
Abstract
The aim of this study is to adapt the Families in Early Intervention Quality of Life Scale (FEIQoL) into Turkish and determine its psychometric properties. Family members of 351 children with different types of disabilities participated in this study. During the adaptation process, confirmatory factor analysis determined that the factor structure was consistent with the original form. It was found that the criterion validity of the scale contained meaningful relationships with external criteria, and Cronbach’s alpha coefficient was calculated as .956 for the entire scale. Guttman’s split-half reliability supported the overall reliability of the scale, and item-total correlations indicated that the items adequately represented the scale as a whole. Significant differences between the mean scores of the lower and upper 27% groups revealed that the scale items had high discriminative power. In conclusion, the Turkish version of FEIQoL has been found to be a valid and reliable measurement tool.
Introduction
In recent years, the main focus in research examining the quality of life of children with disabilities has changed from being only the individual, and other family members have also started to be evaluated as a factor in quality of life. These approaches are inclusive approaches that aim to improve the environment rather than the individual, and research is conducted in collaboration with participants (Hsiao, 2018; Scott et al., 2008; Turnbull et al., 2004). The concept of family quality of life is considered as the continuous interaction and communication between groups of individuals connected to each other by a social system (I. Brown, 2003), and is defined as “the conditions in which the needs of the family are met, family members enjoy living together as a family and have the opportunity to do activities that are important to them” (Turnbull et al., 2000; cited in Park et al., 2003). While disability is seen as a risk factor for family well-being in families with children with disabilities, the increased roles and responsibilities of family members are an additional stressor (Gardiner & Iarocci, 2012; Petalas et al., 2012). In this context, family quality of life has begun to be seen as an important outcome of the support services provided for families of children with developmental delays or disabilities who are at risk (McWilliam, 2010; Summers et al., 2007).
In early childhood interventions, the family quality of life approach places the family at the center of the process, ensuring that goals are based on families’ strengths and perceived needs (McWilliam, 2010; Park et al., 2003). Theoretically, family quality of life shaped by family dynamics, individual characteristics, the support and services provided, and the interaction between policies and programs, therefore, has the potential to be effective on family quality of life (García-Grau et al., 2019).
Studies in this field aim to reveal information about how various areas of life are affected by the participation of the child with disability in the family and what family members’ perceptions of family life are (R. I. Brown et al., 2006). Various tools such as Beach Center Family Quality of Life Scale (BCFQoL) (Hoffman et al., 2006; Meral & Cavkaytar, 2013), Family Quality of Life Questionnaire (R. I. Brown et al., 2006; Isaacs et al., 2007), Spanish Family Quality of Life Scale (Giné et al., 2013) are used nationally and internationally to assess family quality of life. In addition to these measurement tools, the systematic review conducted by Francisco Mora et al. (2020) also stated that the most frequently used measurement tools to assess family quality of life in the literature include the Autism Family Experience Questionnaire (Leadbitter et al., 2018), the ITP-Child Quality of Life Questionnaire (Barnard et al., 2003), and the Family Early Intervention Quality of Life Scale (FEIQoL; McWilliam & Casey, 2013).
The scale developed by McWilliam and Casey (2013), which was renamed as Families in Early Intervention Quality of Life-FEIQoL to avoid confusion with the BCFQoL also includes the child’s functionality (participation) unlike the others. In this context, the FEIQoL scale will be adapted into Turkish to assess the perceptions of families regarding the quality of life of Turkish children aged 3 to 6 who have been diagnosed early and receive special education services, considering their functionality in their daily routines, and examined in terms of some variables related to the family. The version translated by McWilliam and Casey (2013) showed valid and reliable psychometric properties in examining the quality of life perceptions of Spanish families receiving early intervention (García-Grau et al., 2019).
There are several reasons for selecting this measurement tool. First, the FEIQoL scale contains the “Child’s Functioning” factor, which includes the child’s comprehension/expression, peer relationships, participation in routines, independence, and behavior. Child functioning (participation) was found to be an important determinant of family quality of life, and the quality of life scores of families of children with different types of disabilities differed (R. I. Brown et al., 2006). Another reason is that it focuses on families with children aged 0 to 6 and can be reliably used, particularly in the context of early intervention for children with disabilities. Furthermore, the factor structure has been examined using various methods, such as Rasch analysis, across different samples and contexts, including Spanish versions (Frugone-Jaramillo & Gràcia, 2023; García-Grau et al., 2021, 2024; Subiñas Medina et al., 2022; Vilaseca et al., 2025). There are few reliable measurement tools in Turkiye that serve a similar multi-purpose use. Furthermore, when evaluating the appropriateness of the adaptation process for this tool, which has been tested many times before in different populations, it was considered that it provides a more scientifically sound starting point. This is because existing systematic reviews and scoping review studies summarize the FEIQoL scale’s place in the context of early intervention, revealing its strong theoretical framework (Alnahdi et al., 2022; Francisco Mora et al., 2020).
In summary, FEIQoL is a critical tool for focusing early intervention processes on a family-centered structure rather than a child-centered approach. It measures the child’s independence, participation, and social relationships in daily routines as an indicator of the family’s perceived quality of life. Its focus on the early intervention stage and natural settings ensures that planning is sensitive to families’ real-life circumstances. Also, it covers not only families of children with disabilities, but also families of children with developmental delays or at risk, and allows for service-delivery-based assessment rather than medical diagnosis (García-Grau et al., 2019, 2021).
Moreover, to evaluate family-focused assessment tools such as FEIQoL in the Turkish context and to carry out adaptation studies, it is considered important to take into account the current structure of the early intervention system in Turkiye. Special education services in Turkiye are carried out in accordance with Decree Law No. 573 on Special Education. This decree explains the basic principles of special education, diagnosis, placement, education levels, inclusion, education in special education schools, special education support, education programs, and evaluation processes (Sak et al., 2020). In addition, the Special Education Services Regulation, updated in 2018, contains principles regarding the continuation of early childhood services for children with special needs from birth to 36 months, including informing and supporting the family. Furthermore, for those who have completed 36 months, the principle is that they should continue their education through integration/inclusion (Ministry of National Education, 2018).
In Turkiye, early childhood special education services are primarily provided within the framework of inclusive education. Under this model, children are educated alongside their peers, while parents are informed and supported throughout the process. Although services can be provided in school, institutions, or home settings, the inclusive education model is the primary approach. However, due to a shortage of specialists, challenges in interagency collaboration, and the limited availability of evidence-based interventions, a comprehensive model for early childhood special education has not yet been established (Tomris & Çelik, 2022).
Educational activities are typically provided through center-based special education and rehabilitation institutions, in the form of approximately 40-min sessions held twice a week (Ministry of National Education, 2018). Consequently, the limited availability of inclusive preschool environments leads to the vast majority of children receiving support either at home or in special education institutions. This situation differs from that of countries such as the United States, where early interventions are based on home-based and inclusive programs. In Turkiye, despite legal regulations, a lack of assessment tools and qualified personnel limits the widespread and inclusive provision of these services (Diken et al., 2012; Tomris, 2020; Tomris et al., 2022). Furthermore, parents with children with disabilities are more vulnerable to physical and mental problems and have a lower quality of life (Akoğlu et al., 2018; Şipoş et al., 2012). At this point, it is necessary to understand the current situation to improve services and strengthen various mechanisms. According to data from the Ministry of Family and Social Services (2023), 33,185 children aged 0 to 4 and 91,059 children aged 5 to 9 in Turkiye hold disability health reports. This situation highlights that early diagnosis and intervention affect many people and underscores the multifaceted support needs of families during the preschool period. Therefore, assessing the quality of family life is of critical importance.
The FEIQoL scale, based on self-reports from family members, is an important tool for understanding experiences of families with children with disabilities. This adaptation contributes to the development of policies and practices aimed at strengthening family support. It also provides evidence-based grounds for policymakers by enabling a more accurate identification of family needs. So, it was aimed to adapt the FEIQoL scale into Turkish by conducting a validity and reliability study. The sub-objectives created in line with this purpose are as follows:
What is the validity and reliability level of the Turkish version of the FEIQoL scale?
How is the factor structure of the Turkish version of the FEIQoL scale?
Method
Research Design
This study is a methodological research designed to examine the psychometric properties of the Turkish version of the FEIQoL scale through validity and reliability analyses. The methodological research model refers to the psychometric study process in scale adaptation studies to adapt a measurement tool to different cultures and languages (Hambleton & Patsula, 1998).
Participants
To adapt the FEIQoL scale into Turkish, family members of children aged 3 to 6 years with both medical and educational diagnoses and receiving special education services were included in the study by random sampling method. Different opinions have been put forward about the sample size expected to be reached to conduct multivariate analyses such as factor analysis in validity studies of measurement tools, but as Büyüköztürk (2014) and Tavşancıl (2018) state, it is considered sufficient to be at least 5 to 10 times the number of observed variables, that is, the number of items, which is 40 for this scale. In this study, 351 family members of children with disabilities participated voluntarily. This sample was accessed through professionals working in special education and rehabilitation centers and private institutions that serve early childhood groups. The research announcement was communicated to families primarily through face-to-face meetings and internal briefings within institutions, as well as through social media posts, thus creating a natural information-sharing process disseminated through these institutions. Approximately 18 of these institutions actively contributed to the data collection process, enabling access to families who volunteered for the study. Families completed the online or printed form provided by the researchers entirely on a voluntary basis and independently. In addition, a pilot study was conducted to test the clarity and applicability of the translated items before collecting data from the main study group. The participants in the pilot study were not included in the main study; the final study group consisted only of families who participated in the primary data collection phase after the pilot study. Demographic characteristics of the participants are summarized in Table 1.
Participant Demographics.
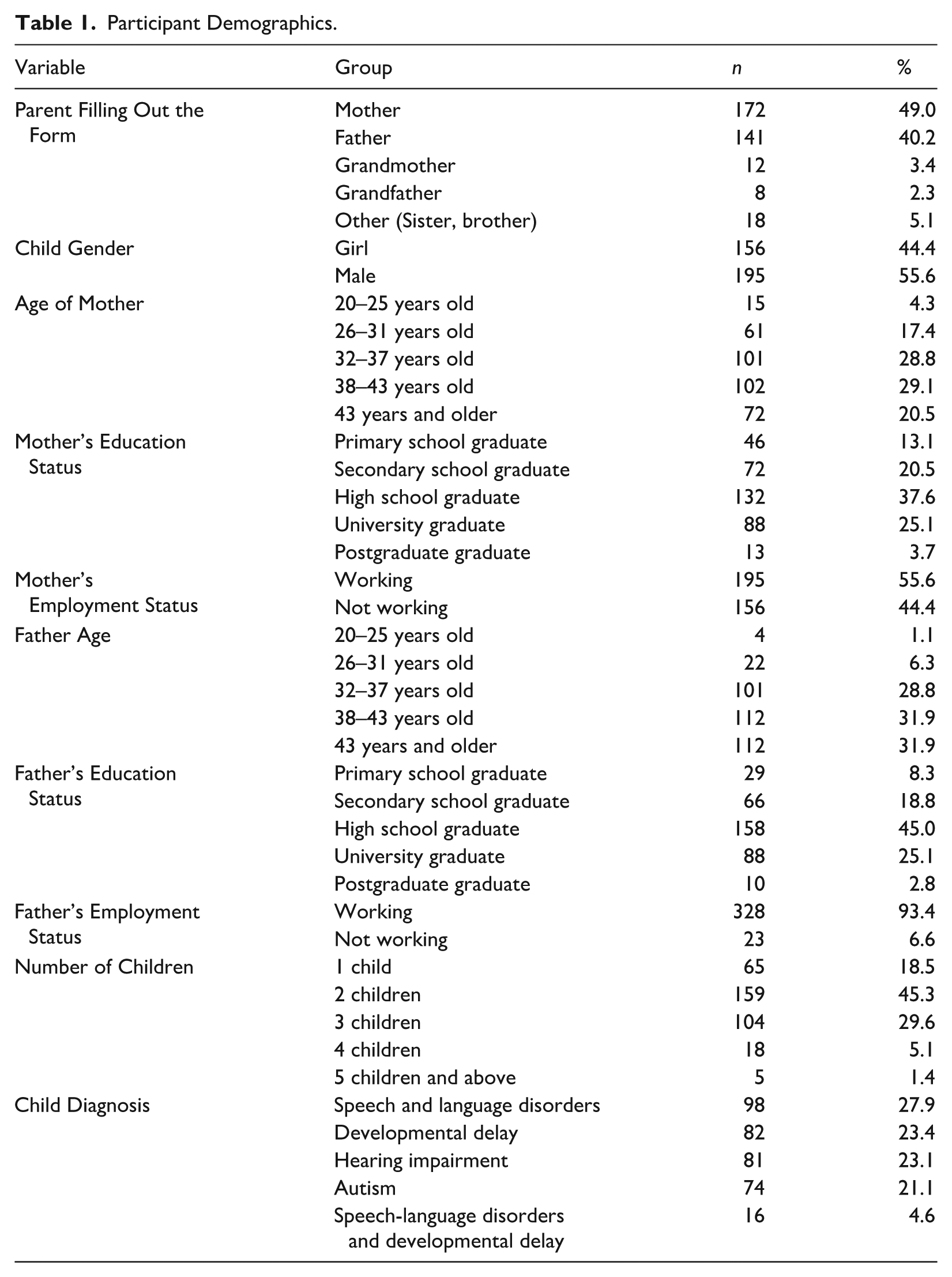
The forms related to the study were primarily completed by mothers and fathers. The gender distribution of the children shows a balanced representation of girls and boys. Most families have two or three children. The most common diagnoses among the children are speech and language disorders, developmental delay, hearing impairment, and autism; some children have multiple diagnoses. The participating children are educated in different educational settings (see Table 2).
Types of Schools Children Attend.
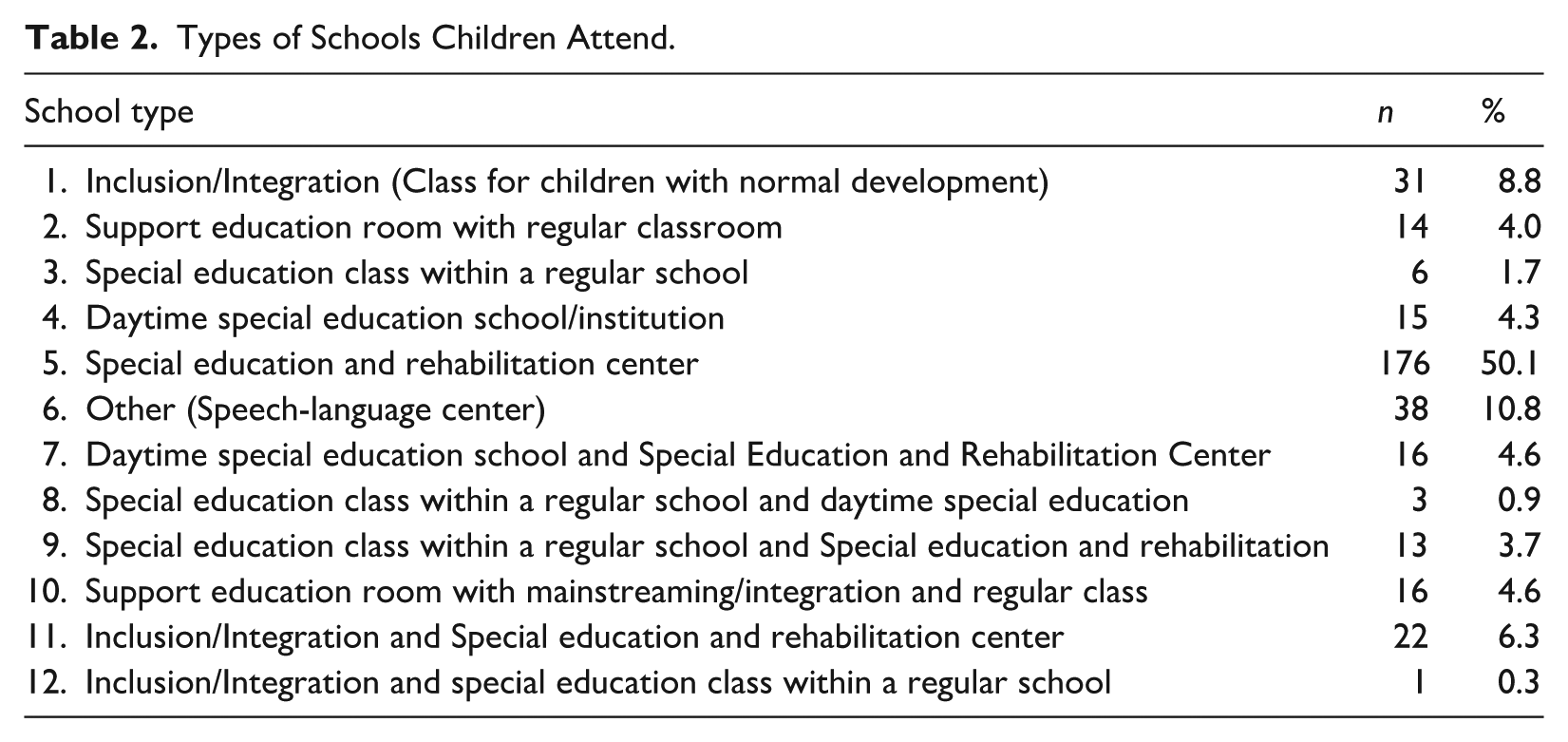
The most represented school type is special education and rehabilitation centers, where 50.1% of children attend. This is followed by speech and language centers (10.8%) and mainstreaming/integration classrooms (8.8%). In addition, some children received services from more than one educational setting. For example, 6.3% attended both an inclusive class and a special education and rehabilitation center, while 4.6% attended a daytime special education institution and a rehabilitation center simultaneously. Other less common combinations are mixed service models that combine a special education classroom with a support education room or a speech and language center.
Data Collection Tools
Personal Information Form
This form prepared by the researchers was used to gather demographic information about the family and the child. Some of the demographic information included in the form are the identity of the family member who filled out the form, the age of the parents, the educational level of the parents, the age of the child, the type of disability, and the gender of the child.
Families in Early Intervention Quality of Life Scale
In this study, the FEIQoL scale developed by McWilliam and Casey (2013) was used to assess the quality of life of families benefiting from early intervention services. This scale focuses on families of children aged 0 to 6 who are disabled, have developmental delays, or are at risk of developmental delays in the context of early intervention. Unlike many measurement tools, it includes statements designed to assess families’ functionality in their natural environments and daily routines. The scale, which consists of 40 items in total, is scored on a 5-point Likert-type scale (1 = poor, 5 = excellent). The original form of the scale has a four-factor structure: (1) Family Relationships (FR) (α = .87), (2) Access to Information and Services (AIS) (α = .82), (3) Child Functioning (CF) (α = .87), and (4) Overall Life Situation (OLS) (α = .79). In the original study, Cronbach’s alpha internal consistency coefficient was reported as .89. In this study, it was calculated as .905, .860, .909, .813, and .956 for Family Relationships, Access to Information and Services, Child Functioning, Overall Life Situation and the total scale score, respectively. In addition, the Guttman split-half reliability coefficient of the scale was found to be .844.
Beach Center Family Quality of Life Scale
In this study, the BCFQoL Scale developed by Hoffman et al. (2006) was used to assess the quality of life levels of families. The Turkish adaptation was done by Meral and Cavkaytar (2013). The scale aims to assess the quality of life of families of individuals with intellectual and/or developmental disabilities in a multidimensional way. The scale consists of a total of 25 items and is scored on a 5-point Likert-type scale (1 = strongly disagree, 5 = strongly agree). The scale addresses family quality of life in five basic dimensions. These dimensions include Family Interaction (FI), Parenting (P), Emotional Wellbeing (EW), Financial/Physical/Material Competence (FPMC), and Disability Related Support (DRS). In the original study of the scale, Cronbach’s alpha values for the sub-dimensions were reported to be between .88 and .94 and .93 for the total scale. In this study, Family Interaction, Parenting, Emotional Wellbeing, Financial/Physical/Material Competence, Disability Related Support, and total scale score were 0.848, 0.814, 0.748, 0.748, 0.772, 0.830, and 0.915, respectively.
Translation and Cultural Adaptation Process
In ensuring the linguistic and cultural validity of the FEIQoL scale, the adaptation process was continued by taking into account the guidelines (Beaton et al., 2000) recommended for cross-cultural scale adaptation. In addition, the translation process of the measurement tool was carried out through a multi-stage, expert-based process to ensure semantic and conceptual equivalence between the English and Turkish versions. First, the first two authors of the study held multiple research meetings and collaboratively performed the initial translation of all items from English to Turkish. The translated draft was then evaluated by an academic teaching English at a university’s School of Foreign Languages, and feedback was obtained on linguistic accuracy and conceptual appropriateness. Based on these notes, the first two authors held a revision meeting and made the necessary changes to ensure consistency with the terminology used in the relevant literature. This updated version was reviewed by an English teacher whose native language is Turkish, who lives in Europe, holds a degree in English Language and Literature, and teaches English at an international kindergarten. The comments obtained from this source were again discussed in online meetings, and revisions were made when the authors reached consensus on the items.
The final linguistic and conceptual review was conducted by a faculty member with a PhD in Child Development and academic experience. This feedback was received in writing, and following the revisions based on these suggestions, expert opinions were sought from a professor, an associate professor, and two PhD-level experts in early intervention and child development. The final version was developed based on written feedback on each item from an expert whose native language is Turkish and whose field of work is early childhood, currently serving as an academic in the field of developmental psychology at a university in Germany. All these expert opinions were discussed by the research team, and revisions based on consensus were made to create the final Turkish version of the tool. Regarding the adjustments made until the measurement tool reached its final form, translation difficulties, cultural adaptations, and the reasons for changes at the item level have been compiled in a table (see Appendix). Although the translation process involved a comprehensive expert review, parents were not asked to directly evaluate the translated items for clarity, cultural appropriateness, or sensitivity. Cognitive debriefing interviews with caregivers were not conducted during the adaptation phase; however, the final form was applied to a separate group from the sample during the pilot study, and its statistical adequacy was examined.
Data Collection Process
First, written permission for the use of the scale was obtained from the relevant researchers and then the necessary ethics committee approval was obtained with the decision of Toros University Scientific Research and Publication Ethics Committee dated March 21, 2024, and numbered 61. A pilot test was conducted with 50 family members to evaluate the comprehensibility of the form. During the pilot test, family members reviewed the items and communicated the incomprehensible items to the researchers. In the pilot study, 90% of those who filled out the form were mothers, 8% were fathers, and 2% were other (brother, sister). When the diagnoses of the children were analyzed, 38% had speech and language disorder, 16% had developmental delay, 2% had hearing impairment, 42% had autism, and 2% had speech and language disorder and developmental delay. The item-total test correlation values of the participants’ answers to the scale questions were examined, and it was determined that there were no items below 0.30. The item-total test correlation values of all items vary between 0.325 and 0.807. In addition, when the results of the reliability analysis were analyzed, it was found that the FEIQoL was a highly reliable scale with a Cronbach’s alpha coefficient of .947. In addition, the sub-dimension reliabilities were found to be in the range of .790 to .896. After the pilot test, the Turkish version of the scale was finalized and the data collection phase started. Participants in the pilot study, which was conducted to test the clarity and feasibility of the translated items before data collection in the main study group, were not included in the main study, the final study group consisted only of families who participated in the primary data collection phase after the pilot study.
Collaborated with the managers of the institutions for the participation of the families included in the study group. Relevant staff at the institutions (usually institutional psychologists) identified eligible families and contacted them to provide detailed information about the purpose and procedures of the study. Family members who agreed to participate were invited to the institutions and asked to sign informed consent forms indicating their voluntary participation. However, some family members living in different cities and contacted through institutions received the survey instruments online. Likewise, these families were also asked to approve the informed consent form indicating their voluntary participation. Parents are the primary responder; however, in situations where parents are unavailable (e.g., due to work commitments, health-related restrictions, or the transfer of caregiving responsibilities within the household), other adult family members who are the child’s primary caregivers (such as grandmother, grandfather, etc.) have completed the form. These individuals are over the age of 18 and are directly involved in the child’s daily care. However, regardless of who completed the survey, collecting demographic information about the parents in the household was found to be more consistent with the theoretical framework of our study. This is because the study is based on presenting the family structure in which the child lives and the characteristics of the parents. Therefore, the demographic questions on the form aim to obtain information about the child’s mother and father. If the person completing the survey was not one of the parents, they were asked to provide this information about the parents.
Data Analysis
In this study, the SPSS 26 software package and R 4.4.2 (R Core Team, 2024) were used for data analysis. First of all, an independent samples t-test was used to determine whether there was a significant difference between online (n = 34) and face-to-face (n = 317) data collection methods in terms of FEIQoL total scores and BCFQoL total scores. According to these analysis results, there was no significant difference in FEIQoL total scores between face-to-face and online responses, with t(349) = 1.23, p = .22; the mean difference was 5.51 and the 95% confidence interval was between −3.31 and 14.34. Similarly, there was no significant difference in BCFQoL total scores between the two groups, with t(349) = −0.49, p = .62; the mean difference was −1.18, with a 95% confidence interval ranging from −5.92 to 3.55. Therefore, analyses were conducted by combining the two groups for both measurement tools.
Subsequently, the distributions of the variables in the data set were examined; since the skewness and kurtosis values remained within the range of ±2, it was evaluated that the data were suitable for parametric analysis (George & Mallery, 2010). Within the scope of descriptive statistics, mean, standard deviation, skewness and kurtosis values of the scales were calculated.
Cronbach’s alpha coefficients and Guttman’s two-half reliability coefficient were calculated to determine the internal consistency level of the scales. In addition, corrected item-total correlations and explained variance ratios were reported for each item. Confirmatory factor analysis (CFA) was conducted to test the construct validity of the FEIQoL scale. Multiple fit indices such as χ2/df ratio, CFI, GFI, RMSEA, and SRMR were used to evaluate model fit.
To assess criterion-related validity, the relationships between the FEIQoL scale and the Beach Center Family Quality of Life Scale were examined with Pearson correlation analysis. The significance level was accepted as .05 in the analyses, and Bonferroni correction was applied in multiple comparisons to reduce the risk of Type I error.
Results
When the descriptive statistics of the two main scales used in the study, namely the FEIQoL and the BCFQoL and their sub-dimensions are examined, it is seen that the averages for both scales are at a medium-high level and the distributions are close to a normal distribution.
The total score of the FEIQoL was 121.98 (SD = 24.89), and the scores of the sub-dimensions FEIQoL (FR) (M = 36.58), FEIQoL (AIS) (M = 35.14), FEIQoL (CF) (M = 31.31) and FEIQoL (OLS) (M = 18.95) were distributed consistently with the structure of the scale. The skewness and kurtosis values of the scale were within ±2 limits, indicating conformity with normal distribution (George & Mallery, 2010). The total score of the BCFQoL was calculated as 92.93 (SD = 13.33); the scores of the sub-dimensions BCFQoL (FI) (M = 23.29), BCFQoL (P) (M = 22.95), BCFQoL (EW) (M = 13.97), BCFQoL (FPMC) (M = 18.58), and BCFQoL (DRS) (M = 14.14) were observed at a similar level. The skewness and kurtosis values of the scale were within the limits of ±2, indicating conformity with normal distribution (George & Mallery, 2010).
In general, the score distributions of the scales used in the study conform to the normal distribution and provide a structure suitable for conducting parametric analyses. The mean and standard deviation values show that the quality of family life perceived by the sample is evenly distributed on the basis of dimensions (see Table 3).
Descriptive and Inferential Statistics for Research Variables.
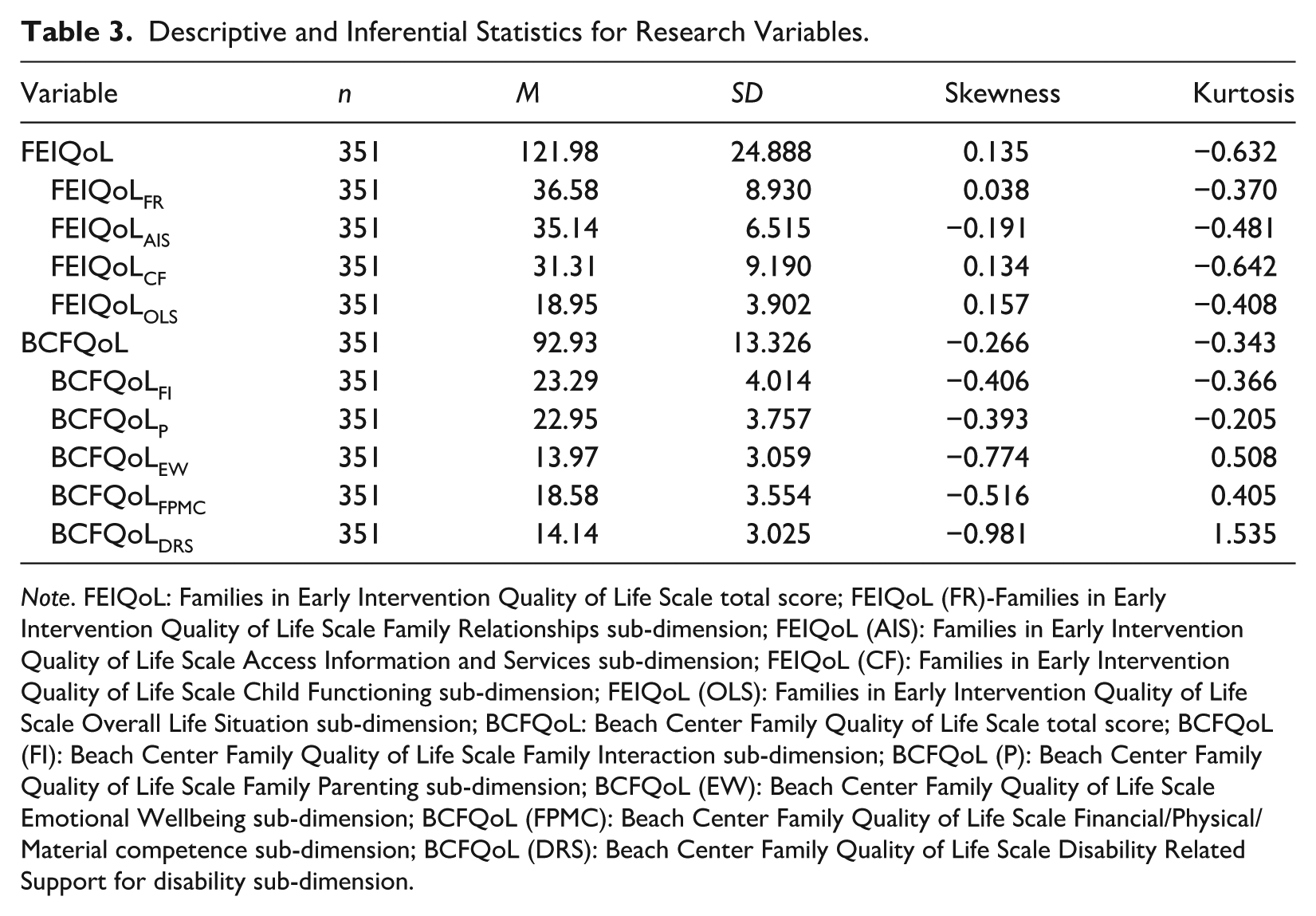
Note. FEIQoL: Families in Early Intervention Quality of Life Scale total score; FEIQoL (FR)-Families in Early Intervention Quality of Life Scale Family Relationships sub-dimension; FEIQoL (AIS): Families in Early Intervention Quality of Life Scale Access Information and Services sub-dimension; FEIQoL (CF): Families in Early Intervention Quality of Life Scale Child Functioning sub-dimension; FEIQoL (OLS): Families in Early Intervention Quality of Life Scale Overall Life Situation sub-dimension; BCFQoL: Beach Center Family Quality of Life Scale total score; BCFQoL (FI): Beach Center Family Quality of Life Scale Family Interaction sub-dimension; BCFQoL (P): Beach Center Family Quality of Life Scale Family Parenting sub-dimension; BCFQoL (EW): Beach Center Family Quality of Life Scale Emotional Wellbeing sub-dimension; BCFQoL (FPMC): Beach Center Family Quality of Life Scale Financial/Physical/Material competence sub-dimension; BCFQoL (DRS): Beach Center Family Quality of Life Scale Disability Related Support for disability sub-dimension.
Validity
Construct Validity
Confirmatory Factor Analysis
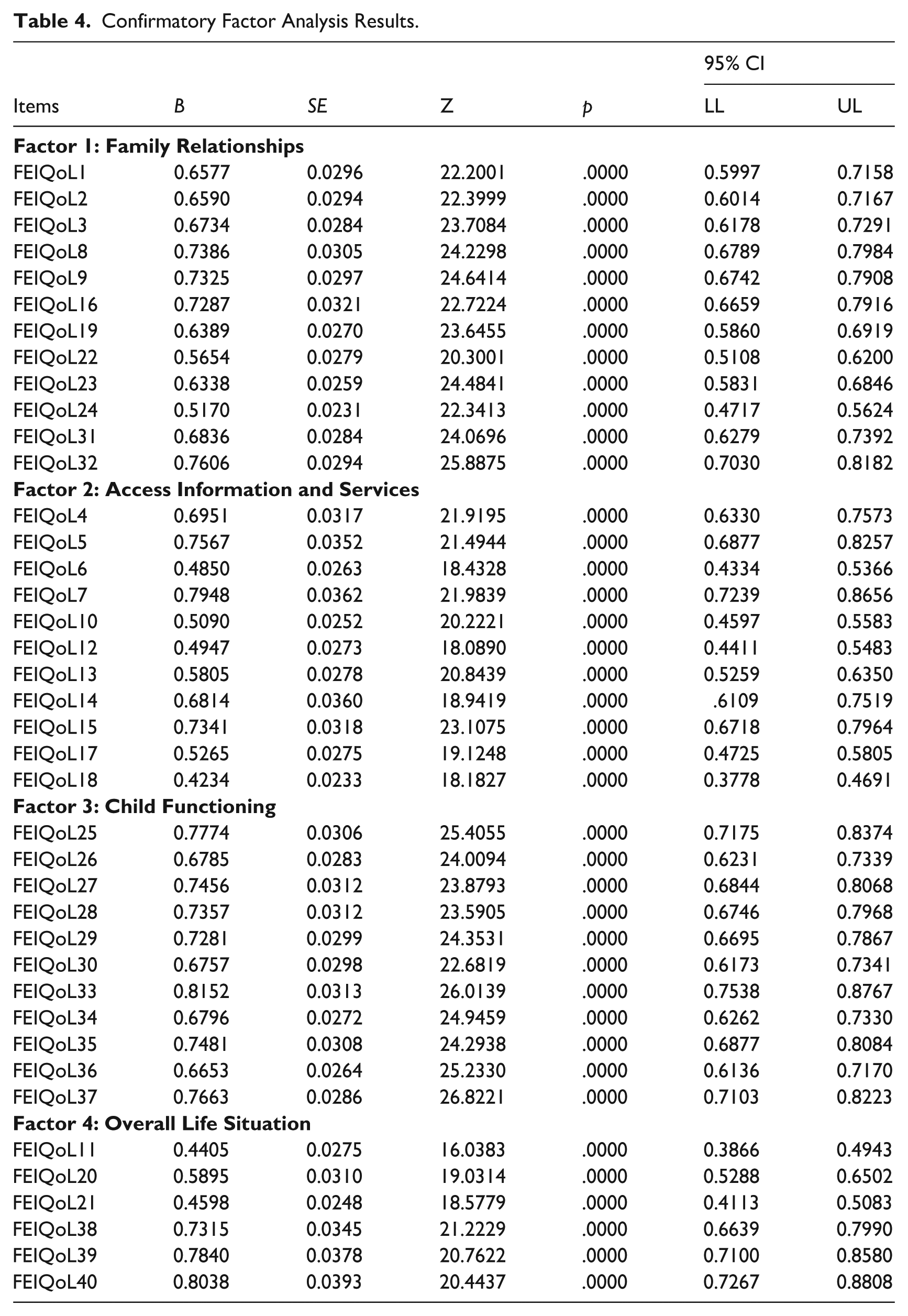
As a result of the analysis, χ2(734. n = 351) = 1,275.07, χ2/SD = 1.7371, RMSEA = 0.0493, SRMR = 0.0747, CFI = 0.9892, GFI = 0.9689, it was determined that the goodness of fit indices and parameter values of the related scale were at acceptable levels according to Hu and Bentler (1999) and Schermelleh-Engel et al. (2003). The standardized factor loadings of all items on the relevant factors ranged from .48 to .84 and all were statistically significant (p < .001). This shows that the power of each item to represent the relevant factor is sufficient. The highest factor loading belongs to FEIQoL33 (0.8152) and the lowest factor loading belongs to FEIQoL6 (0.4850). No post hoc model re-specifications were implemented based on modification indices. The model was tested based entirely on the theoretical structure. The path coefficients and z values for the Confirmatory Factor Analysis are presented in Table 4. Confirmatory factor analysis standardized factor loadings are also presented in Figure 1.
Confirmatory Factor Analysis Results.
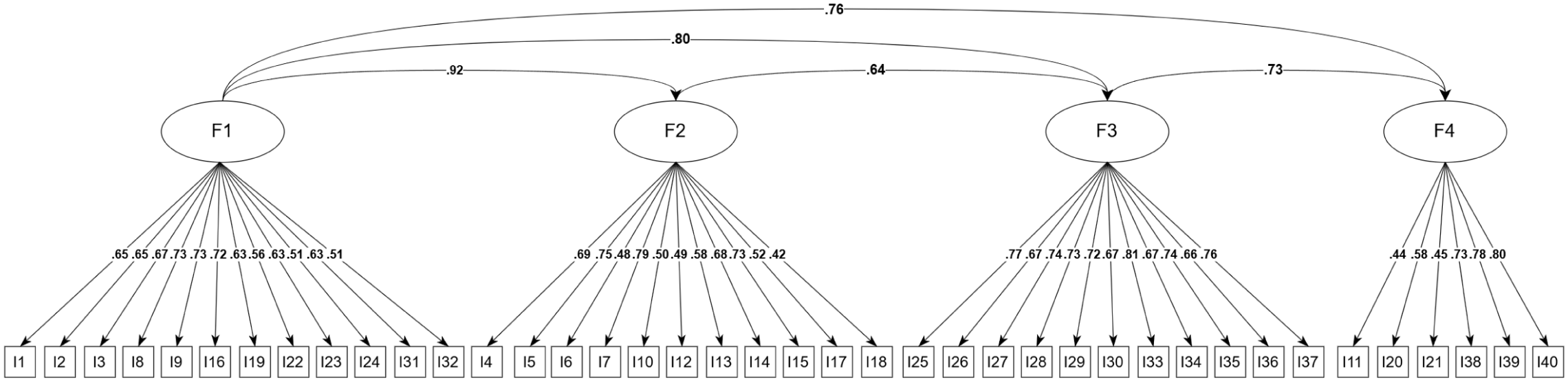
Confirmatory factor analysis standardized factor loadings.
Criterion-Related Validity
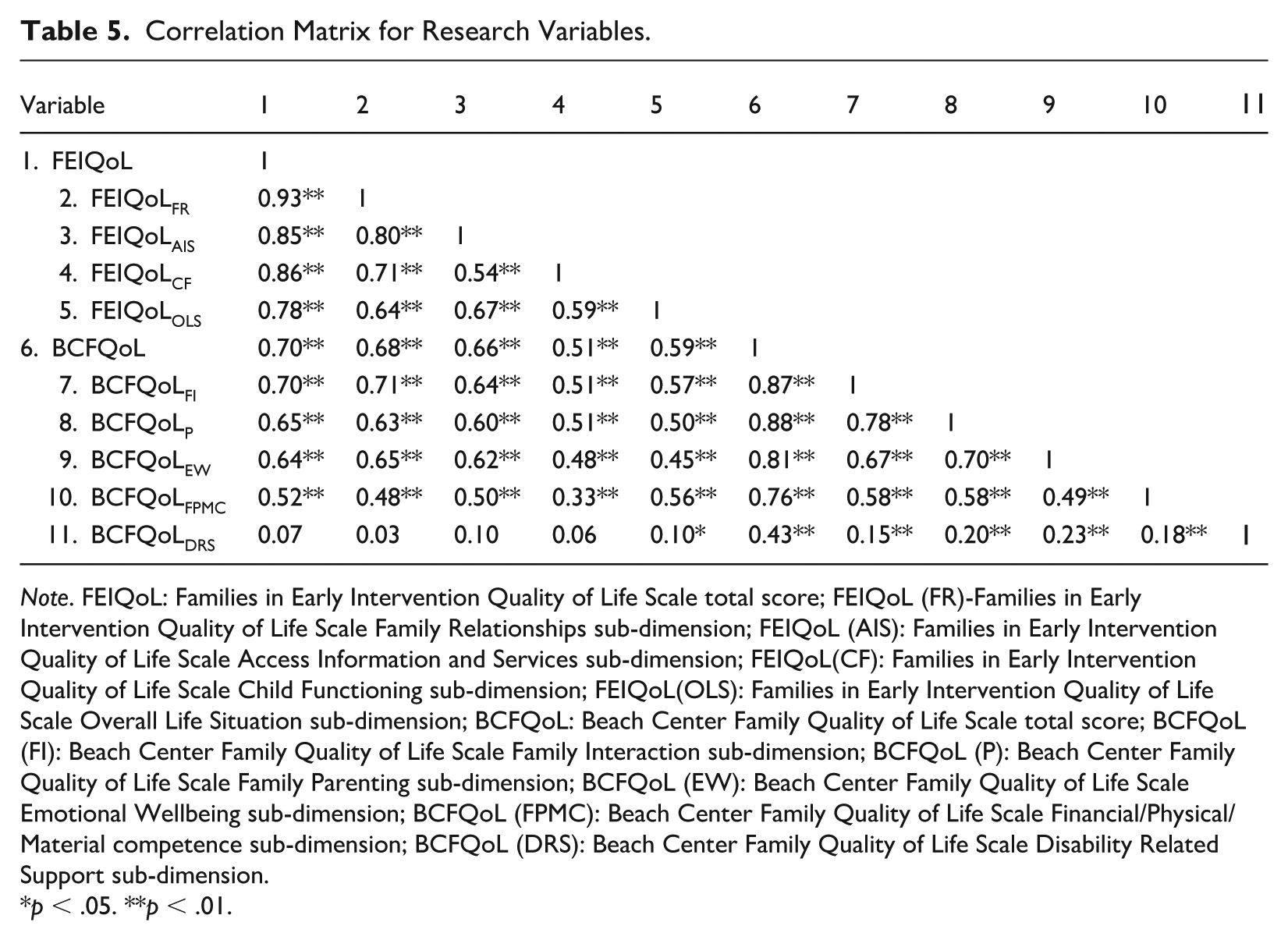
In this study, the criterion-related validity of the FEIQoL was tested through the relationships with the BCFQoL. For this purpose, the relationships between the total scores and sub-dimensions of both scales were analyzed by Pearson correlation analysis. The results of the analysis revealed that there was a significant positive correlation between the total scores of FEIQoL and BCFQoL (r = .70, p < .01) (see Table 5).
Correlation Matrix for Research Variables.
Note. FEIQoL: Families in Early Intervention Quality of Life Scale total score; FEIQoL (FR)-Families in Early Intervention Quality of Life Scale Family Relationships sub-dimension; FEIQoL (AIS): Families in Early Intervention Quality of Life Scale Access Information and Services sub-dimension; FEIQoL(CF): Families in Early Intervention Quality of Life Scale Child Functioning sub-dimension; FEIQoL(OLS): Families in Early Intervention Quality of Life Scale Overall Life Situation sub-dimension; BCFQoL: Beach Center Family Quality of Life Scale total score; BCFQoL (FI): Beach Center Family Quality of Life Scale Family Interaction sub-dimension; BCFQoL (P): Beach Center Family Quality of Life Scale Family Parenting sub-dimension; BCFQoL (EW): Beach Center Family Quality of Life Scale Emotional Wellbeing sub-dimension; BCFQoL (FPMC): Beach Center Family Quality of Life Scale Financial/Physical/Material competence sub-dimension; BCFQoL (DRS): Beach Center Family Quality of Life Scale Disability Related Support sub-dimension.
p < .05. **p < .01.
Significant and positive relationships were also observed between FEIQoL (FR) and BCFQoL (r = .68, p < .01), between FEIQoL (AIS) and BCFQoL (r = .66, p < .01), between FEIQoL (CF) and BCFQoL (r = .51, p < .01), and between FEIQoL (OLS) and BCFQoL (r = .59, p < .01). In addition, significant and positive correlations were observed between FEIQoL (FR) and BCFQoL(FI) (r = .71, p < .01), BCFQoL (P) (r = .63, p < .01), BCFQoL (EW) (r = .65, p < .01) and BCFQoL (FPMC) (r = .48, p < .01); between FEIQoL (AIS) and BCFQoL (FI) (r = .64, p < .01), BCFQoL (P) (r = .60, p < .01), BCFQoL (EW) (r = .62, p < .01), BCFQoL (FPMC) (r = .50, p < .01); between FEIQoL (CF) and BCFQoL (FI) (r = .51, p < .01), BCFQoL (P) (r = .51, p < .01), BCFQoL (EW) (r = .48, p < .01), BCFQoL (FPMC) (r = .33, p < .01); between FEIQoL (OLS) and BCFQoL (FI) (r = .57, p < .01), BCFQoL (P) (r = .50, p < .01), BCFQoL (EW) (r = .45, p < .01), BCFQoL (FPMC) (r = .56, p < .01).
However, no significant correlation was found between BCFQoL (DRS) and FEIQoL (r = .07, p > .05), FEIQoL (FR) (r = .03, p > .05), FEIQoL (AIS) (r = .10, p > .05) and FEIQoL (CF) (r = .06, p > .05). Only the relationship with the FEIQoL (OLS) was found to be significant at a low level (r = .10, p < .05).
Reliability and Item Analysis
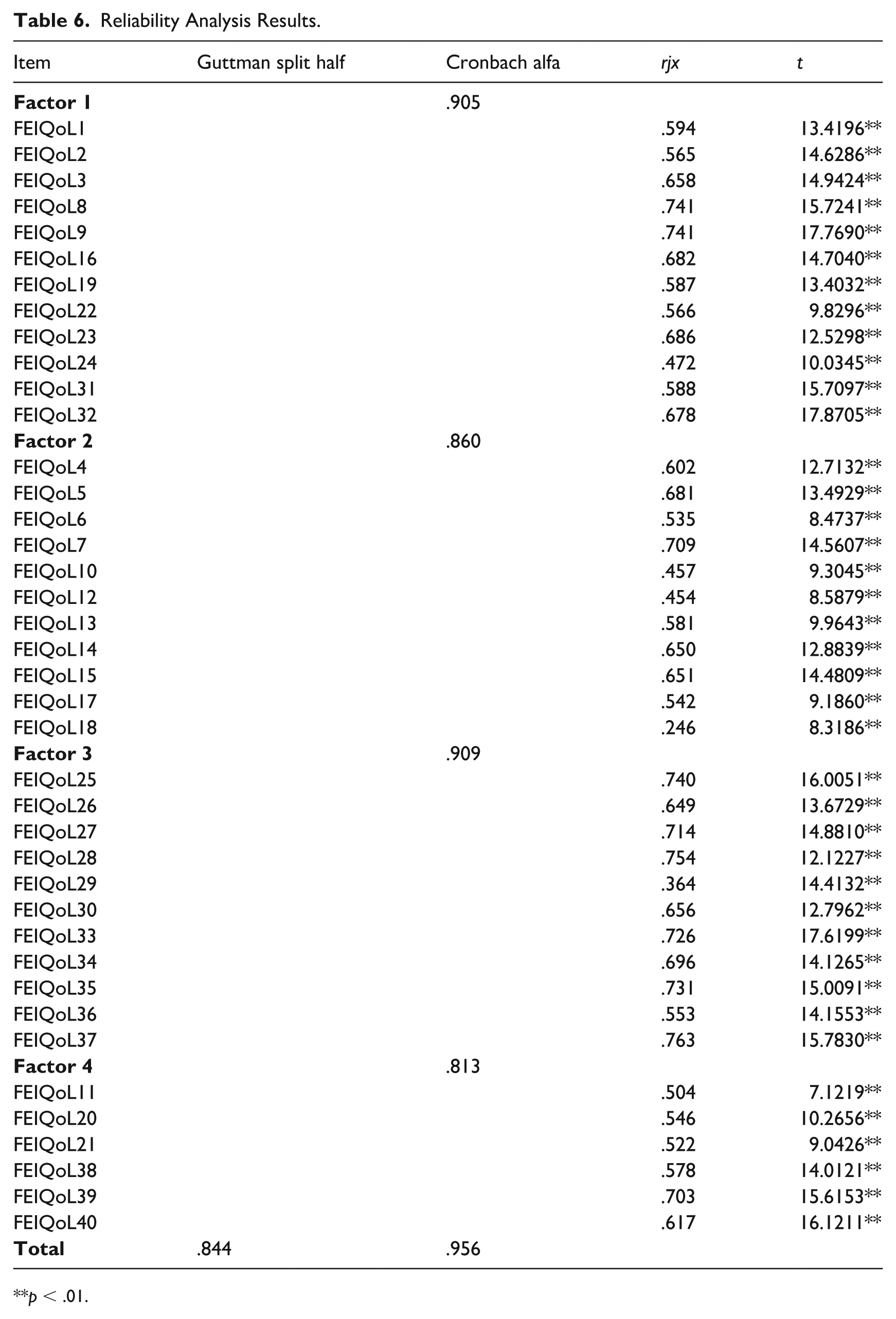
Cronbach’s alpha coefficients, Guttman’s two-half reliability coefficient, corrected item-total correlations (rjx), and independent samples t-tests between the lower and upper 27% groups were analyzed to assess the internal consistency and statistical relevance of the scale at the item level (see Table 6).
Reliability Analysis Results.
p < .01.
The findings of the reliability analyses indicate that the four factors and the total scale score have a high level of internal consistency. Cronbach’s alpha coefficient for the whole scale was calculated as .956. This value shows that the overall scale has a good level of internal consistency. In addition, Guttman’s two-half reliability coefficient was found to be .844, which shows that the scale yields similar results when divided into two halves and exhibits a stable structure. In the evaluations made at the sub-factor level, Cronbach’s alpha value of the first factor was calculated as .905, the second factor as .860, the third factor as .909 and the fourth factor as .813. These values indicate that each factor has a high level of reliability. The corrected item-total correlation values of all items were largely above 0.40. The t-tests between the lower and upper 27% groups produced statistically significant differences for all items (t values between 7.12 and 17.87, p < .001), thus confirming that each item contributed significantly to the scale score.
Discussion
Nowadays, it is important to support family-based practices for children with disabilities and to present factors related to ensuring the quality of life of families with cultural sensitivity to support children. However, there are only a limited number of measurement tools available for assessing the quality of family life, which is beginning to be seen as an important result of the support services provided to families of children with disabilities in Turkiye. Therefore, this study aims to adapt the Turkish version of the FEIQoL scale developed by McWilliam and Casey (2013), to assess the perceptions of families quality of life. This tool considers the functionality of Turkish children aged 3 to 6 who have received an early diagnosis and continue to receive special education services within their daily routines. This scale consists of four factors related to families’ quality of life. One of these is Family Relationships, which reflects families’ perceptions of family communication, parenting, relationships with extended family, and participation in social activities. Another is Access to Information and Services, which focuses on families’ knowledge about child development, managing challenging behaviors, their children’s special needs, and access to resources in their communities. Child Functioning includes items related to families’ perceptions of their child’s participation in daily routines, independence, and social relationships. Finally, Overall Life Situation includes items related to families’ perceptions of the fulfillment of family needs in areas such as family health status, family economy, and employment.
The average total score obtained from the FEIQoL scale indicates that families’ perceptions of their quality of life are generally at a moderate level. The distribution of sub-dimension scores is consistent with the scale structure. However, the relatively low score in the Overall Life Situation sub-dimension indicates that there may be a need for support in this area. When studies conducted with families of children with disabilities in Turkiye and other countries are examined, findings regarding quality of life are generally perceived positively, but there are still some needs or areas that need improvement (Aktan et al., 2020; Alpgan & Alabay, 2021; García-Grau et al., 2019; Ho et al., 2013; Kartal et al., 2021). This situation generally indicates a positive perspective for service providers, but there are differences in scores depending on many variables. Therefore, it is still important to assess individual needs.
The goodness-of-fit indices obtained as a result of the confirmatory factor analysis revealed that the model provided a good fit with the data. When these values are compared with the limit values accepted in the literature (Hu & Bentler, 1999; Kline, 2023), they show that the structural validity of the model is at a sufficient level. The standardized factor loadings of all items on the scale for their respective factors were statistically significant. Generally, factor scores of .40 and above indicate that the item contributes meaningfully to the relevant factor (Hair et al., 2013). FEIQoL, which was reported as a three-factor model in the Spanish sample (García-Grau et al., 2019), exhibits a four-factor structure in this study, which may be related to differences in cultural context and the organization or early intervention services. The fact that the model fit is at an acceptable level indicates that the scale’s theoretical structure is preserved and it is flexibly adapted to different contexts. Factor scores obtained provide strong evidence of the construct validity of the scale. This shows that each item adequately represents the structural dimension to which it is connected.
In this study, the criterion-related validity of the FEIQoL was examined based on its relationship with the BCFQoL. Pearson correlation analysis revealed a highly significant positive correlation between the total scores. A correlation coefficient between 0.30 and 0.70 indicates a moderate relationship, while a coefficient between 0.70 and 1.00 indicates a strong relationship (Büyüköztürk, 2014). This finding reveals that both scales measure similar constructs, and that, in the context of early intervention, the perception of family quality of life is highly correlated with overall family quality of life. The correlation between the total scores of the scales supports the criterion validity of the FEIQoL. However, no statistically significant relationship between the sub-dimensions of FEIQoL (FR, AIS, CF) and the sub-dimension of BCFQoL’s DRS. Only a weakly significant relationship was found between FEIQoL’s OLS dimension and BCFQoL’s DRS. This suggests that some sub-dimensions are independent of each other or focus on different conceptual areas. While the BCFQoL’s disability related support focuses on emotional and practical support from the social environment, friends, extended family or community members (Hoffman et al., 2006), the sub-dimensions of the FEIQoL focus more on dynamics within the nuclear family, such as parent-child interaction, accessibility of early intervention services (García-Grau et al., 2019). This may explain the weak conceptual overlap between the constructs and therefore the lack of significant correlations.
Reliability analysis indicates that the adapted measurement tool had high internal consistency both holistically and at the sub-factor level. The Cronbach’s alpha coefficient for the whole scale demonstrates that the scale has a coherent and holistic structure with all items. In the analyses conducted at the sub-factor level, these values range from .813 to .909. An alpha coefficient at this level indicates that the measurement tool reliably represents the construct it measures and has a high probability of giving similar results with repeated measurements (George & Mallery, 2010; Nunnally & Bernstein, 1994). The fact that the FEIQoL assessment tool also demonstrates high internal consistency in the Spanish sample (García-Grau et al., 2019, 2024) supports the reliability findings obtained in this study and indicates that the scale is capable of providing consistent measurements across different cultural contexts. In addition, Guttman’s two-half reliability coefficient of 0.844 reveals that the scale presents a stable and balanced structure even when divided in half. This indicates that the internal structure of the scale works in a systematic way rather than randomly and that the relationships between the sub-items are significant. In addition, the corrected item-total correlation values of the items were mostly above .40, indicating that each item contributed significantly to the relevant scale score. As noted by Black and Babin (2019), this shows that none of the items in the scale behave in an outlier manner and work in harmony with the overall construct. The fact that statistically significant differences were obtained for all items in the t-tests between the lower and upper 27% groups shows that the discrimination power of the items is high, that is, they can statistically distinguish between individuals with high scores and individuals with low scores (Nunnally & Bernstein, 1994). This indicates that the items are sensitive to the trait they measure and is a supportive finding in terms of scale validity.
It is believed that the findings of this study will have important implications for early intervention policy, research, and practice in Turkiye. In Turkiye, early intervention services have different structural characteristiscs compared to family-centered models commonly implemented in countries where such services are typically integrated into natural settings. Therefore, validation the FEIQoL will provide policymakers and service providers with a culturally appropriate tool for systematically assessing family quality of life and identifying family needs that are not apparent in child-focused assessments. In terms of application, FEIQoL can help identify families’ strengths and potential needs based on the results obtained. This information can then be used as a basis for developing individualized service plans. For example, if the family’s scores in the Access to Information and Services sub-dimension are found to be low, it may be necessary to set the goal of “establishing contact with relevant institutions and support groups.” In addition, it can support monitoring the family’s quality of life throughout the process, strengthen family-professional partnerships, and encourage professionals working in the field of early intervention to adopt more family-centered approaches. When evaluated in a policy context, the use of a standardized family quality of life measure, along with factors such as access to information and services, family relationships, child functioning, and overall life situation, can contribute to the development of responsive and equitable early intervention systems by revealing inequalities related to socioeconomic status, service access, and family roles. In addition, future studies using the FEIQoL tool can examine the impact of service models, children’s disability types, and the regions where families live on family quality of life. They can address the effectiveness of family-focused interventions within Turkey’s early intervention system or continue cross-cultural validity studies. In addition, longitudinal studies can be planned to determine how the perception of family life quality changes over time, depending on the child’s age or the duration of the intervention.
Conclusion
In conclusion, this study aimed to adapt the FEIQoL scale into Turkish as a measurement tool to assess the quality of life perceived by family members in families with children with disabilities at an early age. After ensuring the scale’s linguistic equivalence, its content validity was assessed through expert opinion, followed by a preliminary implementation to test its comprehensibility. The results of this study demonstrate that the FEIQoL is a valid and reliable instrument with good psychometric properties. The scale can be seen as an important tool for researchers and practitioners who want to assess the quality of family life, especially in families with children with various disabilities. Although the study demonstrated acceptable psychometric properties in the context of quality of life for family members of children with various types of disabilities, further validation in larger study groups including children with different types of disabilities and even typically developing children is recommended. This study shows that the perceived family quality of life among participating families was moderate. Indeed, the factors that can be considered in improving families’ quality of life are outlined in detail. The need for increased support for families, particularly in important areas such as health status, family finances, and employment, as well as the overall life situation related to meeting family needs, is highlighted. Therefore, the factors that should be considered in developing family-based services and policies for families with children with disabilities in early childhood are clearly outlined.
It is important to note that this study has some limitations. First, the study population largely consisted of mothers, while fathers and other family members were less represented. To increase the generalizability of the findings, it is important to create a more balanced sample of family members. Furthermore, the absence of significant differences between the data collected online and in person indicates that the data collection method did not significantly affect the family quality of life results. However, when interpreting these findings, it should be noted that there were a limited number of online responses. In addition, family quality of life data in the study were collected solely based on individuals’ own perceptions. This may have limited the diversity of measurements due to the subjective nature of the measurements and their use from a single source. The evaluation of the study results in the context of Turkiye’s specific structural characteristics should consider that the views reported by families regarding family life quality may be related to the limitations of inclusive early childhood environments and the fact that services are generally provided in a centralized manner.
Also, variables such as family sociodemographic characteristics and environmental conditions were not discussed in detail for comparison purposes in the study. In future studies, it is important to reach larger family members suitable for comparison and to include children with different types of disabilities in the study to generalize the findings to different groups. Finally, cognitive debriefing interviews with caregivers were not conducted during the translation phase of the measurement tool. Since parents’ feedback could strengthen the content validity of the translated tool, this can be considered a limitation of the current study. In future research, cognitive interviews with parents could be conducted in addition to pilot studies to ensure that the interpretations of the items are consistent with caregivers’ perspectives and daily practices.
Footnotes
Appendix
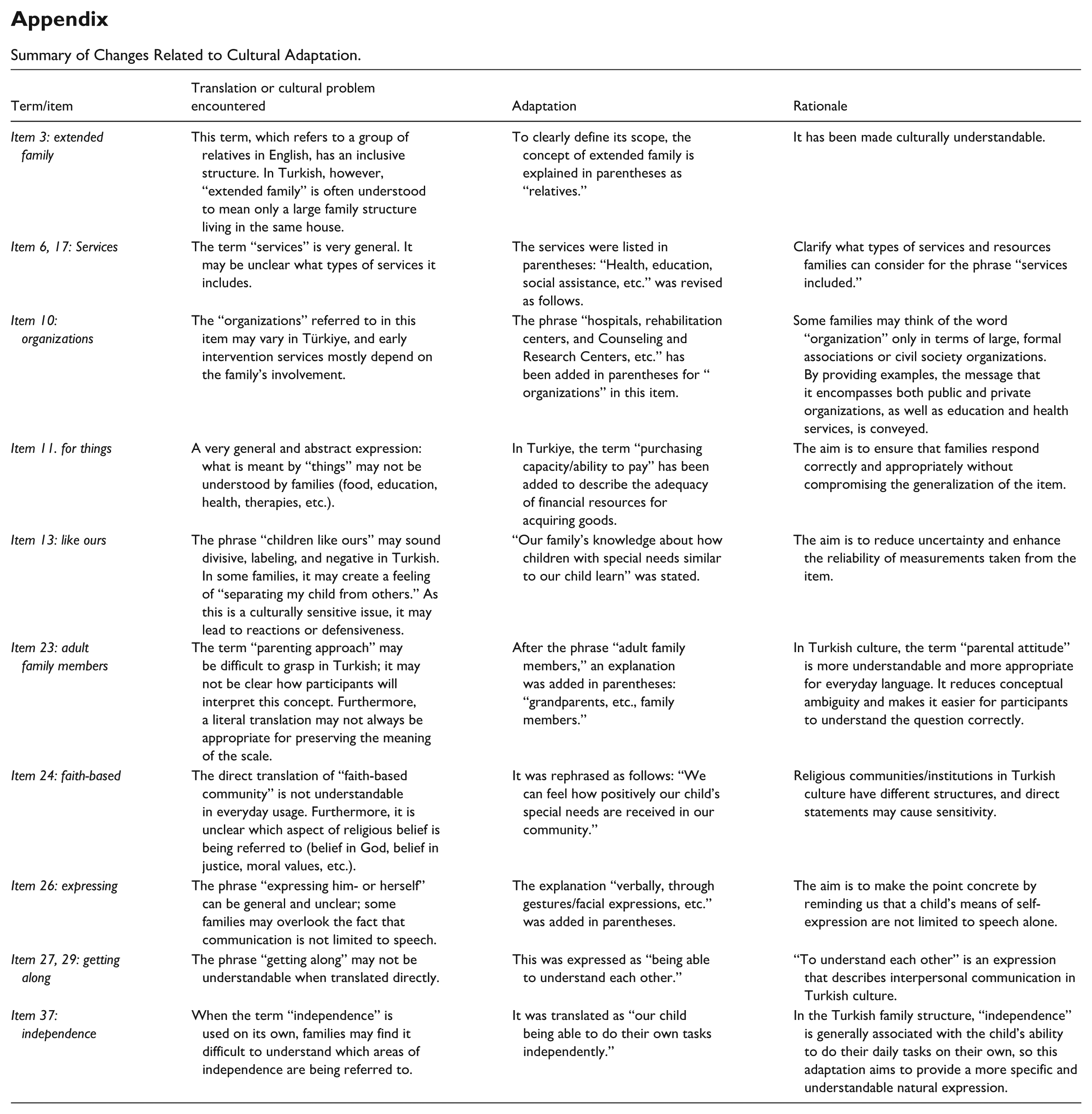
Summary of Changes Related to Cultural Adaptation.
| Term/item | Translation or cultural problem encountered | Adaptation | Rationale |
|---|---|---|---|
| Item 3: extended family | This term, which refers to a group of relatives in English, has an inclusive structure. In Turkish, however, “extended family” is often understood to mean only a large family structure living in the same house. | To clearly define its scope, the concept of extended family is explained in parentheses as “relatives.” | It has been made culturally understandable. |
| Item 6, 17: Services | The term “services” is very general. It may be unclear what types of services it includes. | The services were listed in parentheses: “Health, education, social assistance, etc.” was revised as follows. | Clarify what types of services and resources families can consider for the phrase “services included.” |
| Item 10: organizations | The “organizations” referred to in this item may vary in Türkiye, and early intervention services mostly depend on the family’s involvement. | The phrase “hospitals, rehabilitation centers, and Counseling and Research Centers, etc.” has been added in parentheses for “ organizations” in this item. | Some families may think of the word “organization” only in terms of large, formal associations or civil society organizations. By providing examples, the message that it encompasses both public and private organizations, as well as education and health services, is conveyed. |
| Item 11. for things | A very general and abstract expression: what is meant by “things” may not be understood by families (food, education, health, therapies, etc.). | In Turkiye, the term “purchasing capacity/ability to pay” has been added to describe the adequacy of financial resources for acquiring goods. | The aim is to ensure that families respond correctly and appropriately without compromising the generalization of the item. |
| Item 13: like ours | The phrase “children like ours” may sound divisive, labeling, and negative in Turkish. In some families, it may create a feeling of “separating my child from others.” As this is a culturally sensitive issue, it may lead to reactions or defensiveness. | “Our family’s knowledge about how children with special needs similar to our child learn” was stated. | The aim is to reduce uncertainty and enhance the reliability of measurements taken from the item. |
| Item 23: adult family members | The term “parenting approach” may be difficult to grasp in Turkish; it may not be clear how participants will interpret this concept. Furthermore, a literal translation may not always be appropriate for preserving the meaning of the scale. | After the phrase “adult family members,” an explanation was added in parentheses: “grandparents, etc., family members.” | In Turkish culture, the term “parental attitude” is more understandable and more appropriate for everyday language. It reduces conceptual ambiguity and makes it easier for participants to understand the question correctly. |
| Item 24: faith-based | The direct translation of “faith-based community” is not understandable in everyday usage. Furthermore, it is unclear which aspect of religious belief is being referred to (belief in God, belief in justice, moral values, etc.). | It was rephrased as follows: “We can feel how positively our child’s special needs are received in our community.” | Religious communities/institutions in Turkish culture have different structures, and direct statements may cause sensitivity. |
| Item 26: expressing | The phrase “expressing him- or herself” can be general and unclear; some families may overlook the fact that communication is not limited to speech. | The explanation “verbally, through gestures/facial expressions, etc.” was added in parentheses. | The aim is to make the point concrete by reminding us that a child’s means of self-expression are not limited to speech alone. |
| Item 27, 29: getting along | The phrase “getting along” may not be understandable when translated directly. | This was expressed as “being able to understand each other.” | “To understand each other” is an expression that describes interpersonal communication in Turkish culture. |
| Item 37: independence | When the term “independence” is used on its own, families may find it difficult to understand which areas of independence are being referred to. | It was translated as “our child being able to do their own tasks independently.” | In the Turkish family structure, “independence” is generally associated with the child’s ability to do their daily tasks on their own, so this adaptation aims to provide a more specific and understandable natural expression. |
Ethical Considerations
Ethical approval has been obtained from the Scientific Research and Publication Ethics Committee of Toros University, Turkiye with its decision dated March 21, 2024, and numbered 61.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.