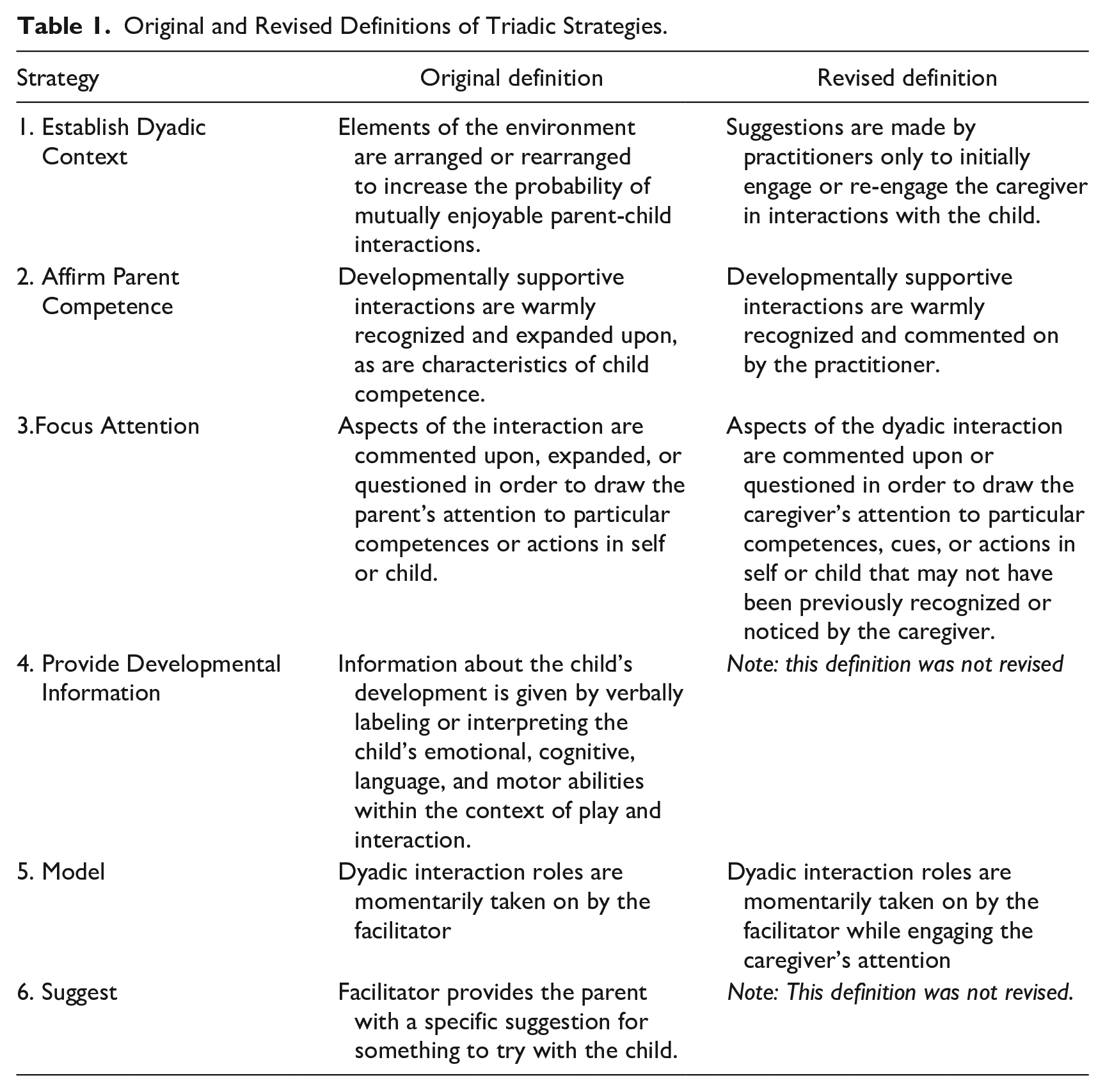
The triadic strategies as presented within the Parents Interacting With Infants (PIWI) framework (McCollum et al., 2001; McCollum & Yates, 2001, 1994) comprise a set of six practitioner strategies (see Table 1) that align with family-centered caregiver coaching practices. The primary aim of the PIWI framework is to improve caregiver–child interactions during family routines and activities. Its emphasis on strengthening the dyadic relationship to promote child and family outcomes is consistent with Division for Early Childhood (DEC) recommended practices (Division for Early Childhood [DEC], 2014) and evidence-based practice in EI (Trivette et al., 2010). To date, the triadic strategies from the PIWI framework have yet to be investigated for their effectiveness in supporting EIPs’ use of a family-centered, capacity-building approach.
Original and Revised Definitions of Triadic Strategies.
EI services provided via teleintervention have the potential to increase triadic interactions among EIPs, caregivers, and children because EIPs are less likely to work directly with children and more likely to interact with caregivers (Ashburner et al., 2016). Furthermore, teleintervention sessions typically occur in the child’s natural learning environment with materials found in their home (Williams & Ostrosky, 2020). Teleintervention has also been suggested as a solution to providing services to families and young children at a distance (Ashburner et al., 2016), thereby reducing travel time, eliminating transportation costs, and allowing EIPs to devote more time to service delivery (Kyzar et al., 2014; Meadan et al., 2020).
Despite more than 30 years of recommendations for EIPs to provide family-centered practice, its implementation in EI remains inconsistent (Movahedazarhouligh, 2021). EIPs frequently report that they feel unprepared to successfully engage families and their young children, despite having preservice training (Bruder, 2010; Dunst et al., 2014). Specifically, EIPs express feeling undertrained in essential family-centered, relationship-based strategies (Banerjee & Luckner, 2014; Bruder et al., 2013). Therefore, EIPs need high-quality professional development to help them effectively implement family-centered practices (Bruder, 2010; Dunst et al., 2014; Romano & Schnurr, 2022). Professional development (PD) that includes training and coaching is more likely to result in skill acquisition, professional confidence, and relationship-building than traditional PD alone (Fixsen et al., 2005; Trivette et al., 2009). Thus, EIPs who receive virtual training and coaching on triadic strategies may feel better prepared to support families via teleintervention and deliver effective family-centered services that increase family capacity (Meadan et al., 2020).
Single-case research designs (SCRD) are commonly used in special education intervention research and allow researchers to assess causal relations between intervention variables, such as training and strategy use (Ledford et al., 2019). Qualitative inquiry is crucial in understanding contextual factors that support or hinder intervention effectiveness. Therefore, using a mixed-methods approach incorporating both SCRD and qualitative research design is ideal for this inquiry, as it has the potential to provide an assessment of the effectiveness and meaningfulness of the intervention for each case (Onghena et al., 2019). In addition, multiple phenomena can be explored to expand the focus of the study and more broadly understand EIPs’ strategy use (Corr et al., 2020; Greene, 2007).
The purpose of this study was twofold. Using mixed methods, we aimed to investigate the feasibility of a virtual training and coaching program for EIPs to increase their use of triadic strategies with caregivers during teleintervention sessions. In addition, we sought to understand the experiences of EIPs and families with training and implementation of triadic strategies. Research questions for this project are as follows:
Method
Research Design
This study employed an explanatory sequential mixed-methods design, beginning with a quantitative phase and extended by a qualitative phase (Creswell & Plano Clark, 2017) (see Figure 1). Specifically, we used SCRD to investigate the effectiveness of training and coaching on increasing EIP’s use of triadic strategies and improving caregiver–child (referred to henceforth as the “dyad”: McCollum & Yates, 1994) interactions during teleintervention. This was followed by qualitative interviews to explore participants’ lived experiences of the intervention. Using an explanatory mixed-methods design was an appropriate fit for this study as it allowed researchers to observe and examine relationships between intervention variables and use qualitative inquiry to help explain data patterns found in quantitative results. It aided in expansion, as using each method helped attain a broader understanding of multiple phenomena regarding strategy use (Greene, 2007). Consistent with explanatory sequential mixed-methods design, results were reviewed after the quantitative phase to inform the development (Greene, 2007) of the qualitative phase and then integrated at the end of qualitative data collection to merge findings.
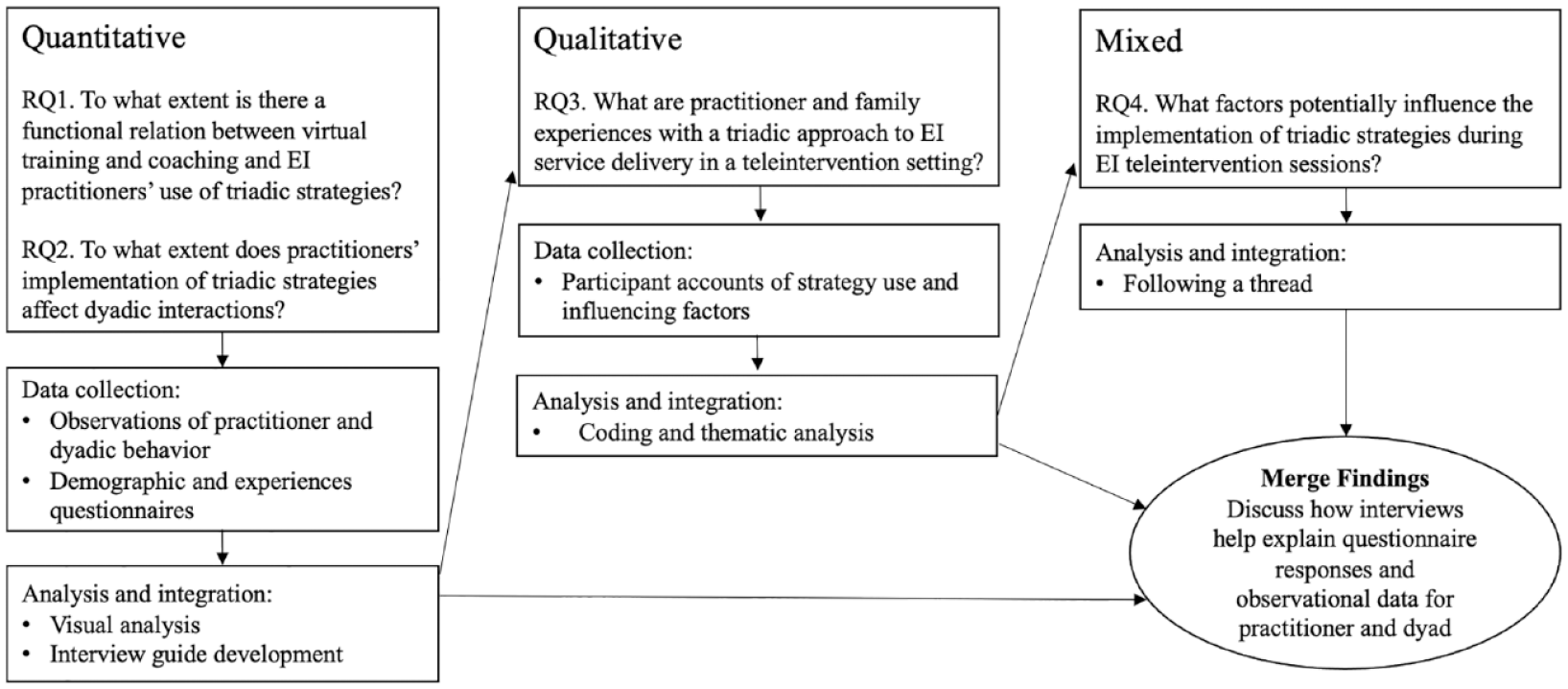
Explanatory Mixed Methods Design (QUAN + Qual).
All study training and procedures were delivered via videoconference by the first author, who has extensive experience providing EI services in community settings and training practitioners to use triadic strategies. At the time of data collection, the first author was a doctoral student engaged in scholarly activities focused on promoting positive child and family outcomes in early childhood special education.
Sample and Recruitment
Participants included four triads, each consisting of one EIP, one child, and the child’s caregiver(s). Participants were recruited as triads: EIPs were recruited initially, and families were selected and recruited through participating EIPs.
Inclusion criteria for EIPs for this study included: (a) work in the role of special educator, speech-language pathologist (SLP), physical therapist (PT), or occupational therapist (OT), with at least a Bachelor’s degree level of education; (b) employed by an agency within the identified state, (c) practicing in their role for at least 6 months; and (d) employed in their current position during the study period. We sought to include EIPs who provided teleintervention visits with families in the child’s natural environment and represented the diverse professional backgrounds of the EI workforce.
We recruited from EI agencies across a Pacific Northwest state who were providing EI services via teleintervention. Agency leaders assisted with recruitment by circulating emails and flyers to EIPs and inviting EIPs to contact researchers for more information. Initially, recruitment emails were circulated to approximately 30 EI programs from across the state and 15 EIPs screened from other studies. Nine program coordinators responded that they would circulate the opportunity among their staff. EIPs interested in joining the study were invited to meet with research staff to ask questions about participation, learn about study procedures, and provide consent to participate. Twelve EIPs scheduled information meetings with the first author; four could not identify a family to participate. Eight EIPs identified families of young children with disabilities whom they served, and interested families contacted the first author. Four triads attritted due to scheduling conflicts or EI service changes. Four remaining triads completed all study procedures and are described below. All interested EIPs and caregivers met individually via Zoom with the first author. During the consenting meeting, the first author presented potential participants with verbal descriptions and visual maps of study procedures and answered questions. EIPs and caregivers were provided respective consent forms to review, complete, and return to the first author online.
Participants
All names are pseudonyms chosen by participants (see Table 2 for participant information). Triad 1 consisted of Jannie, her 2-year-old daughter, and their special educator, Lauren. Lauren identified as a White female, spoke English as her primary language, held a Master’s degree, and worked in EI for three years. Prior to becoming an EIP, Lauren worked in Applied Behavior Analysis (ABA) and spent her first 4 years after receiving her Master’s degree as a K–2 classroom teacher. Jannie and her daughter identified as Asian. Vietnamese was their primary language; an interpreter was present for all EI sessions and study activities. Jannie’s daughter did not have a formal diagnosis but was identified as at risk for disability and had received education and speech therapy services for approximately 1 year.
Participant Demographics.
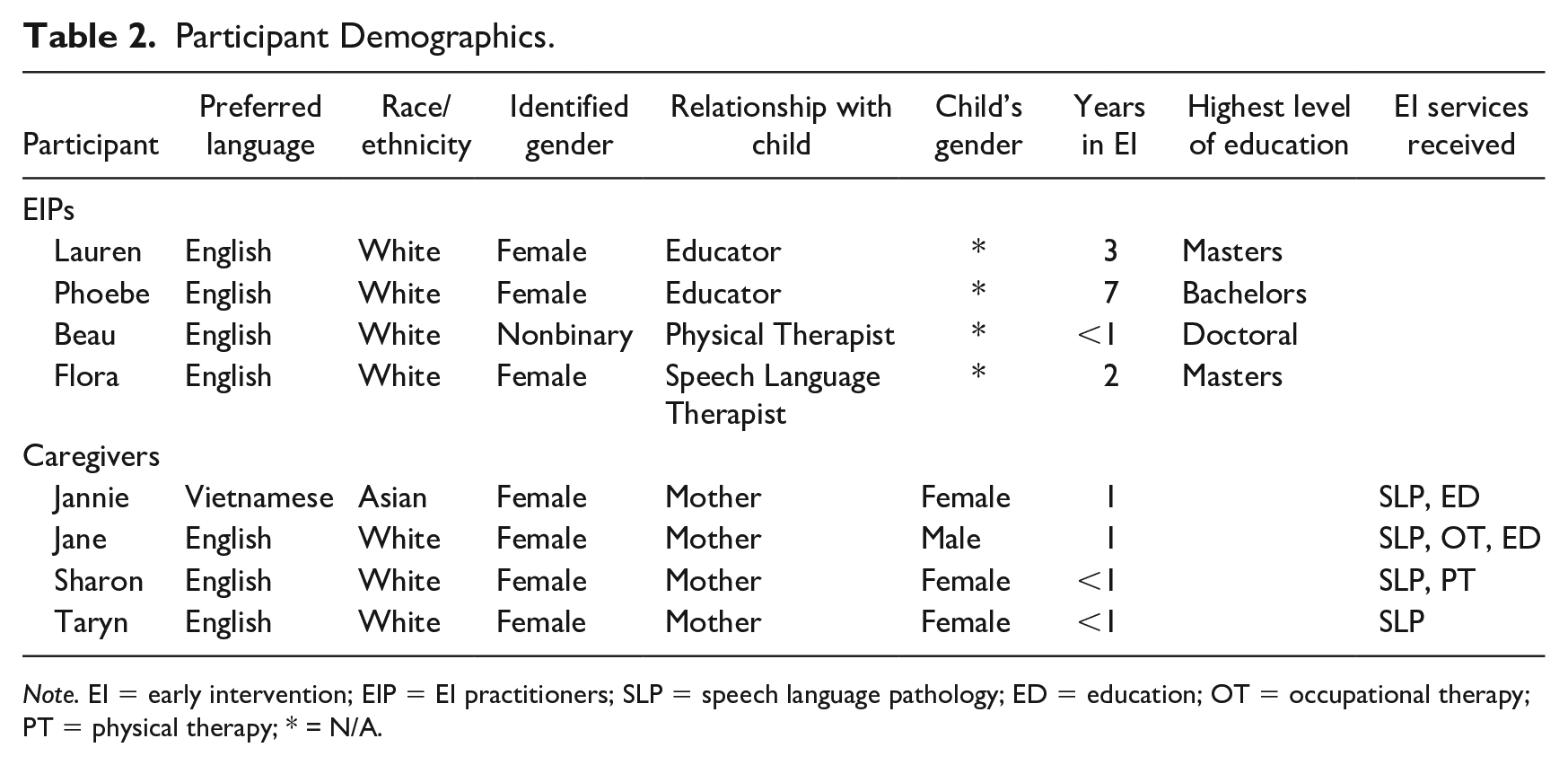
Note. EI = early intervention; EIP = EI practitioners; SLP = speech language pathology; ED = education; OT = occupational therapy; PT = physical therapy; * = N/A.
Triad 2 included Jane, her 15-month-old son, and their EIP, Phoebe. They each identified as White and primarily spoke English. Phoebe, a special educator, was female, held a Bachelor’s degree, and had been working in EI for 7 years. Phoebe had previous experience with both teleintervention and home visiting. Jane identified as female. Jane’s son did not have a formal diagnosis, but their family received education, speech, and occupational therapy services for approximately 1 year. He was also on a waitlist for a neurodevelopmental pediatrician.
Triad 3 included Sharon, her 12-month-old daughter, and their EIP, Beau. They each identified as White and primarily spoke English. Beau was a physical therapist, identified as nonbinary, held a Doctoral degree, and worked as an EIP for less than a year. Sharon’s husband was often present for part of their sessions, sometimes in the room with Sharon and their daughter, sometimes remotely. Their daughter was diagnosed with Global Developmental Delay and qualified for speech therapy; they had received EI services for less than a year.
Triad 4 consisted of Taryn, her 2-year-old daughter, and their speech-language pathologist, Flora. They each identified as White and primarily spoke English. Flora was female, held a Master’s degree, and worked in EI for 2 years. Taryn’s husband was sometimes present for teleintervention sessions either in lieu of or in addition to Taryn. Taryn was female. Her daughter did not have a formal diagnosis, but they had received speech services for less than a year; she was on a waitlist to see a neurodevelopmental pediatrician. Flora had previous experience conducting home visits prior to providing services via teleintervention.
Quantitative Strand
We collected quantitative data first in our mixed methods study using a concurrent multiple-baseline design across participants (What Works Clearinghouse [WWC], 2020). The design included the following phases: baseline (A), intervention (B), and maintenance (C). Phase change decisions were based on several factors, including the triad’s order of enrollment, the consistency of their session schedules, and EIPs’ use of triadic strategies. EIPs were introduced to intervention (B) when they demonstrated a stable baseline data pattern with at least two consecutive sessions occurring prior to the phase change. EIPs submitted weekly video recordings of teleintervention visits conducted with their participating family for data collection purposes. Visits across all phases ranged from 30 to 60 minutes, according to the family’s service plan. Triads met via Zoom with families connecting from their homes.
Baseline (A)
During baseline (A), triads held weekly teleintervention sessions, aligned with Part C service provisions; EIPs did not receive any instructions, training, or coaching during this phase.
Intervention (B) Procedures
Practitioner Training
Immediately following baseline and prior to intervention data collection, the first author individually trained EIPs to implement the PIWI triadic strategies (McCollum et al., 2001; see Table 1) during teleintervention sessions. The six strategies included (a) Establish Dyadic Context, (b) Affirm Parent Competence, (c) Focus Attention, (d) Provide Developmental Information, (e) Model, and (f) Suggest. Training consisted of one 90-min session, which included (a) an introduction to the triadic strategies, (b) descriptions and examples of each strategy, (c) discussion of strategy application to teleintervention, (d) opportunities for rehearsal (EIPs were invited to engage in role play or rehearsal of strategy use with the coach) and feedback, (e) brainstorming and problem-solving, in which EIPs identified potential challenges with strategy use with their participating family and identified potential solutions with the coach, and (f) time for the EIP to ask general questions about the strategies and have them addressed. The training was delivered via Zoom, with a PowerPoint slide deck, using photo and video examples of home visits and teleintervention to illustrate strategies.
Coaching
The week following training, EIPs received coaching from the first author (referred to henceforth as “coach”). For two EIPs, coaching began 7 days after training, for one EIP it began 5 days after training, and for the other EIP training began 8 days after coaching. Coaching was adapted from the Practice-Based Coaching (PBC) framework (Snyder et al., 2015) and occurred weekly throughout the course of the intervention phase. Coaching sessions were approximately 30 to 45 min in length and consisted of (a) debrief of the previous teleintervention session, (b) shared observation of a recording from the triad’s previous teleintervention session, (c) an opportunity for the EIP to reflect on their use of observed strategies and for the coach to provide supportive feedback, and (d) action planning, in which the EIP targeted goals for strategy use in their next teleintervention session with their participating dyad. (See Supplementary Appendix A for the training and coaching fidelity form). For the observation component of coaching, the coach created one 2- to 4-min clip portraying the EIP’s use of triadic strategies during the most recent teleintervention session (Marturana & Woods, 2012) or potential opportunities for the EIP to use strategies with the dyad. We targeted at least five coaching sessions for each EIP.
Trained research assistants (RA) assessed fidelity for all training (4) and coaching (25) sessions, using a 20-item fidelity checklist to review recordings of all training sessions and a 16-item fidelity checklist to review recordings of all coaching sessions. Overall training and coaching fidelity were 100%.
Maintenance (C)
Immediately following the coaching phase of the intervention, EIPs were instructed to continue implementing triadic strategies during teleintervention sessions. Coaching support was no longer provided in this phase; maintenance sessions began the week after coaching was ended. Data collection during this phase continued for one or more consecutive sessions with each triad. Maintenance data were collected for Phoebe, Flora, and Beau (Triads 2–4) only due to frequently missed sessions for Lauren (Triad 1).
Measurement and Data Collection
Two behavioral variables were measured in the SCRD: EIPs’ use of the PIWI Triadic Strategies and Caregiver-Child Dyadic Interactions. Data for the primary dependent variable, EIPs’ use of the six PIWI Triadic Strategies (see Table 1 for strategies and definitions), were collected using the PIWI Strategies Coding Sheet. RAs observed and coded the entirety of each teleintervention session submitted by EIPs using 10-s partial interval recording (Lane & Ledford, 2014). This interval coding system and interval length are used widely in EI and early childhood special education research (Lane & Ledford, 2014). With PIR, researchers record practitioner use of each unique strategy used within a 10-s interval by writing the designated code (e.g., MO for Model) in the field corresponding with the appropriate ten-second interval of time. If a practitioner implements a strategy beyond the 10-s interval, coders continue to apply the code to all subsequent intervals in which the strategy is used. More than one strategy may be coded for any single 10-s interval. Researchers used descriptive analysis (a) to determine the % of intervals in which strategies occurred across the length of the teleintervention visit and (b) to determine the proportions of different strategies used (e.g., what % of triadic strategies used was coded as Model). To determine the EIP’s time spent implementing triadic strategies, the total number of intervals with strategies was divided by the total number of intervals for the session and multiplied by 100 to calculate the percentage. The total number of intervals containing each strategy was then divided by the total number of intervals containing triadic strategies and multiplied by 100 to calculate percentage. The latter calculation represented the proportion of each strategy used by the practitioner.
We also captured occurrences of Caregiver-Child Dyadic Interactions using the Dyadic Interactions Coding Sheet. Dyadic interactions are defined as events when the caregiver and child are engaged in play, routines, and other positive, reciprocal, and developmentally supportive interactions together. Examples include talking, singing, and engaging with an activity, game, or toy together, while the parent attends to the child. Similar to procedures described earlier, RAs observed and coded the entirety of each teleintervention session, using 10-s partial interval recording to record occurrences of caregiver–child interactions during sessions. To determine the time spent in dyadic interactions, the total number of intervals with dyadic interactions was divided by the total number of intervals for the session and multiplied by 100 to calculate the percentage.
Demographic and EI Experiences Questionnaires were developed by the research team to gather differential information for caregivers and EIPs and completed by participants online. Questionnaire items included demographic information such as participants’ gender, race, age, level of education, and employment details. Following the demographic questions, EIPs completed Likert-type scale items elaborating on their experience working in EI. Caregivers reported information related to their family and their experiences in EI (e.g., family members, age of children, years of service received, overall satisfaction with service delivery). In addition, all participants rated their working alliance within their triad (de Greef et al., 2018). For instance, EIPs and caregivers respectively provided a rating for the statement, “Parents and I are working towards mutually agreed upon goals” or “Our EI practitioner and I are working towards mutually agreed upon goals.” Participants also rated their comfort with active family involvement during sessions by indicating how EIPs involve families in sessions (Dunst et al., 2014). Selections were presented via a Likert-type rating scale and included responses, such as “I only observe the service provider working with my child” or “I prefer to involve caregivers in a way where they can continue to do the interventions without my ongoing assistance.” Participants completed the first questionnaire during baseline. The initial questionnaires took approximately 10 to 15 min to complete. At the end of the study, participants completed an abbreviated version of the questionnaire that did not include demographic items. It took approximately 5 min to complete.
Prior to quantitative data collection, four RAs were trained to code recordings of teleintervention sessions for the two variables. RAs were trained over Zoom using recordings of EI teleintervention sessions, coding to 90% agreement on each variable. EIPs submitted weekly video recordings of teleintervention visits conducted with their participating family. Each RA was masked to study conditions and assigned videos for coding to increase internal validity and reduce observer bias.
RAs conducted secondary coding to assess Interobserver Agreement (IOA) using point-by-point (Kelly, 1977) agreement for 10-s partial interval recording for at least 38% of sessions of each participant triad, for each condition, and for observational coding of both practitioner behavior and dyadic behavior, with a targeted minimum threshold of 85% agreement. If IOA dropped below 80%, recalibration occurred, and additional training was provided. Reliability for EIP behavior reflects agreements regarding which of the six strategies (see Table 1) were implemented by a practitioner at any point during the designated interval. The overall mean IOA for EIP behavior was 87% (range = 74%–100%) and agreement data were collected for 44% of sessions. IOA data for dyadic behavior reflect agreements between coders regarding the occurrence of dyadic interactions at any point during a 10-s interval. Dyadic interactions were based on descriptions of caregiver contingent responsiveness and sensitivity (Dunst & Kassow, 2008) and defined as verbal (e.g., talking, singing, and vocalizing together), physical (e.g., playing on a playset or dancing together), and play (e.g., engaging with an activity, game, or toy together) interactions occurring between the caregiver and child. The overall mean IOA for dyadic behavior was 88% (range = 74%–95%) and reliability data were collected for 46% of sessions.
Quantitative Data Analysis
We used visual analysis of single-case data to inform in vivo research decisions, to make adaptations to the conditions as needed while maintaining experimental control (Ledford et al., 2019), and to complement WWC standards. Visual analysis of graphed data for EIP and dyad behavior included vertical analysis for evidence that baseline data paths changed when intervention phases were introduced, and not before intervention procedures were implemented (Wolfe et al., 2019). We also examined level, trend, immediacy of change, stability, variability, and overlap within and across conditions for each triad (Barton et al., 2018) to understand the functional relation between training and coaching and (a) EIPs’ use of triadic strategies during sessions and (b) occurrence of dyadic interactions.
Qualitative Strand
Data Collection
Qualitative data collection consisted of one semi-structured interview conducted with each caregiver and EIP (eight total) within 2 to 3 weeks of the triad’s final observed session. Consistent with an explanatory mixed methods research design, the first author developed caregiver and EIP interview protocols following the completion of the intervention phase (see Supplementary Appendix B for a sample protocol). Caregivers and EIPs answered questions that prompted them to reflect on their role in teleintervention visits, perceived benefits and barriers of a triadic approach, improvements or challenges with using a triadic approach during visits, triadic strategy descriptions, and triad-specific findings from the quantitative strand. Participants were presented with graphs of EIP strategy use and dyadic interactions to explore quantitative results by triad. Sample questions include, “Tell me what was challenging about using triadic strategies during teleintervention visits?” and “I see some changes in your interactions with your practitioner between these two timeframes. What might have influenced this? What other changes have you noticed that might not be reflected in the data?” Interviews were conducted by the first author via Zoom, ranging in length from 47 to 68 min, with an average length of 57 min. Following the interview, participants received a stipend as compensation.
Qualitative and Mixed Data Analysis
Qualitative data analysis allowed us to expand upon results from the quantitative strand. Data mixing occurred throughout qualitative data collection and analysis, with interview data used to fulfill the “explanatory” component of mixed methods data analysis. All interviews were transcribed by a professional transcription service, reviewed by the first author for accuracy against the interview recording, uploaded to Dedoose, and coded by both the first and third authors. We used a thematic analysis process (Braun & Clarke, 2006), beginning with first-round coding to elicit descriptive and structural codes (Saldaña, 2015). We created an initial codebook reflecting themes from foundational theoretical elements and themes discovered in the quantitative data. The second-round coding included writing analytical meta-memos (Saldaña, 2015), creating operational model diagrams to organize themes and their relationships, and critically analyzing proposed claims for their usefulness in explaining quantitative results.
We took several steps during qualitative and mixed data analysis to strengthen the credibility of the findings (Brantlinger et al., 2005). We triangulated interview transcripts by comparing and cross-checking emergent themes across and within participants and triads and sought corroboration with quantitative results (Fetters, 2019). We used a synthesized member check process (Birt et al., 2016) to confirm or disconfirm initial interpretations and develop the validity of the findings. The first author prepared preliminary claims and emergent themes into synthesized summaries, which were presented to participants in the form of a brief Qualtrics survey. Each of the eight participants was invited to share and submit their responses. Four caregivers and three EIPs completed the member check survey in full. Member check responses confirmed initial findings related to caregiver and EIP perspectives presented here.
Data Merging and Interpretation
Mixed methods analysis capitalized on both data strands, utilizing the “following a thread” approach (Moran-Ellis et al., 2006). Key themes from the literature and initial visual analysis (e.g., family-centered, capacity-building practices, and strategy implementation) were threaded through qualitative data collection and analysis (e.g., participant experiences with the intervention and target practices) and then threaded back through quantitative results to provide an expansive explanation and integrate the two strands. For instance, following qualitative analysis, quantitative data were revisited to determine EIP mean use of each strategy per EIP, per phase (see Table 3). To determine each EIP’s mean strategy use per phase, we added together the percent of time spent by the EIP implementing each unique strategy per session within each phase (e.g., baseline, intervention, or maintenance) and divided by the total number of sessions in that phase.
Quant and Qual Evidence for Changes in EIP Use of Strategies.
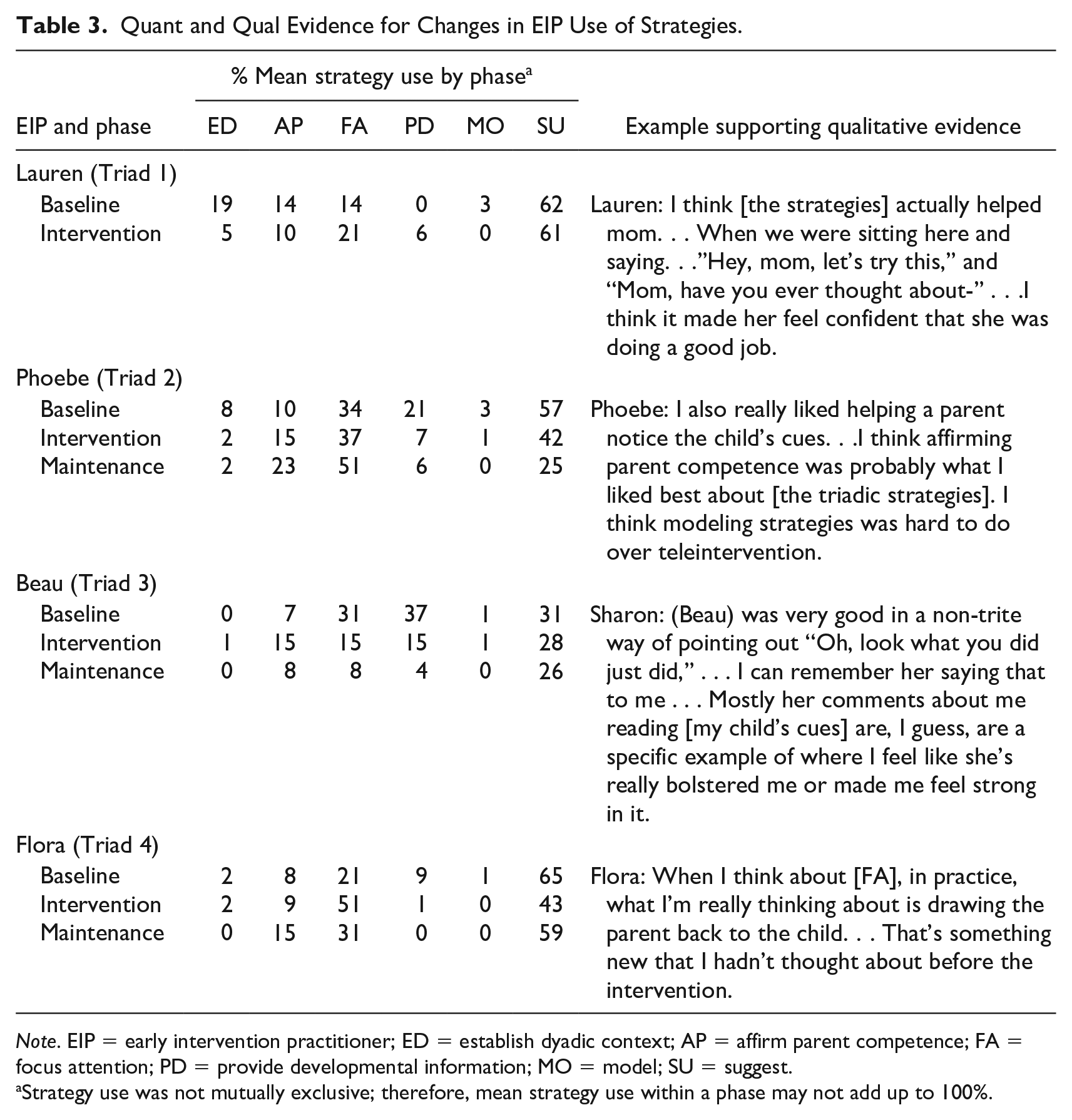
Note. EIP = early intervention practitioner; ED = establish dyadic context; AP = affirm parent competence; FA = focus attention; PD = provide developmental information; MO = model; SU = suggest.
Strategy use was not mutually exclusive; therefore, mean strategy use within a phase may not add up to 100%.
Results
Practitioner Behavior
To answer our first research question, we collected data on EIPs’ use of triadic caregiver coaching strategies during teleintervention sessions (see Figure 2). Across all four EIPs, baseline levels of triadic strategy implementation (noted by a solid line and circle) were low to moderate, with a mean use of strategies for 18% of session time (range = 1–37%). Specifically, mean use of strategies during baseline was 7% (range = 1–13%) for Lauren (Triad 1), 15% (range = 5–24%) for Phoebe (Triad 2), 23% (range = 14–37%) for Flora (Triad 3), and 21% (range = 14–34%) for Beau (Triad 4). While most baseline data points remained below 30%, there were two data points that did not: Week 4 for Beau and Week 12 for Flora. Overall, baseline data demonstrated a slight decreasing, stable trend across all EIPs, except for Phoebe whose data showed a slight increasing, stable trend.
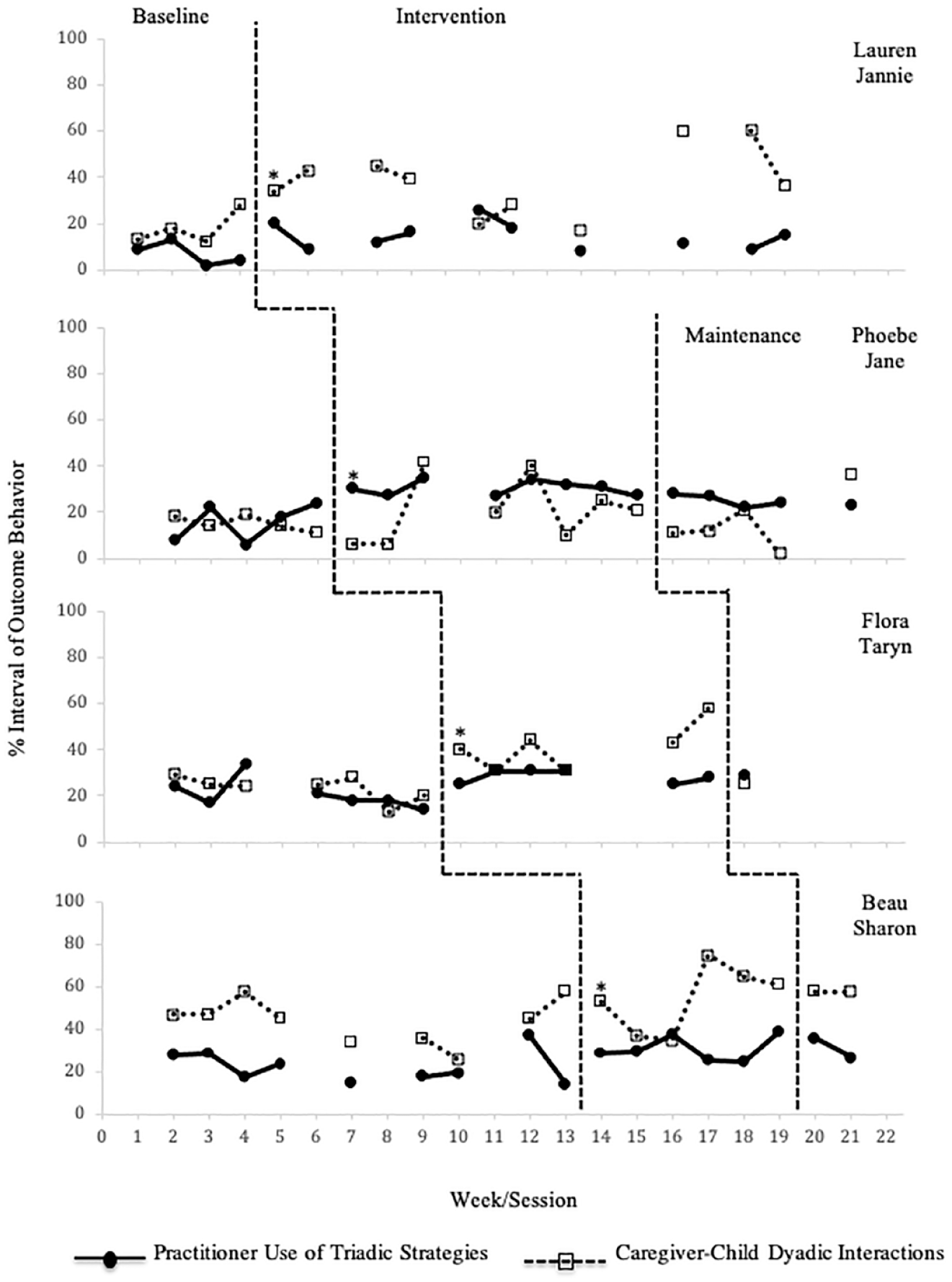
EIP and Dyad Behaviors.
When training and coaching were introduced in the intervention phase, all EIPs demonstrated a slight, but immediate, increase in their level of triadic strategy use with a relatively flat trend and maintained a minimally higher overall level of strategy use throughout as compared with baseline. The mean use of strategies for all four EIPs during intervention was 25% of session time (range = 6%–39%). Mean strategy use was 14% (range = 6%–26%) for Lauren, 30% (range = 27%–34%) for Phoebe, 31% (range = 25%–39%) for Flora, and 29% (range = 25%–31%) for Beau. Phoebe, Flora, and Beau’s data demonstrated increased stability between baseline and intervention. The intervention was functionally related with low confidence to a consistent and reliable increase in EIPs’ implementation level of triadic caregiver coaching strategies for Phoebe, Flora, and Beau, although level changes between baseline and intervention were modest. Phoebe and Flora demonstrated low variability in their strategy use across phases, with overlapping data points for Beau between baseline and intervention. Flora had a somewhat variable baseline that stabilized during the intervention and exhibited multiple overlapping data points. We could not determine a functional relation for Lauren’s data because of its overall overlapping and unstable data path. Due to inadequate data collected for maintenance phases across EIPs, we could not determine if a functional relation between the intervention and EIP behavior was maintained.
Dyadic Interactions
Data collected for dyadic behavior reflected the percentage of time the caregiver–child dyad was engaged in reciprocal interactions during teleintervention sessions with their EIP (see Figure 2) and addressed our second research question. Dyads varied in their time spent in dyadic interactions (noted by a dotted line and open square) during baseline, ranging from low variability and a stable flat (Jane—Dyad 2) or downward trend (Taryn—Dyad 3) to modest variability (Jannie—Dyad 1) or a moderately variable and unstable data line (Shannon—Dyad 4). For Jannie, Jane, and Taryn (Dyads 1-3), time spent in dyadic interaction remained below 30% of session time during baseline, dropping as low as 11% of session time for Jane (Dyad 2; Week 6). Baseline levels of time spent in dyadic interaction were observed to be higher for Shannon (Dyad 4).
Overall, the introduction of EIP training and coaching was likely functionally related to increases in time spent in dyadic interactions, although this relation was modest in some cases. For instance, Jannie, Jane, and Shannon (Dyads 1, 2, and 4) demonstrated consistently higher levels of time spent in dyadic interaction during the intervention phase compared to baseline levels, though they also exhibited moderate overlapping baseline data points. A slightly increasing trend was detected for Taryn (Dyad 3) throughout the intervention phase. Experimental control for the secondary dependent variable of dyadic interactions was not well-established across dyads, although Taryn (Dyad 3) did demonstrate an immediate and marked change in level with the introduction of the intervention. For most of the dyads, increases in time spent in dyadic interactions during sessions with EIPs occurred gradually. As seen in Figure 2, Jane and Shannon (Dyads 2 and 4) first exhibited notable shifts in time spent in dyadic interactions two to three weeks after EIPs were introduced to the intervention, on Weeks 9 (for Jane—Dyad 2) and 17 (for Shannon—Dyad 4). Jannie (Dyad 1) saw an increase much later compared to when their EIP was introduced to the intervention, at Week 17. While these increases in time spent in dyadic interactions do not immediately follow corresponding introductions to the intervention, they also do not align with phase changes for subsequent tiers.
Experiences With a Triadic Approach
Our third research question was addressed by the caregiver and EIP reflections on strategy use during their EI sessions. Participants reported on their observations of EIP and dyadic behavior and how this matched visual data displays. Participants’ reflections informed exploratory data mixing.
Reflections on Strategy Use
During interviews, participants were asked to broadly describe any changes in their teleintervention sessions during the study period and were invited to view and reflect on visual data displays representing EIP and dyad behavior for their triad.
Caregivers
Caregivers provided mixed responses when asked to consider the changes they noticed in practitioner behavior, reporting either no noticeable change or observing EIPs’ use of only select strategies. Two caregivers remarked on EIPs’ increased efforts to facilitate dyadic interactions. Jane recalled her EIP inviting more caregiver-child interactions, such as asking to see her and her child “in different scenarios, trying to get him to make a choice of one thing or the other, having him color and stuff.” Taryn felt that with the introduction of EIP training and coaching, she had more “one-on-one” activities with her daughter. Sharon noticed her EIP providing her with more positive comments or describing more of her daughter’s developmental accomplishments. With the former observation, she described her EIP as engaging in more “cheerleading, in the sense of what you’re doing is great,” and with the latter, “reminding me of the change that’s happened” with her daughter’s development. Conversely, Jannie and Taryn reported subtle differences in their EIPs’ styles. Taryn believed that her EIP had been “pretty consistent [with] no drastic changes in her coaching” and thought it was “nice that she is consistent on that.” Other caregivers echoed this sentiment, such as when Sharon observed that too much change at once could potentially make her EIP’s approach unrecognizable.
In response to viewing the data, most caregivers had additional questions about research activities and shared reflections on their behavior or their EIP’s behavior. For instance, Jane concluded that “there can definitely be a greater effort, on my part, to initiate [my child] being more present” during sessions and engaging in more dyadic interactions. Jane believed this would allow her EIP to get to know her son more and inform her EIP about how to better support her as his caregiver.
Practitioners
Two of the four EIPs felt significant changes occurred in their practice during the study period. Beau and Flora were surprised to see the data and felt that it underrepresented their implementation of strategies. As Beau said, “These numbers seem super low. It feels like they should be higher.” Flora also identified this mismatch between the visual data and her personal experience with the intervention and how it influenced her work. These EIPs felt like they were more intentional in their sessions and held a greater awareness of what they were doing in their work with families and why. Reflecting on the similarity between her use of triadic strategies between baseline and intervention, Flora shared, “Even though I’m using the strategies pretty consistently, I feel like the quality of the use of the strategies changed, but that’s hard to quantify.” Lauren interpreted increases in dyadic interactions as a sign that the caregiver was more comfortable interacting with her child. Phoebe thought the data aligned with her experience, noting the slight shift in her use of strategies between intervention and maintenance. As she said, “during coaching, I did more [implementing of strategies] than I would usually, and then I could feel it kind of slipping [after coaching].”
In response to their mixed responses to data reflections, EIPs’ strategy use was calculated by phase (see Table 3 for the mixed methods visual display). The majority of EIPs’ mean strategy use shifted from baseline to intervention and maintenance phases. All EIPs demonstrated the highest use of the strategy Suggest in baseline as compared with intervention and maintenance. The mean use of Model was low for all EIPs across phases. During the intervention and maintenance phases, strategy use for three of the four EIPs (Phoebe, Beau, and Flora), revealed similar patterns. Mean use of Suggest was lower in intervention and maintenance phases compared with baseline, and mean use of Affirm Parent Competence and Focus Attention were higher. These patterns suggest that following the intervention, most EIPs changed their triadic strategy use to provide caregivers with fewer suggestions and more feedback focused on supporting their competence and confidence or focusing their attention on their child. Table 3 presents quantitative evidence of EIPs’ strategy use within triads across phases and sample qualitative evidence reflecting, or explaining, these shifts.
Factors Potentially Influencing the Implementation of Strategies
Our fourth research question was addressed by questionnaire responses and participant descriptions of factors that may have influenced the implementation of triadic strategies. These findings help to “explain” SCRD results. Below we integrate quantitative and qualitative data and meta-inferences interpreted from these merged data.
EI Experiences Questionnaire Responses
EIPs and caregivers completed the questionnaire pre- and post-intervention. One caregiver only completed the post-questionnaire. At the beginning of the study, EIPs indicated varied comfort levels with services delivered in the home (3.5/5), as demonstrated by response ratings ranging from 1 (low comfort) to 5 (high comfort). Participants shared an overall average increase in comfort with teleintervention services at the end (4.6) compared with baseline (4.1). There was one exception; Lauren indicated a decrease in comfort with teleintervention between these two time points. In addition, participants indicated an increase in working alliance at the end of the study (4.6) compared with the beginning (4.4); one decreased their rating from 5 to 4. Participants reported an average increase in comfort with active caregiver involvement during sessions at the end (4.75) compared with baseline (4.4).
Practitioner Descriptions of Factors
Practitioner Backgrounds
EIPs varied in their educational and professional backgrounds. Several EIPs believed these experiences influenced their work with families. For instance, Beau reported working in the field for just under a year and only had experience providing services via teleintervention. Flora had been working in EI for approximately 2 years but did not feel that her graduate-level education prepared her to actively involve caregivers in sessions. Throughout her program, she said the focus was “we model for the child, and we make suggestions to the parent, and that was about it.” She did not receive guidance on how to work with or coach caregivers. Phoebe indicated that she received her BA and attended webinars and conference presentations on EI topics but did not go into further detail about her training. Lauren was trained as an early childhood special educator, with several years of experience as a K–2 classroom teacher and professional experience in ABA. She described previous professional experiences in which she didn’t have opportunities to provide direct caregiver support,
. . . from the education background of the public school system and we never got to do [caregiver coaching], so I got a lot of the kids who were in Special Ed or Gen Ed not understanding a lot, not really at their age level expectation.
Teleintervention
EIPs had mixed experiences with implementing triadic strategies via teleintervention, with most EIPs reporting that teleintervention services limited their ability to adopt a triadic approach in some way. Specifically, they all shared that modeling strategies for caregivers was much more challenging to do over the screen. Phoebe and Flora also felt it was more difficult to establish a dyadic context and help the family set up dyadic activities. For instance, Flora believed that if she were in the family’s home, she could move about the house and join them in a variety of activities. By delivering services through a screen, she said,
I really think that the family has it in their head that we work at the table because I’m in a computer, so they want to set me on the table. I think it’s a little more stilted than if I was at the house.
Lauren also described challenges with teleintervention, although these were broader. She found that working with the family and trying to “maneuver and figure out how you’re supposed to do all this through a screen” was generally “nerve-wracking.” However, Beau thought teleintervention supported a triadic approach. They described the “benefit” of teleintervention as being that the caregivers “have to be the ones doing it if it’s happening.”
Strategy Use in Service Delivery
Descriptions of EIP and caregiver perspectives of triadic teleintervention service delivery inform their engagement with the implementation of the triadic strategies and participation in dyadic interactions. Consistent with EIPs’ low- to moderate-level changes in strategy use, caregivers described minor shifts in their EIPs’ service delivery, although they did note increases in EIPs’ focus on dyadic interactions and encouragement or suggestions provided for the caregivers. At least half of the EIPs described feeling that their use of triadic strategies increased more than what was reflected in the data. They surmised that this could be related to factors that cannot be quantified and described feeling increasingly more cognizant of how they were working with caregivers, beyond what was represented in the data displays. Such shifts were reflected in the EIPs’ strategy choice. Most EIPs demonstrated an increase in the use of Affirm Parent Competence and Focus Attention in intervention and maintenance phases compared with baseline.
Potentially Influencing Factors
Visual analysis of quantitative data showed a functional relation with low confidence between the intervention and EIP implementation of strategies with low to moderate increases in EIP behavior from baseline to intervention. Experimental control for EIP behavior was demonstrated for three of four participants. To some extent, participant responses to interview questions explained what may have contributed to or served as barriers to EIP use of triadic strategies, such as teleintervention and EIP training. EIPs held varying beliefs regarding teleintervention’s influence on their ability to work with caregivers meaningfully and effectively. For example, Lauren considered teleintervention to be a barrier to strategy use and reported feeling less comfortable with teleintervention at the end of the study compared to the beginning, which may have contributed to low experimental control in her data. All other participants noted an increase in comfort with this service delivery mode by the study’s end.
EIPs believed that their previous education, training, and professional roles contributed to their experiences with the intervention and with the implementation of the triadic strategies. While most EIPs were familiar with EI aims and the mechanisms of family-centered practice, none reported receiving formal training in supporting caregiver learning. Instead, they described learning discipline-specific, child-centered strategies for supporting child development in either classroom (early elementary) or therapy (speech, physical, behavioral) settings during their preservice education.
Discussion
This mixed-methods study contributes to a growing body of literature investigating multiple aspects of EI practice, including PD in EI (Fettig et al., 2016; Snyder et al., 2015) and supporting EIPs with adopting family-centered, capacity-building approaches in their work with families (Brown & Woods, 2015; Marturana & Woods, 2012; Meadan et al., 2020). Mixing methods allowed us to comprehensively understand how the intervention activities influenced multiple aspects of service delivery. There are limited single-case, mixed-methods studies that primarily focus on single-participant case studies and exist outside the field of education (e.g., Ramos & Ramos, 2019). To our knowledge, there are no published mixed-methods studies incorporating both qualitative and SCRD components as we did in the current study. Onghena and colleagues (2019) described this approach, which they call mixed-methods single-case research and defined it as “research in which single case experimental and qualitative case study methodologies, and their accompanying sets of methods and techniques, are integrated to answer research questions that concern one case” (Onghena et al., 2019, p. 462).
Consistent with previous research, a primary finding from this study suggested that a virtual training and coaching intervention supported modest increases in EIP use of triadic strategies (Brown & Woods, 2015; Fettig et al., 2016; Marturana & Woods, 2012; Meadan et al., 2020). Also, dyads demonstrated increased time spent interacting after EIPs were introduced to the intervention. This latter finding was shared by other studies investigating the use of a triadic approach during sessions, in which dyadic interactions were differentially affected by EIP use of strategies (Salisbury & Cushing, 2013). This was also supported by previous literature conceptualizing that a triadic approach to service delivery may increase dyadic interactions during sessions (McCollum & Yates, 1994; Yates, 2011), potentially providing caregivers with more competency-enhancing opportunities (Dunst & Espe-Sherwindt, 2016).
Triadic Strategies and Dyadic Interactions
Increases in EIPs’ use of the triadic strategies were most evident for three of the four EIPs. It is worth noting that for the remaining triad, an interpreter was present during sessions. A considerable amount of time was devoted to interpreting the caregiver and EIP speech during their sessions, potentially reducing the length and depth of the EIPs’ strategy use.
One important consideration with regard to how much time EIPs spend using triadic strategies is that of dosage. More specifically, how much time should EIPs spend focusing on facilitating dyadic interactions during sessions? While this has not yet been determined empirically, research examining the relationship between dyadic interactions, child outcomes, and home visit quality shows promise in approximating a guideline (Hughes-Belding et al., 2019; Raikes et al., 2006). In a study by Hughes-Belding et al. (2019), engagement in triadic strategies with a focus on child-related content (as determined by the Home Visit Observation Form-Revised [HVOF-R]) was associated with higher home visit quality components in practitioner behavior and family engagement. Raikes et al. (2006) investigated multiple home-visiting components and their effects on child outcomes nationally with families of 36-month-old children from 11 Early Head Start programs. Their findings suggest positive child outcomes are strongly supported when approximately 60% or more of session time focuses on dyadic interactions and child development content. In the current study, EIP time spent implementing triadic strategies and time spent in dyadic interaction reflect session content devoted to dyadic interactions and child development, like those measured by Raikes and colleagues (2006). When taken together, time spent focusing on triadic strategies and dyadic interactions reached a threshold of at least 60% of session time during all intervention phase sessions for Flora and Taryn (Triad 3) and Beau and Shannon (Triad 4) and select intervention sessions for Lauren and Jannie (Triad 1) and Phoebe and Jane (Triad 2). Additional research is needed to determine how much session time EIPs should aim to facilitate caregiver–child interactions to positively impact child and family outcomes. If we do adopt this 60% threshold as a guideline for an effective dosage of dyadic interaction and child development content, the current study shows promise in using PD in a triadic approach to reach this goal.
Also, as discovered through mixing methods, the specific strategies EIPs used during sessions changed throughout the study. To our knowledge, this is the first study examining an intervention incorporating a triadic approach using the six strategies presented in the PIWI framework (McCollum et al., 2001). McCollum and Yates (1994) describe these strategies as being on a continuum, moving from more indirect strategies with regard to dyadic interactions (e.g., Establish Dyadic Context) to those providing more direct support (e.g., Suggest). They encourage practitioners to scaffold their support to match the caregiver’s strengths, promote caregiver efficacy, and increase caregiver opportunities for learning. After being introduced to the intervention, most EIPs in this study shifted their practice to increase their use of triadic strategies found at the beginning of the continuum compared with more directive strategies, with potentially greater contributions to caregiver strengths and self-efficacy (McCollum and Yates, 1994). Caregivers noted this increase. Notably, this shift in EIP behavior to favoring less directive strategies may explain why select EIPs perceived marked increases in their overall use of triadic strategies. Providing practitioners in the field with PD in the triadic strategies may support them in becoming more intentional with how, when, and why they use caregiver coaching in their work (McCollum et al., 2001; Yates, 2011).
Participant Factors Influencing a Triadic Approach
This study explored factors that may have influenced EIPs’ implementation of the triadic strategies and caregiver-child interactions. One potential factor was that of the EIPs’ previous training and professional backgrounds. Each participant had a different background of experience and education, relating to their unique specializations. In addition, the majority of EIPs in this study held graduate degrees, which may not be representative of EIPs statewide or nationally. However, they consistently described preservice and PD experiences across disciplines that lacked content and practice opportunities specifically targeting caregiver coaching. These reports are consistent with previous research suggesting that EIP preparation programs and PD opportunities are often limited (Bruder, 2010) and lead to EIPs feeling insufficiently prepared to work with caregivers and children during sessions (Bruder et al., 2013; Douglas et al., 2020). To support practice recommendations provided by professional organizations (e.g., DEC, 2014) and personnel preparation standards (Council for Exceptional Children [CEC] & Division for Early Childhood [DEC], 2020), practitioners need training in family-centered, competency-enhancing practices they can implement with diverse families. Understanding how to maintain focus on caregiver-child interactions, offer caregivers positive feedback, and provide developmental information about their child are critical skills for supporting caregiver competence and confidence. EIPs across disciplines need training and coaching in the use of simple tools, such as triadic strategies, to effectively deliver these practices in teleintervention and in-person settings. Without training opportunities, practitioners may lack the considerable skill needed to develop a productive working alliance with caregivers and facilitate positive caregiver-child interactions during sessions (Roggman et al., 2016).
Limitations and Additional Implications for Research
There are limitations to note for this study. All research activities occurred during the COVID-19 pandemic. During this time, many families prioritized their health, safety, and livelihoods, and family-support professionals were navigating increased caseloads, new technology, and additional public health measures (Jones, 2020). Due to the virtual climate necessitated by the pandemic, all research activities occurred via videoconferencing platforms. This exclusive focus on teleintervention services allowed us to examine participant experiences with the triadic strategies delivered in a virtual setting only. EIPs expressed varying levels of comfort with teleintervention, ranging from feeling ineffective during sessions to finding that teleintervention helped the caregivers in their triad take on an active role in session activities. The latter perspective is especially consistent with a growing body of research in EI teleintervention service delivery, demonstrating its usefulness in providing more flexible support for caregivers (Ashburner et al., 2016) and emphasizing family-centered, capacity-building practices (Meadan et al., 2016). Additional research into the benefits of teleintervention would benefit the field, especially as programs increasingly regard it to be useful for service delivery (Poole et al., 2022; Schiariti & McWilliam, 2021).
Another limitation was the frequency and length of data collection. We embedded data collection into previously established family-EIP relationships. We asked EIPs to include children and families they planned to see weekly instead of monthly or biweekly, allowing us to collect data once each week for each triad. However, families often see each EIP biweekly or monthly as part of their regular, ongoing service delivery. Only including families receiving weekly sessions also excluded many triads from participating in this study. Future research could explore EIP and caregiver experiences with triadic strategy use when delivered less frequently (e.g., during twice monthly sessions), reflecting common service delivery rates. Also, we recognize the maintenance phase was not a sufficient length for determining a functional relation once the intervention was removed. Data collection for this study was collected for several months and was ultimately limited by multiple factors, including participants’ schedule constraints and researcher timelines. Finally, we sought to include EIPs who conducted teleintervention sessions with families in their homes. However, we acknowledge that the EIP participants in this study consisted of a variety of service providers (education, SLP, and OT) and therefore held field-specific knowledge that varied by their field. It is unclear if their different educational and professional backgrounds contributed to the variable results of this study.
Conclusion
This study aimed to contribute to the existing EI literature examining family-centered practices in ongoing EI service delivery. Critically, we investigated the efficacy of a training and coaching intervention for supporting EIP use of strategies and consequent changes in time spent in dyadic interactions. A mixed methods research design allowed for a more thorough understanding of the intervention’s effects than collecting quantitative or qualitative data in isolation. Our field continues to struggle with widespread acceptance and adoption of a family-centered approach to EI. We hope that our findings extend the field’s knowledge of how PD opportunities can support EIP strategies and dyadic relationships. We believe that providing EIPs with simple, applicable methods for enhancing child and family outcomes is crucial.
Supplemental Material
sj-docx-1-jei-10.1177_10538151231200777 – Supplemental material for Virtual Practitioner Training and Coaching of a Triadic Approach in Early Intervention: A Mixed-Methods Investigation
Supplemental material, sj-docx-1-jei-10.1177_10538151231200777 for Virtual Practitioner Training and Coaching of a Triadic Approach in Early Intervention: A Mixed-Methods Investigation by Shawna G. Harbin, Angel Fettig and Elizabeth M. Kelly in Journal of Early Intervention
Supplemental Material
sj-docx-2-jei-10.1177_10538151231200777 – Supplemental material for Virtual Practitioner Training and Coaching of a Triadic Approach in Early Intervention: A Mixed-Methods Investigation
Supplemental material, sj-docx-2-jei-10.1177_10538151231200777 for Virtual Practitioner Training and Coaching of a Triadic Approach in Early Intervention: A Mixed-Methods Investigation by Shawna G. Harbin, Angel Fettig and Elizabeth M. Kelly in Journal of Early Intervention
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.