
Abstract
This study examined the association between Nurse Practitioner (NP) and Physician Assistant (PA) staffing in nursing homes and the effect of a decision aid regarding feeding options in dementia on the frequency of surrogate-provider discussions and on surrogates’ decisional conflict. We compared these outcomes for facilities that had no NPs/PAs, part-time-only NP/PA staffing, and full-time NP/PA staffing. The sample included 256 surrogate decision makers from 24 nursing homes. The decision aid was associated with significant increases in discussion rates in facilities with part-time or no NP/PA staffing (26% vs. 51%, p < .001, and 13% vs. 41%, p < .001, respectively) and decreases in decisional conflict scores (−0.08 vs. −0.047, p = .008, and −0.30 vs. −0.68, p = .014, respectively). Sites with full-time NP/PA staffing had high baseline rates of discussions (41%). These findings suggest that the decision aid and full-time NP/PA staffing can enhance surrogate decision making in nursing homes.
Introduction and Background
Many persons with advanced dementia receive end-of-life care in nursing homes (Houttekier et al., 2010; Mitchell, Teno, Miller, & Mor, 2005). Among the many major treatment decisions, the need to make feeding-related decisions for persons with advanced dementia occurs frequently in this setting. These decisions frequently are made by family members who serve as surrogate, or proxy, decision makers because persons with advanced dementia are unable to consider the options and make a reasoned choice.
Feeding problems are extremely common in persons with advanced dementia and are associated with increased mortality (Mitchell et al., 2009). Options for addressing feeding difficulties range from insertion of a feeding tube to hand-feeding with modified diets or comfort measures. Despite the frequency with which these decisions need to be made, many surrogates report feeling unprepared and unsupported when considering and choosing feeding strategies for persons with advanced dementia (Lewis et al., 2006). This creates unnecessary stress and uncertainty for families and care providers when changes in the residents’ status occur.
This state of uncertainty when faced with a decision that needs to be made is known as decisional conflict. Decisional conflict, as operationalized by O’Connor, describes a state in which a person needs to decide on a course of action that involves risk, uncertainty of outcomes, and/or the potential for regret related to the final decision made. Decisional conflict can result in overall indecision about choices, delays in making a needed decision, and increased stress and decisional regret (Givens, Lopez, Mazor, & Mitchell, 2011; Hickman, Daly, & Lee, 2011; O’Connor, 1993; Wetle, Shield, Teno, Miller, & Welch, 2005).
According to Janis and Mann’s (1977) classic model, decisional conflict can be mitigated by adhering to a stepwise information processing strategy in which the decision maker carefully identifies all options, considers the objectives of the decision (e.g., cure, comfort), carefully weighs all potential risks and benefits of each option, and develops contingency plans if the potential risks materialize. Decision aids have been used in many clinical settings and across a wide range of situations; their effectiveness in enhancing the quality of decision making and decreasing decisional conflict is well established (O’Connor et al., 2007; Stacey et al., 2011). These aids may be used alone or incorporated into a multifaceted intervention to enhance decision making. Mitchell, Tetroe, and O’Connor (2001) developed a decision aid for long-term feeding tube use targeted at surrogates of cognitively impaired older persons. Recently, Hanson et al. (2011) tested an adapted version of Mitchell’s decision aid and found that surrogates who received the decision aid had lower Decisional Conflict Scale (DCS) scores and were more likely to discuss feeding options with a health care provider. The study described in this article is a secondary analysis of the Hanson et al.’s data.
In addition to the use of decision aids, involvement of nursing home–based nurse practitioners (NPs) and physician assistants (PAs) may increase the number of discussions about feeding options, as well as surrogates’ confidence and certainty about their decisions. NPs and PAs have similar roles in nursing homes despite important differences in their educational preparation, regulation by professional organizations, and state laws (Intrator et al., 2005; Mittman, Cawley, & Fenn, 2002). These two provider types are often viewed as one group by regulatory bodies and researchers (American Academy of Phyiscian Assistants, 2011; Intrator et al, 2005; Teno et al., 2011). In addition to evaluating residents and directing treatment, these providers also meet with residents’ families to discuss concerns and answer questions regarding residents’ health status and care (American Academy of Physician Assistants, 2011; American Medical Directors Association, 2011; Mittman et al., 2002). In addition, NPs provide extensive education to residents, their families, and staff members, and they spend more time overall with residents than physicians (Bakerjian, 2008; Bourbonniere & Evans, 2002). The NP/PA role requires good communication skills and the ability to skillfully guide discussions about goals of care and treatment options with residents, families, and nursing home staff (American Association of Colleges of Nursing, 2010; American Medical Directors Association, 2011).
Although the empirical literature on PAs is limited, a recent review of care provided by NPs supports a significant, positive association between utilization of NPs in nursing homes and improved quality of care and reduced hospitalizations (Bakerjian, 2008). There also is some support for the relationship between NP/PA staffing and improved decision making. Teno et al. (2011) reported that NP/PA staffing in nursing homes is associated with decreased terminal hospitalizations. Resnick and Andrews (2002) found that an NP-initiated intervention to educate cognitively intact residents about advanced directives and end-of-life treatment preferences resulted in a 53% increase in identification of residents’ preferences and completed advanced directives when compared to baseline data.
Purpose of the Study
The purpose of this study was to examine how NP/PA staffing influences the effect of a decision aid on the number of surrogates having at least one discussion about feeding options in dementia and on surrogates’ decisional conflict regarding feeding options. We hypothesized that higher NP/PA staffing in the facility would enhance the effect of the intervention. Figure 1 outlines the study variables and their hypothesized relationships.
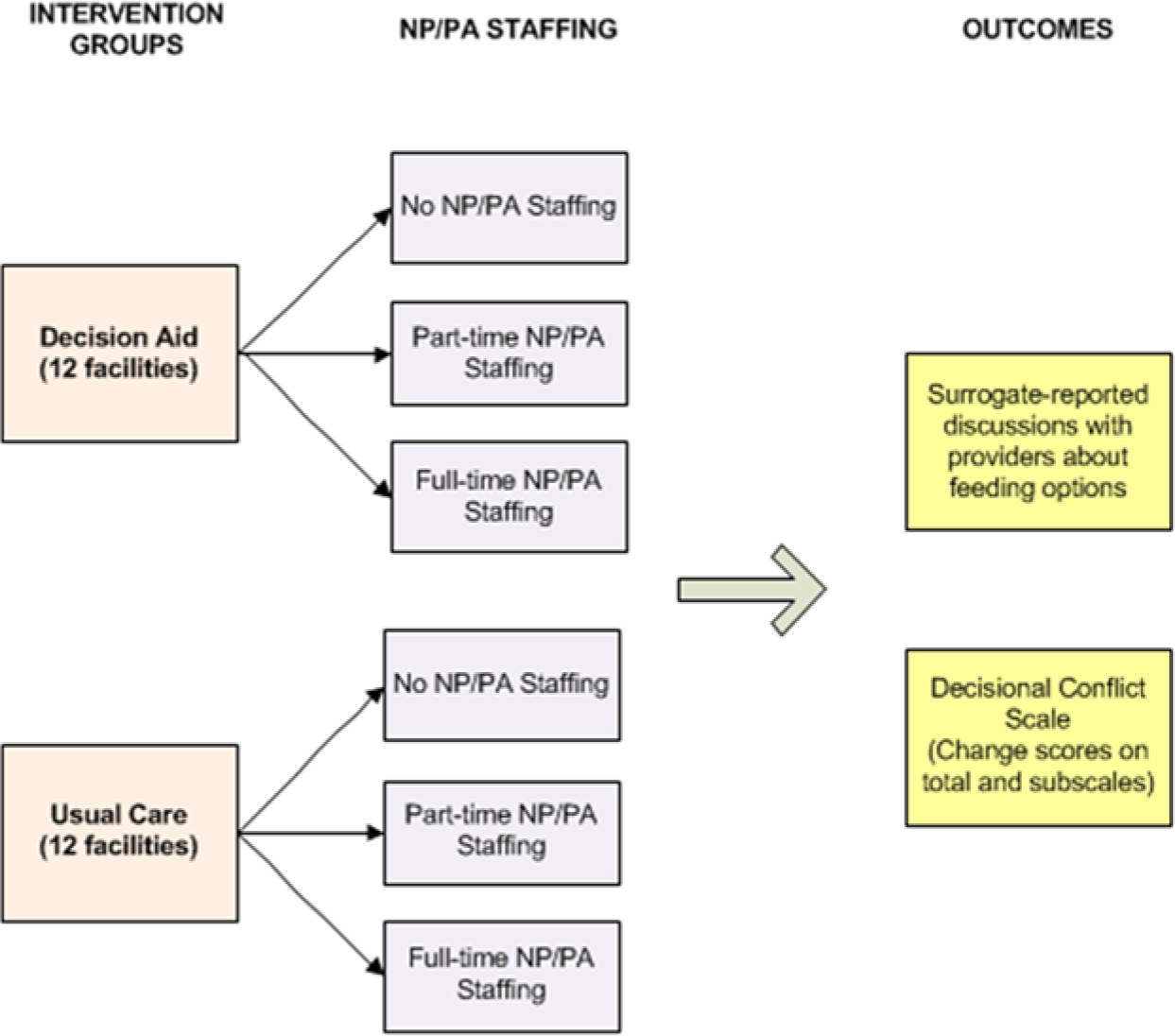
Analytic schema.
Method
Study Design
Data for this study came from a cluster randomized controlled trial (RCT) that examined the efficacy of a decision aid in enhancing the frequency of discussions about feeding options and in decreasing surrogates’ decisional conflict as they relate to tube feeding, assisted oral feeding, and comfort measures for persons with advanced dementia. The intervention group was compared with a usual care control group in 24 North Carolina nursing homes. Study enrollment occurred from August 2007 to July 2009 (Hanson, Gilliam, & Lee, 2010). The main outcome variables included the overall and subscale scores on the DCS and surrogate-reported frequency of discussions with providers about feeding options, both measured at 3 months postintervention. More detailed information regarding study procedures of the parent grant is available elsewhere (Hanson et al., 2011, 2010).
Sample and Setting
Participants were dyads of nursing home residents with advanced dementia and their surrogate decision-makers. Eligibility criteria for residents were: aged ≥ 65, advanced dementia (as defined as a documented diagnosis of dementia and Global Deterioration Scale [GDS] stage 6-7), and documented poor intake, dysphagia, or weight loss. Residents were excluded if they had a feeding tube or a “Do Not Tube Feed” order, were receiving hospice care, or had weight loss attributed to diuresis. Eligible surrogates were guardians or Health Care Powers of Attorney or primary family contacts who reported they were the person most likely to be involved in clinical decision making. Surrogates were excluded if they were unable to speak English.
For this analysis, the resident–surrogate dyads were stratified by NP/PA staffing. That is, resident and surrogate data were grouped within facilities that were characterized by having no NP/PA staff, part-time NP/PA staffing, and full-time NP/PA staffing.
Surrogate decision makers provided written informed consent for themselves and for review of the resident’s medical records; all interview data were from surrogates. All research procedures were approved by the Institutional Review Boards (IRB) of the University of North Carolina, Alamance Regional Hospital, and East Carolina University.
Variables and Measures
Independent Variables
NP/PA staffing
Study liaisons, usually a nurse manager or social worker, from each of the 24 participating facilities completed an organizational survey at the onset of their involvement in the study. One of the questions was, “Do you have a nurse practitioner or a physician assistant who sees patients here?” If answered in the affirmative, the liaison was to indicate whether the practitioner was a PA or NP, and if she or he was working full- or part-time. Facility liaisons reported NPs’/PAs’ full- or part-time status based on their own definition and involvement of the providers.
Intervention: Decision aid
At the time of enrollment, the intervention group received the printed decision aid from research assistants who encouraged surrogates to review it and then to discuss it with a health care provider. Research assistants were trained not to provide additional information about the decision aid or its content. The decision aid presented information about dementia, feeding options, and the advantages and disadvantages of feeding tubes or assisted oral feeding. It was adapted from Mitchell’s decision aid by updating the content, adding information on oral feeding options, and ensuring content was at a sixth grade reading level (Mitchell et al., 2001). The aid was available in printed format or could be viewed on a computer screen with the recorded text available for listening. There was no follow-up (except for data collection) or additional support provided by the research team (Hanson et al., 2011). The purpose of the decision aid was to increase surrogates’ knowledge and confidence in making decisions about feeding options, and thus, significantly decrease decisional conflict. It was also expected that the decision aid would help surrogates recognize that these decisions needed to be discussed with health care providers.
Facility and surrogate characteristics
Facility characteristics (other than the independent variable, NP/PA staffing) included organization- (e.g., ownership, number of beds, number of deficiencies, staffing hours, 5-star quality rating) and resident-level (percentage of residents who are African American and/or have a “Do Not Resuscitate” order, weight loss, or a feeding tube) characteristics. Sources for facility information were the Nursing Home Compare website, Centers for Medicare and Medicaid Services’ Online Survey, Certification and Reporting (OSCAR), and a survey that was completed by the facility liaison for the study.
Surrogates’ demographic data, including race, relationship to resident, and religion, were collected through in-person interviews at enrollment, and outcome measures were collected in telephone interviews at 3 months. These variables were used to describe the sample and also to identify potential factors that could confound study results. For example, nursing home characteristics such as staffing have an impact on choices that surrogates make about end-of-life care (Lopez, Amella, Strumpf, Teno, & Mitchell, 2010; Mitchell, Teno, Roy, Kabumoto, & Mor, 2003) and residents’ race and religion are associated with differences in end-of-life decision making, including feeding tube use (Clarfield et al., 2006; Modi, Velde, & Gessert, 2011).
Dependent Variables
Surrogate-reported discussions about feeding options
Although the intervention did not involve providers, the decision aid was designed to stimulate discussions with providers who may not independently initiate these discussions with surrogates. Thus, increasing the frequency of discussions about feeding options was an expected outcome. To measure this variable, research assistants interviewed surrogates by phone and asked them to report whether or not they had had a discussion about feeding options with treating physicians, NPs, PAs, or nursing home staff in the preceding 3 months. Responses were recorded as “yes” or “no.”
Decisional conflict
This variable was measured using the 16-item DCS. This validated instrument elicits information about decision makers’ (a) uncertainty in making a particular health care choice (Uncertainty subscale); (b) modifiable factors, such as lack of information and ambiguous values that contribute to uncertainty (factors contributing to Uncertainty subscale); and (c) perceptions about the effectiveness of decision making (Effective Decision-Making subscale). The DCS uses a 5-point Likert-type scale ranging from 1 = strongly disagree to 5 = strongly agree, with higher scores indicating greater decisional conflict, after recoding the scores for five negative statements. On the subscales, higher scores indicate (a) extreme uncertainty about the best choice, (b) feelings about the decision, and (c) the perception that the decision was a bad choice (O’Connor, 1993). The DCS has an overall test–retest reliability coefficient of .81 (O’Connor, 1995). Song and Sereika (2006) provided additional evidence for the scale’s convergent and discriminant validity. This and other outcomes were measured during 3-month follow-up interviews with surrogate decision makers. After being asked to reflect on feeding options for the person with dementia, surrogates reported their level of decisional conflict. We used change in DCS scores from baseline to 3 months for all analyses.
Statistical Analyses
Descriptive statistics were calculated for all variables and presented as mean ± standard deviation (SD) for numerical variables and as percentages for categorical variables. We compared the three NP/PA staffing categories (full-time NP/PA, part-time NP/PA, no NP/NP) on resident participants’ demographic and facility-level data using one-way analysis of variance (ANOVA) to compare continuous variables and chi-square tests to compare categorical variables. For ANOVA tests for which there was a significant omnibus F statistic, we conducted pairwise comparisons using the nursing home with full-time NP/PA staffing as a reference category. When comparing variables in proportions such as percentage of residents who are African Americans, with a DNR, had a feeding tube, and with weight loss, we used a total bed size as a weight variable to offset the effect of various nursing home sizes. Homogeneity tests and graphical methods were used to assess the underlying statistical assumptions.
To examine the association of the intervention and nursing home NP/PA staffing on the outcomes, we first tested the significance of the intervention on the dependent variables: discussions about feeding options with PCPs and changes in DCS scores (i.e., total and subscale scores), stratified by the three categories of NP/PA staffing. We then further adjusted the analysis by including facility-level characteristics as well as resident and surrogate-level covariates, in a multilevel modeling framework that takes into account nested sources of variability within nursing homes. However, because of the small number of nursing homes in the study, we relied on robust variance estimation to obtain unbiased hypothesis tests in either least square regression (for decisional conflict) or logistic regression (for frequency of discussion). All p values were calculated by adjusting for nursing home intraclass correlation, and we considered a statistical test with p ≤ .05 as significant. All analyses were conducted using STATA (Stata Statistical Software: Release 10. College Station, TX: StataCorp LP).
Results
A total of 256 dyads in 24 facilities were stratified into 3 categories based on NP/PA staffing and then compared as control and intervention groups across the dependent variables, Seven facilities reported having no NP/PA staffing, nine reported having at least one part-time NP/PA, and eight reported full-time NP/PA staffing.
Table 1 compares facility characteristics among the three NP/PA staffing categories. At baseline, facilities with full-time, part-time, or no NP/PA staffing differed significantly on three resident-level characteristics: race, percentage of residents with chewing and/or swallowing difficulties, and percentage with poor intake. Facilities with full-time NPs/PAs had fewer minority residents, lower tube feeding rates, more residents with DNRs in place, and fewer deficiencies. Surrogate characteristics among the three NP/PA staffing categories were similar, with the exception that, like their residents, surrogates in facilities with full-time NPs/PAs were more likely to be white (85% vs. 62% vs. 58%; p < .0001).
Nursing Home Characteristics by Nurse Practitioner/Physician Assistant Staffing.
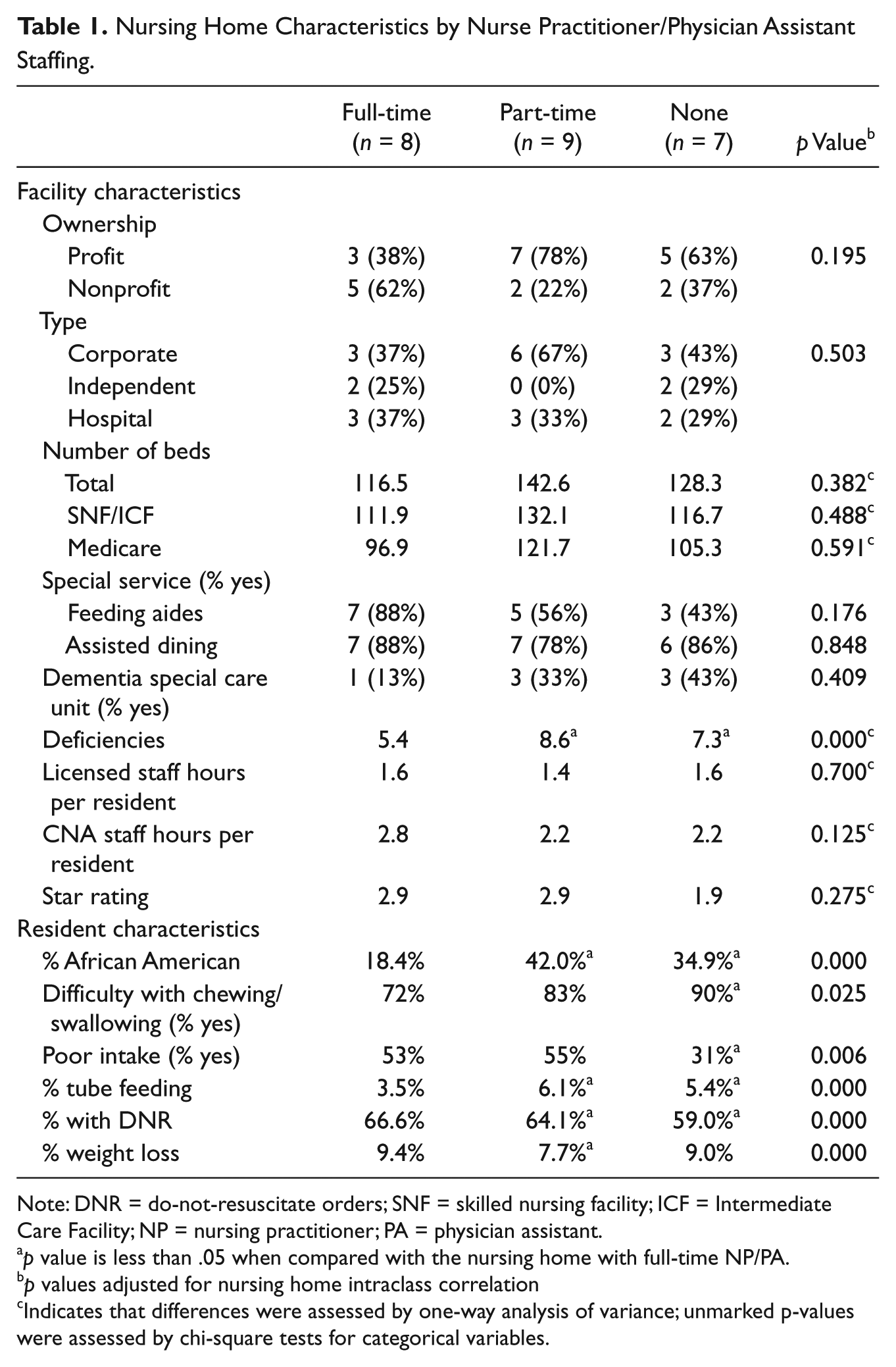
Note: DNR = do-not-resuscitate orders; SNF = skilled nursing facility; ICF = Intermediate Care Facility; NP = nursing practitioner; PA = physician assistant.
p value is less than .05 when compared with the nursing home with full-time NP/PA.
p values adjusted for nursing home intraclass correlation
Indicates that differences were assessed by one-way analysis of variance; unmarked p-values were assessed by chi-square tests for categorical variables.
Table 2 presents the 3-month outcomes for the intervention and control groups across the three NP/PA staffing categories. In facilities with full-time NP/PA staffing, surrogates reported relatively high rates of discussion about feeding options, and there was no difference between intervention and control groups (46% vs. 41%, p = .450). In facilities with part-time and no NP/PA staffing, the intervention was associated with significant increases in percent of surrogates reporting having at least one discussion about feeding options with a PCP (26% vs. 51%, p < .001, and 13% vs. 41%, p ≤ .001, respectively). Decisional conflict scores decreased over 3 months in both intervention and control groups, and across all NP/PA staffing categories, but was statistically significant in the facilities with part-time and no NP/PA staffing.
Effect of the Intervention on Study Outcomes at 3 Months’ Follow-up, Stratified by NP/PA Staffing.
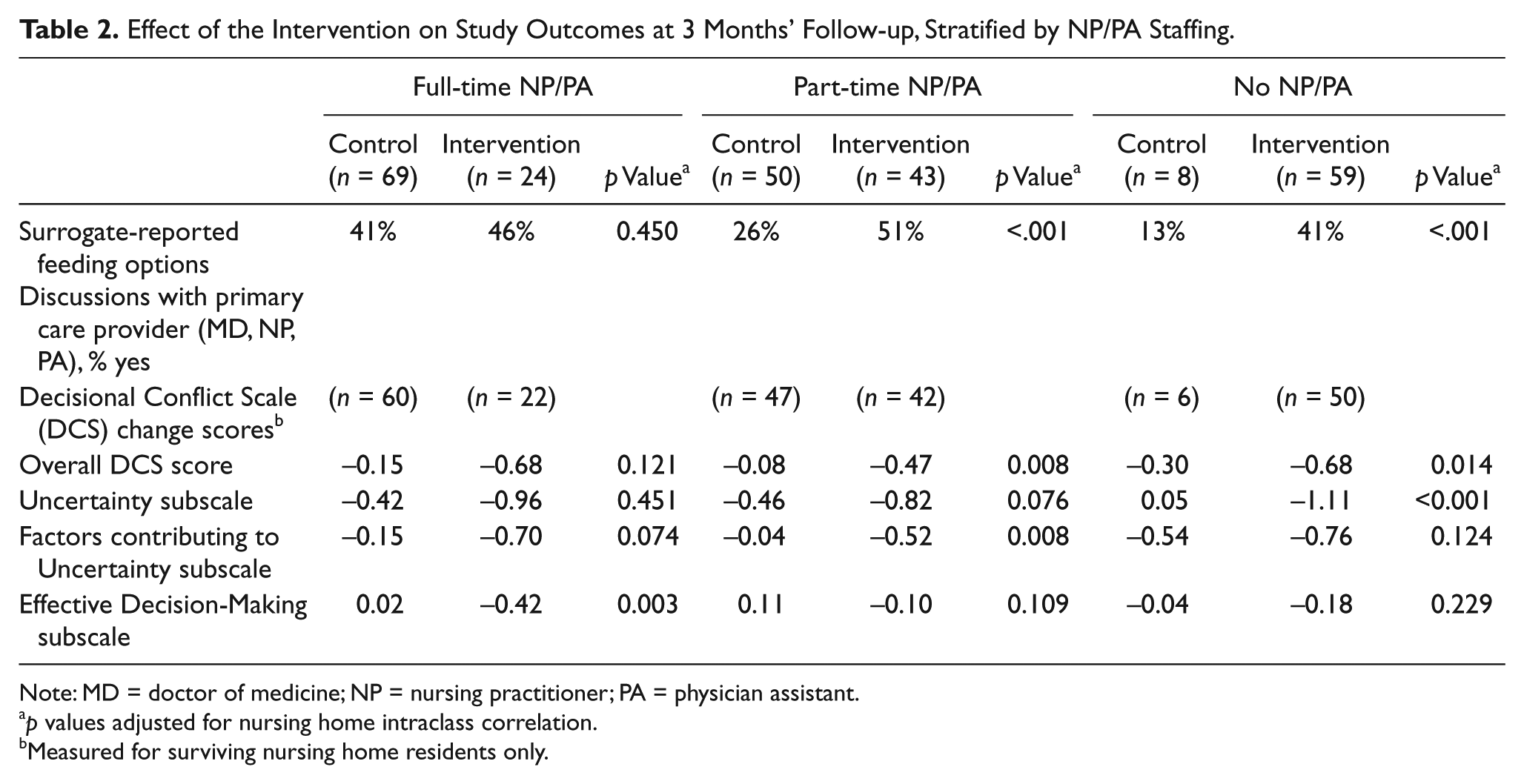
Note: MD = doctor of medicine; NP = nursing practitioner; PA = physician assistant.
p values adjusted for nursing home intraclass correlation.
Measured for surviving nursing home residents only.
To adjust for other differences across sites besides NP/PA staffing, the results of the multilevel regression that incorporated both facility and surrogate covariates are presented in Table 3. The outcomes reflect the percentage of surrogates who reported having at least one conversation about feeding decisions with PCPs, and total and subscale change scores for the DCS. After controlling for the covariates, the intervention no longer had a significant effect on feeding discussions. Part-time and no NP/PA staffing showed a negative association with discussions of feeding options. However, the significant interaction between intervention and NP/PA staffing suggests that the intervention had a greater effect in homes with no or part-time NPs/PAs than in those with full-time NPs/PAs. In the second regression model, NP/PA staffing did not affect overall DCS change or its three subscales. In contrast to the findings about feeding discussions, only the intervention had a significant effect on total and two subscale DCS scores (effective decision making, factors contributing to Uncertainty subscale). Neither the facility type nor the interaction between the intervention and facility type (data not shown) had statistically significant effects on DCS scores.
Multilevel Analyses to Predict Outcomes at 3 Months a .
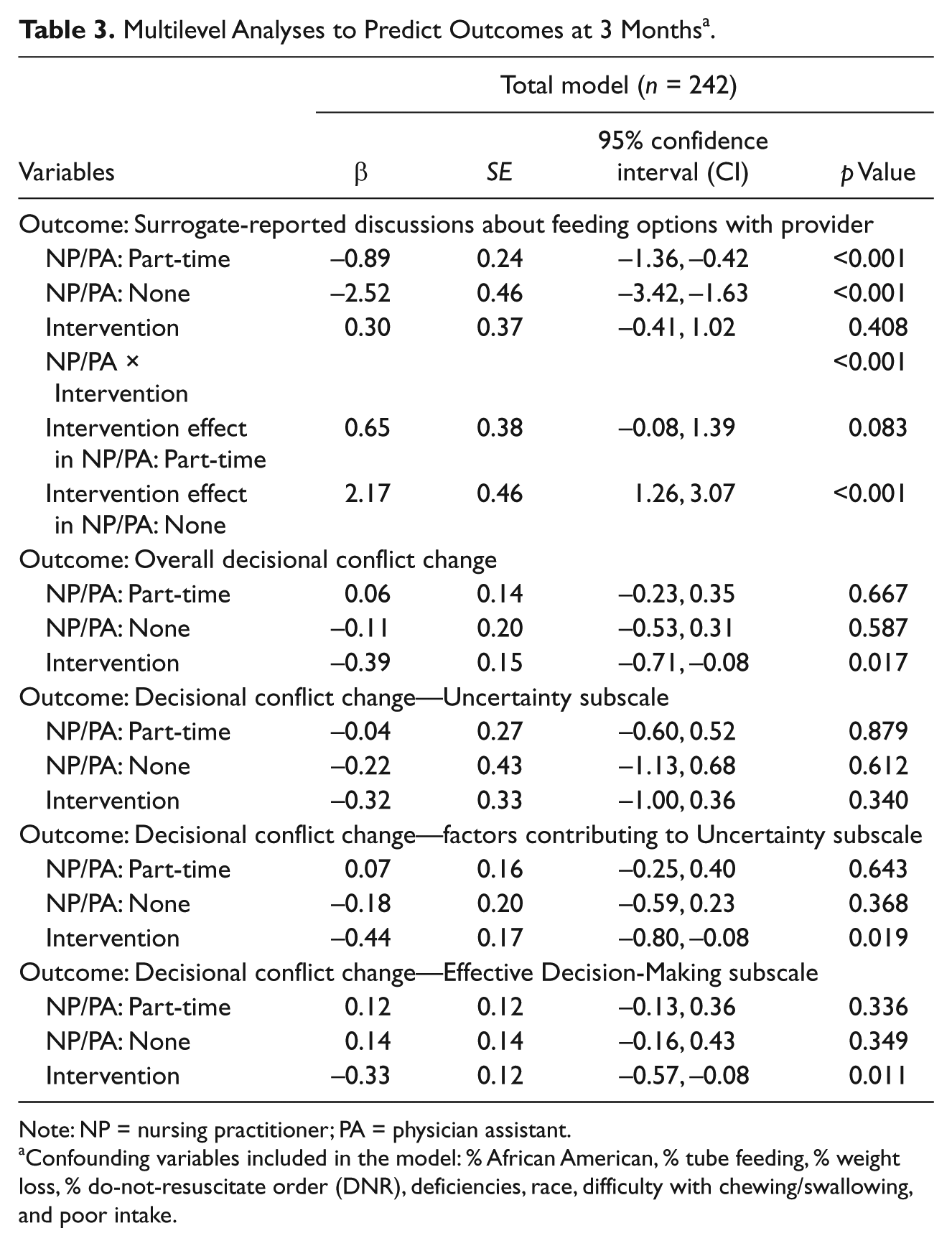
Note: NP = nursing practitioner; PA = physician assistant.
Confounding variables included in the model: % African American, % tube feeding, % weight loss, % do-not-resuscitate order (DNR), deficiencies, race, difficulty with chewing/swallowing, and poor intake.
Discussion and Implications
Studies have demonstrated that decision aids are effective in reducing decisional conflict in surrogates and in increasing discussions about important health care decisions between surrogates and providers. Designed to augment rather than to replace the role of the provider, the results from this study suggest that the level of NP/PA staffing does have a positive effect on the percent of surrogates who discuss feeding options for residents with dementia. Thus, the decision aid had a dramatic, positive effect on the frequency of discussions about feeding options in facilities with part-time or no NP/PA staffing, but little effect in nursing homes with full-time NP/PA staffing. This may have been due to the high background rates of discussion present in our sample of nursing homes, reflected by a rate of 41% in control sites with full-time NP/PA staffing. NPs and PAs may be more likely to provide expert education and engage surrogates and residents in discussions about goals of care, including discussions of feeding options, which is consistent with findings from other studies (Bourbonniere & Evans, 2002; Teno et al., 2011). This more intensive interaction may result in more frequent or more in-depth discussions about treatment preferences, which in turn may limit the need for clinical communication tools such as decision aids. Thus, implementing and distributing decision aids may be more beneficial when targeting facilities that lack full-time NP/PA staffing. In facilities that lack full-time NP/PA staffing, decision support may add significantly to the families’ discussion of feeding options with providers.
That the intervention, but not NP/PA staffing, was associated with significant decreases in decisional conflict suggests that the quality of support for surrogate decision making and subsequent decisions about feeding options could be enhanced in nursing homes regardless of NP/PA staffing patterns. Our multivariate analysis controlled for several resident and organizational factors that differed among facilities with no NPs/PAs, part-time NPs/PAs, and full-time NPs/PAs. Facilities with full-time NP/PA staffing had significantly lower tube feeding rates, fewer deficiencies, and higher percentages of documented DNR orders (Table 2), suggesting higher quality of care in these facilities. This association between better outcomes and NP staffing is consistent with other studies (Bakerjian, 2008; Kane et al., 1991; Mitchell et al., 2003; Teno et al., 2011).
Study limitations need to be acknowledged. One major problem was an imbalance among the three categories of NP/PA staffing. Though the numbers of facilities in each of the three staffing patterns were similar, the patients allocated to intervention and control were not; for example, in full-time NP/PA staffing, out of 95 patients, 71 were in control group and 24 in intervention. In the no-NP/PA category, 11 were in control and 60 in intervention. If the focus of the primary study had been on NP/PA staffing, these imbalances would have been minimized by managing intervention and control facilities on this characteristic. Because this study was a secondary analysis, this matching did not occur. These disparities in sample size may cause problems in interpreting the results due to skewed randomization; however, we adjusted for baseline difference and for intraclass correlation in our analyses. In addition, the measure of NP/PA staffing may lack precision, since surveys that were completed by facility liaisons were not evaluated for accuracy. Finally, the surrogates’ discussions with health care providers about feeding options were measured by asking surrogates to recall if these discussions had occurred in the previous three months, but there was no independent verification of the accuracy of these reports.
Despite the limitations, this study has important clinical implications. First, the decision aid can be used in nursing homes to enhance the quality of discussions and decisions about feeding options including feeding tube use. Decision aids regarding feeding options, specifically for dementia residents, can be easily supplied to surrogates. Surrogates who are exposed to decision aids will be supplied with current evidence-based information that can increase their personal knowledge of the topic. Accurate knowledge can facilitate conversations with providers, prompt additional questions, and ease the decision-making process (Hanson et al., 2011; O’Connor, 1993). Second, a decision aid may have greater impact in facilities with no- or part-time NP/PA staffing because it could increase the frequency of discussions about feeding options between surrogates and physicians and other providers. Surrogates who have a decision aid may feel that they have a positive source of support in their decision-making, and they may make an effort to seek out meeting times with providers for discussions. Third, findings from this study suggest that NPs and PAs may enhance the quality of palliative care through improved communication in nursing homes. Medical directors can be instrumental in expanding teams to include NPs and PAs who can augment physician visits and provide greater availability of skilled professional caregiving to nursing home residents and their surrogates.
Conclusion
This study provides empirical evidence that a decision aid for feeding options in residents with advanced dementia is beneficial. Moreover, the decision aid intervention was found to be most effective in nursing homes where there were part-time NPs/PAs or no NP/PA staffing. Sites with full-time NP/PA staffing had higher surrogate-reported discussions about feeding options at baseline, resulting in less opportunity for improvement with the decision aid. Future studies should examine whether combining NP/PA engagement and training with decision aids further increases the number of discussions between surrogates and providers about feeding options and decreases surrogates’ decisional conflict. A randomized controlled trial will address the methodological and analytic limitations that were encountered in this secondary analysis, such as imbalance among the three categories of NP/PA staffing and lack of precision in the measurement of certain study variables. The potential positive impact of involving NPs and PAs in a decision aid trial merits further investigation.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views, positions, or policies of the National Institute of Nursing Research, the National Institutes of Health, the Department of Veterans Affairs or the United States government. This material is the result of work supported with resources and the use of facilities at the Philadelphia Veterans Affairs Medical Center in Pennsylvania.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by Award Number RO1NR009826 from the National Institute of Nursing Research. JSS was supported by a Jonas Hartford Scholarship.