
Abstract
This purpose of this mixed methods study was to understand access to primary care among older adults who present to an inner city emergency department (ED) for nonurgent care. Questionnaires (N = 62) included demographic, illness characteristics, and health care utilization. Qualitative interviews (N = 20) were conducted. Data was analyzed using descriptive statistics, and qualitative methodology. More than half of the participants were female (60%), African American (57%) and pain was the presenting symptoms among 48% of the participants. Nearly all participants reported barriers to primary care; difficulty with phone systems and staff, and lack of available appointments resulting in an ED visit. Older adults face barriers accessing primary care and as a result, can turn to the ED for their primary care needs. Interventions to improve access for vulnerable older adults might have benefits not only for patient outcomes but also for health policy issues related to cost effective care and overcrowded EDs.
Introduction and Problem
The population of older adults, those 65 and over was 40.4 million in 2010, which is the most recent data available. They represent 13.1% of the population and over the next two decades this number is expected to increase by 31% (Administration on Aging, 2011). Along with increased longevity, older adults may have a greater burden of chronic illness and disability. Prompt access to primary care is critical for older adults and often available (Cheung, Ginde, Lowe, & Wiler, 2012). Despite most U.S. older adults having healthcare coverage under the Medicare program, it has been shown that older adults experience disparities in access to primary care services (Thorpe, Thorpe, Kennelty, & Pandhi, 2011). Barriers to care impact the prevention and management of chronic illness (Ryvicker, Gallo & Fahs, 2012).
The use of emergency departments (EDs) has been steadily rising, while the number of EDs available has been declining (Institute of Medicine, 2006). According to the National Hospital Ambulatory Medical Care Survey, between 1997 and 2007, the number of emergency department) visits in the United States between 1997 and 2007 increased from 94.9 million to 116.8 million, an increase of 23.1%, with the poor and older adults having the highest use (National Center for Health Statistics, 2011).
One of the areas of concern is the increased use of the ED for nonurgent care (Hoot & Aronsky, 2008). A nonurgent visit is usually considered to be a visit that does not require immediate care and can be treated in an ambulatory or primary care setting (Afilalo et al., 2004). It has been suggested that patients who use the ED frequently for nonurgent care lack timely healthcare access (D’Avolio, Feldman, Mitchell, & Strumpf, 2008; Thorpe, Thorpe, Kennelty, & Pandhi, 2011). There is widespread evidence that timely access to healthcare is essential to achieving healthy aging and managing chronic illness (Institute of Medicine, 2008). Therefore, the increased ED visits by older adults for nonurgent care is an area of significant concern because hospital emergency departments were not designed or equipped to provide primary care services to patients (Institute of Medicine, 2006). In addition, utilizing the ED for nonurgent care is expensive. The average cost of an ED visit is US$975 compared to US$250 for a primary care visit (Massachusetts Division of Health Care Finance and Policy, 2012).
Research has indicated that the increased use of the ED by older adults for nonurgent care can significantly contribute to the already existing problem of ED overcrowding and higher costs (Kaskie et al., 2010). Older adults also experience high rates of adverse outcomes and lack of continuity of care after ED discharge, (Aminzadeh & Dalziel, 2002). The typical cost of an ED visit is more than double the cost of a primary care visit. Older adults tend to have chronic illnesses, cognitive deficits, and functional impairment (McCusker, Karp, Cardin, Durand, & Morin, 2003). These types of conditions require continuity of care by primary care providers. EDs can be chaotic, overcrowded, and understaffed. Older adults have reported negative staff interactions and confusion with discharge instructions (Afilalo et al., 2004; Aminzadeh & Dalziel, 2002).
The conceptual frameworks that guided this study were the Vulnerable Populations Model and Anderson Behavioral Model. The Vulnerable Populations Model claims that there are relationships among resources, risk, and health. The lack of adequate environmental and socioeconomic resources can lead to vulnerabilities among certain groups. It defines vulnerable populations as those who have limited resources and, as a result, are at increased risk for morbidity and mortality (Flaskerud & Winslow, 1998; Aday, 1994). The Andersen’s behavioral model is a conceptual model frequently used to explain variation and utilization in healthcare access and services (Andersen, 2008). However, the behavioral model has not explicitly explained ED utilization among inner city older adults (McCusker et al., 2003).
As the use of the ED by older adults continues to increase, little research has been done regarding older adults’ experiences accessing care which in turn can lead to nonurgent ED visits. Having an understanding of their access experiences may lead to interventions to improve access to care for vulnerable older adults. The objective of this study is to describe older adults’ experiences in accessing healthcare services.
Purpose of the Study
The purpose of this study was to understand why older adults with nonurgent illnesses utilize the ED and their experiences in accessing primary care. This study extends a previously conducted study, which explored quantitatively, factors associated with access to care and health-related quality of life (D’Avolio et al., 2008).
Design
A mixed method descriptive design was used to explore older adults’ use of the ED and experiences in accessing care. The quantitative survey assessed demographic information, healthcare utilization, and access to primary care. Participants (N = 62) completed the survey and data were analyzed using descriptive statistics. During the initial enrollment, participants were asked to complete a survey and in-depth interviews. The first 20 participants completed the quantitative surveys and in-depth interviews and after these interviews were conducted, themes and categories became repetitive and redundant. It was then determined that interview data was saturated. Thus after the first 20 participants, the remainder of participants completed the survey tool and were not asked to participate in the in-depth interviews. A qualitative methods approach was essential to collect rich and detailed descriptions of access experiences from a purposely selected sample of older adults using in-depth interviews. Qualitative content analysis methods were used and as is recommended for qualitative studies, data analysis and collection proceeded simultaneously. A qualitative approach to this type of data collection is highly effective in understanding perceptions, beliefs, opinions, and attitudes of individuals when examining topics previously unexplored (Sandelowski, 2000; Sandelowski, 2010). In summary, older adults who seek nonurgent care in the ED are a vulnerable group. Gaining the older adults’ perspective into their access needs may provide insight into how primary care systems can more effectively provide nonurgent care when it is needed.
Setting and Sample
The setting for this study was a Northeastern U.S. inner city ED in a federally designated, safety net hospital with a mission to provide care to vulnerable patients. This study was conducted among older adults who presented to an inner city ED for nonurgent care. A safety net healthcare organization is one that services a significant portion of uninsured or underinsured Medicaid, and other vulnerable populations (Institute of Medicine, 2003). To explore why older adults seek care in the emergency department for nonacute care, a purposive sample of older adults, in nonacute area of the ED were enrolled in the study. In-depth qualitative interviews were conducted among the participants until qualitative data was saturated (N = 20). Participants’ ED visits were classified by acuity status (e.g. nonacute, acute) according to established ED triage criteria.
Inclusion criteria included age greater than or equal to 65 years, nonacute reason for an ED visit, and English, Haitian Creole, and Spanish older adults. The languages to include were based on a prior study in the emergency department which revealed that the predominant languages of non-English speaking older adults were Haitian Creole and Spanish (D’Avolio et al., 2008). In addition, bilingual community experts were consulted to provide guidance and review the translated study tools. Interpreters enrolled and conducted interviews with non-English speaking participants. Exclusion criteria included those who were transferred from an inpatient setting, psychiatric conditions, cognitive impairment, or sensitive issues such as elder abuse. The institutional review boards approved the study and written informed consent was obtained from all study participants.
Method
Procedures and Instruments
Three trained research assistants screened nonurgent ED patients, aged 65 years and older for inclusion and exclusion criteria and obtained written informed consent from eligible participants.
Interviews took place in a private room in the nonurgent department of the ED, either before or after medical evaluation. Interviews were digitally recorded, along with written field notes of observations and thoughts immediately following the interviews, which ranged from 20 to 40 min. The interview guide was pilot tested to ensure that all areas of interest were explored. It consisted of five open-ended probe questions. An example of a question is “When you are sick, how do you arrange an appointment to see your healthcare provider?” This guide encouraged the participants to share their experiences and perceptions with accessing their primary care providers.
Demographic data were collected using standardized questionnaires that included the following: age, ethnicity, income, health insurance coverage, and access to care. Access to care was measured using variables related to healthcare utilization and the ability to access care when needed. Participants were asked if they had a regular source of healthcare and if they were unable to get a healthcare appointment. In addition, they were asked if they had an ED visit or hospitalization in the past 12 months and if they had attempted to call their healthcare provider before coming to the ED.
Data Analysis
The characteristics of the participants and presenting symptoms were analyzed descriptively using SPSS version 16.0 (IBM, 2011). All recorded interviews were transcribed verbatim, checked for accuracy and imported into QRS Nvivo (QRS International, 2000). Data were then analyzed by the first author. The number of in-depth interviews was determined by data redundancy and saturation (LeCompte & Schensul, 1999). The qualitative data were saturated when 20 interviews were obtained. Qualitative content analysis methods were used for data gathering and analysis (Sandelowski, 2000). Transcripts were reviewed and proofed by the principal investigator (PI). Before coding, the PI read and reread the transcripts while listening to the audiotapes. Analysis was focused on identifying and categorizing each participant’s interviews. This process began with open coding in which categories were freely generated. Categories were then created to describe concepts in the data. After open coding, subcategories with similar events and incidents were grouped together as categories and then grouped under higher order category headings (Graneheim & Lundman, 2004). Member checking was performed by asking participants to validate impressions and preliminary findings to confirm, clarify, or discuss additional information (Lincoln & Guba, 1985). An expert in qualitative analysis served as a peer debriefer and reviewed the analysis and descriptive summary (Lincoln & Guba, 1985).
Results
Characteristics of Participants
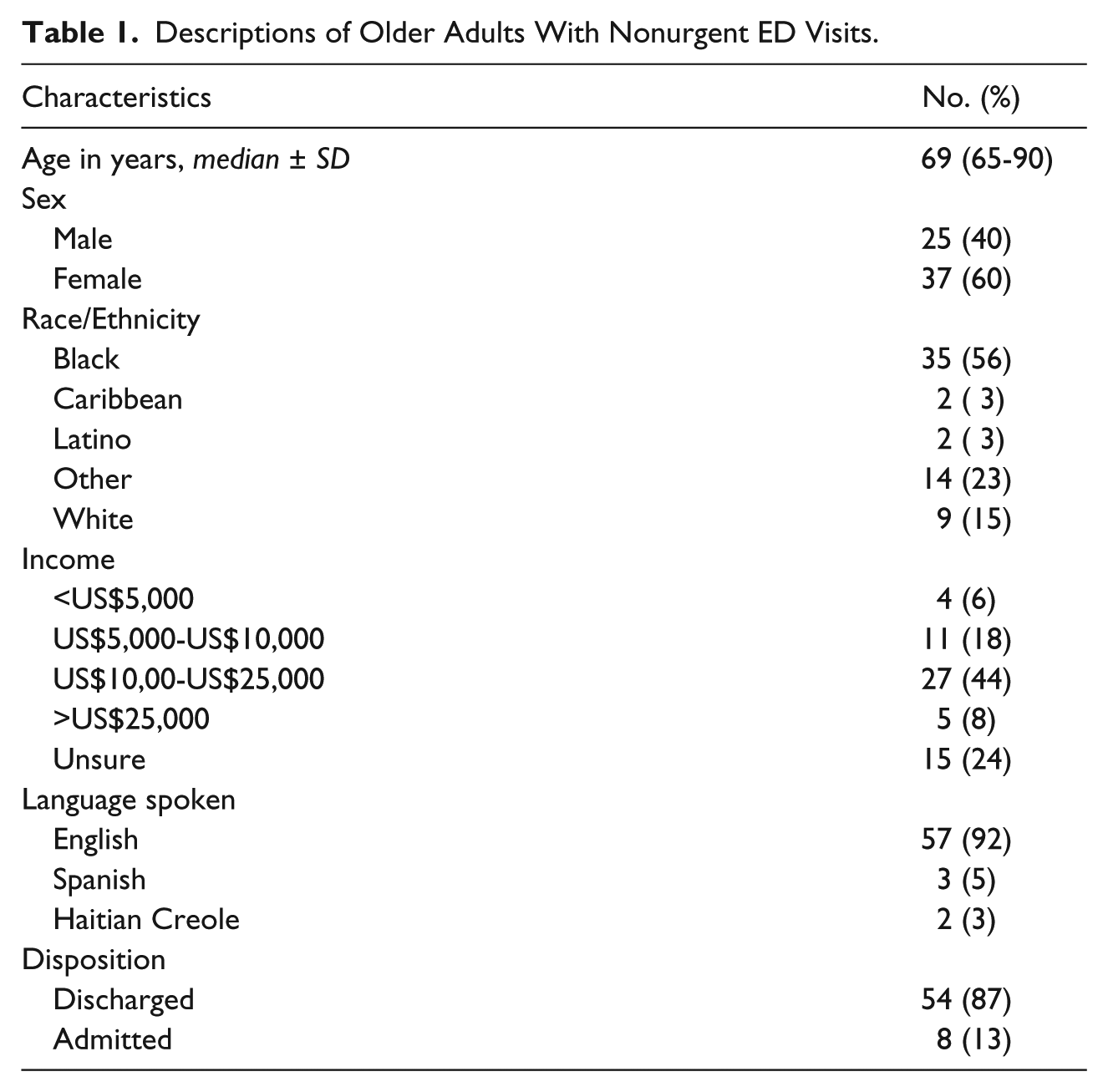
During the 3 months of the study period, a total of 559 older adults were screened, 136 were eligible, and 64 were enrolled. Two participants did not complete the study. One participant reported being too tired and the other participant was discharged. A total of 62 participants completed the quantitative survey portion of the study. Qualitative interviews were conducted among a subset of participants (N = 20) until data was saturated. The sample was 60% female, aged 65-90 years, with a mean age of 71. Approximately half of the participants were African American (57%), with Caucasian (15%), Latino (3%), Caribbean (3%), and other (22%) comprising the remainder of the sample. Most were single, widowed, or divorced (67%). More than half (69%) reported income at or below US$25,000 per year. Nearly half arrived to the ED via private car (45%) and public transportation (44%). Most participants reported preexisting medical conditions (86%), with, hypertension (60%), and diabetes (34%), the most frequently reported conditions. It is important to note that pain was the chief presenting complaint among 48% of the participants. After the ED evaluation, 87% of the participants were discharged to home and 13% were admitted to the hospital. Table 1 presents the sociodemographic and healthcare services data.
Descriptions of Older Adults With Nonurgent ED Visits.
Qualitative Findings
Three main themes related to older adults’ experiences in seeking care emerged: lack of timely access to primary care, difficulties with the automated phone programs, and healthcare system problems. The themes and examples from the participants’ (N = 20) perspectives highlight the challenges they face in attempting to access their primary care providers. One qualitative interview was completed by a Spanish-speaking participant whose reports of access were similar to other participants.
You Just Have to Wait
The majority of participants did have a regular source of primary care and expressed their overall satisfaction with their healthcare providers. They were able to access their primary care for routine health checkups which are scheduled several weeks to months in advance. The significant challenge they faced were related to obtaining timely access for acute or nonacute episodic illnesses. When asked why he was in the ED for evaluation, one man stated, “I have to call and make an appointment or go and make the appointment. Then maybe they would give it to me for probably this month or next month.” One older adult explained the difference between routine visits which are scheduled several weeks in advance and his current need for an episodic visit stated: I see her at least four times a year . . . but as far as getting into see her, like today I couldn’t just go in and see my doctor because she’s busy. In fact I had an appointment in September and something came up and I had to postpone it to October because of her commitments or something.
The participants described a series of barriers encountered when they tried to reach primary care for an episodic sick visit before coming to the ED. Most reported calling their primary care office for an episodic visit and being told that they would have to wait several days or weeks. As a result, the ED became the default site of care.
No they don’t see you right away. Like right now, they give me an appointment until November. So I didn’t have the medicine, I have to wait to November to get it.
One participant described her frustration in being offered an appointment several weeks from the day of her call: See that I don’t like, that’s too far. I mean you can be dead within that time. I think that is kind of ridiculous to have to wait that long. I’m calling them; well you got an appointment in November. Okay do you have another? The earliest one is December. Give me a break. I said I don’t know, I can’t stay here and wait that long. So that’s why I came over.
Several of the older adults did not call their primary care office before coming to the ED. When asked why, they reported lack of timely access for an episodic visit. Thus, going directly to the ED was a successful strategy used to ensure care for symptoms they felt needed prompt attention. One participant described her care seeking strategy this way: “The only way you could get immediate care, you have to come to the emergency. I’ve tried to call the doctor and they tell me to wait.”
All of the participants would have preferred to see their primary care providers but they could not obtain a timely appointment. They expressed the need to have a prompt evaluation within a few days. Therefore, without primary care access through the availability of a timely appointment, the ED became the default site of care.
The Phone; It is the Hardest Thing to Do
Several participants described phone difficulties which ranged from confusing automated messages, long phone queues, leaving voice messages, and not receiving return calls. Being placed on hold was another challenge for these older adults: It aggravates me. Well I just don’t get the service that is owed . . . That’s right they do put you on hold and don’t come back. Say hold on your call is very important to them. You’ll keep holding. After you’ve hold on for about thirty minutes, they’ll turn around and say well call back and leave your name and number.
Older adults shared their need to speak to an actual person rather than leaving a voice mail. One participant explained her frustration this way: “You know you want to hear a human voice. So sometimes if you want to talk to someone, press this and I will press that and stay there and wait.” They described their frustration with having to leave voice mail messages only to find that they did not receive a return call: “If you call them on the phone you get the answering machine or something. Yes, they don’t call me back, never.” One older adult explained her experience waiting for a call back after leaving a message at her primary care office’s automated voice message system: “Leave a message and they don’t call. The doctor don’t call, the people don’t call. Nobody calls.” Another participant described her repeated unsuccessful attempts to make an appointment by phone. In the end, she decided to go directly to her primary care office to obtain an appointment: It seems like a couple of weeks ago; I was trying to get an appointment. It’s the hardest thing to do to talk on the phone to get someone to schedule an appointment for me and usually I have to go to the clinic to talk to someone, a secretary or someone who make an appointment for me because it’s hard on the phone. They just __ you around, here and there, you talk to someone else. Then you have to call later on and you have to wait. It’s really hard on the phone to schedule an appointment.
These results indicate that participants find automated phone systems a barrier to communicating with their primary care providers and attempts to obtain an appointment for care.
It is a Systems Problem
Although healthcare systems may have well-established processes for managing yearly routine visits, there are significant difficulties in managing capacity related to acute, nonacute episodic visits. The older adults in this study were aware of the current challenges which healthcare systems face. They did not fault their healthcare providers for not being able to accommodate their need for a timely visit. One participant discussed her perceptions of the primary care system and her interactions with front line staff: It is a systems problem. Clearly, something needs to be changed because this is not working. The attendance is poor. The secretaries, I put them in their place when they don’t treat me well. However, the overall system is broken. The attendance to patients is very bad. This should not happen.
Another patient described her analysis of what might be the system problem. She explained it this way: “These are the things of life. It’s not the doctors, it is the workers. Because when I go to make an appointment and this problem happens, it is the workers that do these things. It’s not the doctors’ fault. The workers do things poorly.”
Participants perceived the healthcare environment as underresourced with significant challenges. One older adult described his view of the system: “You know how they want to wait. They have so many people that they can take in a day and all of us take too much of their time. So they don’t realize. But if you are sick, they tell you, go to the emergency room. Alright, they will tell you that.” Older adults commonly reported system challenges when trying to make an appointment by phone, one participant stated: “When you call, there’s not any appointment for three or four months or some crap, you know. You got to call back, like that. You call them and say you want an appointment, they ain’t got no appointments. Call back or something, that happens me.”
In addition to system difficulties in obtaining an appointment to be seen in primary care, participants reported system issues which led to fragmentation of care, as described by one patient: And then sometimes I found that the doctor that you’re assigned for, when you come in here, he’s seeing somebody else. You have to see another doctor or he’s not here. He’s on vacation; you know what I’m saying. So they can just put you on anybody in that department and you come in and you ask for one doctor and he’s not here. They give you the doctor for the day or whatever. That’s what I find anyway.
Discussion
This study was undertaken to describe why inner city older adults sought nonurgent care in the ED and their experiences in seeking primary care services. All of the participants had nonurgent reasons for seeking care, health insurance coverage, and a designated healthcare provider. The older adults wanted to be seen by their primary care providers but were unable to gain access for evaluation of their symptoms. Thus, the ED was not their preferred site of care but a default site of care.
As described in the interviews, the participants in this study reported several barriers to accessing their primary care services including lack of available appointments, confusing phone systems, and long wait for appointments. The participants in this study also reported increased challenges in navigating the healthcare system. These findings imply that this vulnerable, safety net population of older adults is at risk for delayed care, unmet healthcare needs, and poor health outcomes. More research about perceived barriers and successes may be helpful in developing and promoting improved access to primary care services for older adults.
The lack of timely primary care appointments was the cause of the nonurgent ED visits. All of the participants would have preferred to see their primary care providers rather than present to the ED for care. The reasons described for seeking nonurgent care in the ED instead of primary care included; lack of available primary care appointments, being told to go directly to the ED, and lack of return calls from their primary care providers for consultation or advice on presenting symptoms. For the few who did not attempt to contact their primary care providers, their explanations ranged from knowing from past experiences they would not be able to get an appointment or talk with their healthcare provider, and difficulties using the automated phone systems.
The participants reported difficulties with automated phone systems which has implications for primary care settings and healthcare organizations. The difficulties ranged from confusion with phone systems, lack of returned phone calls, insensitive office staff answering the calls, not having a “real person” answer the phone, long waits on hold, and complex automated phone queues. In 2012, the American Gerontological Associate reported on the special communication needs of older adults. The report outlines how age related changes can contribute to older adults’ difficulty with complex phone systems. It highlights the facts about hearing impairment among older adults. Hearing impairment is the third most common chronic condition and the prevalence of significant hearing impairment among people 65 to 75 years of age is approximately 30% to 35% and among people 75 years of age or older, the prevalence increases to 40% to 50% . In addition to hearing impairment, reduced information processing and capacity can lead to communication problems among older adults (The Gerontological Society of America, 2012). There are evidence-based strategies which primary care settings can incorporate to improve phone communication with older adults. Office staff can be trained to help older adults access care and guide them to the appropriate type of appointments. Automated systems can be simplified and the initial call can be serviced by a staff member rather than placing older adults on hold or in a long phone queue.
One significant finding was the reports of pain as a chief presenting complaint among nearly half of the participant (48%). Chronic pain symptoms among older adults can interfere with daily activities, which in turn can lead to diminished quality of life. Persistent pain can cause multiple mental and physical limitations, and increase costs and healthcare utilization (Institute of Medicine, 2012). According to the Institute of Medicine report, Relieving Pain in America, pain is often undertreated. Unrelieved or poorly managed pain can cause suffering and decreased quality of life. It also can cause sleep difficulties, and increase anxiety and depression, and disabilities. Unrelieved pain decreases patient satisfaction with the healthcare system. Older adults are the most likely group to experience problems in the adequate treatment of pain (Institute of Medicine, 2012). Racial and ethnic minorities are at greater risk for poor pain assessment. The participants’ reports of pain in this study highlight the need for routine aspect of screening among this population.
Limitations
This study was limited by the small sample of participants from one emergency department in the Northeast, making it difficult to generalize these findings. Despite attempts to enroll more non-English speaking participants, only one Spanish speaking older adult consented to participate in the qualitative interview. Despite these limitations, the study does provide the perspectives of a safety net population on access and barriers encountered when attempting to access primary care services.
Application
Inner city older adult are at risk for poor health outcomes due to factors such as age, poverty, race, resources, and environment (Flaskerud & Winslow, 1998; Institute of Medicine, 2003). Lack of timely access to care or delayed access to care can result in serious illness, complications, and hospital admissions (Bierman, Magari, Jette, Splaine, & Wasson, 1998). Decreased availability of primary care services and the inability of the system, staff, and providers to effectively address patients’ needs can contribute to health disparities. This is especially important among minority patients such as those in this study who are considered a safety net population. Optimal management of chronic disease requires careful monitoring and comprehensive care. This can’t be accomplished when underresourced primary care systems can only accommodate routine visits and not acute, episodic illness which can often happen in chronic disease. The costs of the average ED visit is significantly more expensive than a primary care visit: US$975 compared to US$250 (Massachusetts Division of Health Care Finance and Policy, 2012). As the costs of healthcare continue to rise we need to develop evidence-based interventions to ensure access to primary care and leverage limited resources.
It has been shown that healthcare delivery systems are in need of dramatic change because system barriers affect the quality of care and access for many patients (Carter, Balaji, & Winters, 2006; Koh, Manias, Hutchinson, Donath, & Johnston, 2008; Kohn, Corrigan, & Donaldson, 2000). The findings from this study highlight the importance of the need for significant system changes to facilitate ease of access to care for vulnerable older adults. In exploring participants’ experiences in accessing primary care services and the resulting ED visits, we can begin to understand why older adults may be frequent users of the ED for nonurgent care.
Older adults are the fastest growing age group and at risk for developing chronic diseases and disability. Timely access to care, comprehensive chronic disease management, and health promotion can improve quality of life, wellness, and health outcomes among our elders (U.S. Department of Health and Human Services, 2011). As we begin to prepare for the health care needs of the growing numbers of older adults, it is essential that we also develop new ways to provide timely access to primary care services. Despite national recommendations and the development of several model programs for preventative services and wellness programs for older adults, there is still a considerable gap in the availability of these programs (Institute of Medicine, 2008)
In the recent Institute of Medicine, Robert Wood Johnson Report, The Future of Nursing: Leading Change, Advancing Health, two key recommendations state that nurses should practice to the full extent of their education and training and full partners, with physicians and other health professionals, in redesigning healthcare (Institute of Medicine, 2010). Although the science of chronic illness management has been advancing in the past several years, there are still considerable gaps in knowledge related to health promotion and restoration of optimal health of individuals across the life span. (Wyman & Henly, 2011). Nurses can play a pivotal role in leading other health professionals, in the development of integrated, health system models to improve the health of our nation’s elders. The results from this study are important to help inform healthcare systems about the challenges that older adults encounter and contribute to improving access to primary care for vulnerable older adults.
Footnotes
Acknowledgements
All authors acknowledge the support of the Jones Fund, University of Pennsylvania.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. D’Avolio was supported by a John A. Harford Foundation and Atlantic Philanthropies Claire M. Fagin Postdoctoral Fellowship at the University of Pennsylvania, Philadelphia. All authors acknowledge the support of the Jones Fund, University of Pennsylvania.