
Abstract
Incidence of medication errors in intensive care unit (ICU) can cause irreparable damage for ICU patients. Therefore, it seems necessary to find the causes of medication errors in this section. Work commitment and dynamic might affect the incidence of medication errors in ICU. To assess the mentioned hypothesis, we performed a descriptive-analytical study which was carried out on 117 nurses working in ICU of educational hospitals in Tehran. Minick et al., Salyer et al., and Wakefield et al. scales were used for data gathering on work commitment, dynamic, and medication errors, respectively. Findings of the current study revealed that high work commitment in ICU nurses caused low number of medication errors, including intravenous and nonintravenous. We controlled the effects of confounding variables in detection of this relationship. In contrast, no significant association was found between work dynamic and different types of medication errors. Although the study did not observe any relationship between the dynamics and rate of medication errors, the training of nurses or nursing students to create a dynamic environment in hospitals can increase their interest in the profession and increase job satisfaction in them. Also they must have enough ability in work dynamic so that they don’t confused and distracted result in frequent changes of orders, care plans, and procedures.
Introduction
Patient safety is defined as approaches that prevent from adverse events, including medical errors in hospital (Teng et al., 2009). Medical errors are one of the most important challenges for patient safety worldwide (Baghaei, Khalkhali, & Naderi, 2013). Annual deaths resulting from medication errors account for 7,000 out of the total number of 48,000 to 98,000 deaths due to drug-induced complications. In Iran, it has been estimated that 55,000 medical errors occur each year, resulting 10,500 deaths and 23,000 physical disabilities (Pazokian, Zagheri Tafreshi, & Rassouli, 2014). Several factors including age, severity of damage, blood pressure, body temperature, Glasgow Coma Scale, and some laboratory parameters are involved in prognosis of patients in intensive care unit (ICU; Haghparast-Bidgoli, Hasselberg, Khankeh, Khorasani-Zavareh, & Johansson, 2010; He, Sun, Sun, & Zhan, 2016; Sung et al., 2005). Better prognosis of patients in ICU is associated with better outcome and lower risk of mortality. One of the important factors that should be considered in patients in ICU is medical care quality (Kalina, Tinkoff, Gleason, Veneri, & Fulda, 2009). Better quality of care can decrease the risk of medical errors and improve the patient safety.
Recently, patient safety has become a global concern. Nonsafety services have provided a large burden for patients and health system (Teng et al., 2009). In patient safety, some factors including medication errors, surgical procedures, incorrect diagnosis of disease, equipment failure, hospital infection, and patient fall should be considered (Bourland, Nyenhuis, & Schaefer, 2000; Madady, 2015). Among these factors, medication errors are a global problem leading serious injuries and even patients’ death (Cook & Sandars, 2009; Teng et al., 2009). Despite the much progress in prevention of medication errors in recent years, studies showed that these errors still happen and cause irreparable damage for patients in ICU (Vioque et al., 2014). Critically ill patients in ICU have higher risk for medication errors because of the complexity of their disease that creates challenges in drug dosing, their vulnerability to rapid changes in pharmacotherapy, the intensive care environment providing ample distractions and opportunity for error, the administration of complex drug regimens, and the numerous high-alert medications that they receive (Kane-Gill, Jacobi, & Rothschild, 2010). On average, 1.7 medication errors occur per patient per day in ICU and nurses have an important role in incidence of these errors (Chambers, Mahon, & Walshe, 2009).
Researchers have mainly focused on system approach or organization factors to find the reasons of medication errors. Among organization factors, organizational commitment and work dynamic may affect the errors, especially medication errors. Organizational or work commitment is defined as having interest or willingness to spend time and energy for work (Eisenhardt & Martin, 2000). Moreover, work dynamic is defined as methods which enable individuals to respond to inevitable changes appropriately (Pazokian, Zagheri Tafreshi, Rassouli, & Zayeri, 2013). High workload and inadequate staffs provide an inappropriate work environment and affect the work dynamic (Johnstone & Kanitsaki, 2006). Weissman et al. (2007) reported that a 0.1% increase in the patient-to-nurse ratio led to a 28% increase in the adverse events or medication errors rate. Few studies were done on the association between nurses’ work commitment, dynamic, and incidence of medication errors. (Bratt & Felzer, 2012; Chang & Mark, 2010; Gellatly, Cowden, & Cummings, 2014; Kauffeld, Lehmann, Willenbrock, & Lei, 2012; McDonnell, 2005; Teng et al., 2009). Some of these studies showed a significant relationship between work commitment, dynamic, and incidence of medication errors (Heydari, Kamran, & Novinmehr, 2015; Teng et al., 2009), but others failed to reach any significant association (Bratt & Felzer, 2012; Pazokian et al., 2013). Hence, data in this regard are inconsistent. In addition, most previous studies in this regard are limited to Western nations, and evidences on the relationship between nurses’ work commitment, dynamic, and incidence of medication errors are scarce in Asian countries, especially Iran. The nurses in these countries have different culture and beliefs which can affect the work commitment and dynamic of them. Moreover, we are aware of no studies that examined the relationship between work commitment, dynamic, and incidence of medication errors in ICU nurses in Iran.
Aim
The aim of this study is to determine the relationship between work commitment, dynamic, and medication errors.
Method
This was a cross-sectional, descriptive-analytical study in which relationship between work commitment, dynamic, and medication error from the participants. The study was carried out between January 2015 and March 2016.
Setting
This study was conducted in major educational hospitals in Tehran. Nurses worked in ICUs of these hospitals were considered as study population. These ICUs were general, and different types of patients were admitted in them.
Sampling Process
On the basis of the sample size formula suggested for correlational studies, considering a Type I error rate of 5% (α = .05) and Type II error rate of 10% (β = .10, power = 90%), we determined a sample size of 113 persons for this study (Munro, 2005). Minimum correlation coefficient of .3 for the association between work commitment, dynamic, and medication errors. According to limitation of study population and considering the noncooperation of nurses, we used census method for sampling and selected 120 nurses for this study based on inclusion criteria. Totally, three surveys were excluded due to missing data and outliers. The final sample included 117 nurses.
Inclusion Criteria
These criteria included having at least BSc degree of nursing, at least 2-year experience of working as a nurse, and at least 1-year experience of full-time work in ICU.
Measurement
We first collected demographic information on age, gender, marital status, education (BSc/MSc), work experience as a nurse in hospital (year), work experience as a nurse in ICU (year), employment status (formal/covenant/contract/service commitment), and worked rotating shifts (morning/afternoon/evening/night) by a self-administrated questionnaire. Moreover, we examined the nurses’ commitment, dynamic, and incidence of medication errors by three self-reported questionnaires. To assess the work commitment, we applied scale designed by Minick, Dilorio, Mitchell, & Dudley (2000). Minick scale assessed the extent to which nurses felt responsible for care on their unit, for example, when an order was not quite clear, whether they would continue to search clarification from the physician, and whether nurses would counsel a staff member who presented nonstandard care (Minick & Harvey, 2003). This tool contained eight items with six-option Likert-type scale. In this tool, the lowest score and the highest score were 8 and 48, respectively, and high score was associated with high work commitment. In addition, we used seven-item Likert-type scale of Salyer (1996) to evaluate the work dynamic of nurses. This scale assessed the work complexity of nurses in hospital and their reactions when physicians’ orders were changed frequently or the unit had a high number of transfers and admissions. Participants should choose one option of the six options (totally disagree [score = 1] to totally agree [score = 6]) for each item. Therefore, total score of this scale varied from 7 to 42, and high score of this scale was related to high work dynamic.
Fourteen-item scale of Wakefield et al. was used to assess medication errors of nurses in ICU (Wakefield, Uden-Holman, & Wakefield, 2005). This scale included seven items for intravenous medication errors (wrong patient, wrong dose, wrong time, wrong-route administration, medication is omitted, unordered drug, other preparation error) and seven items for nonintravenous medication errors (wrong patient, wrong dose, wrong time, wrong-route administration, medication is omitted, unordered drug, other preparation error). Wakefield scale was scoring based on percentage of medication errors from 0% to 25% (score = 1) to 75% to 100% (score = 4). High score of medication errors was associated with high incidence of medication errors. The mentioned three questionnaires were reliable and validated as self-assessed instruments.
Validity and Reliability
The psychometric characteristics, validity, and reliability of used scales in this study have been determined in the Pazokian et al. (2013) study. To assess psychometrics of mentioned scales, permission was obtained from the tool designers through correspondence, and then translation and psychometric processes began using Wild et al.’s (2005) method in eight stages, including (a) translation of questionnaire from original to target language, (b) combination and merger of initial translations into a single translation, (c) translation of final translated version back into original language, (d) review of translated version from target to original language, (e) preliminary studies, (f) modification and summing up, (g) determining validity and reliability of translated tool, and (h) final report. These processes provided cultural adjustment of tools. To examine validity in mentioned study, the construct validity was used for scales of work commitment, dynamic, and medication errors. Also intraclass correlation coefficients of .82, .82, and .79 were reported for scales of work commitment, dynamic, and medication errors, respectively. In addition, reliability using Cronbach’s alpha coefficient for internal consistency was reported .9, .78, and .84 for scales of work commitment, dynamic, and medication errors, respectively. Hence, these scales were considered to be valid and reliable.
Ethical Considerations
The study was approved by ethical committee in Tehran in 2015. Potential participants were given a document outlining that participation was voluntary and that collected data would be used solely for scientific purposes. We dedicate a special code for each person (not name and family name) to prevent the disclosure of information. Verbal consent was obtained.
Data Analysis
All analyses were conducted using SPSS statistical software (Version 21.0; SPSS, Inc., Chicago, IL, USA). First, by summing up the score of each item in each scale, we determined the total score of scales. The normality of variables including total score of scales was approved by Kolmogorov–Smirnov test, and therefore, we used parametric test for statistical analyses. To assess the work commitment, dynamic, and medication error scores based on gender, marital status, and education level, we applied an independent-sample t test. In addition, ANOVA was used to evaluate the work commitment, dynamic, and medication error scores according to employment status and working shifts. To examine the association between age, work experience (as a nurse in hospital and ICU), work commitment, dynamic, and incidence of medication errors, we used Pearson’s correlation. For adjustment of confounding variables, linear regression analysis was used in different models to examine the independent relationship between nurses’ work commitment and dynamic with incidence of medication errors. In the first model, we adjusted for age and gender. Further adjustment for marital status and education was done in the second model. The final model was additionally adjusted for work experience (as a nurse in hospital and ICU), employment status, and working shift. The p value less than .05 was considered as significant level.
Interpretation of Results
In this study, out of 120 nurses working in ICU, we had incomplete data on three nurses, which were not considered for statistical analysis. The mean scores of work commitment, dynamic, and total medication errors in nurses of this study were 42.25 ± 4.95, 30.88 ± 5.46, and 22.33 ± 5.78, respectively. Moreover, the mean scores of intravenous and nonintravenous medication error of nurses were 11.18 ± 3.23 and 11.14 ± 2.89, respectively. Based on Wakefield scale, total score of medication errors varied from 14 to 56, and this number for intravenous and nonintravenous medication errors was from 7 to 28.
The relationship between demographic variables, work commitment, dynamic, and incidence of medication errors is indicated in Tables 1 and 2. Demographic variables including age, gender, marital status, education, work experience, employment status, and working shift were not significantly associated with work commitment, dynamic, and incidence of medication errors (p > .05). In contrast, Pearson’s correlation revealed a significant inverse association between work commitment and incidence of medication errors, including intravenous (r = −.21, p = .02), nonintravenous (r = .27, p = .003), and total medication error (r = −.25, p = .006), but no significant relationship was observed between work dynamic and medication errors (r = −.04, p = .65). In addition, work commitment was not significantly associated with work dynamic (r = .14, p = .12).
The Association Between Demographic Data, Work Commitment, Dynamic, and Incidence of Medication Errors.
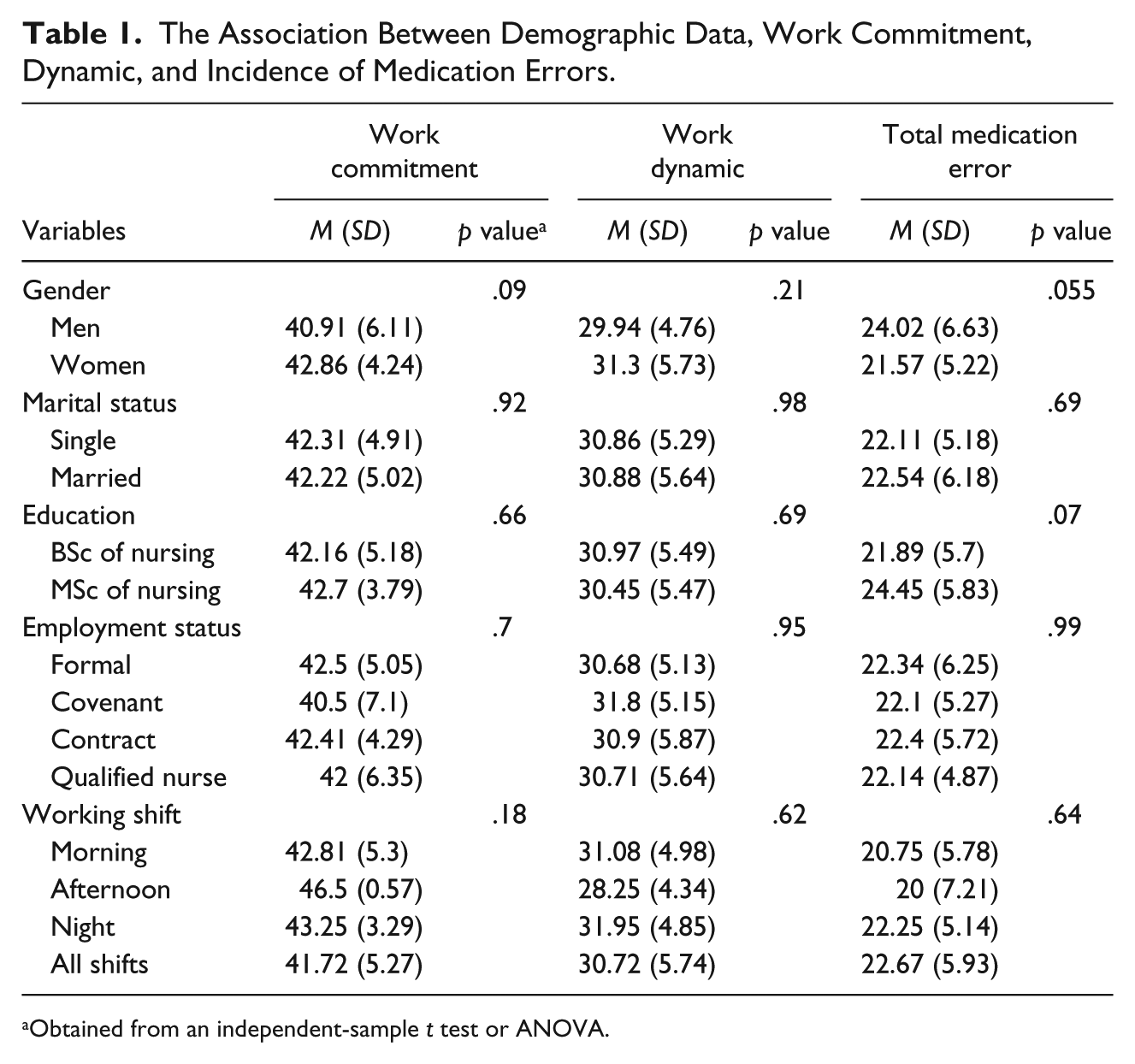
Obtained from an independent-sample t test or ANOVA.
Correlation Between Age, Work Experience, Work Commitment, Dynamic, and Incidence of Medication Errors (N = 117).
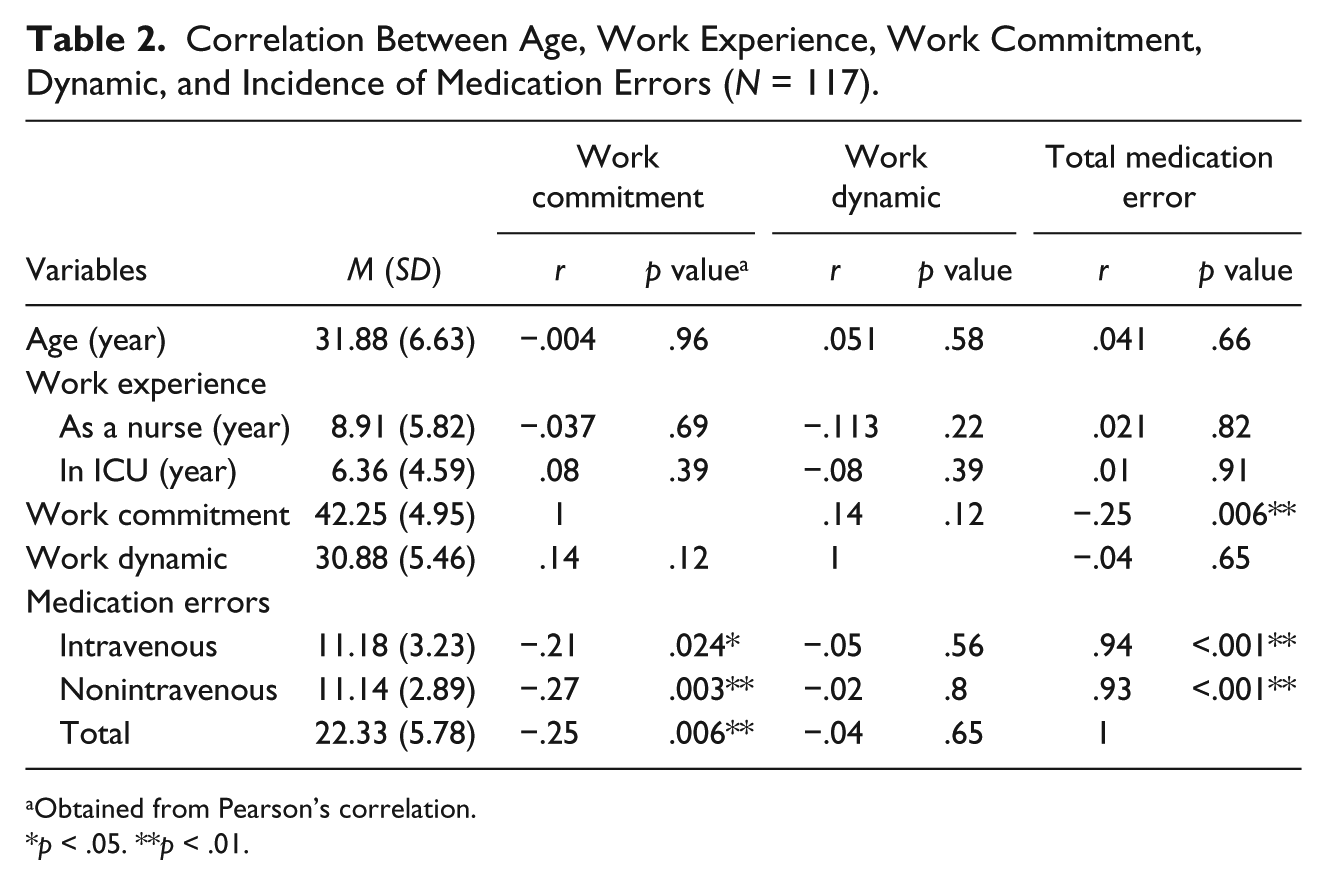
Obtained from Pearson’s correlation.
p < .05. **p < .01.
The relationship between work commitment, dynamic, and medication errors by considering the confounding variables is presented in Table 3. Linear regression revealed that work commitment is inversely associated with incidence of nonintravenous (β = −.16, 95% confidence interval [CI] = [−0.26, −0.05]) and total medication errors (β = −.29, 95% CI = [−0.5, −0.08]). This association remained significant even after adjustment of confounding variables including age, gender, marital status, education, work experience, employment status, and working shift, so that one-unit increase in work commitment caused 0.15 and 0.27 units decrease in incidence of nonintravenous and total medication errors, respectively. In addition, there was a significant inverse relationship between work commitment and incidence of intravenous medication errors (β = −.13, 95% CI = [−0.25, −0.01]). After controlling for age, gender, marital status, and education, this relationship remained significant; so that one-unit increase in work commitment was associated with 0.12 units’ reduction in incidence of intravenous medication errors. No significant association was observed between work dynamic and incidence of medication errors, including intravenous, nonintravenous, and total medication errors. This association was nonsignificant even after adjusting the confounding variables.
Multiple Linear Regression for the Association Between Work Commitment, Dynamic, and Incidence of Medication Errors.
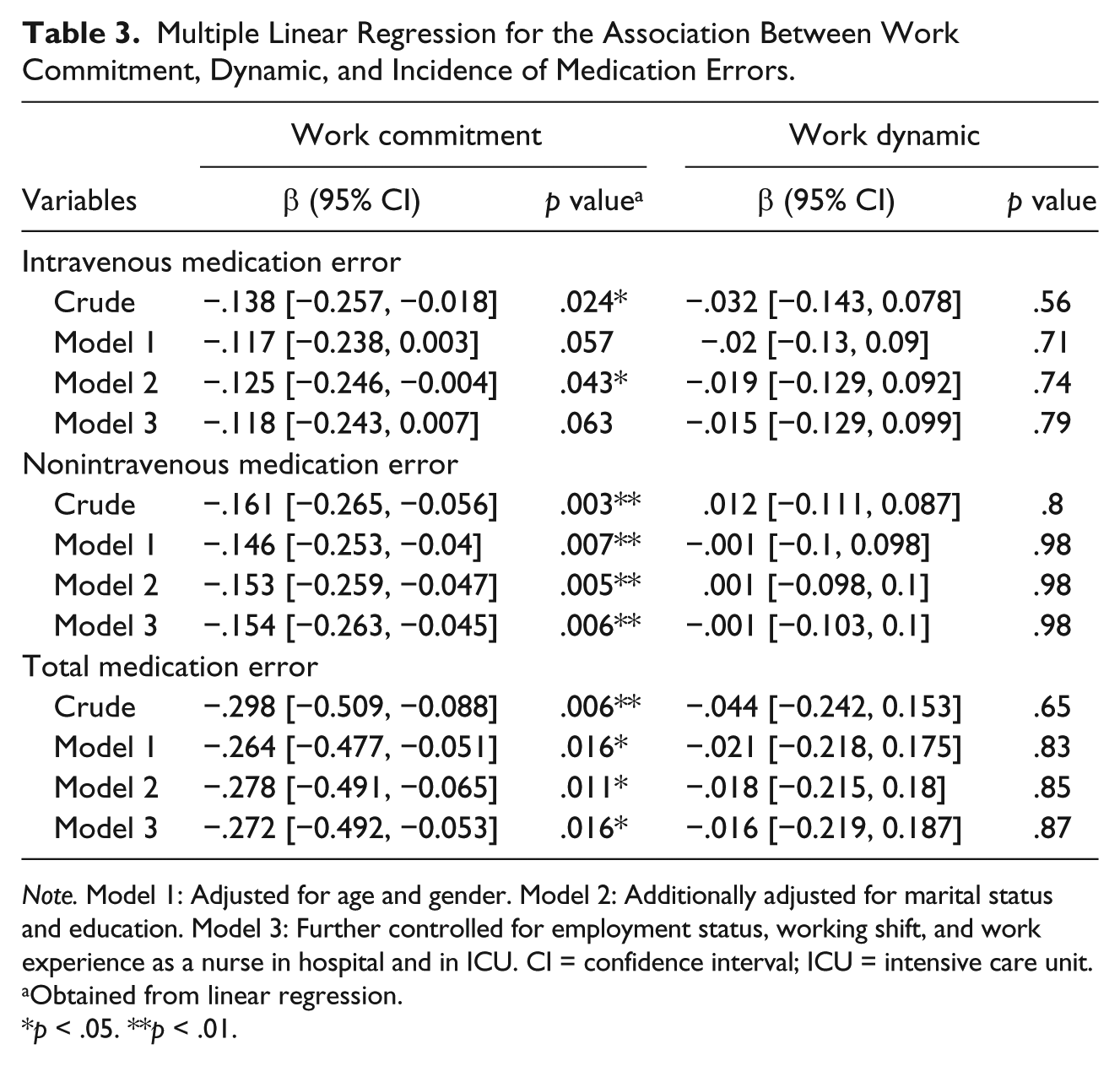
Note. Model 1: Adjusted for age and gender. Model 2: Additionally adjusted for marital status and education. Model 3: Further controlled for employment status, working shift, and work experience as a nurse in hospital and in ICU. CI = confidence interval; ICU = intensive care unit.
Obtained from linear regression.
p < .05. **p < .01.
Discussion
In this study, work commitment was inversely associated with incidence of different types of medication errors, including intravenous, nonintravenous, and total medication errors. Adjustment of confounding variables caused no change in this relationship. In contrast, no significant association was found between work dynamic and incidence of medication errors. This association was unchanged even after adjusting the confounding variables. In addition, demographic variables were not significantly associated with work commitment, dynamic, and medication errors (p < .05). To our knowledge, this study is the first to assess the association between work commitment, dynamic, and incidence of medication errors in ICU nurses.
Medication errors are the major problem affecting in patients and health system in all over the world (Dhillon, Sanghera, & Franklin, 2007). Among different parts of hospital, incidence of medication errors in ICU is more important than other parts (Abdoli, Musarezaie, Irajpoor, Ahmadi, & Momeni-GhaleGhasemi, 2013). Patients in ICU require continuous evaluation and monitoring (Abdoli et al., 2013). Because of complex condition of critically ill patients in ICU and greater mortality of them, medication errors can cause irreparable damages for these patients (Coomber et al., 2002). Therefore, more studies are needed to find methods to control medication errors.
Based on our findings, work commitment was inversely associated with incidence of medication errors. In line with our findings, other researchers reported that high work commitment in nurses is associated with increased patients’ safety and care quality as well as lower incidence of medication errors (Teng et al., 2009). Moreover, Heydari et al. (2015) reported that low work commitment increase the incidence of medication errors. In another study, care quality in nurses with high work commitment was higher than those with low work commitment. Based on mentioned study, nurses with high work commitment had well communication with patients and less desire to withdraw from work. In addition, work commitment of nurses can be improved by increasing their salary (Gellatly et al., 2014). In contrast, Pazokian et al. (2013) indicated no significant association between nurses’ work commitment and incidence of medication errors. Furthermore, it had been shown that work commitment has no effect on nurses’ function, care quality, and also incidence of medication errors (Bratt & Felzer, 2012).
According to our findings, work dynamics was not significantly associated with incidence of medication errors. The results of some previous studies are similar to our findings. Pazokian et al. (2013) reported no significant association between work dynamic and incidence of medication errors. In another study, high work dynamic in hospital caused no effect on nursing errors, especially medication errors. In the mentioned study, it had been shown that learning climate cannot affect the relationship between work dynamic and medication errors (Chang & Mark, 2010). In opposite to our findings, McDonnell (2005) reported that a dynamic system has an important role in management of medication errors. Based on the mentioned study, providing a dynamic workplace in hospital can decrease the medication errors of nurses.
In the current study, we were expected to find an inverse association between work dynamics and incidence of medication errors. Based on previous studies, high workload, inadequate staffs, and inevitable changes in hospital provide an inappropriate work environment and affect adversely on the work dynamic (Johnstone & Kanitsaki, 2006). Mentioned situations can also affect the incidence of medication errors (Weissman et al., 2007). Theoretically, it seems that work dynamics should be inversely associated with incidence of medication errors, but conflicting findings are available in this regard based on earlier studies. These conflicting findings might be due to difference in culture, beliefs, and age range of participants in different studies as well as difference in questionnaires assessing the work dynamic and medication errors and also underreporting of medication errors by nurses or social desirability bias in the self-reported measures. Fear of punishment is a potential reason for underreporting of medication errors. Therefore, further studies are required to shed light on the association between work dynamics and incidence of medication errors.
Limitations
First, self-reporting is believed by many researchers to contribute to the limitations of studies, but with regard to medication errors, it still remains one of the most common and practical means of detecting and estimating error incidence (Joolaee, Hajibabaee, Peyrovi, Haghani, & Bahrani, 2011). The nurses still expressed doubts regarding the confidentiality of the results, which made the work more complicated. The researchers’ good communication with the participants in addition to knowing the research environment helped ensure trust with the nurses. Second, although we controlled some potential confounders, further adjustment made for other confounding variables such as workplace culture and care complexity will be effective in reaching an independent association between work commitment, dynamic, and incidence of medication errors. Third, however, the normality of variables including total score of work commitment, dynamic, and medication errors was approved, but the use of discrete measurements to provide total score of scales as a parametric data might be another limitation for the current study.
Conclusion
Till date, no studies have examined the relationship between work commitment, dynamic, and incidence of medication errors in ICU nurses, while 1.7 medication errors occur per patient per day in ICU and nurses have an important role in incidence of these errors (Chambers et al., 2009). Therefore, finding the approaches that are involved in incidence of medication errors in ICU is important. Based on our findings, work commitment was inversely associated with incidence of different types of medication errors, but no significant association was observed between work dynamic and incidence of medication errors. Further studies in this regard can confirm findings of this study.
Implications for Nursing
Findings of this study revealed that high work commitment can decrease the incidence of medication errors in ICU. Therefore, hospital and nursing managers must apply appropriate strategies to increase the work commitment of nurses in ICU. Appropriate training courses for ICU nurses and nursing students can increase the work commitment. Other strategies are clear definition of responsibilities, effective orientation program, and communication. In addition, work commitment of nurses can be improved by increasing their salary (Gellatly et al., 2014). Although the study did not observe any relationship between the dynamics and rate of medication errors, the training of nurses or nursing students to create a dynamic environment in hospitals can increase their interest in the profession and increase job satisfaction in them. Also they must have enough ability in work dynamic so that they don’t confused and distracted result in frequent changes of orders, care plans, and procedures.
Footnotes
Acknowledgements
The authors thank all the nurses and colleagues at the Nursing and Midwifery School of Shahid Beheshti University of Medical Sciences in Iran.
Authors’ Note
This article was a part of the MS dissertation research project with the Research Council of Shahid Beheshti Medical University.
Author Contributions
M.P. involved in the study conception, design, analysis/interpretation of data, critical revisions for important intellectual content, drafting of the manuscript and review of content. M.Z.T. involved in the study conception, design, and analysis/interpretation of data. A.R. involved in the study conception, design, acquisition of data, analysis/interpretation of data, and review of content. M.N. provided statistical technical support and involved in the study design, provision of statistical technical support, and review of content.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.