
Abstract
Medical interpreters aid in providing culturally sensitive palliative care to patients with limited-English proficiency. However, navigating their complex, and sometimes contradictory, roles and the sensitive nature of the content in palliative care encounters can negatively impact medical interpreters. Compassion fatigue (CF) and secondary traumatic stress (STS) are concepts that have been explored in many healthcare professionals but have not been fully explored in medical interpreters in palliative care. This review examines the psychometric properties of three measures of CF and STS that have been utilized in various populations of healthcare providers. There are no measures of CF or STS that have been shown to be valid and reliable in medical interpreters participating palliative care encounters. Further research is needed to investigate the validity of the reviewed measures in medical interpreters, and it may be beneficial to modify existing tools to measure CF and STS more accurately in this population.
Keywords
Introduction
There are over 7,000 languages spoken worldwide, and while English is the most common combined native and non-native language, there are many people who do not speak or understand English well (Eberhard et al., 2023). For example, in the United States, approximately 22% of the U.S. population 5 years or older speak a language other than English at home; 19% of this population report they speak English “not well” or “not at all,” or have limited-English proficiency (LEP) (Dietrich & Hernandez, 2022). There is robust evidence demonstrating the healthcare disparities experienced by people with LEP including: fewer physician visits, lower vaccination rates, and higher rates of harm from medical errors (Divi et al., 2007; Fiscella et al., 2002). When people with LEP receive palliative care they experience lower rates of advance care planning, poorer pain assessment and management, and lower hospice utilizations rates (Abedini et al., 2022; Payson et al., 2022; Rahemi & Jarrín, 2023). Providing accessible, culturally sensitive care is a priority for the palliative care community as a whole (National Consensus Project for Quality Palliative Care, 2018). To achieve this, including professional medical interpreters as integral members of interprofessional healthcare teams is imperative (Hsieh & Kramer, 2012; Latif et al., 2022b; Slusarz, 2023; Wu & Rawal, 2017).
Although secondary traumatic stress (STS) and vicarious trauma have been investigated in medical interpreters caring for refugees and other populations, there is minimal quantitative data regarding the emotional impact of palliative care encounters on medical interpreters (Goldhirsch et al., 2022). Research has demonstrated medical interpreters play many roles when interpreting for palliative care patients such as interpreting language and meaning, acting as a cultural broker, and advocating for patients and families (Hordyk et al., 2017; Kirby et al., 2017; Latif et al., 2022a; Silva et al., 2020; Slusarz, 2023; Weaver et al., 2022). Interpreters have reported that navigating these complex and sometimes contradicting roles can present moral and ethical dilemmas that can cause emotional distress (Hordyk et al., 2017; Kirby et al., 2017; Norris et al., 2005; Rhodes et al., 2021; Silva et al., 2020). In qualitative studies, interpreters have reported that participating in palliative care encounters requires compartmentalization or suppression of their emotions (Kirby et al., 2017; Schenker et al., 2010; Silva et al., 2020). The emotional burden of the encounters has been reported to be linked to the content of the conversation and the emotional intensity of the participants (Weaver et al., 2022).
Given the need to include medical interpreters as members of the interprofessional team when caring for patients with LEP and the National Consensus Guidelines for Palliative Care mandate for emotional support of the interprofessional team, it is important to attempt to measure and address the emotional burden that medical interpreters experience (National Consensus Project for Quality Palliative Care, 2018). While the emotional burden of palliative care conversations on medical interpreters has been somewhat explored in qualitative literature, there has not been an attempt to quantify, measure, and address the emotional impact of these encounters (Hancox et al., 2023).
To understand the experiences of medical interpreters more research is needed in this population of medical professionals. Compassion fatigue (CF) is a concept that refers to the exhaustion experienced by members of helping professions as a result of prolonged and repeated exposure to compassion stress (Sorenson et al., 2016). It is closely related to the concepts of burnout and STS, with some authors using the terms CF and STS interchangeably (Baqeas et al., 2021). CF is associated with physical, emotional, and work-related symptoms as well as potential patient harm (Sorenson et al., 2016). CF has been explored across many healthcare workers including other palliative care provider populations, but has not been fully explored in medical interpreters participating in palliative care encounters (Baqeas et al., 2021; Cavanagh et al., 2020). Thus, this paper will examine the psychometric properties of existing measures of CF or STS to address the following question: does participating in palliative care encounters increase CF or STS in professional medical interpreters?
Literature Review
Ethical Considerations
Medical interpreters are not the typical subject of palliative care research; however, the nature of their work warrants consideration of ethical issues that pertain to research with this specific group of professionals. For example, medical interpreters may experience emotional burden when participating in palliative care encounters, so it is important to consider the concepts of vulnerability and sensitivity (Pilbeam et al., 2022). Interpreters not only interpret emotionally laden language, but also navigate complicated roles that can result in moral distress. Thus, researchers interested in exploring the experiences of medical interpreters in palliative care must consider and attempt to mitigate the risk of discussing emotional experiences and provide appropriate support to research subjects (Mitchell & Irvine, 2008; Pinto et al., 2022).
In addition to the sensitivity of the research topic, medical interpreters themselves may be members of cultural or ethnic minority groups. Therefore, the development and execution of the research with medical interpreters should be conducted using a culturally sensitive approach. To achieve this, members of the population of interest should be involved in the research at every stage, including research design (Gil & Bob, 1999; Marshall & Batten, 2004; The PCORI Approach to Patient-Centered Outcomes Research, 2020 ). Additionally, specifically related to instrument selection, most instruments have been developed for white, North American, or European populations. It may not be possible to utilize the same instruments in research with members of cultural or ethnic minority groups because their experiences and viewpoints may differ significantly (Gil & Bob, 1999).
Finally, privacy is a noteworthy concern in the protection of medical interpreters and their patients. In some small communities, such as the Inuit population studied in rural Quebec, professional interpreters may have social or professional connections to their patients (Hordyk et al., 2017). This may not only impact the emotional experience of interpreting the palliative care encounter, but it may also pose a concern for the privacy of the patients when conducting research on their medical encounters. Additionally, the privacy and data protection of the medical interpreters themselves is vital. During the research, they will be sharing information regarding challenging and sometimes negative aspects of their work. To share this information freely without fear of retaliation or termination of their employment, the data collected must be anonymized and store securely (Kisselburgh & Beever, 2022).
Importance of Reliable and Valid Tools
The use of valid and reliable tools underpins rigorous, sound research (DeVon et al., 2007). Construct validity is a key issue when choosing tools that measure CF, given that it closely associated with several other concepts (DeVon et al., 2007). Additionally, as mentioned previously, since medical interpreters may be members of cultural and ethnic minority groups, reliability of tools among different ethnic and cultural groups is important (Gil & Bob, 1999). Finally, utilizing valid and reliable tools allows for identification of at risk populations and establish mitigation strategies to prevent potential harm caused by CF.
Methods
A search was conducted utilizing Google Scholar, PubMed, and PsycINFO in September 2023. The search terms included a combination of (CF OR STS OR vicarious trauma) AND (medical interpreters) AND (palliative care OR serious illness). No date restrictions were included. No results were found for a tool measuring CF or STS specifically in medical interpreters or palliative care providers. However, related results included several tools that were initially developed to measure CF or STS in other populations that have been applied to healthcare workers, palliative care providers, and even medical interpreters. Three tools were selected for this analysis based on their frequency of use and validity.
Results
ProQOL
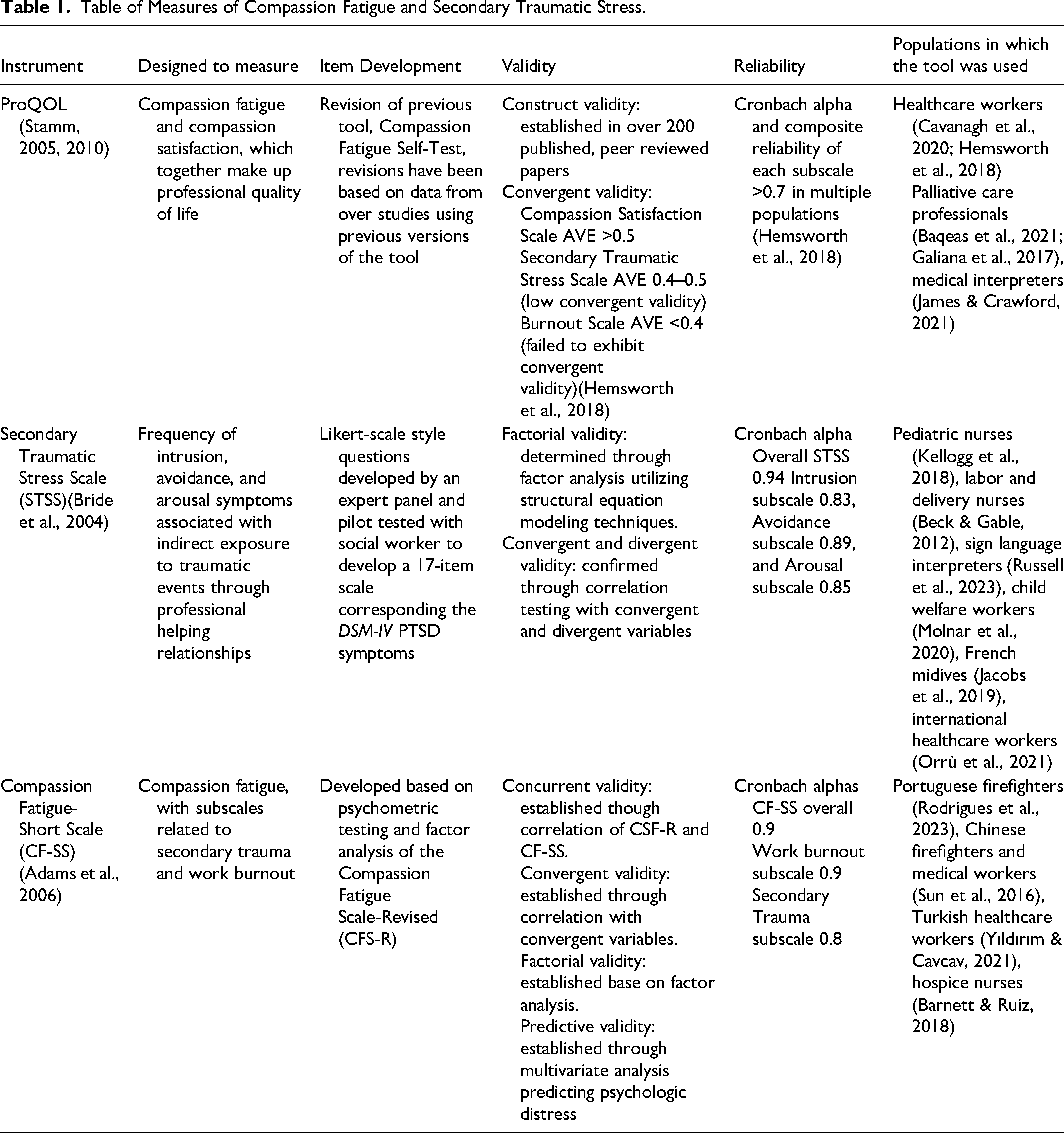
ProQOL is a 30-item self-administered scale with three 10-item distinct subscales that aims to measure professional quality of life which is comprised of two aspects: Compassion Satisfaction and CF (Stamm, 2010). The Compassion Satisfaction subscale measures positive aspects of an individual's professional quality of life, while the Burnout and Secondary Traumatic Stress scales (STSSs) measure the negative aspects, or CF (Stamm, 2010). ProQOL is the most recent revision of the Compassion Fatigue Self-Test (Figley, 1995; Stamm, 2010). The Compassion Fatigue Self-Test was initially developed based on clinical experience in caring for individuals who cared for traumatized people (Figley, 1995). While ProQOL has undergone several revisions to reach its current form, using data reported in studies utilizing earlier versions of the tool, there is no discussion regarding stakeholder involvement in development of the tool (Stamm, 2005, 2010).
Construct validity was reported to have been established with over 200 peer review papers published (Stamm, 2010). Each ProQOL subscale is intended to measure separate constructs. The Compassion Satisfaction scale is distinct, with 2% shared variance with the STSS (r = −.23; co-σ = 5%; n = 1187) and 5% shared variance with the Burnout Scale (r = −.14; co-σ = 2%; n = 1187) (Stamm, 2010). There is significant shared variance between the STSS and the Burnout Scale (r = .58; co-σ = 34%; n = 1187) as both scales measure negative affect (Stamm, 2010). A recent study of Canadian nurses, Australian nurses, and Australian palliative care providers aimed to investigate the psychometric properties of ProQOL. Reliability was assessed for each subscale; both Cronbach alpha and composite reliability values were calculated to be greater than 0.70, confirming the reliability of the tool (Hemsworth et al., 2018).
ProQOL has been widely adopted. It has been translated into several languages and utilized in many fields, especially in healthcare (Galiana et al., 2017; Samson et al., 2016; Stamm, 2010). In fact, in a systematic review of CF in healthcare workers, ProQOL was utilized in 67 of 71 included studies (Cavanagh et al., 2020). ProQOL has been utilized in physicians, nurses, palliative care workers, and even medical interpreters (Baqeas et al., 2021; Cavanagh et al., 2020; James & Crawford, 2021; Mehus & Becher, 2016). While the tool has been widely adopted, some psychometric testing has demonstrated issues with the burnout and STS subscales in regards to their convergent validity (Galiana et al., 2017; Hemsworth et al., 2018; Samson et al., 2016; Sheppard, 2015).
Secondary Traumatic Stress Scale
The STSS was developed to assess the frequency of intrusion, avoidance, and arousal symptoms associated with the indirect exposure to traumatic events through professional helping relationships (Bride et al., 2004). An initial pool of Likert-scale style questions was developed by a panel of experts and subsequently pilot tested with social workers (Bride et al., 2004). Through several iterations, a 17-item self-administered tool was developed with each item corresponding to one of the DSM-IV symptoms of PTSD. These items were separated into three distinct subscales measuring intrusion, avoidance, and arousal symptoms (Bride et al., 2004).
Initial validity was determined through a survey of randomly selected social workers in the southeastern United States (Bride et al., 2004). Survey respondents were primarily Caucasian and female (Bride et al., 2004). The study examined convergent validity through examining the correlations of the total STSS score and the subscale scores of the individual respondents to the extent to which a respondent's clinical population is traumatized (extent), the frequency in which their work addresses traumatic stress of their clients (frequency), and the severity of depressive symptoms experienced by the respondent (Bride et al., 2004). Significant correlations were determined between each of the convergent variables; however, correlations between extent and frequency were of relatively low magnitude. Divergent validity was assessed through determining that there were no significant correlations between the STSS scale and subscales and age, income, and ethnicity. Finally, confirmatory factor analysis utilizing structural equation modeling techniques confirmed factor validity (Bride et al., 2004). Cronbach alpha for the 17-item scale was 0.94 and the Intrusion, Avoidance, and Arousal subscales had alphas of 0.83, 0.89, and 0.85, respectively (Bride et al., 2004).
While initially developed to measure STS in social workers, the STSS has been applied and validated in several other populations and translated into multiple languages (Beck & Gable, 2012; Jacobs et al., 2019; Kellogg et al., 2018; Molnar et al., 2020). The STSS has been used in healthcare workers, especially following the COVID-19 pandemic; however, it has not yet been applied to palliative care providers or medical interpreters. It has been utilized in sign language interpreters, but it has not undergone psychometric testing in that population (Russell et al., 2023).
Compassion Fatigue Short Scale
The Compassion Fatigue Short Scale (CF-SS) was designed to measure compassion fatigue through measuring both work burnout and secondary trauma (Adams et al., 2006). It was developed based on psychometric testing and factor analysis of the Compassion Fatigue Scale-Revised (CFS-R) in a group of randomly selected social workers in New York City following the 11 September 2001 attacks (Adams et al., 2006). A factor analysis determined that the CFS-R was measuring multiple underlying factors (Adams et al., 2006). Therefore, items were eliminated until only two factors remained, work burnout and secondary trauma. The CF-SS is a 13-item self-administered scale with two distinct subscales; an eight-item subscale measuring burnout and a five-item scale measuring secondary trauma (Adams et al., 2006). There was no discussion regarding stakeholder involvement regarding the development of the scale.
Initial validity was assessed through correlating the scales with each other and with stress exposure, psychological resource, and psychologic distress variables (Adams et al., 2006). Statistically significant correlation with existing validated tools demonstrated concurrent validity (Adams et al., 2006). Additionally, predictive validity was established throughout multivariate regression analyses which demonstrated the CF-SS, as well as the individual subscales, predicted psychologic distress (Adams et al., 2006). Factorial validity was established based on the factorial analysis complete to construct the CF-SS (Adams et al., 2006). Each subscale demonstrated good internal reliability with Cronbach alphas of 0.9 and 0.8 for the burnout and the secondary trauma scales, respectively (Adams et al., 2006). Cronbach alpha for the entire CF-SS was 0.9 (Adams et al., 2006).
Since its development, the CF-SS has been utilized in many populations and has been translated and validated in other languages (Rodrigues et al., 2023; Sun et al., 2016; Yıldırım & Cavcav, 2021). It has been utilized in many healthcare professions, including hospice nurses, but has not been utilized in other palliative care professionals or medical interpreters (Barnett & Ruiz, 2018). (Table 1).
Table of Measures of Compassion Fatigue and Secondary Traumatic Stress.
Discussion
This review presents three tools commonly used to measure CF or STS and discusses the psychometric properties of each tool to identify an appropriate tool to assess CF or STS in medical interpreters who participate in palliative care discussions. While all three tools, ProQOL, STSS, and CF-SS, have been utilized in several populations of healthcare professionals, none of the tools have been validated with medical interpreters. Additionally, all these tools were developed as screening tools for CF or STS and have been subsequently utilized as measurement tools (Adams et al., 2006; Bride et al., 2004, 2007; Stamm, 2010). Screening tools are intended to prevent false negative results, and therefore these tools may overestimate the true rate of CF or STS (Bride et al., 2007). Finally, no tool measures all aspects of CF (Bride et al., 2007). Given this, there are several benefits and drawbacks to utilizing each of these tools to investigate CF or STS in medical interpreters.
Based on this review, it's clear ProQOL that is the most widely accepted and utilized tool to measure CF, and it has even been utilized in studies of medical interpreters (James & Crawford, 2021). Additionally, it measures not only CF, but also compassion satisfaction, which has been shown to be inversely related to CF. Therefore, ProQOL may provide a fuller understanding of an individual's experience than the other tools. However, there have been several recent studies that have identified problems with ProQOL's validity, particularly related to the Burnout Scale and reverse-coded questions (Galiana et al., 2017; Hemsworth et al., 2018; Samson et al., 2016; Sheppard, 2015). ProQOL would benefit from a revision based on these findings prior to attempting to complete psychometric testing with medical interpreters.
The STSS and CF-SS have been less widely adopted than ProQOL; however, both have been demonstrated to be both valid and reliable in many populations. Additionally, they are both shorter instruments with STSS and CF-SS having 17 and 13 items respectively, compared to ProQOL's 30 items. STSS has been utilized in sign language interpreters, but not in spoken language interpreters and the CF-SS has not been utilized in any interpreter population (Russell et al., 2023). CF-SS accounts for both Burnout and Secondary Trauma in its measurement of CF, while STSS was developed to exclusively measure STS. This is reflective of one of the challenges related to CF research. There is no consensus on the definition of CF, and the terms CF and STS are frequently used interchangeably in the literature. This has resulted in several disparate tools to identify CF and STSS (Bride et al., 2007).
There are particular challenges and limitations in employing these tools in research of medical interpreters in palliative care with the unique roles and challenges medical interpreters. Given that interpreters may be a part of different cultural and ethnic groups than the tools have been developed and validated in, and therefore may not accurately measure CF or STS in individual interpreters. In qualitative research with medical interpreters in palliative care, there has been evidence of CF and STS reported. However, this has not been demonstrated in the limited attempts to measure CF with existing tools in medical interpreters (Graves et al., 2023; James & Crawford, 2021; Silva et al., 2020). None of these tools were developed with the input of medical interpreters, so it calls into question the ability to use the tools in their present form to measure CF or STS accurately in medical interpreters in palliative care encounters.
Conclusion
This review examines the psychometric properties of tools commonly used to measure CF and STS and discuss how these existing tools may be applied to research with medical interpreters participating in palliative care encounters. While ProQOL, STSS, and CF-SS have all been utilized in many populations of healthcare workers and in multiple languages, medical interpreters have not been a part of psychometric testing. ProQOL, while it remains the most widely adopted tool to measure CF, requires alterations to address concerns surrounding the validity of the measurement of CF. STSS only measures the secondary trauma component of CF, which likely does not capture the full range of factors impacting CF. The CF-SS is an intriguing option given its brevity and strong psychometric properties. However, it has not been as widely adopted as the other tools and has not been utilized in medical interpreters in the past.
Further research is needed regarding the validity of these tools in medical interpreters. Additionally, given the unique roles and challenges medical interpreters face, it may be beneficial to consider modifying existing tools with input of medical interpreters to measure the experience of CF or STS more accurately in this population. This would allow palliative care teams to accurately assess and work to mitigate CF and STS in medical interpreters, who are vital members of the interprofessional team for patients with LEP.
Footnotes
Acknowledgements
Thank you to Dr. Patricia Moyle Wright (University of Scranton) for your guidance and expertise in the preparation of this manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.