
Abstract
The risk of pressure ulcers is widely assessed using the Braden Scale for Predicting Pressure Ulcer Risk, which describes patient characteristics for various severity levels. However, many of these characteristics are described in vague terms that nurses may interpret inconsistently, potentially threatening scale reliability. To examine the consistency of nurses’ interpretations of five vaguely described patient characteristics on the Braden Scale we surveyed a convenience sample of 102 nurses and compared their interpretations with those of two nurse experts. The results show large variations in nurses’ interpretations. Although the highest frequency of nurses’ responses to the majority of descriptions was consistent with the experts’ interpretation, the large variation in responses may seriously threaten consistent and accurate assessment of pressure-ulcer risk with the Braden Scale. Our findings suggest that training programs provide operational definitions of these vague patient descriptions, so the Braden Scale can be used consistently in patient care.
Pressure ulcers are a serious patient safety concern, which nurses play a pivotal role in preventing (Delmore, Lebovits, Baldock, Suggs, & Ayello, 2011; Thompson, 2011). The first step in preventing these ulcers is the crucial and challenging task of identifying patients at risk of developing a pressure ulcer. Assessing these at-risk patients is a complex decision process that requires interpreting various aspects of patient status. Patient status for risk of pressure ulcers is widely assessed using the Braden Scale for Predicting Pressure Ulcer Risk, which rates patients on six risk factors: sensory perception, nutrition, activity, mobility, skin moisture and presence of friction, and shearing force (Bergstrom, Braden, Kemp, Champagne, & Ruby, 1998). Nurses assess these factors at various severity levels according to detailed descriptions of patient characteristics on the Braden Scale. However, many of these descriptions are at a general level requiring an additional step of interpretation to be operationalized for actual assessment practice. We consider that nurses’ idiosyncrasies in interpreting those descriptions are potential threats to the reliability of this scale in assessing pressure-ulcer risk.
To better describe the issues associated with idiosyncratic interpretations of the Braden Scale’s descriptions of patient characteristics, we surveyed nurses to determine how consistently they interpreted five vaguely described patient characteristics in the Braden Scale and compared their responses to those of two nurse experts, which served as the gold standard.
Problem
The quality of clinical nursing care is indicated by several factors, including skin integrity (Meraviglia, Becker, Grobe, & King, 2002). Thus, a newly developed pressure ulcer is considered a hospital-acquired safety problem, for which Medicare no longer reimburses treatment costs (Armstrong et al., 2008; Centers for Medicare & Medicaid Services, 2006).
Patients’ risk of pressure ulcer is widely assessed by nurses using the Braden Scale (Bergstrom et al., 1987). Although this scale has been shown to be valid in many studies (Bergstrom et al., 1998; Bergstrom & Braden, 2002; Braden & Maklebust, 2005), its interrater reliability has been verified less successfully. For example, an unsatisfactory level of interrater reliability was reported for this scale, especially at the individual parameter level (Anthony, Papanikolaou, Parboteeah, & Saleh, 2010; Kottner & Dassen, 2008, 2010). Furthermore, accurately and reliably assessing pressure-ulcer risk with the Braden Scale has been shown to depend on a comprehensive understanding of patient status and correct application of patient characteristics as defined for each scale parameter (Kottner & Dassen, 2008, 2010; Magnan & Maklebust, 2008; Maklebust & Magnan, 2009). The findings of these studies indicate that the accuracy and interrater reliability of the assessment were improved by explicitly defining the characteristics required to determine a patient’s risk level.
To facilitate determination of risk scores for pressure ulcers, we developed decision algorithms based on explicitly defined patient data from an electronic medical record system and data synthesis methods for assessing risk of pressure ulcers at three academic medical centers (Kim, Choi, Secalag, et al., 2010; Kim, Choi, Thompson, et al., 2010). While developing decision rules, however, we observed that many patient characteristics in the Braden Scale were described in vague terms, making it challenging to translate them to measurable characteristics. For example, two patient characteristics are “walks occasionally during day, but for very short distances” and “skin is often, but not always moist” (italics indicate terms open to interpretation). Since these descriptions of patient characteristics in the Braden Scale serve as the criteria for differentiating the severity of patient risk, they must be clear to all scale users. Such vague descriptions are, therefore, potential barriers to accurately and consistently assessing pressure-ulcer risk with the Braden Scale, and to developing a computerized decision-support system that can assist clinical nurses in assessing risk of pressure ulcer.
Purpose of the Study
To better understand how vague descriptions of patient characteristics may impact the practice of assessing pressure-ulcer risk, we surveyed nurses on how they interpreted five vague descriptions in the Braden Scale as identified in our prior studies (Kim, Choi, Secalag, et al., 2010; Kim, Choi, Thompson, et al., 2010). We compared nurses’ responses to the gold standard of responses generated by two nurse specialists in pressure-ulcer care. We also examined if nurses’ responses differed by their specialty area and nursing experience (in years). The purposes of this study were to examine (a) how different nurses interpreted and operationalized the Braden Scale parameters, (b) how closely their responses matched the interpretations and operational definitions of two experts who served as a gold standard, and (c) if nurses’ responses differed by their specialty area and nursing experience.
Method
For this descriptive, paper-based survey study, we recruited a convenience sample of 102 nurses from two academic medical centers, a rehabilitation hospital, and a tertiary acute care hospital, in Massachusetts. In collaboration with two nurse specialists, we developed a questionnaire to explore respondents’ interpretation and operationalization of five vague descriptions. The questionnaire had two parts: (a) demographic questions on nurses’ specialty area, nursing experience and education (in years), and (b) questions on interpreting the five vague descriptions identified as particularly challenging to operationalization by the expert nurses in our prior studies (Table 1). In the second part, five questions were designed to take responses in a free-text format, and context was provided by including associated parameters and phrases containing the vague descriptions. For example, the question on “over most of body” was as follows:
The Sensory Perception parameter of the Braden Scale is scored from 1 to 4, where 1 indicates Completely Limited, i.e., “limited ability to feel pain over most of body.” Please indicate what you might consider as “over most of body” by typing in the percentage of body surface affected (e.g., over 80%, over 75%, etc.).
Vague Descriptions of Patient Characteristics in the Braden Scale.
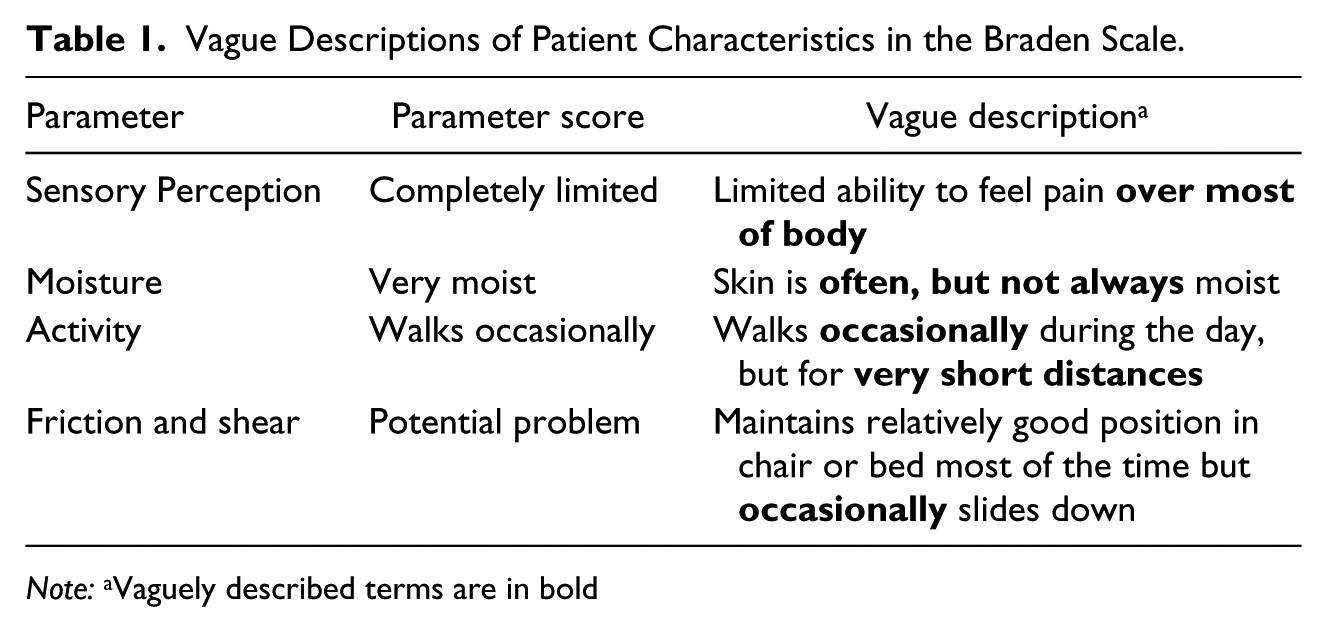
Note: aVaguely described terms are in bold
After the study was approved by the Institutional Review Board at each participating hospital, nurse respondents at the two study sites completed our paper-based survey. One nurse expert from each hospital, both certified in wound, ostomy and continence care, provided gold-standard interpretations for the items surveyed in this study. They were master’s prepared nurse specialists in pressure-ulcer care and education, with more than 10 years of nursing experience. In two focus group interviews, the experts were asked to operationalize the terms in the questionnaire. Consensus on operational definitions of each vague term was reached though discussions.
Data Analysis
Responses were analyzed descriptively using SAS version 9.2. Since responses were significantly skewed, the assumption of normal distribution for parametric statistics was not met (Plichta & Kelvin, 2012). Thus, we used the nonparametric Kruskal-Wallis test to determine whether responses differed by respondents’ nursing experience or specialty area.
Findings
Respondents’ Demographics
Respondents at the two study sites did not differ significantly in years of nursing experience (p = .17) and education level (p = .10). The two groups of nurses also did not differ significantly in their responses. Thus, data from the two participating hospitals were aggregated for analysis.
Overall, 102 nurses at the two study sites provided responses (Table 2). Among these respondents, 27.5% (n = 28) specialized in care of medical inpatients, 24.5% (n = 25) in surgical inpatients, and 22.5% (n = 23) in rehabilitation. Their specialty experience ranged from less than 2 years (28.4%, n = 29) to more than 10 years (17.6%, n = 18). Most nurses held a baccalaureate degree (83.4%, n = 85).
Respondent Characteristics.
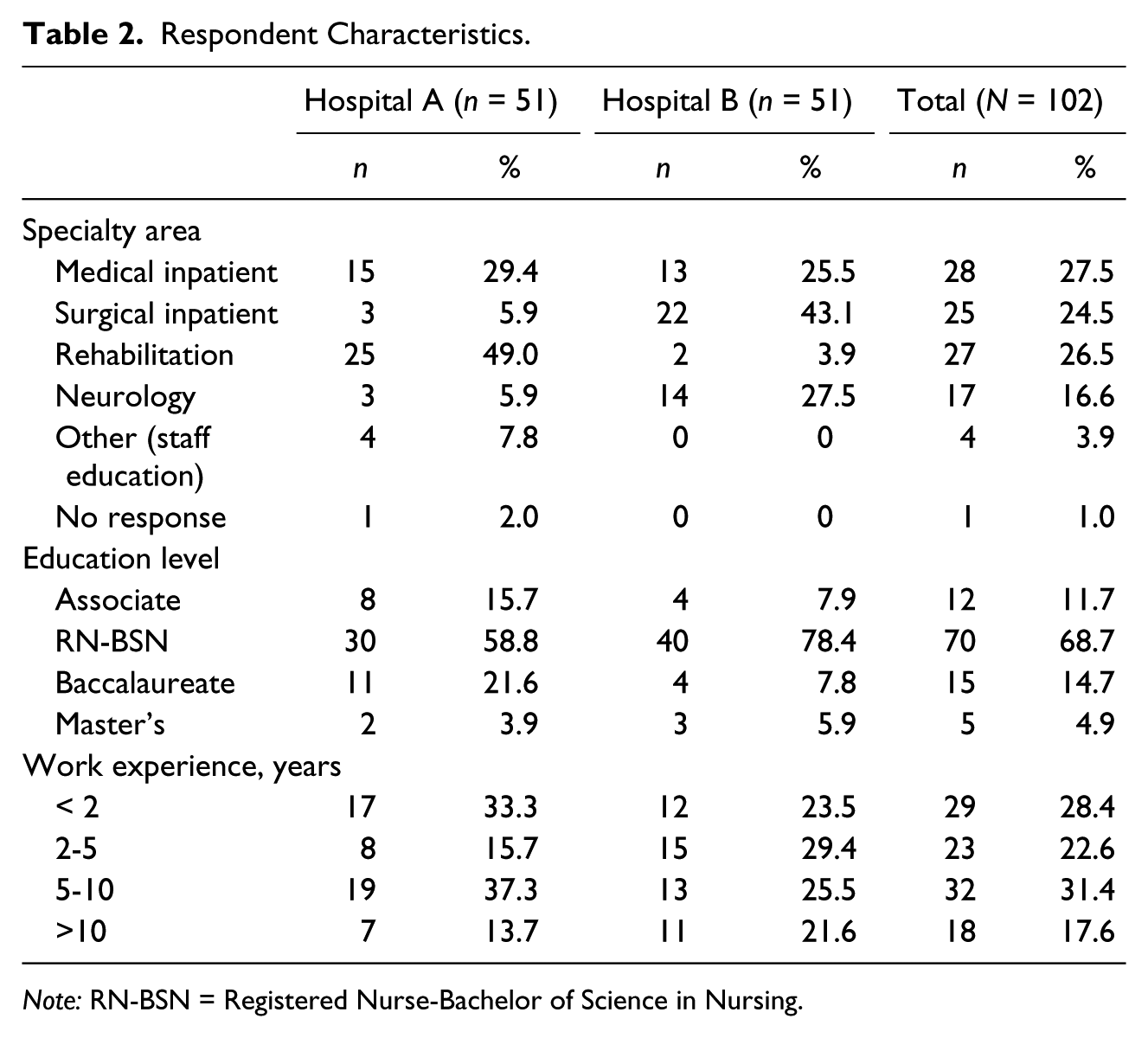
Note: RN-BSN = Registered Nurse-Bachelor of Science in Nursing.
Experts’ Responses
The experts agreed that in the sensory perception parameter, “over most of the body” was operationalized as “75% or greater” body surface affected. In the moist parameter, “often, but not always” was operationalized as “50% of the time.” In the activity parameter, “occasionally walks” was operationalized as “one to two times in an 8-hour shift,” and “walks very short distances” as “walks up to 25 feet.” In the friction and shear parameter, “occasional” sliding down was operationalized as “sliding down three to four times in an 8-hour shift.”
Nurses’ Responses
Nurses’ responses to each of the five vague descriptions of patient conditions are shown in Figure 1 as percentages, with blue bars presenting experts’ operational definitions. These data show large variability in nurses’ responses to every item. Among the five items, “walks very short distances” (for the activity parameter) had the most diverse responses. This description was interpreted in 19 different ways from “walks 1 foot” (1%) to “walks 250 feet” (1%). About one fourth (24.7%) of respondents considered “very short distance” as 25 feet, which was the same as experts’ interpretation.
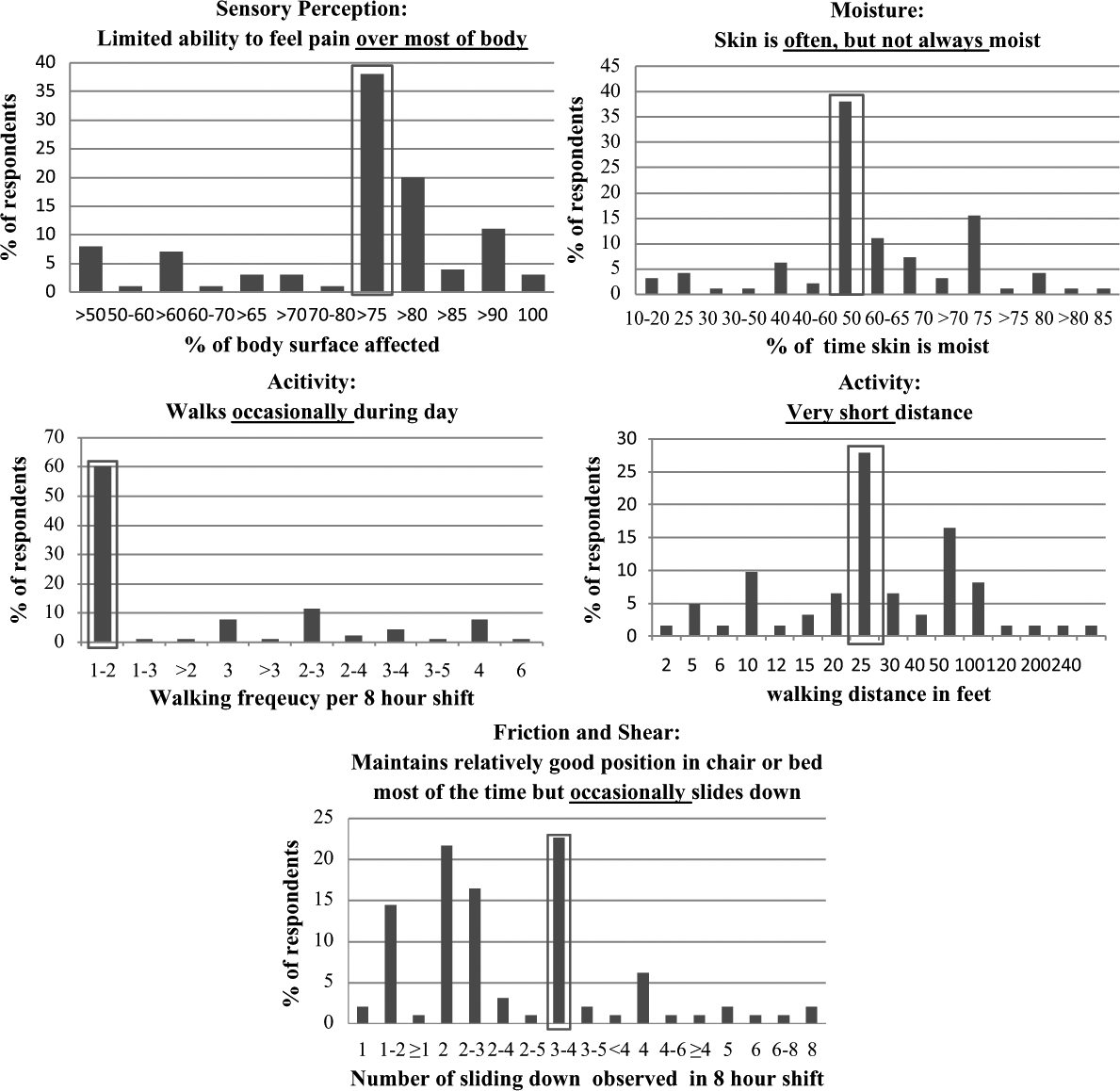
Percent of nurses’ responses in each of five vague descriptions in the Braden Scale.
“Occasional sliding down” (for the friction and shear parameter) was the second most diversely interpreted description, having 17 different responses from “sliding down once” (2%) to “sliding down eight times” (2%) in an 8-hour shift. The most frequent response was “sliding down three to four times in an 8-hour shift” (23%), which matched the experts’ interpretation.
“Skin is often, but not always moist” (for the skin moisture parameter) was interpreted in 15 different ways, from “10 to 20% of the time” (3%) to “over 85% of the time” (1%). The largest shared interpretation was “50% of the time” (38%), which matched the experts’ interpretation.
“Impaired over most of body” (for the sensory perception parameter) was interpreted in 12 different ways, from “greater than 50%” (9%) to “100%” (3%). The most frequent response was “over 75% of body” (38%), which was the same as the experts’ interpretation.
“Walks occasionally” (for the activity parameter) was interpreted in 11 different ways, from “one to two times per 8-hour shift” (60%) to “six times per 8-hour shift” (1%). The nurses’ largest shared operational definition was “one to two times per 8-hour shift” (60%), consistent with the experts’ interpretation.
Nurses’ Responses by Specialty and Years of Nursing Experience
When we examined differences among responses by nursing experience, only the responses to “walks occasionally” differed significantly (p < .05). The findings indicated that nurses with more than 5 years of nursing experience were more likely than nurses with less experience to agree with the experts on interpreting this description.
When examined by specialty areas, the responses to differed significantly for two vague descriptions: “over most of the body” (p = .02), and “often, but not always” (p < .01). For “over most of the body,” the highest agreement with experts’ interpretation was among rehabilitation nurses (43.5%), followed by nurses specializing in care of medical inpatients (42.4%), and surgical inpatients (35%). For “often, but not always,” the highest agreement with experts’ interpretation was among nurses with a specialty in surgical inpatient care (50%), followed by rehabilitation nurses (47.8%), and those caring for medical inpatients (33.3%).
Discussion
The survey results show large variations in how nurses interpret vague descriptions of patient characteristics in the Braden Scale. Although the highest frequency of nurses’ responses to the majority of surveyed descriptions was consistent with the experts’ interpretation, the large variation in responses is a potentially serious threat to consistent and accurate assessment of pressure-ulcer risk with the Braden Scale.
One interesting finding is that the experts from the two hospitals interpreted the same frequency descriptor “occasionally” differently depending on the context. “Occasionally slides down” was interpreted as three to four times per 8-hour shift and “walks occasionally” as one or two times per 8-hour shift. This difference implies that such generic descriptors need to be operationalized differently according to the context of use. In contrast, the nurse respondents interpreted “occasionally” the same in both contexts, one to two times per 8-hour shift. The findings of this study may provide nurse educators with useful insights into accurate and reliable operational definitions of patient descriptions in the Braden Scale.
Responses to some items differed significantly among the nurses by their nursing experience or specialty area. Nurses with more than 5 years of working experience agreed more with the experts than nurses with less experience on interpreting “walks occasionally.” Rehabilitation nurses agreed most often with the experts on interpreting “over most of body,” while nurses from the medical inpatient specialty agreed most often with the experts on interpreting “often, but not always.” However, these differences could not be explained by any clear pattern. Caution is warranted in interpreting these differences since we relied on only two experts and the sample of nurses was small.
Application
The findings emphasize areas upon which nurse educators may focus by using accurate and reliable operational definitions of patient descriptions in the Braden Scale. The study findings can be used as a reference when orienting nurses who will regularly assess patients using the Braden Scale and update patients’ risk of pressure ulcer in the nursing care plan over the course of hospitalization. All hospitals offer training to newly hired nurses on assessing patients with the Braden Scale. These training programs provide specific patient examples that represent cases with different risk levels assessed using the Braden Scale. Our findings suggest that these training programs should provide operational definitions of many vague patient descriptions in the Braden Scale, so the scale can be used consistently in various patient care settings. After training, interrater reliability of the Braden Scale should be assessed to ensure a satisfactory level of reliability among nurses. In addition, such operational definitions can serve as the basis for developing a decision-support system for assessing risk of pressure ulcers. Accurate and consistent assessment of patients’ level of pressure-ulcer risk will lead to more effective mitigation of identified risk, which will ultimately improve patient safety.
The study findings show large variations in nurses’ interpretation of patient characteristics in the Braden Scale. These findings are consistent with the result of studies by Anthony et al. (2010) and Kottner and Dassen (2008, 2010), in which there were inconsistencies in assessment and judgment at the individual parameter level of the Braden Scale. However, future studies are suggested using a larger sample and more nurse experts to further validate the study findings.
Footnotes
Acknowledgements
The authors thank Sarah Thompson, RN, MSN, and Lindsay Meeker, RN, for invaluable input on developing the survey questionnaire.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was partially supported by the Partners Siemens Research Council # 500215 (Jeeyae Choi, PI).