
Abstract
Over the last decade, wilderness therapy research has increased substantially in both quality and quantity and has begun to establish a base of evidence and literature. However, there is still much to be learned about the clients served and their clinical profile. The authors examined diagnostic data from discharge summaries of 929 clients (192 young adults and 737 adolescents) who enrolled in wilderness therapy at four sites across the nation. We explored trends and differences in primary diagnosis and overall prevalence of disorders according to gender and age. Central themes emerged such as the pervasiveness of substance issues, the overwhelming impact of Mood Disorders, and the clinical complexity of wilderness therapy clients. How these findings fit in with industry trends are discussed, as well as the conceptualization of behavioral issues from adolescent to adult populations, variances between adults and adolescents, and gender differences.
Historically, psychotherapy research with adolescents has lagged behind research with adults (Casey & Berman, 1985; Dagley, Gazda, Eppinger, & Stewart, 1994; Kazdin, 2004; Kazdin, Siegel, & Bass, 1990; Tramonta, 1980). Kazdin’s (2004) review of psychotherapy outcomes with children and adolescents, noted that there were more than 1,500 controlled trials of therapy and more than 550 forms of therapy for children and adolescents (Kazdin, 2000). He also expressed concern that most of these treatments have not been examined empirically and suggested there was considerable work to be done to identify what aspects of these treatments work and with whom. Even though a large number of treatment approaches are available, several researchers have expressed concern about the lack of therapy services for adolescents (Koplewicz, 2008; Russell & Gillis, 2010).
Wilderness therapy, also identified as Outdoor Behavioral Health Care (OBH), is a relatively new treatment modality that has improved in clinical sophistication over the course of its development (Russell, Gillis, & Lewis, 2008). What once was referred to as a “boot camp” intervention has taken on an increasingly sophisticated approach as it has developed as a treatment modality for adolescents and young adults (Russell, 2001). Similar to the improvements in research with children and adolescents in general (Kazdin, 2004; Weisz, Weiss, Han, Granger, & Morton, 1995), research with wilderness therapy programs has improved significantly over the past 10 to 15 years. A clear definition of wilderness therapy and its methods have been established (Russell, 2001, 2003b), and outcome studies have begun to provide some evidence of efficacy (Behrens, Santa, & Gass, 2010; Behrens & Satterfield, 2007; Hoag, Burlingame, Reedy, Parsons, & Hallows, 1999; Hoag, Savicki, & Burlingame, 2001; Russell, 2003a, 2005, 2007; Young & Gass, 2010). Even with this growth of research, the evidence and literature within this field still lacks depth and methodological sophistication, and has been limited in the scope of what it has examined. In 2008, Russell et al. stated “an increased understanding of OBH programs is of great importance to policymakers, consumers, and parents” (p. 59). For years, research among wilderness programs primarily focused on dissertations or small-sample size studies that provided conclusions that were difficult to generalize (Russell, 2001, 2003b, 2007; Russell et al., 2008; Scott & Duerson, 2009). Furthermore, data on young adults in wilderness therapy is even more limited.
As we developed an outcome research program, we realized the importance of further examining the diagnostic profile of clients in wilderness therapy, as it impacts treatment approach and programming. While several studies have included some data on the primary reason for referral or the primary diagnosis at intake; missing data, differences in data collection methods, and nonsystematic reviews leaves the picture unclear. We had considerable demographic and diagnostic information, which allowed us to conduct an in-depth and systematic examination of clients based on their disorders as defined by the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association [APA], 2013). Client disorders were categorized during data collection into nine categories: Substance-Related Disorders, Mood Disorders, Behaviors Disorders, Anxiety Disorders, Learning Disorders, Pervasive Developmental Disorders, Attachment Disorders, Psychotic Disorders, and V Codes. By looking at both the population as a whole and as subgroups, this study extracts trends and highlights differences among individuals entering a wilderness therapy program.
We feel this responds to the challenge given by Kazdin (2004) to better understand the population served in wilderness therapy and is similar in scope to studies done with residential treatment centers (Baker, Archer, & Curtis, 2005; Connor, Doerfler, Toscano, Volungis, & Steingard, 2004; Drais-Parrillo, Baker, Gunn, Kurkland, & Schnur, 2004) and studies examining how client characteristics affect outcomes in wilderness or residential settings (Magle-Haberek, Tucker, & Gass, 2012). Our research questions included the following:
Method
We conducted a secondary analysis of records at four Second Nature Wilderness Program locations. Two of the programs were located in Utah, one in Georgia, and one in Oregon. Second Nature’s therapeutic wilderness model incorporates primitive living, ceremony and metaphor, the group process, and task accomplishment to build self-efficacy. This model lends itself well to natural and logical consequences rather than verbal, didactic therapy models. Second Nature incorporates a strong clinical emphasis into the wilderness setting that uses staff as a part of the treatment team instead of merely as outdoor guides. The adolescent or young adult leaves the comfort of home and is immersed in a new culture, where therapists, staff, and the group provide a myriad of opportunities for self-reflection and learning opportunities (Gass, Gillis, & Russell, 2012; Russell, 2001).
We examined diagnostic data found in discharge summaries for clients who were admitted between October 2010 and November 2011. We used discharge summaries as this was the most accurate source for diagnosis information given that the therapist had the entire course of the program to clarify and confirm diagnoses. There were a total of 929 participants in our analysis. Of these 737 were adolescents (218 females, 519 males), and 192 were adults (35 females, 157 males). The majority of the clients in this wilderness program were Caucasian and past reviews of clientele in this wilderness program indicate that 85% of clients were identified as White or Caucasian (Hoag, Massey, Roberts, Logan, & Poppleton, 2011).
The typical wilderness client has multiple Axis I diagnoses. For example, a client may have both a mood and substance-related disorder along with a V-Code diagnosis. From the discharge summaries, the first four diagnoses were exported into a spreadsheet and then further statistical analysis was done using the computer program SPSS (IBM Corp, 2012). In this study, we distinguished between the primary diagnosis and the first four diagnoses (referred to as “prevalence” for the purposes of this study) listed in the client discharge summary.
We grouped diagnoses according to the nine most common DSM diagnostic categories found in our population: Substance-Related Disorders, Mood Disorders, Behaviors Disorders, Anxiety Disorders, Learning Disorders, Pervasive Developmental Disorders, Attachment Disorders, Psychotic Disorders, and V Codes (APA, 2013). To distinguish between primary diagnosis and prevalence, we created prevalence variables for each of the diagnostic categories. The primary diagnosis was the first diagnosis listed on the discharge summary. The prevalence variables indicated whether or not a student had a disorder in a specific diagnostic category within their first four diagnoses (see Figure 1).
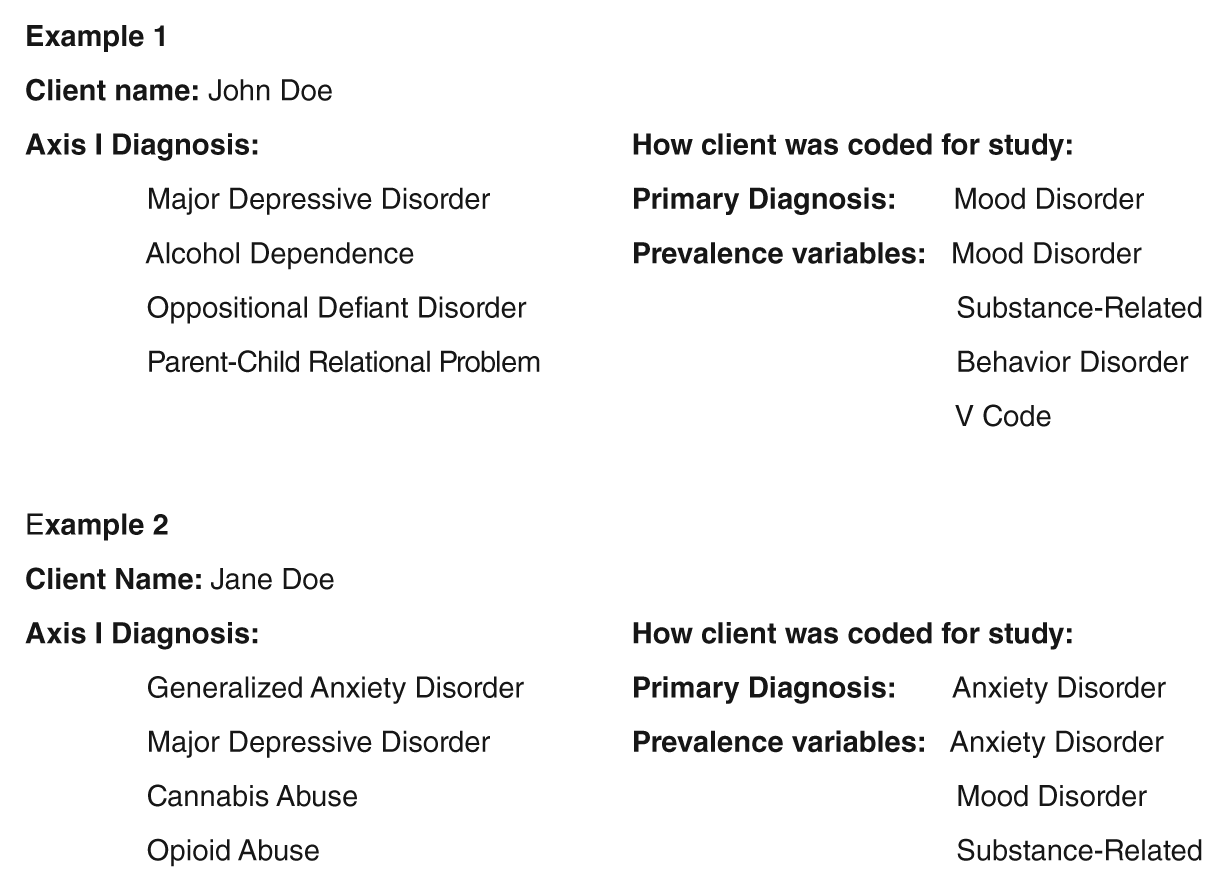
An example of coding the first four Axis I diagnoses into the primary diagnosis and the prevalence variables.
Results
Out of the 929 participants, 29% were female and 71% male; 21% were adults and 79% were adolescents. The adults found in wilderness therapy are generally young adults and are often considered an extension of the adolescent population. For adolescents, the median age was 16 and the mean age was 15.6 years. For young adults, the median age was 19 years and the mean age was 20.3 years.
Seventy-four percent of adolescents were diagnosed with four or more diagnoses. Among adolescents, the primary diagnosis and overall prevalence followed each other closely. As seen in Figures 2 and 3, Mood Disorders were the most common primary diagnosis and also accounted for the highest prevalence. It is noteworthy that Mood Disorders were roughly twice as common as any other primary diagnostic category. In regard to prevalence, Mood Disorders were only slightly higher than Behavior Disorders, Substance-Related Disorders, and Anxiety Disorders.
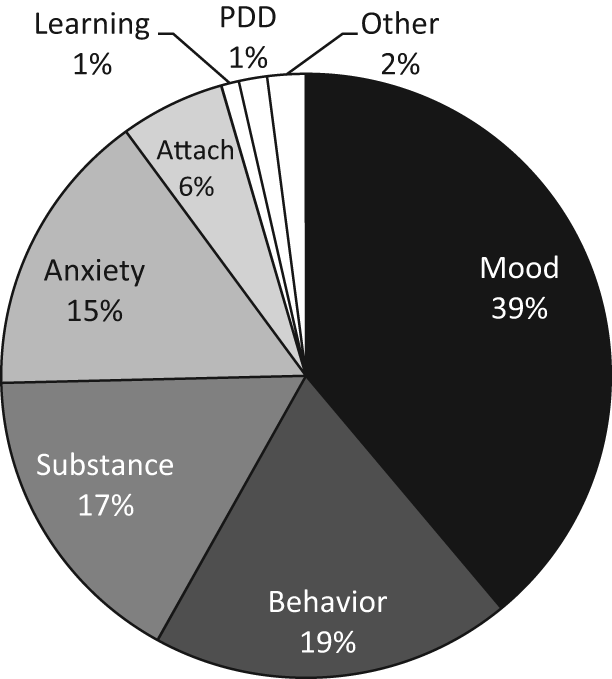
Adolescent clients’ primary diagnosis at discharge.
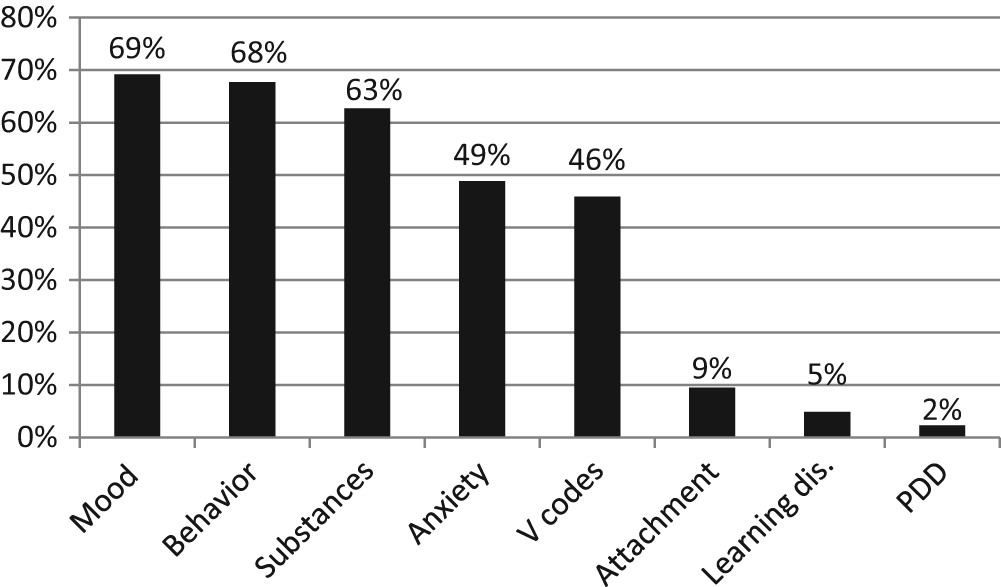
Adolescent prevalence of diagnoses in a specific diagnostic category at discharge.
In our population of young adult clients, 55% had four or more diagnoses. Similar to adolescents, Mood Disorders were the most common primary diagnosis and nearly twice as common as the second largest category (see Figures 4 and 5). In regard to prevalence, Substance-Related Disorders surpassed Mood Disorders affecting more than 80% of the young adult population.
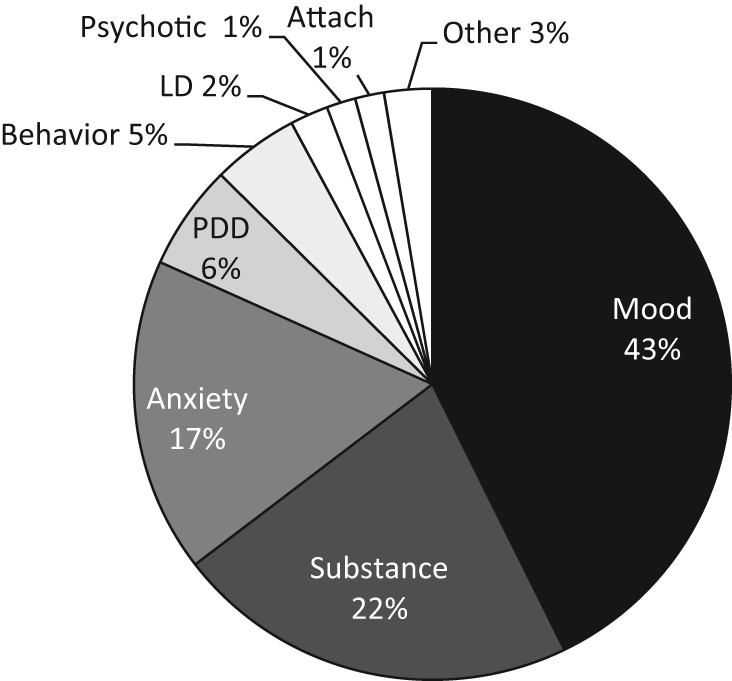
Adult clients’ primary diagnosis at discharge.
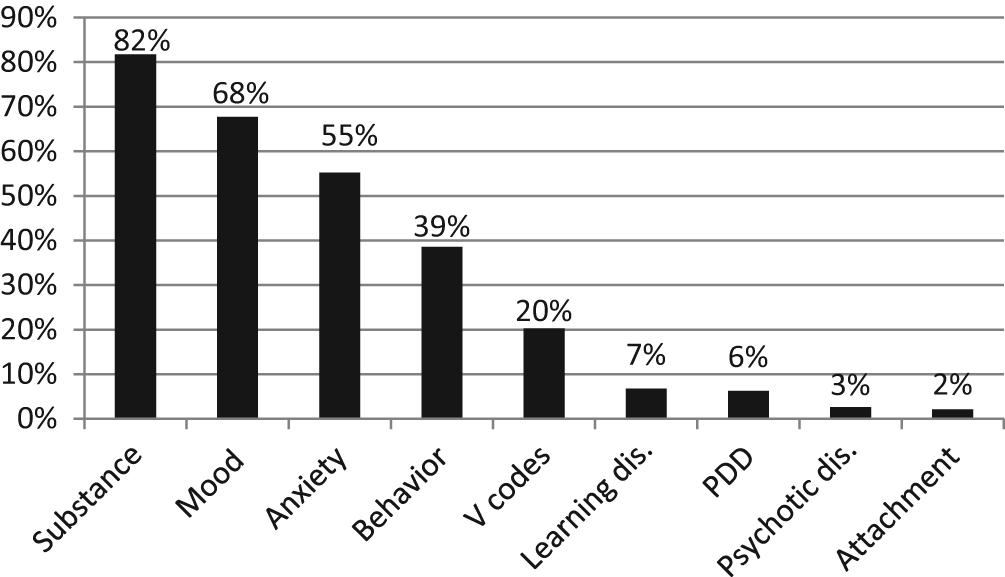
Adult clients’ prevalence of diagnoses in a specific diagnostic category at discharge.
Mood disorders consisted of Major Depressive Disorder, Depressive Disorder Not Otherwise Specified (NOS), Bipolar Disorder, and Dysthymic Disorder. Rates of these were fairly similar across groups, though adults tended to have higher rates of Bipolar Disorder, compared with adolescent clients. Clients with Substance-Related Disorders as a primary diagnosis were most often using cannabis, alcohol, or a combination of substances. Compared with adolescents, adults had lower rates of cannabis and higher rates of alcohol and other drugs (i.e., cocaine, opioids, and amphetamines) as the primary diagnosis. Behavioral Disorders primarily consisted of Attention-Deficit/Hyperactivity Disorder (AD/HD) and Oppositional Defiant Disorder (ODD). For adults with a Behavioral Disorder as the primary diagnosis, roughly 90 were AD/HD. Among adolescents, a different trend appears with only 49% of behavioral issues in the primary diagnosis being AD/HD and 50% being ODD (see Figures 6-8).
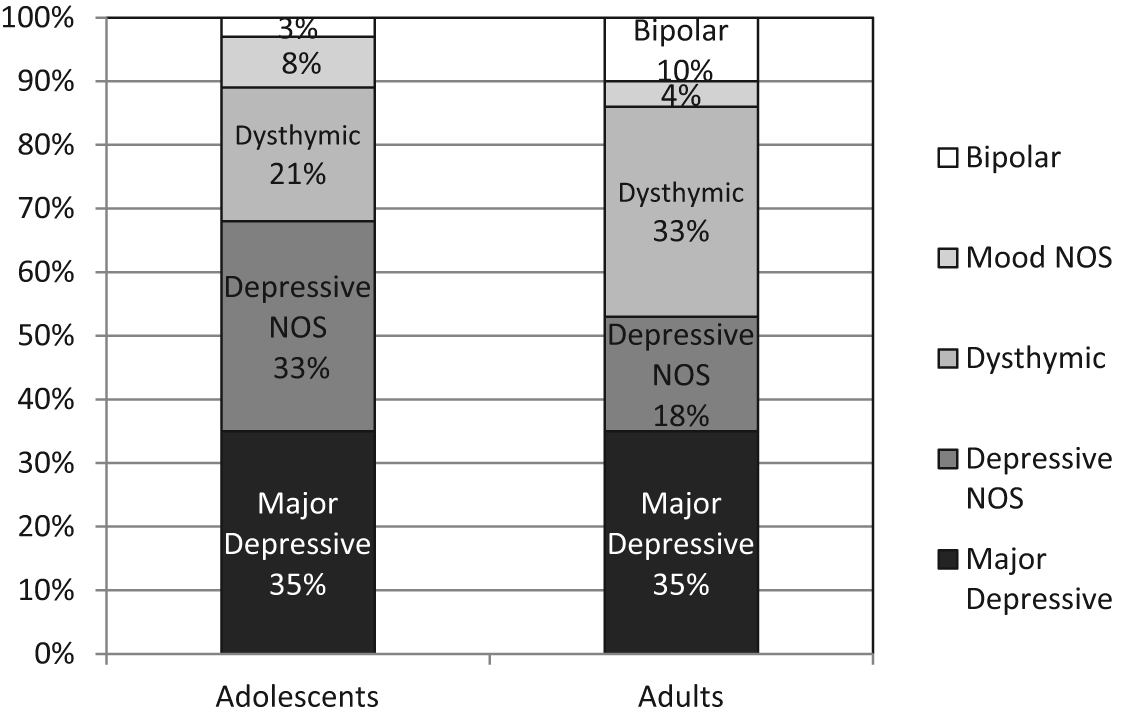
Mood disorders in the primary diagnosis among adolescents and young adults.
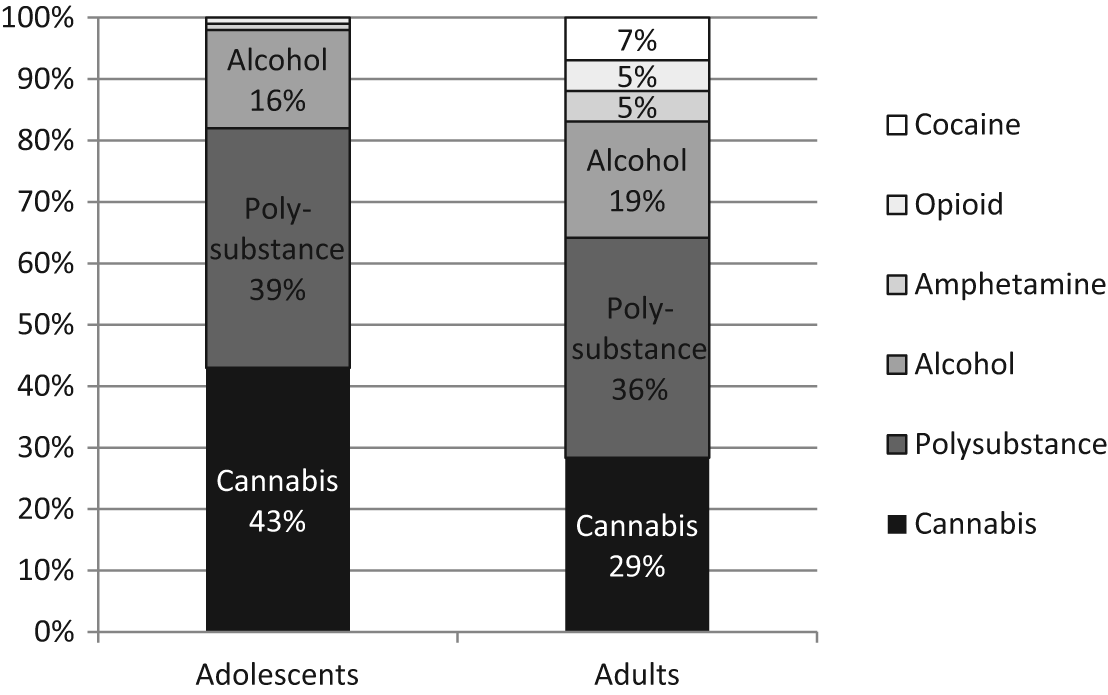
Substance disorders in the primary diagnosis among adolescents and young adults.
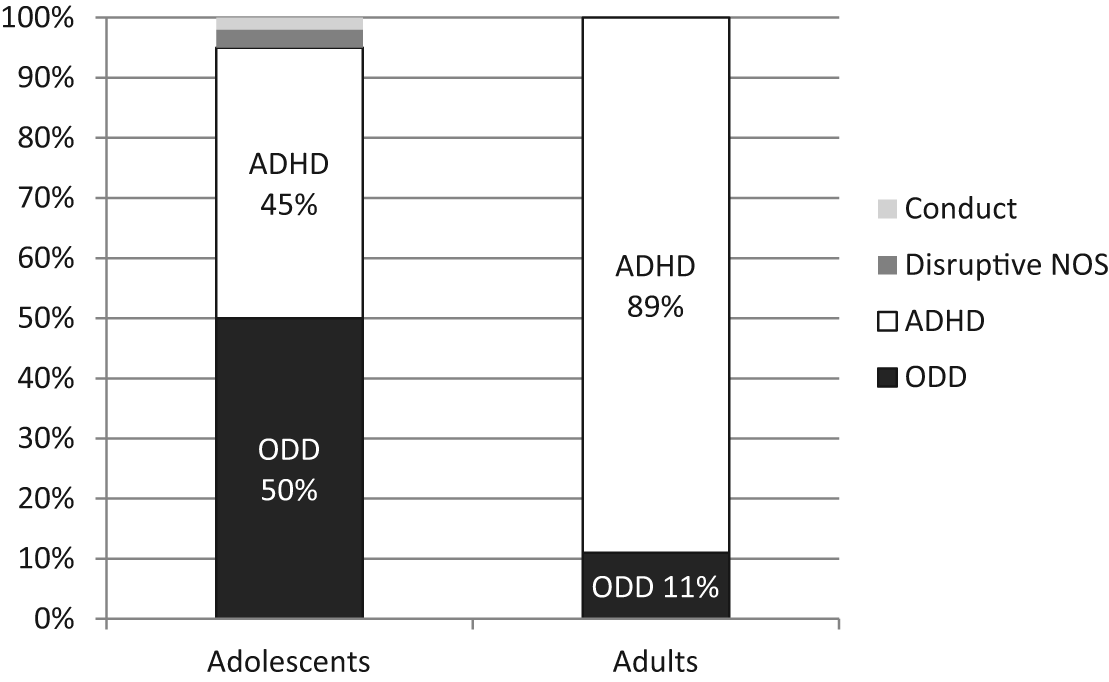
Behavior Disorders in the primary diagnosis among adolescents and young adults.
Are Young Adult and Adolescent Clients Diagnostically Different?
Using the chi-square test of independence, we found that adult and adolescent clients had statistically different prevalence rates in five of the diagnostic categories (see Table 1). Adult clients had significantly greater rates of Substance-Related Disorders and Pervasive Developmental Disorders; while adolescents had significantly greater rates of Behavior Disorders, Attachment Disorders, and V Codes. Rates of Anxiety, Mood, and Learning Disorders were not statistically different between adults and adolescents.
Comparing Prevalence of Disorders Among Young Adult and Adolescent Clients—Chi-Square Test of Independence (N = 929).
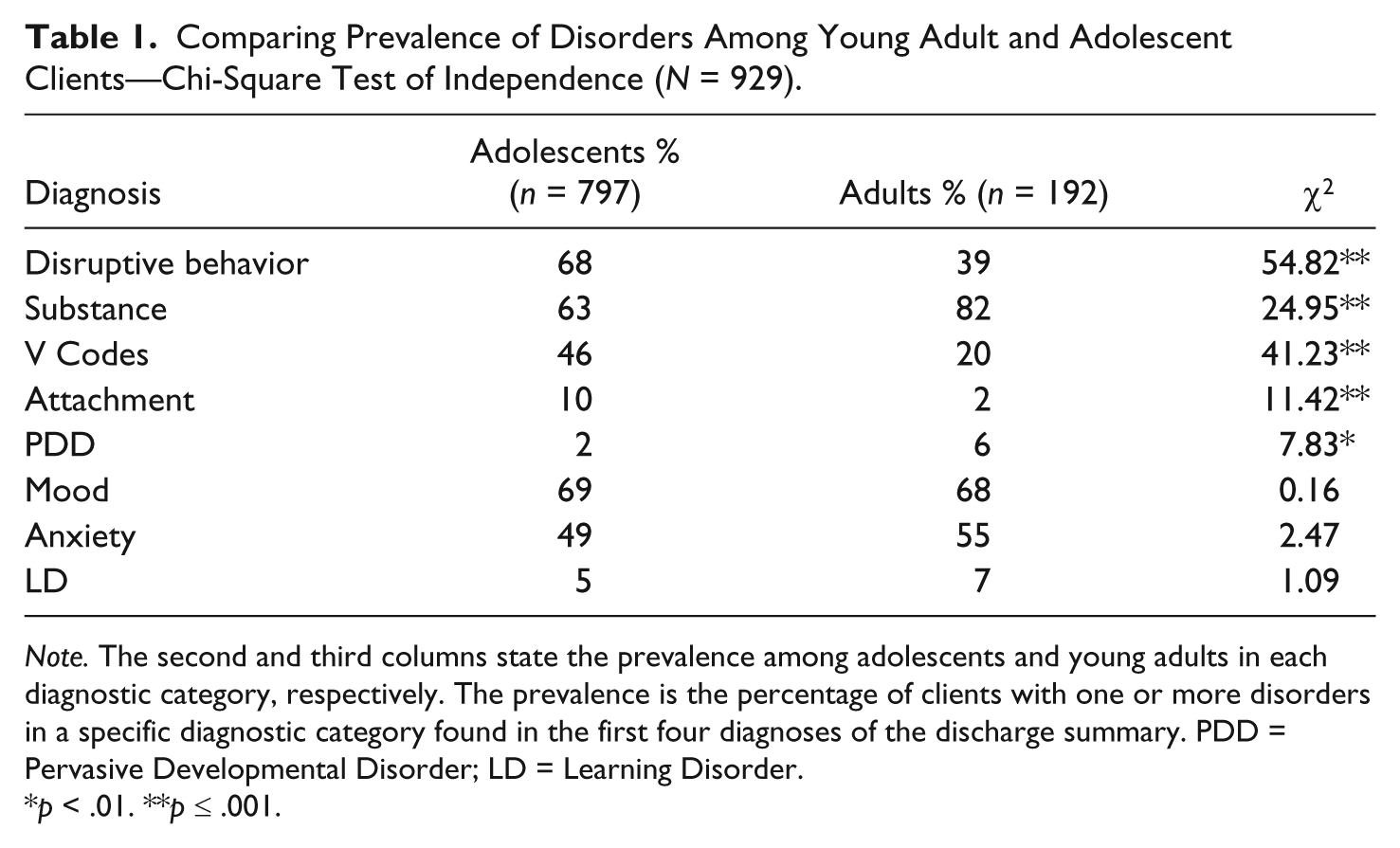
Note. The second and third columns state the prevalence among adolescents and young adults in each diagnostic category, respectively. The prevalence is the percentage of clients with one or more disorders in a specific diagnostic category found in the first four diagnoses of the discharge summary. PDD = Pervasive Developmental Disorder; LD = Learning Disorder.
p < .01. **p ≤ .001.
In addition, we found two other distinctions between adults and adolescents when looking within the same gender. Though the overall rate of Mood Disorders between adults and adolescents was not statistically different, the difference between adolescent and adult females was significant. Seventy-three percent of adolescent females and only 51% of adult females had a Mood Disorder, χ2(1, N = 253) = 6.98, p = .008. Similarly, when comparing only males, adults had a higher rate of Anxiety Disorders than adolescent males (56% of adult males and 44% of adolescent males), χ2(1, N = 676) = 6.66, p = .010.
Are Male and Female Clients Diagnostically Different?
Male and female adults had different rates of prevalence in two of the diagnostic categories: Mood Disorders and Behavior Disorders. Roughly 71% of adult males had a Mood Disorder compared with 51% of adult females (the lowest of any group), χ2(1, N = 192) = 5.19, p = .023. Behavior Disorders occurred with 45% of adult males and 11% of females, χ2(1, N = 192) = 13.28, p = .000.
Male and female adolescents had different rates of prevalence in three of the diagnostic categories: Substance-Related Disorders, Behavior Disorders, and Anxiety Disorders. Adolescent males had significantly higher rates of Substance-Related Disorders at 67%, compared with their female counterparts at 53%, χ2(1, N = 737) = 11.88, p = .001. Adolescent boys also had a higher rate of Behavior Disorders (males 70%, females 62%), χ2(1, N = 737) = 4.73, p = .030. Adolescent girls had higher a rate of anxiety than boys with 60% of girls and 44% of boys having an anxiety related diagnosis, χ2(1, N = 737) = 14.41, p = .000.
Length of Stay
The mean and median length of stay for adolescents was 9.9 weeks. For young adults, the mean and median length of stay was 9.8 and 9.6 weeks, respectively. Using the t test, we tested whether a diagnosis within a specific DSM category had a longer or shorter length of stay than those not in that DSM category. Adolescent clients with a substance diagnosis (M = 10.1, SD = 2.4) stayed 0.64 weeks longer (p = .001), than those without a substance diagnosis (M = 9.5, SD = 2.7), t(734) = 3.34, p = .001. Adult clients with a behavior diagnosis (M = 9.1 weeks, SD = 2.9) stayed about 1 week less than clients who did not have a behavior diagnosis (M = 10.2 weeks, SD = 3.5), t(190) = −2.27, p = .025. There was no difference in length of stay between adolescents and adults, or between males and females.
Discussion
The findings in this study both support and expand upon research trends within OBH (Behrens & Satterfield, 2007; Russell et al., 2008; Young & Gass, 2010). Given our review of the literature, we believe that this is the first study to utilize rigorous methods to examine the clinical profile of wilderness therapy clients. Analyzing data from the discharge summaries adds a level of accuracy and quality, and distinguishing between primary diagnosis and prevalence adds clarity and depth of insight to previous findings. This systematic analysis confirms the pervasiveness of dual diagnosed clients and substance issues, as well as brings to light the significant impact of Mood Disorders.
Studies consistently document that wilderness therapy clients have multiple diagnoses; though the data on the primary concern fluctuates. Looking at trends in OBH, a 2008 survey of 65 OBH programs reported that substance abuse was most frequently mentioned as the top reason for referral; the second was behavioral issues (Russell et al., 2008). These findings contrasted a 2001 survey that found that substance abuse was not in the top 10 issues for wilderness therapy clients. Russell et al. (2008) explained that “clinical issues have shifted from behavioral and emotional disorders to substance use issues as the primary clinical issue” (p. 68). Similarly, in 2007, Behrens and Satterfield’s study with 1,027 adolescents in private residential treatment centers, the most frequent focus of treatment was Disruptive Behavior Disorders (50%), Substance Use (40%), and Mood Disorders (34%). Eighty-two percent of their sample was being treated for multiple issues. In 2010, Young and Gass found that 77% of students from 10 OBH programs had three or more reasons for referral. Rather than substance-related diagnoses though, Young and Gass found that the most common primary diagnosis was Mood Disorders/Depression, followed by ODD/Conduct Disorders.
Our sample supports that Substance-Related Disorders strongly affect this population with 82% of adult clients and 68% of adolescent clients. However, our data also show that Mood Disorders are by far the most pressing issue. For both age groups, a Mood Disorder was the most frequent primary diagnosis, with the next category 20 percentage points behind. Some of these differences may be in part due to methodological differences and our use of discharge summaries while other studies used intake and referral documents. In addition, several studies utilized clients from residential treatment centers who may be qualitatively different than wilderness therapy clients.
In contrast to earlier research suggesting that wilderness programs were primarily focusing on behavioral and substance abuse issues (Behrens & Satterfield, 2007; Russell et al., 2008), diagnostic trends in our sample of wilderness therapy clients were mostly congruent with other models of inpatient treatment as mood, disruptive behavior, and anxiety were the most common diagnoses (Baker et al., 2005; Bettman & Jasperson, 2009; Connor et al., 2004; Drais-Parrillo et al., 2004; Hooper, Murphy, Devaney, & Hultman, 2000; Lazerle et al., 2001; Lyons, Terry, Martinovich, Peterson, & Bouska, 2001). One difference was that this study showed a greater amount of diagnoses related to substances, particularly as a primary diagnosis. In our sample, 17% of adolescents and 22% of adults had a Substance-Related Disorder as their primary diagnosis. Due to a lack of clarity and consistency in how reasons for referral were reported, we hesitate to draw conclusions from these comparisons.
New Trends and Findings
The difference between rates of Behavior Disorders between adults and adolescents was striking, particularly because the adult population is often considered to be similar to the adolescent population in wilderness. Nineteen percent of adolescents, compared with just 5% of adults, had a behavioral issue as their primary diagnosis. The type of behavioral diagnosis also differed between age groups with 50% of adolescent and 10% of adult Behavior Disorders being ODD (see Figures 6-8). Adolescents may be over diagnosed with ODD, and their struggles with mood and substance issues interpreted as oppositional or noncompliant behavior, especially because many young adults do not have the parenting dynamic present in their life in the same way adolescents do. Often young adults are seen as making their own choices, as opposed to defying authority figures such as parents and teachers. This can be seen as a sort of aging-out of Behavior Disorders as clients mature and become more independent. In addition, due to the parent–child struggle in adolescence, behavioral issues may be seen as requiring treatment, whereas with young adults behavioral issues could be less likely to lead to treatment without comorbid conditions such as mood issues, substance abuse, or legal trouble. Finally, it is possible that several of the diagnoses present with young adults have had time to solidify from when they were adolescents.
There appear to be notable differences among gender as well. Similar to other studies among adolescents, we found that Behavior Disorders were more likely to be present among males than females (Connor et al., 2004). However, the greater distinction in rates of Behavior Disorders in our sample was between adults and adolescents, not males and females. Moreover, previous studies have supported that girls are more likely to be diagnosed with Mood and Anxiety Disorders (Connor et al., 2004). In our sample, adolescent girls did not have a significantly higher rate of Mood Disorders than adolescent boys. In fact, for adults it is the opposite; adult males have a significantly higher rate of Mood and Anxiety Disorders than adult females.
A study on co-occurring trajectories of anxiety, depression, and oppositional defiant symptoms lends insight into diagnostic patterns seen in our sample. The trajectory of anxiety increased for males and females, while depressive symptoms increased for males only. Oppositional symptoms declined for females, and showed a nonsignificant linear pattern for males indicating a leveling of oppositional symptoms over time (Leadbeater, Thompson, & Grupposo, 2012). This trend is reflected in our sample with depression and anxiety remaining great concerns for young adults, and the level of behavioral issues having less impact.
Russell et al. (2008) predicted that substance use would become a more prevalent diagnosis than emotional or mood issues. In this study, substance use was found to be more prevalent for adults than any other single diagnostic category. The fact that 82% of adults had a substance use or addiction problem indicates a growing problem for this population. An intriguing angle to examine is that while the vast majority of adults have a substance-based diagnosis, only 22% of adults had a Substance-Related Disorder as their primary diagnosis. Such a difference implies that a large number of client’s substance use is secondary to other issues. A possible explanation for this is the use of substances to self-medicate for underlying issues. This theory is supported by the fact that 60% of all adult clients and 54% of all adolescent clients had either a Mood or Anxiety Disorder as their primary diagnosis.
It is important to note that Substance-Related Disorders affected the greatest number of clients (82% of adults, 63% of adolescents) only when Mood and Anxiety Disorders were separated from each other. When combined, 85% of adults and 81% of adolescents had a Mood or Anxiety Disorder (or both) within their first four diagnoses. In addition, more than half of the population in this study had a Mood or Anxiety Disorder as their primary diagnosis. This indicates that wilderness is being used for much more than behavioral or substance use problems, as the average wilderness client is now presenting with a clinically complex diagnostic profile. Wilderness field instructors and therapists are no longer just providing a sober experience; rather, they are providing intensive mental health treatment in the setting of the wilderness.
Implications
A central theme of this study is that the typical wilderness therapy client appears more clinically complex compared with earlier research (Behrens & Satterfield, 2007; Russell, 2001; Russell et al., 2008). This carries several implications including approach to therapy, staff training and support, and careful admissions screening. The presence of more varied and complex profiles demands that an array of interventions and treatment modalities be implemented to best serve each client. Therapists and managers must be well-trained and keep abreast of the latest research to assure that appropriate and effective practices are implemented for the presenting issues of each client. Ethical issues surrounding nonmaleficence also arise as there is an increasing risk of doing damage or harm to clients with more complex emotional and personality dynamics. Second, these findings further highlight the need for staff equipped to deal with multiple clinical issues, as opposed to primarily serving as outdoor staff providing a structured, sober experience. There is a potential for higher burnout and turnover when staff are asked to deal with more challenges (Marchand, 2008). Managers must be attuned to staff well-being and competency and do whatever possible to support staff through training, emotional support, and time-off. The last important implication is that, it may be more likely that a client, whose needs are too much for wilderness, is still referred for admission. Employees who work in admissions must be trained to identify this or defer to clinical directors to assure proper placement.
Conclusion
The chief diagnoses affecting clients in this sample were Mood Disorders, Substance-Related Disorders, Behavior Disorders, and Anxiety Disorders. There are differences and nuances to how these affect client groups, particularly between adults and adolescents. This study provides further evidence that wilderness therapy has evolved to become a treatment modality that serves a diverse population with increasingly clinical and sophisticated diagnostic profiles. While Substance Disorders were present with 82% of adults and 63% of adolescents, Mood Disorders were by far the most common primary concern for all groups. When combining Mood and Anxiety, these two categories dominate the primary concern and prevalence of diagnoses for both adolescents and young adults in this study. In addition, the majority of adolescents and adults had more than four diagnoses.
We feel these results begin to answer Kazdin’s (2004) challenge to better describe what treatments work better and for whom. This particularly applies to adults in wilderness therapy, as this population is largely absent from the current literature base. As the field of wilderness therapy develops and matures, it is important to understand the population we serve and how the individuals within that population may differ from one another. This knowledge can be used to inform treatment, enhance the recognition of wilderness therapy as a viable treatment option for a wide range of treatment issues, and challenge programs to meet the increasing complexities of the wilderness therapy client. This underscores the need for exploring the effectiveness of a wilderness therapy intervention for varying disorders and clinical profiles.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.