
Abstract
This study reports the association between parental uncertainty and characteristics of 123 parent–child dyads prior to the child’s herniorrhaphy. A cross-sectional study design and Mishel’s Parents’ Perception of Uncertainty Scale (PPUS) were used. Parent participants were married (98%), had a university degree (45%), identified with a religion (77%), and worked (69%). More boys (76%) than girls (23%) underwent herniorrhaphy (average age = 2.26 years); 60% were the first-born child and 25% were premature. More children presented with unilateral (63.4%; right = 44.7%, left = 18.7%) than bilateral (36.6%) hernias and most were primary (98%). Overall uncertainty was perceived as moderate and ambiguity had the highest score. Religion, birth order (first child), and hernia site (bilateral) explained 20.6% of total variance of uncertainty. Providing information about postoperative symptom and pain management is important for all parents, particularly for parents identified with a religion and whose first-born child had bilateral hernias.
Introduction
Understanding the experiences and perceptions of parents of an ill child is important because they can influence parental caring ability and management of a child’s medical condition (Cacchione, 2016; Modi et al., 2012; Trowbridge & Mische-Lawson, 2014). When children undergo surgery, it can be a stressful and anxious time for parents, who often receive an array of medical information regarding their child’s diagnosis and disease progress, surgical procedure, anesthesia, postoperative care, and prognosis (Salisbury, La Montagne, Hepworth, & Cohen, 2007). Parental experience of childhood illness and uncertainty was studied by Mishel (1981, 1983, 1990, 1999); however, the area lacks an abundance of recent evidence. Past studies have included parents of hospitalized children (Mishel, 1983), children with epilepsy (Mu, Ma, Hwang, & Chao, 2002), children with cancer (Mu et al., 2001; Yeh, 2001, 2003), children with critical illness (Santacroce, 2003; Tomlinson, Kirschbaum, Harbaugh, & Anderson, 1996), and premature infants (Miles, Funk, & Kasper, 1992). One recent study used Mishel’s theories of uncertainty to develop a conceptual model of coping and growth in parents of children with cancer, indicating that parental uncertainty has a negative effect on coping and can be determined by the child’s health condition and the parents’ perception of social support (Lin, Yeh, & Mishel, 2010). The dearth of studies about parents who care for children requiring surgery warrants investigation because parents are the primary caregivers for the children, and this study highlights important aspects of the care context and issues related to parental support.
Although limited reports attempt to estimate the incidence and to describe clinical profiles of children with hernia, infantile or congenital inguinal hernia tends to first occur when a child is aged below 12 months old (Kingsnorth & LeBlanc, 2003). Inguinal hernias are common in the general population, and even more so among children; they occur in 27% of men and in 3% of women and are estimated to account for 10% to 15% of all surgery (Primatesta & Goldacre, 1996; Schumpelick & Wantz, 1995). Prompt surgical intervention is important because of the therapeutic implications of hernia and lifelong outcomes on health. Herniorrhaphy has become the choice of surgical intervention and standard treatment in hernia. It is estimated that more than 20 million inguinal hernia repairs are performed each year globally with an incidence of one to three per 1,000 population (Bay-Nielsen et al., 2001; Kingsnorth & LeBlanc, 2003). A report on the mortality of inguinal hernia in 1971 based on U.S. Medicare discharge data revealed a mortality rate of 0.005 (five per 100,000) in comparison with a mortality rate of 0.05 (five per 1,000) when inguinal hernia complicated by obstruction underwent surgery. The mortality rate, however, had fallen to three per 100,000 in 1998 as the result of the success of elective surgery (Kingsnorth & LeBlanc, 2003) remains low.
Background
Definition of Inguinal Hernia
Although most inguinal hernias can be palpable at diagnosis, ultrasound examination is the most accurate method to distinguish the differences in hernia location and size (Kingsnorth & LeBlanc, 2003). When a groin hernia is diagnosed, surgical repair is required, especially if it is complicated by incarceration or strangulation. Groin hernia is a defect of the transversalis fascia where the myopectineal orifice is an area of weakness formed by several muscles of the internal oblique, the transverse abdominal, iliopsoas, rectus and sheath, and the pectin of the pubis. Oblique appearance of the inguinal canal (a sphincter-like structure of the internal ring) and the transversalis fascia determines the intactness of abdominal wall. The common classification systems attributed to Nyhus, Gilbert, Bendavid, and Schumpelick of Aachen have been used by surgeons to determine the types of inguinal hernia and the repair matched in accordance with the defect (Schumpelick & Wantz, 1995). Nyhus’s classification proposes four different groups according to the diameter and status of the fascia transversalis in the posterior wall of the inguinal and femoral canal. Gilbert’s classification uses five grades (I-III = indirect, IV-V = direct) according to the anatomical and functional defects of the internal ring and posterior wall. Bendavid’s classification is based on the dimensions of the hernia by the definition of types, stages, and measurements in its classification system. Schumpelick of Aachen’s classification uses a European anatomical method by classifying as direct and indirect inguinal and femoral hernias with three different measurements of the orifice (<1.5 cm, 1.5-3.0 cm, >3.0 cm).
Parents of Children With Illness
Parents are the key persons contributing to the quality of a child’s illness experience and recovery trajectory. An ill child’s psychosocial context can affect compliance with treatment and care; they are largely dependent on the ways their parents effectively manage distressed behavior and their caregiving role, including the delivery of medical care (Holm, Patterson, Rueter, & Wamboldt, 2008; Modi et al., 2012). Effective outcomes require a parent to quickly process (appraise) a wide array of medical information that may be foreign to their experience, and this adds to the emotional turmoil of dealing with a child who is ill and requires surgery. Parents who are well informed and understand information provided by health professionals in relation to their child’s illness course, treatment regime, surgical procedures, symptom management, and prognosis tend to cope better with the events that occur during the process (Wang, Lin, Lee, & Lee, 2016). Importantly, for parents of an ill child to cope effectively, they require a successful cognitive appraisal process. Cognitive appraisal processes relate to decision making and can be influenced especially by any uncertainty of the parent(s) of a child with illness. The components of parental uncertainty include ambiguity, lack of clarity, lack of information availability, and unpredictability of the medical information pertinent to their child’s treatment and care (Mishel, 1981, 1988, 1999; Mishel & Clayton, 2008; Mishel, Padilla, Grant, & Sorenson, 1991; Neville, 2003).
Parents’ Uncertainty and Characteristics
Literature related to the relationship between parental uncertainty and the characteristics of a child with illness is minimal. Studies on the experience of parents of children with illness indicate greater stress and uncertainty in the management of a child’s care and greater concerns with respect to a child’s recovery and development (Caicedo, 2014; Cohen, 1993; Wang & Barnard, 2004, 2008). Survey studies have attempted to estimate both the level of parental uncertainty and also influencing factors (Santacroce, 2003), but these types of studies remain limited. Current literature indicates that parents of a child undergoing an illness experience have an increased level of perceived stress and uncertainty (Miles et al., 1992; Wang et al., 2016). A study examined stress, uncertainty, and anxiety for 23 parents of preterm infants and found an elevated level of perceived uncertainty, particularly in the aspect of unpredictability in relation to illness course and outcome (Miles et al., 1992). There are also differences between mothers and fathers in relation to parental uncertainty (Lin, Yeh, & Mishel, 2010; Mu, 2005; Mu et al., 2001). Although both mothers and fathers can score high for levels of parental uncertainty in the dimension of unpredictability, overall mothers experience higher levels of perceived uncertainty in all dimensions compared with those of the fathers, particularly in the parental role alteration (Miles et al., 1992). Although very limited, when examining the association(s) between parental uncertainty (or stress) and the child’s characteristics in the context of childhood illness, factors such as the child’s younger age, severity of illness symptoms, degree of dependence on medical care and equipment, and gender (male) in a Chinese family have been associated with parental stress (Wang et al., 2016). The association between parental uncertainty and a child’s characteristics in the context of childhood surgery warrants further investigation because of the current predominance of Western literature reporting parental uncertainty in the childhood illness which may be different in the Chinese parents. This study focused on describing the uncertainty of Chinese parents of children undergoing herniorrhaphy.
Conceptual Framework
This study used the uncertainty in illness theory developed by Mishel as its conceptual framework (Mishel, 1981, 1988, 1990). In the context of illness, uncertainty is defined as discernment of an event or situation and characterized as an incapacity to comprehend the meaning of illness episodes and to control management of symptom events and health outcomes. Individuals experience uncertainty, especially when information is unclear, conflicting, or varied regarding the treatment for illness and use of the health care system. Perceived uncertainty is regarded as one of the key factors contributing to a stress response of an adult patient toward an illness experience and can hinder coping (Mishel, 1981).
Mishel developed four dimensions related to conceptualizing perception of uncertainty of parents caring for hospitalized children: ambiguity, lack of clarity, lack of information, and unpredictability (Mishel, 1983). Ambiguity is defined as an inability to give a rationale for the cause and effect of an event. Feeling of uncertainty is heightened when a trigger or stimulus (such as childhood illness) is thought to be ambiguous. During the need to support a child through an illness experience, the context of the health care system and medical technology can lead to an experience of ambiguity. Parents of an ill child are challenged by complicated processes associated with health care systems and the importance of decision making. They become vulnerable when faced with dependence on medical technology (including equipment and surgery) especially when it has a role in controlling the health of their ill child (Wang & Barnard, 2008). Feelings of ambiguity are particularly overwhelming when parents cannot understand or manage their child’s discomfort, either from the disease course or as a result of surgery (Mishel, 1981, 1983).
Lack of clarity is the second dimension of parental uncertainty and relates to incomprehension and incomplete explanation(s) of events pertinent to a child’s disease and treatment(s). Comprehension of information often depends on each parents’ educational level, and their own health experience. In health care contexts, incomplete information can be a feature because health professionals are busy or use medical jargon that is foreign to parents (Whiting, 2014).
Lack of information is the third dimension of parental uncertainty and refers to a lack of available information relevant to their child’s disease and treatment. Lack of information related to diagnosis, procedures, treatments, and care does not assist decision making and can result in initial feelings of being out of control with their ill child.
Unpredictability is the fourth dimension of parental uncertainty and implies concerns and issues related to a child’s illness outcome and the parental role in the care of a child. Parents feel uncertain when they are not in control of their child’s care and future health status. Parents with children hospitalized for a prolonged period of time can feel increased unpredictability as the tasks of parenting are medicalized by the health care system. In addition, the sensation of being out of control can be exacerbated by a feeling of loss of “ownership” of their child if medical information pertinent to the child’s treatment and care is not provided and explained in ways that parents can understand (Salisbury et al., 2007; Trowbridge & Mische-Lawson, 2014; Wang & Barnard, 2008).
The Study
Aims
In this study, we hypothesized that parents of children undergoing herniorrhaphy show uncertainty and that the associated factors of parental uncertainty can be identified based on caregiver and child characteristics. The aims of the study were to (a) describe the characteristics of parent–child dyads, (b) examine the parents’ perceived level of uncertainty, and (c) identify the explanatory variables associated with parental uncertainty based on characteristics.
Method
The study used a descriptive, cross-sectional design to examine the perceived uncertainty of parents of children undergoing herniorrhaphy by using the Parents’ Perception of Uncertainty Scale (PPUS) modified from Mishel Uncertainty in Illness Scale (MUIS) as developed by Mishel (1981).
Participants
A purposive sampling of parents was used based on the following three inclusion criteria (a) They were ≥20 years old, (b) they had a child (aged <18 years) undergoing inguinal hernia repair according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) OP Codes 530~531, and (c) they had no medical diagnosis of psychological diseases.
In this study, we used the ICD-9-CM Operation Codes 530~531 to identify children diagnosed with inguinal hernia undergoing herniorrhaphy. The ICD-9-CM OP Code 530 was defined as unilateral repair of inguinal hernia and 531 as bilateral repair of inguinal hernia.
Data Collection
Data were collected from the researchers in the outpatient department (OPD) of a pediatric surgical center and the newborn and pediatric surgical ward of a children’s teaching hospital in Taipei, Taiwan, between 2012 and 2013. After obtaining informed consent, the participants were asked to complete the questionnaires, which collected the demographic information (the parents and their children) and their psychometric scale of uncertainty using the PPUS. Each completed questionnaire and scale was returned to the investigators prior to the end of surgery.
Measures
Specific demographic information of the participants included age, gender, education level, employment, marital status, religion, monthly family income, and family history of hernia. Specific characteristics of the children undergoing herniorrhaphy included age, gender gestational age, premature versus matured at birth, hernia sites (unilateral vs. bilateral), recurrent episode, birth order, presence of other diseases, and operation arrangement (outpatient vs. inpatient).
The PPUS had been previously translated from English into Chinese (Mu et al., 2002; Mu et al., 2001). In this study, the demographic questions and psychometric scale of PPUS regarding the semantic equivalence and content validity index (CVI) were assessed by five pediatric experts (nurses and doctors) and tested on 15 pilot participants.
PPUS
The PPUS measures the perceived level of uncertainty of parents when confronting their child’s illness (Mishel, 1981). The Chinese version of PPUS was translated by Mu (2005) who investigated the perceived level of uncertainty of mothers of children with cancer. The original Chinese version of the PPUS for mothers of children with cancer had a Cronbach’s alpha coefficient of .79 to .91 (Mu et al., 2001) with a reported reliability of .89 (Mishel, 1999). In this study, we had a report of reliability of .92 and CVI of 0.88. The PPUS has 31 items and uses a 5-point Likert-type scale (strongly agree = 5, agree = 4, undecided = 3, disagree = 2, and strongly disagree = 1), with higher scores denoting the higher level of perceived uncertainty. The original PPUS comprises the four dimensions of ambiguity, lack of clarity, lack of information, and unpredictability—with 31 items in total and an alpha coefficient of .86 to .93 (Mishel, 1983). We had 33 items in this study with additional items added pertaining to information about hernia repair and care, contained in the dimension of lack of information. The coefficient alpha for the total PPUS in this study was .79.
Ambiguity
This subscale has 13 items measuring the level of perceived uncertainty of parents with respect to their child’s surgery and care information that is ambiguous and inconclusive. An example of a question in this subscale is “I am unsure if my child’s illness (hernia) is getting better or worse.” The subscale obtained a Cronbach’s alpha coefficient of .87 in the study.
Lack of Clarity
This subscale has nine items measuring the degree of perceived uncertainty of primary caregivers in comprehending the problem and treatment in relation to their child’s hernia and surgery. An example of a question in this subscale is “I understand the explanation of my child’s hernia repair and anesthetics given by health professionals.” The reported Cronbach’s alpha coefficient of this subscale was .66.
Lack of Information
This subscale contained seven items evaluating the level of perceived uncertainty of the parents regarding the availability of information about the child’s hernia and care including surgery. “I don’t know what is wrong with my child” was an example of the questions in this subscale. There were three additional general questions specific to disease and treatment information of hernia and herniorrhaphy. Statements used were “The reason for my child suffering a hernia is because he/she cries too hard,” “Hernias in children will get better as they grow up so that it does not need to be operated on now,” and “My child is too young to have his/her hernia repaired.” The reported Cronbach’s alpha coefficient of this subscale was .62.
Unpredictability
This subscale has four items measuring the level of perceived uncertainty of the parents in dealing with the outcomes of the child’s hernia and general condition. An example of the question in this subscale is “I can predict how long my child’s illness will last.” The subscale obtained a Cronbach’s alpha coefficient of .57 in the study.
Ethical Considerations
The research team obtained the ethical approval for the study from the participating institution (a children’s teaching hospital in Taiwan) and written consent from the participants (IRB no.12MMHIS080).
Data Analysis
As there was no similar study investigating the uncertainty of parents of children receiving herniorrhaphy, we assumed a medium effect size (R2). Given the medium effect size of .15, α (Type I error) of .05, power (1 − Type II error) of 0.80, and a possible maximum number of predictor number of 10 in the final regression model, a sample size of 118 was required.
We used descriptive statistics such as number and frequency to present the characteristic of parents (demographic information) and children (demographic and clinical information; Aim 1). Other descriptive statistics including mean and standard deviation were carried out for describing the perceived levels of uncertainty of the parents; the correlation between uncertainty and characteristics was tested using independent sample t test, one-way analysis of variance, Scheffé’s test posterior comparison (α = .05), and Pearson’s product–moment correlation (Aim 2). We performed a multivariable linear regression to determine the explanatory variables of uncertainty based on the parent’s and the child’s characteristics (Aim 3). Prior to the multivariable linear regression analysis, the problem of multicollinearity among associated factors of uncertainty was counteracted by measuring variance inflation factor (>10 indicating multicollinearity), which ranged from 1.11 to 2.74 in this study. We used SPSS 18.0 (IBM SPSS Inc., Chicago, IL) for all of the data analyses.
Results
Aim 1: Characteristics of the Parents and the Children
The participants included 123 parents; 13 males (10.6%) and 110 females (89.4%, 108 mothers and two grandmothers; Table 1). All but three parents were married, 45% had a university degree, 77% specified a religion, and 67% worked. A majority of parents had more than one child (54%), 65% had no history of hernia occurring in the family, and 56% had a monthly family income of ≥2,000 USD (equivalent to 60,000 NTD).
Characteristics of the Parents and Children Undergoing Herniorrhaphy (N = 123).
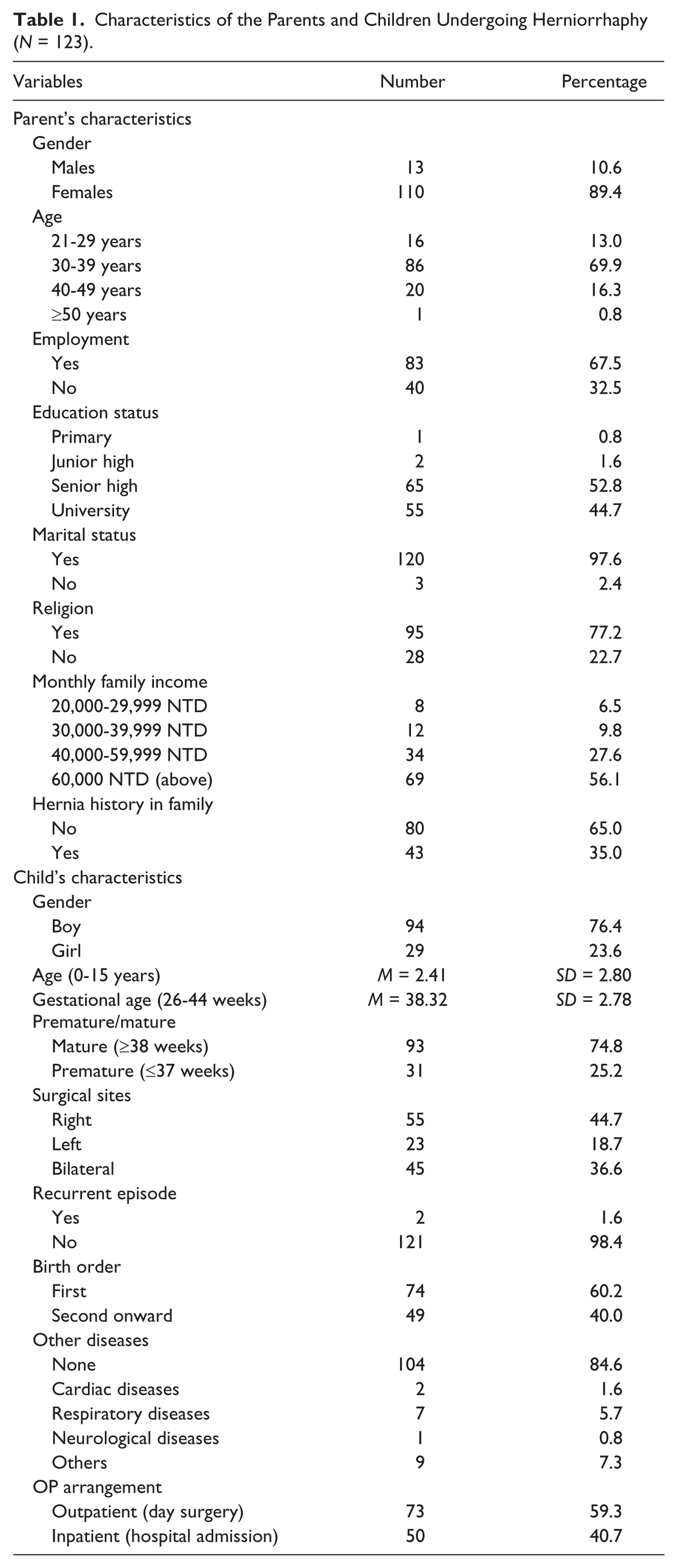
More boys (76%) than girls (24%) underwent herniorrhaphy with an average age of 2.26 years. Sixty percent of the children were the first child, and 25% of the children were born premature. More children presented with unilateral hernia (63.4%, right = 44.7%, left = 18.7%) than bilateral hernias (36.6%), and most children had a primary hernia (98%). Most children had no other diseases; there were a few children who had cardiac diseases (two), respiratory diseases (seven), neurological diseases (one), or other condition (nine). Nearly 60% of the children undergoing herniorrhaphy had the procedure as day surgery in an OPD. The children in our study, all had an open hernia repair.
Aim 2: Perceived Level of Uncertainty and Its Association With Characteristics
The perceived level of uncertainty of the parents was moderate (M = 2.65, SD = 0.42). The dimension of ambiguity had the highest scores (M = 2.97, SD = 0.61), whereas the dimension of unpredictability followed with the mean of 2.57 (SD = 0.68). In sequence, the dimension of lack of clarity had a mean of 2.53 (SD = 0.51) and the dimension of lack of information had the lowest mean score of 2.30 (SD = 0.51). Among the four dimensions of uncertainty, the first three highest levels of uncertainty items were related to the aspect of ambiguity, which were in sequence of (a) “It is unclear how bad my child’s pain will be” (M = 3.67, SD = 1.02), (b) “My child’s symptoms continue to change unpredictably” (M = 3.62, SD = 1.00), and (c) “I am unsure if my child’s illness (hernia) is getting better or worse” (M = 3.53, SD = 1.04).
Among the four dimensions of uncertainty, except for the dimension of lack of information, statistically significant variables were found in the parents’ characteristics (Table 2) and the child’s characteristics (Table 3). Caregiver’s religion (t = 2.29, p < .05) and child’s birth order (t = 2.35, p < .05) were the two variables that correlated with total parental uncertainty. In the dimension of ambiguity, the two statistically significant variables were monthly income (t = −2.10, p < .05) and child’s birth order (t = 2.35, p < .05). Another variable that was significant in the dimension of ambiguity but not shown in the table was the child’s age (r = −.22, p < .05), whereas the variable of gestational week was not significant in any dimension of uncertainty. In the dimension of lack of clarity, the two significant variables were religion (t = 2.34, p < .05) and child’s birth order (t = 2.19, p < .05). In the dimension of unpredictability, monthly income (t = −2.04, p < .05) and operation arrangement (t = −2.88, p < .01) were the only two significant variables.
Correlation Between Parent’s Uncertainty and Characteristics (N = 123).
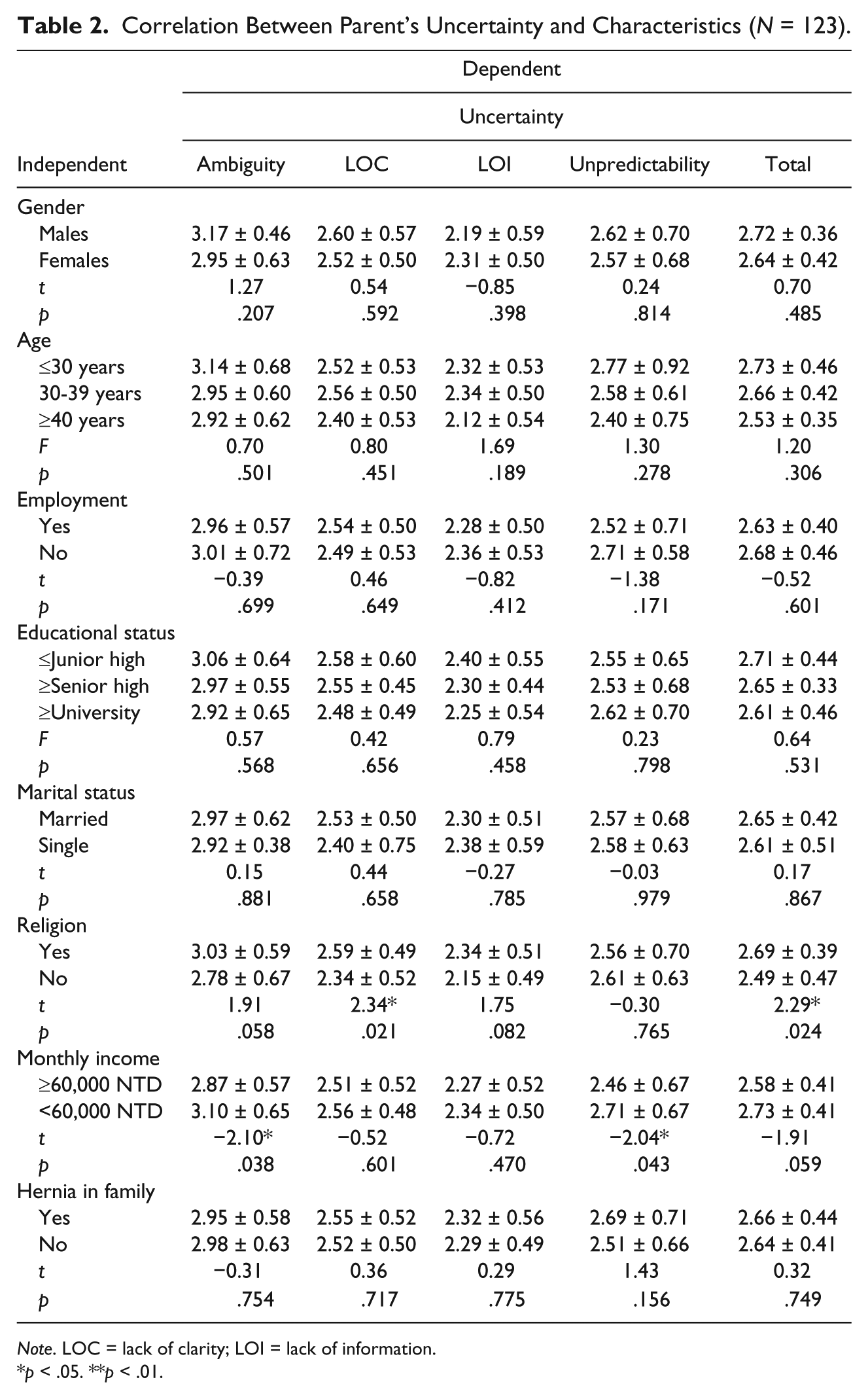
Note. LOC = lack of clarity; LOI = lack of information.
p < .05. **p < .01.
Correlation Between Parent’s Uncertainty and Child’s Characteristics (N = 123).
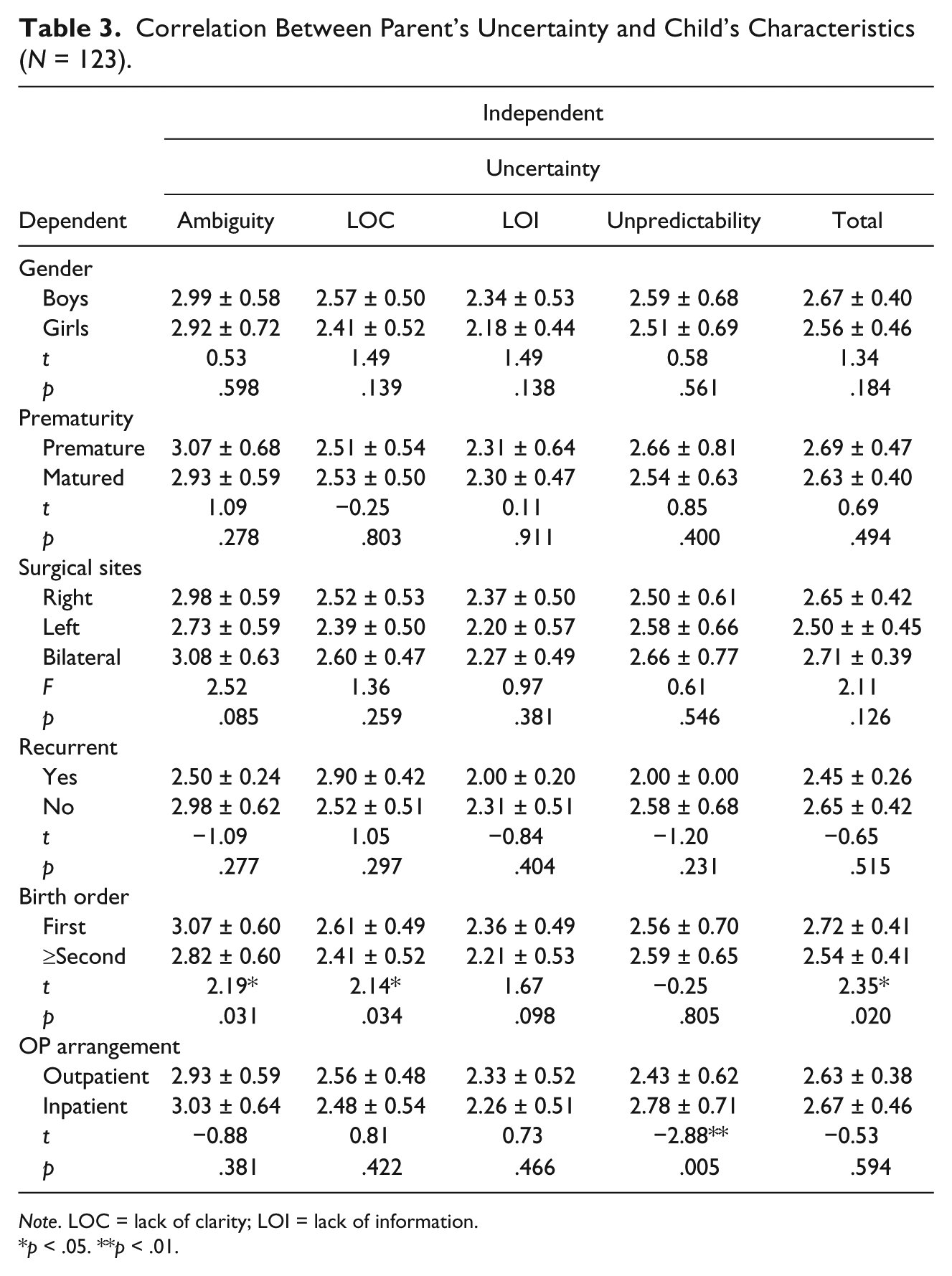
Note. LOC = lack of clarity; LOI = lack of information.
p < .05. **p < .01.
Aim 3: Explanatory Variables Associated With Parents’ Uncertainty
The significant explanatory variables of parental uncertainty included religion (β = .20, p < .05), the child’s hernia sites (left, β = −.29, p < .01), and the child’s birth order (β = .28, p < .01), which accounted for 20.6% of the total variance of parental uncertainty (R2 = .206; Table 4). Those parents who had a religious affiliation and cared for a child presenting with bilateral hernias who was also their first child perceived higher levels of uncertainty prior to the child’s herniorrhaphy.
Multivariable Linear Regression for the Explanatory Variables of Uncertainty Based on Characteristics.
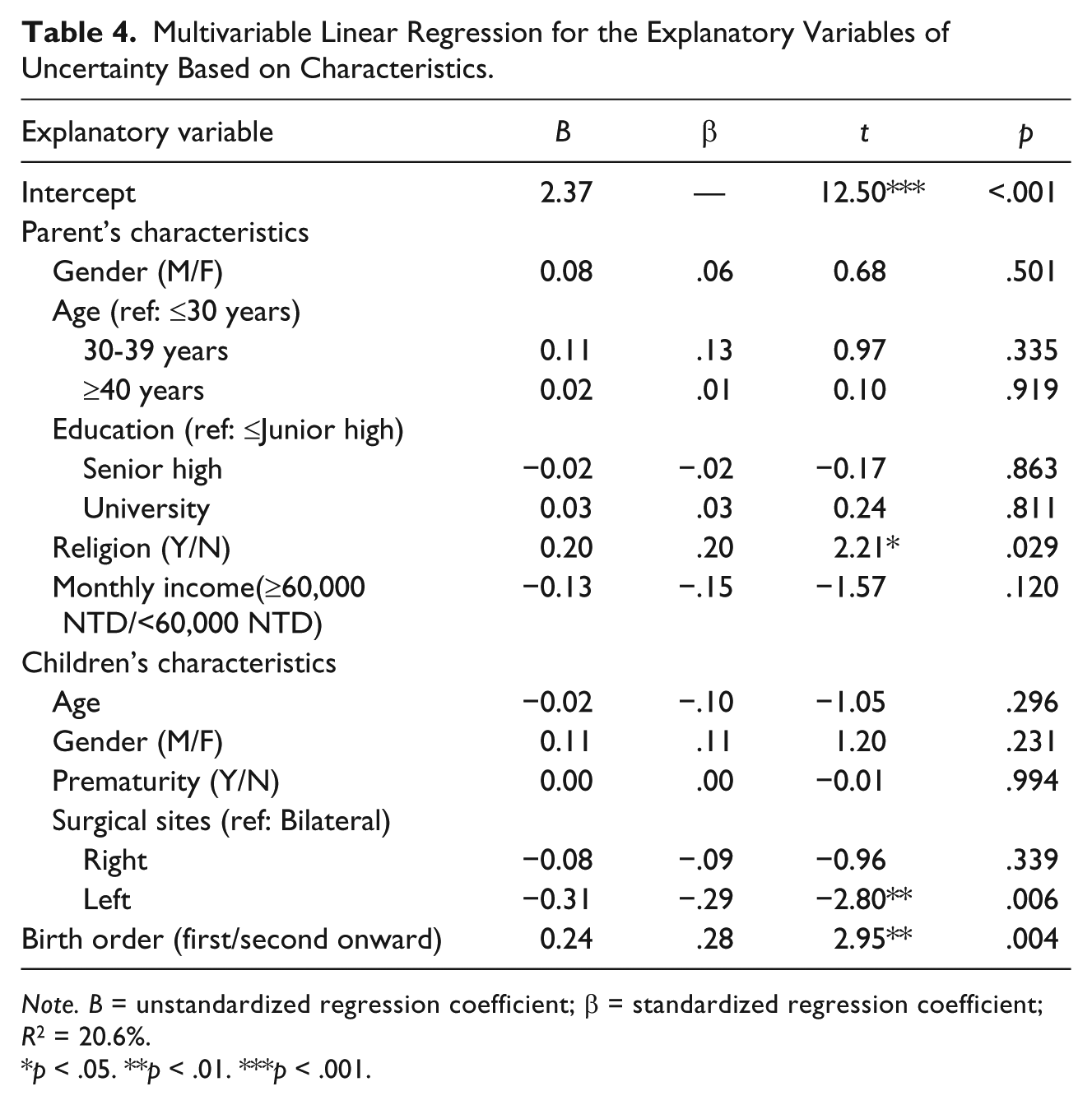
Note. B = unstandardized regression coefficient; β = standardized regression coefficient; R2 = 20.6%.
p < .05. **p < .01. ***p < .001.
Discussion
Characteristic Differences in Children Undergoing Herniorrhaphy
This study has described the characteristics of 123 children undergoing herniorrhaphy. Current evidence reporting gender characteristics of patients with inguinal hernias focuses more on adult populations, and men are reported to be twice more likely to undergo hernia repair than women, whereas the right hernia site is the most frequent type of inguinal hernia that accounts for 30% of all hernia repairs (Kingsnorth & LeBlanc, 2003; Schumpelick & Wantz, 1995). In this study, more boys than girls (3:1) underwent herniorrhaphy with 45% having right hernia repair and 36% with bilateral hernias, which is a higher proportion than the adult population with inguinal hernia.
Parental Uncertainty and Its Associated Factors in Childhood Illness and Surgery
In the context of childhood day surgery, ambiguity in parental uncertainty scored the highest for all parents in this study; parents felt ambiguous about information provided to them regarding care and pain management of their child and the health care system. Information support from health professionals was found to be significant in decreasing parental stress when caring for children with illness and aligns with earlier evidence (Wang et al., 2016). Parents’ with high levels of ambiguity in the study highlighted the importance of providing clear and relevant information in relation to management of their child’s postoperative care and discomfort. This result is consistent with evidence from an earlier study examining parents’ stress and coping during adolescents’ spinal surgery where concerns and uncertainty about the children’s pain and recovery outcomes were most obvious (Salisbury et al., 2007).
The results of the study are consistent also with other related studies examining the relationship between parental uncertainty and parental characteristics in the context of childhood illness. Parental lower monthly income was found to be associated with unpredictability of parental uncertainty and is similar to outcomes found in a study of caregivers’ stress in caring for oxygen-dependent children which identified financial burden as one of the predictors of parental stress (Wang et al., 2016). It affirms literature suggesting financial support can be helpful in maintaining family functions and the health status of parents caring for children with illness (Trowbridge & Mische-Lawson, 2014).
Furthermore, the highest level of perceived uncertainty identified in the group of parents were those with a religious affiliation which may be due to cultural beliefs and ritual practices in Taiwan. Ritual activities in various religions including Buddhism, Taoism, and temple-like Gods are common in Taiwan. Specific lunar dates in each religion require particular ritual practices and activities to bring luck, health, and peace. Studies have indicated that parents of children with illness in Taiwan tend to seek spiritual meaning and carry out religious activities as a way of coping with the uncertainty in their child’s illness (Lin et al., 2010; Yeh, 2001, 2003). These findings are important for parental well-being and need to be acknowledged and built into strategies to assist parents with religious affiliation.
Commonalities and differences have been found between the results of this study and other similar studies of parents caring for a child with illness examining the association between parental stress, uncertainty, and the child’s characteristics. The study found that bilateral hernia repair was associated with greater parental uncertainty and is similar to results from a study exploring the stress of parents caring for an oxygen-dependent child (Wang et al., 2016). Severity of signs and symptoms of the child’s illness is a major factor associated with the parental stress, is linked to a younger age of the child, and in a Taiwanese context is heightened more often associated with surgery on boys. This study has found that the younger the age of child undergoing herniorrhaphy, the greater the ambiguity of the parental uncertainty; however, it did not find any association between the child’s gender and parental uncertainty. In Chinese families, the value of a boy in the role of kinship for family progression is common. However, the inconsistent results of the effect of child’s gender may be because of the difference in the nature of illness course and symptom severity. In addition, this study identified birth order (the first child) also as a factor in determining perceived uncertainty of parents, which has not yet been reported in other studies of parental uncertainty in childhood surgery. Parents of a first child undergoing surgery may lack experience in providing postoperative care for their child, which indicates that these parents need support and health education from health professionals.
With advances in information technology, clinical practice is increasingly assisting better educated parents who are capable of searching for information in relation to their child’s disease and treatment. This study has found two dimensions of perceived uncertainty of the parents—lack of clarity and lack of information. The parents in this study tended to have an educated background (53% with senior high school degree and 45% with a university degree), which means that they would generally know how to search for information and understand the medical information provided to them; availability of medical information would likely not become an issue for them.
In contrast, although medical information is now readily available as patient education in material and electronic formats, the parents in this study perceived a higher level of uncertainty regarding the dimension of ambiguity. Quality of information in terms of consistency and clarity can be crucial when explained by health professionals who can involve the parents with care (Bruce, Lindh, & Sundin, 2016), provide critical information regarding the child’s condition and care (Segre, Orengo-Aguayo, & Siewert, 2016), and place an emphasis on the management of illness-related events and symptom-control episodes including pain reduction for parents of a child undergoing herniorrhaphy (Hatfield & Polomano, 2012).
Clinical Implications
The study shows evidence that Taiwanese parents of children undergoing herniorrhaphy perceive moderately high levels of uncertainty, particularly in the dimension of ambiguity. Results highlight that provision of clear information regarding care of symptoms after hernia repair and pain management is essential. Parental uncertainty prior to a child’s herniorrhaphy may be reduced through interventions that targeted support of parents who have a religious affiliation and have a first-born child requiring bilateral herniorrhaphy.
This study has three significant implications. First, health information in relation to illness-related events and symptoms management is important for parents of children undergoing surgery such as herniorrhaphy. Second, health professionals should encourage parents with a religious affiliation to seek ritual activities at their own pace and level of comfort to assist their feelings of uncertainty. Third, specific support should be actively offered to those parents whose first child is undergoing herniorrhaphy and presenting with bilateral hernias.
Limitations
The study has limitations in terms of its cross-sectional research design and because it only examined parental uncertainty in their encounters with their child’s herniorrhaphy, and the low levels of coefficient alpha reported in the subscales of PPUS that may be the result of a lack of psychometric testing on the changes in the scale. Future longitudinal investigations on the changes in biophysical and psychosocial measurements of parents of children undergoing surgery and the differences between mothers and fathers are warranted so that appropriate outcomes can be studied when effective interventions are implemented. The study also had a modest sample size of 123 participants and was conducted in a single recruitment institution, which may limit the generalizability of the results. Future research may attempt to re-examine the subscales of PPUS with a larger sample size of parents in the broader context of childhood surgery and explore the perceptual differences of parents caring for children with different illness courses and care management.
Conclusion
When children are undergoing day surgery such as herniorrhaphy, Chinese parents can experience a moderate level of uncertainty, including feelings of ambiguity with regard to their child’s pain and discomfort, and feelings of unpredictability with respect to health care outcomes and care. Clear information regarding symptom assessment and management, including possible recurrent episodes and postoperative pain, is important for parents. Clinicians may find it helpful to focus on those parents who are at risk of feeling uncertain, especially those who have a religious affiliation and a first-born child with bilateral hernias.
Footnotes
Acknowledgements
The authors thank the caregiver participants involved in the study and the institute of review board (IRB) of Mackay Memorial Hospital and the kind support from Mackay Medical College.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.