
Abstract
A woman’s psychological health can affect prenatal behaviors. The purpose of this study was to examine the relationship between maternal beliefs, prenatal behaviors, and preterm birth (PTB) in a multiethnic population. This was a planned secondary analysis of a cross-sectional trial of postpartum women with singleton gestation. In all, 210 participants were given the Fetal Health Locus of Control (FHLC) scale to measure three primary maternal beliefs that influenced their prenatal behaviors (Internal Control, Chance, Powerful Others). Women who experienced preterm delivery and those who smoked during pregnancy scored the Chance category significantly higher than those who delivered term infants (p = .05; p = .004, respectively). This suggests those who smoked during pregnancy had a greater degree of belief that Chance influenced their infant’s health status. Cultural differences also emerged specific to the impact of health care providers on PTB; with Hispanic women scoring Powerful Others the highest among the groups (p = .02). Nurses can plan a critical role in identifying at-risk women (smoking, strong Chance beliefs) while providing a clear message that taking action and modifying high-risk behaviors can reduce risk for adverse pregnancy outcome.
Introduction
A woman’s psychological health during pregnancy is associated with her health behaviors and may affect pregnancy outcome. Fetal health locus of control (FHLC) is a concept that addresses pregnant womens’ beliefs specific to the health of their infants (Labs & Wurtele, 1986). Over the past two decades, the rate of preterm birth (PTB) in the United States has increased from 9.4% to 12.8% (Hamilton, Martin, & Ventura, 2010a). Recent statistics show an encouraging 3% drop from 2007 to 2008 (Hamilton, Martin, & Ventura, 2010b). Interestingly, the improved PTB rate still remains higher than any year from 1981 to 2002 (Centers for Disease Control [CDC], 2011) signifying that this negative pregnancy outcome remains a serious health concern. PTB is defined as infants delivered at less than 37 completed weeks of gestation and is the leading cause of infant death in the United States (CDC, 2006). PTB is not a single gene disorder but rather a complex disorder that culminates when there is an adverse reaction between maternal environmental, psychological, and physiological factors. Two predictors of PTB are a mother’s ethnicity and smoking status; however, the interaction between these predictors and a woman’s thought process regarding her pregnancy has not been studied.
There is no debate that prenatal smoking places women at greater risk for preterm premature rupture of membranes, preterm delivery, and delivery of a low birth weight or small for gestational age infant (CDC, 2004a; Floyd, Rimer, Giovino, Mullen, & Sullivan, 1993; Shah & Bracken, 2000). Over the past decade, U.S. maternal smoking rates have been consistently declining (11%); however, 24% of women in Kentucky continue to smoke tobacco during pregnancy (CDC, 2004b). Women who smoke during and after pregnancy are often single, younger age, less educated, have a partner who smokes, and less likely to engage in healthy behaviors such as attending prenatal care or breastfeeding their infant (O’Campo, Faden, Brown, & Gielen, 1992; Schneider & Schütz, 2008). While current research primarily focuses on the risks to the unborn child, research is limited on the interaction between maternal thought process and smoking behaviors during pregnancy (S. Higgins, 2002). Ethnic differences also exist when predicting smoking behaviors during pregnancy (Floyd et al., 1993). Among White women, education, age, and parity predicted cessation, whereas intention to breastfeed predicted cessation among Black women (O’Campo et al., 1992).
The purpose of this study was to assess the relationship of FHLC with smoking status, ethnicity, and PTB status. Our primary hypothesis is that women who engage in modifiable high-risk prenatal behaviors (prenatal smoking), are more likely to believe the concept of Chance affects their prenatal/fetal health compared with women who do not smoke during pregnancy. Although prenatal smoking and secondhand smoke (SHS) exposure pose a significant risk for PTB (Ashford, Hahn, Hall, Peden, & Rayens, 2011), there are also socioeconomic and demographic factors (education, income, race, and ethnicity) that are linked to PTB. PTB has become a national epidemic, as well as an epidemic of racial and ethnic disparities (CDC, 2006). For example, approximately 10% of all births in the United States are premature; however, the prematurity rate for African American women is double that of Caucasian women (Reagan & Salsberry, 2005). African American women and women who smoke are more likely to experience PTB; however, how these factors influence a mother’s locus of control regarding fetal health and pregnancy outcome has not been studied.
Several studies have shown an association between the FHLC scale and healthy behaviors such as breastfeeding and attending prenatal classes (Haslam, Lawrence, & Haefeli, 2003; Walker, Cooney, & Riggs, 1999), and the FHLC scale has also been significantly linked to unhealthy behaviors during pregnancy, such as smoking tobacco and drinking alcohol (Haslam & Lawrence, 2004; Stewart & Streiner, 1994, 1995). Clarke and Gross (2004) showed that the FHLC is associated with physical exercise participation in pregnant, nulliparous women. The contribution of each of these studies is important in evaluating the impact of maternal thought processes on decisions made during pregnancy; however, the body of literature is limited on exploration of the relationship of maternal FHLC with smoking status and PTB in a multiethnic population.
Method
Design and Sample
A cross-sectional study design was used to investigate the relationship of maternal FHLC with smoking status, ethnicity, and PTB status. Based on an a priori power analysis, the goal was to recruit 200 mother–infant couplets; this would allow for at least 90% power to detect a regression R2 as small as .15 with up to 10 regressors and an alpha level of .05. Quota sampling was used to ensure a roughly equal distribution of women who were smokers, nonsmokers/passive exposed, and nonsmokers/nonexposed during pregnancy. Of the 210 mothers who were recruited, 53 were smokers (25%) and 157 were self-identified nonsmokers. Of the nonsmokers, 66 reported being exposed to SHS (31%) and 91 were nonsmokers/nonexposed during pregnancy. Less than 10% of those invited to participate refused, and 82 nonsmoking women were excluded due to quota sampling procedures. Nearly all women were Caucasian, African American, or Hispanic; the six who had other ethnicities were not included in this analysis because the emphasis was on racial/ethnic comparisons and the number of Asian women (n = 2), and those in the “Other” race category (n = 4) were too small for these comparisons. Participants were offered a choice of two incentives: a one-time payment of US$25 or the equivalent of US$25 in diapers.
Procedure
The study was approved by the University’s Institutional Review Board. Content verification of all written study materials was conducted by expert translators. Within 48 hr of birth, participants completed a retrospective review of their prenatal health/behaviors (FHLC) and smoking history based on recommendations by the American College of Obstetricians and Gynecologists (ACOG): Smoking Cessation During Pregnancy: A Clinician’s Guide to Helping Pregnant Women Quit Smoking and previous published hair sampling studies (Hahn, Lee, Peiper, & Troutman, 2006; Jaakkola & Jaakkola, 1997; Okoli, Hall, Rayens, & Hahn, 2007). Average survey completion time was 22 min.
Measures
Demographic variables
The demographic variables of ethnicity, marital status, education, and income were determined using single items. The ethnicity item included five response options (“Caucasian,” “African American,” “Hispanic,” “Asian,” and “Other”). Only the first three ethnic categories were used in this analysis as the six women who responded either “Asian” or “Other” constituted too small a number to use as a subgroup. Responses to the marital status measure were combined into one of two categories “Married, living with spouse” and “Not married or not living with spouse.” The latter group included women who were separated from their spouse, divorced, never married, or widowed. Education was collected using a six-category ordinal variable with response choices ranging from “Grades 1 to 8” to “Graduate work past college.” Income was assessed with a nine-category ordinal scale ranging from “US$4,999 or less” to “US$50,000 or more.”
Smoking indicators
The questionnaire assessed smoking and SHS exposure. A woman was classified as a self-reported “smoker” (S) if she responded “yes” to the question, “Have you smoked a cigarette, even a puff, in the past 7 days?” NicAlert (2007), a valid and cost-effective commercial urine assay, used cutoff limits of urine cotinine levels to validate smoking status in adults. NicAlert measurement correlates well with more complex laboratory tests using High Performance Liquid Chromatography (HPLC) used in the CDC laboratory (Bernert, Harmon, Sosnoff, & McGuffey, 2005). In this study, nonsmokers were defined by urine cotinine < 99 ng/mL (Level 00-02). Current smokers were defined by urine cotinine > 100 ng/mL (Level 03-06). Bernert et al. (2005) reported classification sensitivity and specificity were 88% and 92, respectively, for cotinine measured by NicAlert. NicAlert cutoffs for smoking validation are consistent with previous reported urine cotinine ranges (S. T. Higgins et al., 2007). Ashford et al. (2010) further reported a strong correlation between urine cotinine (via NicAlert) and self-reported smoking status in pregnant women (ρ = .88; p < .0001).
SHS exposure is defined as the contact of passive smoke “to the eyes, the epithelium of the nose, mouth, and throat, and the lining of the airways and alveoli” (Jaakkola & Jaakkola, 1997). For our study, SHS exposure was categorized based on self-report. The daily average number of cigarettes smoked for each family member and visitor (within the past week) was calculated based on the following five categories: 1 to 5, 6 to 10, 11 to 15, 16 to 20, >20 (Al-Delaimy, Crane, & Woodward, 2002). If the participant did not quantify any exposures (days or hours) to any of the exposure questions (home, car/vehicle, work), they were classified as “nonsmoking/nonexposed” (NS/NE). If a participant answered “yes” or quantified exposure (days or hours) to any of the smoking exposure questions, they were classified as “nonsmoking, passive-exposed” (NS/PS; Hahn et al., 2006; Okoli et al., 2007).
Infant characteristics and PTB status
The infant outcome of PTB was collected by the research team from the medical record within 48 hr of birth. PTB was coded as “yes” if the completed gestation was less than 37 weeks and “no” for 37 weeks or more. In addition to gestational age of birth, infant weight, length, sex, and Apgar scores (1, 5 min) were collected.
FHLC
Participants were given the 18-item FHLC scale to assess their perception of factors that influenced their pregnancy within 2 days of delivery. The FHLC scale was inspired by the Wallston, Cohen, Wallston, Smith, and DeVellis (1978) and the Multidimensional Health Locus of Control (MHLC) scale (Labs & Wurtele, 1986). This scale was developed to predict identifiable factors contributing to a mother’s compliance with health-related recommendations during pregnancy. This modified scale consists of 18 items, categorized in three subscales (6 items) with a 5-point ordinal response set (strongly agree, agree, don’t know, disagree, or strongly disagree). Questions assess the mother’s perception of influential factors relative to her infant’s health. Three distinct concepts are measured (each composed of six questions): (a) Internal FHLC measures a mother’s belief that she is directly responsible for the health of her infant; (b) Chance FHLC assesses degree of belief that the infant’s health is based on chance/fate; and (c) Powerful Others FHLC measures belief that the responsibility for perinatal outcomes belongs to health professionals (Labs & Wurtele, 1986). Example questions include Internal: By attending prenatal classes taught by competent health professionals, I can greatly increase the odds of having a healthy, normal baby; Chance: If my baby is unhealthy or abnormal, nature intended it to be that way; Powerful Others: My baby will be born healthy only if I do everything my doctor tells me to do during pregnancy (Labs & Wurtele, 1986). Reliability of the FHLC scale has been supported in diverse populations (Stewart & Streiner, 1995; Webb, Siega-Riz, & Dole, 2009). In the original psychometric assessment, Cronbach’s alpha coefficients for each subscale were .88, .83, and .76 respectively, and test–retest reliabilities were similar over a 2-week interval (.80, .86, and .67; Labs & Wurtele, 1986). Walker et al. (1999) reported alpha coefficients of .75, .80, and .76 respectively, when using the FHLC to explore the relationship of psychosocial variables to health behaviors during pregnancy.
Statistical Analysis
Descriptive statistics were used to summarize demographic, smoking indicators, and PTB status variables of the participants. Bivariate group comparisons of locus of control outcomes by race/ethnicity, smoking status, and PTB status were accomplished using one-way analysis of variance or two-sample t tests, as appropriate. Post hoc comparisons for significant ANOVA F tests were accomplished using Fisher’s least significant difference procedure for pairwise comparisons. Multiple linear regression was used to assess the demographic and personal characteristics (including ethnicity, smoking indicators, and PTB status) that predict the locus of control variables of Internal, Chance, and Powerful Others, with separate models for each outcome. Variance inflation factors were used to assess for the presence of multicollinearity in each of the models. The bivariate analysis was done to determine the degree of association between locus of control and each of the demographic and personal factors. The multiple regression analysis assessed the simultaneous impact of personal and demographic variables on locus of control. Data were analyzed using SAS for Windows, version 9.3; an alpha level of .05 was used throughout.
Results
Slightly more than half of participants were Caucasian (58%). About one fourth were Hispanic (26%) and 16% were African American (Table 1). The sample was roughly evenly divided between married (48%) and not married (52%). The majority of women had at most a high school education or General Educational Development (GED; 58%). More than half of participants had an annual income of less than US$20,000 (53%). One quarter of women were active smokers (25%). Nearly one third were nonsmoking but were passively exposed to SHS (32%), and the remaining participants were nonsmoking and nonexposed to SHS (43%). One fifth of women had a PTB (20%). With regard to infant and PTB indicators, on average infants weighed 3,159 grams; were 49.9 cm in length; and had 1, 5 min Apgar scores of 8. There were more male infants (57%) than females (43%); and 43 infants were born premature.
Frequency Distributions for Demographic Variables, Smoking Indicators, and Preterm Birth Status (N = 204).
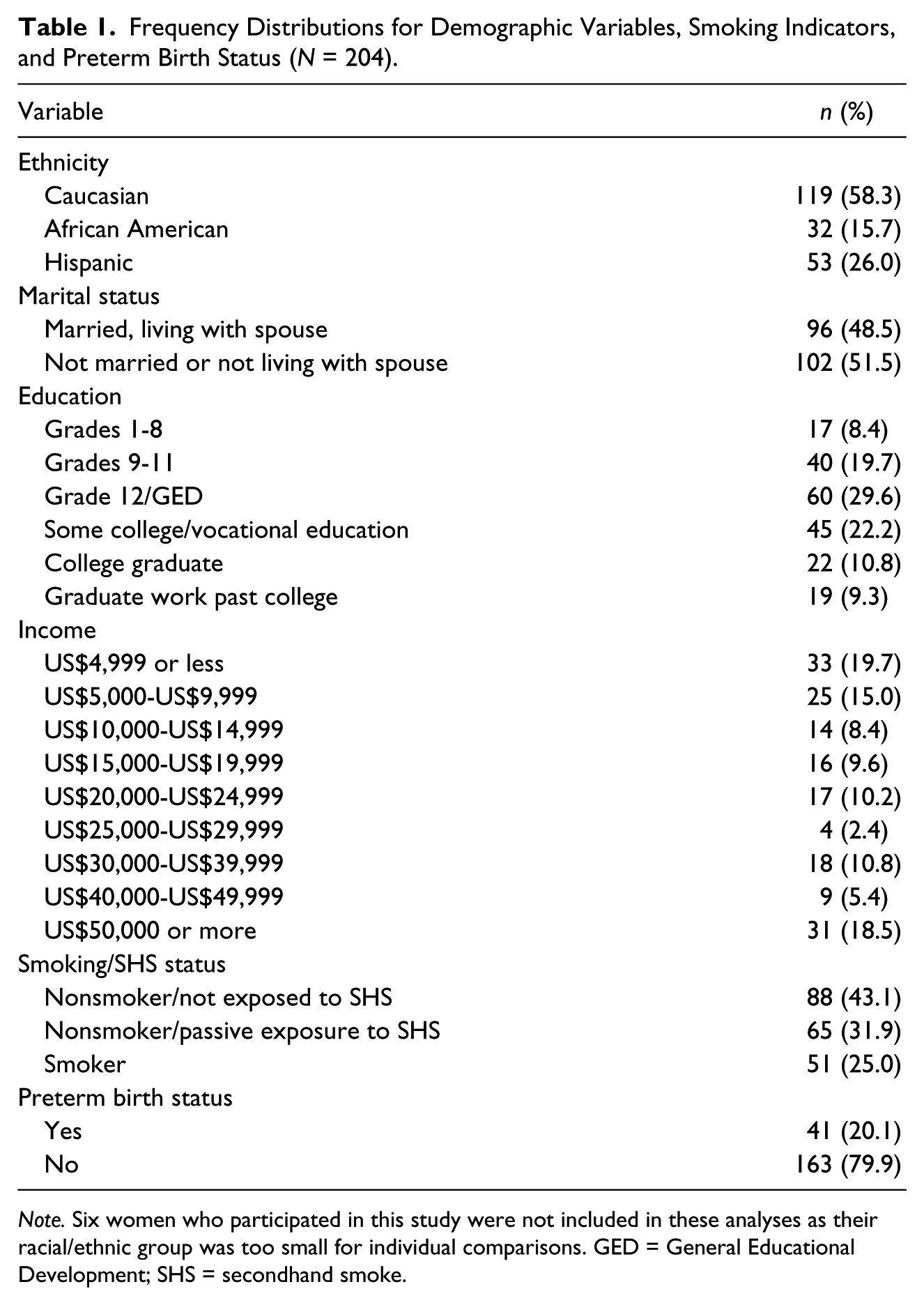
Note. Six women who participated in this study were not included in these analyses as their racial/ethnic group was too small for individual comparisons. GED = General Educational Development; SHS = secondhand smoke.
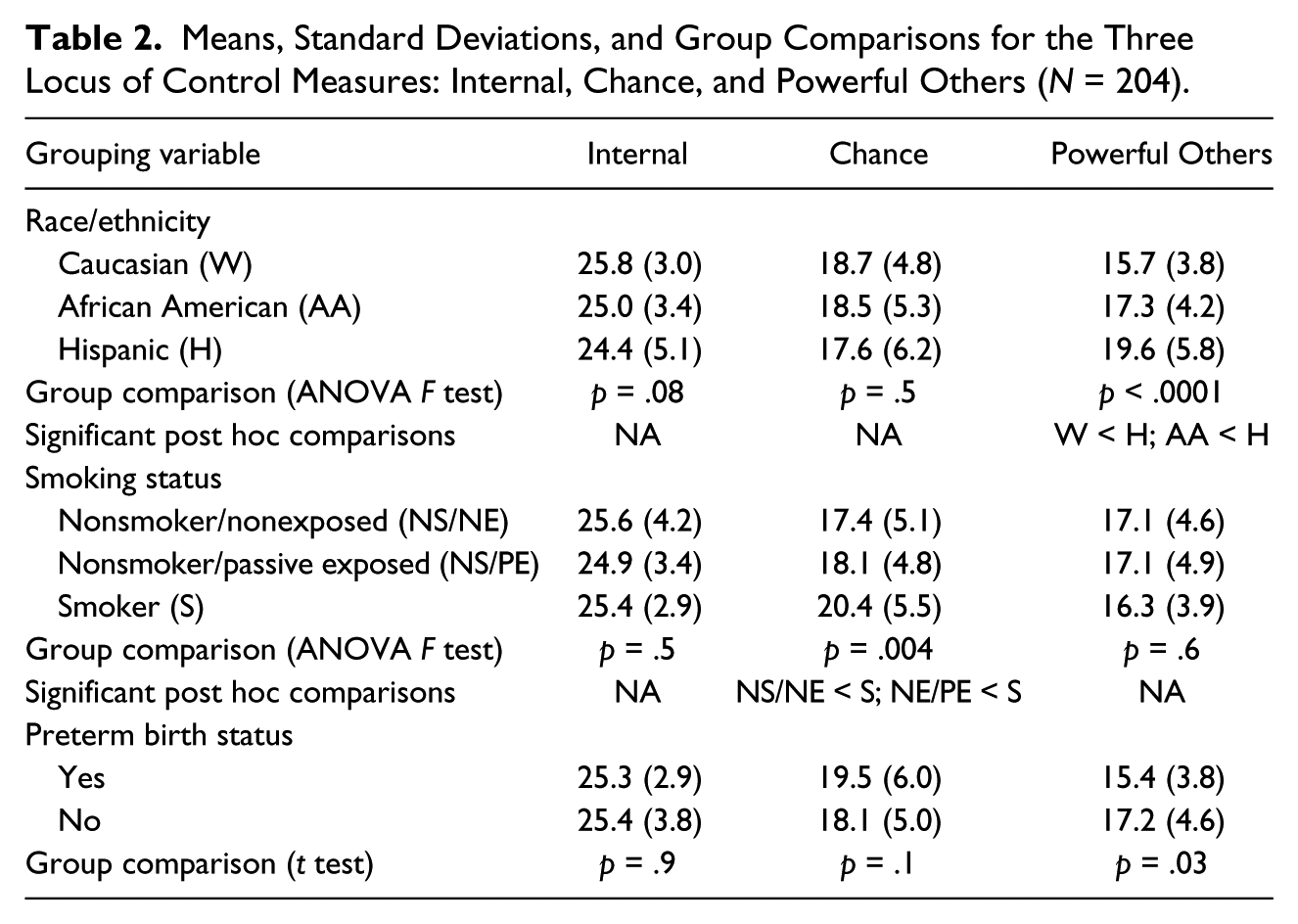
The average score on the Internal Locus of Control scale was 25.4 (SD = 3.6) and scores ranged from 5 to 30. The mean for the Chance Locus of Control scale was 18.4 (SD = 5.2) and the range was from 1 to 30. The average for the Powerful Others Locus of Control was 16.8 (SD = 4.5), with scores ranging from 6 to 30.
The comparisons of the three locus of control scales among the ethnic categories, smoking status categories, and between the PTB categories are summarized in Table 2. For the racial/ethnic comparisons, only the Powerful Others subscale had a significant group effect. The overall F test was significant (p < .0001); post hoc analysis indicated that Hispanic mothers scored significantly higher on this scale compared with each of the Caucasian women and African American women, but there was no difference between the latter two groups. The only significant difference in scores among the smoking status categories was for the Chance subscale. The overall F test was significant (p = .004); post hoc analysis demonstrated that smoking women had significantly higher scores for this subscale than nonsmoking/nonexposed women and nonsmoking/passively exposed women, while the latter two groups were not significantly different in Chance score. The two-sample t tests comparing the subscale scores between women with PTBs and full-term births were not significant for Internal locus of control or Chance, but the comparison for Powerful Others was significant (p = .03). Women with full-term births rated this outcome as higher than those with PTBs.
Means, Standard Deviations, and Group Comparisons for the Three Locus of Control Measures: Internal, Chance, and Powerful Others (N = 204).
As shown in Table 3, the overall model for Internal Locus of Control was significant at the .05 level, with an R2 of .081. The only significant predictor was marital status; women who were married had an Internal Locus of Control that was 1.2 points higher than unmarried women on average. The overall model for Chance Locus of Control was significant at the .01 level, with an R2 of .11. Marital status and active smoking status predicted this outcome. Married women had a Chance Locus of Control score that was nearly 2 points higher than women who were not married. Women who were active smokers had a Chance score of more than 3.5 points higher than those who were either nonsmokers or nonsmoking/passively exposed women. Finally, the overall model for Powerful Others was significant at the .0001 level, with an R2 of .16. Hispanic women had significantly higher scores than Caucasian or African American women. On average, Hispanic women scored more than 4.5 points higher on the Powerful Others scale compared with the other two racial/ethnic groups. The variance inflation factors for each of the models were all less than 3, suggesting a lack of multicollinearity.
Regression Models for Each of the Three Locus of Control Measures: Internal, Chance, and Powerful Others (N = 204).
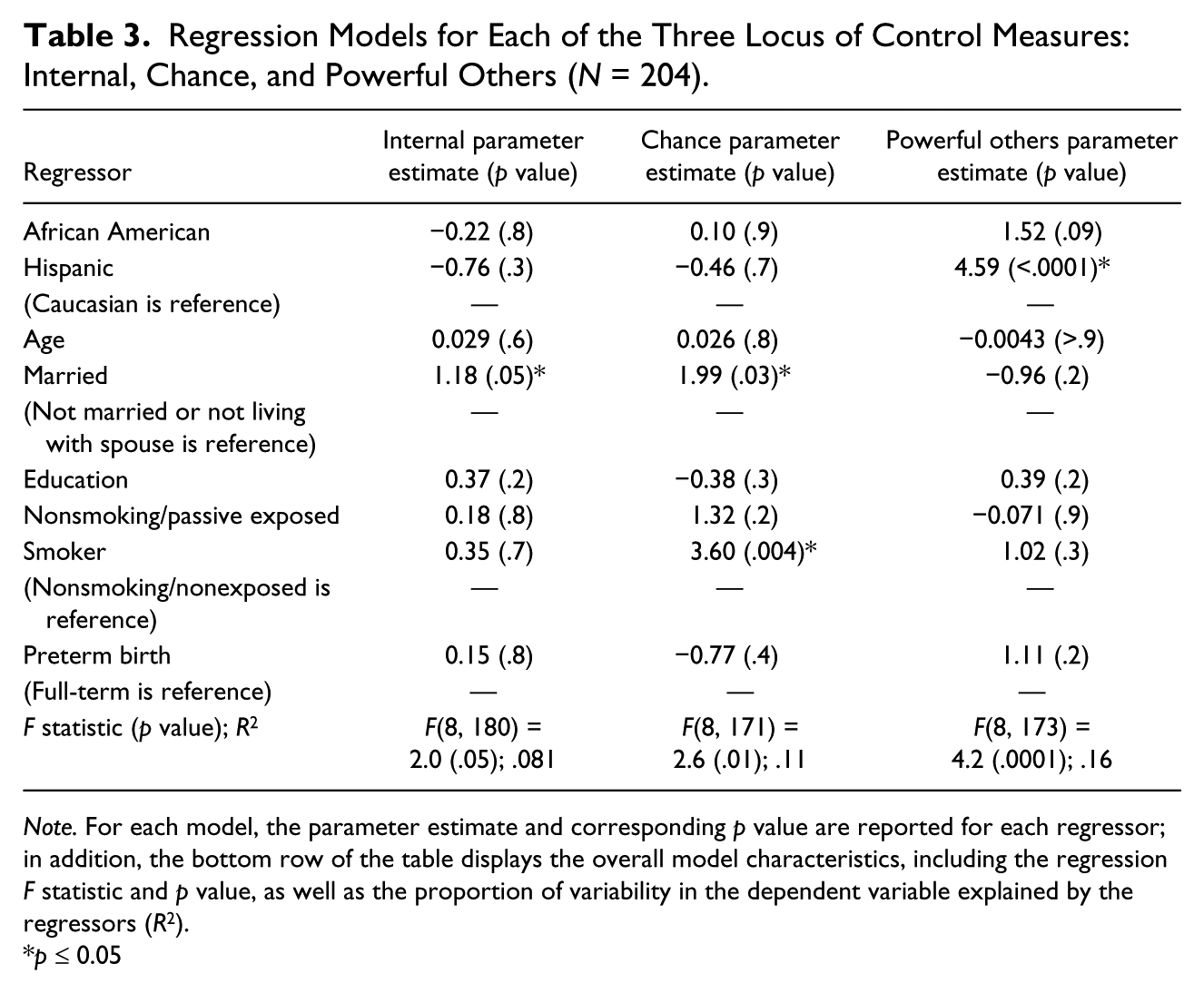
Note. For each model, the parameter estimate and corresponding p value are reported for each regressor; in addition, the bottom row of the table displays the overall model characteristics, including the regression F statistic and p value, as well as the proportion of variability in the dependent variable explained by the regressors (R2).
p ≤ 0.05
Discussion
The FHLC scale was validated by Labs and Wurtele (1986) in a sample of 63 pregnant women. Similar to their sample demographics, our sample was primarily young (25.4 years old), White, and married. Conversely, our sample had a greater proportion of Hispanic women (25% vs. 1%) and was significantly poorer, with the majority of women reporting a household income of less than US$30K per year.
Internal Control consistently had the highest score of the three subscales regardless of ethnicity. All three racial/ethnic subgroups of participants ranked their Internal Control as having the highest impact on pregnancy outcome and their infants’ health. In a study of pregnant women, Haslam and Lawrence (2004) reported the concept of Internal FHLC was most predictive of healthy behaviors during pregnancy (p = .01). The only subscale that differed significantly among the racial/ethnic subgroups was the Powerful Others score. Hispanic women placed higher significance on health care provider influence over their perinatal health when compared with Caucasian and African American mothers. Hispanic mothers scored significantly higher in this Powerful Other measure, even with other demographic and personal characteristics included in the multiple regression model. Wallace, DeVoe, Rogers, Malagon-Rogers and Fryer’s (2007) study of patient interactions with health care providers found that their Hispanic study population reported more positive interactions. The Hispanics “were more likely to report that their health care provider “always” listened carefully, explained things so that they understood, respected them, and spent enough time with them” (Wallace et al., 2007).
PTB status was associated with score on the Powerful Others subscale in the bivariate analysis, but this variable was a significant predictor of Powerful Others score in the multiple regression analysis. The two-sample t test demonstrated that women with full-term infants rated this locus of control scale more positively than those whose infants were born prior to 37 weeks gestation. Sellick, Russell, and Beckmann (2003) organized a study on the effects of primary nursing on patients’ perception of care. Primary nursing, which was first discussed by Manthey, Robertson, and Harris in 1970, “emphasizes (nurse) accountability, patient-centered individualized care, and continuity of care from admission through to discharge” (Sellick et al., 2003, p. 548). The researchers found that the patients perceived the care by the primary nurse as showing a better understanding of the patient, exhibiting and communicating concern for the patient and family, as well as being more likely to give helpful information regarding the health situation (Sellick et al., 2003). The likely result of the primary nursing framework would be a better-informed client who believes their nurse has taken the time to evaluate their unique circumstances. Implicating a similar format to nursing care in prenatal and antenatal clinics may allow for an increase in the number of patients who perceive health care providers as having a significant impact on the outcome of their pregnancy.
The importance of the client’s perception of the health care provider–patient relationship was also revealed in the Peterson, Sword, Charles, and DiCenso (2007) study of postpartum adolescents patients, and in Walker et al.’s (1999) study of the psychosocial and demographic factors related to health behaviors in pregnancy. In each of these studies, it is the client’s perception of care that determines the quality of care. Patients in these studies identified common themes on which they based their perception of the provider–patient relationship such as a feeling of respect and concern, patience, friendliness, and recognition of individual needs. Similarly, de Crespigny (2003) found the very language a health care provider used when speaking with patients had a great impact on patients’ thinking. Identifying common themes of the provider–patient relationship is important to build a mutually trusting relationship thus improving a patient’s willingness to accept provider recommendations.
Evaluation of the Chance subscale revealed significantly higher scores in active smokers compared with nonsmokers and nonsmoking/exposed women in the bivariate analysis. With other demographic and personal factors included in the model, active smoking and marital status predicted Chance score. These results about smoking are consistent with Stewart & Streiner (1995), who reported that smokers were significantly more likely than nonsmokers to believe in Chance (p < .02) and less likely to believe that Internal Control (p < .001) or Powerful Others (p < .001) influenced fetal health. Similarly, Labs and Wurtele (1986) reported that all subscales were found to be significantly associated with smoking status (p < .001). The link between marital status and Chance has not yet been described. Given that marital status was the only significant predictor of Internal FHLC as well, it may be that women who are married and living with their spouse rate their FHLC scores higher in general, compared with women having a different relationship status. Webb et al. (2009) also evaluated the Chance subscale on perinatal outcomes using the Institute of Medicine recommendations on gestation weight gain ratios (ratio of observed/expected weight gain) and reported stronger beliefs in chance were positively associated with lager gestational weight ratios.
The National Vital Statistics Report for births in 2011 provides total preterm birth percentages (birth at <37 weeks gestation) by race/ethnicity: Caucasian, non-Hispanic births (10.49%); African American, non-Hispanic births (16.75%); and all Hispanic births (11.66%) (Hamilton et al., 2011). MacDorman, Callaghan, Mathews, Hoyert, and Kochanek (2007) reported the rate of infant mortality due to PTB in non-Hispanic Black women to be 3.5 times higher than in non-Hispanic Caucasian women. Despite research to the contrary, the number of PTBs among our African American study population was low (11%), whereas PTB among our Hispanic women was higher than national averages (15%). Recent literature on the effect of English acculturation on pregnant Hispanic women suggests there is an increase in adverse pregnancy outcomes; to the degree that acculturated Hispanic women have a fourfold increase in risk of a PTB (Ruiz et al., 2008).
Women who delivered term infants placed higher value on Powerful Others/healthcare provider influence and less value on Chance when compared with women who delivered preterm infants. Women delivering healthy term infants also reported a stronger belief that a health care providers’ knowledge and expertise could affect their prenatal/fetal health. Previous evaluation of FHLC and perinatal behaviors demonstrated women who ranked Powerful Others higher than Chance were more likely to attend scheduled prenatal appointments (Walker et al., 1999). Furthermore, higher Internal FHLC scores were reflected in women who consistently attended prenatal care appointments and attended childbirth classes. These women were also more likely to avoid unhealthy prenatal behaviors such as smoking and drinking alcohol (Haslam & Lawrence, 2004; Stewart & Streiner, 1994, 1995).
Conclusion
Peripartum women rank Internal Control highest among the FHLC subscales, suggesting a strong belief that their prenatal health behaviors influence the health of their fetus. Controlling for other demographic and personal factors, only marital status predicted Internal Control, with married women scoring higher than women who were not married or who were not living with their spouse. Significant differences also emerged when examining the scores of the other two subscales, Chance and Powerful Others. In the multiple regression, the belief that chance guides perinatal outcomes was higher in women that smoked during pregnancy and among married women. Powerful Others scores were higher among Hispanic women and among women with full-term births in the bivariate analysis, but only Hispanic ethnicity was a significant predictor of Powerful Others score in the multiple regression.
Key Clinical Message
Smoking is the most modifiable risk factor associated with adverse perinatal outcomes. Addressing a woman’s beliefs regarding her control over the health of her fetus/pregnancy may provide the basis for developing educational and behavior-modification interventions that highlight her responsibility in taking control of the pregnancy. Furthermore, a woman’s locus of control regarding her perinatal health has cultural and behavioral implications. Hispanic women and women who delivered term infants were more likely to embrace health provider feedback and participate in healthy perinatal behaviors. Conversely, women who believed Chance governed their overall perinatal health were more likely to dismiss provider feedback and smoke during pregnancy. Using a tailored approach to address prenatal smoking cessation, weight gain, and other modifiable high-risk pregnancy behaviors may affect the rate of PTB as well as other perinatal complications. Culturally appropriate and tailored behavior-modification interventions need to be developed to include specific information about the risk that relying on chance versus individual control over high-risk behaviors. For example, women who score Chance high on the FHLC scale should be offered more focused health messaging on the risks associated with prenatal smoking; while stressing the impact of their (Internal) control of their adverse health behaviors on their pregnancy. Nurses and other health care providers can play a critical role in identifying at-risk women (smoking, strong Chance beliefs) while providing a clear message that taking action and modifying high-risk behaviors can reduce risk for adverse pregnancy outcome.
Footnotes
Acknowledgements
The authors offer a special acknowledgment to Mandy Donaldson, BA, BSN, who contributed to the concept and introduction of the paper when working as an undergraduate nursing research intern at the University of Kentucky College of Nursing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Center for the Biologic Basis of Oral/Systemic Disease, NIH/NIGMS 8P20GM103538-09 (PI)—September 23, 2004, to July 31, 2014.