
Abstract
The purpose of this article is to provide an analysis of the concept Deaf to increase health care provider (HCP) understanding from a cultural perspective. Deaf signers, people with hearing loss who communicate primarily in American Sign Language (ASL), generally define the term Deaf as a cultural heritage. In the health care setting, the term deaf is most often defined as a pathological condition requiring medical intervention. When HCPs are unaware that there are both cultural and pathological views of hearing loss, significant barriers may exist between the HCP and the Deaf individual. The concept of Deaf is analyzed using the Wilsonian method. Essential elements of the concept “Deaf” from a cultural perspective include a personal choice to communicate primarily in ASL and identify with the Deaf community. Resources for HCPs are needed to quickly identify Deaf signers and provide appropriate communication.
Keywords
The purpose of this article is to provide an analysis of the concept Deaf to increase health care provider (HCP) understanding of differences between a cultural and pathological view of hearing loss. Deaf signers, people with hearing loss who communicate primarily in American Sign Language (ASL), generally define the term Deaf as a cultural heritage. In the health care setting, the term deaf is generally defined as a pathological condition (hearing loss) requiring correction or rehabilitation. When HCPs are unaware that there are both cultural and pathological views of hearing loss, significant barriers may exist between the provider and the Deaf individual. HCPs’ lack of awareness of Deaf signers’ cultural and linguistic differences is often cited as a major factor contributing to communication barriers faced by Deaf signers.
The concept of Deaf is analyzed using the Wilsonian method. Essential elements of the concept Deaf from a cultural perspective are identified through this concept analysis including a personal choice to primarily communicate in ASL and identify with Deaf culture. The inability to hear spoken language well enough to communicate is an essential element, although with less significance. Typically, ASL is the first and primary language of Deaf signers. As with other linguistic minorities, professional interpreters are often needed for effective communication with English-speaking HCPs. Resources are needed for HCPs to quickly identify Deaf signers and their preferred communication preferences. After this first essential step, resources must be available to then provide the preferred communication.
The purpose of this article is to provide an analysis of the concept Deaf to increase HCP understanding of differences between a cultural and pathological view. The awareness of a cultural perspective of deafness will help to illuminate the unique communication needs of people whose primary language is ASL. People who are deaf and associate themselves with cultural deafness distinguish the difference in writing by using a lowercase “d” for the physiological state of absence of hearing. The uppercase “D” denotes deafness as a cultural identity with little ties to hearing ability. The author uses this connotation to differentiate between different perspectives of the term Deaf.
Significance
The Americans With Disabilities Act of 1990 (ADA) mandating HCPs provide effective communication for people who are deaf and hard of hearing (D/HH) has been in effect for a quarter of a century; however, studies that examine perspectives of people who are D/HH consistently show that they are not able to effectively communicate with their HCPs resulting in negative health outcomes, decreased patient satisfaction, and avoidance of use of health care until emergent (Hoang, LaHousse, Nakaji, & Sadler, 2011).
Method
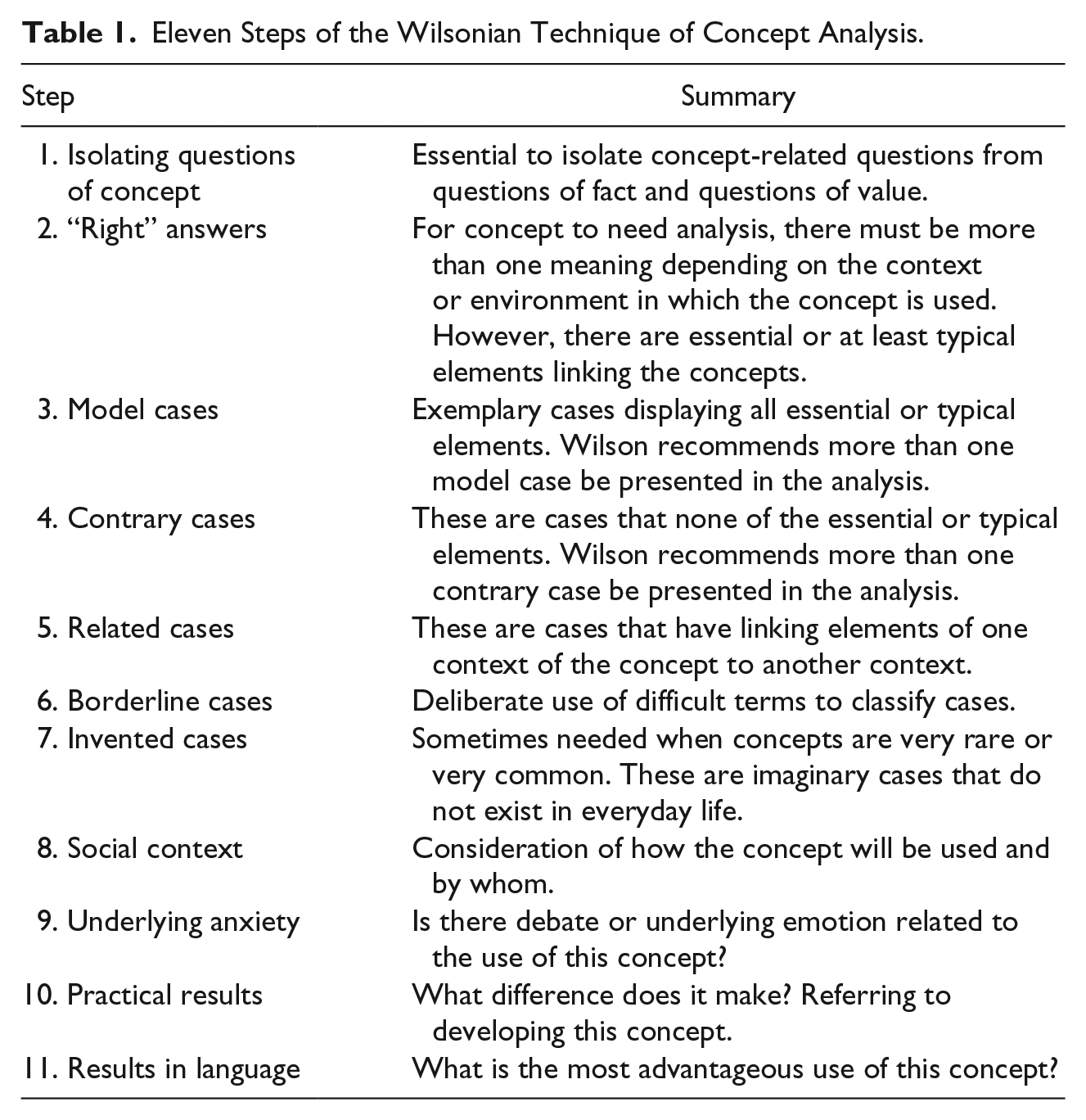
The Wilson (1963) method of conceptual analysis is used in this article to analyze the concept of Deaf. The Wilson method is useful in clarifying a concept when one word has more than one meaning in different contexts by using case development (see Table 1).
Eleven Steps of the Wilsonian Technique of Concept Analysis.
Isolating the Concept
The first step in case development is to isolate the concept from questions of fact and value. Examples of factual and value question are as follows: “What are the ADA mandates concerning communication between HCP and people who are deaf and hard of hearing?” and “Should people who are deaf be taught speech-reading or sign language or both?” Questions regarding facts or requiring ethical and moral judgment are not a part of concept analysis.
“Right” Answers
Essential elements must be identified when the right definition of a word is being considered in different contexts (Wilson, 1963). Essential elements of the word Deaf are analyzed.
Disability or pathology definition
The predominately hearing society views being physically unable to hear as an undesirable state or disability. Holcomb (2013) states, “In the hierarchy of disability, being deaf has been repeatedly identified in the literature as one of the most debilitating disabilities” (p. 243).
In the field of health care, the term deaf refers to a physical state of decreased or absence of hearing measurable in degrees of hearing ability or loss. Hearing loss is categorized by decibels lost ranging from slight hearing loss at 16 to 25 dB to profound hearing loss at greater than 90 dB. In addition, hearing loss is defined by the physiological breakdown of transmission of sound to the interpretation by the brain (Shah & Lotke, 2015). A baby born with hearing loss is considered a negative event in health care. Children are screened at health care visits for possible hearing difficulties to intervene with the optimal care for the child’s development. One medical resource for HCPs states, Hearing deficits in early childhood can result in lifelong impairments in receptive and expressive language skills. The severity of the handicap is determined by the age at which the hearing loss occurred; the nature of the loss (its duration, the frequencies affected, and the degree); and the susceptibilities of the individual child. (Niparko, 2012, para. 2)
This excerpt illustrates the perspective of many HCPs regarding hearing loss as a pathological condition requiring treatment. The pathology definition is inexplicably linked with the disability view as the pathological view an inability or reduced ability leading to a disability viewpoint.
Cultural definition
The term Deaf has a different meaning for a significant linguistic minority of people. Those who identify as part of a cultural Deaf community typically were born with no hearing or experienced profound hearing loss at an early age. This early hearing loss is often referred to as early deafened or prelingually deaf. Prelingual deafness suggests that the hearing loss was severe enough and occurred early enough to make phonetic language development almost impossible. Most adults who are classified as having prelingual hearing loss use one of the visual–spatial languages, commonly known as sign language, for primary communication. One variation, ASL, is the dominant language among those who identify as part of Deaf culture in the United States. ASL is identified as the single most binding factor of Deaf culture, not the actual physiological state of deafness. Furthermore, many Deaf adults do not consider themselves disabled, as they feel quite capable of living full lives (Holcomb, 2013; Sheppard, 2014). For those who identify themselves with Deaf culture, “belonging to a linguistic community supersedes everything else and, for Deaf people, ASL brings them together” (Holcomb, 2013, p. 8). In contrast, people who have significant hearing loss after language development rarely communicate primarily in ASL.
Case Development
Wilson (1963) suggests presenting cases that fully represent the qualifiers of the concept to analyze a concept. Table 2 outlines analysis of key elements of the cases that follow.
Analysis of Essential Elements.
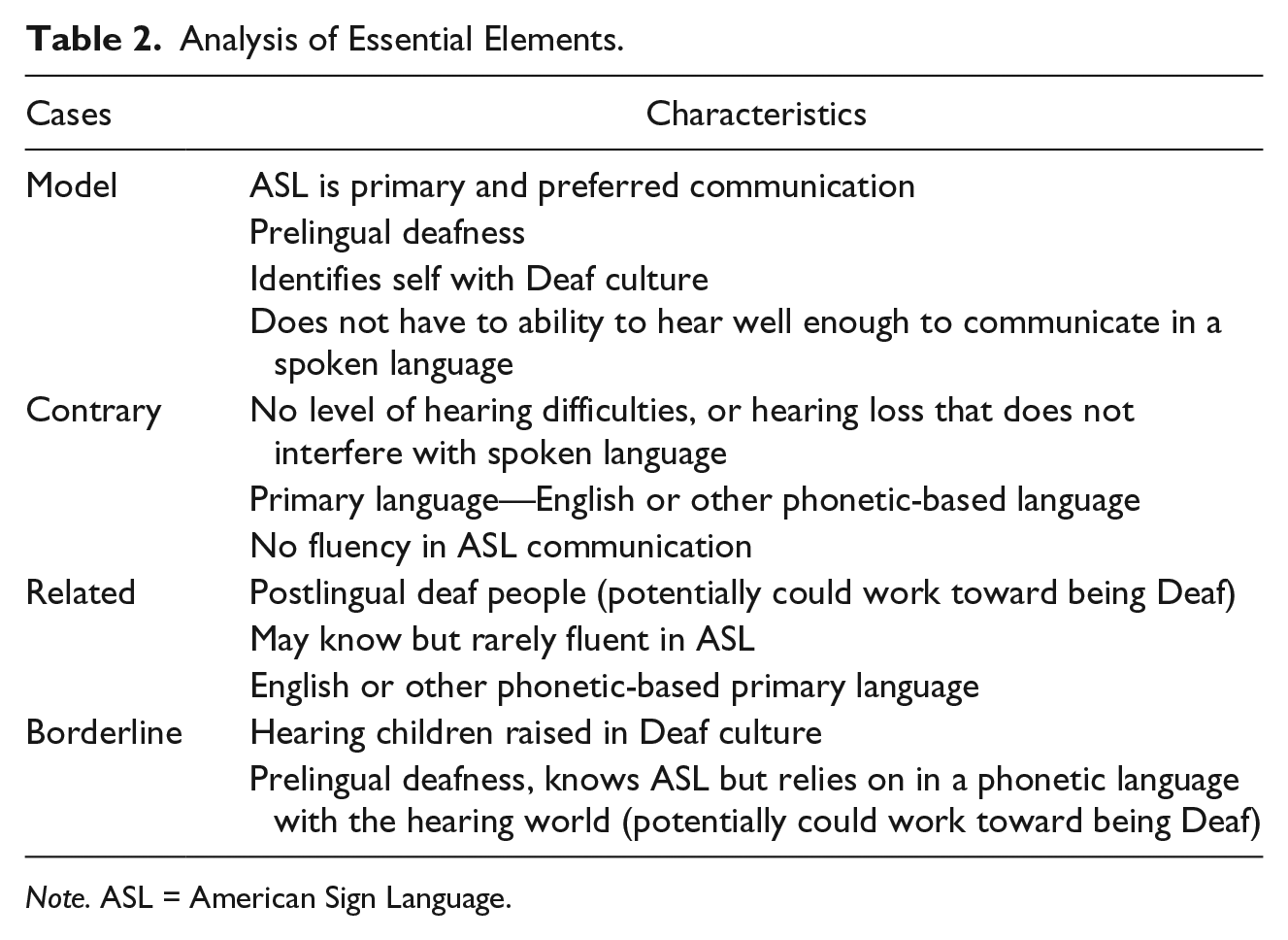
Note. ASL = American Sign Language.
Model Cases
Case 1
CC, a 30-year-old college graduate, was born with profound hearing loss and communicates primarily in ASL. She has several Deaf friends with whom she spends a significant amount of time and enjoys the long conversations and laughs they share. In the near future, CC plans to accompany her hearing parents on a trip to visit hearing relatives, which will entail 4 days of travel and 3 days of staying with relatives. She is looking forward to seeing her extended family but has a sense of dread as well. She knows her family loves and accepts her, but leaving her community means disconnecting herself from any fluent conversation for a full week. CC’s mother has tried to learn sign language but the only signing opportunity her mother has is with her daughter. With a full-time job and two other children, her mother has not been able to devote enough time to becoming fluent with ASL. Although CC and her mother can communicate fairly well with each other, the conversations are almost always fragmented and often end in feelings of frustration and exhaustion by both mother and daughter.
Case 2
MI, a 54-year-old male, experienced profound hearing loss at the age of 2 and communicates fluently in ASL with his wife and their friends, all whom are also Deaf. MI has begun having chest discomfort when he walks and seeks his friend’s advice. His friend suggests antacids for the discomfort. MI takes his friend’s advice, but antacids do not seem to help. As the discomfort becomes more frequent, MI has noticed that he gets short of breath easily with activity. MI’s wife, aware of his recent symptoms, expresses concern to her friend that this could be heart-related. Her friend assures her that MI is too young and healthy to have heart problems. The couple has not found a HCP with whom they can communicate so they are relieved the symptoms are not serious enough to seek treatment. MI continues to adjust his activity to reduce symptoms. Then one night, the pain becomes severe, is accompanied by shortness of breath, and is not relieved with rest or antacids. MI tells his wife he thinks he is dying. The wife drives her husband to the closest emergency room and hopes that someone will understand them enough to intervene in time to save her husband’s life.
Discussion
Key elements shared with both of the aforementioned cases include Deaf cultural identity, fluency of ASL communication with other people, primary language of ASL, early onset of deafness, and hearing loss significant enough to prevent development of a phonetic-based language.
Deaf people are generally very social with other Deaf people. They often work in environments where they cannot casually communicate with their hearing coworkers so they spend a lot of time with other Deaf people when possible. When they do not have contact with their cultural community, they often feel isolated in the hearing world where everyone around them is talking (Sheppard, 2014). Quite often, the only fluent conversation Deaf individuals ever experience is with other Deaf individuals. Because of the language barrier between Deaf adults and their families, Deaf persons usually identify with Deaf culture more than their families’ cultures. Horizontal or peer-to-peer transmission of attitudes, values, and beliefs are more common among the Deaf community than are the typical vertical parent to child transmission. Therefore, Deaf people frequently learn more from other Deaf members as this is often the only time they may be involved in fluent communication. Deaf adults often marry other members of their culture (Hauser, O’Hearn, McKee, Steider, & Thew, 2010). Logically, this is the population with whom they can communicate fluently (Pollard & Barnett, 2009). The horizontal transmission of information extends to health care also. Deaf children with hearing parents often do not experience learning through modeling of complex system navigation such as health care. These children are not able to learn through hearing/observation of patient–provider communication, exchange of information through appointments, medication instructions, and so on (Hauser et al., 2010). Deaf adults have expressed frustration with not knowing how to navigate the health care setting (Sheppard, 2014).
Contrary Cases
Contrary cases help to illustrate what the concept is not. This helps to identify elements that cause exclusion from the concept (Avant, 2000).
Case 1
RJ is a high school English teacher. She has been recognized for her exceptional teaching style and ability to teach students how to apply lessons to the art of oral debate. She had a child in her class 1 year who was hard of hearing, so she made adjustments to move the child to the front of the class. Other than that, she has no experience with people who are D/HH.
Case 2
HH is a 75-year-old man who worked around loud machinery without ear protection for many years. He now wears hearing aids in both ears and continues to have difficulty with hearing normal conversation. He complains that people around him mumble, and if they would just talk a little louder, he would be able to understand them.
Discussion
As noted in Table 2, key elements in the above scenarios that are contrary to the concept are hearing ability and use or preference to use a phonetic language. A contrary case of Deaf would be a person with no hearing loss, who is born into a family with hearing parents and hearing siblings. The person is able to hear, speak, and comprehend the English language fluently without communication aids. This population is generally referred to as “the hearing” (Holcomb, 2013). Another contrary case is the presence of hearing loss that may impede spoken communication, yet lacks key components of Deaf. Presbycusis, gradual hearing loss associated with the aging process, is a common condition (Shah & Lotke, 2015). This type of hearing loss is not connected with cultural identity of Deaf (Holcomb, 2013). The following cases help to illustrate.
Related Cases
Related cases are cases that share common components and may help to further clarify essential elements by analyzing what shared elements make them related (Avant, 2000).
Case
HI suffered irreversible profound hearing loss at age 10 after experiencing head trauma. Through extensive rehabilitation, HI has been able to regain his speaking abilities and has learned speech-reading. He has a small amount of residual hearing and uses hearing aids to amplify some sound. He has learned ASL and has achieved a high degree of proficiency. He sees HCPs on a regular basis and always asks for written literature when he does not fully understand.
Discussion
The case of HI demonstrates elements of physiological deafness, common to the hearing and medical definition. The essential element of fluency in ASL is also present. However, the use of a phonetic language as the preferred communication mode and postlingual deafness are contrary to the concept of Deaf.
Hearing loss that occurred after the development of phonetic language does not prevent oral communication, and does not usually influence cultural identity (Holcomb, 2013). Postlingual D/HH adults are less likely to primarily communicate using ASL but rather the language which was used in their home as a child. They may learn ASL to facilitate understanding as hearing loss worsens but because their first language was phonetically based, the needs and challenges of literacy and other communication are somewhat different. Because these individuals have a phonetic understanding of spoken language, they are the population who most often use speech-reading to compensate for hearing loss (Holcomb, 2013).
Borderline Cases
Borderline cases are helpful in identifying key elements that a case must have to be the concept. Borderline cases have similarities of the concept but are missing key components (Avant, 2000). Wilson recommends cases be deliberately designed to look very close to the concept to better identify the concept.
Case 1
MM, a 30-year-old female deaf since birth, was brought up in a home where no other family member was deaf. Her parents felt that learning sign language would further her disability and found a school that taught speech-reading. Learning to sign was discouraged; however, as MM grew older, gesturing to be understood became habit. She was fairly good at speech-reading, but as an adolescent, she also sought out sign language instruction. She communicates fairly well in both hearing and Deaf worlds but feels she does not completely fit in either world.
Case 2
HC, a 22-year-old woman, has never experienced hearing difficulties. However, her first language is ASL. Although fluent in both languages, English is a second language. Growing up with Deaf parents, HC has several Deaf friends. She has many stories of experiences as a child and adolescent interpreting for her parents in many encounters with the hearing world including health care visits. At the age of 17, HC recalls being horrified as she translated her father’s urinary difficulties and the HCP’s explanation of an enlarged prostate. Recently, she completed a rigorous education program to become a certified professional ASL interpreter. She works as a freelance certified ASL interpreter when work is available; however, she also works as a waitress because there is not enough demand for an ASL interpreter to support herself.
Discussion
The two cases above have some key elements of the concept Deaf. However, all the key elements are not present. In the first case, the person had hearing loss that prevented development of a phonetic language, and communicated well in ASL. However, MM’s first language was based on the English language. Her cultural identity lies somewhere in between the hearing and Deaf worlds (Maxwell-McCaw & Zea, 2011); however, she could potentially pursue stronger ties with the Deaf community (Hauser et al., 2010). With the second case, HC possesses the key components missing from the first case; however, HC does not have hearing difficulty that prevents her from developing phonetic language. Both cases not only have ties to Deaf culture but also identify with the hearing world.
Early deafened or prelingual deaf adults who are trained to use a form of communication other than ASL as their primary language are not considered by many Deaf people as a full member of their culture. Although they may not be able to use hearing to communicate, their primary use of a language other than ASL distinguishes them from the culture of the Deaf. They may interact within the Deaf community, but may be viewed somewhat as an accepted close outsider (Kusters & De Meulder, 2013).
Hearing children of Deaf parents are often reared in homes where ASL is the primary language. They are often fully accepted as a hearing member of Deaf culture. However, hearing children are exposed to spoken language regularly through television and hearing people around them. As these children grow and become school age, they are taught English and often become proficient in both ASL and English. Generally, as these children become adults and enter the hearing world, English becomes their most frequently used language. Children of deaf adults, referred to as CODAs, often refer to themselves as living between the hearing and Deaf worlds (Kusters & De Meulder, 2013), become advocates for the Deaf community in decreasing communication barriers, and often enter occupations related to deaf services (Pizer, Walters, & Meier, 2013).
Social Context and Underlying Anxiety
According to results of many studies, Deaf adults often report inadequate communication with HCPs, leading to misdiagnosis, medication errors, fear, embarrassment, mistrust, and avoidance of seeking health care (Ferguson-Coleman, Keady, & Young, 2014; M. M. McKee, Barnett, Block, & Pearson, 2011; Sheppard, 2014). In contrast, when culturally appropriate health care communication is delivered in ASL, Deaf adults have improved outcomes, higher levels of health care knowledge, more positive experiences with health care encounters, and increased participation in health promotion (Hickey et al., 2013; Jensen et al., 2013; Kuenburg, Fellinger, & Fellinger, 2016; M. M. McKee et al., 2011; M. McKee et al., 2011).
Practical Results
Extensive discussion is often necessary to clarify how the term d/Deaf is defined promoting Deaf awareness, educating hearing people about Deaf issues, and reporting Deaf scholarly research. Some of the terms used include Deaf ASL users (M. M. McKee, McKee, Winters, Sutter, & Pearson, 2014), culturally Deaf adults (Ferguson-Coleman et al., 2014), and Deaf linguistic minority (M. M. McKee et al., 2011). However, these terms must be continuously defined and explained.
Epidemiological data of persons who are d/Deaf vary widely, in part due to the differing definitions of d/Deaf. The inconsistencies result from differing or unclear inclusion/exclusion criteria as to who qualifies as d/Deaf. The ambiguity as to what is meant by d/Deaf influences the results of studies. One study may ask the participant to self-identify whether or not he or she is deaf while other studies may list subcategories such as degree of hearing difficulty or to what degree of disability the hearing difficulties cause A question asking Deaf people to identify themselves as deaf based on degree of disability is problematic because many Deaf people do not see themselves as having a disability (Hoang et al., 2011; Smith & Chin, 2012). In addition, Deaf community members are often excluded from studies due to linguistic challenges or delivery method such as telephone surveys (Barnett, McKee, Smith, & Pearson, 2011; Graybill et al., 2010; M. McKee et al., 2012; Pollard & Barnett, 2009). Adding to the complexity is the question of when does a person stop being considered hearing and begin being hard of hearing or deaf (Holcomb, 2013).
Results in Language
The health care community and members of Deaf culture have differing definitions of the term d/Deaf. While no one use is wrong, conflicting definitions occur when a person whose primary language is ASL enters the health care system. Use of the same term deaf for the medical view of the pathological state and the cultural identity of Deaf creates conflicting viewpoints about Deaf patients. HCPs must continue to consider the term deaf as pathologic in most of their clients and provide care to prevent or reduce potential disability. When providing health care for a Deaf person, the HCP is to consider the term Deaf not as pathological or disabling, but as a linguistic and cultural minority with specific communication needs. While HCPs want to provide optimal care in a culturally sensitive manner, those who are not completely immersed into the needs and issues of Deaf culture may be unprepared or ill equipped to provide health care for this population. The use of the same word for two very different approaches to patient care is problematic and may actually add to barriers to health care for Deaf.
Even when a HCP has many d/Deaf clients, established organizational protocols for hiring interpreters, and a current contact list for professional interpreters, the logistics of scheduling an interpreter and patient for a visit are complex. For a HCP in a rural clinic who rarely sees d/Deaf clients, and has no resources such as organizational protocol or contact information for obtaining an interpreter, the provision for effective communication is nearly impossible. Consider the following scenario: a 68-year-old Deaf person arrives at a busy family practice clinic as a new patient. The nurse tells the nurse practitioner the patient is deaf. In the 7 years, the nurse practitioner has been seeing patients, and she has seen several elderly people who have presbycusis. However, she has not had experience with a person whose primary language is ASL. For the nurse practitioner to provide effective communication, she must (a) recall what was learned in training about appropriate communication methods and accurately assess what is the best form of communication, (b) know or find the clinical protocol in obtaining and paying for interpreter services, (c) locate contact information for interpreters and arrange for the interpreter to come to the clinic, (d) have the interpreter and patient in the same room at the same time, and (e) begin the health care encounter with the patient. Unfortunately, even the first obstacle may never be overcome.
Conclusions, Implications, and Recommendations
The concept of d/Deaf as studied in this article refers to individuals who were born with limited hearing or developed hearing loss before acquiring a phonetic language and who use ASL as their primary language. The Deaf community is a cultural and linguistic minority within the United States, and is often overlooked by the hearing population (M. M. McKee et al., 2015).
Essential or typical elements of Deaf include prelingual deafness, preference for ASL as primary communication, identity with Deaf culture, and lack of the ability to hear well enough to communicate in a spoken language. Table 2 presents analysis of key elements.
Uses of the term d/Deaf vary within the context of the environment and with the user of the word. Unfortunately, the use of one word to refer to the level or absence of audiological ability, and a social context of a linguistic minority with unique makeup and needs influencing health care access continues to be a problem. The problem will likely continue to exist as long as one term simultaneously refers to a pathological condition potentially leading to disability and a sociocultural minority with a proud heritage of cultural identity. Currently, in the English language, the only way to clearly establish what a researcher, HCP, and/or Deaf person mean by the term d/Deaf is with a lengthy explanation. This is problematic when a Deaf person is seen in a busy clinic, where the decision of communication method must be made almost instantaneously. One recommendation is that a unique term defining Deaf as outlined in this conceptual analysis be created. Using a term other than d/Deaf may help to streamline education and Deaf awareness to the hearing population and HCPs leading to decreasing barriers to health care experienced by Deaf people. Holcomb (2013) points out, “Only when the communities determine the most appropriate labels and terms for themselves can they truly become liberated and empowered” (p. 58).
With the identification of a Deaf signer and awareness of communication barriers, the next step for the HCP is to provide effective communication. Some Deaf people believe HCPs have negative attitudes and misunderstand Deaf signer communication needs. Future research could explore HCP attitudes toward Deaf adults and knowledge of language barriers and determine whether these factors influence delivery of health care to Deaf signers. Yet, HCPs do not make decisions in isolation. In the complex environment of health care delivery, the HCP works within the health care laws and policies, professional and ethical guidelines, organizational structure, as well as demands of patient load and availability of resources such as support staffing. Because the responsibility for providing effective patient–provider communication falls to the HCP, barriers to providing this communication should be examined with consideration of the complexities of the health care environment in which the HCP delivers care.
This concept analysis demonstrates very different perspectives of the word d/Deaf. As HCPs, we must be aware of these views and make decisions as to the best way to communicate with a d/Deaf person. Understanding the different meanings is a first step to decreasing barriers to health care for Deaf people.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.