
Abstract
The purpose of the study was to illuminate the meanings of the lived experiences of support as disclosed by fathers of children with congenital heart defect (CHD). Narrative interviews were conducted individually with five fathers of children diagnosed with CHD. A phenomenological-hermeneutic method was used to interpret the verbatim transcribed narrative interviews. The meanings of the lived experiences of support for the fathers were identified in two themes and illustrate the fathers’ feelings of being supported when being in a mutual relationship with others. A third theme illustrates the situation when support is absent. Our findings indicate that support for fathers of children with CHD might be best promoted by the philosophy of family-centered care.
Introduction
Health care professionals have to look beyond the medical perspective to view a family’s needs as a whole. Meeting those needs can be done in terms of family-centered care (FCC; Doherty et al., 2009). FCC stresses that health care professionals provide care for the entire family, even when only a single family member is sick, for example, a child. FCC prioritizes treating the entire family, and the core component in FCC is to archive a partnership with the family (Shelton & Stepanek, 1994). At the same time, FCC considers not only patients’ physical health but also the emotional and psychological health of the family unit (Harrison, 2010). Along the lines of FCC, Higham and Davies (2013b) have studied fathers’ roles in caring for sick children and reported that fathers had an active role and wanted to be with and care for their children as much as mothers, though the children’s nurses sometimes perceived fathers to be marginal in the children’s care. Because fathers were not always involved as equal partners in their children’s care, the care can appear to relate only to mothers, not the whole family (Higham & Davies, 2013a). The ways in which fatherhood is understood affect how health care is designed to support parents and parenting (Premberg, Hellström, & Berg, 2008). Masculinity is considered to be a social construction influenced by the contemporary cultures in which men live and the lifestyles that they exhibit (Connell, 1987). Research has found parenting to be deeply embedded within gender ideologies (Matta & Knudson-Martin, 2006). Historically, fatherhood has been regarded as a function in which a father supports motherhood by protecting and guiding the mother in the care of children, though the mother is considered to be the children’s primary caregiver (Premberg et al., 2008). However, current social norms for Swedish fathers encourage a better balance of work and family, whereas the ideals and role models for men’s relations in parenting have transitioned toward more gender-equal conditions (Johansson, 2011). Among fathers in Nordic countries, those from Sweden take the longest periods of parental leave, which may be explained by Sweden’s more liberal parental leave legislation (Kaul, 1991).
Fathers’ experiences with caring for children with a congenital heart defect (CHD) have received only limited attention, whereas even fewer studies have investigated fathers’ experiences with support for these children. The incidence of CHD cases needing specialized cardiac care is roughly 3 out of every 1,000 live births, and no evidence corroborates any difference among countries regarding the prevalence of CHDs (Hoffman & Kaplan, 2002). Thanks to significant developments in medical and surgical treatments, survival rates for children with CHD increased between the early 1990s and the early 2000s (Allen, Gauvreau, Bloom, & Jenkins, 2003; Lundström, Berggren, Björkhem, Jögi, & Sunnegârdh, 2000). This progress thus increased the number of surviving child patients needing regular treatment and guidance, which consequently placed higher demands on specialized pediatric cardiac care that attempts to meet the needs of families with these children.
Research in nursing has suggested that support for patients and families entails social support (Ericson-Lidman, Norberg, & Strandberg, 2007; Neufeld & Harrison, 2010; Stoltz, Andersson, & Willman, 2007). In Ericson-Lidman et al.’s (2007) study, support is viewed from a different perspective, that is, as being provided, perceived, received, and desired. Ericson-Lidman et al. suggested that at least one provider and receiver are needed for social support and that their relationship determines how the provided support is perceived by the recipient. Meanwhile, Stoltz et al. (2007) described support in two dimensions: the tangible, concrete, and generally impersonal dimension, which concerns increasing family caregivers’ capacity to provide care, and the intangible, abstract, and highly individual dimension, which concerns family caregivers unburdening their minds to another dedicated person. More recently, Neufeld and Harrison (2010) argued that social support entails interactive relationships; they also report that social support can be seen not only in a positive light but also in a negative one—namely, when the support itself is perceived to be nonsupportive, which occurs when interactive relationships are dysfunctional.
In a survey study, Tak and McCubbin (2002) investigated the relationships among family stress, perceived support, and parental coping among parents of children with CHD and found that more perceived support resulted in a higher positive level of individual parental coping strategies among fathers. Being a father of a child with CHD may necessitate support in different forms and to different extents. Parenting these children as a father can involve both challenges and limitations in daily living (Moola, 2012; Rempel, Ravindran, Rogers, & Magill-Evans, 2013). In general, parents of children with CHD must negotiate the involuntary situation of having to deal with the child’s heart condition (Green, Meaux, Huett, & Ainley, 2009; Pye & Green, 2003). Clark and Miles (1999) studied fathers’ experiences with their newborns’ being diagnosed with CHD and found that fathers’ experiences included contradictory reactions: On one hand, the joy of being a father, on the other hand, the grief and fear related to their child’s illness. Fathers must also negotiate the challenges of becoming attached while also facing the fear of the infant’s vulnerability and mortality. The few studies examining fathers of children with CHD have nevertheless tended to include both mothers’ and fathers’ experiences and estimations about psychosocial morbidity. Though parents in general experience symptoms of psychosocial morbidity (e.g., anxiety, stress, distress, hopelessness, and vulnerability; Franck, McQuillan, Wray, Grocott, & Goldman, 2010; Lawoko & Soares, 2006), parents of children with severe CHD experience more psychosocial morbidity than those of children with other diseases or of healthy children (Lawoko, 2007; Lawoko & Soares, 2006; Sarajuuri, Lönnqvist, Schmitt, Almqvist, & Jokinen, 2012; Vrijmoet-Wiersma, Ottenkamp, van Roozendaal, Grootenhuis, & Koopman, 2009). The risk of psychosocial morbidity increases if the parental caregiving burden is high, if parents are dissatisfied with care or feel socially isolated, and/or if they are economically disadvantaged and/or foreigners (Lawoko & Soares, 2002, 2006). Some coping strategies (e.g., alcohol use) have also been identified more regularly among fathers than mothers (Doherty et al., 2009).
Rempel, Rogers, Ravindran, and Magill-Evans (2012) reported that social support intervention is needed to help parents face the challenges of having a child with complex CHD. The kind of support that is actually beneficial for fathers, however, still remains to be studied, whereas more knowledge about the phenomenon of support in the complex context of how fathers perceive such support is generally needed as well. Thus, the purpose of this study was to illuminate the meanings of support as disclosed by fathers of children with CHD.
Method
Design
A phenomenological-hermeneutic method was used for this study, because it has been deemed appropriate for research aiming to elucidate the meaning of lived experiences of any phenomenon, including that of support (cf. Lindseth & Norberg, 2004). The epistemological foundation of the phenomenological-hermeneutic method occurs in philosophy, specifically in philosopher Paul Ricoeur’s work with phenomenology, hermeneutics, and structuralism. Phenomenology is the practice of searching for the essence of a phenomenon, whereas structuralism contributes to the explanation of one part of a text. Meanwhile, hermeneutics generally refers to any interpretive approach. These philosophies are used so that mutual interaction occurs where understanding, explanation, and interpretation merge, to gain understanding of the meanings of lived experiences with phenomena (Ricoeur, 1976). Lindseth and Norberg (2004) have developed a phenomenological-hermeneutic research method for interpreting narrative interviews in health care research as a way of forming an understanding of meanings surrounding health care phenomena. Their method builds upon Ricoeur’s work and provides a model for the interpretive procedure. This model distinguishes understanding, explanation, and interpretation with the aim of not only describing individuals’ experiences but also reaching an understanding of the meaning of the lived experiences with the phenomenon under study. These divisions are practically accomplished in the three phases of the interpretive process.
Setting and Participants
The inclusion period commenced in January 2009 and continued until 25 children with CHD were identified. Both parents of each of these 25 children were identified from the pediatric cardiac outpatient clinic’s registry, and a nurse at the outpatient clinic assisted in the selection of parents to approach for their participation. The selected parents were used in two concurrent studies; the mothers’ experiences are presented in another study (Bruce, Lilja, & Sundin, 2014). Inclusion criteria required fathers to have children born between 1996 and 2006 (i.e., were 3-12 years old in 2009), diagnosed with one or more CHD, and who had been visiting the pediatric cardiac reception at least once per year. Children with intellectual impairment, which could possibly contribute to other support needs, as well as fathers who did not speak Swedish, were excluded from the sample.
Five fathers consented to participate, all of whom lived with their child’s mother; three were married, whereas two cohabited. All participating fathers were employed, and their mean age was 37.8 years (range: 24-47 years). Two of the fathers had multiple children, only one of whom had CHD. The mean age of children with CHD—one girl and four boys—was 6.6 years. The children had been diagnosed with aortic stenosis, hypoplastic left heart syndrome, tetralogy of Fallot, or pulmonary atresia.
Data Collection
Data collection consisted of narrative interviews (cf. Mishler, 1986) conducted individually with each father one time, with the exception of one father who wanted to be interviewed together with his partner. The interviews lasted from 40 to 120 min and were conducted by the same researcher (E.B.); the researcher and the fathers had never met before the interview. All fathers were invited to choose an interview setting that would allow them to feel relaxed and free to share their experiences. The location for the interviews was chosen by the fathers—four fathers wished to be interviewed at the university, and one father chose to be interviewed at his home. Older fathers had neither more nor less to tell than the younger fathers. The interview that lasted longest (120 min) involved both the father and mother of a family who decided to conduct the interview together for family reasons. All interviews were conducted using the same interview guide, which consist of the following open-ended questions: (a) Can you please tell me what support means to you in your situation? (b) Can you please describe a situation in which you and your child received the desired support? and (c) Can you please share with me a situation when you and your child received what was meant to be “support” but, as you experienced it, was not the kind of support you desired? Additional probing questions such as “Who?” “When?” “What do you mean?” and “Can you tell me more?” encouraged more detailed explanations. The interview guide draws upon the work of Ricoeur (1976), who stated that people use language to express the reality and world in which they live, as well as that of Mishler (1986), who has suggested that narration allows interviewees to highlight what is most important to them in their lived experiences. In this study, all interviews were digitally recorded and transcribed verbatim, with the addition of emotional expressions marked in parentheses in the transcript (e.g., “crying,” “laughing,” “talking intensely,” “talking slowly”). The interview conducted with both parents was transcribed using a different color for each parent.
Ethics
A university ethics committee approved the study, and the head of the pediatric cardiac outpatient clinic at a hospital in Sweden approved our request to select fathers and mothers from the clinic’s visitor register. Written information was sent to both the mother and father of each selected child, along with a request for his or her informed consent to participate. The fathers were also informed that they could withdraw from participating at any time without having to provide any explanation.
Data Interpretation
The phenomenological-hermeneutic method involves a movement from understanding to explanation and then to deeper understanding, all by progressing from the whole to the parts and so on to a deeper understanding, as described in the method’s three phases: naive understanding, structural analysis, and comprehensive understanding (cf. Lindseth & Norberg, 2004).
In the first phase, a naive reading of the interview texts as a whole was performed by reading the text over and again until an initial understanding of the meanings of the phenomenon was reached. During the second phase, a structural analysis was conducted to structure and process the interview text to reach an explanation. The text was then divided into meaning units. Here, a meaning unit refers to anything from a few words to several sentences, though each unit represents only a single meaning. The meaning units were then subjected to an additional step of condensation and abstraction, and the abstracted meaning units with the same meaning were grouped and formulated into subthemes, which were further grouped into themes. In this way, structural analysis validated the naive understanding. The third phase of interpretation consisted of gaining a comprehensive understanding, which involves a comprehensive, critical reflection upon the naive understanding, subthemes, and themes that have emerged in structural analysis, as well as the study’s context and purpose, the researchers’ pre-understanding, and the related literature, all to reach a deeper understanding of the meanings of support according to fathers of children with CHD and to illustrate what the text has indicated and pointed to (cf. Lindseth & Norberg, 2004).
Rigor
Our study’s trustworthiness was carefully assessed throughout the process of planning and implementing the study. Though only five fathers chose to participate, there was a substantial variation in their experiences due to age differences and variation among their children’s CHD. Both kinds of variation resulted in data collection consisting of rich, detailed interviews. Using an interview guide and an experienced interviewer also bolstered the study’s credibility.
Transferability was achieved through a detailed description of the data collection, analytical process, and results. Though this study’s results are not generalizable, they may be transferable to other groups of fathers of children with CHD or another chronic disease. All researchers were involved in the analytical process as a means of providing dependability. To achieve confirmability, interviews were digitally recorded and transcribed verbatim. The “Findings” section of this article includes quotations from the interviews that enhance the findings (cf. Hanson, Balmer, & Giardino, 2011).
Findings
Naive Understanding
For fathers of children with CHD in our study, feeling supported means being involved in their children’s care and having opportunities to be connected with others, including their families, health care professionals, and other significant persons in their environment. Fathers emphasized that, when the whole family is involved in the child’s care, it becomes possible for all family members to support each other. If such collaboration is possible, fathers seemed to feel secure, pleased, and supported. When the need of the fathers and their families to be involved is not taken into account, the fathers appeared to feel that support is lacking, which thereby caused confusion and a lack of affirmation. The fathers seemed to feel a lack of support when they had to struggle for their child’s or family’s right to the desired support, which put considerable pressure on them and led to significant concern, anxiety, sorrow, and loss of energy.
Structural Analysis
The structural analysis of the meaning of support for fathers of young children with CHD produced three themes: “Feeling supported and safe when receiving opportunities to be involved in care,” “Feeling supported through connectedness with others,” and “Lacking support.” The themes are presented in Table 1.
Overview of Themes and Subthemes Concerning Meanings of Support for Fathers to Children With Heart Defects.
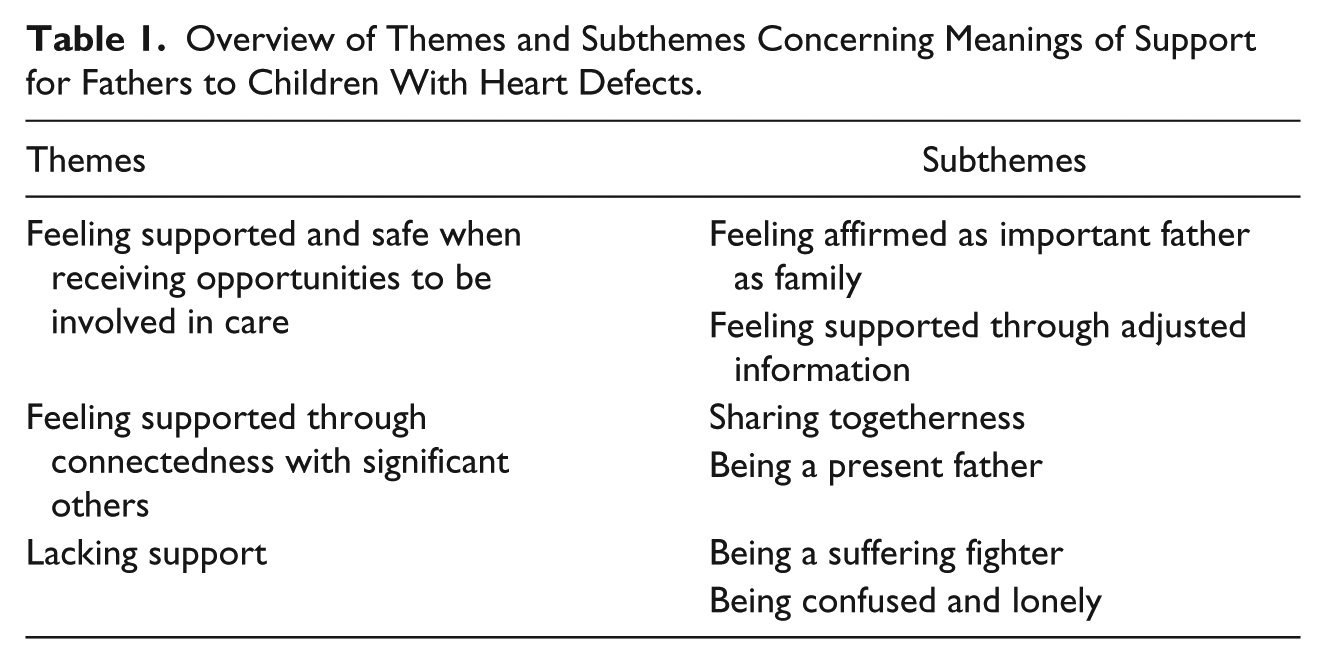
“Feeling supported and safe when receiving opportunities to be involved in care.”
This theme reflects fathers’ feelings of being safe when health care professionals see them and their families as important and also when fathers and their families are involved in the child’s care. When fathers were involved in their child’s care, they experience having not only a better understanding of the situation but also a greater sense of control over it.
The subtheme “Feeling affirmed as important father as family” refers to fathers’ feelings that health care professionals treat their families as unique and prioritize their child’s care and well-being in addition to the family’s needs. If health care professionals included fathers in the child’s care, then fathers appeared to feel they are important to the child, their family, and the health care professionals, which implied that the fathers feel more secure and in control. Hence, they feel that they are being supported. Fathers also experience feeling more secure when the health care professionals are highly qualified, have specialized knowledge, and have experience treating families and children with CHD. In this sense, skilled health care professionals support fathers and their families by meeting their needs and affirming their concerns.
. . . [The health care professional was] incredibly professional and impressive . . . she really knew what she was talking about, and she could really take care of people in shock, you know. This has meant a lot for me. This is the situation I always will remember. (Father 3)
Fathers feel supported when they have confidence in health care professionals, which most readily occurs by the health care professionals’ affirming that the family is normal, acting interested in the family, and talking about topics other than the child’s disease. Meanwhile, a feeling of being secure occurs when the families have opportunities to meet repeatedly with the same health care professionals and when those professionals know the family and their unique needs and wishes. Fathers appeared to experience secure and gain peace of mind during meetings with health care professionals who approaches sympathetically. Fathers also feel safe and recognized as an important member of the family when health care professionals not only give their time but also stand by the fathers’ side and help them fight for their families’ right to get information and be together.
The subtheme “Feeling supported through adjusted information” means that informative meetings with health care professionals make fathers feel supported and secure, when involved in their child’s care. Fathers appeared to feel fortunate when such care is designed using the latest research in the field. In addition, fathers feel safe when they have information about their children’s heart defects. Such understanding means relief to fathers as they seemed to feel it easier to bear the grief of their children’s heart conditions when they receive knowledge about the disease.
. . . when I got the bad news . . . it was like a stone was falling on me . . . yes. . . it was heavy—heavy—but at the same time, it was great to have a picture of what was wrong [clears his throat]. (Father 1)
When fathers are met by calm and informative health care professionals during chaotic situations, they feel stronger and are more involved in the situation, which also makes them feel supported. Knowing to whom they can turn with different kinds of questions and problems also calms the fathers. When they receive information about their children’s future possibilities, especially the children’s chances of regaining a normal life, they experience hope, which is another source of strength.
“Feeling supported through connectedness with significant others.”
This theme means that fathers feel it is possible for them to be the fathers they wish to be. This feeling of competency helps fathers cope with their experiences and feel like someone without a sick family member.
Within this theme, the subtheme “Sharing togetherness” refers to fathers’ needs to share their experiences with their family and friends and to feel like normal fathers of normal families. When fathers have the opportunity to share their experiences and to find solutions together, they seemed to feel a significant sense of relief. Sharing their experiences with other families of children with heart defects means that fathers seemed to feel less alone. Sharing experiences also appeared to give fathers the feeling of being part of a whole family.
. . . So, all the bad news we received, we received it together, and she [my partner] has always been there for me. (Father 3)
When fathers know that there are other families who resemble their own families, they find it comforting, and it generates an experience of not being alone and of being a normal family. This feeling of normalcy also fostered confidence. Fathers also seemed to find satisfaction when their child socializes with other children. In addition, sharing their experiences with a health care professional who knows the family and their unique situation makes fathers feel supported.
. . . great support . . . It is the small joys in life, such as when she [my daughter] got a tool—an electric bike—for which she was very grateful. It has meant a lot to her; she can get to and from friends’ houses by herself . . . It feels good to know that she does not experience life negatively . . . it feels good. (Father 5)
The subtheme “Being a present father” refers to fathers receive support from health care providers that enables them to be a present father and to focus on their children, and thus feeling supported. Furthermore, fathers wanted help coping with siblings and everyday life.
. . . The older brother was a little disappointed and became angry and slightly on the offensive against the little brother [with CHD]. We should have provided support to the boys all along, so that there would not be any uncertainty between them. (Father 2)
When health care professionals help the family provide information to school staff about the constraints and opportunities of living with CHD, fathers seemed to feel secure and supported. Furthermore, fathers experience that their child does not feel alone and that the child knows there are others who share his or her experience. For this reason, they appeared to feel relieved and supported when health care professionals give the child tools to deal with difficult situations.
“Lacking support.”
This theme means suffering in loneliness and feeling forced to fight to receive the support desired by fathers.
The subtheme “Being a suffering fighter” means that fathers experience themselves as being in a battle for their child’s and their family’s health and well-being, a perception that arise when looking for possibilities to be together, get information about the child’s disease, and be involved in the child’s care. During such times, fathers struggle to cope with their own experiences and feelings. In their efforts to get others to understand their child’s situation and needs, fathers seemed to feel drained of energy. Fathers also feel exhausted when they have to fight for the family’s right to be together and be there for each other while the child is undergoing complicated treatment.
. . . with these trips to the heart clinic, the policy at our county council is that only one parent can follow the child, when I attempt to fight them [the health care professionals], they will say no. It feels so hard in this situation that you can’t help but be sour and angry . . . (Father 4)
The subtheme “Being confused and lonely” refers to the emotions that fathers experience when they are not involved in the care of their child. When information from health care professional is missing or unclear, fathers seemed to feel alone and confused. If fathers are hindered from being near their child and are not invited to be involved in their child’s care, they appeared to experience confusion and loneliness as a father, partner, and person. Fathers seemed to experience disorientation in their role as fathers when they see their child hidden behind medical equipment and when health care professionals do not include them in what is happening or explain what they can do for their child. If fathers feel that their employers or friends do not understand their wish to be close to their child, they experience alienation. When fathers are hindered from being with their child, they seemed to feel worried all the time, and that gives them anxiety.
Yes, I feel concerned and everything, all the time; there is never a quiet moment. It feels like the hardest time is when I am at work. I am completely disconnected from her [daughter], and you never know. I am worried that I will not have time to keep up with her in time. I am simply worried. (Father 1)
Fathers experience alienation when they and their family were unable to participate in activities together with the whole family because the child with CHD cannot participate. When family members are separated from each other, fathers feel vulnerable.
Comprehensive Understanding and Reflection
The meaning of support to fathers in our study points to support as supportive relationships in shared togetherness. Fathers desire to be supported as a whole family so that the family can support each other and share the experience of being a family with a child with CHD. Through fathers’ perspectives of support, being supported as a whole family contributes to feelings of being a normal family and being able to handle the demands of life. Our findings mirror Wright and Leahey’s (2009) theory about family units. Wright and Leahey noted that all family members are linked together to form a whole and that they together strive for common balance. However, if any member undermines this balance—for example, by getting a disease—it will somehow inevitably affect all other family members. Our findings illustrate fathers’ desires for their families to be supported as whole families and that, when support is provided according to fathers’ desires, fathers seem to feel confident and satisfied with their own situation and that of their families. This finding closely mirrors Fägerskiöld’s (2006) findings from studying fathers of infants and their expectations for their child’s health care. The core category of Fägerskiöld’s findings stresses trusting relationships between fathers and nurses—relationships that are considered to be a precondition for support to be experienced—which was also found in our study. Fägerskiöld’s findings, in addition, refer to fathers’ desires to be involved in their child’s care.
Our findings also suggest that masculinity is subject to an ongoing process of change. In general, fathers in our sample seemed unsatisfied with the detached, passive role traditionally assigned to fathers. In this sense, Swedish society’s new demands on fathers and fatherhood appear to be in line with this study’s fathers’ wanting support to facilitate shared parenting. This transformation reflects Connell and Messerschmidt’s (2005) thoughts on masculinity as a concept that evolves and is influenced by culture. Our study’s findings more specifically illuminate fathers’ desires for support in the form of interactive relationships, which previously have been assumed to belong to femininity, because women have traditionally been expected to seek support in social relationships to maintain their health and well-being (cf. Connell, 2005). These findings are also in line with those of Connell and Messerschmidt, who argued that men can strategically adopt or distance themselves from hegemonic masculinity according to their needs for interaction. Indeed, the present study’s findings do not point to fathers feeling trapped in structures of hegemonic masculinity. They simply struggle to achieve a common sense of well-being for the whole family and harmony and balance in the family unit. This is confirmed by Schofield, Connell, Walker, Wood, and Butland’s (2000) conclusion regarding the importance of seeing men’s and women’s health in relation to the other. In addition, Connell and Messerschmidt (2005) suggested that hegemonic masculinity needs to incorporate a more holistic understanding of gender hierarchy, which is an argument also in line with the meaning of support to the fathers in our study. Therefore, fathers can be seen to appreciate the kinds of support that will enable them to achieve harmony and balance in their family lives, which can in turn help them to feel whole as persons, as fathers, and family.
Supportive relationships in shared togetherness are experienced by fathers when their and their families’ unique needs are recognized and treated as if worthy of consideration. In such a situation, fathers appear to feel that they are important, and thus safe. Haugstvedt, Graff-Iversen, Bukholm, Haugli, and Hallberg (2013) reported a similar finding in their study, about parents’ experiences when living with children with disabilities. They described parents’ perceptions of their own value as sources of new energy and satisfaction. Our findings point to a similar description of positive interactive relationships made by Neufeld and Harrison (2010). Their description of positive interactive relationships involves being met as a unique and important person and family. Health care professionals must seek out and identify each family’s unique needs and desires, which vary depending on the situation. A reciprocal exchange between health care professionals and families is also necessary to achieve effective interaction.
In our study, supportive relationships as part of a shared togetherness are also generated when fathers are included in an informational exchange with health care professionals. This seems to foster feelings of security and makes it easier for fathers to bear their grief. Similar findings were reported by Ringnér, Jansson, and Graneheim (2011), who focused on parents in pediatric oncology who had experienced being acknowledged as a person of significance. In these situations, parents felt safe and secure when they were well informed, despite the inherent uncertainty of the situation. In this sense, the meaning of support in our study indicates relationships in which the family is informed, meaning that information is going back and forth between the family and health care professionals. This finding is similar to Neufeld and Harrison’s (2010) description of the key ingredients of functioning and supportive relationships, one of which is a reciprocal exchange between family and health care professionals.
Supportive relationships as part of a shared togetherness allow fathers to be present and appeared to provide them with a feeling of being able to cope and deal with everyday life. Our findings reflect Kratz, Uding, Trahms, Villareale, and Kieckhefer’s (2009) findings, which highlight effective strategies for coping with challenges faced by parents of children with special health needs. According to their study, a cornerstone of managing special health care needs is developing a trusting relationship with health care professionals, which parents have emphasized as crucial to a family’s quality of life.
When supportive relationships as part of a shared togetherness are lacking, fathers appear to be forced to go into battle for their families and then they suffer from these feelings of having to be a warrior. A lack of support such as this occurs when the need for sharing, informative relations with health care professionals is not taken into account. Neufeld and Harrison (2010) described similar experiences and note that a lack of interaction is perceived as being a part of nonsupportive relationships. Neufeld and Harrison have pointed toward three major forms of nonsupportive interactions: negative interactions that undermine credibility as caregivers, interactions in which expected support is ineffective, and interactions in which expected support is absent. Negative interactions include minimizing caregivers’ concerns, not understanding their intent, and/or not believing their stories.
An absence or lack of support means that fathers are excluded or not seen as being part of a related whole. In such an absence of support, the situation brings on greater suffering (e.g., Neufeld & Harrison, 2010). In our study, when such a relationship was lacking, fathers seemed to feel a lack of trust; they were distressed and might have been in conflict with health care professionals about the child’s treatment plans and/or their participation, or they may feel blocked from or in the way of treatment.
From a nursing perspective, the interpretations of the present study’s findings suggest that the meanings of support for fathers of children with CHD probably can be best promoted by the philosophy of FCC in pediatric nursing (Harrison, 2010). On this point, Svavarsdottir and McCubbin (1996) have reported that parents of children with CHD should be met by the health care system from a family perspective. Higham and Davies (2013a) have illustrated that even nurses who practice FCC tend to focus on mothers and overlook fathers’ experiences. They further argued that it is important that nurses involve fathers as partners in the child’s care, which our findings also clearly point toward. Fathers desire attention from health care professionals so they can become involved and share in the care of their child. This idea is supported by Higham and Davies as well, who found that the father’s role is often overlooked and downplayed and that fathers are rarely perceived to be equal partners in care.
In a review of literature addressing FCC, Harrison (2010) identified eight core elements of how nurses should provide FCC to families: (a) the family should be considered to be constant; (b) it is important to facilitate family−medical staff collaboration; (c) complete and unbiased information should be exchanged between family and staff in a supportive way; (d) cultural diversity and individuality in the families should be recognized and honored; (e) different coping methods should be recognized and respected, and support should be adapted to the families’ needs; (f) a family-to-family supportive network should be encouraged and facilitated; (g) flexible and accessible care should respond to families’ unique needs; and (h) it should be understood that families possess a breadth of strengths, concerns, thoughts, and aspirations beyond their need for medical interventions. Similar to the eight elements in Harrison’s study, the meaning of support for fathers of children with CHD in our study—both desired and perceived—include being involved in their child’s care, being in informative, caring meetings with skilled health care professionals, and being treated as a unique family, meaning that the child’s needs are prioritized, but that the whole family’s needs are also given prominence as well.
Limitations
Only a few fathers consented to participate in the present study, even though our initial request and additional reminders were sent to 25 fathers of children with CHD. All of the fathers who participated in our study cohabited with their child’s other parent. No interviews were conducted with fathers who were single or who lived apart from or were divorced from their child’s other parent, though those fathers’ experiences would have further enriched our findings.
Conclusion
The meaning of support as disclosed by the fathers of children with CHD in our study is about being in a sharing relationship with others—both within the family and with health care professionals—and that health care professionals should involve fathers as significant partners in the care of their children. Though fathers want to be strong and to support their partner and the rest of the family, fathers also need emotional support. Based on the meaning of fathers’ lived experiences with desired and perceived support, our study highlights supportive relationships as part of shared togetherness, which for fathers entails well-being. Well-being, in turn, involves opportunities for support within the family, which helps to provide fathers with a sense of wholeness and significance as a person, as a father, and as a part of a family. When the required support is absent, however, fathers may feel forced to fight for themselves and their families’ needs. Such a lack of support also induces feelings of hardship and alienation. In these situations, a father’s and his family’s value seems to be reduced, and a father’s ability to manage and understand his personal and his family’s situation becomes complicated. According to our findings, health care professionals should therefore be careful not to treat mothers and fathers according to traditional gender roles, but instead to listen to the needs of each individual, each unique father, and each family. Such patient−health care professional relationships are embodied in FCC, a nursing philosophy concerned with the relationship between families and health care professionals. Despite ongoing work for gender equality, when it comes to the nursing philosophy of FCC, traditional approaches toward acknowledging and accommodating fathers and mothers continue to predominate, though doing so effectively marginalizes fathers in the care of their children. In response, our findings suggest that support for fathers of children with CHD may be best promoted by FCC.
Footnotes
Acknowledgements
The researchers are grateful to the fathers who participated in the study.
Authors’ Note
K.S. and E.B. made the study design, and E.B. did the interviews; all authors have contributed to the data interpretation and the manuscript in preparation. The manuscript has been approved by all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.